Embed Size (px)
Citation preview

30
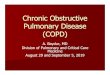
DISORDERED PULMONARY FUNCTIONIN EMPHYSEMA
By E. J. MORAN CAMPBELL, M.D., Ph.D., M.R.C.P.Assistant, The Medical Unit, The Middlesex Hospital, London, W.I
IntroductionThe remarkable advances in pulmonary physio-
logy during the last decade have provided newtechniques with which to analyse the complexdisorders present in lung disease. The increasedprecision of these new methods has led to theappearance of symbols, equations, graphs and thefrightening paraphernalia of mathematics. Themain aim of this article is to show how thesemeasurements have improved our understandingof emphysema by discussing the data obtainedfrom one patient who has been extensivelystudied. Although the various disorders havebeen separated into groups for the purposes ofdiscussion it is important to realize that they areall interrelated.A complete assessment of emphysema (or any
other lung disease) requires many measurements.However, as so often happens, improved physio-logical knowledge has led to improved ability tointerpret clinical evidence. Therefore, at the end,I have suggested a simple scheme for the evalua-tion of emphysema making use of clinical informa-tion and tests most of which are so simple as to bewithin the capabilities of any reasonably equippedhospital.
In the various tables and illustrations reasonablenormal values for a man of 60 years have beengiven for comparison. No technical details aregiven in the text. For the further elucidation ofthe underlying pulmonary physiology referenceshould be made to 'The Lung' (Comroe,Forster, Dubois, Briscoe and Carlsen, I955).References are only given to aspects of the subjectnot covered in that work.
Clinical DetailsThe patient (Mr. F.H.T.), a motor engineer, is
aged 59, 5 ft. 9 in. tall and I.8 sq.m. in surfacearea. He has suffered from increasingly severedyspnoea for 33 years. There is no history oflongstanding cough or sputum preceding theonset of dyspnoea. He has been increasinglyincapacitated for the last seven years and beforeadmission could only walk 25 yards. He hascontinued to work by driving his car from the door
of his house to the desk in the garage where he isemployed. Climbing the 14 stairs in his housecauses intense distress lasting o to I5 minutesand often forcing him to kneel on the stairs. Hehas not walked out of the front gate of his housefor ten years nor had a pair of shoes repaired forseven years. He has great difficulty in dressinghimself and in eating his food. In recent yearshe has had a variable amount of mucoid sputumwhich causes bouts of coughing leading to intensedyspnoea, and interrupting his sleep every fewhours. He sleeps more comfortably lying flatthan when propped up. Clinically and radio-logically he has the changes of severe emphysema.He is cyanosed at rest and becomes very cyanosedon slight exertion. There is no clinical evidenceof heart failure. On screening the right ventricleis moderately enlarged and the main pulmonaryarteries are prominent. E.C.G. shows an in-complete right bundle branch block. Repeatedbacteriological examination of the sputum has notshown any pathogenic organism to be persistentlypresent. The Hb concentration is 19 g. perIoo ml. and the P.C.V. 63 per cent.By way of introduction some personal data and
the results of some simple well-known pulmonaryfunction tests performed on him are shown inTable i.
TABLE I
Mr. F.H.T. Normal
Age (year) .. .. .. 59Height (in.) .... .. 69Weight (lb.) .. .. 135Surface area (sq. m.) ... x.8Vital capacity (L./B.T.P.) . . 2.4 4Forced exp. vol. in i sec.
(L./B.T.P.) . .. .. 0.75 3.2Max. vol. ventilation (M.B.C.)
(L./min.) .. .. 24 > IooArterial CO2 tension (mm. Hg.) 58 40Arterial 02 saturation (per cent.) 82 >95
Evidence of EmphysemaThe lungs in emphysema are voluminous,
inelastic and there is destruction of alveoli,alveolar walls and lobular septa, and of pulmonarycapillaries. This sentence briefly summarizes the
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

January 1958 CAMPBELL: Disordered Pulmonary Function in Emphysema
pathological description of the condition which, inthe absence of knowledge of a specific lesion, is theonly way in which the disease can be identified.The first physiological studies to be described arethose which satisfy these three criteria: increasein volume, inelasticity, loss of functioning lungsurface.
TABLE 2
LUNG VOLUMES
Mr. F.H.T. Normal
Total lung capacity, L./B.T.P. 10.3 7.oResidual volume .. .. 7.9 3.0Vital capacity .. .. .. 2.4 4.0Inspiratory capacity ... . .7 3.oFunctional residual capacity .. 8.6 4.0
12 -
FEV, T10 - EMPHYS. ./-10-75
VC 24
VOLUMEL. 1
4* 19 RESID.VOL.
RESID.2 VOL.
SECS. O 1 4 8
FIG. I.-The lung volumes and the forced vital capacity.V.C., vital capacity; F.E.V.1 forced expired volumein i sec.
The Volume of the Lungs (Table 2 and Fig. I)There is increase in the resting volume of the
lungs (the Functional Residual Capacity, F.R.C.).There is also increase in the volume of air whichcannot be expelled by a voluntary expiratory effortso that this residual volume represents 77 per cent.of the total lung capacity. At the age of 60 theresidual volume should only be 45 per cent. oftotal lung capacity.The Elastic Properties
Before considering the elastic properties of thelungs the term ' elasticity' must be discussedbecause as commonly used it has not the samemeaning as it has to the physicist or physiologist.Strictly, elasticity is the property of a substance or
structure by virtue of which it returns to itsoriginal shape and dimensions when a deformingforce has been removed. Thus a rubber balloonis elastic if after it has been inflated it will emptyitself to its original volume. If it remainspartially inflated then it has partially lost itselasticity. No unit of measurement is employed.If a physicist wishes to describe how much a sub-stance will change its dimensions in response to adeforming force he determines the modulus ofelasticity which relates stress to strain. When aphysiologist wants to describe the distensibility ofthe lungs he measures their compliance, that is thechange in volume (the strain) produced by a givenchange in pressure (the stress). In Fig. 2 the
12 -
10
EMPHYSEMA
8 -
LUNGVOL.L.
NORMAL
2 -
O I a a_ _ I I
O 2 4 6 12 18
RECOIL PRESSURE cm H,O
FIG. 2.-The elastic properties of the lungs. Thisdiagram relates the volume of the lungs to theirelastic recoil pressure as measured in the pleura oroesophagus.
volume of the lungs is plotted against the oeso-phageal pressure. (The oesophageal pressureclosely resembles intrapleural pressure and there-fore may be used to study the pressure developedwhen the lungs are distended.) It can be seenfirstly, that when the oesophageal pressure isatmospheric (that is when the lungs are relaxed)their volume is 8 1. instead of 3 1. That is to saythey have partially lost their elasticity. Secondly,for any given change in oesophageal pressure thelungs change in volume more than they ought to.Their compliance (900 ml./cm. HO2) is greaterthan normal (250 ml./cm.). Conversely, for anygiven volume of distension they exert less recoilpressure (i.I cm. H20/l. instead of 4.0 cm. H20/I.).
Dl
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

32 POSTGRADUATE MEDICAL JOURNAL January 1958
The Area and Permeability of the Alveolar-capillary MembraneThe volume of 02 or CO2 which diffuses across
the alveolar-capillary membrane per minutedepends upon the following factors: the differencein the partial pressure of the gas between thealveolar air and the pulmonary capillary blood;the solubility of the gas; the area and thickness ofthe membranes and fluid barriers between thealveolar air and the red blood corpuscles; the rateof certain physico-chemical processes within thered cell. Of these factors the most importantphysiologically is the solubility of the gas. CO2is much more soluble than 02 and consequentlydiffuses 20 times more rapidly. The importantconsequence of this difference between the twogases is that disease processes which destroy thealveolar-capillary surface or make it less permeablehave a much greater effect on O2 uptake by theblood than on CO2 output. So great is thedifference, in fact, that O2 uptake becomes inade-quate to support life before a significant CO2pressure difference between the pulmonary capil-lary blood and the alveolar air appears.
In an attempt to study changes in the alveolar-capillary membrane physiologists measure theoxygen diffusing capacity, which is defined as thevolume of 02 which crosses from the alveolar airto the pulmonary capillary blood per unit pressuregradient per unit time. The units of diffusingcapacity are therefore ml. of O2/mm. Hg./min.The O2 diffusing capacity (Do2) is difficult to
measure for a number of physiological andtechnical reasons. Therefore carbon monoxide isnow widely used for the measurement of thediffusing capacity (Dco) because its diffusionproperties are similar to those of 02, and becauseits affinity for haemoglobin removes some of thedifficulties.Apart from disease the diffusing capacity can be
affected by other factors notably physical exercisewhich raises it by increasing the number offunctioning pulmonary capillaries. It is custo-mary, therefore, to specify the level of activity atwhich the measurement was made. The condi-tions of most clinical interest are the resting diffus-ing capacity and the maximum diffusing capacity.
In Table 3 it can be seen that the diffusingcapacity measured by three different methods wasfound to be very low. If we take the value for themaximum diffusing capacity we can calculate thesignificance of this measurement. The Do2(Max) is 8 ml. 02 per min. per mm. Hg. tensiondifference between the alveolar air and thepulmonary capillary blood. If the alveolar 02tension was normal (about Ioo mm. Hg.) and themean 02 tension in the pulmonary capillarieswas o mm. Hg. (which is impossible) the greatest
TABLE 3THE DIFFUSING CAPACITY
Mr.F.H.T. Normal
Resting diffusing capacity, ml./CO/min. mm. Hg.:CO (single breath method) .. 2.7 15CO (steady state method) .. 4.2 15
Maximal diffusing capacity (02method), ml./O2/min. mm. Hg. .. 8 40
The single breath Dco was measured by the method ofOgilvie et al. (I957). The steady state Dco wasmeasured by Method II of Bates et al. (I955). TheDo, was measured by Riley's method. The valuesobtained for Dco and Do, are not directly comparablebecause CO and 0, have different physical properties.They can be approximately compared by using thefollowing ratio:
Do, = 1.3 X Dco
volume of 02 that could be taken up by his lungswould be 800 ml./min. In fact, as his alveolarPo, is about 80 mm. Hg. and the mean pulmonarycapillary Po2 is about 15 mm. Hg. on exercise, thenthe maximum 02 uptake he can achieve is onlyabout 520 ml./min. Such a severe reduction indiffusing capacity is unusual.
The Mechanics of BreathingEvidence has already been presented that the
lungs have partially lost their elasticity and havebecome abnormally distensible. These changes,together with changes in the walls of the airways,are probably of dominant importance in mostcases of emphysema.Airway Obstruction
It is well known that patients with emphysemahave difficulty in expelling the air during expira-tion. In Fig. i it can be seen that the volume ofair expelled by Mr. F.H.T. in i sec. (ForcedExpired Volume in i sec., F.E.V.1) is only 0.75instead of 3.2 1. A normal subject expels all hisvital capacity in less than 4 secs., whereas expira-tion was still proceding after 8 sec. in the emphy-sematous patient when he had to give up and takeanother breath.
Expiratory obstruction in emphysema is usuallyattributed to ' bronchospasm' or other processesin the walls of the airways, whereas in fact most ofthe airway obstruction is due to loss of elasticityand there may be relatively little organic narrowingof the airways.The resistance of the respiratory passages to
airflow can be estimated by measuring the pressuredifference between the mouth and the alveolar airand dividing it by the rate of airflow at the instantthe measurement was made. The value obtainedis called the flow, non-elastic, or viscous resistance.
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

January 1958 CAMPBELL: Disordered Pulmonary Function in Emphysema 33TABLE 4
THE MECHANICAL PROPERTIES OF THE LUNGS
Mr. F.H.T. Normal
Lung compliance (zero frequency), ml./cm. H20 .. 900 250Elastic resistance of lungs (elastance), cm. H20/l:During slow inspiration .. ....... . 4.0Breathing frequency 19 per min. .. . .. 7.9 4.0
Non-elastic Resistance (flow-or viscous-resistance),cm. H20/l./sec.:
Interrupter method ... .. .... 3.7 <3.oOesophageal pressure method . .. 47 <2.5
Maximum effective intrathoracic pressure, cm. H20 . 2 > 25
The units are usually cm. HO2/l./sec. [Thereare several methods by which one can attempt tomeasure the pressure of the air in the alveoli (seeComroe et al, chap. 7). There are theoreticaland technical difficulties about each of them, butthese difficulties detract little from their valuein clinical studies of chronic lung disease.] InTable 4 the resistance to airflow during inspirationis shown to be less than twice the normal valuewhereas in asthma the flow resistance is usuallyfive to ten times the normal value. The flowresistance was measured during inspiration becauseduring expiration the airways are narrowed byexternal pressure and the flow resistance measuredunder these conditions is very variable and doesnot represent the resistance due to organicnarrowing of the airways. In most patients withemphysema the resistance to airflow duringinspiration is increased, presumably because thereis associated bronchitis. This increase in re-sistance is however, small compared with thatoccurring in asthma and may, as in the present case,be relatively slight. The obstruction to expirationin emphysema is not due to ' bronchospasm ' butto the loss of lung elastic recoil. Expiration duringnatural breathing both at rest and on exercise isproduced by the passive recoil of the lungs(Campbell, 1958). The recoil pressure of thelungs, as it drives the air up the airways, maintainsthe pressure in them above that in the surroundingintrapleural space. This mechanism is sufficientfor all physiological levels of ventilation in healthbut not in emphysema. In emphysema theelastic recoil of the lungs is largely lost. If anattempt is made to accelerate the rate of airflow byusing expiratory muscles then the intrapleuralpressure narrows the airways as well as increasingalveolar pressure. The flow resistance may thenrise to very high levels. In the present case itexceeded 80 cm. H20/l./sec. during a forcedexpiration. One can measure the level of intra-pleural pressure at which the airways are socompressed that their resistance is greatly in-creased to the point at which no further increase inflow rate occurs with increasing effort. This
maximum effective intrathoracic pressure (Camp-bell, Martin and Riley, 1957) in normal subjects isapproximately 30 cm. HO2. In Mr. F.H.T. it is2 cm. H2O.These factors which cause obstruction to
expiration also impair the efficiency of coughing.The linear velocity of the airflow in the trachea ofMr. F.H.T. during coughing is probably aboutoo00 miles per hour instead of about 600 m.p.h.The Mechanics of Breathing and the MaximumBreathing Capacity and Forced Vital CapacityTestsA patient's performance in these very useful
tests of ventilatory function is limited by the flowresistance of his airways during expiration.Unfortunately these tests do not distinguishbetween the mechanisms which may be re-sponsible for the resistance. Thus results may beobtained in a patient during an attack of asthma,whose lungs are not affected by emphysema,which are similar to those found in a patient withairway obstruction due to loss of elastic support inwhom there is little ' bronchospasm.'
It is to be hoped that the application of morerefined techniques will enable the influence of thedifferent mechanisms to be separately evaluatedin individual patients.The Mechanics of Breathing and the Distributionof VentilationThe respiratory exchanges between the alveolar
air and the pulmonary capillary blood shouldideally take place with the minimum of ventilationand pulmonary capillary blood flow and with themaintenance of normal arterial blood composition.If perfection is to be achieved, the distribution ofventilation relative to blood flow must be the samein all parts of the lungs. To take an extremeexample, the ventilation of one lung and theperfusion of the other will not result in adequategaseous exchange whatever the volume of ventila-tion or pulmonary blood flow. Similar reasoningapplies at the alveolar level. If every alternatealveolus is overventilated and every other one is
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

34 POSTGRADUATE MEDICAL JOURNAL January 1958
O -5 cm HO2FIG. 3A
20- B
15VOLUME I
10
I
III
l
I I
X Y ZTIME -
FIG. 3BFIG. 3.-The mechanical properties of the lungs srnd
the distribution of ventilation.
overperfused then the arterial blood will not benormal. In Fig. 3a a simple situation is showndiagrammatically to illustrate how the mechanicalproperties of the lungs affect the distribution of air.Two 'lung units' (e.g. alveoli, lobules, lobes) areshown which are assumed to have equal volume(say, io c.mm.). One of these (A) is less dis-tensible than the other so that when the pressurearound them is lowered to -5 cm. H20 it enlargesto 15 c.mm. while the other (B) enlarges to20 c.mm.
Therefore, if they both have the same capillary-blood flow, then B will be overventilated relativeto A. Of course, compensation can occur byadjusting the capillary blood flow so that moregoes to B than to A. However, this compensationmay be difficult to achieve particularly if thefollowing factors are also considered. The air-way leading to A is shown to be wide and offeringlittle resistance to airflow whereas that to B is
shown to be narrow. In Fig. 3b the effect ofthis difference on the ventilation of A and B isconsidered. It is assumed that at point X thepressure round them is suddenly reduced to-5 cm. H20. Air will rapidly enter A whichenlarges to 15 c.mm. Air enters B more slowlyand it does not reach its final volume of 2o c.mm.for some time. If the surrounding pressurereturned to its resting value at point Y then Awould have been more ventilated than B, whereasif it did not return until Z, then B would have beenmore ventilated than A. Thus, at a high rate ofbreathing A would be more ventilated than B,and at a low rate of breathing B would be moreventilated than A.The effect of the rate of breathing on the distri-
bution of ventilation cannot yet be shown directlybut, following the more advanced reasoning ofOtis et al. (I956), we can strongly suspect that itexists in Mr. F.H.T. because the apparent elasticrecoil pressure exerted by his lungs increases athigher rates of breathing. [In Table 4 it can beseen that the apparent elastic resistance whenbreathing at I9 per minute in a normal subject isthe same as the true static elastic resistance;whereas in Mr. F.H.T. the apparent elasticresistance of the lungs at 19 breaths per min. was7.9 cm. H20/1. compared with a true elasticresistance of I.I. cm. H20/1. This difference isexplained by the fact that there is a true cessationof airflow throughout the lungs of the normalsubject at the end of inspiration, whatever the rateof breathing. In the patient with emphysema,on the other hand, although airflow through themouth stops at the end of inspiration there arestill pressure differences between different partsof the lungs which cause airflow to continuewithin the lungs themselves. These factors causethe pressure difference between the pleura and themouth to be greater than it is under truly staticconditions.]The Distribution of Ventilation andPulmonary Blood Flow
If all alveoli receive the same amounts of air andof blood then the cencentration of the gases in allthe alveoli will be the same. Even in normalsubjects these perfect conditions of distributionare not achieved and in emphysema distribution isfar from perfect. This imperfection can beanalysed by using the concept of' ideal' alveolarair.
In any subject with a given alveolar ventilationand a given pulmonary capillary blood flow withmixed venous blood of a given composition, thecomposition of the air in each alveolus will varydepending upon the ratio of ventilation to bloodflow. The ' ideal' alveolar air composition for
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

January 1958 CAMPBELL: Disordered Pulmonary Function in Emphysema 35
TABLE 5DISTRIBUTION OF VENTILATION AND PULMONARY BLOOD FLOW
Mr. F.H.T. Normal
Physiological dead space, ml. .. .. .. . 330 i6oPhysiological dead space as per cent. of tidal volume .. 66 30Alveolar-arterial O2 tension difference, mm. Hg. . . 50 < oVenous-admixture or ' shunt effect,' per cent. of cardiac
output .. ... .. .. .. 30 <5Mixing efficiency, per cent. .. .. .. .. 44 >76Alveolar N2 per cent. after 7 min. 0, breathing, per cent. 6.5 <2.5
any subject under given conditions is that compos-tion which every alveolus would have if they allhad the same ventilation in relation to blood flow.Alveoli which have too great a ventilation will havea lower CO2 tension and a higher 02 tension thanthe ' ideal ' value. Alveoli which have too great avolume of blood flow will have a higher CO2*tension and a lower 02 tension than the 'ideal'value. Now, let us assume that a particularalveolus has 0.5 of the 'ideal' CO2 concentrationand that it contributes x ml. of alveolar air to theexpired air. This x ml. can be regarded as beingequivalent to x/2 ml. of 'ideal' alveolar air, andx/2 of unchanged, inspired or dead space air.Let us now turn to the pulmonary circulation andassume that a particular alveolus has too muchblood flow so that the blood only takes up o.5 ofthe amount of 02 which is required to bring it tothe 'ideal' value. If this alveolus has y ml. ofblood flow then its contribution to the arterialblood can be regarded as equivalent to y/z ml. of'ideal' blood and y/2 ml. of mixed venous orshunted blood.
In a normal subject the volume of the pulmonarydead space is approximately equal to the volumeof the conducting airways. In Table 5 it can beseen that the dead space in Mr. F.H.T. is 170 ml.greater than normal. Most of this increase is dueto ventilation of parts of the lung where thecapillary circulation is relatively inadequate.
In normal subjects there is a slightly unevendistribution of pulmonary blood flow which, asexplained above, causes a 'shunt-like' effect.There are also small volumes of 'true' shuntthrough bronchial and Thebesian veins. Togetherthe' true ' shunt and' shunt-like ' effects cause theadmixture of a volume of mixed venous bloodequal to about 2 to 5 per cent. of the cardiac output.In table 4 the apparent shunt in Mr. F.H.T. willbe seen to equal 30 per cent. of the cardiac output.(The great bulk of this apparent shunt must bedue to the impaired distribution of blood flow,because his arterial blood becomes fully saturatedif he breathes Ioo per cent 02. If he had much'true' shunt, breathing 02 would not producefull saturation.)
Distribution of Inspired AirIn the above account the term ' distribution' is
used to describe ventilation in relation to pul-monary blood flow. It can also be used in thesense of spatial distribution of the air within thelungs. Using the term in this sense, perfectdistribution implies that all alveoli during inspira-tion receive at the same time air of the samecomposition and in an amount proportional totheir volume. There are several techniques bywhich the degree of perfection of the distributionof air in this sense can be estimated. Most ofthem depend upon suddenly changing thecomposition of the inspired air and studying thechanges in the composition of the expired air inrelation to time. Thus, if there are parts of thelungs which receive too small a proportion of theinspired air they will take longer to reach a newsteady level. The unevenness of distribution ofthe inspired air in Mr. F.H.T. was assessed by twomethods. First, he breathed Ioo per cent. O2 for7 mins. and at the end of that time his alveolar aircontained 6.5 per cent. N2 instead of the expectedvalue of less than 2.5 per cent. This findingshows that there are large parts of his lungs whichare poorly ventilated and from which the N2 wasnot' washed out.' Secondly, we used the methodof Bates and Christie (1950), which depends uponthe rate of mixing of a foreign gas (helium) in thelungs. The normal 'mixing efficiency' by thistechnique is over 70 per cent. In Mr. F.H.T. thevalue was 44 per cent.
The Control of BreathingIn normal subjects and even in patients with
severe disease of the lungs the arterial CO2 tensionis maintained at 40 mm. Hg. (± 5 mm.). Thisstability is achieved because the respiratory centreis very sensitive to changes in the arterial CO2tension and adjusts the ventilation accordingly.In some patients with very severe lung disease thearterial CO2 tension is elevated. In the presentcase that value is about 60 mm. Hg. showing thatthe alveolar ventilation is only 2/3 of that requiredto keep the tension normal. Initially this raisedPco2 would seem to suggest that the respiratory
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

36 POSTGRADUATE MEDICAL JOURNAL January I958
TABLE 6THE WORK OF BREATHING
Mr. F.H.T. Normal
At Rest (ventilation 9.l/min.):Mechanical work, KgM./min .. .. .... 0.7 0.4Oxygen cost, ml. 02/min. . .. .. .. 20-30 5Efficiency, per cent. .. .. .. .. .. -2 5-Io
Exercise (ventilation x6.1/min.):Total 02 consumption, ml./min. .. .. .. 500 50002 consumption of respiratory muscles, ml./min. .. 80-Ioo Io
The data were obtained by the methods of Campbell, Westlake, and Cherniack (I957).The normal values for a man of 60 are not known with any confidence.
centre has lost some of its sensitivity to CO2.However, most of the CO2 retention can probablybe explained by the mechanical difficulty inventilating the lungs. (The mechanical difficultyrequires greater muscular force. Greater muscularforce required a greater discharge from therespiratory centre. The greater discharge by therespiratory centre demands a greater stimulation-a higher arterial CO2 tension.) It is not yet knownwhether or not there is, in addition to the mechani-cal limitation, a true diminution of the sensitivityof the respiratory centre to Pco2 in emphysema.The excessive reduction of ventilation whenanoxia is relieved suggests that there probably issome alteration in sensitivity to CO2 tension.When breathing Ioo per cent 02 our patient'sarterial Pco2 rose from 60 to 70 mm. Hg. showingthat the alveolar ventilation had decreased byabout I5 per cent. This is only a moderatechange compared with those seen in patients whodevelop CO2 narcosis.
The Respiratory MusclesThe intercostal, external oblique and sterno-
mastoid muscles were examined electromyo-graphically (Campbell, I958). The lower inter-costals and the sternomastoids were found tocontract during inspiration even at rest. Theyrelaxed completely during expiration. There wasno expiratory muscle activity even when he wasbreathless. The diaphragm cannot be examinedelectromyographically but on clinical examinationand screening it was found to be very low andflattened so that the base of the thorax was con-stricted instead of expanded by its contraction;the vertical excursion during quiet breathing wasless than i cm. (normal I.5 cm.); during forcedexpiration the diaphragm initially was depressedinstead of elevated and its subsequent ascent wasslow and jerky.The Work of BreathingThe mechanical work performed by the respira-
tory muscles could be calculated if the pressureexerted by them and the volume of air displaced
by this pressure were measured. Unfortunatelysuch measurements are difficult to make. Themetabolic work performed by the respiratorymuscles can be calculated by estimating their O2consumption. Table 6 shows that the work ofbreathing and the 02 consumption of the respira-tory muscles is somewhat increased in Mr. F.H.T.at rest and greatly increased at higher levels ofventilation. These studies of the work of breathingwere made with the subject seated and with hisback, shoulders and head supported to obtainmaximum relaxation of the accessory muscles.When standing without such support there wasclearly much more effort involved and the OScostof breathing must have been even greater. Itappeared, in fact, that at 12 to 14 l./min. (hisventilation when standing) he had no O2 to sparefor exercise and if he increased his ventilation the02 cost of breathing was greater than the extraOg intake.
The Arterial BloodIn Table 7 the 02 tension at different levels in
the pathway from inspired air to arterial blood atrest and during exercise are shown for Mr. F.H.T.and a normal subject. The level of exercise inMr. F.H.T. was sufficient to double his 02consumption. (In a normal subject the valuesquoted would remain substantially the same up tomuch greater levels of exercise.) The relativeimportance of the various abnormalities can beappreciated. Thus the severe fall in arterial 02tension on exercise can be seen to be due to thelow diffusing capacity. Underventilation couldhave played no part in this arterial desaturationbecause the alveolar air composition did notchange.The inter-relationships between the arterial
pH, CO2 tension, total CO2 content and bicar-bonate-concentration are very important in theunderstanding of the acidosis of pulmonaryemphysema. They are, however, problems whichdemand an account of acid base regulation whichspace does not permit. For an understanding of
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

January 1958 CAMPBELL: Disordered Pulmonary Function in Emphysema 37
TABLE 7OXYGEN TRANSPORT
Mr. F.H.T. Normal Physiological Explanation ofRest Exercise Rest and Exercise Difference
Arterial CO2 tension, mm. Hg .. .. 60 6o 40 Alveolar underventilation at rest.Not more marked during exersice
Inspired O2 tension (room air), mm. Hg. I50 150 150Alveolar O2 tension, mm. Hg. .. .. 80 80 Ioo Alveolar underventilationPulmonary end capillary 02 tension:mm. Hg. .. .. .. .. 75 35 99.9 Lo diffusing capacitySaturation, per cent... 93 6o 98.5using capacity
Arterial O0 Tension:mm. Hg .... ..... 50 25 95 Xmm. Hg. .. .. .. .. 50 25 95 Venous admixture effectSaturation, per cent. .. .. 82 40 98s J
a xte
Rounded figures are given to simplify comparisons.
them, reference should be made to Comroe et al.,or to Davenport (I950).The Assessment ofa Patient with Emphysema
Studies such as have been described in thisarticle are outside the range of any but a fewcentres. It is, however, desirable that much moreattention be paid to the assessment of patients withchronic lung disease of all types. At the presenttime the attention paid to the assessment of thesepatients compares very unfavourably with thatdevoted to those with heart, liver or kidney disease.The individual patient benefits from such
studies because diagnosis, progress and theresponse to treatment are all much better assessedwhen objective measurements as well as the usualclinical data are available. Furthermore, ourunderstanding of this very neglected group ofconditions-asthma, bronchitis, emphysema-willimprove if we can advance beyond the purelydescriptive clinical criteria which at present areall that we have for defining these conditions.
Unfortunately, those who are tempted toemploy pulmonary function tests are often dis-mayed by the array that face them. They hopefor a single simple test that will give them a figureor a value which will tell them how ' good' thepulmonary function is. It should be clear fromthis article that there is no single test that canadequately assess all patients with chronic lungdisease. However, provided one has an apprecia-tion of the elements of pulmonary physiology, avery good assessment can be made of any patientusing clinical data and tests that are all within thecapacity of a reasonably equipped hospital. Irecommend that when faced with a patient withchronic lung disease one should ask threequestions:
(I) How good is the mechanical or bellowsfunction of the lungs ?
(2) Is ventilation adequate to maintain a normalarterial CO2 tension ?
(3) Are the processes affecting O2 uptake in thelungs adequate for the maintenance of the normalarterial 02 concentration ?
I will now suggest how these questions can beanswered at three levels of precision.
I. These questions can often be simplyanswered at least partially by physical examinationalone:
(I) The bellows function can be assessed bylooking for the signs of reduced chest movementor airway obstruction.
(2) Ventilation is probably inadequate if thepatient has a raised pulse rate and other evidenceof vasodilation. Unfortunately, ventilation ismost likely to be inadequate when there is an acuterespiratory infection in a patient with chroniclung disease. In those circumstances the signsof underventilation and CO2 retention are oftenobscured by those of infection and heart failure.It must be stressed that the absence of cyanosis isnot evidence of adequate ventilation. Alveolarventilation must be reduced almost by half beforesignificant arterial desaturation occurs.
(3) The adequacy of 02 uptake in the lungs canbe assessed by exercising a patient to the limit oftolerance. If cyanosis does not develop, then thediffusing capacity and the distribution of pul-monary blood flow are adequate, and the limit torespiratory exchange is being set by the ventilation.
II. Very simple tests which will suffice in themajority of patients are as follows:
(I) The mechanical function can be assessed byany of the following: fluoroscopy; the F.E.V.1test (Forced Expired volume in i sec.); theM.B.C.; or (less satisfactory) the Vital Capacity.
(2) The adequacy of ventilation can be assessedby measuring the plasma CO2 content, bicarbonateconcentration or (less satisfactory) the alkalireserve.
(3) The adequacy of 02 uptake in the lungs canbe assessed by measuring the arterial 02 saturation
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from

38 POSTGRADUATE MEDICAL JOURNAL January 1958
(for clinical purposes an ear oximeter is adequate)at rest and exercise.
III. More complex measurementsi but whichshould be well within the capabilities of any centretaking a special interest in these conditions are asfollows:
(i) The elastic properties of the lungs and theirresistance to airflow.
(2) The arterial pH and CO2 tension.(3) The alveolar-arterial 02 tension difference
and, possibly, the diffusing capacity.If facilities for such studies are available then the
more advanced techniques referred to in thisarticle will be within range.
It is preferable that the development offacilities should be as even as possible. It isunbalanced, say, to spend large sums of moneyon an apparatus for measuring differential lungfunction or the CO diffusing capacity in alaboratory where the arterial blood CO2 tensioncannot be measured.
SummaryThe disordered pulmonary function in emphy-
sema is described using data obtained from onepatient.
An approach to the problem of pulmonaryfunction assessment is suggested.-0
AcknowledgementsI wish to thank Dr. R. M. Marshall and Dr.
G. H. Apthorp who performed the Dco deter-minations and some of the mechanics studies atSt. Bartholomew's Hospital. I would also liketo thank Professor Kekwick, Dr. P. S. Andrews,Dr. C. J. Dickinson and Dr. E. K. Westlake forreading the manuscript.
BIBLIOGRAPHYBATES, D. V., BOUCOT, N. G., and DORMER, A. E. ('955),
9'. Physiol., 129, 237.BATES, D. V., and CHRISTIE, R. V. (I950), Clin. Sci., 9, 17.CAMPBELL, E. J. M. (5958), 'The Respiratory Muscles and the
Mechanics of Breathing,' London, Lloyd-Luke.CAMPBELL, E. J. M., MARTIN, H. B., and RILEY, R. L. (1957),
Bull. Johns Hopk. Hosp., in press.CAMPBELL, E. J. M., WESTLAKE, E. K., and CHERNIACK,
R. M. (I957), J. appi. Physiol, ii, 303.COMROE, J. H., FORSTER, R. E., DUBOIS A B BRISCOE,
W. A., and CARLSEN, E. A. (I95S), 'The Lung,' Chicago,Year Book.
DAVENPORT, H. W. (I950), 'The ABC of Acid-Base Chemistry,'Chicago, Univ. of Chicago Press.
OGILVIE, C. M., FORSTER, R. E., BLAKEMORE, W. S., andMORTON, J. W. (1957), J. clin. Invest., 36, I.
OTIS, A. B., McKERROW, C. B., BARTLETT, R. A., MEAD, J.McILROY, M. B., SELVERSTONE, M. J., and RADFORD,E. P. (s956),J. appl. Physiol., 8, 427.
ANAESTHEICS(Postgraduate Medical Journal)
Price: 3s. 9d. post free
THE MODERN VIEW OF ANAESTHSIA CHLORPROMAZINE AND ALLIEDG. S. W. Organe, M.D., D.A., F.F.A.R.C.S. SUBSTANCES
THE PRODUCTION OF John Beard, M.D., D.A., F.F.A.R.C.S.,UNCONSCIOUSNESS D.C.H.B. G. B. Lucas, D.A., F.F.A.R.C.S. CONTROLLED HYPOTHERMIA
ANALGESIA E. J. Delorme, M.D., F.R.C.S.(C.)J. B. Wyman, M.B.E., D.A., F.F.A.R.C.S. MANAGEMENT OF THE APNOEIC
MUSCLE RELAXATION IN SURGERY PATIENTAngus Smith, F.F.A.R.C.S. Ronald Woolmer, D.A., F.F.A.R.C.S.
CONTROL OF THE BLOOD PRESSURE THE USE OF ANTIDOTES INAND CONTROLLED HYPOTENSION ANAESTHESIAC. F. Scurr, M.V.O., D.A., F.F.A.R.C.S. B. A. Sellick, D.A., F.F.A.R.C.S.
Published by
THE FELLOWSHP OF POSTGRADUATE MEDICINE
60, Portland Place, London, W.1
copyright. on M
ay 16, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.34.387.30 on 1 January 1958. D
ownloaded from