Embed Size (px)
Citation preview

Do neurobiological understandings of smoking influence quitting self-
efficacy or treatment intentions?
Kylie Morphett PhD a,e*, Adrian Carter PhD b,c, Wayne Hall PhDb,d, Jayne Lucke PhDa,f,
Brad Partridge PhDg,h, and Coral Gartner PhD a,b
a University of Queensland School of Public Health, Public Health Building, Corner of
Wyndham Street and Herston Road, Herston, 4029, Queensland, Australia. b University of Queensland Centre for Clinical Research, Royal Brisbane and Women’s
Hospital Site, Herston, 4029, Queensland, Australia.c School of Psychological Sciences and Monash Institute of Cognitive and Clinical
Neurosciences, Monash University, Clayton, 3800, Victoria, Australia. d University of Queensland Centre for Youth Substance Abuse, Floor K, Mental Health
Centre, Royal Brisbane and Women’s Hospital, Herston, 4029, Queensland, Australia. e University of Queensland School of Medicine, Royal Brisbane and Women’s Hospital
Site, Herston, 4029, Queensland, Australia.f LaTrobe University, Australian Research Centre in Sex, Health and Society, Melbourne,
3000, Australia. g Research Development Unit, Caboolture Hospital, Metro North Hospital and Health
Service (MNHHS), Caboolture, 4510, Queensland, Australia.h The University of Queensland, Prince Charles Hospital Northside Clinical Unit, School of
Clinical Medicine, Herston, 4029, Australia.
* Author to whom correspondence should be addressed; Kylie Morphett, University of
Queensland School of Public Health, Public Health Building, Corner of Wyndham Street
and Herston Road, Herston, 4029, Queensland, Australia. E-Mail: [email protected];
Tel: +61-(0)7-3346-5475.
Competing interests: None

Keywords: health communication, neuroscience, nicotine addiction, lay beliefs, smoking
cessation.
Word Count: 4,108
ABSTRACT
Introduction: Addiction is increasingly defined as a “brain disease” caused by changes to
neurochemistry. While nicotine addiction has historically been excluded in the brain disease
model of addiction (BDMA), it is beginning to be labelled a chronic brain disease. We
investigated whether Australian smokers endorse brain-based explanations of smoking, and
whether these beliefs are associated with quitting self-efficacy or treatment intentions.
Method: Cross-sectional study of Australian smokers (N=1,538) who completed a survey
measuring their agreement with statements on the brain's role in smoking. Logistic
regressions tested associations between these items and sociodemographic variables, quitting
self-efficacy and intention to use cessation medications.
Results: The majority (57.9%) agreed that smoking changed brain chemistry and 34.4%
agreed that smoking was a brain disease. Younger and those with more education were more
likely to endorse brain-based understandings of smoking. Participants who agreed smoking
changed brain chemistry were more likely to report an intention to use cessation medicines
(OR 1.5, 95% CI 1.0-2.2) as were those who agreed that smoking was a brain disease (OR
1.5, 95% CI 1.1-2.1). Self-efficacy did not differ between those who agreed and disagreed
that smoking changed brain chemistry. However, those who agreed that smoking was a brain
disease had higher self-efficacy than those who disagreed (OR 1.7, 95% CI 1.3-2.3).
Conclusion: A neurobiological view of smoking does not dominate public understandings of
smoking in Australia. Endorsement of neurobiological explanations of smoking were

associated with increased intention to use cessation aids, but were not associated with
reduced self-efficacy.
IMPLICATIONS
Explaining tobacco dependence in neurobiological terms is unlikely to induce feelings of
fatalism in relation to smoking cessation. Those who endorse biomedical explanations of
smoking may be more open to using cessation pharmacotherapies. Describing smoking in
terms of alterations in brain chemistry may be more acceptable to smokers than labelling
smoking a “brain disease” or “brain disorder.”

INTRODUCTION
Drug addiction is increasingly portrayed as a biological phenomenon in which the brain plays
the central role. The National Institute of Drug Abuse (NIDA) have long argued that
addiction is a “chronic and relapsing brain disease” [1]. In 2016, the US Surgeon general
released a report claiming that addiction is a brain disease, and treating it as such would
reduce the stigma and blame associated with addiction, overcoming many of the barriers to
addiction treatment [2]. Similarly the American Society for Addiction Medicine have defined
addiction as a “primary, chronic disease of brain reward, motivation, memory and related
circuitry” [3]. While nicotine has historically been treated differently to other psychoactive
drugs [4], the “brain disease model of addiction” (BDMA) also encompasses nicotine
addiction because, like other drugs, nicotine produces long-term changes to neurochemical
pathways in the brain [5-7]. Hence, smoking is increasingly medicalised by being labelled a
“chronic brain disorder” [8] and a “chronic disease.” [9-11]. A recent report on e-cigarettes
and young people by the US Surgeon General has emphasised the potentially damaging
effects of nicotine on the adolescent brain [12] and an associated video warns the public of
the dangers of “brain risks” to young people from use of e-cigarettes [13].
Smokers are exposed to biomedical explanations of tobacco dependence via the media, where
the neurobiological aspects of smoking are reported in articles with titles such as “Smokers
who quit may have brains hard-wired for success” [14] and “Quitting is a brain game.” [15].
Some clinicians have recommended discussing neurobiological aspects of nicotine addiction
with smokers in clinical consultations to help them understand why quitting is difficult and to
reduce self-blame [16]. Also, novel treatments for smoking cessation based on neuroscience,
such as transcranial magnetic stimulation and various new pharmacotherapies, are being
investigated [17, 18].
4

Proponents of the BDMA believe it will reduce the stigma of drug dependence and lead to the
development of more efficacious treatments [19-21]. Those critical of biomedical models
have expressed concern that the belief that addiction is “hard-wired” in the brain may lead to
fatalism and a diminished sense of self-efficacy [22-24]. Neuroscience based explanations
could contribute to what Dweck has labelled a “fixed mindset” where individuals believe that
nature determines their behaviour, rather than a “growth” mindset that encourages attempts to
change problematic behaviours [25].
Alternatively, understanding addiction as a neurobiological disorder may increase positive
perceptions of targeted cessation pharmacotherapies. Knowing that medications are available,
and understanding how they work, could make quitting smoking seem easier and encourage
more quit attempts. Research from the genetics field has looked at the impact of genetic
understandings of tobacco addiction on smokers’ sense of control and treatment preferences
[26-28]. Mixed findings and variations in study design limit the conclusions that can be
drawn from these studies. Moreover, it remains to be seen if people respond to genetic and
neuroscience information in similar ways, given important differences between the two [29].
This paper examines the extent to which Australian smokers endorse neurobiological
explanations of smoking, and whether endorsement of neuroscientific explanations of
smoking are associated with quitting self-efficacy or preferences for using particular smoking
cessation methods.
METHOD
5

Design and Sampling
An online survey was completed by 1,538 Australian smokers. All participants were recruited
from a commercial online research panel in 2015. Panel members were recruited from online
and offline sources. Survey completers received points for participation that could be
converted into gift vouchers. The invitation strategy was adjusted daily with quotas to obtain
a sample representative of the demographic profile of the population of Australian smokers in
terms of age and gender [30]. In order to be eligible, participants had to be 18 years old or
older, an Australian citizen or resident, to smoke daily, and to have smoked more than 100
cigarettes in their lifetime. The Human Research Ethics Committee of the University of
Queensland granted ethics approval for this study (Approval number: 2009001022).
Of the 6,520 invited participants who clicked on the link to the survey, 4,273 did not smoke
daily, 49 had not smoked at least 100 cigarettes and 16 exited the survey before completing
the eligibility questions and were excluded. Of those who met the eligibility criteria
(N=2,182), 625 dropped out before completing the survey. Seven identified as duplicate cases
caused by a computer error were removed from the dataset. Despite reporting daily smoking
on the screening questions, 12 participants stated that they smoked zero cigarettes per day on
a subsequent question and were excluded from the dataset. For further details of the
recruitment process see Supplementary File 1.
Measures
The survey was informed by a literature review and the results of a qualitative study that has
been published elsewhere [31]. Given the paucity of research in this area, the survey design
was also informed by research in related areas, such as studies of the attitudes of persons
experiencing other drug addictions towards the role of the brain in their addictions [32-34].
6

Sociodemographic variables are included in Table 1. Level of nicotine dependence was
measured using the Heaviness of Smoking Index (HSI) [35]. Desire to quit was assessed by
the item “How much do you want to give up smoking?” with response options of: not at all, a
little bit, quite a bit, or very much. Those who responded “not at all” were classified as
having no to desire to quit, and compared to all others who expressed some level of desire to
quit. Quitting self-efficacy was measured using a single item: “If you decided to give up
smoking completely in the next six months, how sure are you that you would succeed?” This
item has been used extensively in the International Tobacco Control Policy Evaluation
Project (ITC) [36-38] and other national surveys [39]. Response options were: “not at all
sure, slightly sure, moderately sure, very sure, or extremely sure.” There is no consensus in
the literature on how to analyse this item, and it has been treated as a continuous or
categorical variable in various studies. Because it is a single item five point item that is not
part of a larger scale, we decided against treating it as a continuous variable, and
dichotomized the responses for ease or interpretation. For the purposes of analysis, responses
were dichotomized so that those who responded “not at all” or “slightly sure” were labelled
as having low self-efficacy, and the remaining responses were combined to represent
“moderate/high” self-efficacy.
Participants were provided with a list of smoking cessation strategies and asked to check all
that they had previously used. Those who reported having used nicotine replacement therapy
(NRT) or prescription medicines (Champix or Zyban) were coded as having used a cessation
medication. Intention to use pharmacotherapy in future quit attempts was assessed with the
question “If you decided to make a quit attempt, how likely is it that would use the following
method.” Response options were: “definitely wouldn’t use, probably wouldn’t use, probably
would use, definitely would use, and don’t know". Those who selected “probably” or
7

“definitely would use” for NRT or prescription medicines were categorised as intending to
use medications. All other responses were classed as not intending to use medication.
Four items were developed to assess strength of endorsement of beliefs about the role of
neurobiology in smoking. Participants were asked to rate the extent to which they agreed with
the following statements on a four-point scale (strongly disagree, disagree, agree, strongly
agree) with the option of “don’t know” response: “Smoking is a brain disease”; “Smoking
changes the chemistry of the brain”; “Smoking damages the brain”; and “Smoking is a
brain disorder.”
Data analysis
From the four brain beliefs items, two key items measuring the strength of endorsement of
brain-based explanations of smoking were selected for further analysis: 1)“Smoking changes
the chemistry of the brain”; and 2) “Smoking is a brain disease.” These two items were
chosen for further investigation because they represented two ways that the role of the brain
in smoking has been portrayed. The first item selected for further analysis, that “Smoking
changes the chemistry of the brain” represents the scientific view that smoking influences
neurobiological mechanisms that then make it difficult to quit. The second item chosen,
“Smoking is a brain disease” represents the controversial NIDA labelling of addiction as a
chronic “brain disease.” Empirically, the brain disease and brain chemistry items elicited
different response patterns amongst participants, while there was significant covariance
between other items (for example between “Smoking is a brain disease” and “Smoking is a
brain disorder”), which contributed to the decision to retain only these two items for further
analysis.
8

For each of these items, the five point Likert scale was converted into a dichotomous variable
comprised of disagree (disagree combined with strongly disagree = 0) and agree (agree
combined with strongly agree = 1). We conducted chi-squared and t-tests to determine
differences between those who selected “don’t know” compared to those who expressed an
opinion about brain-based explanations of smoking (Table 1). Because our primary research
question was whether opinions on brain-based explanations of smoking are related to
outcome variables, we excluded from the primary analyses those who selected “don’t know”
responses on these items.
For each of these two key brain-related items, contingency tables and the Pearson’s chi-
squared statistic were used to examine which categorical variables were associated with
scores on these two items. Age and level of nicotine addiction (HSI) were analysed as
continuous variables using t-tests. Categorical independent variables were gender (male=0,
female=1), education (did not complete Bachelor degree = 0, completed Bachelor degree =1),
intention to use cessation medication (no intention = 0, intention=1), and self-efficacy
(low=0, moderate or high =1).
A binary logistic regression analysis then explored the relationship between endorsement of
each of the two key neurobiological explanations of smoking and intention to use medication
in a quit attempt. Intention to use medication was entered as the outcome variable (0=no
intention and don’t know, 1=intend to use). SPSS v22 was used for data analysis. All
variables were entered into the model simultaneously, with categorical variables dummy
coded. Demographic variables and smoking characteristics were gender (male=0, female=1),
age, level of education (did not complete Bachelor degree=0, completed Bachelor degree=1),
HSI score, self-efficacy (low=0, moderate or high=1), desire to quit (0=no desire, 1=some
9

desire) and past use of cessation medications (0=no, 1 = yes). The included brain-based items
were “Smoking is a brain disease” (0=disagree, 1=agree) and “Smoking changes the
chemistry of the brain” (0=disagree, 1=agree).
Another binary logistic regression analysis investigated the relationship between
endorsements of neurobiological explanations of smoking and self-efficacy. The outcome
variable was a dichotomised version of self-efficacy (0=low, 1= moderate or high). Predictor
variables were the same smoking characteristics and brain-related items used in the logistic
regression described above.
RESULTS
Participant demographics
Participant demographics are presented in Table 1. Of the entire sample, participant age
ranged from 18-88 years old with a mean of 43 years (SD 16.1). The proportion of the sample
born in Australia aligned closely with national population data (72.8% born in Australia)
[40]. In relation to education, 26.4% had no post-secondary qualification, 32.2% had
completed some post-secondary education at less than bachelor degree level, and 31.3% had
completed a bachelor degree or higher.
The mean number of cigarettes smoked per day was 15 (SD 9.6). Based on previous studies,
where the HSI has been categorized as low dependence for scores 0 or 1, moderate
dependence for scores 2-4, and high dependence for scores 5-6 [36, 41], 74.2% of
participants reported moderate or high nicotine dependence. Only 7.9% of participants
expressed no interest in quitting, with 38% stating that they wanted to give up “a little bit”
and 54.2% wanting to quit “quite a bit” or “very much.” Almost half (47%) reported low
levels of quitting self-efficacy, and 49.6% had used cessation medication for a past quit
10

attempt (either NRT or prescription medication). Approximately two thirds (67.2%) of
participants said that they would use cessation medications if they were to make a quit
attempt.
Table 1 shows differences between those who were excluded from the logistic regressions
because they responded “don’t know” to either of the two brain-related items, and those who
provided an opinion for both. Those who gave a “don’t know” response were older and had
lower levels of education.
Endorsement of brain-based explanations of smoking
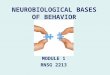
Figure 1 shows the percentage of the entire sample (N=1,538) who agreed or disagreed with
the items about the role of the brain in smoking. The majority (57.9%) agreed or strongly
agreed that smoking changes brain chemistry. The findings were similar for the statement that
smoking damages the brain (54.6% agree or strongly agree). Fewer participants agreed that
smoking was a brain disease (34.4% agree or strongly agree) or a brain disorder (32.6% agree
or strongly agree). There were high proportions of “don’t know” responses for each item,
suggesting that many were unfamiliar with the role of the brain in smoking, or did not feel
confident enough to make a judgment. As a neutral option was not included in the scale, it is
also possible that those who had a neutral position selected the “don’t know” option.
Who endorses brain-based explanations of smoking?
After excluding the participants who selected “don’t know” for either of the key brain-related
items, agreement with the statement that “smoking changed brain chemistry” was not
significantly associated with gender, level of self-efficacy, or level of nicotine dependence
but it was strongly associated with age (see Table 2). There was a statistically significant
11

difference in age (p<0.001) between those who agreed that smoking changed the chemistry of
the brain (M=39.6, SD=14.6) and those who disagreed (M=44.1, SD=17.6)
Endorsement was also associated with education. Those who had a Bachelor degree were
more likely than those without a degree to agree that smoking changed brain chemistry
(p=0.02) Those who agreed that smoking changed brain chemistry were more likely than
those who disagreed to intend to use medication on their next quit attempt (p<0.001). There
was no statistically significant association between agreement that smoking changed brain
chemistry, or level of self-efficacy. Those who expressed a desire to quit smoking were more
likely than those who had no desire to quit to agree that smoking changed brain chemistry
(p<0.001).
The findings were similar for endorsement of the statement that “smoking is a brain
disease”. Level of nicotine dependence was not related to endorsement while age was
strongly related. Participants who agreed that smoking was a brain disease were younger
(M=38.2 years, SD=16.6) than those who disagreed (M=43.7 years, SD=14.3) (p<0.001).
Females were significantly more likely to disagree that smoking was a brain disease than
males (56.9% versus 49.2%). Again, those with a university degree were more likely to agree
that smoking was a brain disease (55.3%) than those without a degree (42.9%). Those who
agreed that smoking was a brain disease had higher self-efficacy (p<0.001), were more likely
to express an intention to use medication (p<0.001), and were more likely to report a desire to
quit (p<0.001).
12

Is intention to use medication associated with beliefs about the neurobiological basis of
smoking?
Table 3 shows that intention to use cessation medication was not related to age (OR 0.99,
95% CI 0.98-1.00) or gender (OR 1.18, 95% CI 0.87 -1.60), once other sociodemographic
factors were controlled for. Education was significantly related to intention to use cessation
medications: those who had a university degree were more likely than those with no high
school education to intend to use medications (OR 1.55, 95% CI 1.12-2.20). Those with
higher levels of nicotine dependence were more likely (OR 1.13, 95% CI 1.02-1.25) to intend
to use medications than those with lower levels of nicotine dependence. There were no
statistically significant difference in intention to use medication between those with low and
higher levels of self-efficacy, or between those with high or low desire to quit. Participants
who agreed that smoking changed the chemistry of the brain were more likely to report an
intention to use medication (OR 1.51, 95% CI 1.03-2.21) as were those who agreed that
smoking was a brain disease (OR 1.54, 95% CI 1.11-2.13). These effect sizes were
statistically significant but only of moderate size. The biggest predictor of intention to use
medications was past use: those who had used cessation medications in the past were more
than twice as likely to intend to do so in the future (OR 2.68, 95% CI 1.94-3.70).
Is smoking cessation self-efficacy associated with beliefs about the neurobiological basis
of smoking?
The results of the binary logistic regression analysis testing the relationship between self-
efficacy and beliefs about the role of the brain in smoking are shown in Table 4. Gender,
education, and past use of medication did not make a statistically significant contribution to
the final model. Those who were younger were less likely to report low self-efficacy (OR
13

0.98, 95% CI 0.98-0.99), although this effect was small. Those who desired to quit had
greater odds of reporting higher self-efficacy (OR 2.70, CI 1.57-4.64).
As expected, participants with high dependence had significantly lower levels of self-efficacy
than those with low dependence (OR = 0.79, 95% CI 0.0.72-0.87). There was no difference in
self-efficacy between those who agreed and those who disagreed that smoking changed the
chemistry of the brain (OR 0.80, 95% CI 0.55-1.16). For the brain disease item, there was a
statistically significant difference between those who agreed and disagreed: those who
agreed that smoking was a brain disease were more likely to have high self-efficacy than
those who disagreed (OR 1.70, 95% CI 1.26-2.30).
DISCUSSION
One aim of this study was to investigate the proportion of Australian smokers who endorse
brain-based explanations of smoking. Such research has not been conducted in Australia
previously, but it can indicate the extent to which smoking has been medicalised and whether
smokers have adopted neuroscientific explanations of addiction. The results demonstrate that
around one third of our sample of Australian smokers agreed that smoking was a brain
disease, and a similar proportion did not know whether this was true. A higher proportion of
participants agreed that smoking changes the chemistry of the brain, but a substantial
proportion of participants were uncertain. This is consistent with recently published
qualitative work, which found that most of the participants acknowledged that smoking
influenced their brain while disagreeing that it was a brain disease [42]. They believed the
brain disease terminology was inaccurate and likely to lead to an increase in stigma.
14

We also found that those who were less educated were more likely to select the “don't know”
response. This is consistent with other research on health and public understandings of
science [43, 44]. It was unclear whether this is because the less educated have less knowledge
of the topic of smoking and the brain, or they are less likely to express opinions on unfamiliar
topics. The complexities of the “don’t know” response have been outlined by social science
researchers [45, 46]. A “don’t’ know” response does not always signify ignorance, but can
reflect “the absence of representation, to a sense that the question is irrelevant to the
respondent and/or it may relate to the defensive needs of the individual.” [45] Other items in
the survey did not have such high proportions of participants selecting the “don’t know”
response. For example, on the items asking about intention to use various quitting options,
rates of “don’t know” responses were mostly between 10-14%, suggesting that the high levels
of “don’t know” options for the brain-related questions was not due to a general
disengagement with the survey.
Another aim was to examine whether socio-demographic variables predicted endorsement of
brain-based understandings of smoking. Endorsements of brain-based beliefs about smoking
were not uniform across social groups. Those who endorsed the stronger form of the “brain
disease” explanation of smoking were more likely to be: male, younger, have greater self-
efficacy, more years of education, a desire to quit smoking, and intended to use medication
on their next quit attempt. Those who agreed with the less controversial language that
smoking changes the chemistry of the brain were also younger, more highly educated, and
were more likely to intend to use medication than those with disagreed. These findings are
discordant with predictions that the biomedical models of addiction will reduce self-efficacy
in addicted individuals [23] but supports predictions that it could be related to the use of
15

medications for cessation. As these are cross-sectional data, it is not possible to determine the
direction of the relationship.
A third aim was to assess whether endorsement of brain-based explanations of smoking were
associated with intention to use medication. While there was a positive relationship between
intention to use cessation medication and endorsement of brain-based explanations of
smoking, the strength of the association was modest. Based on these results, promoting brain-
based explanations of smoking is unlikely to substantially increase the use of cessation
medications. But it is unlikely to discourage uptake of cessation aids. A greater effect was
seen for past use of medication, with those who had used medication in the past around three
times more likely to do so in the future. This is consistent with research that those who have
used cessation pharmacotherapies often report finding them helpful [47], and that smokers
who had used NRT or bupropion in the past were more likely to perceive them as helpful
than those who had not tried them [48].
The last aim was to investigate whether acceptance of smoking as a brain disease was
associated with self-efficacy. We found that agreement that smoking was a brain disease was
associated with higher self-efficacy. This conflicts with predictions that promotion of
biomedical understandings of addiction will increase fatalism about smoking [23]. While
more research is required to confirm the findings, this suggests that neuroscience
explanations of addiction, at least in relation to smoking, are not associated with a “fixed”
mindset of behaviour that results in reduced self-efficacy [25]. In fact, the qualitative
evidence on this topic shows that addicted individuals often emphasise autonomy, choice and
responsibility, which more closely represents a “growth” mindset [31,42].
16

The size of many of these statistically significant associations were small, reflecting the large
sample size used in this study. Statistical significance does not necessarily mean that the
predictor variable will have practical significance or that changing the variable will have a
substantial population level impact on smoking. Our findings suggest that endorsement of
brain-based explanations of smoking have a relationship with treatment preferences and self-
efficacy, but that the effect sizes are relatively small. However, the belief that smoking
changes brain chemistry or is a brain disease in some cases had a larger effect than age,
gender and level of nicotine dependence. Overall, the promotion of neurobiological models of
smoking appear unlikely to negatively impact quitting at the population level.
A number of limitations of our study must be acknowledged. Firstly, participants were not
recruited via random sampling. Participants were members of an online market research
panel so may differ from smokers who were not members of this panel. While resourcing
requirements ruled out the possibility of other sampling methods, such as random digit
dialling, the changing nature of survey recruitment means that online panels are increasingly
being used as a cost-effective and valid means of collecting survey data [49]. In addition, the
validity of older methods of random sampling is being undermined by the increasing use of
mobile phones and reductions in survey response rates [50, 51]. Also, our sample closely
matched the Australian population of smokers in relation to age, gender, and being born
overseas.
Future studies could employ more sophisticated educational materials to better inform
participants about the neurobiology of smoking and assess its impact on cessation attempts
and self-efficacy, or focus groups to allow greater discussion and analysis of the complexity
of neuroscientific research. Moreover, only self-reported attitudes have been investigated thus
17

far, and it is unknown whether intentions and attitudes will impact on behaviour. Behavioural
choice experiments examining the impact of neurobiological explanations on participants’
actual behaviour (e.g., smoking, treatment choices, and quit attempts) are recommended.
On these results, it is possible that emphasising the role of the brain could increase intention
to use cessation pharmacotherapies but any such effect is likely to be small. Many factors
influence a smoker's preference for cessation methods and their sense of self-efficacy, and the
complexity of smokers’ conceptions of addiction, the brain, and agency have been
demonstrated in qualitative studies [31, 52, 53]. Overall, our results suggest that a
neurobiological view of smoking does not dominate public understandings of nicotine
addiction among smokers in Australia. When smokers do endorse brain-based explanations of
smoking, this does not appear to reduce cessation self-efficacy, as has been suggested by
some critics of medicalisation.
ACKNOWLEDGEMENTS
The authors would like to thank the participants who took the time to complete the survey.
Thank you to Taverner Research and the Online Research Unit (ORU) for administering the
survey. This work was funded by an Australian Research Council Discovery Grant (Grant ID:
DP120100732) awarded to WH. KM was supported by an Australian Postgraduate Award
and a UQ Advantage top up scholarship. WH was supported by a National Health and
Medical Research Council Australia Fellowship (Grant ID: 569738). CG and AC were
supported by National Health and Medical Research Council Fellowships.
REFERENCES
18

1. National Institute on Drug Abuse. Drugs, brains, and behavior: The science of addiction, Maryland: National Institutes of Health; 2007. Available at: https://www.drugabuse.gov/publications/drugs-brains-behavior-science-addiction/preface
2. U.S. Department of Health and Human Services Office of the Surgeon General. Facing Addiction in America: The Surgeon General's Report on Alcohol, Drugs, and Health, Washington. 2016. Available at: https://addiction.surgeongeneral.gov/surgeon-generals-report.pdf
3. American Society for Addiction Medicine. Definiton of Addiction; 2015. Available at: http://www.asam.org/for-the-public/definition-of-addiction
4. Hughes J. R. Nicotine don't get no respect: A replication test, Nicotine Tob Res 2013: 15: 588-590.
5. D'souza M. S., Markou A. Neuronal mechanisms underlying development of nicotine dependence: Implications for novel smoking-cessation treatments, Addict Sci Clin Pract 2011: 6: 4-16.
6. Picciotto M. R., Mineur Y. S. Molecules and circuits involved in nicotine addiction: The many faces of smoking, Neuropharmacology 2014: 76: 545-553.
7. Ray R., Schnoll R., Lerman C. Nicotine dependence: Biology, behavior, and treatment, Annu Rev Med 2009: 60: 247-260.
8. Prochaska J. J., Benowitz N. L. The past, present, and future of nicotine addiction therapy, Annu Rev Med 2016: 67: 467-486.
9. Fiore M. C., Jaen C. R., Baker T. B., Bailey W. C., Benowitz N. L., Curry S. J. et al. Treating tobacco use and dependence: 2008 update Rockville, Maryland: U.S. Department of Health and Human Services; 2008.
10. Morphett K., Carter A., Hall W., Gartner C. Medicalisation, smoking and e-cigarettes: evidence and implications, Tob Control 2016. doi: 10.1136/tobaccocontrol-2016-053348
11. Wolff F., Hughes J. R., Woods S. S. New terminology for the treatment of tobacco dependence: a proposal for debate, J Smok Cessation 2013: 8: 71-75.
12. U.S. Department of Health and Human Services. E-cigarette Use Among Youth and Young Adults: A Report of the Surgeon General: Department of Health and Human Services, Centers for Disease Control and Prevention; 2016. Available at: https://e-cigarettes.surgeongeneral.gov/documents/2016_SGR_Full_Report_non-508.pdf
13. U.S. Surgeon General. Know the Risks: E-cigarettes and Young People; 2016. Available at; https://e-cigarettes.surgeongeneral.gov/knowtherisks.html
14. Rapaport L. Smokers who quit may have brain hard-wired for success [media article]. Reuters, 22 May 2015. Available at: http://www.reuters.com/article/us-smoking-cessation-brain-wiring-idUSKBN0O62J820150522
15. Author Not Attributed. Quitting is a brain game [newspaper article]. The Gold Coast Bulletin, 19 March 2011.
16. Leone F. T., Evers-Casey S. Developing a rational approach to tobacco use treatment in pulmonary practice: A review of the biological basis of nicotine addiction, Clin Pulm Med 2012: 19: 53-61.
17. Beard E., Shahab L., Cummings D. M., Michie S., West R. New Pharmacological Agents to Aid Smoking Cessation and Tobacco Harm Reduction: What Has Been Investigated, and What Is in the Pipeline?, CNS Drugs 2016: 1-33.
18. Li X., Hartwell K. J., Owens M., Lematty T., Borckardt J. J., Hanlon C. A. et al. Repetitive transcranial magnetic stimulation of the dorsolateral prefrontal cortex reduces nicotine cue craving, Biol Psychiatry 2013: 73: 714-720.
19

19. Dackis C., O'brien C. Neurobiology of addiction: treatment and public policy ramifications, Nat Neurosci 2005: 8: 1431-1436.
20. Gardner P. D., Tapper A. R., King J. A., Difranza J. R., Ziedonis D. M. The neurobiology of nicotine addiction: Clinical and public policy implications, J Drug Issues 2009: 39: 417-441.
21. Leshner A. I. Addiction is a brain disease, and it matters, Science 1997: 278: 45-47.22. Caron L., Karkazis K., Raffin T. A., Swan G., Koenig B. A. Nicotine addiction
through a neurogenomic prism: Ethics, public health, and smoking, Nicotine Tob Res 2005: 7: 181-197.
23. Chapman S., Mackenzie R. The global research neglect of unassisted smoking cessation: Causes and consequences, PLoS Med 2010: 7: e1000216.
24. Dingel M. J., Karkazis K., Koenig B. A. Framing nicotine addiction as a "disease of the brain": Social and ethical consequences, Soc Sci Q 2011: 92: 1363-1388.
25. Dweck C. S. Mindsets and human nature: Promoting change in the Middle East, the schoolyard, the racial divide, and willpower, Am Psychol 2012: 67: 614-622.
26. Cappella J. N., Lerman C., Romantan A., Baruh L. News about genetics and smoking - Priming, family smoking history, and news story believability on inferences of genetic susceptibility to tobacco addiction, Comm Res 2005: 32: 478-502.
27. Park E. R., Kleimann S., Youatt E. J., Lockhart A., Campbell E. G., Levy D. E. et al. Black and White adults' perspectives on the genetics of nicotine addiction susceptibility, Addict Behav 2011: 36: 769-772.
28. Wright A. J., Weinman J., Marteau T. M. The impact of learning of a genetic predisposition to nicotine dependence: An analogue study, Tob Control 2003: 12: 227-230.
29. Greene R. M. From Genome to Brainome: Charting the lessons learned. In: Illes J., editor. Neuroethics: defining the issues in theory, practice, and policy, New York: Oxford University Press; 2006, p. 105-121.
30. Australian Institute of Health and Welfare. National Drug Strategy Household Survey detailed report 2013, Drug Statistics Series 2014: no.28. Cat. no. PHE 183.
31. Morphett K., Carter A., Hall W., Gartner C. A qualitative study of smokers' views on brain-based explanations of tobacco dependence, Int J Drug Pol 2016: 29: 41-48.
32. Meurk C., Partridge B., Carter A., Hall W., Morphett K., Lucke J. Public attitudes in Australia towards the claim that addiction is a (brain) disease, Drug Alcohol Rev 2014: 33: 272-279.
33. Netherland J. "We haven't sliced open anyone's brain yet": Neuroscience, embodiment and the governance of addiction. In: Pickersgill M. & Van Keulan I., editors. Sociological Reflections on the Neurosciences (Advances in Medical Sociology): Emerald Group Publishing Ltd; 2011.
34. Pescosolido B. A., Martin J. K., Long J. S., Medina T. R., Phelan J. C., Link B. G. "A disease like any other"? A decade of change in public reactions to schizophrenia, depression, and alcohol dependence, Am J Psychiatry 2010: 167: 1321-1330.
35. Heatherton T., Kozlowski L. T., Frecker R. C., Rickert W., Robinson J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day, Br J Addict 1989: 84: 791-800.
36. Borland R., Yong H.-H., Balmford J., Cooper J., Cummings K. M., O'connor R. J. et al. Motivational factors predict quit attempts but not maintenance of smoking cessation: Findings from the International Tobacco Control Four country project, Nicotine Tob Res 2010: 12: S4-S11.
20

37. Hyland A., Borland R., Li Q., Yong H.-H., Mcneill A., Fong G. T. et al. Individual-level predictors of cessation behaviours among participants in the International Tobacco Control (ITC) Four Country Survey, Tob Control 2006: 15: S83-S94.
38. Siahpush M., Yong H.-H., Borland R., Reid J. L., Hammond D. Smokers with financial stress are more likely to want to quit but less likely to try or succeed: Findings from the International Tobacco Control (ITC) Four Country Survey, Addiction 2009: 104: 1382-1390.
39. Bonevski B., Twyman L., Paul C., D'este C., West R., Siahpush M. et al. Comparing socially disadvantaged smokers who agree and decline to participate in a randomised smoking cessation trial, BMJ Open 2015: 5: e008419.
40. Australian Bureau of Statistics. Migration, Australia, 2011-12 and 2012-13. 34120; 2013. Available at: http://www.abs.gov.au/ausstats/[email protected]/Lookup/3412.0Chapter12011-12%20and%202012-13
41. Cooper J., Borland R., Yong H.-H., Mcneill A., Murray R. L., O’connor R. J. et al. To what extent do smokers make spontaneous quit attempts and what are the implications for smoking cessation maintenance? Findings from the International Tobacco Control Four country survey, Nicotine Tob Res 2010: 12: S51-S57.
42. Morphett K., Carter A., Hall W., Gartner C. Framing Tobacco Dependence as a "Brain Disease": Implications for Policy and Practice, Nicotine Tob Res 2017. doi: 10.1136/tobaccocontrol-2016-053348
43. Bauer M. Socio-demographic correlates of DK-responses in knowledge surveys: self-attributed ignorance of science, Soc Sci Inf 1996: 35: 39-68.
44. Waters E. A., Hay J. L., Orom H., Kiviniemi M. T., Drake B. F. “Don't Know” Responses to Risk Perception Measures: Implications for Underserved Populations, Med Decis Making 2013: 33: 271-281.
45. Bauer M., Joffe H. Meanings of self-attributed ignorance: an introduction to the Symposium, Soc Sci Inf 1996: 35: 5-13.
46. Sturgis P., Roberts C., Smith P. Middle Alternatives Revisited: How the neither/nor Response Acts as a Way of Saying “I Don’t Know”?, Socio Meth Res 2014: 43: 15-38.
47. Hung W., Dunlop S., Perez D., Cotter T. Use and perceived helpfulness of smoking cessation methods: Results from a population survey of recent quitters, BMC Public Health 2011: 11: 592.
48. Hammond D., Mcdonald P. W., Fong G. T., Borland R. Do smokers know how to quit? Knowledge and perceived effectiveness of cessation assistance as predictors of cessation behavior, Addiction 2004: 99: 1042-1048.
49. American Association for Public Opinion Research. AAPOR Report on Online Panels: AAPOR; 2010. Available at: http://www.aapor.org/AAPORKentico/AAPOR_Main/media/MainSiteFiles/AAPOROnlinePanelsTFReportFinalRevised1.pdf
50. Australian Communications and Media Authority. Research Snapshots: Older Australians resist cutting the cord; 2014. Available at: http://www.acma.gov.au/theACMA/engage-blogs/engage-blogs/Research-snapshots/Older-Australians-resist-cutting-the-cord#Roy%20Morgan%20Single%20Source,%20December%202013
51. Fogliani M. Low response rates and their effects on survey results. National Statistical Service, November 1999 Service. Available at: http://www.nss.gov.au/nss/home.NSF/75427d7291fa0145ca2571340022a2ad/4fc144d438726fbbca2571ab00247118?OpenDocument
21

52. Amos A., Wiltshire S., Haw S., Mcneill A. Ambivalence and uncertainty: experiences of and attitudes towards addiction and smoking cessation in the mid-to-late teens, Health Educ Res 2006: 21: 181-191.
53. Bottorff J. L., Johnson J. L., Moffat B., Grewal J., Ratner P. A., Kalaw C. Adolescent Constructions of Nicotine Addiction, CJNR: Can J Nurs Res 2004: 36: 22-39.
22

Table 1 - Participant demographics
Total Sample n=1538
With opinionn=930
Excluded due to don’t know response
Age, mean (SD)* 43.0 (16.1) 39.7 (15.2) 48.1 (16.4)Gender % Male Female
5446
5545
5248
Educational attainment % * No Bachelor degree Bachelor degree
68.731.3
62.337.7
78.621.4
Born in Australia % 75.3 75.9 74.3
* Statistically significant at the p<0.05 level.
23

Table 2 - Proportion of smokers who endorsed brain-based explanations of smoking stratified by demographics and smoking
characteristics
Strata Smoking changes the chemistry of the brain Smoking is a brain diseaseAgree Disagree p Agree Disagree p
Gender (%, N) Male Female
81.9 (484)81.7 (406)
18.1 (107)18.3 (91)
0.5050.8 (308)43.1 (221)
49.2 (298)56.9 (292)
0.01
Age (M, SD) 39.55(14.55)
44.12 (17.64)
<0.001 38.18 (14.26)
43.66(16.63)
<0.001
Highest education No Bachelor degree Bachelor degree or higher
79.9(560)85.3(330)
20.1 (141)14.7 (57)
0.0242.9 (309)55.3 (220)
57.1 (412)44.7 (178)
<0.001
Desire to quit (%, N) Not at all To some extent
62.5 (50)83.3 (840)
37.5 (30)16.7 (168)
<0.00122.1 (19)49.4 (510)
77.9 (67)50.6 (523)
<0.001
Level of dependence (HSI) (M, SD)
2.53 (1.54) 2.64 (1.60) 0.39 2.54 (1.56) 2.53 (1.56) 0.92
Self-efficacy (%, N) Low Moderate/High
79.9 (365)83.2 (525)
20.1 (92)16.8 (106)
0.0938.2 (186)54.3 (343)
61.8 (301)45.7 (289)
<0.001
Intention to use medication Intend to use medication No intention to use medication
85 (661)73.9 (229)
15 (117)26.1 (81)
<0.00151.5 (401)37.5 (128)
48.5 (377)62.5 (213)
<0.001
Chi-square tests of independence used to test for statistical significance for categorical variables. T-test used for continuous variables. Agree = agree plus strongly agree, disagree = disagree plus strongly disagree. Medication = prescription medication or NRT.
24

Table 3 - Binary logistic regression model regressing intention to use cessation
medications on socio-demographic and smoking characteristics
Factor B Odds Ratio
95% (CI) confidence interval around OR
P-value
Lower UpperMale sex (reference = females) 0.16 1.18 0.87 1.60 0.30Age -0.01 0.99 0.98 1.00 0.13EducationNo Bachelor degree (ref)Bachelor degree or higher 0.44 1.55 1.12 2.20 0.01Nicotine dependence (HSI) 0.12 1.13 1.02 1.25 0.02Self-efficacyLow (ref)High 0.01 1.01 0.73 1.39 0.96Desire to quitNo (ref)Yes 0.48 1.62 0.95 2.77 0.08Prior use of medicationNo (ref)Yes 0.99 2.68 1.94 3.70 <0.001Agreement that smoking changes brain chemistryDisagree (ref)Agree 0.41 1.51 1.03 2.21 0.03Agreement that smoking is a brain diseaseDisagree (ref)Agree 0.43 1.54 1.11 2.13 0.01
N=930. Outcome variable: no intention to use medications=0, intend to use medications =1. Sex: Female = 0, Male =1. Nicotine dependence (HSI):0-6. Desire to quit: 0 = No desire, 1=Yes. Self-efficacy: 0=Low, 1=Moderate/High. Prior use of medication = ever use of NRT or prescription medications for smoking cessation. Agreement that smoking changes the chemistry of the brain = agree and strongly agree. Disagree that smoking changes the chemistry of the brain = disagree and strongly disagree. Agreement that smoking is a brain disease = agree and strongly agree. Disagree that smoking is a brain disease = disagree and strongly disagree.
25

Table 4 - Binary logistic regression model regressing level of self-efficacy on socio-demographic and smoking characteristics
Factor B Odds Ratio
95% (CI) confidence interval around OR
P-value
Lower Upper
Male sex (reference = females) -0.19 0.83 0.62 1.10 0.19Age -0.02 0.98 0.98 0.99 0.001EducationNo Bachelor degree (ref)Bachelor degree or higher 0.26 1.29 0.96 1.74 0.09Nicotine dependence (HSI) -0.23 0.79 0.72 0.87 <0.001Desire to quitNo (ref)Yes 0.99 2.70 1.57 4.64 <0.001Prior use of medicationNo (ref)Yes -0.24 0.79 0.59 1.06 0.11Agreement that smoking changes brain chemistryDisagree (ref)Agree -0.22 0.80 0.55 1.16 0.24Agreement that smoking is a brain diseaseDisagree (ref)Agree 0.53 1.70 1.26 2.30 <0.001
N=930. Self-efficacy: low = 0, moderate and high = 1. Sex: Female=0, Male = 1. Desire to quit: 0=No desire, 1= some desire, Prior use of medication = ever used NRT or prescription medications for smoking cessation. Agreement that smoking changes the chemistry of the brain = agree and strongly agree. Disagree that smoking changes the chemistry of the brain = disagree and strongly disagree. Agreement that smoking is a brain disease = agree and strongly agree. Disagree that smoking is a brain disease = disagree and strongly disagree.
26

Figure 1. Endorsement of brain-based explanations of smoking
Smoking ch
anges the ch
emistry
of the brain
Smoking ca
uses b
rain damage
Smoking is
a brain disease
Smoking is
a brain disorder
0102030405060708090
100
12.9 16.3
38.4 40.6
57.9 54.6
34.4 32.629.3 29.2 27.2 26.7
Disagree Agree Don’t know
27