Embed Size (px)
Citation preview

*Equal contribution to the work.
Acknowledgments: the authorsthank Christophe Marzac, BrunoVaret, Aurélie Hummel and BrunoCassinat for their precious help in recruiting patients and SylvieHermouet for scientific discus-sions.
Funding: this work was supported by grants from the “Associationpour la Recherche sur le Cancer”(ARC), the French NationalCancer Institute (“INCa”, PNESRein, and Réseau NationalPrédispositions héréditaires aucancer du rein) and the FrenchLigue Nationale contre le Cancer(Comités du Cher et de l’Indre) aswell as by the HypoxiaNet COSTAction TD0901. DH is supported by a postdoctoral Marie Curie IEFFellowship from the EuropeanCommission and the SassellaStiftung. DH and RHW are supported by grants from the State Secretariat of Education and Research (C10.0106) andfrom the NCCR Kidney.CH, funded by the SNF.
Manuscript received onMarch 28, 2011. Revisedversion arrived on July 6, 2011.Manuscript accepted on September 5, 2011.
Correspondence: Betty Gardie, Laboratoire deGénétique Oncologique EPHE,INSERM U753, Institut deCancérologie Gustave Roussy,Villejuif, France. E-mail: [email protected]
The online version of this articlehas a Supplementary Appendix.
Distinct deregulation of the hypoxia inducible factor by PHD2 mutants identifiedin germline DNA of patients with polycythemia Charline Ladroue,1* David Hoogewijs,2* Sophie Gad,1 Romain Carcenac,1 Federica Storti,2 Michel Barrois,3
Anne-Paule Gimenez-Roqueplo,4 Michel Leporrier,5 Nicole Casadevall,6 Olivier Hermine,7 Jean-Jacques Kiladjian,8
André Baruchel,9 Fadi Fakhoury,10 Brigitte Bressac-de Paillerets,3,11 Jean Feunteun,12 Nathalie Mazure,13
Jacques Pouysségur,13 Roland H. Wenger,2 Stéphane Richard,1,14 and Betty Gardie1
1Génétique Oncologique EPHE, INSERM U753, Institut de Cancérologie Gustave Roussy, Villejuif et Faculté de Médecine Paris-Sud,Le Kremlin-Bicêtre, France; 2Institute of Physiology and Zürich Center for Integrative Human Physiology ZIHP, University of Zürich,Zürich, Switzerland; 3Service de Génétique, Institut de Cancérologie Gustave Roussy, Villejuif, France; 4Assistance Publique-Hôpitaux de Paris, Hôpital Européen Georges Pompidou, Service de Génétique, Paris, France; INSERM, UMR970, Paris-Cardiovascular Research Center at HEGP, Paris, France; Université Paris Descartes, Faculté de Médecine, Paris, France; 5CHU deCaen, Service d’Hématologie Clinique, France; 6Hôpital Saint Antoine, Assistance Publique–Hôpitaux de Paris and Pierre et MarieCurie University, Institut Gustave Roussy, Inserm, UMR790, Villejuif, France; 7Service d’Hématologie, Hôpital Necker-EnfantsMalades, AP-HP, Paris, France; 8Centre d’Investigations Cliniques, Hôpital Saint-Louis, AP-HP, Paris, France; 9Service d’Hématologie,Hôpital St. Louis, Paris, France; 10Service de Néphrologie, Hôpital Necker, Paris, France; 11Unité INSERM U946, Variabilité Génétiqueet Maladies Humaines, Fondation Jean Dausset/CEPH Unité, Paris, France; 12Institut de Cancérologie Gustave Roussy, CNRS-UMR8200, Villejuif, France; 13Institut de Biologie du Développement et Cancer, Université de Nice - Sophia Antipolis, CNRS UMR-6543, France, and 14Centre Expert National Cancers Rares INCa “PREDIR” and Réseau National INCa, AP-HP, Service d'Urologie,CHU, Le Kremlin-Bicêtre and Service de Néphrologie, Hôpital Necker, Paris, France
BackgroundCongenital secondary erythrocytoses are due to deregulation of hypoxia inducible factor result-ing in overproduction of erythropoietin. The most common germline mutation identified in thehypoxia signaling pathway is the Arginine 200-Tryptophan mutant of the von Hippel-Lindautumor suppressor gene, resulting in Chuvash polycythemia. This mutant displays a weak defi-ciency in hypoxia inducible factor α regulation and does not promote tumorigenesis. Other vonHippel-Lindau mutants with more deleterious effects are responsible for von Hippel-Lindaudisease, which is characterized by the development of multiple tumors. Recently, a few muta-tions in gene for the prolyl hydroxylase domain 2 protein (PHD2) have been reported in casesof congenital erythrocytosis not associated with tumor formation with the exception of onepatient with a recurrent extra-adrenal paraganglioma.
Design and MethodsFive PHD2 variants, four of which were novel, were identified in patients with erythrocytosis.These PHD2 variants were functionally analyzed and compared with the PHD2 mutant pre-viously identified in a patient with polycythemia and paraganglioma. The capacity of PHD2to regulate the activity, stability and hydroxylation of hypoxia inducible factor αwas assessedusing hypoxia-inducible reporter gene, one-hybrid and in vitro hydroxylation assays, respec-tively.
ResultsThis functional comparative study showed that two categories of PHD2 mutants could be dis-tinguished: one category with a weak deficiency in hypoxia inducible factor α regulation anda second one with a deleterious effect; the mutant implicated in tumor occurrence belongs tothe second category.
ConclusionsAs observed with germline von Hippel-Lindau mutations, there are functional differencesbetween the PHD2 mutants with regards to hypoxia inducible factor regulation. PHD2 muta-tion carriers do, therefore, need careful medical follow-up, since some mutations must be con-sidered as potential candidates for tumor predisposition.
Key words: hypoxia inducible factor, hypoxia-inducible transcription factor, PHD2, erythro-cytosis.
Citation: Ladroue C, Hoogewijs D, Gad S, Carcenac R, Storti F, Barrois M, Gimenez-Roqueplo A-P, Leporrier M, Casadevall N, Hermine O, Kiladjian J-J, Baruchel A, Fakhoury F, Bressac-dePaillerets B, Feunteun J, Mazure N, Pouysségur J, Wenger RH, Richard S, and Gardie B. Distinctderegulation of the hypoxia inducible factor by PHD2 mutants identified in germline DNA of patientswith polycythemia. Haematologica 2012;97(1):9-14. doi:10.3324/haematol.2011.044644
©2012 Ferrata Storti Foundation. This is an open-access paper.
ABSTRACT
haematologica | 2012; 97(1)
ORIGINAL ARTICLES
9

Introduction
Secondary erythrocytosis is due to external factors suchas increased production of erythropoietin, the origin ofwhich is variable and may result from germline mutationsin genes encoding factors involved in the oxygen-sensingpathway. The primary cellular component implicated inoxygen homeostasis is the hypoxia-inducible transcriptionfactor (HIF). HIF operates as a heterodimer composed of aconstitutively expressed beta subunit, also known as arylhydrocarbon receptor nuclear translocator, and an alphasubunit (1α, 2α or 3α) that is tightly regulated by oxygen viapost-translational modification. The prolyl-4-hydroxylasedomain (PHD) enzymes hydroxylate proline residues locat-ed in the oxygen-dependent degradation (ODD) domain ofHIF-α. This hydroxylation allows the binding of the vonHipple-Lindau protein (pVHL), the substrate recognitionsubunit of an E3 ubiquitin ligase complex that induces ubiq-uitination and subsequent degradation of HIF-α by the pro-teasome.1,2 In the absence of oxygen, HIF-α is stabilized,heterodimerizes with HIF-1b and induces expression ofhundreds of genes involved in cell survival, angiogenesis,erythropoiesis and cell proliferation.2,3 There is somerestricted target gene specificity depending on the HIF-αsubunit of the HIF-α/b heterodimeric transcription factor.For example, renal and hepatic erythropoietin is regulatedby the HIF-2α subunit in vivo.4-7 Germline mutations ingenes involved in the HIF pathway have been reported inassociation with syndromes that predispose patients toboth neoplasms and/or congenital secondary erythrocyto-sis.8 The most frequent mutations involve the VHL tumorsuppressor gene. Heterozygous germline mutations in thisgene are responsible for von Hippel-Lindau (VHL) disease,an autosomal dominant condition predisposing to multipletumors including central nervous system and retinal heman-gioblastomas, clear-cell renal cell carcinoma, pheochromo-cytomas and pancreatic endocrine tumors.8 Established cor-relations between genotype and phenotype predict the riskof paraganglioma/pheochromocytoma, with VHL deletionsor truncating mutations being associated with a low risk(VHL type 1) and VHLmissense mutations being associatedwith a high risk (VHL type 2).9,10In addition, a homozygous 598C>T (R200W) VHL
germline mutation has been shown to account for Chuvashcongenital polycythemia, an autosomal recessive disease,endemic in the Chuvash Autonomous Republic of theRussian Federation.11 Homozygous carriers of the R200W-VHL germline mutation do not develop tumors but insteadhave Chuvash congenital polycythemia due to high levelsof erythropoietin.11 The lack of tumor development in thisdisorder is due to a weak defect of the mutation in terms ofits HIF-α regulation (leading to delayed ubiquitination)because of its localization outside pVHL functionaldomains.11 Other homozygous and compound heterozy-gous polycythemia-associated VHL mutations have alsobeen reported.10 Functional studies of some of these mutantshave shown a weak to undetectable defect of HIF-1α regu-lation (unpublished data).Recently, a similar phenotype of high erythropoietin-
associated polycythemia without associated tumors hasbeen reported in carriers of heterozygous germline muta-tions in the PHD2 and HIF-2A genes,12-19 with the exceptionof one patient carrying a H374R-PHD2mutation.20 This par-ticular patient simultaneously developed congenital second-ary erythrocytosis and recurrent paraganglioma, a tumor
originating from neural crest cells similar to pheochromocy-toma but with an extra-adrenal localization.20 The analysisof the tumor showed a loss of heterozygosity including thewild-type PHD2 allele, suggesting a potential tumor sup-pressor role of PHD2.PHD2 and VHL act in concert to regulate HIF-α. Based on
the observation that VHLmutation carriers display differentphenotypes depending on the relative capacity of the VHLmutants to regulate HIF, we sought to define the genotype-phenotype relationship regarding the capacity of PHD2mutants to differentially regulate HIF-α. Here we report afunctional study comparing five PHD2 variants associatedwith isolated congenital secondary erythrocytosis with themutation identified in a patient with recurrent paragan-glioma.
Design and Methods
Patients and mutation screeningThirty-four patients who did not fulfill World Health
Organization diagnostic criteria for polycythemia vera were inves-tigated. The local ethics committee of Kremlin Bicetre Hospitalapproved the study and all patients provided written informedconsent. Blood samples were collected from all patients andgermline DNA was extracted and analyzed by direct sequencing.20
DNA from the blood of healthy donors of Caucasian origin wasused as a control.
Assay of hypoxia inducible factor transcriptional activityIn order to assay HIF transcriptional activity, dual luciferase
assays were performed in Hek293T cells as described previously.20
A pGL3promoter vector expressing luciferase under the control ofhypoxia response elements21 was used. Cells were exposed tohypoxic conditions (1% O2) for 4 h before extraction.
Assay of hypoxia inducible factor stabilityHeLa cells were transiently co-transfected with increasing
amounts (50-200 ng) of an expression vector encoding the HIF-2αODD domain (amino acids 404-569), fused to yeast Gal4 DNA-binding domain and Herpes simplex VP16-derived transactivationdomain, together with the Gal4-response element driven fireflyluciferase reporter, pGRE5xE1b (125 ng), and a Renilla luciferasecontrol plasmid (4 ng).22 Twenty-four hours post-transfection, cellswere cultured under either normoxic (20% O2) or hypoxic (1% O2)conditions for an additional 16 h, and firefly luciferase activity wasdetermined and normalized to Renilla luciferase activity.
Hydroxylation assayPHD2 and HIF-ODD proteins (plasmid pcDNA3-HA-Gal4-HIF-
1α-ODD was a generous gift from WG Kaelin Jr, Dana-FarberCancer Institute, Boston, USA)23 were produced in wheat germextract in vitro using the TnT transcription-translation kit(Promega). The hydroxylation reaction was carried out by mixingPHD2 and HIF-1α-ODD (amino acids 536-652) proteins in a reac-tion buffer containing co-factors (Fe2+, ascorbic acid and 2-oxoglu-tarate) as described previously.24 The samples were incubated at30°C, collected at different time points, and immunoblotted withanti-HA (Tebu) and anti-HIF-1α (Pro 564)-OH (Cell-SignalingTechnology) antibodies.
Results
We sequenced the PHD2 gene on germline DNA from a
C. ladroue et al.
10 haematologica | 2012; 97(1)

series of Caucasian patients with unexplained poly-cythemia associated with normal or elevated serum ery-thropoietin levels (Figure 1A). Four novel heterozygoussequence variants were identified in the PHD2 gene[c.G471C, p.Gln157His (Q157H); c.C599A, p.Pro200Gln(P200Q); c.G760C, p.Asp254His (D254H); c.C1192T,p.Arg398X (R398X)] as well as the already describedc.G1112A, p.Arg371His (R371H) mutation16 (Figures 1A andB). Genetic testing was performed on available parents andrelatives of the PHD2 mutation carriers, but no mutationwas found except in the mother of the PHD2-R398X carrierwho presented characteristics of polycythemia (Figure 1A).She harbors the PHD2mutation but with a mosaic status asdemonstrated by the reduced height of the peak on thesequence chromatogram (Figure 1B). The low proportion ofthe mutated allele was confirmed by a quantitative allele-specific oligonucleotide method (data not shown). Concerning the other families, only a few relatives were
available for further genetic and clinical investigations butthere was no history of familial polycythemia. Briefly, thebrother, the sister and the son of patient #2295 and thefather of patient #2403 agreed to genetic testing and werenot carriers of PHD2mutation. Other parents had died pre-viously, of known causes in two cases: esophageal cancerfor the mother of patient #2403 and colon cancer for themother of patient #2412. Finally, patient #0424 was anadopted child, without children.The frequencies of the different variants were evaluated
in a control population (Figure 1C). Only the Q157H variantwas found and was, therefore, classified as a polymor-phism. Analysis of amino acid conservation supports thisconclusion, as the Q157 amino acid is not conserved eitherbetween species or within the PHD protein family (PHD1and 3) (Online Supplementary Table S1). In contrast, aminoacids P200 and R371 are highly conserved and the D254amino acid is fully conserved, similar to H374 described inour previous study.20 As far as concerns the location of the
amino acids in the protein, D254, like H374, is part of thePHD2 catalytic site.25 The P200 amino acid is located withinthe nuclear localization signal (NLS) implicated in the shut-tling of PHD2 between the cytoplasm and the nucleuswhich plays a crucial role in HIF regulation.26 We tested theshuttling of the P200Q mutation by immunofluorescencebut we did not observe any impact of the mutation on thecapacity of PHD2 to shuttle (data not shown).The functional consequences of these mutations on
PHD2 activity were first evaluated using a hypoxia reporterassay based on the transcriptional activity of endogenousHIF (accumulated during 4 h of hypoxia). A luciferasereporter gene driven by a hypoxia response element derivedfrom the erythropoietin 3' enhancer was used. Addingwild-type PHD2 led to a dose-dependent suppression ofHIF-α-mediated luciferase expression (Figure 2A). Asexpected, the PHD2 variant with the Q157H polymor-phism reduced luciferase activity to the same extent aswild-type PHD2 (Figure 2A). Within the different missensemutations, we observed two types of mutants: one type(including PHD2-P200Q and R371H) did not affect thecapacity of PHD2 to regulate HIF-α transcriptional activity,whereas a second type (including PHD2-D254H andH374R) completely abrogated PHD2 activity (Figure 2A). We next studied the PHD2 mutants using a one-hybrid
reporter assay based on the capacity of PHD2 to induceHIF-α protein instability. Cells were co-transfected withexpression vectors containing the different PHD2 mutants(50 to 200 ng), the oxygen-dependent degradation domainof HIF-2α (HIF-2α-ODD) fused to yeast Gal4 DNA-bindingdomain and Herpes simplex VP16-derived transactivationdomain, together with a reporter vector expressingluciferase under the control of a Gal4-response element. Inthis assay, luciferase expression reflects the stability of HIF-2α-ODD. A trend similar to that in the previous test wasobtained: there was no detectable effect of the P200Q andR371H substitutions on PHD2 activity (which was compa-
Deregulation of HIF by PHD2 mutants
haematologica | 2012; 97(1) 11
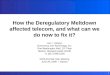
Figure 1. Identification of PHD2mutations in patients with poly-cythemia. (A) Table of patients diag-nosed with erythrocytosis and aPHD2 variation. Ht: hematocrit; Hb:hemoglobin; RC: number of redcells; EPO: erythropoietin; m: male;f: female; N: normal; NA: not avail-able; *: previously described.20 (B)Sequence chromatogram of PHD2 inthe area of the mutated nucleotide.Wild-type DNA was used as refer-ence (Ref) (top) and compared togermline DNA of the patient (bot-tom). Only one relative of a patientwas available for genetic testing (themother of the PHD2-R398X carrier).She harbors the PHD2 mutation butwith a mosaic pattern as demon-strated by the reduced height of thepeak on the sequence chro-matogram. (C) Frequency of thePHD2 variations in a control popula-tion.
A
B
C

rable to that of the wild-type PHD2) and there was totalabolition of the D254H mutant activity (comparable to thatof the truncated PHD2 variant R398X) (Figure 2B). Identicalresults were obtained using a HIF-1α-ODD stabilityreporter (data not shown). The experiment was repeatedwith the P200Q-PHD2 mutant in oxygen-regulated ery-thropoietin-expressing cells (including the humanhepatoma cell line Hep3B and renal erythropoietin-produc-ing cells, a new cell model isolated from the tumor-free tis-sue of a patient with renal carcinoma) but no significant dif-ference was observed (data not shown).27We next performed a sensitive in vitro assay in order to
test the ability of the PHD2 mutants to hydroxylate HIF-1αin a time-dependent manner. In this assay, in vitro-translatedPHD2 proteins were mixed with HIF-1α-ODD in the pres-ence of co-factors necessary for the hydroxylation reaction.The capacity of the different PHD2 mutants to hydroxylateHIF-1α was measured by immunoblotting using an anti-body specific for the hydroxylated HIF-1α-ODD (HIF-OH,Figure 3A). The H374R and D254H substitutions totallyimpaired HIF-1α hydroxylation (Figure 3A). By contrast theR371H mutant behaved like the wild-type PHD2 and theP200Q mutant, although capable of hydroxylating HIF-1α(Figure 3A), showed a reproducible and consistent delay(Figure 3B).
Discussion
Taken together, these results show that PHD2mutationscan be divided into several different classes in terms oftheir effects on HIF regulation. Genotype/phenotype corre-lations cannot be established for PHD2 mutations becausethey are rare events that have been reported in only ten
families to date (including those in the present study), incontrast to the 945 families described with a VHL muta-tion.10 In addition, the parents of the PHD2 mutation carri-ers reported in the literature were either dead or not avail-able for further genetic and clinical investigations (includ-ing one parent who died of esophageal cancer18). In ourstudy, only one parent was genetically tested and diag-nosed as a mosaic carrier which prevents any conclusionregarding the developed phenotype. Nonetheless, regard-ing the close functional relation between VHL and PHD2 inthe regulation of HIF and the implication of the HIF path-way in the genesis of pheochromocytoma,28-31 we canhypothesize similarities between the various types ofmutants and raise the question of a possible risk of devel-opment of paraganglioma/pheochromocytoma in PHD2mutation carriers. Subjects with one category of mutantion(P200Q and R371H) display features similar to those withthe VHL-R200W mutantion responsible for Chuvash poly-cythemia without any increased risk of neoplasia.11 Likethe VHL-R200W mutant, which is located outside func-tional domains, the PHD2-P200Q and R371H mutationsare not located in the catalytic domain of the enzyme andhave a moderate impact on HIFα regulation. In addition,the VHL-R200W mutant only induces delayed ubiquitina-tion of HIFα which may be comparable to the delayedhydroxylation of HIFα observed with the PHD2-P200Qmutant. Interestingly, Pro200 is only one residue N-termi-nal to Cys201 which has been shown to chelate zinc andcadmium ions, providing evidence for the existence of asecond metal binding site on PHD2.32,33 This Cys201 affectsPHD2 hydroxylation activity and appears to be implicatedin redox signaling in vitro.34 The very close location to thefunctionally important Cys201 residue could be the causeof the delayed hydroxylation of HIF-1α by the PHD2-
C. ladroue et al.
12 haematologica | 2012; 97(1)
Figure 2. Functional study of PHD2 mutants using luciferase reporter assays. (A) PHD2-dependent regulation of endogenous HIF in an assaybased on a hypoxia response element reporter gene. Cells were co-transfected in a 12-well format with various amounts of pcDNA3-HA-PHD2 expression vectors (to enable the expression of the same amount of PHD2 proteins) in addition to pGL3 reporter vectors encodingfirefly luciferase under the control of a sensitive hypoxia response element and Renilla luciferase as a control of transfection efficiency. Cellswere placed in hypoxic conditions (1% O2) for 4 h in order to accumulate endogenous HIFα before being collected. Results are given in per-centage of firefly luciferase activity normalized to Renilla luciferase activity. The amount of HA-PHD2 transfected (PHD2) was quantified byimmunoblotting using an anti-HA antibody. (B) The effect of PHD2 effect on HIF-2α protein stability in a one-hybrid reporter assay. Cells werecotransfected in a 6-well format with various amounts of pcDNA3-HA-PHD2 expression vectors (200, 100 and 50 ng), a Gal4-VP16-HIF-2αODD (amino acids 404-569) construct as well as a Gal4 response element-driven firefly luciferase reporter and a Renilla luciferase controlplasmid. Twenty-four hours post-transfection cells were incubated for 16 h in normoxic or hypoxic conditions. Results are mean values ofthree independent experiments performed in triplicate.
A BNormoxiaHypoxia Normoxia
Hypoxia
PHD2wt Q157H P200Q R371H D254H R398X
PHD2wt Q157H P200Q R371H D254H H374R
PHD2(ng):
IB PHD2
0 0 40 20 10 40 20 10 40 20 10 40 20 10 40 20 10 320160 80
Relative luciferase activity
(Firefly/Renilla ratio)
Luciferase activity (%
)
4
3,5
3
2,5
2
1,5
1
0,5
0
120
100
80
60
40
20
0

P200Q mutant. Intriguingly, concerning the R371Hmutant, the previously reported loss-of-function effect ofthis mutant16 could not be confirmed by any of the threetests of our study. The R371H mutation segregates witherythrocytosis in two different families (described hereinand by Percy et al.16) and is unequivocally involved in thispathology. We currently cannot explain why, in our hands,the R371H mutation failed to abolish PHD2 catalytic activ-ity. The PHD2 expression vectors were re-sequenced andtheir functions confirmed by immunoblotting. Parallelexperiments with other PHD2 mutants confirmed thevalidity of our assays. For this category of mutants whichhave a moderate impact on HIFα regulation, we cannotrule out potential indirect regulation on the oxygen sensingpathway via PHD2-interacting proteins. Indeed, during thepast decade a large number of PHD2-interacting proteinshave been discovered, including both upstream regulatorsand downstream targets of PHD2, substantially increasingthe complexity of the PHD/HIF oxygen-sensing regulationpathway.7 Moreover, PHD2 has been reported to havehydroxylation-independent gene regulatory functions.35-37Another category, including the PHD2-R398X mutation
and three other PHD2 truncated mutations described previ-ously,12 can be compared to the VHL truncation mutations(VHL disease type 1) which are not associated with thedevelopment of pheochromocytomas. Subject with thesefirst two categories could be considered at low risk of devel-oping paraganglioma/pheochromocytoma.A last category could be compared to the VHL missense
mutations involved in VHL disease type 2, associated witha high risk of paraganglioma/pheochromocytoma. This cat-egory includes the previously described PHD2-H374Rmutation identified in a 43-year-old patient with paragan-
glioma. A loss of the PHD2 wild-type allele was demon-strated in the patient with this tumor, arguing for a tumorsuppressor role of PHD2.20 No PHD2 mutations have beenidentified in other series of patients affected by pheochro-mocytomas (73 patients with hereditary paraganglioma andpheochomocytoma syndrome, Gimenez-Roqueplo,Hôpital Européen Georges Pompidou, Paris, unpublisheddata) and/or renal carcinoma,38 but the risk that germlinePHD2 mutation carriers have of developing tumors shouldnot be underestimated. Indeed, like His374, Asp254 is high-ly conserved, and located in the catalytic site of PHD2.25Moreover, the D254H mutation results in a severe loss offunction. Therefore, although no cases of paraganglioma orpheochromocytoma have yet been detected in the D254H-PHD2mutation carrier, this mutation may be considered asa potential candidate for tumor predisposition.In conclusion, using three different approaches we
demonstrated that distinct PHD2 mutations have differen-tial effects on HIF regulation. We suggest that, by analogyto VHL mutations, carriers of particular PHD2 mutationsmay be prone to tumor development. These patients wouldthen require screening for tumor prevention and earlydetection.
Authorship and Disclosures
The information provided by the authors about contributions frompersons listed as authors and in acknowledgments is available withthe full text of this paper at www.haematologica.org.Financial and other disclosures provided by the authors using the
ICMJE (www.icmje.org) Uniform Format for Disclosure ofCompeting Interests are also available at www.haematologica.org.
Deregulation of HIF by PHD2 mutants
haematologica | 2012; 97(1) 13
Figure 3. Functional analysis of PHD2 mutants using an in vitro hydroxyla-tion assay. (A) Immunoblot estimation of HIF-1α-ODD protein hydroxylationin vitro. PHD2 and HIF-1α-ODD proteins were synthesized separately by invitro transcription-translation reactions. The hydroxylation reaction was thenprocessed by mixing HA-PHD2 and HA-HIF-1α-ODD proteins in a reactionbuffer containing PHD2 enzymatic co-factors. The reaction was carried outat 30°C and samples were collected after 0, 10, 30, and 60 min of incuba-tion. For immunoblotting, 10 mL aliquots of the hydroxylation reaction assayswere separated by SDS-PAGE, blotted, and incubated with an anti-HA anti-body [to quantify PHD2 and total HIF-ODD (HIF)] and anti-hydroxylated HIF-1� antibody [to quantify hydroxylated HIF-ODD (HIF-OH)]. (B) Quantification ofhydroxylated HIF-1α. The proportion of hydroxylated HIF-1α was measuredand related to total HIF-1α. The 100% value corresponds to the quantity ofHIF-1α hydroxylated by the PHD2-WT protein after 1 h. Means were obtainedwith three independent experiments.
A
B
HIF-ODD vectorPHD2 vector
PHD2
time:
HIF
HIF-OH
PHD2 WT P200Q D254H Q157H R371H H374R
0 10 30 60 0 10 30 60 0 10 30 60
10’ 30’ 60’ 10’ 30’ 60’
Hydroxylated HIF (%
) 100
80
60
40
20
0
WT P200Q
0 10 30 60 0 10 30 60 0 10 30 60

C. ladroue et al.
14 haematologica | 2012; 97(1)
References
1. Kaelin WG, Jr. The von Hippel-Lindautumour suppressor protein: O2 sensing andcancer. Nat Rev Cancer. 2008;8(11):865-73.
2. Pouyssegur J, Dayan F, Mazure NM.Hypoxia signalling in cancer and approach-es to enforce tumour regression. Nature.2006;441(7092):437-43.
3. Wenger RH, Stiehl DP, Camenisch G.Integration of oxygen signaling at the con-sensus HRE. Sci STKE. 2005;2005(306):re12.
4. Rankin EB, Biju MP, Liu Q, Unger TL, RhaJ, Johnson RS, et al. Hypoxia-inducible fac-tor-2 (HIF-2) regulates hepatic erythropoi-etin in vivo. J Clin Invest. 2007;117(4):1068-77.
5. Rosenberger C, Mandriota S, Jurgensen JS,Wiesener MS, Horstrup JH, Frei U, et al.Expression of hypoxia-inducible factor-1alpha and -2alpha in hypoxic andischemic rat kidneys. J Am Soc Nephrol.2002;13(7):1721-32.
6. Warnecke C, Zaborowska Z, Kurreck J,Erdmann VA, Frei U, Wiesener M, et al.Differentiating the functional role ofhypoxia-inducible factor (HIF)-1alpha andHIF-2alpha (EPAS-1) by the use of RNAinterference: erythropoietin is a HIF-2alphatarget gene in Hep3B and Kelly cells. FasebJ. 2004;18(12):1462-4.
7. Wenger RH, Hoogewijs D. Regulated oxy-gen sensing by protein hydroxylation inrenal erythropoietin-producing cells. Am JPhysiol Renal Physiol. 2010;298(6):F1287-96.
8. Richard S, Graff J, Lindau J, Resche F. VonHippel-Lindau disease. Lancet. 2004;363(9416):1231-4.
9. Maher ER, Webster AR, Richards FM,Green JS, Crossey PA, Payne SJ, et al.Phenotypic expression in von Hippel-Lindau disease: correlations with germlineVHL gene mutations. J Med Genet.1996;33(4):328-32.
10. Nordstrom-O'Brien M, van der Luijt RB,van Rooijen E, van den Ouweland AM,Majoor-Krakauer DF, Lolkema MP, et al.Genetic analysis of von Hippel-Lindau dis-ease. Hum Mutat. 2010;31(5):521-37.
11. Ang SO, Chen H, Hirota K, Gordeuk VR,Jelinek J, Guan Y, et al. Disruption of oxy-gen homeostasis underlies congenitalChuvash polycythemia. Nat Genet. 2002;32(4):614-21.
12. Al-Sheikh M, Moradkhani K, Lopez M,Wajcman H, Prehu C. Disturbance in theHIF-1alpha pathway associated with ery-throcytosis: further evidences brought byframeshift and nonsense mutations in theprolyl hydroxylase domain protein 2(PHD2) gene. Blood Cells Mol Dis. 2008;40(2):160-5.
13. Gale DP, Harten SK, Reid CD, TuddenhamEG, Maxwell PH. Autosomal dominanterythrocytosis and pulmonary arterialhypertension associated with an activatingHIF2 alpha mutation. Blood. 2008;112(3):919-21.
14. Martini M, Teofili L, Cenci T, Giona F, TortiL, Rea M, et al. A novel heterozygousHIF2AM535I mutation reinforces the roleof oxygen sensing pathway disturbances inthe pathogenesis of familial erythrocytosis.Haematologica. 2008;93(7):1068-71.
15. Percy MJ, Beer PA, Campbell G, DekkerAW, Green AR, Oscier D, et al. Novel exon12 mutations in the HIF2A gene associatedwith erythrocytosis. Blood. 2008;111(11):5400-2.
16. Percy MJ, Furlow PW, Beer PA, Lappin TR,McMullin MF, Lee FS. A novel erythrocyto-sis-associated PHD2 mutation suggests thelocation of a HIF binding groove. Blood.2007;110(6):2193-6.
17. Percy MJ, Furlow PW, Lucas GS, Li X,Lappin TR, McMullin MF, et al. A gain-of-function mutation in the HIF2A gene infamilial erythrocytosis. N Engl J Med.2008;358(2):162-8.
18. Percy MJ, Zhao Q, Flores A, Harrison C,Lappin TR, Maxwell PH, et al. A familywith erythrocytosis establishes a role forprolyl hydroxylase domain protein 2 inoxygen homeostasis. Proc Natl Acad SciUSA. 2006;103(3):654-9.
19. van Wijk R, Sutherland S, Van Wesel AC,Huizinga EG, Percy MJ, Bierings M, et al.Erythrocytosis associated with a novel mis-sense mutation in the HIF2A gene.Haematologica. 2010;95(5):829-32.
20. Ladroue C, Carcenac R, Leporrier M, GadS, Le Hello C, Galateau-Salle F, et al. PHD2mutation and congenital erythrocytosiswith paraganglioma. N Engl J Med. 2008;359(25):2685-92.
21. Dayan F, Roux D, Brahimi-Horn MC,Pouyssegur J, Mazure NM. The oxygensensor factor-inhibiting hypoxia-induciblefactor-1 controls expression of distinctgenes through the bifunctional transcrip-tional character of hypoxia-inducible fac-tor-1alpha. Cancer Res. 2006;66(7):3688-98.
22. Koditz J, Nesper J, Wottawa M, Stiehl DP,Camenisch G, Franke C, et al. Oxygen-dependent ATF-4 stability is mediated bythe PHD3 oxygen sensor. Blood. 2007;110(10):3610-7.
23. Ohh M, Park CW, Ivan M, Hoffman MA,Kim TY, Huang LE, et al. Ubiquitination ofhypoxia-inducible factor requires directbinding to the beta-domain of the vonHippel-Lindau protein. Nat Cell Biol. 2000;2(7):423-7.
24. Huang J, Zhao Q, Mooney SM, Lee FS.Sequence determinants in hypoxia-inducible factor-1alpha for hydroxylationby the prolyl hydroxylases PHD1, PHD2,and PHD3. J Biol Chem. 2002;277(42):39792-800.
25. McDonough MA, Li V, Flashman E,Chowdhury R, Mohr C, Lienard BM, et al.Cellular oxygen sensing: crystal structure ofhypoxia-inducible factor prolyl hydroxy-lase (PHD2). Proc Natl Acad Sci USA. 2006;103(26):9814-9.
26. Steinhoff A, Pientka FK, Mockel S,Kettelhake A, Hartmann E, Kohler M, et al.Cellular oxygen sensing: importins andexportins are mediators of intracellular
localisation of prolyl-4-hydroxylases PHD1and PHD2. Biochem Biophys ResCommun. 2009;387(4):705-11.
27. Frede S, Freitag P, Geuting L, Konietzny R,Fandrey J. Oxygen-regulated expression ofthe erythropoietin gene in the human renalcell line REPC. Blood. 2011;117(18):4905-14.
28. Dahia PL, Ross KN, Wright ME, HayashidaCY, Santagata S, Barontini M, et al. AHIF1alpha regulatory loop links hypoxiaand mitochondrial signals in pheochromo-cytomas. PLoS Genet. 2005;1(1):72-80.
29. Eisenhofer G, Huynh TT, Pacak K,Brouwers FM, Walther MM, Linehan WM,et al. Distinct gene expression profiles innorepinephrine- and epinephrine-produc-ing hereditary and sporadic pheochromo-cytomas: activation of hypoxia-drivenangiogenic pathways in von Hippel-Lindausyndrome. Endocr Relat Cancer. 2004;11(4):897-911.
30. Favier J, Briere JJ, Burnichon N, Riviere J,Vescovo L, Benit P, et al. The Warburgeffect is genetically determined in inheritedpheochromocytomas. PLoS One. 2009;4(9):e7094.
31. Pollard PJ, El-Bahrawy M, Poulsom R, EliaG, Killick P, Kelly G, et al. Expression ofHIF-1alpha, HIF-2alpha (EPAS1), and theirtarget genes in paraganglioma andpheochromocytoma with VHL and SDHmutations. J Clin Endocrinol Metab.2006;91(11):4593-8.
32. Mecinovic J, Chowdhury R, Flashman E,Schofield CJ. Use of mass spectrometry toprobe the nucleophilicity of cysteinylresidues of prolyl hydroxylase domain 2.Anal Biochem. 2009;393(2):215-21.
33. Mecinovic J, Chowdhury R, Lienard BM,Flashman E, Buck MR, Oldham NJ, et al.ESI-MS studies on prolyl hydroxylasedomain 2 reveal a new metal binding site.ChemMedChem. 2008;3(4):569-72.
34. Nytko KJ, Maeda N, Schlafli P, Spielmann P,Wenger RH, Stiehl DP. Vitamin C is dispen-sable for oxygen sensing in vivo. Blood.2011;117(20):5485-93.
35. Bordoli MR, Stiehl DP, Borsig L, KristiansenG, Hausladen S, Schraml P, et al. Prolyl-4-hydroxylase PHD2- and hypoxia-induciblefactor 2-dependent regulation of amphireg-ulin contributes to breast tumorigenesis.Oncogene. 2011;30(5):548-60.
36. Chan DA, Kawahara TL, Sutphin PD,Chang HY, Chi JT, Giaccia AJ. Tumor vascu-lature is regulated by PHD2-mediated angio-genesis and bone marrow-derived cellrecruitment. Cancer Cell. 2009;15(6):527-38.
37. Shao Z, Zhang Y, Powell-Coffman JA. Twodistinct roles for EGL-9 in the regulation ofHIF-1-mediated gene expression inCaenorhabditis elegans. Genetics. 2009;183(3):821-9.
38. Astuti D, Ricketts CJ, Chowdhury R,McDonough MA, Gentle D, Kirby G, et al.Mutation analysis of HIF prolyl hydroxy-lases (PHD/EGLN) in individuals with fea-tures of phaeochromocytoma and renal cellcarcinoma susceptibility. Endocr RelatCancer. 2010;18(1):73-83.