Embed Size (px)
Citation preview

Dislocated Wrap After PreviousReduction Aortoplasty CausesErosion of the Ascending AortaMatthias Bauer, MD, Onnen Grauhan, MD, PhD, andRoland Hetzer, MD, PhD
Department of Cardiothoracic and Vascular Surgery,Deutsches Herzzentrum Berlin, Berlin, Germany
We report a patient with bicuspid aortic valve anddilatation of the ascending aorta who had previous aorticvalve replacement and reduction aortoplasty with wrap-ping. After 4 years, reoperation because of coronaryartery disease and paravalvular leakage revealed an ero-sion of the aortic wall due to dislocation of the wrap. Thiscomplication confirms the need for secure anchoring andgood fitting of the Dacron wrap to avoid alterations of theunderlying aortic wall.
(Ann Thorac Surg 2003;75:583–4)© 2003 by The Society of Thoracic Surgeons
Reduction aortoplasty with or without external pros-thetic support is one of the operative techniques
currently used to treat patients with ascending aortadilatation and aneurysms [1, 2]. The surgical methodshows good long-term results [3]. Complications such asdevelopment of false aortic aneurysms or aortic ruptureare extremely rare [4, 5]. We present the intraoperativefinding of an ascending aorta erosion caused by a dislo-cated Dacron (C.R. Bard, Haverhill, PA) wrap in a patientwho had undergone aortic valve replacement and reduc-tion aortoplasty with external support 4 years before.
The patient underwent surgery in July 1997 at the age of50 years in another institution, involving aortic valvereplacement, reduction aortoplasty, and external Dacronwrapping of the ascending aorta because of combinedaortic valve disease and dilatation of the ascending aorta.He had a bicuspid aortic valve and the diameter of theascending aorta was 6.0 cm. The operation and theperioperative course were uneventful. In June 2001 hehad an acute myocardial infarction.
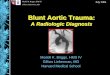
Coronary artery angiography showed a 75% stenosis ofthe left main trunk and angiography of the ascendingaorta revealed an indentation of the vessel in the regionof the inner curve (Fig 1). Echocardiography examinationshowed reduced left ventricular function, a paravalvularleakage at the aortic valve prosthesis, and a normaldiameter of the ascending aorta.
Reoperation was planned for aortic valve prosthesisreplacement, coronary artery revascularization, and in-spection of the ascending aorta for the cause of theindentation. Intraoperatively it became evident that theDacron wrapping had moved to the distal part of the
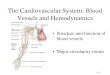
ascending aorta, creating a sharp fold at the inner curveof the vessel. Inspection of the inner surface of theascending aorta revealed extreme rarefaction of the aor-tic wall in the region of the fold of the Dacron wrap. Thetissue of the Dacron material was clearly visible thoughthe remnants of the aortic wall (Fig 2). Because of theimpending danger of rupture of the ascending aorta inthis region, we replaced the ascending aorta with avascular prosthesis using graft-inclusion technique, inaddition to undertaking coronary artery bypass graftingand aortic valve replacement. The patient left hospital onthe seventh postoperative day after an uneventful course.
CommentSurgeons can choose from a large spectrum of surgicaltechniques to handle ascending aortic pathology. Dilata-tion and aneurysms of the ascending aorta combinedwith aortic valve disease can be treated by separatereplacement of the aortic valve and ascending aorta, aswell as by composite graft implantation, valve-sparingascending aorta replacement, or the Ross procedure [6].
An alternative method is reduction aortoplasty with orwithout external prosthetic support as proposed by Ro-bicsek [1]. The procedure consists of replacing the aorticvalve, reducing the aortic diameter by excision of an ovalsegment of the aortic wall, placing a well-tailored Dacronvascular graft around the ascending aorta, and anchoringthe graft with previously placed sutures driven throughthe sewing ring of the valve prosthesis and through theaortic wall.
The technique is suitable for patients with fusiformaneurysms and poststenotic dilatation of the ascendingaorta [1, 2]. In patients with bicuspid aortic valve anddilatation of the ascending aorta Robicsek’s techniquealso shows good long-term results, when an optimal
Accepted for publication Aug 22, 2002.
Address reprint requests to Dr Bauer, Department of Cardiothoracic andVascular Surgery, Deutsches Herzzentrum Berlin, Augustenburger Platz1, 13353 Berlin, Germany; e-mail: [email protected].
Fig 1. Angiography of the ascending aorta in left anterior obliqueprojection shows an indentation of the vessel in the region of theinner curve (arrow).
583Ann Thorac Surg CASE REPORT BAUER ET AL2003;75:583–4 EROSION OF THE ASCENDING AORTA
© 2003 by The Society of Thoracic Surgeons 0003-4975/03/$30.00Published by Elsevier Science Inc PII S0003-4975(02)04338-2
CA
SE
RE
PO
RT
S

reduction in diameter (to less than 35 mm) is achievedperioperatively [3].
To prevent late complications, especially redilatation ofthe ascending aorta due to dislocation of the wrap, secureanchoring of the prosthetic wrap to the aorta is manda-tory. This is achieved in the Robicsek technique in theabove-mentioned fashion. Carrel sets the anchoringstitches in the noncoronary sinus and at the threecommissures.
Complications during the long-term course in patientswith aortoplasty and external wrapping are extremelyrare. Neri and colleagues [4] reported on 2 patients whodeveloped false aneurysm of the ascending aorta after 7and 11 years, respectively. Histologic examination of theaortic wall underlying the reinforcement cuff revealedextensive wall degeneration. Dhillon and associates [5]observed late ruptures after wrapping of descendingaorta aneurysms. In all 3 cases the aortic wall had beeneroded.
On reoperation after aortic valve replacement andreduction aortoplasty with wrapping, we found in 1patient that the Dacron wrapping had become dislocatedby moving to the distal part of the ascending aorta,creating a sharp fold at the inner curve of the vessel. Inthis region we noted extreme rarefaction of the aorticwall with impending rupture.
Or observation confirms the need for secure anchoringof the Dacron wrap when carrying out reduction aorto-plasty with external support. To avoid alterations of theaortic wall, the prosthetic wrapping has to be well fittedto prevent the creation of folds, which become areas ofhigh mechanical stress.
We are grateful for editorial assistance from Anne Gale.
References1. Robicsek F. A new method to treat fusiform aneurysms of the
ascending aorta associated with aortic valve disease: analternative to radical resection. Ann Thorac Surg 1982;34:92–4.
2. Carrel T, von Segesser L, Jenni R, et al. Dealing with dilatedascending aorta during aortic valve replacement: advantagesof conservative surgical approach. Eur J Cardiothorac Surg1991;5:137–43.
3. Bauer M, Pasic M, Schaffarzyk R, et al. Reduction aortoplastyfor dilatation of the ascending aorta in patients with bicuspidaortic valve. Ann Thorac Surg 2002;73:720–4.
4. Neri E, Massetti M, Tanganelli P, et al. Is it only a mechanicalmatter? Histologic modifications of the aorta underlying ex-ternal banding. J Thorac Cardiovasc Surg 1999;118:1116–8.
5. Dhillon JS, Randhawa GK, Straeley CJ, McNamara JJ. Laterupture after Dacron wrapping of aortic aneurysm. Circula-tion 1986;74(Suppl 1):11–4.
6. Ergin MA, Spielvogel D, Apaydin A, et al. Surgical treatmentof the dilated ascending aorta: when and how? Ann ThoracSurg 1999;67:1834–9.
Left Atrial Dissection After DoubleValve ReplacementMikio Ninomiya, MD, Shinichi Takamoto, MD, YutakaKotsuka, MD, and Toshiya Ohtsuka, MD
Department of Cardiothoracic Surgery, Faculty of Medicine,University of Tokyo, Tokyo, Japan
Left atrial dissection, a rare complication occurringmainly after mitral repair, is reported after double valvereplacement in a patient with a connective tissue disease.A 63-year-old woman with systemic sclerosis underwentdouble valve replacement. Laceration of the tissue be-tween the two mechanical prostheses and dissection ofthe left atrial wall emerged postoperatively and regurgi-tation through the dissection caused heart failure, whichlater improved without surgery. The possible causes ofthe dissection were thought to be shear forces against thetissue between the two prostheses and tissue fragilitydue to systemic sclerosis and corticosteroid therapy.
(Ann Thorac Surg 2003;75:584–6)© 2003 by The Society of Thoracic Surgeons
Left atrial dissection is an extremely rare complicationoccurring mainly after mitral valve repair. We en-
countered left atrial dissection after mitral and aorticvalve replacement in a patient with systemic sclerosisand herein report that case.
A 63-year-old woman who underwent open mitral com-missurotomy for rheumatic mitral stenosis in 1974 wasreferred to our hospital. She had congestive heart failuredue to mitral stenosis (mitral valve area was 1.1 cm2),aortic stenosis (pressure gradient was 43 mm Hg), andtricuspid regurgitation since July 2000. She also hadprogressive systemic sclerosis, which had been treatedsince 1992 with 2 mg a day of methylprednisolone.
Accepted for publication Aug 14, 2002.
Address reprint requests to Dr Ninomiya, 6-15-13-902 Hon-Komagome,Bunkyo-ku, Tokyo 113-0021, Japan; e-mail: [email protected].
Fig 2. Intraoperative inspection of the inner surface of the ascendingaorta reveals an extreme rarefaction of the aortic wall in the regionof the fold of the Dacron wrap (arrows).
584 CASE REPORT NINOMIYA ET AL Ann Thorac SurgLEFT ATRIAL DISSECTION 2003;75:584–6
© 2003 by The Society of Thoracic Surgeons 0003-4975/03/$30.00Published by Elsevier Science Inc PII S0003-4975(02)04301-1
CA
SE
RE
PO
RT
S