Embed Size (px)
Citation preview
Disorders of Sodium and Disorders of Sodium and Potassium MetabolismPotassium Metabolism
OutlineOutline
1.1. Review of sodium and potassium Review of sodium and potassium metabolismmetabolism
2.2. Paradigm for analyzing pathophysiologyParadigm for analyzing pathophysiology
3.3. Abnormalities of potassium balanceAbnormalities of potassium balance
4.4. Abnormalities of sodium and water Abnormalities of sodium and water balancebalance
5.5. Example casesExample cases
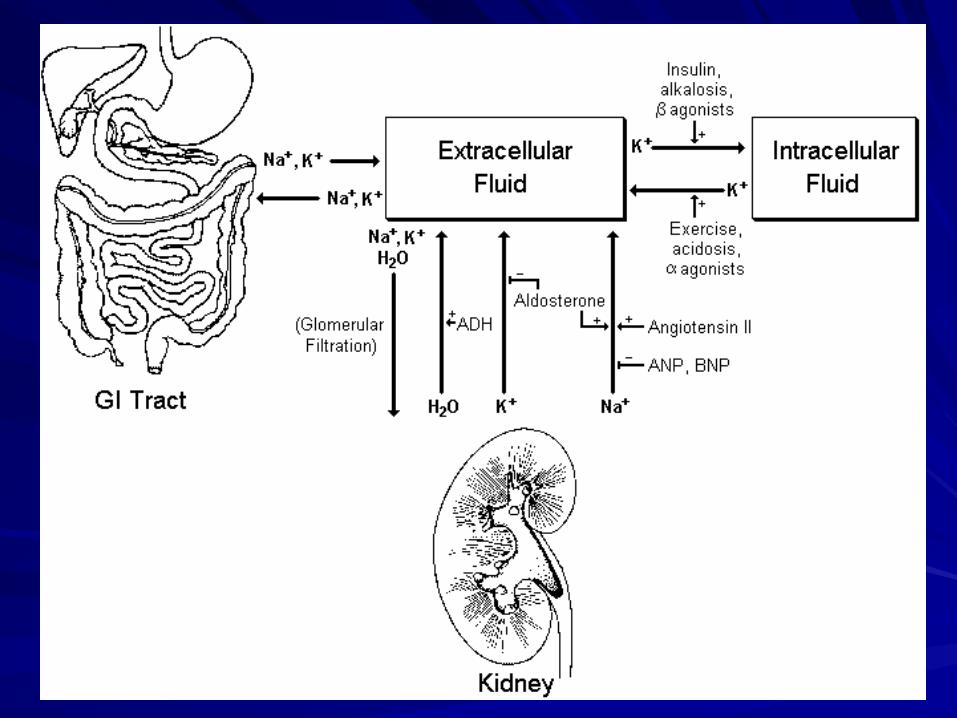
Major Mediators of Sodium and Major Mediators of Sodium and Water BalanceWater Balance
Angiotensin IIAngiotensin II
AldosteroneAldosterone
Antidiuretic hormone (ADH)Antidiuretic hormone (ADH)
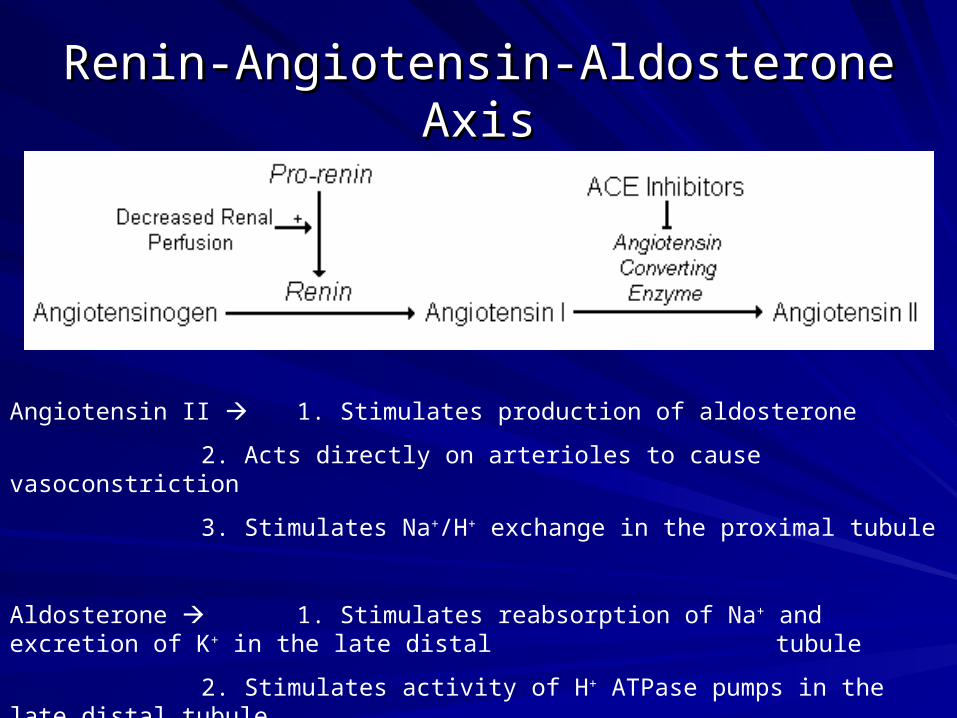
Renin-Angiotensin-Aldosterone AxisRenin-Angiotensin-Aldosterone Axis
Angiotensin II 1. Stimulates production of aldosterone
2. Acts directly on arterioles to cause vasoconstriction
3. Stimulates Na+/H+ exchange in the proximal tubule
Aldosterone 1. Stimulates reabsorption of Na+ and excretion of K+ in the late distal tubule
2. Stimulates activity of H+ ATPase pumps in the late distal tubule
Role of ADH (antidiuretic hormone)Role of ADH (antidiuretic hormone)
Synthesized in the hypothalamus and stored in the Synthesized in the hypothalamus and stored in the posterior pituitaryposterior pituitary
Released in response to plasma hyperosmolality and Released in response to plasma hyperosmolality and decreased effective circulating volumedecreased effective circulating volume
Actions of ADH Actions of ADH 1. Increases the water permeability 1. Increases the water permeability of of the collecting tubulethe collecting tubule
2. Mildly increases vascular 2. Mildly increases vascular resistanceresistance
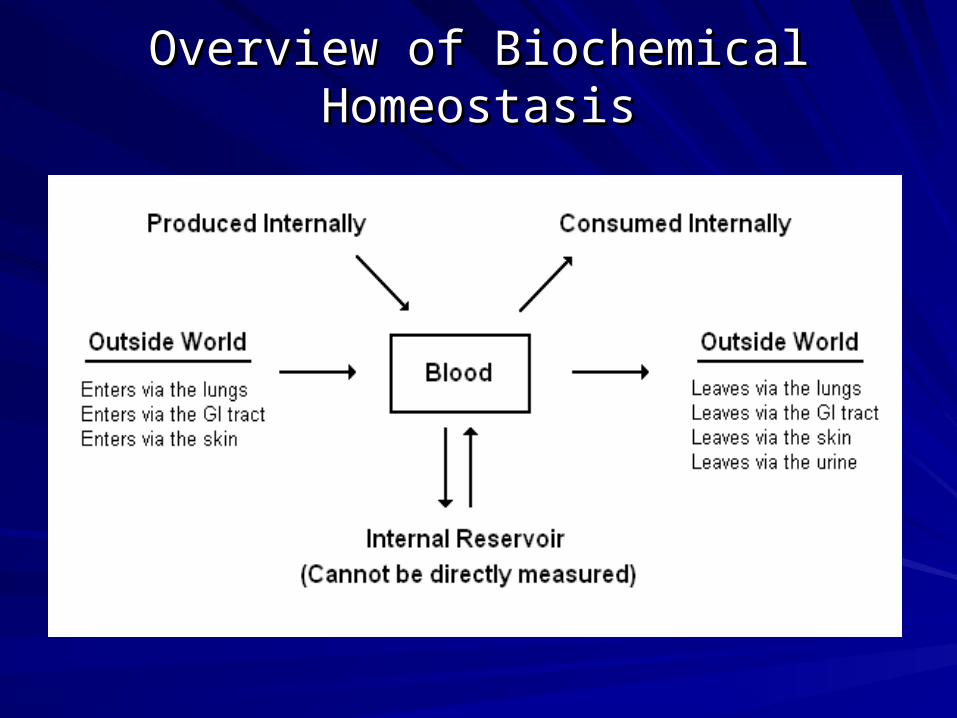
Overview of Biochemical HomeostasisOverview of Biochemical Homeostasis
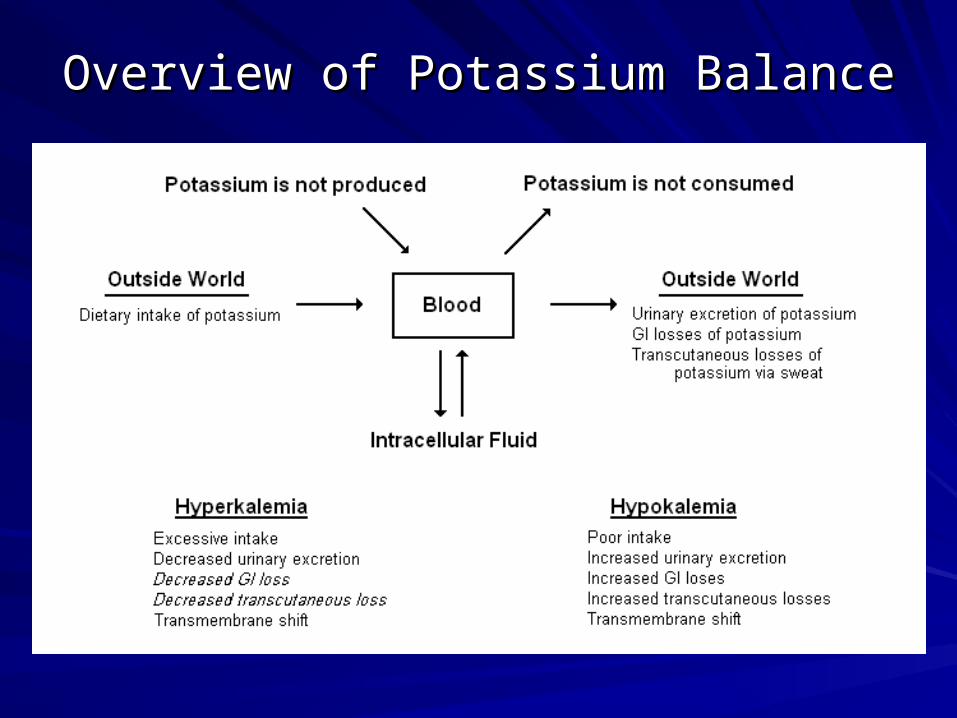
Overview of Potassium BalanceOverview of Potassium Balance

Etiologies of HyperkalemiaEtiologies of Hyperkalemia
Excessive Dietary Intake
Decreased Urinary Excretion
Decreased GFR
Aldosterone deficiency
Adrenal insufficiency
ACE inhibitors
Hyporeninemic hypoaldosteronism
Diabetic nephropathy
Aldosterone resistance
Potassium sparing diuretics
Internal Redistribution
Transmembrane Shift
Acidosis
Exercise
Cell Lysis
Rhabdomyolysis
Tumor lysis syndrome
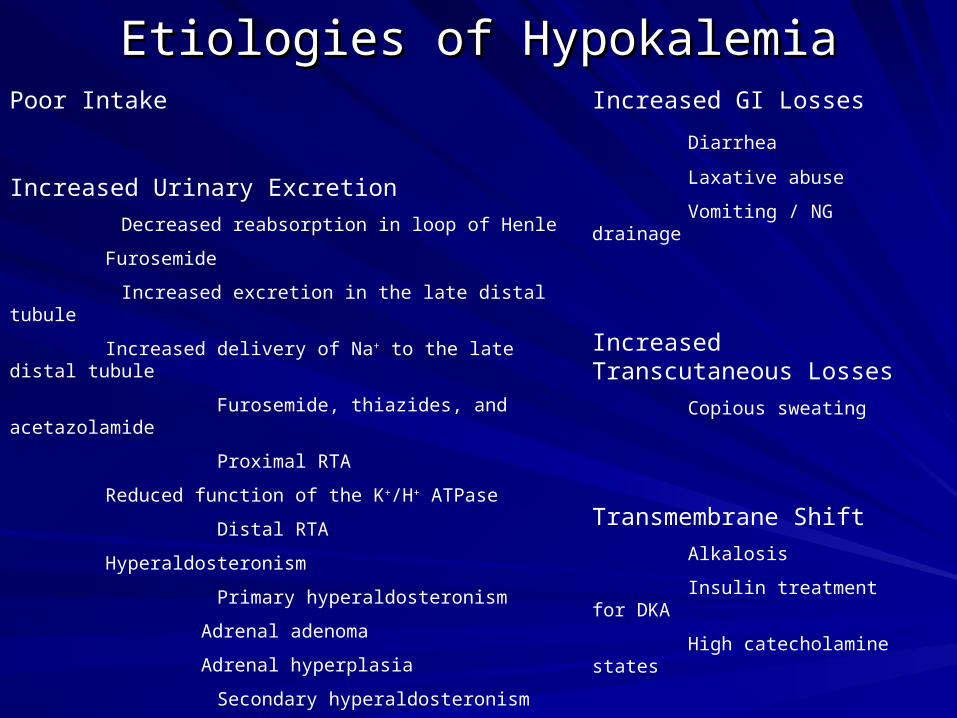
Etiologies of HypokalemiaEtiologies of HypokalemiaPoor Intake
Increased Urinary Excretion
Decreased reabsorption in loop of Henle
Furosemide
Increased excretion in the late distal tubule
Increased delivery of Na+ to the late distal tubule
Furosemide, thiazides, and acetazolamide
Proximal RTA
Reduced function of the K+/H+ ATPase
Distal RTA
Hyperaldosteronism
Primary hyperaldosteronism
Adrenal adenoma
Adrenal hyperplasia
Secondary hyperaldosteronism
Renovascular hypertension
Renin-secreting tumor
Increased GI Losses
Diarrhea
Laxative abuse
Vomiting / NG drainage
Increased Transcutaneous Losses
Copious sweating
Transmembrane Shift
Alkalosis
Insulin treatment for DKA
High catecholamine states
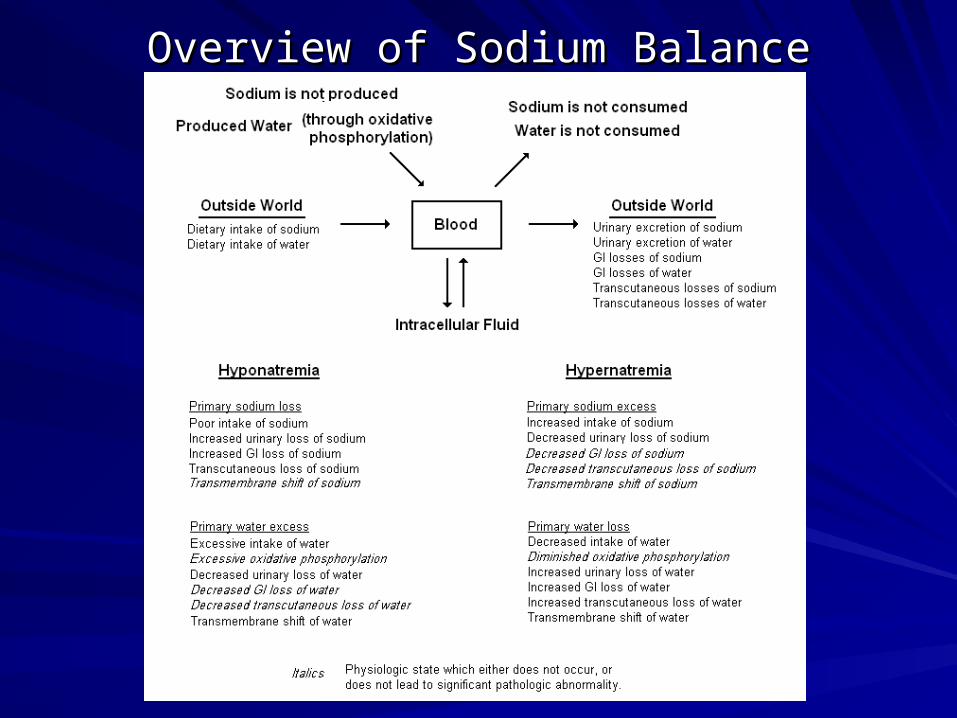
Overview of Sodium BalanceOverview of Sodium Balance
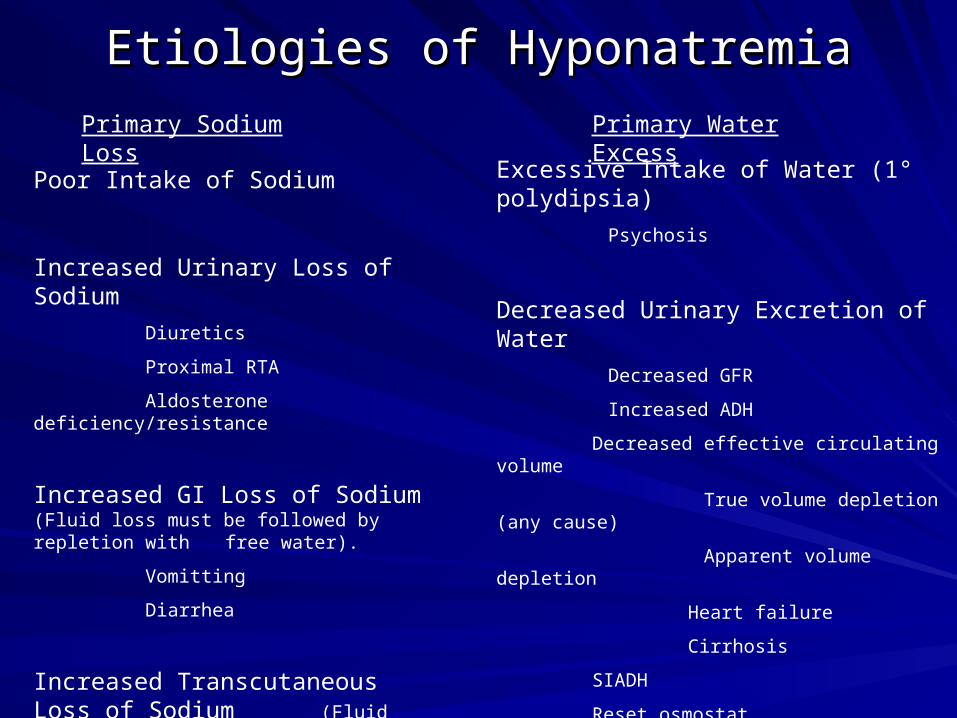
Etiologies of HyponatremiaEtiologies of Hyponatremia
Poor Intake of Sodium
Increased Urinary Loss of Sodium
Diuretics
Proximal RTA
Aldosterone deficiency/resistance
Increased GI Loss of Sodium (Fluid loss must be followed by repletion with free water).
Vomitting
Diarrhea
Increased Transcutaneous Loss of Sodium (Fluid loss must be followed by repletion with free water).
Excessive Intake of Water (1° polydipsia)
Psychosis
Decreased Urinary Excretion of Water
Decreased GFR
Increased ADH
Decreased effective circulating volume
True volume depletion (any cause)
Apparent volume depletion
Heart failure
Cirrhosis
SIADH
Reset osmostat
Transmembrane Shift of Water
Hyperglycemia
Primary Sodium Loss Primary Water Excess
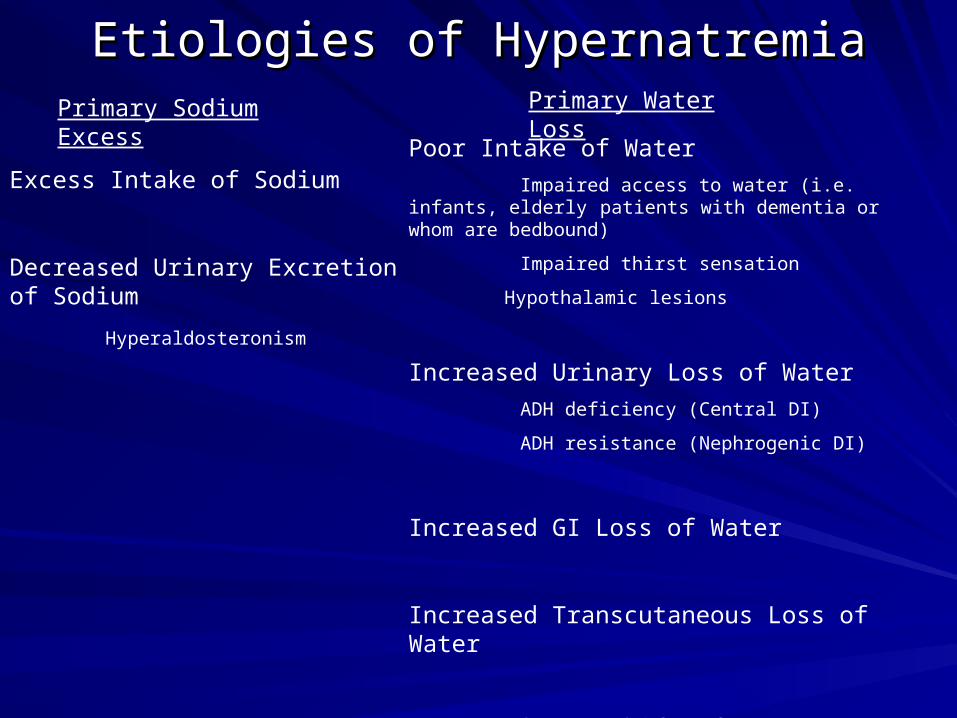
Etiologies of HypernatremiaEtiologies of HypernatremiaPrimary Sodium Excess
Excess Intake of Sodium
Decreased Urinary Excretion of Sodium
Hyperaldosteronism
Primary Water Loss
Poor Intake of Water
Impaired access to water (i.e. infants, elderly patients with dementia or whom are bedbound)
Impaired thirst sensation
Hypothalamic lesions
Increased Urinary Loss of Water
ADH deficiency (Central DI)
ADH resistance (Nephrogenic DI)
Increased GI Loss of Water
Increased Transcutaneous Loss of Water
Transmembrane Shift of Water (most often due to rapid production of intracellular lactate)

Case 1Case 1
Mrs. L is a 62 y/o woman with a past medical history Mrs. L is a 62 y/o woman with a past medical history significant only for hypertension. She has a 45 pack year significant only for hypertension. She has a 45 pack year smoking history. She comes to the urgent care clinic today smoking history. She comes to the urgent care clinic today complaining of a cough and shortness of breath for the past complaining of a cough and shortness of breath for the past week. Her physical exam is notable for both mild wheezing week. Her physical exam is notable for both mild wheezing and rhonchi, more pronounced on the right side than the and rhonchi, more pronounced on the right side than the left.left.
Labs include the following:Labs include the following:
Na 126Na 126 Cl 95Cl 95 BUN 12BUN 12 Glucose 102Glucose 102
K 4.4K 4.4 HCOHCO33 25 25 Cr 1.4Cr 1.4
Her CBC shows mild normocytic anemia.Her CBC shows mild normocytic anemia.
Case 2Case 2
Mr. R is an 85 y/o man with advanced dementia who was Mr. R is an 85 y/o man with advanced dementia who was sent to the ER from his skilled nursing facility for non-sent to the ER from his skilled nursing facility for non-responsiveness since the morning nursing shift started responsiveness since the morning nursing shift started about 8 hours ago. The remainder of his past medical about 8 hours ago. The remainder of his past medical history is unknown. Aside from his mental status, his history is unknown. Aside from his mental status, his physical exam is remarkable for a HR of 110 and BP of physical exam is remarkable for a HR of 110 and BP of 100/50.100/50.
Labs include the following:Labs include the following:
Na 164Na 164 Cl 126Cl 126 BUN 50BUN 50 Glucose 98Glucose 98K 4.8K 4.8 HCOHCO33 28 28 Cr 2.6Cr 2.6
Case 3Case 3
Miss K is a 28 y/o woman who presents for her first routine Miss K is a 28 y/o woman who presents for her first routine clinic visit. She has no complaints, and her medical history clinic visit. She has no complaints, and her medical history is unremarkable. On physical exam you note that her BP is is unremarkable. On physical exam you note that her BP is 162/94. 162/94.
You send her for some routine labs which find the following:You send her for some routine labs which find the following:
Na 147Na 147 Cl 105Cl 105 BUN 12BUN 12 Glucose 102Glucose 102
K 2.8K 2.8 HCOHCO33 3232 Cr 0.7Cr 0.7
UA unremarkable.UA unremarkable.
Case 4Case 4
Mr. W is a 65 y/o man with a past history significant for CHF secondary from an Mr. W is a 65 y/o man with a past history significant for CHF secondary from an MI 4 years ago. He comes to general medicine clinic today for a routine MI 4 years ago. He comes to general medicine clinic today for a routine appointment. He states that he was complaining of some mild dyspnea on appointment. He states that he was complaining of some mild dyspnea on exertion at his cardiology appointment 2 weeks ago. In response, his exertion at his cardiology appointment 2 weeks ago. In response, his cardiologist told him to double one of his medications, which the patient did, but cardiologist told him to double one of his medications, which the patient did, but at the moment he can’t remember which medication this was. He does report at the moment he can’t remember which medication this was. He does report that his shortness of breath is now better.that his shortness of breath is now better.
Routine fasting labs reveal the following:Routine fasting labs reveal the following:
Today Today Na 128Na 128 Cl 89Cl 89 BUN 32BUN 32 Glucose 135Glucose 135K 3.1K 3.1 HCOHCO33 32 32 Cr 1.4Cr 1.4
2 months ago2 months ago Na 132Na 132 Cl 97Cl 97 BUN 24BUN 24 Glucose 128Glucose 128K 3.8K 3.8 HCOHCO33 27 27 Cr 1.2Cr 1.2