Embed Size (px)
Citation preview

Operationalizing the OR
Supply update: saline solution
Smart inventory management
2018: ISSUE 9
Ideas to improve clinical, financial & operational efficiencies
Medline Account Manager Steve Stankevich with Robyn Hemphill, CEO/director of nursing, Monroe Surgical Hospital
DISTRIBUTION DONE RIGHTHow to avoid supply pitfalls, save money and make better decisions for your ASC
SAVING MONEY WITH CONSIGNMENT Monroe Surgical Hospital

Soon you will be able to get biological indicator readout results for steam in just 24 minutes.*
With biological indicator results in just 24 minutes for both steam* and vaporized hydrogen peroxide sterilization, Every Load Monitoring across sterilization methods is a practical reality.
3M continues to drive improvements that support standardization and consistency across your department, helping you simplify training, reduce workfl ow errors, increase compliance with protocols and support patient safety.
*24-minute results for steam pending 510(k) clearance.
24-minute* results for steam.
Know EVEN Sooner. Know for Sure.
Get the Attest™ Brand Advantage for consistent sterilization monitoring across modalities.
3M and Attest are trademarks for 3M. © 3M 2018. All rights reserved.
Visit go.3M.com/steam to learn about our latest innovations in sterile processing.
*
Know EVEN Sooner.
*

No one said running an ambulatory surgery center was easy. Growing competition, reimbursement pressures and increasing reporting demands are among the many issues keeping you up at night. You can’t do it alone.
In this issue of Outpatient Outcomes, we focus on the important benefits gained by collaborating with a distributor and optimizing supply management. The distributor-ASC relationship should involve more than just delivering the right products. The right distribution partner, who understands your needs, can help you navigate the changing landscape and achieve your goals.
In our cover story “Distribution done right,” you’ll learn how effective distribution will help you avoid common supply pitfalls, save money and make better decisions for your surgery center.
If you’re like many ASCs, your team spends too much time pulling products and setting up cases. In the article “Operationalizing the OR,” discover how Tri-State Surgery Center in Dubuque, Iowa, partnered with Medline to overhaul its supply chain, so that staff gathers only a handful of supplies from one location.
Have you considered partnering with an aggregator to help reduce costs? In “Aggregators versus GPOs,” learn how your distributor can work with an aggregator to get even more aggressive cost savings and additional value-added benefits.
Another innovative way to save money but ensure you don’t run out of crucial supplies is through a supply consignment program.
The article “Saving money with consignment,” shares how Monroe Surgical Hospital in Louisiana uses consignment to maintain a stocked storeroom without tying up money in supply inventory.
Your distributor can also offer great value by finding hard-to-get products. As we learn in “Supply update: saline solution,” a good distributor can work directly with manufacturers, provide the most current information and leverage its supply chains to help get you the products you need, so there’s no disruption to patient care.
As the new senior vice president of Medline’s Ambulatory Surgery Center Division, I’m excited to bring you this latest issue of Outpatient Outcomes. I hope you come away with insights and information useful to you and your staff, and I encourage your continued feedback to make sure we’re meeting your needs. Please feel free to contact us at [email protected] with your ideas, comments and suggestions.
Sincerely,
Zach PocklingtonSenior Vice President,Ambulatory Surgery Center Division Medline Industries, Inc.
welcomeDistributors can be a valued partner to your success
Zach Pocklington
Issue 9 3
Soon you will be able to get biological indicator readout results for steam in just 24 minutes.*
With biological indicator results in just 24 minutes for both steam* and vaporized hydrogen peroxide sterilization, Every Load Monitoring across sterilization methods is a practical reality.
3M continues to drive improvements that support standardization and consistency across your department, helping you simplify training, reduce workfl ow errors, increase compliance with protocols and support patient safety.
*24-minute results for steam pending 510(k) clearance.
24-minute* results for steam.
Know EVEN Sooner. Know for Sure.
Get the Attest™ Brand Advantage for consistent sterilization monitoring across modalities.
3M and Attest are trademarks for 3M. © 3M 2018. All rights reserved.
Visit go.3M.com/steam to learn about our latest innovations in sterile processing.
*
Know EVEN Sooner.
*

8
14
2O
26
30
6
©2018 Medline Industries, Inc. All rights reserved.Medline is a registered trademark of Medline Industries, Inc.
Medline Industries, Inc. Three Lakes Drive
Northfield, IL 600931-800-MEDLINE (1-800-633-5463)
www.medline.com/[email protected]
Published by Convero
835 Sharon Drive, Suite 200 Westlake, OH 44145
(844) 428-8844 www.converoinc.com
Editor: Laura MarzecCopy Editor: Sue OstrowskiArt Director: Stacy Vickroy
Project Manager: Michelle Almenar
7
27

CONTENTSspotlightWelcome letter . . . . . . . . . . . . . . . . . . . . . . . . 3
Briefs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Featured products . . . . . . . . . . . . . . . . . . . . 10
featuresOperationalizing the OR . . . . . . . . . . . . . . 12
Cover story: Distribution done right . . . 14
Saving money with consignment . . . . . . 19
Preventing the spread of drug-resistant bacteria . . . . . . . . . . . . . . . 22
Aggregators versus GPOs . . . . . . . . . . . . . . 24
ASCs react to ruling on total joints . . . . . 26
Supply update: saline solution . . . . . . . . . 28
Smart inventory management . . . . . . . . . 30
24
1310
21
Issue 9 5

briefsSPOTLIGHT
TALK TO USHave a comment on something
you’ve read in Medline’s Outpatient Outcomes
magazine? Have an idea for a story in a future issue?
Please submit comments and suggestions to
6 OUTPATIENT OUTCOMES 2018
Recent mergers bring together insurers and providersThe healthcare industry announced five mega-mergers in December, showing a trend of large insurers seeking to get more involved in delivery of care.
• CVS (known for its pharmacy chain and pharmacy benefit management company, CVS/Caremark) will buy health insur-er Aetna for $69 billion.1
• UnitedHealth Group Inc. will pay $4.9 billion to acquire DaVita Medical Group, including its clinics, urgent care centers and outpatient surgery centers.2
• Health insurer Humana will purchase a 40 percent share in Kindred Healthcare’s home healthcare division, paying $800 million.
The recent surge of M&A activity also included the merger of several prominent healthcare providers.3 On Dec. 7, Dignity Health and Catholic Health Initiatives announced they would combine to create a nonprofit Catholic health system spanning 28 states. In February, federal and Illinois regulators approved the merger of Advocate Health Care and Aurora Health Care, forming the 10th largest nonprofit system.4

CMS 2018 final payment rule: What’s changed?The Centers for Medicare and Medicaid Services (CMS) 2018 final payment rule for ASCs went into effect Jan. 1, 2018.5 Here is a list of the major changes.
• ASC payment increase. CMS increased ASC payment by an average 1.2 percent in CY 2018. It expects total ASC payment to increase by approximately 3 percent for that same period, after accounting for the CPI-U factor increase and enrollment, case-mix and utilization changes.
• Three new ASC covered surgical procedures. CMS approved two certain total disc arthroplasty (artificial disc) procedures and a laparoscopy surgical procedure with total hysterectomy for the ASC covered procedures list in 2018.
• Ambulatory Surgical Center Quality Reporting (ASCQR) program updates. CMS will remove three measures from the 2019 payment determination, including (1) ASC-5: Prophylactic Intravenous (IV) Antibiotic Timing; (2) ASC-6: Safe Surgery Checklist Use; and (3) ASC-7: Ambulatory Surgical Center Facility Volume Data on Selected Ambulatory Surgical Center Surgical Procedures. In addition, ASCs will need to begin collecting data on two new measures beginning in 2018: (1) ASC-13: Normothermia Outcome and (2) ASC-14: Unplanned Anterior Vitrectomy.6
For 2022 payment determination, CMS also approved two new measures collected through claims: (1) ASC-17: Hospital Visits after Orthopedic Ambulatory Surgical Center Procedures and (2) ASC-18: Hospital Visits after Urology Ambulatory Surgical Center Procedures.
REFERENCES1. CVS Health to acquire Aetna for $69 billion in year’s largest acquisition. www.reuters.com/article/us-aetna-m-a-cvs-health/cvs-health-to-acquire-aetna-for-69-billion-in-years-largest-acquisition-idUSKBN1DX0NC.2. Humana Vows To ‘Modernize’ Home Care With Kindred Stake. www.forbes.com/sites/brucejapsen/2017/12/19/huma-na-wants-to-modernize-home-care-with-stake-in-4b-kindred-deal/#466b3f582710.3. Healthcare mega-mergers dominate 2017. www.modernhealthcare.com/article/20171226/NEWS/171229957.4. Federal, Illinois regulators approve Advocate-Aurora merger. www.modernhealthcare.com/article/20180215/NEWS/180219942. 5. CMS Releases 2018 OPPS/ASC Payment Systems Final Rule. www.healthlawdiagnosis.com/2017/11/cms-releases-2018-oppsasc-payment-systems-final-rule. 6. Quality Reporting. www.ascassociation.org/federalregulations/qualityreporting.7. What is CAIP? www.aboutcaip.org/about-caip/what-is-caip.
New certification designed for ASC infection preventionistsThe Board of Ambulatory Surgery Certification (BASC) has announced a new certification program for infection preventionists in the ASC industry.7
The Certified Ambulatory Infection Preventionist™ (CAIP™) credential is the first certification designed for infection preventionists who work in ASCs. Achieving CAIP certification demonstrates the infection preventionist’s leadership in ambulatory surgery infection prevention standards and best practices, as well as a dedication to personal development. To learn more, visit www.aboutcaip.org.
Issue 9 7

SPOTLIGHT
events
MAY 2018
AST SURGICAL TECHNOLOGY CONFERENCEMay 31-June 2Walt Disney World Swan and Dolphin ResortOrlando, FloridaThis Association of Surgical Technologist’s conference is the number one surgical technology and surgical assisting trade show in the country. Attendees participate in education led by nationally distinguished surgeons. For more information, visit www.ast.org/AboutUs/Conference.
JUNE 2018
BECKER’S 16TH ANNUAL FUTURE OF SPINE + THE SPINE, ORTHOPEDIC AND PAIN MANAGEMENT-DRIVEN ASC CONFERENCEJune 14-16Swissotel ChicagoChicago, IllinoisLearn the latest best practices and trends in spine, orthopedic and pain management at this annual ASC-fo-cused event. For more information, visit www.beckersasc.com/ conferences-and-events.html.
TASCA FALL CONFERENCE & TRADE SHOWSept. 14-15Park Vista DoubleTreeGatlinburg, TennesseeThe Tennessee Ambulatory Surgery Center Association’s annual conference is a chance to network with ASC profession-als, healthcare experts and exhibitors while learning about industry trends, regulations and strategies to help your ASC excel. For more information, visit www.tnasca.org.
OCTOBER 2018
BECKER’S ASC 25TH ANNUAL MEETING: THE BUSINESS AND OPERATIONS OF ASCSOct. 18-20Swissotel ChicagoChicago, IllinoisJoin ASC owners, surgeons and adminis-trators as they discuss changing business and legal issues impacting outpatient surgery centers. You’ll come away with ideas to manage challenging clinical, business and financial issues and improve your ASC. For more information, visit www.beckersasc.com/confer-ences-and-events.html.
If you would like to have your event listed here, please send an email to [email protected].
AASCA ANNUAL CONFERENCEJune 28-29JW Marriott Camelback Inn & SpaScottsdale, ArizonaJoin other ASC professionals at this annual event of the Arizona Ambulatory Surgery Center Association. The conference includes two days of educational seminars focused on the latest practices and standards of care. For more information, visit www.arizonaasc.org/conference/ 2017-conference-exhibit-information.
JULY 2018
FSASC ANNUAL CONFERENCE & TRADE SHOWJuly 18-20Hyatt Regency Grand CypressOrlando, FloridaNetwork with ASC professionals, industry experts and vendors at the Florida Society of Ambulatory Surgical Centers’ annual conference. With diverse topics ranging from clinical to manage-ment to business, the event provides something for everyone. For more information, visit www.fsasc.org.
SEPTEMBER 2018
OASCA ANNUAL CONFERENCE & TRADE SHOWSept. 12-13Erb Memorial Union at The University of OregonEugene, OregonAttend roundtable discussions and breakout sessions, and interact with vendors, at this annual event hosted by the Oregon Ambulatory Surgery Center Association. For more information, visit www.ascoregon.org.
8 OUTPATIENT OUTCOMES 2018

Dermabond Advanced
Celebrating 20 years of expertise in skin closure for excellent outcomes.
StrengthensWhen used in addition to sutures, DERMABOND ADVANCED® Topical Skin Adhesive was shown ex vivo to add 75% more strength to the wound closure than sutures alone.1
Inhibits bacteriaDemonstrated in vitro inhibition of gram-positive bacteria (MRSA and MRSE) and gram-negative bacteria (E coli).2*
Provides a microbial barrierProvides a flexible microbial barrier with 99% protection in vitro for 72 hours against organisms commonly responsible for surgical site infections.2†
For more information, contact your representative or call 1-877-ETHICON.
1. Protocol to determine the strength benefits when adding DERMABOND ADVANCED™ Topical Skin Adhesive to a wound or incision using suture as the primary closure, July 2012.
2. Bhende S, Rothenburger S, Spangler DJ, Dito M. In vitro assessment of microbial barrier properties of DERMABOND® Topical Skin Adhesive. Surg Infect (Larchmt). 2002;3(3):251-257.2002;3(3):251-257.
© 2018 Ethicon US, LLC. 029680-180214
*Clinical significance is unknown. †Staphylococcus epidermidis, Staphylococcus aureus, Escherichia coli, Enterococcus faecium, Pseudomonas aeruginosa.
For complete indications, contraindications, warnings, precautions, and adverse reactions, please reference full package insert.
S:7.875”S
:10
.37
5”
T:8.375”T:1
0.8
75
”
B:8.625”B
:11
.12
5”

SPOTLIGHT
PICO™ single-use negative pressure wound therapy
“I use this on every patient.”
It’s a phrase that Smith & Nephew, the makers of PICO single-use negative pressure wound therapy (NPWT) product, hears from surgeons frequently — especially those serving patients in the outpatient surgery space.
A recent meta-analysis published on PICO’s use on closed surgical
10 OUTPATIENT OUTCOMES 2018
incisions across multiple specialties demonstrated significant reductions in surgical site infections (58 percent) and dehiscence (26 percent).1 Other studies have reported reductions in surgical site complications and hematoma and seroma formations.2 In addition to positive clinical outcomes, PICO has also demonstrated high patient satisfaction levels (97 percent).3
PICO’s unique mode of action makes it a great fit for the management of both closed surgical incisions and open wounds. The system manages wound fluid through both evaporation and absorption, with a single kit providing up to seven days of therapy. Additionally, for procedures where reducing edema is important post-operatively, PICO expands NPWT benefits beyond the incision site only by providing compression to the periwound area — a mechanism that may help reduce edema and improve perfusion.4
Now, with the launch of a new PICO innovation — Multisite with Soft Port technology — PICO is raising the bar even further. This newest shape, paired with a newly designed Soft Port, conforms to joints and curves with ease, while the Soft Port technology reduces the risk of pressure points during therapy.5
Is there an existing product that has worked great for your facility? We want to hear from you. Send us your story at [email protected].
Share your experience.
REFERENCES
1. Meta-analysis of comparative trials evaluating a prophylactic single-use negative pressure wound therapy system for the prevention of surgical site complications. Surgical Infections. Vol 18 No. 00 (2017). 2. Incisional negative pressure wound therapy dressings (iNPWTd) in routine primary hip and knee arthroplasties. Bone Joint Res 2016;5:328–337. 3. Evaluating the costs and benefits of innovations in chronic wound care products and practices. Ostomy Wound Management. June 2013. 4. World Union of Wound Healing Societies (WUWHS) Consensus Document. Closed Surgical Incision Management: Understanding the Role of NPWT. Wounds International. 5. Palmer S. Smith & nephew data on file 42. Volunteer Trial to Assess Dressing Performance of PICO Multisite vs Control. April 2014.
With PICO, patients can be sent home with confidence that their incisions are protected. They are on the path to the best possible recovery.
The importance of positive patient outcomes — and a positive patient experience — can’t be overstated. We encourage you to ask Medline about enhancing your facility through PICO use. To learn more, visit www.possiblewithpico.com or www.medline.com/asc.
featured products

Issue 9 11
QuickSuite® turnover kits
Time in the operating room is invaluable. With the growth in today’s surgery centers, and the continuing pattern of ASCs taking on more complex procedures, the days of “7-to-10-minute turnover time” are becoming less and less the norm. Multiple studies value every minute in the operating room at $60-$100, so it is crucial that ASCs are looking into all possible ideas to improve operational efficiency.
Customized kits for your ASC
Are your nurses and techs spending their mornings pulling specific linen components for the coming day? Or running through OR hallways between cases to ensure all items are collected? Whether it is room setup, takedown or both that is slowing your team down, QuickSuite turnover kits can help.
With QuickSuite, Medline will kit your linens, so your nurses and techs can allocate their valuable time to more important needs. Our extensive team of dedicated ASC sales and product specialists will assess current turnover practices, determine areas of improvement, develop a cost analysis and savings plan, and build a customized turnover kit tailored exactly to your facility’s needs.
Goals of QuickSuite
• Boost efficiency - From the loading dock to the OR halls, have everything in one place tailored to your center’s needs.
• Promote safety - Increase the standard of care through the adoption of single-use disposables.
• Contain costs - Eliminate wasted linen, protect expensive capital equipment and increase annual procedure count.
Not sure what you need? To facilitate an easy transition from reusable linens, we have two ASC Stocked Turnover Kits. These kits are perfect to start the conversation and create the perfect custom kit for your surgery center.
Since 2014, more and more surgery centers have seen the positive impact QuickSuite can provide. Get your trial up and running today.
To learn more or to discuss a customized turnover kit for your facility, contact your Medline ASC representative or email [email protected].
Pictured: DYKQSUITEASC
*Data on file
ASC Complete Turnover Kits

FEATURE
Tri-State Surgery Center in Dubuque, Iowa, is marking one year after launching a major quality initiative to overhaul its supply chain logistics and maximize staff productivity.
A year ago, Susan Gourley, director of nursing for Tri-State, spoke with other surgery centers about the center’s processes, confirming her belief that Tri-State was spending significantly more time setting up cases and handling supplies than comparable facilities.
“Being on two floors, we’d run up and down the steps to get the supplies we needed for our cases, which takes a lot of time,” Gourley explains.
Distributor analysisTo further improve Tri-State’s supply handling and case set up, Gourley and her staff asked Medline to evaluate the surgery center’s supply chain logistics and make recommendations.
12 OUTPATIENT OUTCOMES 2018
Medline brought in its perioperative logistics and clinical experts to observe Tri-State’s staff and conduct a thorough review of the center’s inventory management procedures, including case set up, pulling products, ordering, sterilization, preference cards, storeroom layout, case turnover time and overall costs.
The analysis uncovered some very powerful data and observations. • Tri-State conducts approximately
4,800 surgeries each year with an annual supply budget of $2,033,600.
• Each case requires nine steps, seven of which involve handling individual supplies.
• There are approximately 82,212 individual components used each year from all cases.
• Annually, the staff produces approximately 575,484 touchpoints (82,212 times seven steps).
OPERATIONALIZING THE OR
Tri-State Surgery Center
saves time and cost by
partnering with a distributor
for a complete supply solution
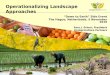
Element Measured Before CDS After CDSAnnual total components 82,212 3,768No. of steps per case handling components
7 7
Annual staff touch points (total components x 7 steps)
575,484 26,376
Estimated annual staff hours handing products (touch points x 13 seconds per item)
2,078 hours 95 hours
Fig. 1: Supply management results
“The bottom line is that our staff is now
spending less time gathering products for cases. This gives them
more time to spend with their patients.”
– Susan Gourley, director of nursing, Tri-State Surgery Center

FEATURE
Issue 9 13
• The number of touchpoints equates to an estimated 2,078 staff hours (575,484 times 13 seconds). In addition, Medline identified
several key areas of improvement, which included: • Reducing the excess number of
supplies being sterilized, including towels, light handles and basins
• Reducing the number of individual products being ordered and stored
• Addressing inaccurate gown mix, including many different gown types with varying levels of protection
• Reducing staff time spent case picking and restocking unused supplies.
A customized solution Medline recommended streamlining Tri-State’s supply management process with a customized solution. That solution involved transitioning the surgery center to its Complete Delivery System (CDS), redesigning the store room and reducing product costs.
CDS, Medline’s exclusive supply management solution for high-volume cases, places all disposable perioperative supplies in one convenient container.
“With the CDS, we no longer have to pull individual packs and countless items for each case,” Gourley says. “The time savings is substantial, both on the front end — having to pull fewer supplies — and on the back end, not having to restock items.”
Gourley cited a podiatry case in which the staff needed to pull between 20-25 individual items to set up the case. With CDS, the staff can pull just one container and about three additional items.
Tri-State also has the flexibility to include products of its own choosing, explains Mollie Fagan, surgical tech and
materials manager for Tri-State. “In each CDS, we converted about
a quarter of the products to the Medline brand, and for many physician preference items, we could stay with the national brands,” Fagan says.
Fagan notes that, along with acquisition savings on Medline-branded items, Tri-State saved money by eliminating distribution fees on Medline products because Medline is a manufacturer-distributor. On non-Medline products, Medline provided contract pricing accessed through Tri-State’s GPO for additional savings.
In all, Tri-State converted 11 cases to CDS modules along with two endo packs, which impacted approximately 3,768 surgical procedures, or 75 percent of its total surgical volume.
Seeing resultsConverting to CDS has helped Tri-State’s staff significantly improve efficiency and reduce handling times. [See Fig. 1]
“The bottom line is that our staff is now spending less time gathering products for cases,” Gourley says. “This gives them more time to spend with their patients and makes their jobs much more enjoyable and satisfying.”
In addition, Medline’s logistical experts reviewed Tri-State’s supply storage space to see how it could be maximized given the conversion to the CDS modules and the reduction of individual supplies.
“The new schematic [See Fig. 2] was tailored to our new supply environment of larger boxes and fewer individual items,” Gourley says. “We’ve eliminated many of the individual items we used to order and stock, which has reduced our investment in these products and saved us considerable ordering time and space.”
Gourley also credits CDS with reducing sterilization time at the surgery center. Many items her staff had to sterilize, such as light covers and towels, are now included as disposable supplies in the CDS.
Gourley estimates that Tri-State is saving nearly $20,000 per year with Medline and its CDS program, though she says the benefits go way beyond cost savings. The surgery center has experienced vastly greater efficiency in case set up, and when handling products and stocking items.
“Our staff would not be happy if we went back to the old way of doing things,” Gourley says.
Fig. 2: Improving storeroom space
and logistics

14 OUTPATIENT OUTCOMES 2018
COVER STORY

Issue 9 15
Distribution
Patient care and quality outcomes are top priorities at any surgery center, but ASCs still have a bottom line. Learning the ins and outs of medical supply distribution — and how your distributor can support your needs — can help your center achieve lasting savings and efficiencies that go straight to that bottom line.
3 common supply chain mistakes “Surgery centers are businesses that are often run by clinicians. The same clinicians hired to focus on patient care,” says Zach Pocklington, senior vice president of sales in the Ambulatory Surgery Center Division at Medline. Supply issues such as case costing and inventory manage-ment can be put on the back burner to maintain a focus on patient outcomes.
As a result, surgery centers share some common pitfalls in their supply chain operations. The first step to avoiding those mistakes is recognizing them.
Effective distribution will help you avoid common supply pitfalls, save money and make better decisions for your surgery center. Here’s what you need to know.
DONE RIGHT

16 OUTPATIENT OUTCOMES 2018
1. Not knowing your case costs. How much does it cost to perform cases across the different specialties in a center? Many surgery center leaders do not have an exact answer to this question, which means their supply-ordering strategies are not tailored to fit their centers.
Benchmarking can be a great place to start when it comes to determining the supply element of your case cost. Here are some helpful supply cost metrics, broken down by specialty, according to Avanza Healthcare Strategies.1• ENT. High: $400; Low: $300• Gastroenterology. High: $200; Low:
$85• General surgery. High: 500; Low:
$350• Gynecology. High: $525; Low: $300• Ophthalmology. High: $750;
Low: $400• Orthopedics. High: $800; Low: $600• Pain Management. High: $100;
Low: $50• Urology. High: $300; Low: $200
Knowing your average case costs
and the supply cost component means you can order exactly what you need, when you need it. You won’t order excess products that might go to waste or take up unnecessary space.
2. Inefficient ordering. Surgery centers are often run by small, very talented teams. This means everyone must wear different hats, and many people have one foot in the business sphere and the other in the clinical sphere. When this happens, the most important part of ordering supplies becomes simply ordering what you need as soon as you realize you need it.
and review your contracts with you, take advantage of that. Keep the lines of communication open and cultivate a strong relationship with your rep.
“Be collaborative with your rep, and they will fight for your center,” says Greg Hylton, vice president of vendor relations at Medline. “Reps have a lot more opportunity to help ASCs if the relationship is more than simply transactional.”
Distribution FAQsMedical supply distribution can be a mystery. Contracts are complex and prices change. ASC leaders can be left feeling confused and frustrated. Instead of remaining in the dark, use the resources at your disposal (like your rep) to get answers to some of your most burning questions.
How do my contracts work? Your contracts determine your supply costs and often where you get your supplies. So, it’s important to understand how
This strategy seems effective — you order supplies as the need arises instead of putting it off for later. Yet, this inefficient method leaves a lot of savings on the table and takes up more time than necessary. Surgery centers that take an ‘as-needed’ approach to ordering will find they are sending out multiple purchase orders each week, and they might not even know if they are ordering supplies included in their existing contracts. “The understanding of contract costs and how that connects to the goods you order often gets lost,” Pocklington explains. “Plus, every time an order is placed you are potentially taking someone away from their clinical job.”
Rather than placing orders on demand, surgery centers can be more strategic about their ordering. Review your contracts and your current orders. Is everything you order on contract? If not, could you switch to something that is on contract or talk to your rep about getting the supply you need on a contract?
“Make sure you are getting the correct price,” Pocklington advises.
Once you know your costs, take time to organize your ordering process. Ordering supplies once per week is more efficient than ordering on an as-needed basis. Work with your team to balance communication on supply needs and timing.
3. Not making use of your distributor relationship. Distributors have a vast amount of resources at their disposal, and those resources can be invaluable for ASCs. If your rep offers to sit down
“When empowered, reps can do a lot for a
surgery center. They can advocate for the center
and find better contracts for them to access.”
– Greg Hylton, vice president of vendor relations, Medline Industries, Inc.
COVER STORY

Issue 9 17
those costs are set. A surgery center’s group
purchasing organization (GPO) will do all the bidding and contracting for the thousands of facilities in that group. Medical manufacturers will compete with one another to offer the best price.
Typically, the best offer will land the contract. The distributor then purchases the product at list price and ships it to their contracted facilities at the contracted price. If an ASC is buying a product off-contract, the distributor will likely sell it at list price with a markup.
“Your distributor has visibility to GPO pricing,” Pocklington says. “They can run a report in 30 seconds. Every distributor should have regular conversations with their customers about the contracts they are accessing — and those they aren’t.”
Why did a price change on my contract? It can be frustrating to see a price change on your contract. It is important to know though that manufacturers set the price, not distributors. Distributors are simply accessing the contracted prices. Your distributor might have some awareness about those price changes, and owns any technical issues with getting an appropriate contract connected. However, your manufacturer rep should explain the decision. Ask your distributor rep to facilitate such an important conversation when looking into these issues.
How can I make ordering as easy as possible? For ordering to be an efficient, streamlined process, it should work for your center. Many distributors offer different ways to place orders: EDI, web-based platforms, over the phone or via fax. What would the
THE VALUE OF A MANUFACTURER-DISTRIBUTOR
Medline not only manufactures its own products, many of which are made specifically for ASCs. It also has partnerships with other major manufacturing companies. This gives ASC customers access to a robust portfolio of products.
“Our partnerships with other national brands in the market help us serve our ASC customers, whether the product has Medline on the box or not,” says Greg Hylton, vice president of vendor relations at Medline.
As a manufacturer-distributor, Medline can get ASCs the products they need, while managing costs.
“We can control costs on 60 to 70 percent of what we sell our customers,” explains Zach Pocklington, senior vice president of sales in the Ambulatory Surgery Center Division at Medline. “We also have contracts and a rebate team that make sure we are connecting the right products at the right tiers, which drives down costs.”
Medline’s ASC sales reps educate customers to help them make the right supply decisions. All Medline reps are specialized to the surgery center market and trained to identify solutions that are the best fit for each customer.
WE CAN CONTROL COSTS ON 60 TO 70 PERCENT OF WHAT WE SELL OUR CUSTOMERS.

18 OUTPATIENT OUTCOMES 2018
person in charge of ordering at your ASC be most comfortable with and prefer? Your rep can explain your options.
How often do you want supply shipments? Where should those shipments go? You can answer those questions for your rep to make the process work best for your center.
How else can your distributor help?Distributors have a lot of strategic value to offer ASCs. Learn how to put your rep to work for you.
Dedicated resources. Distributors have vast resources at their disposal, and those resources can be put to work on behalf of ASCs. Be proactive and ask your medical distributor what resources they bring to bear. Many even have solutions tailored specifically for the surgery center market. Often those solutions can be customized to fit your center’s needs.
Additionally, strong distributors are constantly looking for ways to improve, which translates to more resources for the customer. “If I were an ASC customer, I would be interested to know which distributors are investing in their own infrastructure,” Hylton says. Is the distributor adding more warehouses? Is the company looking for new technologies to support greater efficiency? Distributors that can answer “yes” to those questions can support your needs in the present and down the road.
Empowered sales reps. While distributors have a lot to offer their surgery center customers, it is important that ASC leaders know how to access those resources. The gateway to a strong relationship with any distributor is through your designated sales rep. If you want to know what your distributor can do for you, trust and empower your reps to
do their job. “When empowered, reps
can do a lot for a surgery center,” Hylton says. “They can advocate for the center and find better contracts for them to access.” Reps who know a surgery center customer values their relationship will go the extra mile to ensure that the distributor is doing everything it can to meet the center’s supply needs, improve
efficiencies and drive down costs, Pocklington notes. They
are in it for the long term.Insight into your center’s
needs. Knowing your needs is a big part of putting your rep and your
distributor to work for you. “Reps ask administrators questions so they can understand the surgery center better,” Pocklington says. “Then they can provide the solutions that are most meaningful to that customer.”
Your distribution rep will want to know how big your case load is, how you place your orders, when you want to receive deliveries, how often you want to see a rep and what GPO you use. Administrators can do a lot for their centers by having that information readily available for reps.
Armed with this information, your rep will know how to guide your ASC toward a more efficient supply chain — whether that’s by helping you set appropriate inventory levels or implement a more efficient ordering system.
Transparency. Medical distribution can be confusing and time-consuming for ASC leaders who already have their plates full with staffing issues, physician privileging, quality control and patient care. Reps can step in and be a helpful resource. They can explain how contracts work, why a price has changed and what your ASC could do differently to achieve greater supply chain efficiency.
Distribution and how it affects your ASC’s supply chain does not have to be a mystery. Talk to your rep, create a valuable relationship and use the resources you have at your disposal to reap the many benefits of effective distribution.
REFERENCES
1. Avanza Healthcare Strategies. Ambulatory Surgery Center Special Report: 2017 Benchmarks. www.avanzastrategies.com/wp-content/uploads/2014/05/Avanza_ASC_Benchmarks_2017.pdf.
– Josh C
“Every time an order is placed you are
potentially taking someone away from
their clinical job.”– Zach Pocklington, senior vice president
of sales, Ambulatory Surgery Center Division, Medline Industries, Inc.
COVER STORY

Issue 9 19
Hospitals and ambulatory surgery centers have ordered on consign-ment for decades. Now, as healthcare providers face increased pressure to control costs, ASCs are reexamining consignment’s potential to streamline supply ordering and control costs.
What is consignment?With more patients moving to outpatient facilities, lean-operating, fast-moving ASCs must stay on top of inventory management more than ever. Many facilities choose some combination of outright ownership, bulk and just-in-time purchasing and consignment.
Under a consignment purchasing agreement, facilities order what they need for a defined time period, such as one month or quarter. The sup-plier provides the products, and bills for those products as your ASC uses them. Consignment ordering allows you to stock supplies needed for both expected and emergency cases while reducing up-front expenses.
Healthcare providers can also tai-lor their orders based on need — an advantage to surgery centers, which need a lower volume of supplies than a hospital, and may have less predictable schedules.1 Under some consignment agreements, your ASC
can order less of a particular product than it would if you purchased the product outright, which not only saves money, but also valuable storage space.
ASCs may order some or all of their products on consign-ment as a way to free up availa-ble funds. They may also benefit from lower overall supply costs, explains Medline Account Manager Steve Stankevich.
“The customers I’ve worked with saved money, based off the purchase value of all the items in a given time period compared to what we billed out,” Stankevich says. “There’s always a savings.”
Saving money — and spaceRobyn Hemphill, CEO/director of nursing for Monroe Surgical Hospital in Monroe, Louisiana, says her facility saved about $9,000 in supply costs in one year by moving a portion of its supplies to consignment. The 10-bed facility, which serves North Louisiana, Mississippi and Southern Arkansas, also benefitted from about $2,000 in product rebates.
Consignment shifts some of the inventory management from the ASC to the supplier, which also eases the burden on busy staff. For example,
at the end of each month — or the surgery center’s preferred billing period — a Medline account manager works with the ASC to count what’s left on shelves.
“We’ll do that with each and every item an ASC has in the consignment program,” Stankevich says.Making it work for your centerWhen incorporating consignment into a supply-ordering strategy, Stankevich recommends ASCs set up
Saving money with consignment
“We have to keep a tight inventory.
For a small surgical facility, consignment
is a win-win.”– Robyn Hemphill, CEO/director of nursing, Monroe Surgical Hospital
ASCs turn to consignment to control costs and optimize cash flow
FEATURE
PHO
TOS
BY S
UH
AN
AN
D D
ALE
WA
LLAC
E

par levels — a minimum quantity that it must always keep in stock — for inventory supplies. They can then re-place products based on those levels.
ASCs should also set up a system to help staff identify which items are and are not on consignment. “This makes it easier for staff to know which items not to count when they do their inventory reports,” Stankevich explains. “They wouldn’t count consignment items, because the product doesn’t belong to a center until it’s billed out.”
When reviewing a consignment agreement, pay attention to product pricing. Some suppliers try to mark up product prices, incorporate addi-tional fees or offer smaller discounts off the list price to cover inventory management expenses.2
An industry-leading supplier will offer the same prices, whether a customer orders by consignment or by traditional methods. However, products can’t sit on the shelf forever. Your ASC will likely be billed for any products not used after six months. This means Materials staff should
not completely ignore consignment inventory.
Other questions to ask your supplier include:• How do you handle lost, damaged
or expired items?• How involved are you in inventory
management?• How will you work with my ASC
to optimize inventory levels and improve efficiency?With proper planning and close
communication with suppliers, ASCs can realize cost and operational bene-fits from consignment purchasing.
“Most hospitals our size have to keep a tight inventory,” Hemphill says. “They get their inventory in, and it’s immediately dispersed to the depart-ments. For a small surgical hospital, consignment is a win-win.”
REFERENCES
1. Buying in bulk, just in time purchasing, consignment: Which supply-ordering pattern is right for your ASC? Sept. 12, 2014. Accessed March 1, 2018. www.beckersasc.com/asc-supply-chain-materials-management/buying-in-bulk-just-in-time-purchasing-consignment-which-supply-ordering-pattern-is-right-for-your-asc.html.
2. When Consignment is a Crutch. Becker’s Hospital Review. June 5, 2014. Accessed March 1, 2018. www.beckershospitalreview.com/hospital-management-administration/when-consignment-is-a-crutch.html.
20 OUTPATIENT OUTCOMES 2018
FEATURE

Issue 9 21
PARTNERING TO STREAMLINE OPERATIONSMonroe Surgical Hospital in Monroe, Louisiana, uses Medline’s Complete Delivery System (CDS) program for its disposable perioperative supplies and other items not contained in surgical packs. Medline packs these supplies in containers, and Monroe Surgical sends them to various departments. Surgery, endoscopy, orthopedics and gynecological services departments each receive their own containers. The hospital consigns all items that fall under the CDS program.
Using a combination of container storage and consignment ordering has helped Monroe Surgical cut costs and save space. Medline Account Manager
Steve Stankevich with Robyn Hemphill, CEO/director of nursing,
Monroe Surgical Hospital
PHO
TOS
BY S
UH
AN
AN
D D
ALE
WA
LLAC
E

22 OUTPATIENT OUTCOMES 2018
FEATURE
PREVENTING THE SPREAD OF
In 2014, one surgery center was cited for infection control lapses following an investigation by its state health department. The fear was that 1,100 patients may have been exposed to Hepatitis B, Hepatitis C and HIV. Thankfully, no one contracted any of these infectious diseases.1,2 However, imagine the consequences if any of the patients had contracted hepatitis or HIV. It’s a scary thought for any healthcare professional.
That surgery center is not alone. According to a Centers for Disease Control and Prevention (CDC) report published in 2010, lapses in infection control are common among U.S. ambulatory surgery centers (ASCs). In fact, two-thirds of ASCs in the study had at least one lapse in infection control. Common
errors included: using single-dose medication vials for more than one patient (28.1 percent), failing to adhere to recommended practices regarding equipment reprocessing (28.4 percent), and lapses in
handling of blood glucose monitoring
equipment (46.3 percent).3 During 2001
through 2011 there were up to 18 outbreaks of viral hepatitis associated with unsafe injection practices in outpatient settings, including ASCs.4
A recent study of outpatient facilities in Los Angeles County revealed that ASCs were common settings for infection outbreaks. Some of the most common infection control breaches were associated with injection safety, equipment processing and sterilization, and environmental cleaning. Injection safety violations included reuse of single-dose medications and not using aseptic technique to enter multidose vials.4
And then there are the infections that don’t make the news. An estimated 2,049,442 Americans get sick and 23,000 die of infections caused by antibiotic-resistant bacteria — i.e., methicillin-resistant Staphylococcus aureus (MRSA). These insidious invaders are concentrated in healthcare facilities — including surgery centers.5 Operating rooms are another high-risk area for infection, especially surgical site infections.
Infection control measuresNo one asked these deadly bugs to come around, but the good news is you can help decrease their spread by adapting new behaviors. Here are some recommendations from the CDC for how you can limit the effects of drug-resistant bacteria in your ASC: • Do everything you can to prevent the spread
of infection. Drug-resistant bacteria spreads from person to person, from food animals
How to avoid infection control lapses at your ASC
DRUG-RESISTANT BACTERIA
An estimated 2,049,442 Americans get sick and 23,000
die of infections caused by antibiotic-resistant bacteria.
One improperly cleaned scope or instrument can lead to a host
of infection control issues.

Issue 9 23
to people, and from objects in the environment to people.
• Discuss antibiotic use with your physicians. Although antibiotics can be lifesaving, they are not optimally prescribed in up to 50 percent of cases.5 Stopping even some unnecessary use of antibiotics can help slow the spread of resistant bacteria.
• Track your infection rates. Data analysis informs process improvements by helping you revise your practices to attain the best outcomes.
Working with your distributorYour medical supply distributor can also help you improve infection control at your surgery center. Partner with them to explore:• New ways to increase hand
hygiene awareness and compliance. Excellent hand hygiene is one of the cornerstones to helping stop infection in its tracks. To encourage your staff to maintain hand hygiene compliance, ask about alcohol-based hand sanitizer with emollients to soothe dry hands. Educational materials, in the form of hand hygiene awareness posters and online courses, are also available from vendors, saving you the time it takes to develop your own.
• Optimal environmental cleaning methods and innovative products. Manufacturers are always developing more advanced cleaning fluids and accessories to remove bacteria from hard surfaces. Ask your distributor to introduce you to these products and show you how to use them most effectively.
• Best practices in device and instrument sterilization and reprocessing. One improperly cleaned scope or instrument can lead to a host of infection control
issues. Though the manufacturer defines the proper cleaning and reprocessing protocols, your distributor can be another set of eyes to help you identify lapses in your sterilization process and to recommend best practices. If you are concerned about meeting guidelines for sterilization procedures, you might also consider outsourcing your reprocessing.
1. Tracking Infections in Ambulatory Surgery Centers Visit: www.cdc.gov/nhsn/ambulatory-surgery/index.html
2. Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care
Visit: www.cdc.gov/hai/settings/outpatient/outpatient-care-guidelines.html
3. Oregon Ambulatory Surgery Center Infection Prevention & Control Toolkit
Visit: www.oregonpatientsafety.org/resource-center/opsc-resources/oregon-ambulatory-surgery-center-infection-prevention-control-toolkit/436
4. Continuing Education in Sterile Processing Visit: www.medlineuniversity.com/lms/
search?query=sterile%20processing
5. Best Practices for Removing Bioburden Visit: mkt.medline.com/advancing-blog/best-practices-
for-removing-bioburden-in-busy-operating-rooms
5 ONLINE RESOURCES TO HELP YOU FIGHT INFECTION
REFERENCES
1. Centers for Disease Control and Prevention. Outbreaks and Patient Notifications in Outpatient Settings, Selected Examples, 2010-2014. www.cdc.gov/hai/settings/outpatient/outbreaks-patient-notifications.html.
2. York County surgical center notifies patients of possible Hepatitis & HIV risk. fox43.com/2014/05/30/surgical-center-notifies-patients-of-possible-hepatitis-hiv-risk.
3. Centers for Disease Control and Prevention. Infection Control Assessment of Ambulatory Surgery Centers. www.cdc.gov/injectionsafety/pubs-ic-assessment-ambulatory-surgical-centers.html.
4. Health care-associated infection outbreak investigations in outpatient settings, Los Angeles County, California, USA, 2000−2012. Emerging Infectious Diseases. 2015;21(8):1317-1321. wwwnc.cdc.gov/eid/article/21/8/14-1251_article.
5. Centers for Disease Control and Prevention. Antibiotic/Antimicrobial Resistance. www.cdc.gov/drugresistance/about.html.

Shrinking reimbursements, increased competition and tight margins mean ambulatory surgical centers must continually look for ways to increase revenue and decrease costs. Medical and surgical supplies average nearly 22 percent of an ASC’s operating expense.1
One way to lower medical supply costs is by working with a group purchasing organization (GPO) to negotiate with manufacturers and obtain better pricing. Most ASCs currently work with a GPO, says Medline’s Nile Whitney, vice president of corporate accounts, Ambulatory Surgery Center Division. However, if you want to get even more aggressive cost savings — and additional, value-added benefits — your ASC may want to consider partnering with an aggregator through your supply distributor.
Aggregators versus GPOsHave you considered partnering with an aggregator? If not, here are five reasons to explore your options.
FEATURE
24 OUTPATIENT OUTCOMES 2018
How aggregation works“Aggregators pool purchasing to get better tier pricing [a price per unit within a range],” Whitney explains.
The more customers an aggregator has, the better it’s purchasing power. A good aggregator can take customers from tier one (the highest costs) to tier four or, sometimes, even tier five. Increasing your surgery center’s tier pricing for sutures and other high-use items can add up to significant cost savings.
“Aggregators are constantly trying to grow their membership to increase their tiers to make themselves more attractive to future partners,” Whitney says. When you join an aggregation group, you’ll still be a part of your GPO, but the aggregation group will help drive up your tiers.
What are the advantages of using an aggregator?
Cost savings. “While a GPO uses its purchasing power to drive down costs, an aggregator takes that to another level, and does it in a way so that free-standing, physician-owned surgery centers can almost purchase near the level of large organizations,” Whitney says. “The aggregator helps protect the margins and financial health of smaller, independent surgical centers.”
Accurate contract connections. Aggregators are committed to capturing data that helps them negotiate with manufacturers to get higher tier pricing. Because of this laser focus on the details, they stay on top of ever-changing contract dates.
A missed contract connection means you

don’t get the lower negotiated prices until someone catches the mistake. Over time, your ASC incurs additional, and unexpected, supply costs.
“Aggregators need these contract connections to track spending to go back to the manufacturer and negotiate new tiers. So they are all over it,” Whitney says. “When you work with an aggregator, you’re putting yourself at better odds of not missing contract connections and ensuring you have the most accurate contract connection possible.”
Ongoing value analysis. In addition to conducting an initial cost study, aggregators will periodically review your spending to see how your cost savings compared with predicted savings. Even if you increased your usage of a product, driving up your
Issue 9 25
overall costs, the aggregator can extrapolate the increased quantity and show you how much you saved on the additional volume. “That’s a big value-added service,” Whitney notes.
Product standardization. Using cost-effective, alternative medical supplies that offer as good as (or better) outcomes can further compound your cost savings. Whitney says Medline is extremely sensitive to physicians’ loyalty to certain products, so when they are working with an aggregator on an ASC’s behalf, they will pursue product savings opportunities when physicians feel comfortable exploring alternatives and respect those where brand loyalty trumps costs.
REFERENCES1. VMG Health. www.vmghealth.com/Downloads/VMGIntellimarker2012.pdf.
“When you work with an aggregator, you’re
putting yourself at better odds of not missing
contract connections and ensuring you have the
most accurate contract connection possible.”
– Nile Whitney, vice president of corporate accounts, ASC Division, Medline Industries, Inc. IS AGGREGATION
RIGHT FOR YOUR ASC?
Medline is strategic about picking its aggregation partners and works with aggregators that partner with different GPOs, explains Nile Whitney, vice president of corporate accounts for Medline’s ASC division.
“We’re GPO neutral,” Whitney says. “Our customers and prospective customers decide what GPO they want to work with.”
For some ASCs, partnering with an aggregator through Medline can help them improve financially while accessing the same — or better quality — medical products, delivered on time where they need them.
“We’ve identified which aggregators have the best tiers in a surgery center’s highest spending areas, so if those items are among your biggest spends, an aggregator can help you improve your cost savings quite a bit,” Whitney says.
Your Medline representative can analyze your historical purchasing patterns and the types of procedures you do most frequently. “By knowing your history and key products, we can really help guide you to maximize your cost savings,” Whitney explains.

26 OUTPATIENT OUTCOMES 2018
FEATURE
By removing total knee replacements (TKRs) from its Medicare inpatient-only list in 2018, the Centers for Medicare and Medicaid Services (CMS) opened the door for ambulatory surgery centers to become a viable option for Medicare-age patients who need these procedures. However, CMS’ 2018 Outpatient Prospective Payment Systems Final Rule did not add TKRs to the ASC Covered Procedures List. The latest rule maintains that all TKRs performed on fee-for-service Medicare beneficiaries still be performed at hospitals.
“Yes, this was a disappointment,” admits Sandra Berreth, administrator at Sansum Clinic Foothills Surgical Center. The Santa Barbara, California-
ASCs REACT TO RULING ON TOTAL JOINTS
Though CMS declined to include total knee replacements on its 2018 ASC Covered
Procedures List, administrators remain
optimistic about future reimbursement.
Left to right: Gina Hoffman, administrative director, and Tracey Ziegler, RN clinical director, Ophthalmology and Surgical Institute of Central Pennsylvania.
“Any time that our facility can offer our patients procedures that were
previously only done in a hospital, that’s a win for us and for our patients.”
– Gina Hoffman, administrative director, Ophthalmology and Surgical
Institute of Central Pennsylvania
based surgery center performs TKRs (non-Medicare), shoulder-joint replacements, and most joint arthroscopy “as applicable to the patient.”
“The ASC healthcare community will continue discussing with CMS the financial benefits of performing these procedures in ASCs,” Berreth says. “Ultimately, it is the healthcare provider’s responsibility to determine the right candidates for the right place of service based on anesthesia requirements, pain management and comorbidities.”
For now, TKRs remain a hospital-centric debate — focused on the difference in recovery times for inpatient versus outpatient TKRs in hospitals, not ASCs. That could soon change.
CMS has requested data to understand how to adjust reimbursement as it determines whether to add total joint procedures to

Issue 9 27
the ASC Covered Procedures List. With some centers already performing such cases, the request highlights the need to collect and share outcomes data from total joints procedures along with the financial benefits.
There’s always next year Many ASC administrators, like Berreth, expect that CMS will add total knee replacement to the ASC Covered Procedures List in 2019. The decision to remove TKRs from the inpatient-only list is a step in the right direction.
“I believe that, for 2019, the addition of total knee replacements is likely,” says Tracey Ziegler, RN clinical director at the Ophthalmology and Surgical Institute (OSI) of Central Pennsylvania in Carlisle, Pennsylvania. “For our facility, I’m unsure about [performing] total hip replacements because recovery time is longer than what we can provide. It is better that we start with knee replacements before taking the leap to hip replacements.”
Still, Ziegler says she believes there are U.S. surgery centers that could perform knee, hip, and shoulder replacements.
As a recipient of two hip replacements, Gina Hoffman, administrative director at OSI of Central Pennsylvania, says she is very aware of the pain-management challenges stemming from these procedures. Hoffman says that ASCs could perform total joint replacements given the right circumstances and the right patients. Age and health are important factors.
“Knee replacement recipients tend to be younger, so that helps in the grand scheme of things,” Hoffman explains. Like Ziegler, she agrees, “It’s great to start with knee replacements and then work our way into more complicated procedures.”
Hoffman confirms that her facility
will explore adding TKRs moving forward. “And,” she adds, “should total hips be added to the mix one day, then we will certainly explore our options with those procedures, as well.”
Looking aheadSo, what happens next? ASCs will continue collecting data around all procedures — returns to the OR, infections, post-operative pain, patient satisfaction, hospital transfers and, new for 2019, normo-thermia on all patients receiving gen-eral anesthesia. Total joints procedural data would also be a helpful addition, both to address CMS’ request for data and to prepare for the day when CMS approves total joint procedures for ASC reimbursement.
Those preparations are already beginning for some ASCs.
“We’re working with one of our pro-viders of orthopedic devices,” Ziegler says. “We have a surgeon interested in doing these knee replacements at our center, and he had to complete training on procedures using the provider’s equipment. Also, the provider will have a company representative in the OR, initially, to answer questions.”
If, and when, CMS covers total joint procedures in the ASC setting, the additional revenue won’t come without challenges. New processes will need to be developed, costs for equipment, supplies and staff will increase, and administrators will find themselves working hard at negotiating fair pay-ments for these new procedures.
However, many ASCs may wel-come these challenges as they look forward to increased income and procedure opportunities, as well as
the patient-centric benefits.“Any time that our facility can offer
our patients procedures that were previously only done in a hospital, that’s a win for us and for our patients,” Hoffman says. “For us — because we are always looking for opportunities to increase our revenues, help our staff add new skills and grow our center. For our patients — because it offers the opportunity to have a procedure at an outstanding facility, yet still be able to recover at home.”
Ziegler notes, “Studies have shown time and time again that patient out-comes in ASCs are phenomenal. Patient and surgeon satisfaction is very high, and infection-control rates are essen-tially zero.”
And, of course, it’s hard to discount the opportunity to provide high-quality care for orthopedic patients at lower costs. “The cost savings associated with ASCs should be a major consideration for Medicare and all other payers,” Berreth says.
“The cost savings associated with
ASCs should be a major consideration
for Medicare and all other payers.”– Sandra Berreth, administrator,
Sansum Clinic Foothills Surgical Center

COLUMN
28 OUTPATIENT OUTCOMES 2018
Coordinator Mimi Bercan. “Sometimes, cases show up just
in the nick of time,” Bercan says. “Other times, we are able to make substitutions like utilizing 100ml bags when we are short 50ml bags.”
How the right distribution partner can helpThe Federal Drug Administration (FDA) has taken steps to mitigate the shortage, including allowing for the importation of saline, extending expiration dates on products where safety is not affected, and approving two additional companies (Fresenius Kabi and Laboratorios Grifols) to supply the U.S. market.2 The agency expects improvement within the coming months. However, it will take time for par levels to stabilize. Meanwhile, manufacturers are limiting their inventory to existing customers and capping orders at historic levels.
As the shortage begins to ease, the right medical supply distribution partner can continue to serve as a strategic ally. Top distributors work directly with manufacturers and have the most current information. They can leverage their supply chains and scour the marketplace for available product.
Purchasing through industry-
leading distributors also ensures that — during a crisis — the supplies you receive for your patients continue to meet the highest quality and safety standards.
“I have been fortunate to have strong relationships with all my distributors,” Copeland says. “They have been proactive in looking out for us and helping us secure product wherever it is available.”
REFERENCES
1. Statement from FDA Commissioner Scott Gottlieb, M.D., on ongoing efforts to mitigate impact of saline shortages during this flu season. www.fda.gov/NewsEvents/Newsroom /PressAnnouncements/ucm595020.htm.
2. FDA Commissioner Scott Gottlieb, M.D., updates on some ongoing shortages related to IV fluids. www.fda.gov/NewsEvents/Newsroom PressAnnouncements/ucm592617.htm.
Ever-present at patient bedsides and operating tables, sterile bags of IV fluids are medicine’s first responders. So, what happens when the supply runs dry?
The United States has experienced intermittent shortage of saline solution since 2014, as the three U.S. manufacturers, B. Braun Medical, Baxter Healthcare and Hospira (now part of ICU Medical), have worked to overcome challenges including maintenance shutdowns, supply constraints and increased demand. The situation became drastic in September 2017 when Hurricane Maria devastated Puerto Rico, knocking out power at the manufacturing facilities of Baxter Healthcare and disrupting its production of small-volume saline (50ml and 100ml). Recently, demand for fluid of all sizes has spiked because of this season’s widespread flu outbreak.1
“It has been arduous,” says Gigi Copeland, materials manager at Melville Surgery Center in Long Island. “At one point, I was down to two days’ worth of product. Restricting fluids throughout the center requires teamwork between our doctors and staff. They must determine the lowest impact fluid management for patients to have their procedures completed safely and effectively.”
The Surgery Center in Middleburg Heights, Ohio, is facing similar challenges, says Materials Management
Supply update: SALINE SOLUTION
“Sometimes, cases show up just in the nick of time. Other times, we are able
to make substitutions like utilizing 100ml bags when
we are short 50ml bags.”– Mimi Bercan, materials management
coordinator, The Surgery Center
With the IV saline shortage expected to continue through midyear, ASCs can look to distributors for help.

$$INVOICE
INVOICE
INVOICE
PO APPROVED
√√√
Mobile and Tablet applications o�er Barcoding and Template based ordering – Point and Click Purchasing.

30 OUTPATIENT OUTCOMES 2018
COLUMN
With supply costs being one of the largest expenses for ASCs, it’s imperative that surgery centers commit to improving inventory management. Poor inventory practices can lead to a supply surplus, expired or lost supplies, and incorrect supply orders — all of which negatively affect your ASC’s bottom line.
An inventory management system can help your ASC unlock operational efficiencies and control costs by streamlining purchasing and inventory processes. Benefits of a comprehensive inventory management system include:
Automated ordering. An inventory management system helps save time and increases accuracy of orders by reducing human error. Time-consuming paperwork and multiple data-entry portals are consolidated, and low supply levels are easily identified, ordered and tracked.
Transparent pricing. With a clear picture of inventory and product pricing, ASCs can be certain they are receiving the most competitive price on supplies. Plus, consolidated sources help maintain pricing consistency.
Accurate invoicing. Automating invoices and payment processes through a fully featured inventory management system can help ASCs reduce financial errors and improve performance.
Spend management. Through their software, ASCs can easily obtain reporting and spend analytics, and track and measure cost-saving initiatives with confidence.
reviewed, discussed, understood, accepted and followed by all team members.
Develop a common language. A supply may not be described the same way by everyone. To avoid confusion, regularly discuss the language you are using to describe supplies and confirm that everyone is on the same page.
Utilize your partners. Working with your current technology partner, distribution partner and the inventory management vendor, you can compile the resources you need to make your case for implementation to your managing board or physicians group.
Thank you to Steven Britt, managing partner at Inventory Optimization Solutions, and Micah McClelland, vice president of business development at Hybrent, for their contributions to this article.
Smart inventory managementAutomate your supply chain with inventory management software to streamline operations and control costs
Keys to implementing a successful systemA well-designed inventory management platform should align all the departments within the ASC toward a common goal with:• A simple, intuitive
user interface • Modular functionality • Advanced technology
that keeps pace with the accelerating rate of change in healthcare
• Synchronization with vendors• Opportunities to integrate with
other software systems • Strong technical support during
implementation and operation.During the due diligence
process, your team will interact with multiple software company representatives, including account management, customer success, implementation and IT. To achieve your desired return on investment, it’s important to set your ASC up for success from the start.
Get everyone involved in the decision-making process. Inventory management is the responsibility of everyone in the ASC. That includes staff members who order and stock supplies, choose supplies for a case, schedule cases, update medical records and perform coding and billing. Physicians are also stakeholders, so involve at least one physician from each specialty.
Collaborate throughout the process. Every step should be
With a clear picture of inventory and product
pricing, ASCs can be certain they are receiving the most
competitive price on supplies.

Powerful. Flexible. Smart. Let Envi® Surgical Drive Your Supply Chain.
Envi® Surgical from IOS delivers uniquely powerful, modular, web-based supply chain solutions, with the flexibility to support facilities throughout your continuum of care.
Our commitment is to guide our customers to a better supply chain, providing high-touch support, industry best-practices, deep healthcare expertise and continuously evolving solutions that help them succeed.
Our goal is to ensure IOS customers have more time for their most important role each day: caring for patients.
✓ Smart purchasing
✓ Product usage tracking
✓ Inventory control
✓ Robust reporting
✓ World-class customer service
✓ Enterprise product catalog
✓ Preference cards
✓ 3-Way invoice matching
✓ Simple receiving
✓ Complete mobility
Top 10 Reasons to Choose Envi Surgical:
CL102_MedlineAd_2.23C.indd 1 2/23/18 3:56 PM

Medline Industries, Inc.Three Lakes DriveNorthfield, IL 60093
DID YOU KNOW ? Our EZPlus models offer a closed-doordrying system.
WHY IS THIS IMPORTANT ? This ensures the door remains closed throughout the dry cycle to maintain sterility and efficient drying of packs and pouches.
$450 orTo redeem, the end user must visit www.tuttnauerUSA.com/Q2-2018-rebate, upload the dealer invoice dated April 1 thru June 30, 2018 (with doctor’s and/or practice/facility name and date purchased), complete the information required on the form (which includes the serial number of the autoclave), and select “Submit”. All information will be verified by Tuttnauer USA upon submission. A confirmation email will be sent for your records. Keep the confirmation until goods or rebate are received. Redemption deadline is July 31, 2018. Please allow 4 weeks for receipt of rebate or shipment of free goods. Excludes reconditioned and scratch and dent machines.
CANNOT BE COMBINED WITH ANY OTHER MANUFACTURER OFFERS OR PROMOTIONS.
Buy any new EZPlus, EZ or Elara11 from April 1 thru June 30, 2018 and get your choice of a $450.00 manufacturer’s rebate or a FREE 1 gallon Water Distiller
A$ 714RetailValue
Manufacturer’sRebate
FREE WaterDistiller
Designed to meet the most current sterilization standards ANSI/AAMI ST55
12
3
LARGEST SELECTION
BEST WARRANTY
BIGGEST CHAMBER SIZES
• 2 Year Parts & Labor Warranty* • 10 Year Chamber Warranty
*Fully automatic units only
Q2 2018 Rebate Offer
THE BIG
3Use promo code MedlineAd2018 for an add'l. $50 manufacturer's rebate
*
Tel: (800) 624 5836, (631) 737 4850 Email: [email protected], www.tuttnauerUSA.com
MKT1897365 / LIT997R / 4K