Embed Size (px)
Citation preview

Disorders of the adrenal glands

Objectives
• Define adrenocortical insufficiency and Addison’s disease• Distinguish between primary and secondary adrenal
insufficiency and their clinical presentation• Discuss clinical diseases and syndromes associated with over
and under secretion of hormones in the adrenal glands including disorders of glucocorticoids, mineralocorticoids and catecholamines and their metabolites
• Describe the clinical presentation, investigation and management of adrenal disorders

Zona glomerulosa Zona fasciculata Zona reticularisCHOLESTEROL
17 -a Hydroxy-pregnenolone
Dehydroepi-androsterone DHEA
Pregnenolone
17 -a Hydroxy-progesterone
AndrostenedioneProgesterone
11-DeoxycortisolDeoxycorticosterone
CortisolCorticosterone
Aldosterone

Disorders of the adrenal cortex• Hyperfunction
– Excess stimulation• CRH/ACTH• Renin
– Neoplasm or hyperplasia• Benign or malignant
• Hypofunction– Insufficient stimulation
• Lack of ACTH
– Destruction• Autoimmune• Infection eg. TB, meningococcus• Vascular – infarction or bleed
– Enzymatic defect (unable to produce hormones)• Adrenal masses
– May be non-functionning or functionning adenomas or carcinomas
[Unit name – Lecture title – Prof name]

Outline
• Disorders of glucocorticoids– Excess– Insufficient– Congenital adrenal hyperplasia
• Disorders of mineralocorticoids– Excess– insufficient
• Adrenal cortex neoplasms• Disorders of catecholamines
– excess

Disorders of the Adrenal Glands
1. Glucocorticoids

Cushing’s SyndromeThe constellation of symptoms
and signs that result from excessive glucocorticoid action

Causes of Cushing’s Syndrome
• ACTH-dependent – Pituitary ACTH-dependent Cushing’s syndrome (Cushing’s disease)– Ectopic ACTH syndrome– Ectopic CRH syndrome
• ACTH-independent – Adenoma– Carcinoma– Adrenal hyperplasia (Micro- and macro-)– Glucocorticoid administration

Normal
ACTH (+) (-) Cortisol
CRH (+)

ACTH (+) (-) Cortisol
CRH (+)
ACTH-dependent Cushing’s disease
Autonomous ACTH secreting tumour

ACTH (+) (-) Cortisol
CRH (+)
Ectopic ACTHsyndrome
Ectopic ACTH secreting tumour

ACTH (+) (-) Cortisol
CRH
(+)Ectopic CRHproducing tumour
Ectopic CRH secreting tumour

ACTH (+) (-) Cortisol
CRH (+)
Adrenocortical tumour
Autonomous cortisol secreting tumour

ACTH (+)
CRH (+)
Exogenous Hydrocortisone
(-) Cortisol
IatrogenicCushing’s Syndrome
(-)

Clinical features suggestive of Cushing’s syndrome
• Fat redistribution/weight gain– Especially supraclavicular area
• Metabolic effects– Diabetes– Hypertension– hypokalemia
• Catabolic effects present– Thinning of skin– Easy bruising– Abdominal striae– Poor wound healing– Osteoporosis– Proximal myopathy
• Associated mood/cognitive changes

Cushing’s SyndromeDiagnosis
• Step 1 - Documentation of hypercortisolism– Screen
• 24-hour urinary free cortisol• 1 mg overnight dexamethasone suppression test• AM and PM p. cortisol for diurnal rhythm
– Low dose (2 mg) dexa. supp. test over 2 days
• Step 2 - Determination of cause of hypercortisolism– Plasma ACTH, DHEA-S – High dose dexa. supp. test over 2 days– Inferior petrosal sinus sampling
• Step 3 – imaging– MRI scan of pituitary, CT adrenals, site of ectopic ACTH production

Screening Tests
Hypercortisolemia Loss of normal circadian rhythm
Disturbed feedback of HPA axis
24 hr UFC800 and 2200 cortisol (salivary)
1 mg. ON dex suppression

Management of Cushing’s Disease
• Transsphenoidal resection of pituitary tumour• Bilateral adrenalectomy (a complication of this is Nelson’s
syndrome)• Radiotherapy• Medical therapy
– Adrenal enzyme inhibitors (eg. Ketoconazole)– Suppress ACTH production (paseriotide)– RU 486, a glucocorticoid receptor antagonist

Management of Adrenal Cushing’s Syndrome
• Surgical resection of adrenal tumour• Radiotherapy• Adrenal enzyme blockers (metyrapone,
aminoglutethimide, ketoconazole)• Mitotane

Management of Ectopic ACTH Syndrome
• Treatment of primary tumour• Adrenal enzyme blockers• Mitotane• Bilateral adrenalectomy

Adrenocortical Insufficiency
• Primary– Acute– Chronic
• Secondary– Hypopituitarism
• Tertiary– Hypothalamic

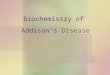
Primary adrenal failure- Addison’s disease
ACTH (+) (-) Cortisol
CRH (+)
Adrenal failure

ACTH (+) (-) Cortisol
CRH (+)
Secondary Adrenal failure
Pituitary failure
Secondary Adrenal Failure - Hypopituitarism

ACTH
Cortisol Androgens Aldosterone
Renin-angiotensin
Aldosterone will still be produced normally even with ACTH deficiency because of renin-angiotensin system

Causes of Primary Adrenal Insufficiency
• Autoimmune• Tuberculosis• Acute adrenal infarction
– haemorrhage– embolism– adrenal vein thrombosis– sepsis
• Adrenalectomy• Others
– Viral – eg. HIV, CMV– Adrenal haemorrhage– Metastases– Infiltrative disorders – medications

Primary adrenal insufficiency
• High ACTH– hyperpigmented
• Low cortisol– Nausea, vomitting– Fatigue– Hypotension– Hypoglycemia
• Low androgens– Loss of pubic hair in women
• Usually normal mineralocorticoids

[Unit name – Lecture title – Prof name]

Acute Adrenal Insufficiency Adrenal Crisis
• Untreated or undertreated adrenal insufficiency exposed to stress of surgery, trauma, infection, fluid and electrolyte loss
• Acute adrenal infarction– haemorrhage– embolism– adrenal vein thrombosis– sepsis

Adrenal CrisisClinical Features
• Shock, with hypotension• Dehydration• Fever• Nausea, vomiting• Hypoglycaemia• Hyponatremia• Change in level of consciousnes• Vague abdominal symptoms and signs

Adrenal Crisis
No time to hesistate! This is a medical emergency
Obtain blood sample for electrolytes, cortisol and ACTH
Then immediately treat with:– i.v. cortisol– i.v. fluids and electrolytes and glucose– Treat infection or other precipitating cause
Investigate later

Investigations for adrenal insufficiency
• Na (usually mildly low)• K+ (usually high)• Serum cortisol (only if >500 mmol/L) can you be sure NOT
adrenal insufficiency• ACTH level high in primary adrenal insufficiency
• ACTH stimulation test – can be done urgently

Primary adrenal insufficiency -Management
Glucocorticoids– hydrocortisone– cortisone acetate– prednisone– dexamethasone
Mineralocorticoid– fludrocortisone
Prevention of adrenal crisis - increase dose when under stress Wear MedicAlert bracelet

Congenital Adrenal Hyperplasia
• Group of autosomal recessive disorders resulting from the deficiency of one of the 5 enzymes required for synthesis of cortisol in the adrenal cortex
• Common feature is decreased negative feedback inhibition of cortisol on pituitary ACTH secretion
• Clinical consequences are those of:– deficient synthesis of cortisol and, in some types, aldosterone– excess secretion of precursors

21-Hydroxylase Deficiency
• Accounts for over 90% of all cases of congenital adrenal hyperplasia
• Cortisol deficiency leads to high ACTH• High ACTH leads to overproduction of adrenal androgens
leading to virilization• About two-thirds of patients also have mineralocorticoid
deficiency, resulting in hyponatraemia, hyperkalaemia, volume depletion and increased plasma renin activity

21-Hydroxylase Deficiency• Diagnosis is made by obtaining an elevated serum
17a-hydroxy progesterone (precursor)
• It is a single-gene autosomal recessive disorder
• Treatment consists of glucocorticoid and mineralocorticoid replacement and suppression of ACTH and androgen production

Zona glomerulosa Zona fasciculata Zona reticularisCHOLESTEROL
17 -a Hydroxy-pregnenolone
Dehydroepi-androsterone DHEA
Pregnenolone
17 -a Hydroxy-progesterone
AndrostenedioneProgesterone
11-DeoxycortisolDeoxycorticosterone
CortisolCorticosterone
Aldosterone
21 Hydroxlyase Deficiency

Clinical presentation
GirlsAmbiguous genitalia
BoysHyperkalemia, hyponatremia (Lack of aldosterone, salt losers)Failure to thrive (cortisol deficiency)Early puberty


Long-term consequences of CAH and its treatment
• Compromised final adult height• Osteoporosis• Obesity• Fertility• Sexuality• Hyperinsulinism


Zona glomerulosa Zona fasciculata Zona reticularisCHOLESTEROL
17 -a Hydroxy-pregnenolone
Dehydroepi-androsterone DHEA
Pregnenolone
17 -a Hydroxy-progesterone
AndrostenedioneProgesterone
11-DeoxycortisolDeoxycorticosterone
CortisolCorticosterone
Aldosterone
11 Hydroxlyase Deficiency

11-Hydroxylase Deficiency
• The main difference between this and 21-hydroxylase deficiency is that this condition is associated with hypertension
• The hypertension is probably due to accumulation of 11-deoxycorticosterone, a weak mineralocorticosteroid
• Diagnosis is established by measurement of plasma 11-deoxycortisol
• Treatment consists of replacement with glucocorticoid

Zona glomerulosa Zona fasciculata Zona reticularisCHOLESTEROL
17 -a Hydroxy-pregnenolone
Dehydroepi-androsterone DHEA
Pregnenolone
17 -a Hydroxy-progesterone
AndrostenedioneProgesterone
11-DeoxycortisolDeoxycorticosterone
CortisolCorticosterone
Aldosterone
17α- hydroxylaseDeficiency
Salt retention
&
Hypertension

Zona glomerulosa Zona fasciculata Zona reticularisCHOLESTEROL
17 -a Hydroxy-pregnenolone
Dehydroepi-androsterone DHEA
Pregnenolone
17 -a Hydroxy-progesterone
AndrostenedioneProgesterone
11-DeoxycortisolDeoxycorticosterone
CortisolCorticosterone
Aldosterone
3b-hydroxysteroid dehydrogenasedeficiency
Death In utero
High DHEA-S

Zona glomerulosa Zona fasciculata Zona reticularisCHOLESTEROL
17 -a Hydroxy-pregnenolone
Dehydroepi-androsterone DHEA
Pregnenolone
17 -a Hydroxy-progesterone
AndrostenedioneProgesterone
11-DeoxycortisolDeoxycorticosterone
CortisolCorticosterone
Aldosterone
P 450 Deficiency
Death In utero

Disorders of the Adrenal Glands
2. Mineralocorticoids

Renin-Angiotensin
Potassium
ACTH
Aldosterone
Factors controlling Aldosterone Secretion

Liver
Adrenal
JGA
Angiotensinogen
Angiotensin I
Angiotensin II
AldosteroneRenal sodium retention
ECF expansion
Renin-Angiotensin-Aldosterone System
ECF depletionDec. art. pressNervous stim.U. sod. conc.
S
I
I
Renin
Converting Enzyme

Metabolic Effects of Mineralocorticoid Excess
Sodium retention high normal serum sodium,
hypertension Potassium loss
hypokalaemia Hydrogen ion loss
metabolic alkalosis

Excess Aldosterone
• Primary (high aldo, low renin)– Adrenal aldosterone producing adenoma (Conn’s syndrome)– Adrenal hyperplasia
• Secondary (high aldo, high renin)– Physiologic
• Pregnancy• Sodium depletion
– Nephrotic syndrome– Hepatic cirrhosis with ascites– Congestive cardiac failure– Idiopathic edema– Salt losing nephritis– Bartter’s syndrome– Accelerated hypertension– Oral contraceptive pills– Thiazide-induced– JGA cell renin producing tumours

High aldosterone/renin ratio

Conn’s Syndrome
• Hypertension• Hypokalaemia with inappropriate kaliuresis• Metabolic alkalosis• Serum sodium > 140 mmol/l• Suppressed plasma renin activity• High and nonsuppressible plasma aldosterone• Normal plasma and urine cortisol

Primary Hyperaldosteronism: Investigations• Demonstration of renin suppression
– Measure plasma renin activity (PRA) after applying known stimuli of renin secretion such as upright posture, a dose of furosemide and a few days of low salt diet. PRA is low or undetectable in primary aldosteronism
• Demonstration of non-suppressible plasma aldosterone levels– Measure plasma aldosterone before and after infusion of saline. P. aldosterone does not drop in
primary aldosteronism
• Image – CT or MRI scan of adrenals are useful. Often able to distinguish between an adenoma and
hyperplasia but not always. APA are usually small (1-2 cm diameter)– Iodo-cholesterol scan - adrenocortical tumours take up this isotope– Selective venous sampling to obtain blood for measurement of aldosterone -

Primary Hyperaldosteronism: Management
• APA - Surgical resection or spironolactone• Hyperplasia - Spironolactone

Selective or Isolated Hypoaldosteronism
A clinical disorder in which adrenal production of aldosterone is reduced without associated reduction in adrenal production of cortisol

Consequences of Hypoaldosteronism
• Hyperkalaemia• Metabolic acidosis• Hyponatraemia• Fluctuation in GFR• Excessive natriuresis

Isolated Aldosterone Deficiency
Primary (problem resides in the adrenals)– High plasma renin activity (PRA) , low plasma
aldosterone
Secondary (problem is inability to produce normal amounts of renin and angiotensin)– Low PRA, low plasma aldosterone
Pseudohypoaldosteronism (problem is resistance of target tissue to action of aldosterone)– High PRA, high plasma aldosterone

Primary HypoaldosteronismCauses
• Adrenal enzyme deficiency• Autoimmune adrenalitis• Post-resection of an aldosterone
producing adenoma

Secondary Hypoaldosteronism
Hyporeninaemic Hypoaldosteronism

Conditions Associated with Hyporeninaemic Hypoaldosteronism
• Old age• Chronic renal failure• Diabetes mellitus• Nephrolithiasis• Cystic disease of kidneys• Hypertensive nephrosclerosis• Gouty nephropathy• Pyelonephritis• Analgesic abuse• Hyperparathyroidism• Hypothyroidism

Adrenocortical Tumours
• Functional– Cushing’s syndrome– Conn’s syndrome– Hyperandrogenism and hyperoestrogenism syndromes
• Non-functional (Many are discovered incidentally - called “incidentalomas”)

Clinical Features of Adrenocortical Carcinomas
• Symptoms– Abdominal pain– Weight loss– Weakness– Fever– Anorexia, nausea and vomiting
• Signs– Abdominal mass– Lymphadenopathy, hepatomegaly– Hypertension– Endocrine manifestations

Disorders of the Adrenal Glands
3. Disorders of the Adrenal Medulla

Hormones of the Adrenal Medulla
Catecholamines– Epinephrine (adrenaline)– Norepinephrine (noradrenaline)– Dopamine

THE CATECHOLAMINES Epinephrine
– 80% of the catecholamines in adrenal medulla
– Not much synthesis elsewhere Norepinephrine
– Neurotransmitter in CNS and sympathetic nervous system
Dopamine– Found in adrenal medulla, brain,
sympathetic ganglia, carotid body

CATECHOLAMINESMetabolism
Reuptake by nerve endings Excretion by kidneys Breakdown
– Epinephrine/norepinephrine
– Metanephrine/normetanephrine
– Vanillylmandelic acid (VMA)
Catecholamine O-methyl transferase (COMT)Monoamine oxidase (MAO)
MAO/COMT
MAO

Tumour- chromaffin cells– 80% unilateral adrenal medulla– 10% bilateral adrenal medulla– 10%extra-adrenal - paragangliomas
Produces Catecholamines Most present with episodic or sustained Hypertension Rare cause of hypertension
– 0.1-0.2%– Treatable and curable
Pheochromocytoma

PHEOCHROMOCYTOMAClinical Features
• Sustained hypertension 61%– with crises 27%– without crises 34%
• Paroxysmal hypertension 27%• Hypertension of pregnancy 3%• No hypertension 9%

PHEOCHROMOCYTOMAClinical Features
SymptomsHeadaches
Sweating
Palpitations
Nervousness
Nausea/vomiting
Chest/abd. pain
SignsSweating
Tachycardia
Arrhythmia
Pallor
Weight loss

Familial disorders associated with pheochromocytoma
• Multiple endocrine neoplasia 2A and 2B (MEN 1 is not associated with pheo)– 2A
• Medullary cell carcinoma of the thyroid• hyperparathyroidism
– 2B• Mucousal neuromas• Medullary cell carcinoma of the thyroid• Marfinoid habitus
• Von Hippal Lindau disease
– Retinal angiomas– Cerebellar hemangioblastoma– Renal/pancreatic cysts– Renal cell carcinoma
• Neurofibromatosis

PHEOCHROMOCYTOMADiagnosis
BIOCHEMICAL TESTS– urinary catecholamines– urinary VMA - vanyllmandelic acid– urinary metanephrines/normetanephrines– other - serum catecholamines
LOCALIZATION– CT, MRI– radionucleide scans– arteriography

PHEOCHROMOCYTOMAManagement
FIRST - a receptor blockadeSECOND - b receptor
blockadeTHIRD - surgeryFOURTH - post-operative Rx

Summary
• Disorders of the adrenal cortex can be result of:– Excess production
• Hyperstimulation eg. ACTH, renin• Functionning neoplasm eg. Cortisol or aldosterone producing adenoma
– Inadequate production• Inadequate stimulation eg. Hypopituitarism, low renin• Destruction of gland eg. Autoimmune or TB
– Abnormal enzyme• CAH
• Disorders of adrenal medulla– Primarily excess production (pheo)
• Can also have mass lesions in adrenal glands that do not disrupt function– Eg. Metastatic disease, non-functionning adrenal adenoma