Embed Size (px)
Citation preview
1
EVALUATION OF ARTHROSCOPIC ACL
RECONSTRUCTION BY 3 DIFFERENT TECHNIQUES
DISSERTATION SUBMITTED TO UNIVERSITY OF SEYCHELLES
AMERICAN INSTITUTE OF MEDICINE
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE
M.Ch (Orthopaedic Surgery)
By DR. AMIT AHLUWALIA
Orthopaedic Surgeon
2013

2
Special thanks to co-author and my colleague
Dr. Atul Mishra
3
INTRODUCTION
• The goal of arthroscopic ACL reconstruction is to restore joint function by recreating as closely as possible normal knee kinematics.
• Biomechanical studies have demonstrated that single bundle ACL reconstruction is insuf ficient for controlling rotation in extension.
• Double bundle ACL reconstruction has been shown to provide more improvement in knee stability theoretically because it more closely mimics the anatomic structure of ACL.
Aim
• To analyze the clinical outcome of arthroscopic anterior cruciate ligament (ACL) reconstruction done in 58 patients over a period of 1 year by 3 different surgical techniques using hamstring autograft.
3 different surgical techniques:
1. Hamstrings [semitendinosis and gracilis (STG) combined] by Double Bundle anatomical reconstruction (DB)
2. Quadrupled Single Bundle reconstruction (SB)
3. Over the top with Lateral Plasty {OTLP (combined intra and extra-articular tenodesis technique)}
MATERIALS AND METHODS
• The records of 58 consecutive patients who underwent arthroscopic ACL reconstruction in the year 2007 were evaluated.
• The patients were selected if they met the following criteria:
1. Presence of unilateral isolated monoligamentous injury
2. No history of surgery on the contra lateral knee or extremity
3. No history of surgery on the ipsilateral extremity
•
Demog
Surgica
No of p
Mean a
Male/F
Mean t(month
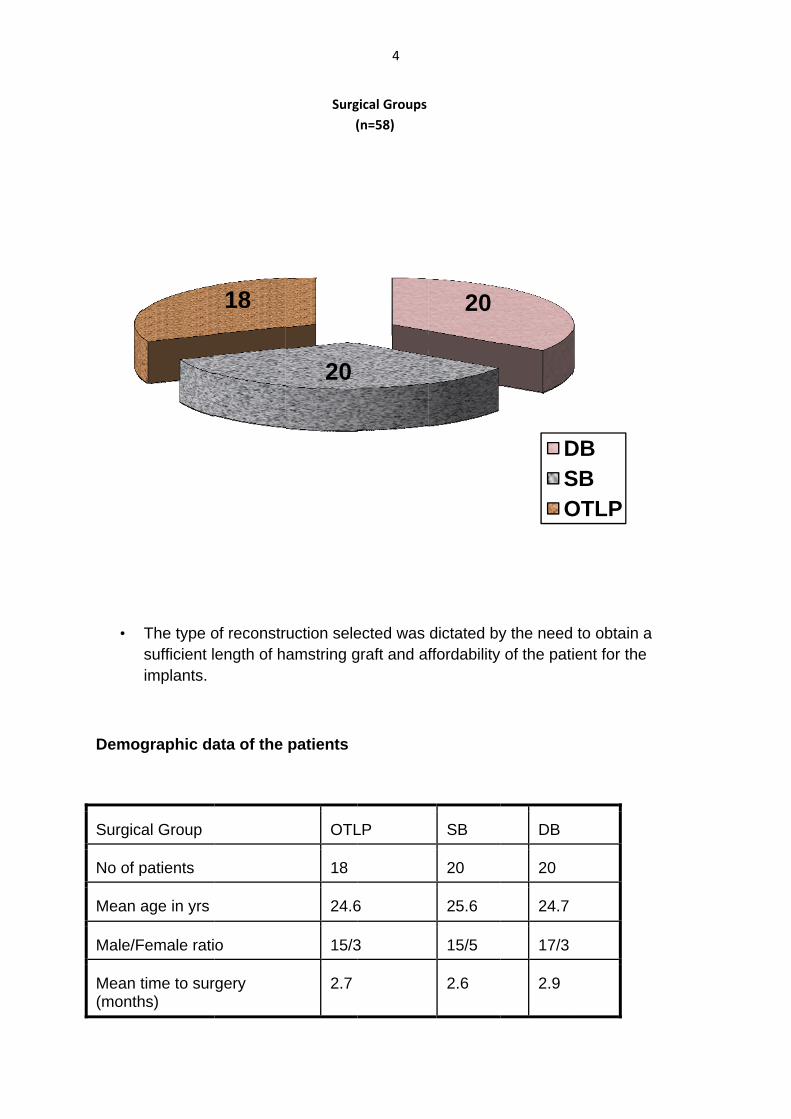
The type osufficient limplants.
graphic da
al Group
patients
age in yrs
Female rati
time to surhs)
of reconstrength of h
ata of the
o
rgery
18
Surg (
uction seleamstring g
patients
OTL
18
24.6
15/3
2.7
20
4
gical Groups(n=58)
ected was graft and af
LP
6
3
dictated byffordability
SB
20
25.6
15/5
2.6
20
y the needof the pat
DB
20
24.7
17/3
2.9
DSO
to obtain ient for the
DBSBOTLP
a e
5
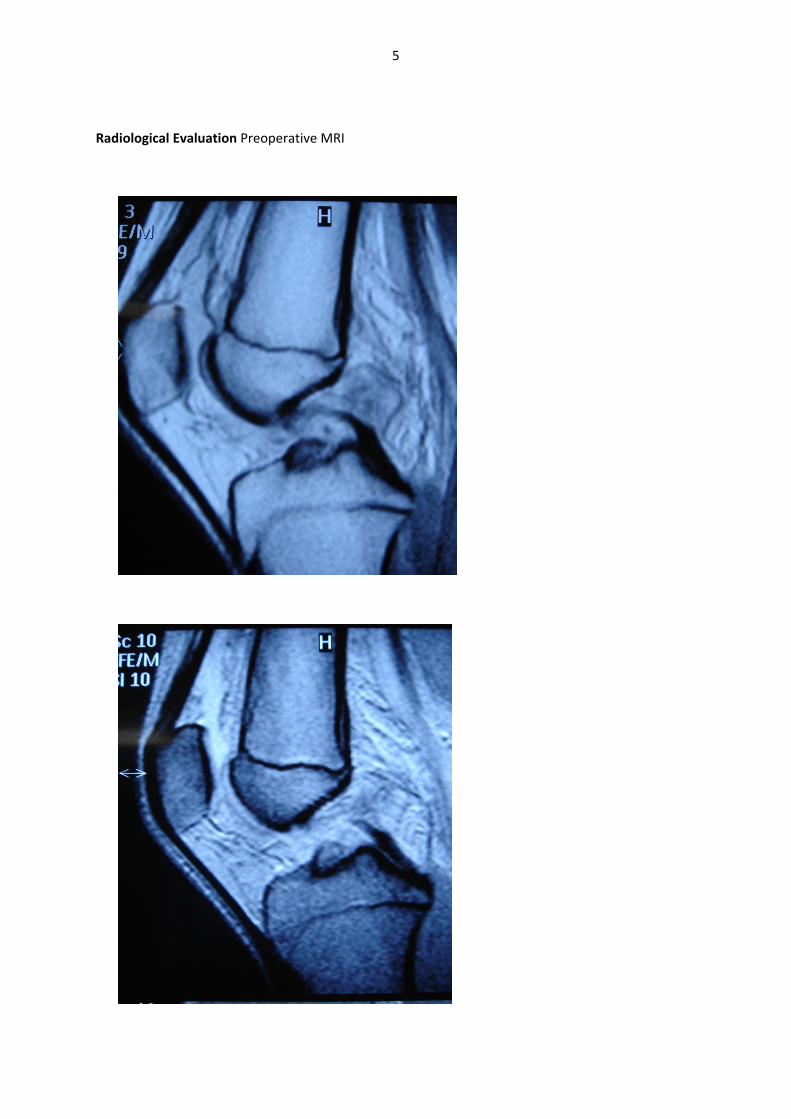
Radiological Evaluation Preoperative MRI
SurgicOver th
•
•
Prepar
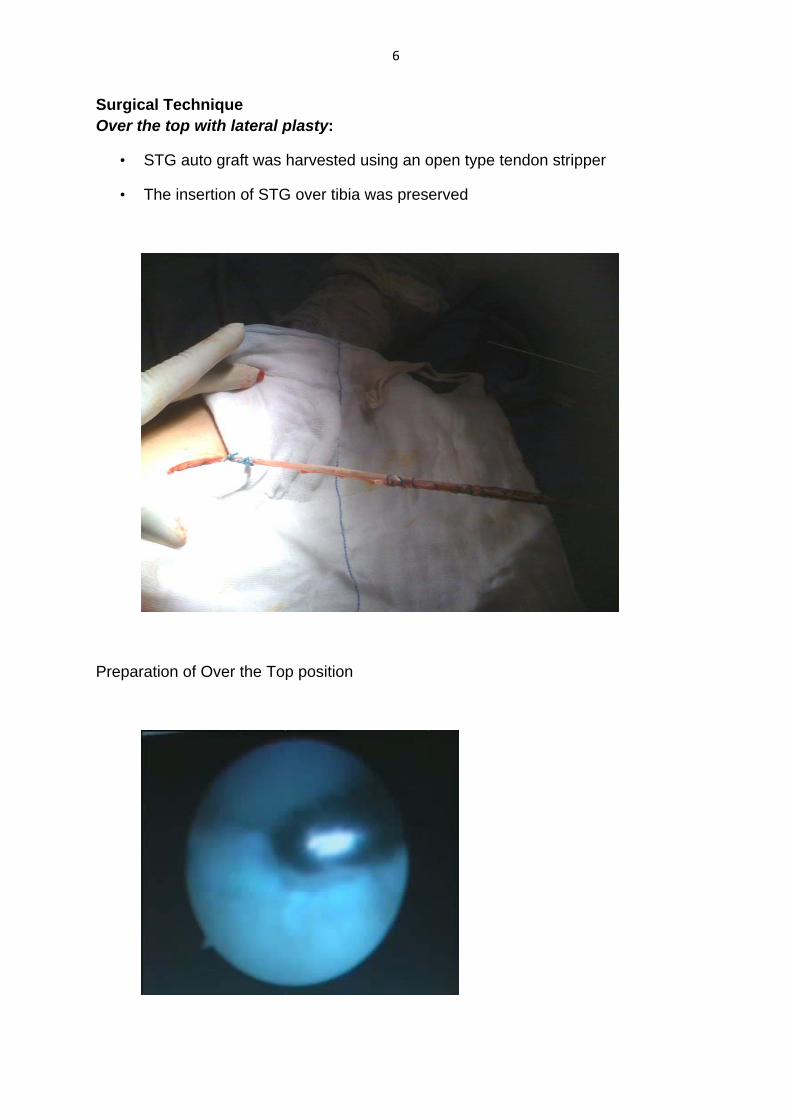
cal Technihe top wit
STG auto
The insert
ration of Ov
que th lateral p
graft was
tion of STG
ver the Top
plasty:
harvested
G over tibia
p position
6
using an o
a was pres
open type t
erved
tendon striipper
7
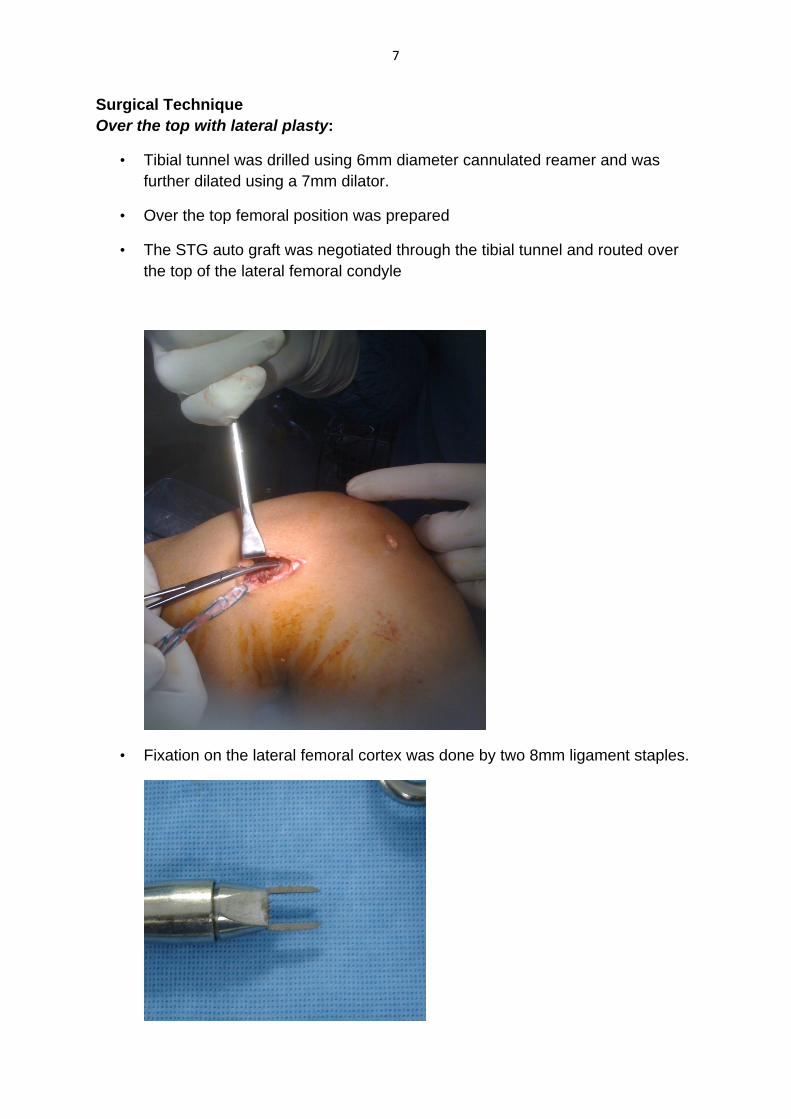
Surgical Technique Over the top with lateral plasty:
• Tibial tunnel was drilled using 6mm diameter cannulated reamer and was further dilated using a 7mm dilator.
• Over the top femoral position was prepared
• The STG auto graft was negotiated through the tibial tunnel and routed over the top of the lateral femoral condyle
• Fixation on the lateral femoral cortex was done by two 8mm ligament staples.

8
• Prior to fixation manual tensioning of the graft was done by constantly pulling the graft and subjecting the knee through a full range of motion 10 times
• Fixation was done keeping the knee in 900 flexed position while maintaining a posterior push on the tibia and externally rotating the tibia by 100.
• The remaining graft was negotiated distally beneath the facia lata and fixed on Gerdys tubercle with one ligament staple keeping the knee in the same position as above.
• Notchplasty was not done.
•
•
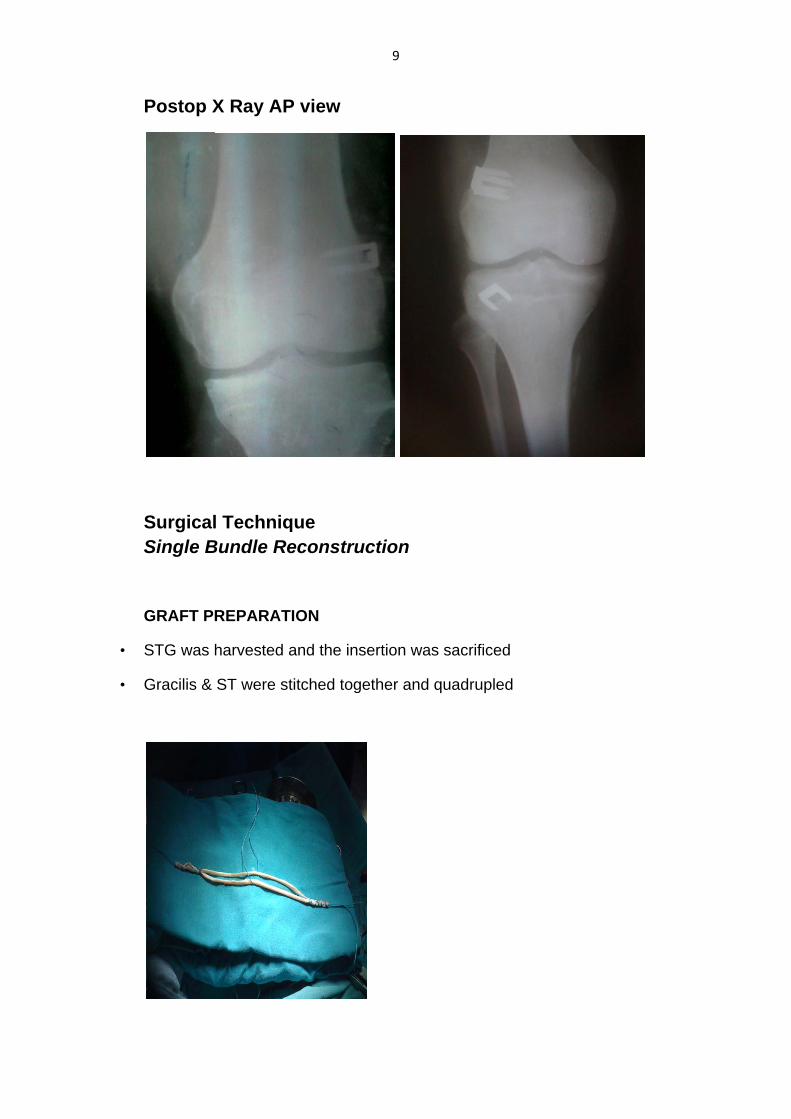
Postop X
SurgicalSingle B
GRAFT P
STG was
Gracilis &
X Ray AP
l TechniqBundle R
REPARAT
harvested
ST were s
P view
que Reconstru
TION
and the in
stitched tog
9
uction
sertion wa
gether and
as sacrifice
quadruple
ed
ed
•
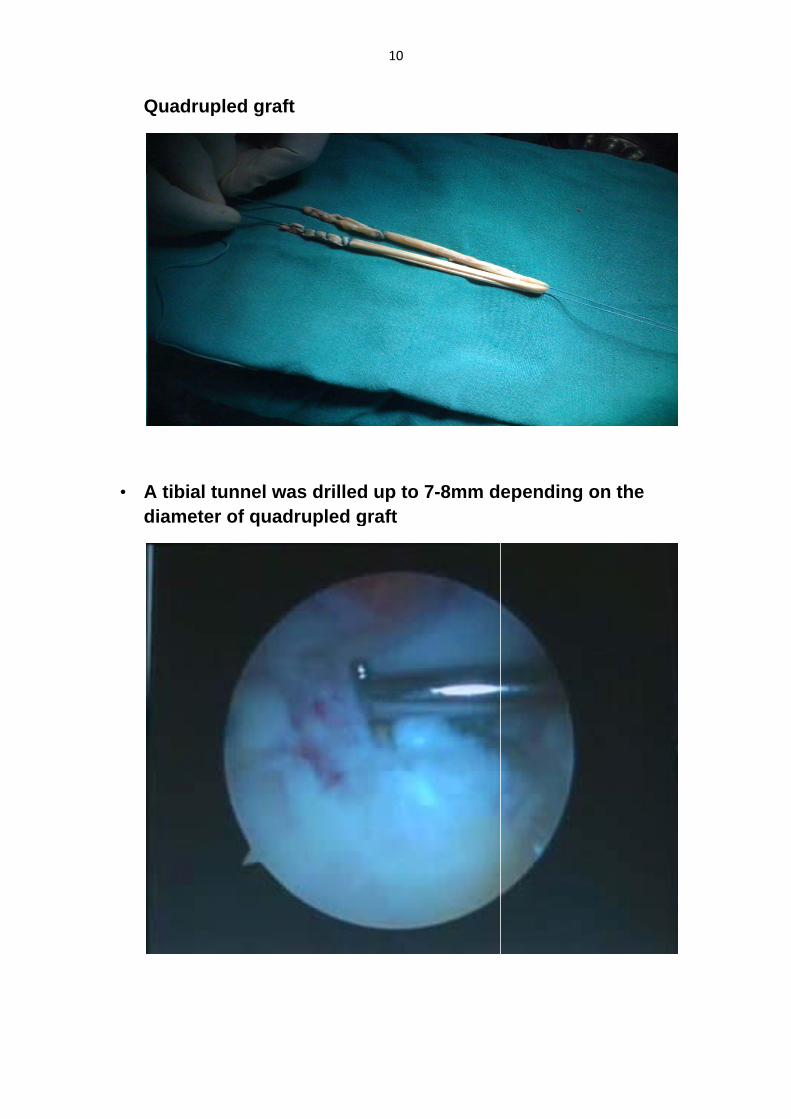
Quadrup
A tibial tdiamete
pled graf
tunnel wr of quad
ft
was drilledrupled g
10
d up to 7graft
7-8mm depending on the
e
•
•
•
•
•
A femoral 1.30 0’clocappropriat
An approp
Manual tesubjecting
Femoral fi
Tibial fixatinterferenc
guide pin wck on the lete offset de
priate size t
nsioning o the knee t
xation was
tion was doce screw.
was positioeft knee wevice inser
tunnel was
f the graft through a
s done usin
one keepin
11
oned at 10ith 90-1100
rted throug
s prepared
was done full range o
ng endobu
ng the knee
0.30 0’clock0 flexion ath the AM p
d
by constanof motion 1
tton (CL, M
e in 300 fle
k on the rigt the knee,portal.
ntly pulling10 times.
Mersilene t
exion with m
ght knee a using an
g the graft a
tape)
metal/ bio
nd
and

Postop X
X-Ray APP and La
12
ateral vie
ews
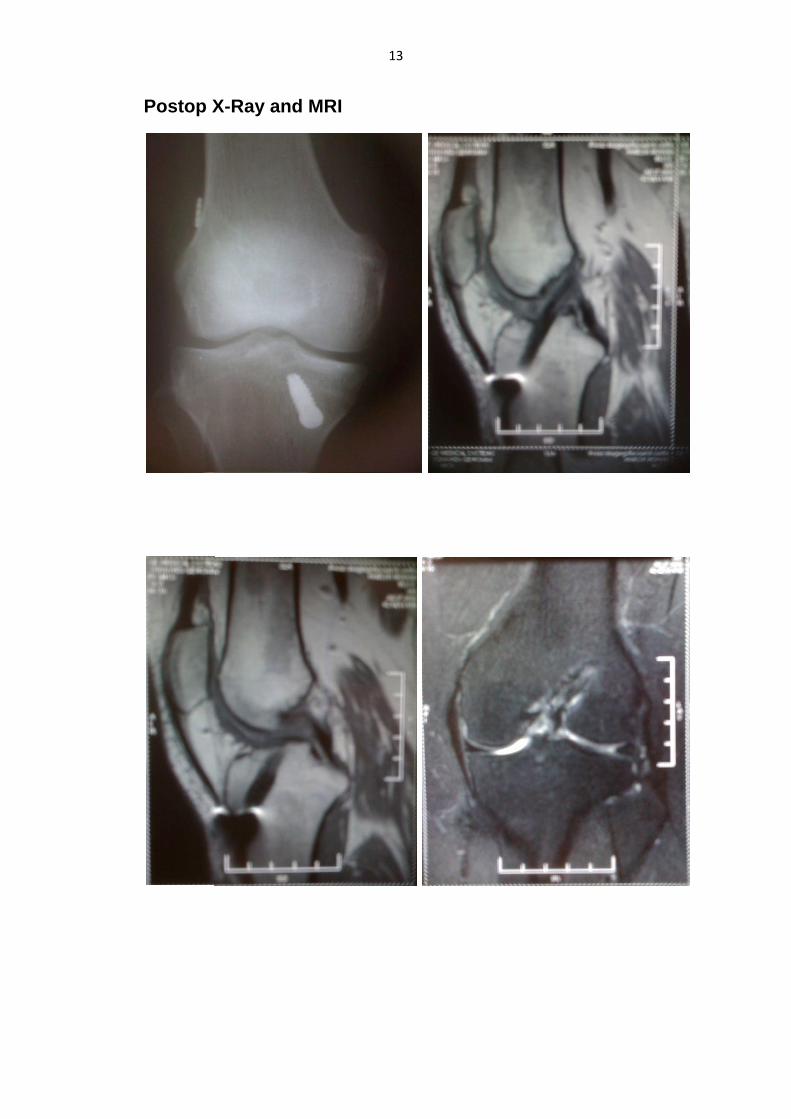
Postop X
X-Ray annd MRI
13
14
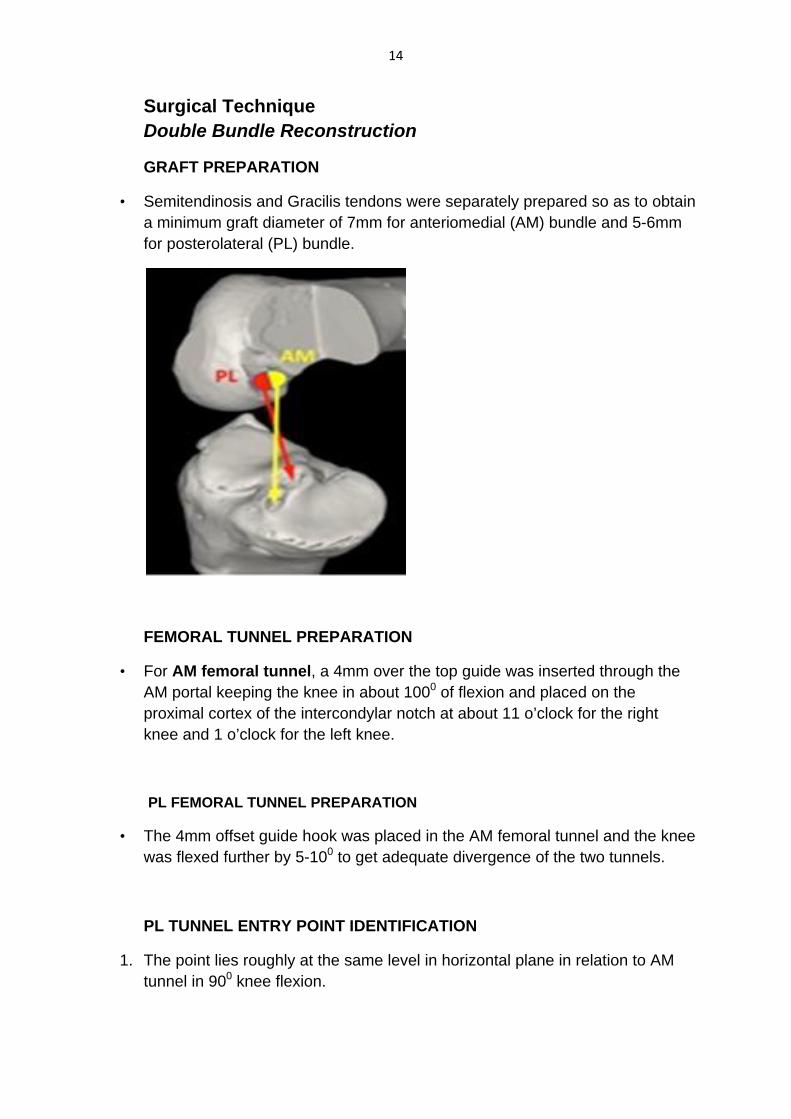
Surgical Technique Double Bundle Reconstruction
GRAFT PREPARATION
• Semitendinosis and Gracilis tendons were separately prepared so as to obtain a minimum graft diameter of 7mm for anteriomedial (AM) bundle and 5-6mm for posterolateral (PL) bundle.
FEMORAL TUNNEL PREPARATION
• For AM femoral tunnel, a 4mm over the top guide was inserted through the AM portal keeping the knee in about 1000 of flexion and placed on the proximal cortex of the intercondylar notch at about 11 o’clock for the right knee and 1 o’clock for the left knee.
PL FEMORAL TUNNEL PREPARATION
• The 4mm offset guide hook was placed in the AM femoral tunnel and the knee was flexed further by 5-100 to get adequate divergence of the two tunnels.
PL TUNNEL ENTRY POINT IDENTIFICATION
1. The point lies roughly at the same level in horizontal plane in relation to AM tunnel in 900 knee flexion.
15
2. The center of the PL bundle footprint is approximately located at the crossing point of the long axis line of the ACL attachment and a vertical line drawn through the contact point between the femoral condyle and tibial plateau at 900 of knee flexion
3. The socket was placed at 9 o’clock position for the right knee and 3 o’clock position for the left knee.
4. The position of the guide wire was rechecked by switching the arthroscope from anterolateral to anteromedial portal
TIBIAL AM & PL TUNNEL PREPARATION
• The tibial guide pin was inserted using a normal tibial guide tip aimer through the anterior part of ACL footprint
• With the guide pin in place the same tibial aimer was used to pass another guide pin in the posterior part of the ACL footprint.
• Two leading sutures were passed through the two femoral tunnels.
• The suture in the AM femoral tunnel was pulled out through the AM tibial tunnel
• The leading suture in the PL femoral tunnel was pulled out into the PL tibial tunnel.
• Care was taken that the PL leading suture remains posterior to the AM leading suture.
• The PL bundle was negotiated first through the tibial and femoral tunnels followed by the AM bundle.
TENSIONING & FIXATION
• The graft loops were secured on the femoral side with endobutton CL or endobutton with mersiliene tape loop and on the tibial side with bio interference screws.
• The AM bundle is isometric and the PL bundle is anisometric.
• Therefore the PL bundle is secured on the tibial side first keeping the knee in 100 flexion using bioabsorbable interference screw.
• The AM bundle is secured later with the knee in 300 flexion.

Posto
Follow
op X-Ray
w up X-ra
ys AP and
ay
d Latera
16
l views

Postopeerative Re
17
ehabilitaation Prootocol:

18
Clinical Assessment:
• Recorded prior to surgery and at 1 year follow up.
• Ligament stability was assessed by the use of Lachmans and Anterior Drawer Test.
• Cincinnati Knee Score was used to evaluate the functional outcome.
• Pivot shift test was not used for clinical assessment as it is less reproducible and more subjective.
• The Cincinnati score includes hard shifts, cuts and pivots.
Preoperative findings on physical examination
Grade 0 1 2 3
Anterior Drawer test
OTLP (n=18) 0 0 11 7
SB (n=20) 0 1 13 6
DB (n=20) 0 0 12 8
Lachman’s test
OTLP (n=18) 0 1 10 7
SB (n=20) 0 0 14 6
DB (n=20) 0 0 13 7
19
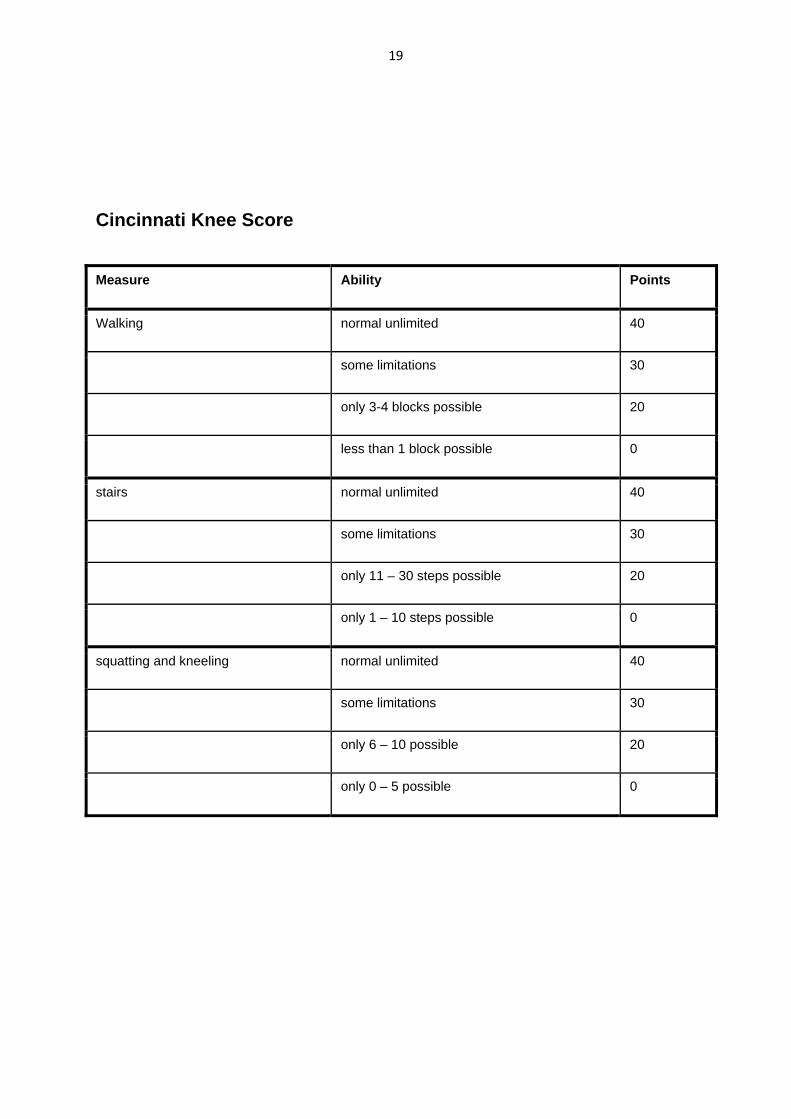
Cincinnati Knee Score
Measure Ability Points
Walking normal unlimited 40
some limitations 30
only 3-4 blocks possible 20
less than 1 block possible 0
stairs normal unlimited 40
some limitations 30
only 11 – 30 steps possible 20
only 1 – 10 steps possible 0
squatting and kneeling normal unlimited 40
some limitations 30
only 6 – 10 possible 20
only 0 – 5 possible 0
20
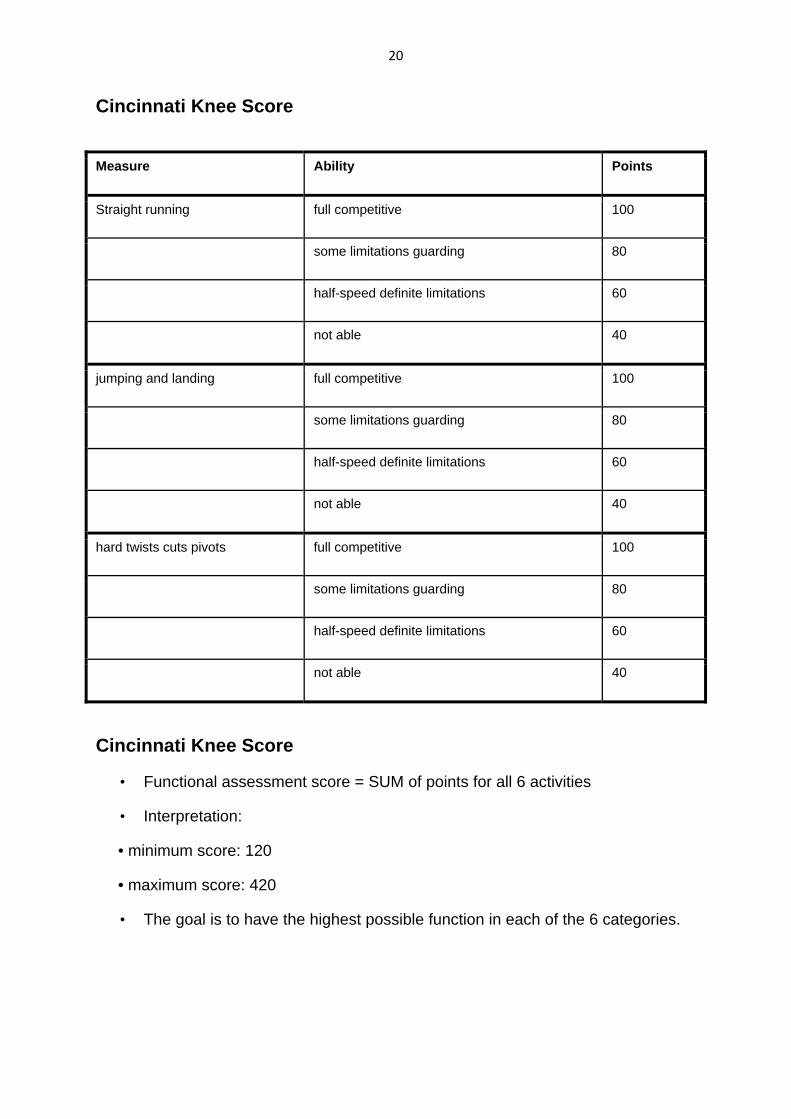
Cincinnati Knee Score
Measure Ability Points
Straight running full competitive 100
some limitations guarding 80
half-speed definite limitations 60
not able 40
jumping and landing full competitive 100
some limitations guarding 80
half-speed definite limitations 60
not able 40
hard twists cuts pivots full competitive 100
some limitations guarding 80
half-speed definite limitations 60
not able 40
Cincinnati Knee Score
• Functional assessment score = SUM of points for all 6 activities
• Interpretation:
• minimum score: 120
• maximum score: 420
• The goal is to have the highest possible function in each of the 6 categories.
•
Mean A
Male: F
0
5
10
15
20
25
30
0
2
4
6
8
10
12
14
16
18
20
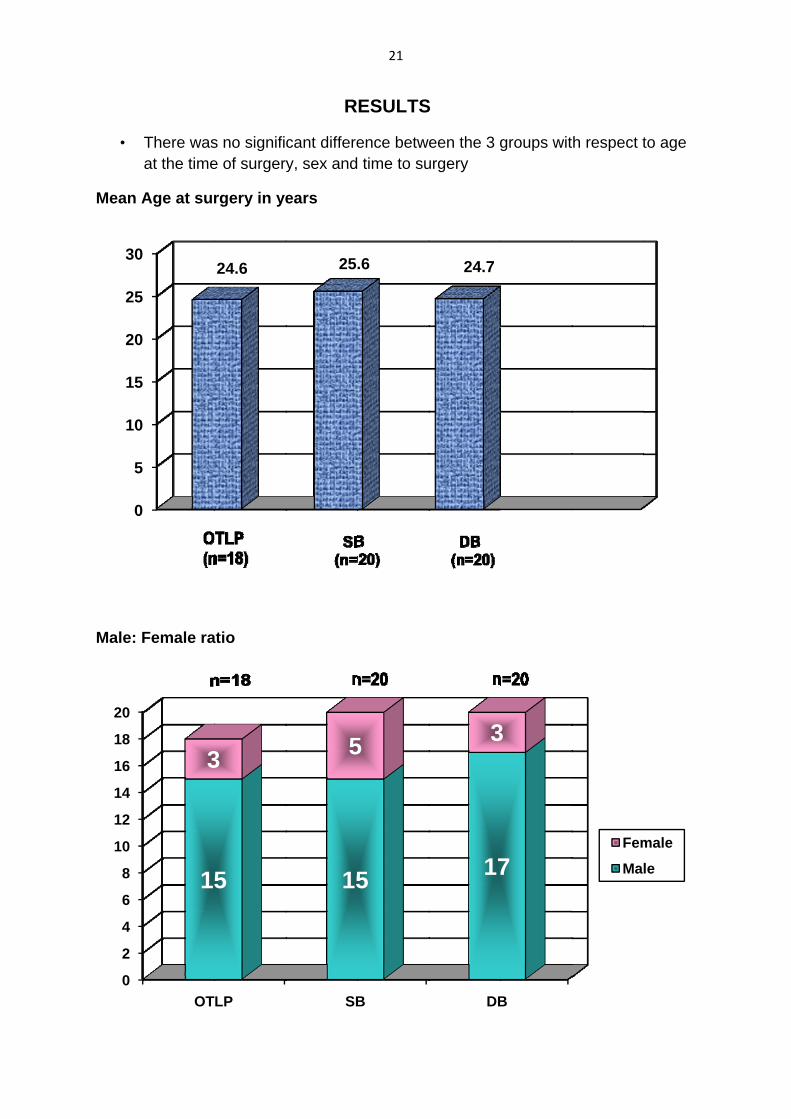
There wasat the time
Age at sur
Female ra
OT
1
3
s no signifie of surgery
rgery in ye
atio
24.6
LP
5
3
R
cant differey, sex and
ears
25
SB
15
5
21
ESULTS
ence betw time to su
.6
B
5
5
S
een the 3 gurgery
24.7
DB
17
3
groups wit
B
7
3
th respect t
Fem
Ma
to age
male
le
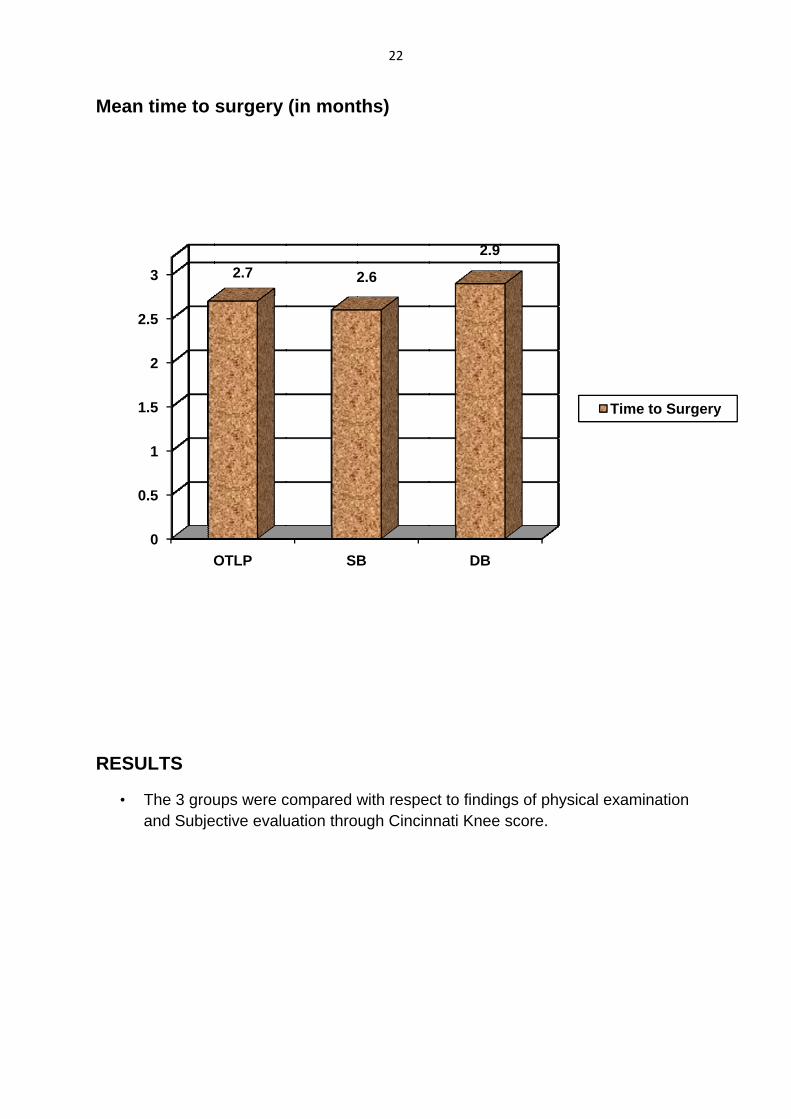
Mean
RESU
•
0
1
2
time to
ULTS
The 3 grouand Subje
0
0.5
1
1.5
2
2.5
3
O
surgery
ups were cective evalu
OTLP
2.7
(in mont
compared wuation thro
SB
2
22
ths)
with respeugh Cincin
B
2.6
ct to findinnnati Knee
DB
2.9
ngs of physscore.
sical exami
Time
ination
e to Surgeryy
23
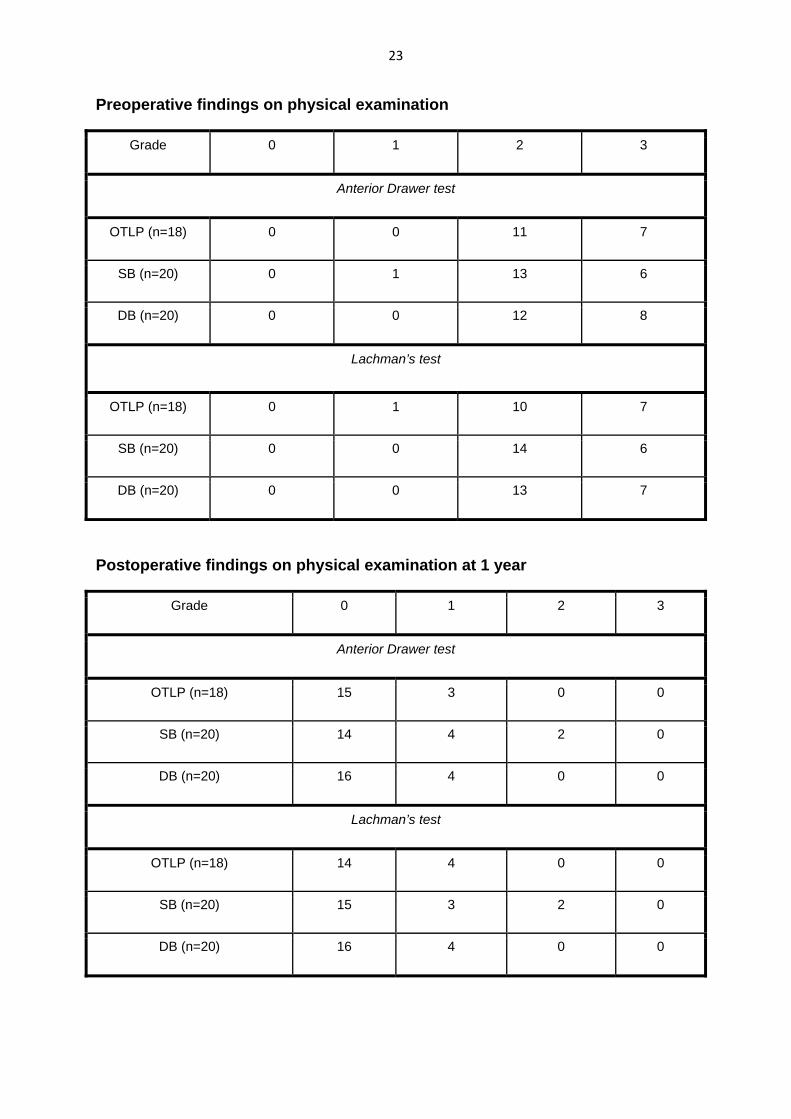
Preoperative findings on physical examination
Grade 0 1 2 3
Anterior Drawer test
OTLP (n=18) 0 0 11 7
SB (n=20) 0 1 13 6
DB (n=20) 0 0 12 8
Lachman’s test
OTLP (n=18) 0 1 10 7
SB (n=20) 0 0 14 6
DB (n=20) 0 0 13 7
Postoperative findings on physical examination at 1 year
Grade 0 1 2 3
Anterior Drawer test
OTLP (n=18) 15 3 0 0
SB (n=20) 14 4 2 0
DB (n=20) 16 4 0 0
Lachman’s test
OTLP (n=18) 14 4 0 0
SB (n=20) 15 3 2 0
DB (n=20) 16 4 0 0
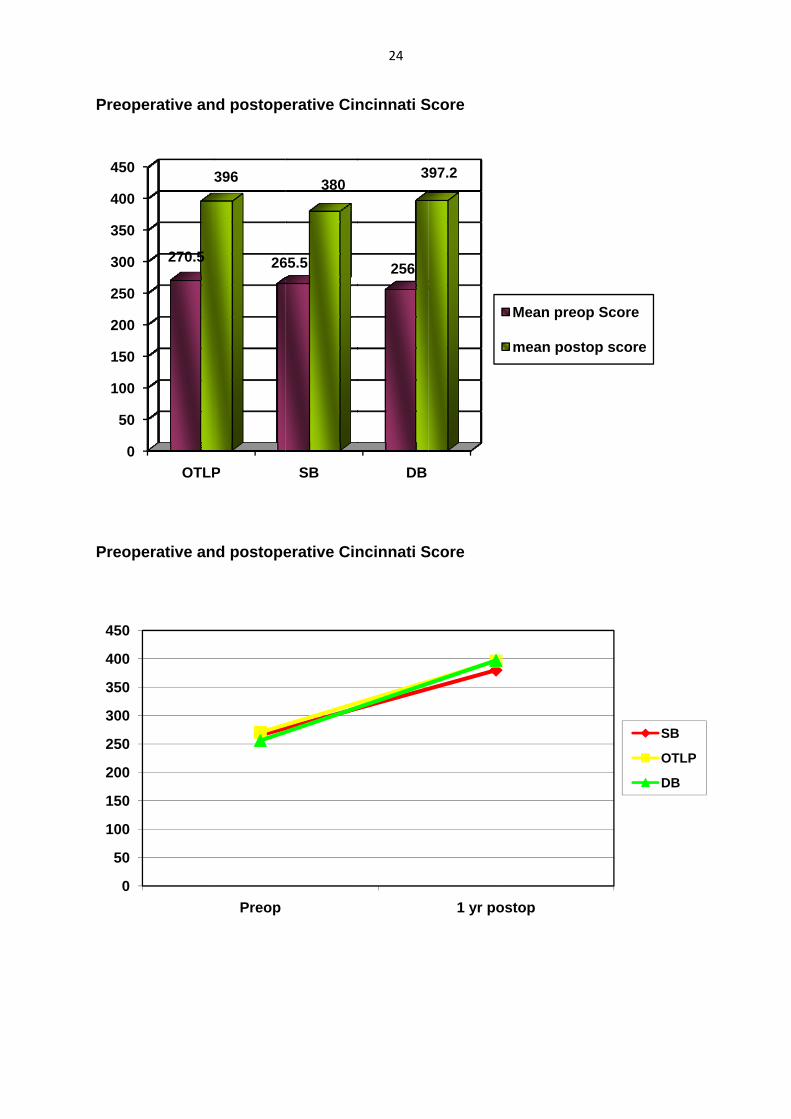
Preope
Preope
0
50
100
150
200
250
300
350
400
450
0
50
100
150
200
250
300
350
400
450
erative an
erative an
OTLP
270.5
3
d postope
d postope
P
26
396
Preop
erative Cin
erative Cin
SB
65.5
380
24
ncinnati S
ncinnati S
DB
256
3
Score
Score
97.2
1 yr po
Mean pre
mean po
ostop
eop Score
ostop scoree
SB
OTLP
DB
25
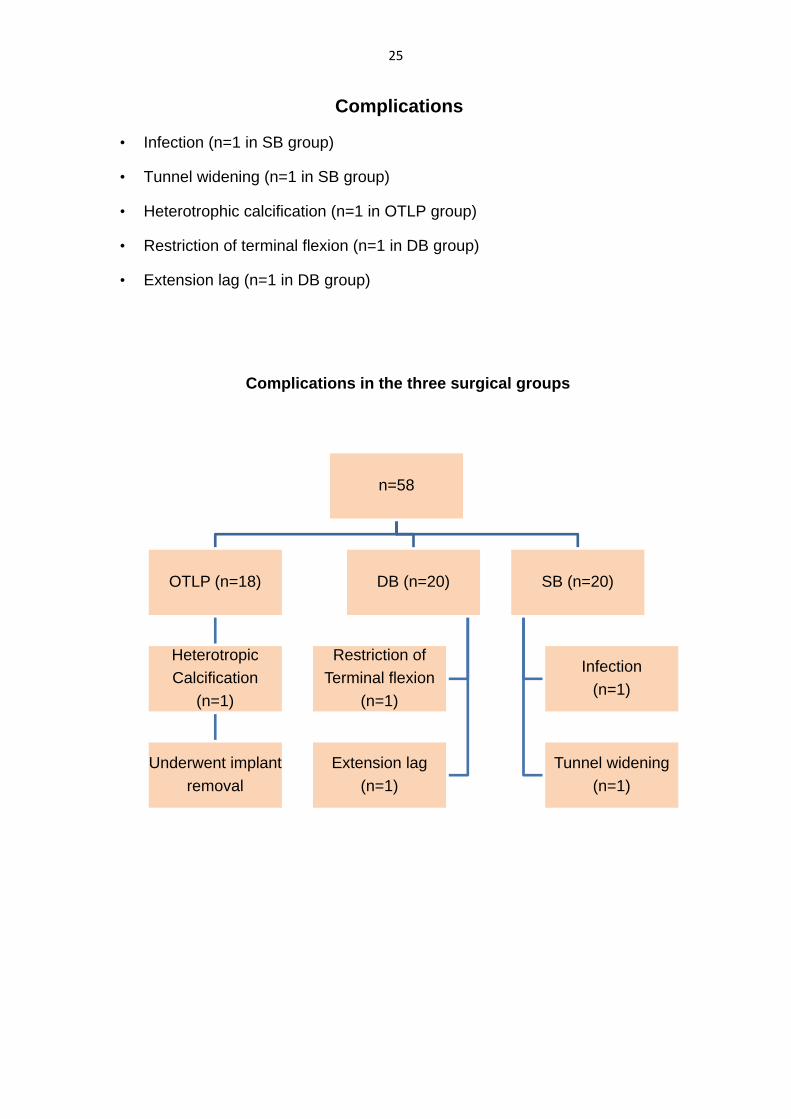
Complications
• Infection (n=1 in SB group)
• Tunnel widening (n=1 in SB group)
• Heterotrophic calcification (n=1 in OTLP group)
• Restriction of terminal flexion (n=1 in DB group)
• Extension lag (n=1 in DB group)
Complications in the three surgical groups
n=58
OTLP (n=18)
Heterotropic Calcification
(n=1)
Underwent implant removal
DB (n=20)
Restriction of Terminal flexion
(n=1)
Extension lag(n=1)
SB (n=20)
Infection(n=1)
Tunnel widening(n=1)
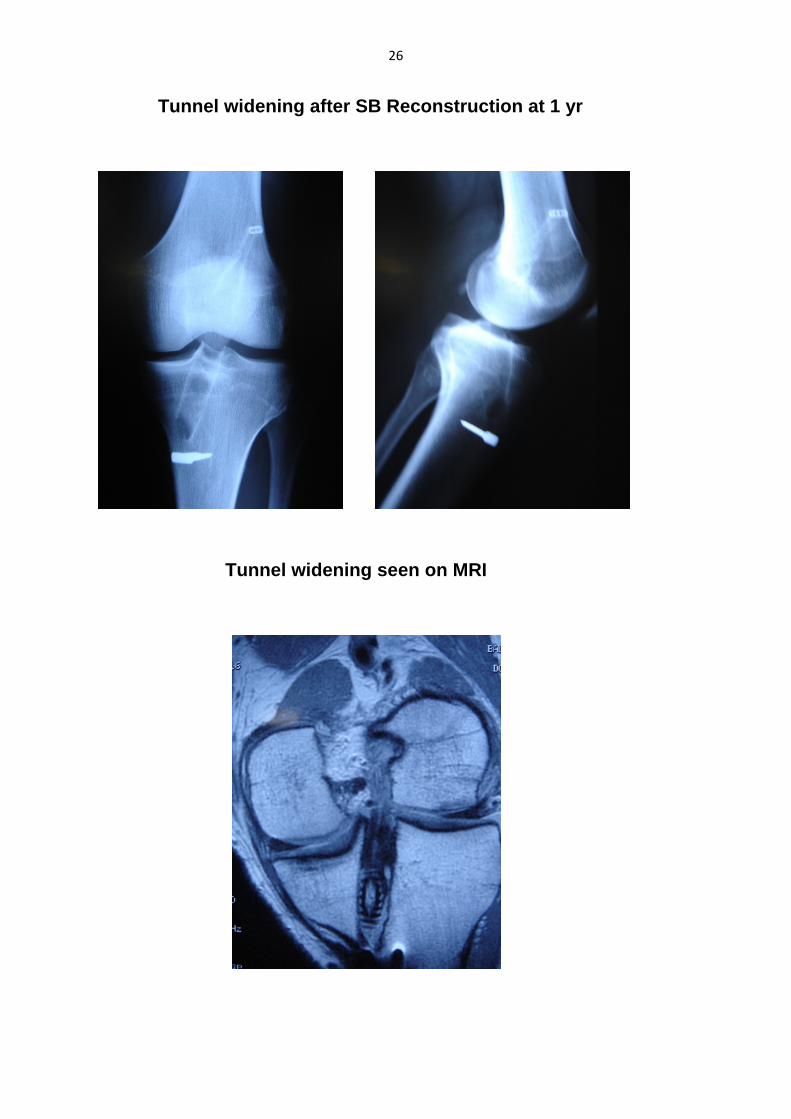
26
Tunnel widening after SB Reconstruction at 1 yr
Tunnel widening seen on MRI
27
DISCUSSION
• The overall results were comparable in all 3 groups.
• The incidence of antero-posterior laxity was less in the DB and OTLP groups as compared to the SB group.
• There was no incidence of kneeling pain.
• Hypoesthesia around the graft harvest site was seen in few patients and can be attributed to the involvement of saphenous nerve
28
Conclusions and recommendations
• The sample size was small and hence statistical analysis was difficult.
• The patients were not allotted to the 3 treatment groups in a randomized manner due to graft length issues and patients’ financial constraints.
• Since we did not evaluate pivot shift test preoperatively, we were unable to determine whether rotational laxity influenced patient satisfaction with regard to surgical outcome
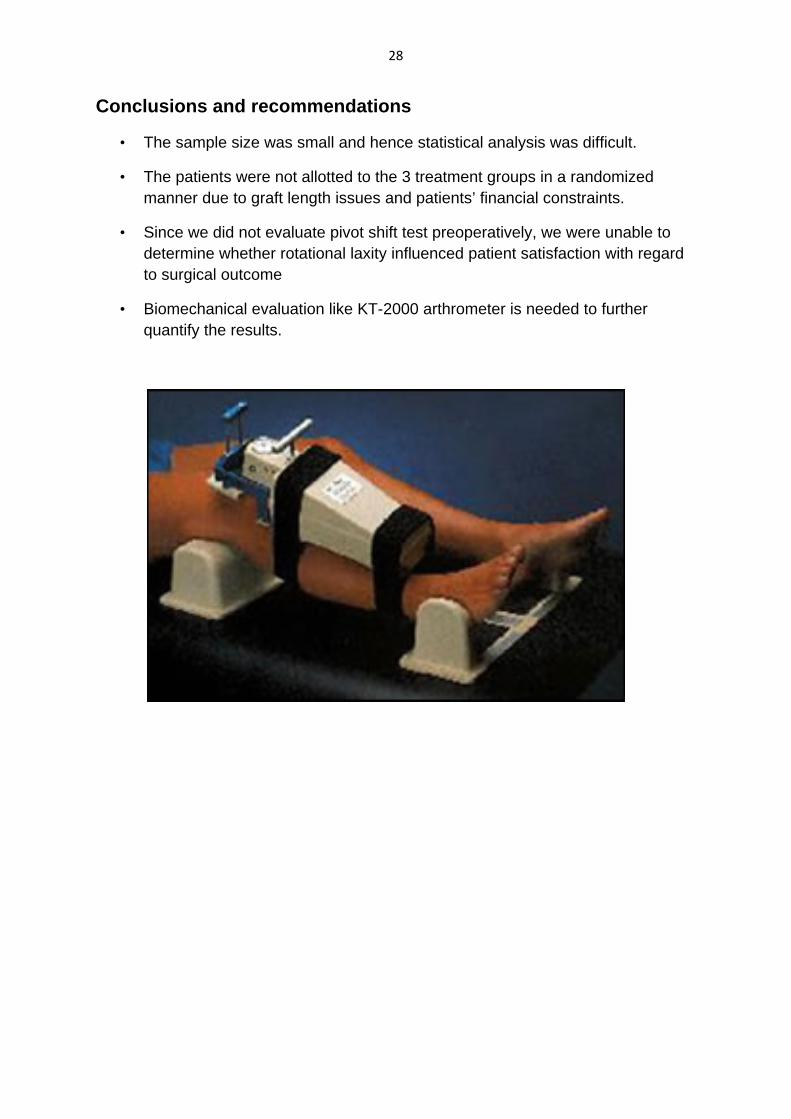
• Biomechanical evaluation like KT-2000 arthrometer is needed to further quantify the results.
29
REFRENCES
1. Yasuda et al, Arthroscopy. 2006 Mar;22(3):240‐51
2. Fu F H et al Sports Med. 2006;36(2):99‐108
3. Kurosaka et al, Clin Orthop Relat Res. 2007 Jan;454:100‐7.
4. Noyes FR et al.Clin Orthopaedics and Related Research. 1989; 246: 238-249
30





























