Embed Size (px)
Citation preview

CASE REPORT
Disseminated congenital tuberculosis presenting as peritonitisin an infant
Mi Hyun Lee • Gye-Yeon Lim • Jae Hee Chung •
So-Young Kim
Received: 18 September 2012 / Accepted: 11 December 2012 / Published online: 12 January 2013
� Japan Radiological Society 2012
Abstract Congenital tuberculosis is a rare disease which
is curable after early diagnosis. Making an early diagnosis
of tuberculosis in an infant is difficult, however, because of
its nonspecific clinical findings. It therefore requires a high
index of suspicion. In this paper we report the case of an
infant with disseminated congenital tuberculosis involving
the chest, liver, spleen, abdominal lymph nodes, mesentery,
and peritoneum, and which presented as chylous ascites
with peritonitis.
Keywords Congenital tuberculosis � Tuberculosis �Ascites � Infant
Introduction
Congenital tuberculosis is a rare disease; to date, approx-
imately 300 cases have been reported in the world literature
[1]. Tubercular infection during fetal life may occur from
an infected placenta through the umbilical vein, forming a
primary complex in the liver. Alternatively, fetal ingestion
or aspiration of infected amniotic fluid may result in a
primary complex in the gastrointestinal tract or the lungs,
respectively [1]. Early diagnosis of congenital tuberculosis
is important because the outcome is invariably poor in the
absence of early institution of anti-tuberculous therapy.
Symptoms and clinical findings of congenital tuberculosis,
for example respiratory distress and fever, are nonspecific
and may be present in bacterial sepsis and in other con-
genital infections and can lead to misdiagnosis of neonatal
pneumonia or sepsis. Because early diagnosis and timely
treatment depend on a high index of suspicion, familiarity
with both the common and uncommon manifestations of
congenital tuberculosis is required of physicians. We report
a case of disseminated congenital tuberculosis involving
the chest and abdomen which presented as peritonitis in a
three-week-old neonate. We wish to emphasize the ultra-
sonography (US) and whole-body magnetic resonance
imaging (MRI) findings.
Case report
A 19-day-old, male infant was referred to our hospital with
a one-week history of a low-grade fever and abdominal
distention. The infant was delivered by Caesarean delivery
at 41 ? 1 weeks and had a birth weight of 3.55 kg. The
immediate neonatal period was uneventful. At the time of
delivery the mother’s past history of tuberculosis was
unknown.
On physical examination, the infant’s respiratory rate
was 44/min and his body temperature was 38.6 �C. His
abdominal circumference was 44.5 cm. There was no
cyanosis, jaundice, or significant lymphadenopathy. Lab-
oratory studies revealed a decreased WBC count of
4670/mm3, a platelet count of 49000/mm3, and increased
C-reactive protein of 9.93 mg/L. These findings increased
the possibility of sepsis. The patient’s liver function tests
M. H. Lee � G.-Y. Lim (&)
Department of Radiology, St. Mary’s Hospital, The Catholic
University of Korea, #62, Yeouido-dong, Yongdungpo-gu,
Seoul 150-713, Korea
e-mail: [email protected]
J. H. Chung
Department of Surgery, St. Mary’s Hospital,
The Catholic University of Korea, Seoul, Korea
S.-Y. Kim
Department of Pediatrics, St. Mary’s Hospital,
The Catholic University of Korea, Seoul, Korea
123
Jpn J Radiol (2013) 31:282–285
DOI 10.1007/s11604-012-0174-4

were normal. The Mantoux test was positive, resulting in
an induration of 10 mm at 48 h.
A radiograph obtained on the day of the patient’s
referral revealed centralization of bowel loops with lateral
abdominal bulging and patchy lesions in the right parahilar
and left apical regions (Fig. 1). Abdominal US revealed
multiple, hypoechoic foci in the liver and spleen, con-
glomerated hypoechoic lymph nodes in the porta hepatis or
hepatic hilum region, and a large amount of ascites con-
taining debris with fluid–fluid level (Fig. 2). Contrast-
enhanced, whole body MRI confirmed the US findings and
also revealed pronounced enhancement of thickened peri-
toneum, mesenteric leaves, bowel wall, and omentum
(Fig. 3). Necrotic lymph nodes in the porta hepatis region
and in the subcarinal region of the mediastinum showed
peripheral enhancement with central low signal intensity
(Fig. 3). No definite brain abnormality was noted on either
the US or the whole-body MRI.
Analysis of the ascites fluid revealed a white blood cell
count of 360/mm3 with 63 % lymphocytes, a triglyceride
level of 459 mg/dL, a total cholesterol level of 69 mg/dL,
total protein level of 2.9 mg/dL, and an adenosine deami-
nase level of 42.6 IU/L. These results suggested the pres-
ence of chyle. No organisms were detected in the smears or
cultures obtained from the ascitic fluid. Specimens obtained
from blood, urine, gastric aspirate, and cerebrospinal fluid
to assess the presence of acid-fast bacilli (AFB), were
negative and no growth of any organism was found.
Sputum culture was positive for AFB. Laparoscopic
omentum biopsy revealed caseous granulomatous inflam-
mation and multinucleated giant cells. The infant’s mother
declined endometrial biopsy and examination for AFB. The
infant was started on anti-tuberculosis drugs, and his clinical
condition improved. Calcifications in the liver and spleen
and lymphadenopathy were noted on follow-up US obtained
7 weeks after treatment, and increased calcific changes of
lesions were noted on serial follow-up US (Fig. 4).
Fig. 1 Radiograph of a three-week-old infant shows centralization of
bowel loops with lateral abdominal bulging and patchy lesions in the
right parahilar and left apical lung regions
Fig. 2 a Longitudinal sonogram of the left upper quadrant shows
multiple, hypoechoic foci in the spleen. b Axial sonogram of the liver
shows conglomerated, hypoechoic lymph nodes in the porta hepatis or
hepatic hilum region (arrows). c Axial sonogram of the right lower
quadrant shows a large amount of ascites containing fluid–fluid level
(arrows)
Jpn J Radiol (2013) 31:282–285 283
123

Discussion
Congenital tuberculosis is thought to be transplacentally
transferred to the fetus from the infected mother, after
which it forms a primary complex in the infant’s liver and
has secondary hematogenous spread; it can also occur as a
result of aspiration or ingestion of infected amniotic fluid
which becomes primarily focused in the infant’s lung or
gastrointestinal tract [2–5]. The established diagnostic cri-
teria for congenital tuberculosis [2] include proven tuber-
culosis lesions in an infant and at least one of the following:
– lesions occurring during the first week of life;
– the existence of primary hepatic complex;
– maternal genital tract or placental tuberculosis; or
– exclusion of postnatal transmission by thorough inves-
tigation of contacts.
For our patient there was no investigation of tuberculous
infection of the maternal genital tract or placenta, although
other criteria, for example primary involvement of the liver
and exclusion of the possibility of postnatal transmission
by hospital attendants or other family members, should be
considered to enable correct diagnosis of congenital
tuberculosis. The modes of presentation, treatment, and
immediate prognosis of tuberculosis do not differ signifi-
cantly between that seen in congenital infection and that in
early, post-natally acquired tuberculosis [4–6].
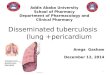
Fig. 3 Contrast–enhanced, whole-body MRI obtained during the
third week of the infant’s life. Axial T1-W (a), T2-W (b), and
enhanced T1-W (c) MR images of the abdomen show multiple,
conglomerated, enlarged lymph nodes in the porta hepatis region
(arrows) with peripheral rim enhancement. Multiple, tiny, low-signal-
intensity nodular lesions were scattered throughout the spleen
(c, arrowheads). Coronal T1-W (d) and enhanced T1-W
(e, f) images of the chest and abdomen show large amount of ascitic
fluid and marked thickening with enhancement of the peritoneum
(arrows). Tiny, low-signal-intensity nodular lesions were scattered in
the liver and spleen (e, f, arrowheads). Necrotic lymph nodes with
rim enhancement are also noted in the subcarinal region of the
mediastinum (f, arrow)
Fig. 4 Follow-up abdominal US obtained 13 weeks after treatment
shows calcifications within multiple foci of the spleen
284 Jpn J Radiol (2013) 31:282–285
123

The liver and lung are the two most commonly involved
sites of congenital tuberculosis. Frequently reported
imaging findings include multiple pulmonary nodules,
necrotic mediastinal lymphadenopathy, parenchymal infil-
tration, hepatosplenomegaly, and multiple focal lesions in
the liver and spleen [4, 6, 7]. Early in the course of the
disease, chest radiographs may be normal, with profound
radiological abnormalities only developing later [4, 6, 7].
In our patient, no definite abnormality was detected on the
initial chest radiograph, although necrotic mediastinal
adenopathy was noted on whole-body MRI scanning per-
formed at the same time.
To the best of our knowledge, there are only a few case
reports describing congenital tuberculosis presenting as
ascites [5, 7, 8]. According to one report which analyzed
170 cases of congenital tuberculosis, only 10.5 % of the
patients had ascites [7]. These patients eventually devel-
oped abdominal distension with low-grade fever mani-
fested by peritonitis with chylous ascites. Tuberculous
chylous ascites is rare and, when present, fluid–fluid level
or debris can be seen on US, as in our patient. Although
tuberculous involvement limited to the peritoneum is rare,
peritoneal involvement is seen in association with wide-
spread abdominal disease. Involvement of the peritoneal
cavity, mesentery, and omentum seems to occur because of
rupture of mesenteric lymph nodes, presence of the primary
complex of tuberculosis just beneath the spleen or liver
surface, or serosal continuity from adjacent structures. In
our case, enhanced, whole-body MRI revealed extensive
tuberculous peritonitis appearing as enhanced thickening of
the peritoneum and mesentery, matted bowel loops, a
smudged pattern of the omentum, and a large amount of
viscous ascitic fluid.
Because early diagnosis of congenital tuberculosis
requires a high index of suspicion, imaging is essential to
ensure correct diagnosis. This disease is usually evaluated
by using chest radiographs, US, and CT. To evaluate chest
lesions, CT is useful for identifying parenchymal lesions
and lymphadenopathy, because it is superior to radiography
and capable of earlier detection than radiography [6].
Because US does not involve a risk of exposure to ionizing
radiation, it is a very useful imaging modality for detecting
abdominal abnormalities, not only for early lesion dem-
onstration but also for confirmation of lesion etiology by
guided biopsy. However, US is generally used for regional
evaluation rather than to evaluate the entire extent of dis-
ease. Congenital tuberculosis is frequently disseminated
throughout the body. In addition, as in this case, evaluation
for necrotic adenopathy and peritoneal involvement of
congenital tuberculosis requires contrast-enhanced
examinations. However, contrast-enhanced CT is not
desirable in infants because it delivers a significant radia-
tion dose. Contrast–enhanced, whole body MRI enables
acquisition of images of the entire body in a matter of
minutes and without exposure to ionizing radiation. As
intravenous contrast agents are not used in routine, whole-
body MR examinations, we perform contrast examinations
for this reason. Whole-body MRI is thought to have rela-
tively poor ability to detect lung lesions or small lymph
nodes, although we had no difficulty using this modality to
detect mediastinal nodes and the presence of abdominal
involvement. To the best of our knowledge, whole-body
MRI can be successfully used as a supplemental diagnostic
method followed by sonography to assess the extent of
disease in infants with congenital tuberculosis.
In this case, calcifications in the liver and spleen and
lymphadenopathy were noted on follow-up US after ther-
apy had been started. Serial US can also be used as a
follow-up modality for lesions, and for monitoring calci-
fications seen as part of the healing process in patients with
congenital tuberculosis.
Although congenital tuberculosis is a rare disease, it
should be included in the differential diagnosis for infants
who have extensive peritoneal involvement and wide-
spread abdominal disease.
Conflict of interest The authors declare that we have no conflict of
interest.
References
1. Grover SB, Tanejs DK, Bhatia A, Chellani H. Sonographic
diagnosis of congenital tuberculosis: an experience with four
cases. Abdom Imaging. 2000;25:622–6.
2. Cantwell MF, Shehab ZM, Costello AM, Sands L, Green WF,
Ewing EP, Jr., et al. Brief report: congenital tuberculosis. New
Engl J Med. 1994;330(15):1051–4 (Epub 14/04/1994).
3. Kang GH, Chi JG. Congenital tuberculosis–report of an autopsy
case. J Korean Med Sci. 1990;5(1):59–4 (Epub 01/03/1990).
4. Chen A, Shih SL. Congenital tuberculosis in two infants. AJR Am
J Roentgenol. 2004;182(1):253–6. (Epub 20/12/2003).
5. Berk DR, Sylvester KG. Congenital tuberculosis presenting as
progressive liver dysfunction. Pediatr Infect Dis J. 2004;23(1):
78–80 (Epub 27/01/2004).
6. Neyaz Z, Gadodia A, Gamanagatti S, Sarthi M. Imaging findings
of congenital tuberculosis in three infants. Singapore Med J.
2008;49(2):e42–6 (Epub 28/02/2008).
7. Peng W, Yang J, Liu E. Analysis of 170 cases of congenital TB
reported in the literature between 1946 and 2009. Pediatr
Pulmonol. 2011;46(12):1215–24 (Epub 01/06/2011).
8. Aelami MH, Qhodsi Rad MA, Sasan MS, Ghazvini K. Congenital
tuberculosis presenting as ascites. Arch Iran Med. 2011;14(3):
209–10 (Epub 03/05/2011).
Jpn J Radiol (2013) 31:282–285 285
123