Embed Size (px)
DESCRIPTION
disease of mouth, esophagus, and stomach
Citation preview

Gastrointestinal PathologyDisease of the
Mouth,Esophagus and Stomach
DEPARTEMEN PATOLOGI ANATOMI
FK-UMI

DISEASES OF THE MOUTH

INFLAMMATIONS OF SALIVARY GLANDS

Mucoceles are most often found on the lower lip and are the result of trauma.
Clinically, they present as fluctuant swellings of the lower lip and have a blue translucent hue to them.
Histologically, mucoceles demonstrate a cystlike space that is lined by inflammatory granulation tissue or by fibrous connective tissue. The cystic spaces are filled with mucin as well as inflammatory cells, particularly macrophages.

Mucoceles. A, Fluctuant fluid-filled lesion on the lower lip subsequent to trauma. B, Cystlike cavity filled with mucinous material and lined by organizing granulation tissue.

Ranula is histologically identical to a mucocele. However, this term is reserved for mucoceles
that arise when the duct of the sublingual gland has been damaged.

CYSTS OF JAW AND ORAL CAVITY
Dentigerous cyst is defined as a cyst that originates around the crown of an unerupted tooth and is thought to be the result of a separation of the dental follicle.
Odontogenic keratocyst (OKC) is an important entity to differentiate from other odontogenic cysts because of its potential to be aggressive.
Periapical cyst (also called periapical granuloma), in contrast to the two lesions described above, is inflammatory in origin. These are extremely common lesions found at the apex of teeth.

TUMORS OF ORAL CAVITY AND OROPHARYNX

BENIGN TUMORS OF ORAL CAVITY

Ameloblastoma, which arises from odontogenic epithelium and shows no ectomesenchymal differentiation. It is commonly cystic, slow growing, and locally invasive but has a benign course in most cases.
Odontoma, the most common type of odontogenic tumor, arises from epithelium but shows extensive depositions of enamel and dentin. Odontomas are probably hamartomas rather than true neoplasms and are cured by local excision.

LEUKOPLAKIA
The term leukoplakia is defined by the World Health Organization as "a white patch or plaque that cannot be scraped off and cannot be characterized clinically or pathologically as any other disease."
Simply put, if a white lesion in the oral cavity can be given a specific diagnosis it is not a leukoplakia.
Found between ages 40 and 70, with a 2:1 male preponderance.
Lesions have multifactorial origins, the use of tobacco (cigarettes, pipes, cigars, and chewing tobacco) is the most common antecedent.

Leukoplakias may occur anywhere in the oral cavity (favored locations are buccal mucosa, floor of the mouth, ventral surface of the tongue, palate, and gingiva).
On histologic examination, they present a spectrum of epithelial changes ranging from hyperkeratosis overlying a thickened, acanthotic but orderly mucosal epithelium to lesions with markedly dysplastic changes sometimes merging into carcinoma in situ.

Leukoplakia. Clinical appearance of leukoplakias is highly variable and can range from A, smooth and thin with well-demarcated borders. B, diffuse and thick. C, irregular with a granular surface. D, diffuse and corrugated.

Clinical, histologic, and molecular progression of oral cancer. A, The typical clinical progression of oral cancer. B, The histologic progression of squamous epithelium from normal, to hyperkeratosis, to mild/moderate dysplasia, to severe dysplasia, to cancer. C, The sites of the most common genetic alterations identified as important for cancer development.

MALIGNANT TUMORS

At least 95% of cancers of the head and neck are squamous cell carcinomas (HNSCC), arising most commonly in the oral cavity.
Squamous cell carcinoma may arise anywhere in the oral cavity, but the favored locations are the ventral surface of the tongue, floor of the mouth, lower lip, soft palate, and gingiva.
The malignancies themselves are typically preceded by the presence of premalignant lesions.

a Well-diff erentiated squamous cell carcinoma. b Moderately differentiated squamous cell carcinoma. c Poorly diff erentiated squamous cell carcinoma

TUMORS OF SALIVARY GLANDS

About 65% to 80% arise within the parotid, 10% in the submandibular gland, and the remainder in the minor salivary glands, including the sublingual glands.
Approximately 15% to 30% of tumors in the parotid glands are malignant. In contrast, approximately 40% of submandibular, 50% of minor salivary gland, and 70% to 90% of sublingual tumors are cancerous.

These tumors usually occur in adults, with a slight female predominance, but about 5% occur in children younger than age 16 years.
The benign tumors most often appear in the fifth to seventh decades of life. The malignant ones tend, on average, to appear somewhat later.

PLEOMORFIC ADENOMA
Clinical Features. These tumors present as painless,
slow-growing, mobile discrete masses within the parotid or submandibular areas or in the buccal cavity.
The recurrence rate (perhaps months to years later) with parotidectomy is about 4% but, with simple enucleation, approaches 25%.


Morphology. Most pleomorphic adenomas present
as rounded, well-demarcated masses rarely exceeding 6 cm in the greatest dimension.
The cut surface is gray-white with myxoid and blue translucent areas of chondroid (cartilage-like).


Histopatologi The dominant histologic feature is the
great heterogeneity mentioned. The epithelial elements resembling ductal cells or myoepithelial cells are arranged in duct formations, acini, irregular tubules, strands, or sheets of cells. These elements are typically dispersed within a mesenchyme-like background of loose myxoid tissue containing islands of chondroid and, rarely, foci of bone


MUCOEPIDERMOID CARCINOMA
Morphology. Mucoepidermoid carcinomas can
grow as large as 8 cm in diameter and although they are apparently circumscribed, they lack well-defined capsules and are often infiltrative at the margins. Pale and gray-white on transection, they frequently contain small, mucin-containing cysts.

Histologi The basic histologic pattern is that of
cords, sheets, or cystic configurations of squamous, mucous, or intermediate cells. The tumor cells may be regular and benign appearing or, alternatively, highly anaplastic and unmistakably malignant. Accordingly, mucoepidermoid carcinomas are subclassified into low, intermediate, or high grade.


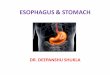
DISEASES OF THE ESOPHAGUS

Histology of esophagus
Low-power view of the normal esophagus showing the mucosa (M), submucosa (SM), and muscularis propria (MP).

CONGENITAL ANOMALIES
Ectopic tissue rests are not uncommon in the esophagus ectopic gastric mucosa in the upper third of the esophagus ("inlet patch”) most common, sebaceous glands or ectopic pancreatic tissue are much less frequent.
Embryologic formation of the foregut can also give rise to Congenital cysts.

ATRESIA and FISTULA
Atresia a segment of the esophagus is represented by only a thin, noncanalized cord, with a proximal blind pouch connected to the pharynx and a lower pouch leading to the stomach. It rarely occurs alone, but is usually associated with a fistula connecting the lower or upper pouch with a bronchus or the trachea.
Associated anomalies include congenital heart disease, neurologic disease, genitourinary disease, and other gastrointestinal malformations.

Esophageal atresia and tracheoesophageal fistula. A, Blind upper and lower esophageal segments. B, Fistula between blind upper segment and trachea. C, Blind upper segment, fistula between blind lower segment and trachea. D, Blind upper segment only. E, Fistula between patent esophagus and trachea. Type C is the most common variety.

WEBS, RINGS AND STENOSIS Esophageal mucosal webs are uncommon ledgelike
protrusions of the mucosa into the esophageal lumen. These are semicircumferential, eccentric, and most common in the upper esophagus. The webs consist of squamous mucosa and a vascularized submucosal core.
Esophageal rings are concentric plates of tissue protruding into the lumen of the distal esophagus. A ring located above the squamocolumnar junction of the esophagus and stomach .
B ring (Schatzki ring) located at the squamocolumnar junction of the lower esophagus. Histologically, these rings consist of mucosa, submucosa, and sometimes a hypertrophied muscularis propria.

Inferior esophageal ring formation

Esophageal stenosis consists of fibrous thickening of the esophageal wall, particularly the submucosa, with atrophy of the muscularis propria. The lining epithelium is usually thin and sometimes ulcerated.

ESOPHAGITIS


Viral esophagitis. A, Postmortem specimen with multiple herpetic ulcers in the distal esophagus. B, Multinucleate squamous cells containing Herpesvirus nuclear inclusions. C, Cytomegalovirus-infected endothelial cells with nuclear and cytoplasmic inclusions.

Esophagitis. A, Reflux esophagitis with scattered intraepithelial eosinophils. Although mild basal zone expansion can be appreciated, squamous cell maturation is relatively normal. B, Eosinophilic esophagitis is characterized by numerous intraepithelial eosinophils. Abnormal squamous maturation is also apparent.

BARRETT ESOPHAGUS
Barrett esophagus is a complication of chronic GERD that is characterized by intestinal metaplasia within the esophageal squamous mucosa.
Barrett esophagus is most common in white males and it typically presents between 40 and 60 years of age.
The greatest concern in Barrett esophagus is that it confers an increased risk of esophageal adenocarcinoma.

Clinical feature :Barrett esophagus can only be identified thorough endoscopy and biopsy, which are usually prompted by GERD symptoms.
Periodic endoscopy with biopsy, for detection of dysplasia, has an important role.
Macrocopically, Barrett esophagus can be recognized as one or several tongues or patches of red, velvety mucosa extending upward from the gastroesophageal junction.

Microscopically, diagnosis of Barrett esophagus requires both endoscopic evidence of abnormal mucosa above the gastroesophageal junction and histologically documented intestinal metaplasia.
Goblet cells, which have distinct mucous vacuoles that stain pale blue by H&E and impart the shape of a wine goblet to the remaining cytoplasm, define intestinal metaplasia and are necessary for diagnosis of Barrett esophagus.

Barrett esophagus. A, Normal gastroesophageal junction. B, Barrett esophagus. Note the small islands of paler squamous mucosa within the Barrett mucosa. C, Histologic appearance of the gastroesophageal junction in Barrett esophagus. Note the transition between esophageal squamous mucosa (left) and Barrett metaplasia, with abundant metaplastic goblet cells (right).

TUMORS OF THE ESOPHAGEAL

ADENOCARCINOMA
Adenocarcinoma of the esophagus typically arises in a background of Barrett esophagus and long-standing GERD.
Risk factor : dysplasia and is further increased by tobacco use, obesity, and prior radiation therapy.
Reduced by diets rich in fresh fruits and vegetables.
Esophageal adenocarcinoma occurs most frequently in Caucasians and shows a strong gender bias, being sevenfold more common in men.

Transition from Barrett esophagus to adenocarcinoma.

Clinical feature : pain or difficulty in swallowing, progressive weight loss, hematemesis, chest pain, or vomiting.
Macroscopically, Esophageal adenocarcinoma usually occurs in the distal third of the esophagus and may invade the adjacent gastric cardia. Initially appearing as flat or raised patches in otherwise intact mucosa, large masses of 5 cm or more in diameter may develop. Alternatively, tumors may infiltrate diffusely or ulcerate and invade deeply.

Microscopically Barrett esophagus is frequently present adjacent to the tumor. Tumors most commonly produce mucin and form glands , often with intestinal-type morphology; less frequently tumors are composed of diffusely infiltrative signet-ring cells (similar to those seen in diffuse gastric cancers) or, in rare cases, small poorly differentiated cells (similar to small-cell carcinoma of the lung).

SQUAMOUS CELL CARCINOMA
In the United States, esophageal squamous cell carcinoma occurs in adults over age 45 and affects males four times more frequently than females.
Risk factors include alcohol and tobacco use, caustic esophageal injury, achalasia, Plummer-Vinson syndrome, and frequent consumption of very hot beverages.

Clinical feature : dysphagia, odynophagia (pain on swallowing), obstruction, extreme weight loss and debilitation result from both impaired nutrition and effects of the tumor itself, hemorrhage and sepsis may accompany tumor ulceration.
Macroscopically, in contrast to adenocarcinoma, half of squamous cell carcinomas occur in the middle third of the esophagus. Early lesions appear as small, gray-white, plaque-like thickenings polypoid or exophytic and protrude into and obstruct the lumen. Other tumors are either ulcerated or diffusely infiltrative lesions that spread within the esophageal wall and cause thickening, rigidity, and luminal narrowing.

Microscopically, Most squamous cell carcinomas are moderately to well-differentiated. Less common histologic variants include verrucous squamous cell carcinoma, spindle cell carcinoma, and basaloid squamous cell carcinoma.

MALIGNANT TUMORS

MALIGNANT TUMORS

Esophageal cancer. A, Adenocarcinoma usually occurs distally and, as in this case, often involves the gastric cardia. B, Squamous cell carcinoma is most frequently found in the mid-esophagus, where it commonly causes strictures.

Microscopic view of malignant intestinal-type glands in adenocarcinoma arising from Barrett esophagus.

Squamous cell carcinoma of the esophagus: low-power microscopic view showing invasion into the submucosa.

Esophageal cancer. A, Esophageal adenocarcinoma organized into back-to-back glands. B, Squamous cell carcinoma composed of nests of malignant cells that partially recapitulate the organization of squamous epithelium.

DISEASES OF THE STOMACH

Anatomy and histology
Anatomy and histology of the stomach. A, Gross anatomy. B, Microscopic view of antral mucosa. C, Microscopic view of fundic mucosa.

GASTRITIS

ACUTE GASTRITIS
Acute gastritis is a transient mucosal inflammatory process that may be asymptomatic or cause variable degrees of epigastric pain, nausea, and vomiting. In more severe cases there may be mucosal erosion, ulceration, hemorrhage, hematemesis, melena, or, rarely, massive blood loss.

Mechanisms of gastric injury and protection. This diagram illustrates the progression from more mild forms of injury to ulceration that may occur with acute or chronic gastritis. Ulcers include layers of necrosis (N), inflammation (I), and granulation tissue (G), but a fibrotic scar (S), which takes time to develop, is only present in chronic lesions.

Clinical feature : depending on the severity of the anatomic changes, acute gastritis may be entirely asymptomatic; may cause variable epigastric pain, nausea, and vomiting; or may present with overt hemorrhage, massive hematemesis, melena, and potentially fatal blood loss.

Histologically, mild acute gastritis may be difficult to recognize, since the lamina propria shows only moderate edema and slight vascular congestion. The surface epithelium is intact, although scattered neutrophils may be present among the epithelial cells or within mucosal glands.

Acute gastritis. A, Gross view showing punctate erosions in an otherwise unremarkable mucosa; adherent blood is dark due to exposure to gastric acid. B, Low-power microscopic view of focal mucosal disruption with hemorrhage; the adjacent mucosa is normal.

Acute Gastric Ulceration Focal, acutely developing gastric mucosal defects are a well-known complication of therapy with NSAIDs, also appear after severe physiologic stress.
Some of these are given specific names, based on location and clinical associations :
Stress Ulcers Curling Ulcers Cushing Ulcers perforation

PEPTIC ULCERACUTE GASTRITIC ULCER

CHRONIC GASTRITIS
Chronic gastritis is defined as the presence of chronic mucosal inflammatory changes leading eventually to mucosal atrophy and intestinal metaplasia, usually in the absence of erosions. The epithelial changes may become dysplastic and constitute a background for the development of carcinoma.

The major etiologic associations of chronic gastritis are: • Chronic infection by H. pylori • Immunologic (autoimmune), in association with pernicious anemia • Toxic, as with alcohol and cigarette smoking • Postsurgical, especially following antrectomy with
gastroenterostomy with reflux of bilious duodenal secretions • Motor and mechanical, including obstruction, bezoars (luminal
concretions), and gastric atony • Radiation • Granulomatous conditions (e.g., Crohn disease) • Miscellaneous—amyloidosis, graft-versus-host disease, uremia.

Clinical feature : chronic gastritis usually causes few symptoms. Nausea, vomiting, and upper abdominal discomfort may occur. Individuals with advanced gastritis from H. pylori or other environmental causes are often hypochlorhydric, owing to parietal cell damage and atrophy of body and fundic mucosa.

Chronic gastritis, showing partial replacement of the gastric mucosal epithelium by intestinal metaplasia (upper left) and inflammation of the lamina propria (right) containing lymphocytes and plasma cells.

Helicobacter pylori. A Steiner silver stain demonstrates the numerous darkly stained Helicobacter organisms along the luminal surface of the gastric epithelial cells. Note that there is no tissue invasion by bacteria.

TUMORS OF THE STOMACH

BENIGN TUMORS OF STOMACH
Polyp is applied to any nodule or mass that projects above the level of the surrounding mucosa.
Uncommon: fundic gland polyps, hamartomatous Peutz-Jeghers polyps, and juvenile polyps.
The adenoma of the stomach constitutes 5% to 10% of the polypoid lesions in the stomach. By definition, an adenoma contains proliferative dysplastic epithelium and thereby has malignant potential.

BENIGN TUMORS OF STOMACH

MALIGNANT TUMOR OF STOMACH
Carcinoma is the most important and the most common (90% to 95%) of malignant tumors of the stomach. Next in order of frequency are lymphomas (4%), carcinoids (3%), and mesenchymal tumors (2%), which include gastrointestinal stromal tumors, leiomyosarcoma, and schwannoma.


Clinical feature : Gastric carcinoma is an insidious disease that is generally asymptomatic until late in its course include weight loss, abdominal pain, anorexia, vomiting, altered bowel habits, and less frequently dysphagia, anemic symptoms, and hemorrhage. As these symptoms are essentially nonspecific, early detection of gastric cancer is difficult.

The location of gastric carcinomas within the stomach is as follows: pylorus and antrum, 50% to 60%; cardia, 25%; with the remainder in the body and fundus.
Gastric carcinoma is classified on the basis of: (1) depth of invasion; (2) macroscopic growth pattern; and (3) histologic subtype.

(1) Depth of invasion. Early gastric carcinoma is defined as a
lesion confined to the mucosa and submucosa, regardless of the presence or absence of perigastric lymph node metastases.
Early gastric carcinoma ≠ carcinoma insitu Advanced gastric carcinoma is a neoplasm
that has extended below the submucosa into the muscular wall and has perhaps spread more widely.

(2) Macroscopic growth pattern Exophytic, with protrusion of a tumor mass
into the lumen; Flat or depressed, in which there is no
obvious tumor mass within the mucosa; Excavated, whereby a shallow or deeply
erosive crater is present in the wall of the stomach

Diagram of growth patterns and spread of gastric carcinoma. In early gastric carcinoma (A), the tumor is confined to the mucosa and submucosa and may exhibit an exophytic, flat or depressed, or excavated conformation. Advanced gastric carcinoma (B) extends into the muscularis propria and beyond. Linitis plastica is an extreme form of flat or depressed advanced gastric carcinoma.

CARCINOMA OF STOMACH

CARCINOMA OF STOMACH

CARCINOMA OF STOMACH

CARCINOMA OF STOMACH

CARCINOMA OF STOMACH

(3) Histologic subtype have been variously subclassified, but the
two most important types, as noted earlier, are the intestinal type and diffuse type of the Lauren classification.

Gastric carcinoma. A, Intestinal type demonstrating gland formation by malignant cells, which are invading the muscular wall of the stomach. B, Diffuse type demonstrating signet-ring carcinoma cells.

TERIMA KASIH