Embed Size (px)
Citation preview

(©Johner/Phototonica)
C H A P T E R 7 C O N C E P T S
� More than half of the adults in the United States weigh more than is healthy.
� Keeping body weight healthy requires balancing calorie intake with calorie expenditure.
� The energy you obtain from food is used to keep you alive and moving and to process food.
� Energy consumed in excess of needs is stored as fat; this stored fat is used when you eat fewer calories than you burn.
� Genetics affect your propensity for storing excess body fat, but yourfood intake and activity level determine what you actually weigh.
� The goal of weight management is to reduce body fat to a healthylevel and maintain that level throughout life.
� Weight loss requires reducing food intake and increasing activity;maintaining weight loss requires a permanent change in eating and exercise habits.
� Eating disorders are psychological disorders that involve abnormaleating behaviors in response to an excessive concern with body sizeand weight.
Do overweight people eat more than thin people?
Is obesity inherited?
Can we stop the obesity epidemic?
Can an eating disorder be life-threatening?
Ju s t A Ta s t e

The Washington Post
Is Obesity a Disease?Insurance, Drug Access May Hinge on AnswerBy Rob Stein, Staff Writer
Monday, Nov. 10, 2003—The rising number ofAmericans who are seriously overweight has triggeredintense debate among scientists, advocacy groups, federalagencies, insurance companies and drug makers aboutwhether obesity should be declared a “disease,” a movethat could open up insurance coverage to millions whoneed treatment for weight problems and could speed the approval of new diet drugs.
To read the entire article, go to www.washingtonpost.com.
187
7Managing Your Weight
We Are in the Midst of an Obesity EpidemicExcess Body Fat Increases Disease RiskA Change in Lifestyle Can Help Stem the Obesity EpidemicBody Fat: How Much and Where Determinesthe RiskThere Are Many Techniques for Measuring Body CompositionBody Mass Index (BMI) Can Determine If Your Weight Is in the
Healthy RangeWhere Your Body Fat Is Located Affects Your Health RisksYour Genes Affect Your Body Size and CompositionObesity Genes Regulate Body Weight and FatnessDefective Obesity Genes May Promote Excess Fat StorageWhat You Weigh Is a Balance Between Your Genes
and Your LifestyleBalance What You Eat with What You DoWe Get Energy from the Carbohydrate, Fat, and Protein
in Our FoodWe Use Energy to Keep Us Alive and Moving and to Process
Our FoodEnergy Can Be Added to or Removed from Body StoresEERs Estimate the Number of Calories You Need for Energy
BalanceAmericans Are Eating More and Moving LessWe Eat More Today than We Used ToWe Move Less than We Used ToTo Be Healthy, Americans Need to Eat Less and Move MoreManaging Your Weight Means Keeping It HealthyAssessing Your Health Risks Determines If You Should
Lose WeightWeight Loss Involves Reducing Intake, Increasing Activity,
and Changing BehaviorWeight Gain Can Be Achieved by Increasing Intake
and Weight TrainingThere Are Many Diets; All Depend on Reducing IntakeSome Weight Loss Programs Use Exchanges and Points
to Help you Choose FoodsSome Programs Use Packaged Meals and Drinks, Limit
Portions, and Eliminate DecisionsLow-Fat Diets Are Not Necessarily Low in CaloriesLow-Carbohydrate Diets Vary in the Amount
of Carbohydrate AllowedDrugs and Surgery May Help WhenConventional Approaches FailAn Ideal Weight-Loss Drug Would Promote Long-Term Weight
Loss without Side EffectsWeight Loss Surgery Reduces the Amount of Food that Can
Be Eaten and AbsorbedEating Disorders Involve an AbnormalConcern with Body Weight and ShapeAnorexia Nervosa Is Characterized by Self-StarvationBulimia Nervosa Is Characterized by Cycles of Bingeing
and PurgingBinge Eating Disorder Is Characterized by Bingeing
without PurgingGenetic, Psychological, and Sociocultural Factors Increase
the Risk of Eating DisordersIdentifying Risks Can Help Prevent Eating Disorders
INTRODUCTION
ancer, diabetes, and atherosclerosis are diseases.How could weighing too much be a disease? Isn’tit simply the result of eating too much and exer-cising too little? Some feel obesity fits the defini-tion of a disease because it is a condition that
affects health in a negative way, but many argue that it isreally a risk factor, like smoking or high blood cholesterol,that predisposes to illness but is not itself a disease.Whether or not it is a disease, the health consequences ofbeing obese are serious. Carrying excess body fat increasesthe risk of other health problems, shortens life expectancy,and increases health care costs. About 400,000 people dieeach year in the United States from obesity-related dis-eases.1 Weight-related health problems are now second only
C

188 Chapter 7 Managing Your Weight
to tobacco use as the leading cause of preventable death in the United States.2 Esti-mates suggest that obesity costs about $99.2 billion—more than the health-care costsincurred by daily smokers and heavy drinkers.3 The more people who are obese, thehigher the nation’s health care expenses and the cost to society as a whole in terms oflost wages and productivity. To solve the obesity problem, we need to understand whyso many of us are overweight and what we can do to change this trend.
We Are in the Midst of an Obesity Epidemic
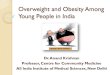
In 1960, 13.4% of adults were obese; in 1991, 23% were obese; and now, a decadelater, 31% are obese (Figure 7.1). The dramatic rise in the incidence of overweightand obesity that has occurred in the United States over the last few decades has ledmedical and public health officials to call the situation epidemic. Obesity-relatedhealth complications directly affect a greater proportion of the population than eitherthe Black Death, a plague that killed about half the population of Europe in the 14thcentury, or the influenza epidemic of 1918, which infected a fifth of the world’s popu-lation. Sixty-four percent of American adults are overweight, and about half of thesepeople carry enough extra fat to be considered obese.4 The obesity epidemic affectsboth men and women and spans every culture in the nation. Among African Ameri-cans, over 60% of men and 78% of women are overweight; among Mexican Ameri-cans, over 74% of men and 71% of women are overweight. The problem is notlimited to adults. Ten percent of children between 2 and 5 years of age are overweight,and 15% of children and teens 6 to 19 years of age are overweight.4
No Data<10%10%–14%15%–19%20%–24%≥25%
F I G U R E 7 . 1
These maps, which show the percentage of the adult populationthat was obese in each state in 1991 (top map) and 2002(bottom map), illustrate the dramatic rise in the incidence ofobesity. In 1991 there were no states that had rates of obesity thatexceeded 19%. By 2002 over half the states had rates of 20% orgreater. (Obesity Trends Among US Adults, BRFSS, 1991–2002,Centers for Disease Control)
Overweight A condition in which bodymass index is 25 to 29.9 kg/m2.�*
Obesity A condition characterized byexcess body fat. It is defined as a BodyMass Index of 30 kg/m2 or greater.
�*

Although the numbers are most striking for the United States, obesity is a growingconcern worldwide. In Canada between 1978 and 1992, obesity increased from 8 to12% among women and from 9 to 14% among men. In Europe, the incidence ofobesity has increased by 10 to 40% in the last 10 years.5 Obesity is even becoming aproblem in developing nations, where we typically think of undernutrition as themain concern. In Brazil between 1974 and 1997, obesity increased from 4.1 to13.9%.6 In Western Samoa, where a strong genetic predisposition toward obesity hadalready made obesity rates high, it increased still further between 1978 and 1991,from 39 to 58% among men and from 60 to 77% among women.7
Excess body fat increases disease riskYour body weight is the sum of the weight of your fat and your lean tissue or leanbody mass, which includes muscles, organs, and bones. A high body weight may bedue to large muscles or to excess body fat. If the extra weight is due to excess fat, thenit increases your risk of a host of chronic health problems, including high blood pres-sure, heart disease, high blood cholesterol, diabetes, stroke, gallbladder disease, arthri-tis, sleep disorders, respiratory problems, and cancers of the breast, uterus, prostate,and colon (Table 7.1). Obesity also increases the incidence and severity of infectiousdisease and has been linked to poor wound healing and surgical complications. It in-creases pregnancy risks for both the mother and child. The more overweight you are,the greater your health risks. The longer you are overweight, the greater the risks;
We Are in the Midst of an Obesity Epidemic 189
T A B L E 7 . 1Excess Weight Increases Health Risks
Cardiovascular disease is more likely when body weight is elevated
• Blood pressure increases as body weight increases
• Triglyceride levels increase as body weight increases
• LDL cholesterol increases as body weight increases
• HDL cholesterol falls as body weight increases
Type 2 diabetes risk increases with body weight
• Fasting blood sugar increases with increasing body weight
• Eighty percent of people with type 2 diabetes are obese
• Incidence increases as much as 30-fold with a BMI �35
Respiratory problems are more common in overweight people
• Sleep apnea is more common in overweight people
• The workload of muscles used for breathing increases
• Asthma is worse
Gallbladder disease is more common in overweight people
Osteoarthritis and degenerative joint disease increase with increasing weight
Menstrual irregularities are increased in overweight women
Cancer risk is higher in overweight people
• Obese women are at increased risk for cancers of the endometrium, breast,cervix, and ovaries
• Obese men are at increased risk for colorectal and prostate cancer
A sedentary lifestyle further increases risk
• Obese individuals who are inactive have higher risks of illness and death
• Inactivity increases the likelihood of developing diabetes and heart disease
For the first time in human history,the number of overweight people in the world rivals the number ofunderweight people.According to theWorldwatch Institute, a Washington,D.C.–based research organization,the number of underfed people hasdeclined slightly since 1980 to about 1.1 billion, while the numberof overweight people has surged to 1.1 billion.
Lean body mass Body massattributed to nonfat body components suchas bone, muscle, and internal organs. It isalso called fat-free mass.
�*

190 Chapter 7 Managing Your Weight
those who gain excess weight at a young age and remain overweight throughout lifehave the greatest health risks.
Carrying excess body fat also has psychological and social consequences. Our soci-ety puts a high value on physical appearance. Being thin is considered attractive andbeing fat is not. Those who do not conform to standards may pay a high psychologicaland social price. For example, overweight children are often teased and ostracized.This teasing about body weight is associated with low body satisfaction, low self-esteem, depression, social isolation, and thinking about and attempting suicide.8,9 Ifobese children grow into obese adolescents and adults, and most of them do, they mayexperience discrimination in college admissions and in the job market, in the work-place, and even on public transportation. Obese individuals of every age are morelikely to experience depression, a negative self-image, and feelings of inadequacy.10 Thephysical health consequences of obesity may not manifest themselves as disease for years,but the psychological and social problems experienced by the obese are felt every day.
A change in lifestyle can help stem the obesity epidemicReversing the obesity epidemic is a monumental but not insurmountable task. Obe-sity is caused by consuming more calories than you burn in activity over a long periodof time. Preventing obesity requires maintaining energy balance by matching intakewith output in the short term and in the long term. On a personal level, this meanspaying attention to which foods you choose, how much you eat, and what you do. Itinvolves choosing more nutrient-dense foods, consuming smaller portions than we areaccustomed to, and learning to incorporate exercise into our recreation and everydaylife. As a society we need to make this doable by transforming cities and communitiesinto places where it is easy to walk or bike to the store, school, or office; by manufac-turing healthier foods and packaging and serving them in more reasonable portionsizes; and by incorporating exercise into the school day and the work day. The onlyway to stop the obesity epidemic is to change the way we eat and the way we live, thefactors that caused average American body weight to increase in the first place. Thecauses of obesity and solutions to the problem for individuals and the population arediscussed more throughout the chapter.
Body Fat: How Much and Where Determines the Risk
Some body fat is essential for health; it cushions our organs, insulates us from changesin temperature and provides stored energy for times of need, but how much is toomuch? The answer depends on who you are. In general, women store more body fatthan men, so the level that is healthy for women is somewhat higher. A healthy levelof body fat for a young adult female is between 21 and 33% of total weight; for youngadult males, it is between 8 and 20%.11 With aging, lean body mass decreases andbody fat increases, even if body weight remains the same (Appendix B). Some of thischange may be prevented by physical activity.
There are many techniques for measuringbody compositionThe proportion of body weight that is fat compared to lean, or body composition, canbe measured by a variety of different techniques (Table 7.2). Some of these measure-ments can be made in a doctor’s office or at a health club; others require expensive, so-phisticated equipment and are most often used in research settings. Currently theeasiest and therefore most popular way to measure body composition is with a tech-nique that measures current flow through the body, called bioelectric impedanceanalysis. This involves holding a meter or standing on a scale that passes a painless,low-energy electrical current through the body; the rate of current flow can be used tocalculate the ratio of lean tissue to fat. Although this measurement is quick and easy
For information thatcan help individualsand communitiesmake positive changes
to improve their healthand the quality of life,
go to America On the Move atwww.americaonthemove.org
Energy balance A state in which bodyweight remains stable because the amountof energy consumed in the diet equals theamount expended.
�*
Bioelectric impedance analysisA technique for estimating body compositionthat measures current flow through the bodyand calculates resistance to flow.
�*

and available at many gyms and health clubs, it is not always accurate. To be accurate,measurements need to be made when your stomach and bladder are empty and youare normally hydrated. Measurements are less accurate after a meal or exercise session.Another inexpensive and non-invasive technique for estimating body composition ismeasuring skinfold thickness. The thickness of the skin and fat layer that lies over themuscles is measured at several locations on the arms, legs, and/or abdomen using acaliper (Figure 7.2). These measurements are accurate if they are done by someonetrained in the technique. A more precise method is underwater weighing. This in-volves weighing someone on land and under water to calculate body density and, sub-sequently, the amount of body fat. Although this method is accurate, it cannot be
Body Fat: How Much and Where Determines the Risk 191
Skinfold thickness A technique that measures the thickness of thesubcutaneous fat layer, which is used to estimate total body fat.
�*
T A B L E 7 . 2Measuring Body Composition
Method How Does It Work? Pros and Cons
Bioelectric Measures current flow through the body; Fast, easy, and inexpensive; inaccurate if body impedance since fat resists current flow, more fat water is not normal, such as after heavy exercise
means more resistance to flow
Skinfold Measures subcutaneous fat at several locations, Fast, easy, inexpensive; can be inaccurate thickness based on the assumption that subcutaneous if not performed by a trained observer
fat is representative of total body fat
Underwater Uses the difference between weight on land Accurate; can’t be used for children or ill orweighing and weight under water to calculate body frail adults
density; if you are more dense, you have less fat
Air displacement Measures air displacement in a closed chamber Accurate and easy for the subject; expensive, (Bod Pod) and uses this to calculate body density; if you not readily available
are more dense, you have less fat
Dilution Measures the concentration of a detectable Accurate; expensive, invasive, and maywater-soluble substance that has been involve the use of radioactive substancesingested or injected into the bloodstream and allowed to mix with the water throughout the body; the more it has been diluted by body water, the greater the amount of lean tissue
Dual-energy X-ray Uses low-energy X-rays for assessing A single investigation can accurately determine absorptiometry body composition total body mass, bone mineral mass, and percent (DEXA) body fat; expensive and it does not distinguish
between visceral and subcutaneous fat
Computerized Uses X-rays to visualize fat and lean tissue Useful for measuring the amount of visceral fat;tomography (CT) expensive
Magnetic Uses magnetic fields to create an Accurately measures visceral fat; expensiveresonance internal body imageimaging (MRI)
F I G U R E 7 . 2
Measurements of skinfold thickness at several locations can beused to estimate total body fat. The triceps skinfold shown here ismeasured at the midpoint of the back of the arm. (David Young-Wolff/PhotoEdit)

192 Chapter 7 Managing Your Weight
used for small children or frail adults, and it is less portable than skinfold or imped-ance measures. Other methods for measuring the amount of fat are listed in Table 7.2;most of these are more expensive and invasive.
Body Mass Index can determine if your weightis in the healthy rangeBody Mass Index (BMI) is an index of body weight in relation to height. Although BMIis not actually a measure of body fat, it is recommended as a better way to assess bodyfatness than measuring weight alone.12 BMI is calculated according to the followingequation:
BMI � weight in kg/(height in m)2
or
BMI � weight in pounds/(height in inches)2 � 703
For example, someone who is 6 feet (72 inches) tall and weighs 180 pounds has aBody Mass Index of 24.5 kg/m2 (180/722 � 703 � 24.5 kg/m2).
Figure 7.3 can be used to determine BMI and see if it is in the healthy range foradults. A healthy BMI for adults is between 18.5 and 24.9 kg/m2. In general, people
6’6”
Height*
6’5”
6’4”
6’3”
6’2”
6’1”
6’0”
5’11”
5’10”
5’9”
5’8”
5’7”
5’6”
5’5”
5’4”
5’3”
5’2”
5’1”
5’0”
4’11”
4’10”50 75 100 125 150 175 200 225 250 275
18.5
25 30
BMI (Body Mass Index)
Pounds† *Without shoes. † Without clothes.
Healthy Weight BMI from 18.5 up to 25 refers to healthy weight.
Overweight BMI from 25 up to 30 refers to overweight.
Obese BMI 30 or higher refers to obesity. Obese persons are also overweight.
F I G U R E 7 . 3
To determine your BMI range, locate your weight (in pounds) on the bottom scale and draw a vertical line up from this point. Locate your height (in feet and inches) onthe left scale and draw a horizontal line that extends into the graph. The point where these two lines meet indicates your BMI status. (Report of the Dietary AdvisoryCommittee on the Dietary Guidelines for Americans, 2000.)
Body Mass Index (BMI) An index ofweight in relation to height that is used tocompare body size with a standard.
�*

with a BMI in this range have the lowest health risks. Those with a BMI of less than18.5 kg/m2are considered underweight. Those whose BMI is between 25 and 29.9kg/m2are overweight, and those with a BMI of 30 kg/m2 or greater are obese.12 A BMIof 40 or over is classified as extreme or morbid obesity.
Being underweight leaves no body reserves Some people arenaturally lean, and this reduces their health risks. Research has suggested that being onthe low side of the body weight standard may reduce the risk of diabetes and otherchronic diseases and may even increase longevity (see chapter 13).13 But body fat isneeded for cushioning, as an insulator, and as a reserve for periods of illness. Peoplewith little energy reserves are at a disadvantage during a famine or when battling a dis-ease such as cancer that causes wasting and malnutrition.
When leanness is due to intentional or forced food restriction rather than a lifetimeof being lean, the health consequences could be severe. Substantial reductions in bodyweight due to starvation or eating disorders decrease the ability of the immune systemto fight disease, and very low body weight is associated with an increased risk of earlydeath.14 Too little body fat can cause problems at all stages of life. During adolescenceit can delay sexual development. During pregnancy, too little weight gain increases therisk that the baby will have health complications, and in the elderly too little body fatincreases the risk of malnutrition. Therefore, statistically a low body weight is associ-ated with an increased risk of early death.
A high BMI doesn’t always mean you have too much fatEven though BMI correlates well with body fat, it is not a perfect tool for evaluatingthe health risks associated with obesity. This is particularly true in athletes who havehighly developed muscles; their BMI may be high because they have an unusuallylarge amount of lean body mass. In these individuals BMI is high, but body fat andhence disease risk are low (Figure 7.4). BMI is also not suitable to evaluate weight inpregnant and lactating women, because a higher body weight is normal. It is also notaccurate in individuals who have lost muscle, such as many older adults. AlthoughBMI can be a useful tool, because of these limitations, other information is alsoneeded to determine nutritional health and fitness. Someone who is in the overweightcategory on the basis of BMI but consumes a healthy diet and exercises regularly maybe more fit and have a lower risk of chronic disease than someone with a BMI in thehealthy range who is sedentary and eats a poor diet.
Where your body fat is located affects your health risksWhere you store your body fat affects the health risks associated with having toomuch. Fat that is located under the skin, called subcutaneous fat, carries less risk thanfat that is deposited around the organs in the abdomen, called visceral fat. An increasein visceral fat is associated with a higher incidence of heart disease, high blood pres-sure, stroke, diabetes, and breast cancer. Generally, fat in the hips and lower body issubcutaneous, whereas fat deposited around the waist in the abdominal region is pri-marily visceral fat. Therefore, people who carry their excess fat around and above thewaist have more visceral fat. Those who carry their extra fat below the waist in thehips and thighs have more subcutaneous fat. In the popular literature, these bodytypes have been dubbed apples and pears, respectively (Figure 7.5).
Where your extra fat is deposited is determined primarily by your genes.15 Visceralfat storage is more common in men than women. African American women store lessvisceral fat than Caucasian women, even though they have a higher overall incidenceof obesity.16 Age and environment also influence where fat is stored.17 After menopause,visceral fat increases in women. Stress, tobacco use, and alcohol consumption predisposepeople to visceral fat deposition, whereas physical activity reduces it.
To determine if your body fat is a concern, you can measure your BMI and waistcircumference. For males, a BMI of 25 to 34.9 kg/m2 and a waist circumference greaterthan 40 inches indicates abdominal fat storage and is associated with increased risk. For
Body Fat: How Much and Where Determines the Risk 193
F I G U R E 7 . 4
Wrestler/actor Hulk Hogan, at 6 feet 8 inchestall and 275 pounds, has a BMI of 30.3,which falls into the category of obese.However, it is unlikely that his high BMI isdue to excess body fat or that it indicates anincreased risk of disease. (Duomo/Corbis)
Underweight A BMI of less than 18.5 kg/m2.�*
Extreme or morbid obesity A conditionin which BMI is greater than 40 kg/m2.�*
Subcutaneous fat Body fat that liesunder the skin.�*
Visceral fat Body fat that lies aroundinternal organs.�*

194 Chapter 7 Managing Your Weight
females in this BMI range, waist circumference of greater than 35 inches increases risks(Table 7.3). In order to monitor body weight and risk, the Dietary Guidelines forAmericans, 2000, recommends that all Americans keep track of their weight and theirwaists and avoid increases in both.
T A B L E 7 . 3Does Your Body Mass Index Increase Your Disease Risk?
Disease Riskb
Men: waist �40 in Men: waist �40 inWeight Class BMIa Women: waist �35 in Women: waist �35 in
Underweight �18.5Normal weight 18.5–24.9Overweight 25.0–29.9 Increased HighObesity (class I) 30.0–34.9 High Very highObesity (class II) 35.0–39.9 Very high Very highExtreme or morbid obesity (class III) �40 Extremely high Extremely high
aBMI � Body Mass Index: body weight (kg)/height squared (m2)bDisease risk for type 2 diabetes, hypertension, and cardiovascular disease relative to individuals with a normal weight andnormal waist circumference.
Data are from National Institutes of Health, National Heart, Lung, and Blood Institute. Clinical Guidelines on theIdentification, Evaluation, and Treatment of Overweight and Obesity in Adults. Executive Summary. Available online at:www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm.
Your Genes Affect Your Body Size and Composition
Are you shaped like your mother or your father? The information that determinesbody size and shape is contained in the genes you inherit from your parents. Some ofus inherit tall, slender bodies with long, thin bones. Others inherit stocky bodies withshort bones. Some people have broad hips and others broad shoulders (Figure 7.6).These characteristics don’t change much over time. Even body weight tends to remainat a particular level or set point for long periods despite changes in the amounts we eator exercise. When energy intake or activity level changes, the body compensates to
Genes A length of DNA that containsthe information needed to synthesize a protein.
�*
F I G U R E 7 . 5
(a): Overweight individuals with apple-shapedbody types deposit more fat in the abdominalregion and are at greater risk of developingheart disease and diabetes. (b): Overweightindividuals with pear-shaped body typesdeposit more fat in the hips and thighs,where it is primarily subcutaneous. (a, Corbis;b, © Tom McHugh/Photo Researchers) (b)(a)

prevent significant changes in weight or fat. This is why your weight remains fairlyconstant even when you increase your exercise level—perhaps on a weekend hikingtrip. It is also why most people gain back weight that they lose when they follow aweight-loss diet.
Obesity genes regulate body weight and fatnessGenes involved in regulating body fatness have been called obesity genes because anabnormality in one or more of these could result in obesity. More than 300 genes andregions of human chromosomes have been linked to obesity.18 These genes are respon-sible for the production of proteins that affect how much food you eat and how muchenergy you expend and regulate the way fat is stored in your body. The combined ef-fects of all these genes help to determine and regulate what you weigh and how muchfat you carry.
To regulate weight and fatness at a constant level, the body must be able to respondboth to changes in food intake that occur over a short time frame as well as to morelong-term changes in the amount of stored body fat. Signals related to food intake af-fect hunger or satiety over a short period of time—from meal to meal—whereas sig-nals from the adipose tissue trigger the brain to adjust both food intake and energyexpenditure for long-term regulation.
How much you eat at each meal is affected by internalsignals How do you know how much to eat for breakfast or when it is time to eatlunch? The physical sensations of hunger or satiety that determine how much you eatat each meal are triggered by signals from the gastrointestinal tract, levels of circulat-ing nutrients, and messages from the brain.19 Some signals are sent before we eat totell us we are hungry, some are sent while food is in the GI tract, and some occur oncenutrients are circulating in the bloodstream.
The simplest type of signal about how much food you have eaten comes from localnerves in the walls of the stomach and small intestine that sense the volume or pres-sure of food and send a message to your brain to either start or stop eating. Once youhave eaten, nutrients in the GI tract send information directly to the brain and triggerthe release of hormones that tell us to stop eating. Once nutrients have been absorbed,circulating levels of nutrients, including glucose, amino acids, ketones, and fatty acids,are monitored by the brain and may trigger signals to eat or not to eat. There aremany different signals that regulate different aspects of food intake. For instance, thehormone insulin is released by the pancreas in response to the intake of carbohydrate.Insulin allows glucose to be taken up by cells, thereby reducing circulating levels of
Your Genes Affect Your Body Size and Composition 195
F I G U R E 7 . 6
The genes we inherit from our parents areimportant determinants of our body size andshape. Some of us inherit long, lean bodiesand others a huskier build and a tendency toput on pounds. (left: Courtesy Lori Smolin;right: Bruce Ayres/Stone/Getty Images)
Obesity genes Genes that code forproteins involved in the regulation of foodintake, energy expenditure, or the depositionof body fat.When they are abnormal, theresult is abnormal amounts of body fat.
�*
Hunger The desire to acquire andconsume food that occurs in response to physiological signals.
�*
Satiety The feeling of fullness andsatisfaction, caused by food consumption,that eliminates the desire to eat.
�*
Adipose tissue Tissue composedprimarily of fat-storing cells.�*
For more information on healthy weightmanagement, go to
the Weight ControlInformation Network at
www.niddk.nih.gov/health/nutrit/htm/

196 Chapter 7 Managing Your Weight
glucose and increasing hunger. The hormone ghrelin may be the reason you typicallyfeel hungry around lunchtime, regardless of when and how much you had for break-fast. It is produced by the stomach and is believed to stimulate your desire to eat atusual meal times. Levels rise an hour or two before a meal and drop very low after ameal. Overproduction of ghrelin could contribute to obesity because levels have beenfound to increase in people who have lost weight, increasing their desire to eat more.20
Another hormone (peptide PYY) causes a reduction in appetite. It is released from thegastrointestinal tract after a meal and the amount released is proportional to the calo-ries in the meal.21 Some food intake signals even trigger the consumption of specificnutrients. For example, when levels of the neurotransmitter serotonin are low, we havebeen found to crave carbohydrate, but when it is high, we prefer protein.
Long-term regulation monitors the amount of body fatSometimes we don’t pay attention to whether or not we are full and make room fordessert anyway. If this happens often enough, it can cause an increase in body weightand fatness. To return fatness to a set level, the body must be able to monitor howmuch fat is present. Some of this information comes from hormones, such as insulinand leptin that are secreted in proportion to the amount of body fat.22 Levels of in-sulin in the blood increase with the amount of body fat. Insulin affects food intakeand body weight by sending appetite-suppressing signals to the brain and by affectingthe amount of leptin produced and secreted. Leptin is a hormone produced by theadipocytes. The amount of leptin produced is proportional to the size of adipocytes,so more leptin is released as fat stores grow. Leptin travels in the blood to the hypo-thalamus, where it binds to proteins called leptin receptors. When leptin levels arehigh, mechanisms that cause an increase in energy expenditure and a decrease in foodintake are stimulated, and pathways that promote food intake and, hence, weight gainare inhibited. When fat stores shrink, less leptin is released. Low leptin levels in thebrain allow pathways that decrease energy expenditure and increase food intake to be-come active. Thus, leptin acts like a thermostat or lipostat to keep body fatness fromchanging (Figure 7.7).
Adipocytes at set point size
Weightgain
Weightloss
Decreasedleptin
Increasedleptin
Decreasedenergy intakeand increased
energyexpenditure
Increasedenergy intakeand decreased
energyexpenditure
Hypothalamus
F I G U R E 7 . 7
Leptin helps maintain body fat at a preset level. When adipocytes gainfat, more leptin is released, triggering events that decrease food intakeand increase energy expenditure. When fat is lost, less leptin is released,causing an increase in food intake and a decrease in energy expenditure.
Ghrelin A hormone produced by thestomach that stimulates food intake.�*
Leptin A protein hormone producedby adipocytes that signals informationabout the amount of body fat.
�*
Adipocytes Fat-storing cells.�*Hypothalamus The region of the brain
that monitors and regulates conditions andactivities in the body, including food intakeand energy expenditure.
�*
Throughout human history, starvationhas threatened survival.Thus, overtime the human body has developedways to conserve body fat stores andprevent weight loss.Today more of usare concerned about eating too muchthan not enough. Unfortunately,preventing weight gain is not in ourevolutionary repertoire.We complainabout how hard it is to lose weight,but it is after all our ability to storeand preserve body fat that hasallowed us to survive the famines that have plagued us in the past.

Your set point for body weight may change over timeIf body weight is regulated at a particular set point, then why are so many of us get-ting fatter? It appears that the mechanisms that defend body weight are not absolute.Changes in physiological, psychological, and environmental circumstances do causethe level at which body weight is regulated to change, usually increasing it over time.For example, body weight increases in most adults between the ages of 30 and 60years, and after having a baby, most women return to a weight that is 1 to 2 poundshigher than their pre-pregnancy weight. This suggests that the mechanisms that de-fend against weight loss are stronger than those that prevent weight gain.23
Defective obesity genes may promote excessfat storageWhen a gene is defective, the protein it codes for is not made or is made incorrectly.When an obesity gene, such as the gene for leptin, is defective, the signals to decreasefood intake and/or increase energy expenditure are not received, and weight gain re-sults (Figure 7.8). A few cases of human obesity have been linked directly to defects inthe genes for leptin and leptin receptors.24 But mutations in single genes such as theseare not responsible for most human obesity. Rather, variations in many genes interactwith one another and affect metabolic rate, food intake, fat storage, and activity level.These in turn affect overall body shape and size.
Most overweight people do not have a slower metab-olism Many overweight people contend that they eat almost nothing and yet con-tinue to gain weight. This would imply that they expend less energy thannormal-weight individuals. One possible explanation for this is that overweight peopleuse their calories very efficiently, so they don’t need to eat as much to maintain theirbody weight. The results of studies comparing food intake and body weight have beenmixed. Part of the problem is that overweight individuals are more likely to under-report their food intake than their lean counterparts. Studies measuring energy expen-diture and body weight show that calorie use increases with increasing body weight;this suggests that overweight individuals need to eat more than their lean counterpartsto maintain their higher body weight.25 Although some individuals may need fewercalories than others to maintain weight, there is little evidence that an efficient metab-olism is a factor in the majority of cases of human obesity.
Overweight people may be less efficient at burning offextra calories Your body has mechanisms that are designed to keep your weightat a specific set point. When you overeat occasionally, your metabolism speeds up toburn the extra calories and prevent weight gain.26 Conversely, when you decrease yourfood intake, the rate at which your body uses calories slows. These changes in theamount of energy you expend in response to changes in circumstance, such as overeat-ing or undereating, changes in temperature, or trauma, are referred to as adaptivethermogenesis.
Several biochemical mechanisms have been proposed to explain adaptive thermo-genesis. One mechanism simply wastes energy by allowing opposing biochemical reac-tions to occur simultaneously. For example, a molecule is formed and then brokendown. The result is that calories are burned, but there is no net change in the numberof molecules in the body and, therefore, no storage of energy as fat. Another mecha-nism that may explain adaptive thermogenesis is that excess energy is dissipated byseparating or uncoupling the breakdown of energy-yielding nutrients from the pro-duction of ATP. When this occurs, energy is lost as heat. Animals have a specializedtype of adipose tissue called brown adipose tissue that is particularly good at wastingenergy as heat. It contains many more mitochondria (where aerobic metabolism oc-curs) than the more common white adipose tissue, and these mitochondria can be un-coupled to release the energy in food as heat. In rats, brown adipose tissue generatesheat to prevent weight gain during overfeeding and to provide warmth when the envi-ronmental temperature is low. Brown adipose tissue is unlikely to play a major role in
Your Genes Affect Your Body Size and Composition 197
F I G U R E 7 . 8
A mouse with a defect in the leptin gene may weigh three times as much as a normalmouse. Both of these mice have defectiveleptin genes, but the one on the right wastreated with leptin injections. (Courtesy JohnSholtis, Rockefeller University, New York/© 1995 Amgen, Inc.)
Overweight people must eatmore than lean individuals of the same age and heightbecause they have more tissueto fuel and maintain. This isfrustrating to dieters because,as they lose weight, the amountthey can eat without weightgain decreases.
Adaptive thermogenesis The changein energy expenditure induced by factorssuch as changes in ambient temperatureand food intake.
�*
Brown adipose tissue A type of fat tissue that has a greater number of mitochondria than the more commonwhite adipose tissue. It can waste energy by producing heat and is believed to beresponsible for some of the change inenergy expenditure in adaptivethermogenesis in rodents.
�*

198 Chapter 7 Managing Your Weight
preventing weight gain in humans because, except for newborns, people have only avery small amount of brown adipose tissue. What may be significant are other tissues,including muscle, white adipose tissue, lung, spleen, white blood cells, bone marrow,and stomach, that may also be able to increase energy output to regulate bodyweight.27
Overweight people may be less active Activity burns calories; thisis true whether the activity is planned exercise, daily activities like housework andwalking between classes, or small, involuntary actions like fidgeting and moving tomaintain your posture. How active you are is affected by your genes and your personalchoices. Studies that compared body fat to activity level have found that those withthe most body fat have the lowest levels of physical activity.28 This tells us that obesepeople are less active, but it does not mean the reduced physical activity is the cause ofthe obesity. Overweight people may be less active because it is more difficult to exer-cise or even to perform simple daily activities when carrying excess weight. However,differences in the amount of involuntary activity, such as fidgeting, may be one reasonsome people gain weight more easily. In a study that overfed normal-weight individu-als, there was a 10-fold variation in the amount of fat they gained. Some subjects wereable to increase energy expenditure to a greater extent and thus gained less fat. Abouttwo-thirds of the increase in energy expenditure that occurred with overfeeding wasfound to be due to an increase in involuntary exercise.29 Those who gained the leastweight had the greatest levels of involuntary exercise. It is still not known what mech-anisms control why some people respond to excess energy by becoming restless andfidgeting more, while others remain lethargic and gain weight.
What you weigh is a balance between your genes and your lifestyleObesity genes determine your propensity to carry extra fat. If one or both of your par-ents is obese, your risk of becoming obese is increased. Individuals with a family his-tory of obesity are two to three times more likely to be obese, and the risk increaseswith the magnitude of the obesity.30 But even if you inherit genes that predispose youto being overweight, your actual weight is determined by the balance between thegenes you inherit and the lifestyle choices you make. Someone with a genetic predis-position to obesity who carefully monitors their diet and exercises regularly may neverbe obese, but someone with no genetic tendency toward obesity who consumes ahigh-energy diet and gets little exercise may end up overweight. When genetically sus-ceptible individuals find themselves in an environment where food is appealing andplentiful and physical activity is easily avoided, obesity is a likely outcome. An exam-ple of human obesity that clearly demonstrates the interaction of a genetic predisposi-tion and an environment that is conducive to obesity is the Pima Indian populationliving in Arizona. More than 75% of the adults in this population are obese. Geneticanalysis has identified a number of genes that may be responsible for this group’s ten-dency to store more body fat.31 Their current lifestyle demands little physical activityand includes lots of high-calorie foods. The outcome is the strikingly high incidenceof obesity. In contrast, there is a genetically similar group of Pima Indians living inMexico, but they are farmers who work in the fields and consume the food theygrow.32 They still have higher rates of obesity than would be predicted from their dietand exercise patterns, suggesting genes that favor high body weight. However, they aresignificantly less obese than the Arizona Pima Indians.
Balance What You Eat with What You Do
How many calories do you need to maintain your weight? The answer depends on howmany calories you use. This varies depending on how big you are, how old you are,whether you are male or female, and how active you are. If you eat the same amount of
We inherit our body size andshape and the tendency tocarry extra pounds, but havingobese parents does not have to mean you too will be obese.The choices you make withrespect to how much you eatand how much you exerciseinteract with the genes youinherit to determine youractual body weight.
“If we could give every individualthe right amount of nourishmentand exercise, not too little and nottoo much, we would have found thesafest way to health.” Hippocratesc. 460–377 BC

energy—or number of calories—as you use, you will be in a state of energy balance andyour body weight will remain the same. This doesn’t necessarily mean you will be at ahealthy weight; it just means that your intake is balanced with your expenditure.
The energy needed to fuel your body comes from the food you eat and the energystored in your body. You use this energy to stay alive, process your food, move, andgrow. If you consume more energy than you expend, the excess energy will be storedfor later use, mostly as fat, and your weight will increase. If you expend more energythan you consume, stored energy will be used to fuel your body and you will loseweight.
We get energy from the carbohydrate, fat,and protein in our foodHow much energy you consume depends on how much and what you eat. The calo-ries in a specific food can be measured in a laboratory with an instrument called abomb calorimeter (Figure 7.9). Since calories are units of heat, the heat generated byburning the food can be measured in calories. Bomb calorimeters were used to deter-mine the amount of energy provided by carbohydrate, fat, protein, and alcohol: 4, 9,4, and 7 Calories per gram, respectively. Vitamins, minerals, and water, though essen-tial nutrients, do not provide energy to the body. If you know the composition of afood, you can use these numbers to calculate the calories it provides. For example, 5grams of sugar, which is almost pure carbohydrate, contains about 20 Calories (5 g �4 Cal/g). Five grams of corn oil, which is almost pure fat, contains about 45 Calories(5 g � 9 Cal/g). Most foods provide a combination of protein, carbohydrate, and fat.For instance, a taco with beef, cheese, sour cream, lettuce, and tomato contains about9 grams of protein, 16 grams of carbohydrate, and 13 grams of fat (Figure 7.10). Itsenergy content is therefore as follows:
(9 g � 4 Cal/g protein) � (16 g � 4 Cal/g carbohydrate) � (13 g � 9 Cal/g fat) � 217 Calories
You can also find out how many calories are in the foods you eat by looking this in-formation up in food composition tables and databases or by reading food labels. Ona food label this information can be found in the Nutrition Facts, which list the totalCalories in a serving of food (see Off the Label: How Many Calories in that Bowl, Box,
Balance What You Eat with What You Do 199
StirrerThermometer
Ignition wire
ater
Dried food sample
Bombchamber
Insulatinglayers
W F I G U R E 7 . 9
A bomb calorimeter consists of a chamber surrounded by a jacket of water.Food is dried, placed in the chamber, and burned. As the food combusts,heat is released, raising the temperature of the water. The increase in watertemperature can be used to calculate the amount of energy in the food on the basis of the fact that 1 Calorie is the amount of heat needed to increasethe temperature of 1 kilogram of water by 1 degree Celsius.
F I G U R E 7 . 1 0
The carbohydrate, protein, and fat in thesetacos contribute to their energy content.(PhotoDisc, Inc./Getty Images)
Bomb calorimeter An instrumentused to determine the energy content offood. It measures the heat energy releasedwhen a food is combusted.
�*

200 Chapter 7 Managing Your Weight
or Bar?). The energy content of foods in a diet can also be estimated from the Ex-change Lists shown in Table 7.4. For example, one starch exchange, whether a slice ofbread, one-half cup of cereal, or six saltines, provides about 80 Calories.
We use energy to keep us alive and movingand to process our foodThe total amount of energy used by the body each day is called total energy expendi-ture (TEE). It includes the energy needed to maintain basic bodily functions such asthe beating of your heart, as well as that needed to process food and to fuel physical
Off the Label: How Many Caloriesin that Bowl, Box, or Bar?
Are you looking for foods that will help you maintain ahealthy weight? Fresh fruits and vegetables are always agood choice. But for packaged foods, you need to check the label. Be sure you know what the terms mean.
The Nutrition Facts portion of a food label lists theCalories per serving, but it is also important to check theserving size. For instance, the standard serving of cookies isusually one ounce, or about three cookies. If you eat 12cookies, you are consuming four times the Calories listed on the label for a standard serving.
People tend to eat in units—one can of juice, one bottleof iced tea, one bag of potato chips—but food labels don’talways reflect the calorie count for that unit. For example,on a hot day a bottle of iced tea or fruit juice may be justwhat you need to cool off. The label says that a serving hasonly 100 Calories. Take a closer look. The serving size is 8ounces and the bottle is 20 ounces. So your cool gulp of icedtea may be giving you 250 Calories, mostly as added sugars.One of the recommendations of the FDA’s Working Groupon Obesity is to label as single servings those foods forwhich the entire contents of the package typically areconsumed at one time. For example, a 20-ounce bottle ofsoda would be labeled as containing 275 Calories per bottlerather than 110 Calories per 8 ounces.1 It has also beensuggested that the label design be changed so that thenumber of Calories is more prominent on the food label.
In evaluating the calorie content of a food, you may also see descriptors such as “low-calorie,” “calorie-free,”“reduced-calorie,” and “light.” These terms are defined sothey can be helpful in selecting foods. A food labeled “low-calorie” must have no more than 40 Calories perserving. A product labeled “calorie-free,” must containfewer than 5 Calories in a serving. “Reduced-calorie” or“fewer calories” on the label means the product contains atleast 25% fewer calories per serving than a reference food.“Light” or “lite” may be used to describe foods that containone-third fewer calories or half the fat of a comparableproduct. For example, the label on “lite” microwavepopcorn or “light” corn chips must state both the number
of Calories per serving and the fact that this is 30% fewerthan the regular product. The terms “light” and “lite” arealso used to describe food properties such as texture andcolor. For example, a label that says “light in texture” meansjust that; it does not mean that the calories are reduced. Theterm “light” may also appear without explanation on foodslike brown sugar, cream, or molasses, which havetraditionally included the term as part of their name.
Watch out for low-fat and low-carbohydrate products.These are often popular choices among dieters, but theyshould be chosen with care. Low-fat foods may containfewer calories than the full-fat version, but the differencemay be minimal. The FDA has not yet defined “low-carb” or“low-carbohydrate,” so these terms are at the discretion ofthe manufacturer. The bottom line on using food labels is toread and understand the entire label before assuming thatyou are making the best choice.
Reference1. U.S. Food and Drug Administration. FDA Proposes Action Plan to Confront
Nation’s Obesity Problem. Available online at www.fda.gov/oc/inititives/obesity/Accessed July 13, 2004.
Nutrition FactsNutrition FactsServing Size 3 cookies (32g)Servings Per Container About 11
Amount Per Serving
Calories 160 Calories from Fat 70
% Daily Value*
12%Saturated Fat 2.5g
Dietary Fiber 1gSugars 5g
3%7%4%0%
12%
Total Fat 8g
Cholesterol 0mg
Total Carbohydrate 21gSodium 105mg
Total energy expenditure (TEE) Thesum of basal energy expenditure, thermiceffect of food (TEF), and the energy usedin physical activity, regulation of bodytemperature, deposition of new tissue,and production of milk.
�*

activity. In individuals who are growing or pregnant, total energy expenditure also in-cludes the energy used to deposit new tissues. In women who are lactating, it includesthe energy used to produce milk. There is also a small amount of energy used to main-tain body temperature in a cold environment.
Most of our energy is used to maintain basic body func-tions About 60 to 75% of the body’s total energy expenditure is for basal metabo-lism. Basal metabolism includes all of the involuntary things your body does to keepyou alive such as breathing, circulating blood, regulating body temperature, synthesiz-ing tissues, removing waste products, and sending nerve signals. The rate at which en-ergy is used for these basic functions is called basal metabolic rate (BMR) and is oftenexpressed in Calories per hour. Basal needs include the energy necessary for essentialmetabolic reactions and life-sustaining functions but do not include the energyneeded for physical activity or for the digestion and absorption of food. BMR is mea-sured in the morning in a warm room before the subject rises and at least 12 hoursafter food intake or activity in order to minimize residual energy being used for activ-ity or processing food. Because of the difficulty of achieving these conditions, mea-sures are often made after about 5 to 6 hours without food or exercise. When determinedunder these conditions, the rate of energy expenditure is referred to as resting metabolicrate (RMR). RMR values are about 10 to 20% higher than BMR values.33
Basal needs are affected by how much you weigh and how much of your weight islean tissue. It increases with increasing body weight and thus is higher in heavier indi-viduals. It also rises with the amount of lean body mass; BMR is generally higher inmen than in women because men have greater lean body mass. BMR decreases withage, partly because of the decrease in lean body mass that usually occurs in older adults.
Basal needs can be altered by certain conditions. For instance, BMR is decreasedwhen calorie intake is consistently below needs.34 This drop in BMR decreases theamount of energy needed to maintain weight. It is a beneficial adaptation in someonewho is starving, but in someone who is trying to lose weight it is frustrating because it
Balance What You Eat with What You Do 201
T A B L E 7 . 4Exchange Lists Estimate the Calories in Your Diet
Exchange EnergyGroups/Lists Foods Serving Size (Cal)
Carbohydrate Group
Starch Rice, cereal, potatoes 1/2 cup 80Bread 1 slice
Fruit Apple, peach, pear 1 small 60Banana 1/2 mediumCanned fruit 1/2 cup
Milk Milk or yogurt 1 cupFat-free or low-fat 90–110Reduced-fat 120Whole 150
Vegetables Cooked vegetables 1/2 cup Varies
Raw vegetables 1 cup
Meat Group Meat 1 ounce
Very lean 35Lean 55Medium fat 75High fat 100
Fat Group Butter, oil, margarine 1 tsp 45
Someone whose total energyexpenditure is 2500 Cal/day mayuse 1500 to 1800 of this for basicbody functions.
Basal metabolism The energyexpended to maintain an awake restingbody.
�*
Basal metabolic rate (BMR) Therate of energy expenditure under restingconditions. It is measured after 12 hourswithout food or exercise.
�*
Resting metabolic rate (RMR) Therate of energy expenditure at rest. It ismeasured after 5 to 6 hours without foodor exercise.
�*

202 Chapter 7 Managing Your Weight
makes weight loss more difficult. Abnormal levels of thyroid hormones can also affectbasal needs. Individuals who overproduce these hormones require more energy, andthose who underproduce them require less energy. The fact that thyroid hormones,produced by the thyroid gland, affect energy expenditure is the reason obesity wasonce explained as a glandular problem. It is now known that obesity due to a lack ofthyroid hormones is rare. An elevation in body temperature, such as that which occurswith a fever, increases energy needs. It is estimated that for every 1 degree Fahrenheitabove normal body temperature, there is a 7% increase in BMR. This extra energy useexplains why people often lose weight when they have a fever.
Energy expended in physical activity varies greatly Physi-cal activity is the second major component of energy expenditure. In most people itaccounts for a smaller proportion of total energy expenditure than basal metabolism:about 15 to 30% of energy requirements in most cases. In some athletes and laborersit may account for a higher percentage of total energy expenditure. The energy ex-pended for activity is the one component of our total energy needs over which wehave control. It includes the energy we use for planned exercise as well as for perform-ing the activities of daily life, such as cooking, gardening, and walking the dog. Oftena person’s occupation has a great effect on their energy needs. For example, a construc-tion worker who spends 8 hours a day doing physical labor uses a great deal more en-ergy in his daily activities than does an office worker who spends most of his daysitting at a desk (Figure 7.11).
The amount of energy expended for various activities depends on how strenuousthe activity is and the length of time it is performed. Jogging for 30 minutes uses moreenergy than walking for 30 minutes, but if you walk for an hour you will probablyburn as many calories as you would jogging for 30 minutes. Energy expenditure is alsoaffected by body size. Because it takes more energy to move a heavier object, theamount of energy expended for many activities increases as body weight increases. Forexample, a 120-pound person uses about 190 Calories walking for an hour, but a 180-pound person will expend 290 Calories for the same walk. The energy costs of specificactivities are listed in Appendix J.
A small amount of energy is needed to digest, absorb,and use the nutrients in food Our energy comes from food, but wealso need energy to digest food and to absorb, metabolize, and store the nutrientsfrom this food. The energy used for these processes is called the thermic effect of food(TEF) or diet-induced thermogenesis. This increase in energy expenditure causes bodytemperature to rise slightly for several hours after eating. The energy required for TEFis estimated to be about 10% of energy intake but can vary, depending on theamounts and types of nutrients consumed. Because it takes energy to store nutrients,TEF increases with the size of the meal. The composition of meals also affects TEF. Ameal that is high in fat has a lower TEF than a meal high in carbohydrate or proteinbecause dietary fat can be efficiently stored as body fat. This difference in the energycost of storing energy means a diet high in fat may produce more body fat than a diethigh in carbohydrate.35
F I G U R E 7 . 1 1
The type of job you have has a huge impacton your daily energy expenditure. A carpentermay burn about 2800 Calories in an 8-hourwork day, whereas a computer technicianburns less than half of this. (a: Ryan McVay/PhotoDisc, Inc./Getty Images; b: RubberballProductions/Getty Images)
The average rider in the Tour deFrance bicycle race expends6,000–7,000 Calories each dayduring the 3-week, 2000-mile bikerace and may use over 10,000Calories on a day when the racegoes through the mountains.
Thermic effect of food (TEF) or diet-induced thermogenesis The energyrequired for the digestion, absorption,metabolism, and storage of food and the nutrients it provides. It is equal toapproximately 10% of daily energy intake.
�*
(b)(a)

Energy can be added to or removed from body storesWhen you eat a meal, the energy contained in that meal is used to fuel your body.When you consume more than you need the extra is stored. Your body stores a smallamount of energy as glycogen and a large amount as fat. Between meals or when youreduce your intake for a longer time, you still need energy, and some of it must comefrom glucose. To get this energy, our bodies rely on energy stores.
When your energy intake exceeds your needs, bodystores get bigger People typically eat three to six times during the day. Thesum of the intake for all of these meals and snacks must meet energy needs for weightto remain stable, but each time we eat we are likely to consume more energy than isneeded at that moment in time. The body must therefore decide which nutrients itwill use immediately and which it will store for later. This is determined on the basisof what the body needs, which nutrients can be stored, and how efficiently they canbe stored. When alcohol is consumed, it is quickly broken down and used for energy.This is because it is toxic and the body cannot store it. When protein is consumed, itsconstituent amino acids are used to synthesize body proteins and other nitrogen-con-taining molecules. Then, any excess amino acids are broken down and used for energy.When carbohydrate is consumed, it is used to supply blood glucose and to buildglycogen stores in the liver and in muscles. Once glycogen stores are full, the remain-ing carbohydrate is used for energy. When fat is consumed, it is used to meet immedi-ate energy needs and any remaining dietary fat is stored as triglycerides, primarily inadipose tissue. These cells grow as they accumulate more fat (Figure 7.12). The greaterthe number of adipocytes an individual has, the greater the ability to store fat. Mostadipocytes are formed between infancy and adolescence. In adulthood, only excessiveweight gain can cause the production of new fat cells.
Most of the fat that is stored in the body comes from fat consumed in the diet (Fig-ure 7.13). This is because excess dietary fat is easy to store as body fat. Dietary fat canbe transported directly to the adipose tissue, where the enzyme lipoprotein lipasebreaks the triglycerides into fatty acids and glycerol, which can then enter theadipocytes, where they are reassembled into triglycerides for storage. The body is capa-ble of converting excess carbohydrate and amino acids into fat for storage. However,under normal dietary circumstances, this doesn’t occur because it involves numerousmetabolic reactions and the body must expend energy in the conversion process.36
When your energy intake does not meet your needs,body stores are used When your diet doesn’t provide enough energy, youmust use your body stores. Between meals, you break down liver glycogen in order tomaintain a steady supply of blood glucose. But liver glycogen is limited. When you
Balance What You Eat with What You Do 203
RememberAs discussed in Chapter 5, the ability ofthe body to store excess triglycerides istheoretically limitless. Adipocytes canincrease in weight by about 50 times, andnew fat cells can be made when existingcells reach their maximum size.
*
ENERGY
Carbohydrate
Glycogen
When you eatmore thanyou need
When youhaven’t eatenin a while
Adipose tissue
Glucose
Bodyprotein
Fatty acids
Fat Protein
F I G U R E 7 . 1 2
Adipocytes contain droplets of fat surroundedby other cell components. As body fat isgained, the size of the fat droplets increases.(Ed Reschke/Peter Arnold, Inc.)
F I G U R E 7 . 1 3
When you eat more than you need at that time, some energy is put intobody stores. Dietary fat is easily stored as body fat. Carbohydrate can bestored as glycogen or converted into fat and excess energy as protein canalso be converted into body fat. When you haven’t eaten in a while, youretrieve energy from these stores. A small amount of body protein is alsobroken down to make glucose. If you don’t eat for a long time, there areother metabolic changes that occur to ensure your energy needs are met.

204 Chapter 7 Managing Your Weight
don’t eat for longer periods of time, your body must find another source of glucose.This source is small amounts of body protein, primarily muscle protein, which arebroken down to yield amino acids that can then be used to make glucose. The break-down of protein to provide energy and glucose results in the loss of functional bodyproteins.
Energy for tissues that don’t require glucose is provided by the breakdown of storedfat (see Figure 7.13). If the supply of glucose is limited, such as during starvation, fattyacids delivered to the liver cannot be completely broken down, so ketones are pro-duced (see Chapter 4). Ketones can be used as an energy source by many tissues. Afterabout 3 days of starvation, even the brain adapts to meet some of its energy needsfrom ketones (see Chapter 5). This reduces the amount of glucose needed and there-fore slows the rate of protein breakdown.
When our meals are a few hours apart, some glycogen and fat stores are used be-tween meals and then replaced by the energy consumed in the next meal so that thereis no net change in the amount of stored energy. However, if energy stores are not re-plenished, the amount of stored energy, mostly fat, will be reduced and weight will de-crease. The amount of weight lost depends on the degree of energy deficit and thelength of time over which it occurs. It is estimated that an energy deficit of about3500 Calories results in the loss of a pound of fat.
EERs estimate the number of calories you need for energy balanceThe current recommendations for energy intake in the United States are the esti-mated energy requirements (EERs).33 Equations to calculate EERs were developed bymeasuring energy expenditure in individuals at various levels of activity. EER equa-tions are available for healthy people of defined age, gender, weight, height, life stage,and level of physical activity. Your EER is the estimated number of calories you needto maintain your current weight.
Energy expenditure can be measured directly or indi-rectly The amount of energy used by the body can be measured in a number ofways. One method measures the amount of heat released by the body. This is calleddirect calorimetry and is based on the fact that the amount of heat your body pro-duces is proportional to the amount of energy used. Direct calorimetry is an accuratemethod for measuring energy expenditure, but it is expensive and impractical becauseit requires that the individual being assessed remain in an insulated chamber to mea-sure heat release throughout the evaluation. Indirect calorimetry determines energy ex-penditure by measuring the amount of oxygen used and carbon dioxide produced bythe body. Energy use can be calculated from these values because the burning of car-bohydrate, fat, and protein in aerobic metabolism uses oxygen and produces carbondioxide. Although the equipment needed for indirect calorimetry is much more com-pact than the insulated chamber needed for direct calorimetry, it is still too cumber-some for long-term use in free-living individuals (Figure 7.14). The least invasivemethod of determining energy expenditure is the doubly labeled water method. Thismethod involves ingesting or injecting water labeled with isotopes of oxygen and hy-drogen. Energy use is estimated by measuring the rate at which labeled oxygen and la-beled hydrogen disappear from body water. The doubly labeled water technique doesnot require the individual to carry any equipment and can be used to measure expen-diture in free-living subjects for periods up to 2 weeks. Measurements made usingdoubly labeled water are the basis of current EER equations.
To calculate your EER, start by estimating your level ofactivity In order to calculate how many calories you need using the EER equa-tions, first you have to estimate your activity level. The DRIs have defined four physi-cal activity levels: sedentary, low active, active, and very active.33 A “sedentary” persondoes not participate in any activity beyond that required for daily independent living,such as housework, homework, yard work, and gardening. To be in the “low active”
F I G U R E 7 . 1 4
Measuring expired gases by having the subjectbreathe under a hood can be used to assessBMR, but this method is too cumbersome tobe used to measure the energy costs of dailyactivity. (St. Bartholomew’s Hospital/CustomMedical Stock Photo)
Estimated Energy Requirement (EER)The amount of energy calculated to maintainbody weight based on age, gender, size,and activity level.
�*
Direct calorimetry A method ofdetermining energy use that measures theamount of heat produced by the body.
�*
Indirect calorimetry A method ofestimating energy use that measures theamount of carbon dioxide expired.
�*
Doubly labeled water methodA technique for determining energyexpenditure based on measuring thedistribution of isotopes of hydrogen andoxygen in body fluids after administrationof a defined amount of water labeled withboth isotopes.
�*
Isotope An alternative form of anelement that has a different atomic mass,which may or may not be radioactive.
�*

category, an adult weighing 70 kg would need to expend an amount of energy equiva-lent to walking 2.2 miles at a rate of 3 to 4 miles per hour in addition to the activitiesof daily living. To be “active,” the same person would need to perform daily exerciseequivalent to walking 7 miles at a rate of 3 to 4 miles per hour, and to be “very ac-tive,” an individual would need to perform the equivalent of walking 17 miles at thisrate in addition to the activities of daily living. In order to maintain a healthy weightand reduce the risk of chronic disease, physical activity at the “active” level is recom-mended. Not all of us have time to walk for an hour and three quarters, but if we en-gage in more intense activity we will expend the same number of calories in less time.
You can estimate your activity level by keeping a daily log of your activities andrecording the amount of time spent in each. Activities can then be categorized as ac-tivities of daily living, moderate, or vigorous (Table 7.5). You can find your activitylevel by estimating the time you spend in each category of activity. As seen in Table7.6, each physical activity level is assigned a numerical physical activity (PA) value thatcan then be used in the EER calculation. It is important to carefully estimate activitylevel because it has a significant effect on calorie needs. For example, a 22-year-oldman who is 6 feet tall and weighs 185 pounds needs about 2770 Cal/day if he is at asedentary activity level. If he increases his activity to “active,” the level recommendedby the DRIs, his EER increases to 3350 Cal/day.
Your gender, age, size, and life stage affect your calorieneeds Your calorie needs are affected by your age, gender, height, weight, and lifestage (Table 7.7 or inside cover). To determine your EER, enter your age in years,height in meters, weight in kilograms, and PA value into the equation that is appro-priate for your age and gender. The EER values for infants, children, and adolescentsinclude the energy used to deposit tissues associated with growth. Beginning at age 3years, there are separate EER equations for boys and girls because of differences ingrowth and physical activity. The EER for pregnancy is determined as the sum of the
Balance What You Eat with What You Do 205
T A B L E 7 . 5How Active Are You?
Activities of Daily Living* Moderate Activities† Vigorous Activities‡
Gardening (no lifting) Calisthenics (light, no weights) Aerobics (moderate to heavy)
Watering plants Cycling (leisurely, 6–7 mph) Ballet
Raking leaves Golf (without cart) Climbing (hills or mountains)
Mowing the lawn Swimming (slow) Cycling (moderate or higher, greater than 10 mph)
Household tasks Walking (3 mph, 20 min/mile) Dancing (square dancing or fast ballroom)
Mopping Walking (4 mph, 15 min/mile) Ice skating
Vacuuming Jogging (12 min/mile or faster)
Walking from the house to car Roller skatingor bus Rope-jumpingLoading/unloading the car Skiing (water, downhill, or cross-country)Walking the dog Squash
Swimming (moderate to fast)
Tennis
Walking (5 mph, or 12 min/mile)
*It is assumed that we spend about 2.5 hours per day in these types of activities.†Activities that expend about 250 to 350 Cal/hour for a 150-lb individual.‡Activities that expend more than 350 Cal/hour for a 150-lb individual.
Physical activity (PA) value A numericvalue associated with activity level that is a variable in the EER equation used to calculate energy needs.
�*
To have your EER calculatedautomatically,
go to the CalorieCalculator at
www.cspinet.org/nah/09_03/calorie_calc.html/

206 Chapter 7 Managing Your Weight
T A B L E 7 . 6Find Your Physical Activity (PA) Value
PA Value
3–18 Years Old �19 Years Old
Physical Activity Level Boys Girls Men Women
Sedentary: Engages in only the activities of daily living and no moderate 1.00 1.00 1.00 1.00or vigorous activities
Low active: Engages in daily activity equivalent to at least 30 minutes 1.13 1.16 1.11 1.12of moderate activity and a minimum of 15 to 30 minutes of vigorous activity, depending on the intensity of the activity
Active: Engages in at least 60 minutes of moderate activities or a 1.26 1.31 1.25 1.27minimum of 30 to 60 minutes of vigorous activity, depending on the intensity of the activity
Very active: Engages in at least 2.5 hours of moderate activity or a 1.42 1.56 1.48 1.45minimum of 1 to 1.75 hours of vigorous activity, depending on the intensity of the activity
T A B L E 7 . 7How Many Calories Do You Need?
To determine estimated energy requirement (EER):
• Find your weight in kilograms (kg) and your height in meters (m)
Weight in kilograms � weight in pounds � 2.2 lbs/kg
Height in meters � height in inches � 0.0254 inches/m
For example: 160 pounds � 2.2 lbs/kg � 72.7 kg
5 feet 9 inches � 69 inches � 0.0254 in/m � 1.75 m
• Estimate the amount of physical activity you get per day and use Table 7.6 to find the PA value for someone of yourage, gender, and activity level. For example, if you are a 19-year-old male who performs 40 minutes of vigorousactivity a day, you are in the active category and have a PA of 1.25.
• Choose the appropriate EER prediction equation below and calculate your EER. For example, if you are an active19-year-old male:
EER � 662 � (9.53 � age in yr) � PA [(15.91 � weight in kg) � (539.6 � height in m)]
Where age � 19 yr, weight � 72.7 kg, height � 1.75 m, active PA � 1.25
EER � 662 � (9.53 � 19) � 1.25 ([15.91 � 72.7] � [539.6 � 1.75]) � 3107 Cal/day
Gender Age (yr) EER Prediction Equation*
Boys, 9–18 EER � 88.5 � (61.9 � age in yr) � PA [(26.7 � weight in kg) � (903 � height in m)] � 25
Girls, 9–18 EER � 135.3 � (30.8 � age in yr) � PA [(10.0 � weight in kg) � (934 � height in m)] � 25
Men, �19 EER � 662 � (9.53 � age in yr) � PA [(15.91 � weight in kg) � (539.6 � height in m)]
Women, �19 EER � 354 � (6.91 � age in yr) � PA [(9.36 � weight in kg) � (726 � height in m)]
*These equations are appropriate for determining EERs for normal-weight individuals. Equations that predict the amount ofenergy needed for weight maintenance in overweight and obese individuals are also available (Appendix G).

total energy expenditure of a nonpregnant woman plus the energy needed to maintainpregnancy and deposit maternal and fetal tissue. During lactation, EER is the sum ofthe total energy expenditure of nonlactating women and the energy in the milk pro-duced, minus the energy mobilized from maternal tissue stores.
Americans Are Eating More and Moving Less 207
P I E C E I T T O G E T H E R
Balancing Intake and ExpenditureApril is unhappy about the 10 pounds she gained during herfreshman year at college. Her parents are both obese, and she is worried that she too will become obese. She is 5 feet 4 inchestall, is 23 years old, and weighs 140 pounds. She would like to weigh 130 pounds.
In analyzing why she gained weight, April realizes that, withher busy college schedule, she gets less exercise than she usedto and often eats candy bars from the vending machinewhile studying late at night. By recording and analyzing herfood intake for 3 days, she determines that she eats about2450 Calories per day. To see how this compares to herrecommended intake, she calculates her EER. She estimatesthat she is in the “low active” activity category.
WHAT IS HER EER?
Your answer (Hint: Use the EER equation in Table 7.7 and the low-active PA value in Table 7.6 for a 23-year-oldwoman.):
HOW DOES HER EER COMPARE TO HER INTAKE?
Your answer:
April realizes she needs to either increase her output ordecrease her intake in order to lose weight. She decides tostart by increasing her activity level. She loves to play tennisand therefore plans to add 2 hours of tennis a day. Tennis isa vigorous activity, so playing 2 hours per day would moveher into the “very active” category.
�
�
WHAT WOULD HER EER BE WITH THE ADDED2 HOURS OF TENNIS PER DAY?
Your answer:
IS THIS A REASONABLE PLAN?
Although April loves tennis and this level of activity wouldallow her to lose weight, she probably won’t play for 2 hourseach day. A more reasonable approach might be to plan on playing tennis 3 days a week while also adding somemoderate activity such as riding her bike to and from class,using the stairs instead of the elevator, and going dancingsome evenings with friends. She is more likely to keep upthis schedule, and this amount of activity will put her in the “active” category, which is the level recommended tomaintain health.
April also wants to change her diet. She decides to startby replacing her high-calorie candy bars with lower-caloriechoices such as fruits.
IF APRIL LOSES 10 POUNDS BUT KEEPS HER ACTIVITY INTHE ACTIVE CATEGORY, HOW WILL IT AFFECT HER EER?
Your answer:
�
�
�
Americans Are Eating More and Moving Less
Although genes are an important determinant of what we weigh, they are not the rea-son more Americans are obese today than 30 years ago. The genetic mix in the popu-lation cannot have changed that fast. What has changed is the environmentalinfluences on what we eat, how much we eat, and how much exercise we get. Simply

208 Chapter 7 Managing Your Weight
put, more Americans are overweight than ever before because we are eating more andburning fewer calories than we did 30 years ago. Food is plentiful and continuouslyavailable, and little activity is required in our daily lives.37
We eat more today than we used toPart of the reason Americans weigh more than they did 30 years ago is that they areeating more.38 Palatable, affordable food is readily available to the majority of the pop-ulation 24 hours a day in supermarkets, fast-food restaurants, and convenience marts.Looking at the food supply, both the numbers of foods and the portions served haveincreased since the 1970s. Does having more food available make you eat more? Toanswer this, think about why you stop for an ice cream cone. Is it because you arehungry or because the ice cream looks good? How do you know when to stop eating?Is it when your plate is empty or when your stomach is full? Your appetite may betriggered or inhibited by the sight, taste, and smell of food, as well as the time of day,your emotions, and social conventions. It is usually appetite and not hunger thatmakes us stop for that ice cream cone on the way home, so having more temptingchoices available does make you eat more.
In addition to having more enticing choices available, we consume more caloriestoday because our food portions have increased. Did your mother tell you to cleanyour plate? Studies of how much people eat have shown that the more that is put infront of us, the more we eat.39 Therefore, bigger portions mean more calories are con-sumed. We tend to eat in units, such as one cookie, one sandwich, or one bag ofchips, regardless of the size of the unit. So, if we are presented with larger units, westill eat the whole thing. One of the best examples of the effect of portion size on ac-tual intake is the servings at fast-food restaurants; the meal of a hamburger and frenchfries served today is two to five times bigger than it was when fast food first appeared(Figure 7.15). You probably wouldn’t order an extra hamburger, but you will finish theone you order even if it is twice as big.
Lifestyle changes that have occurred over the last few decades have also affectedhow many calories Americans eat. The increasing number of single-parent householdsand households with two working parents means that the time families have to pre-pare meals at home is limited. As a result prepackaged, convenience, and fast foodhave become mainstays. These foods are typically higher in fat and energy than whatyou would have prepared at home.
We move less than we used toNot only are we eating more, but we are also exercising less. Along with the increase inenergy intake, there has been a decrease in the amount of energy used in the activities ofdaily life, whether working or playing. Fewer American adults today work in jobs thatrequire physical labor. People drive to work in automobiles, rather than walking or bik-
30 years ago
Soft drinks French fries Cheeseburgers
62% 57% 24%
Today
Percent increase in portion size
F I G U R E 7 . 1 5
The increase in portion sizes that has occurredsince the 1970’s is clearly illustrated by theincrease in the size of a fast-food meal. (Adaptedfrom Nielsen, S.J., and Popkin, B.M. Patterns andtrends in food portion sizes, 1977–1998. JAMA289:450–453, 2003; photo: Andy Washnik)
Appetite The desire to consumespecific foods that is independent of hunger.�*
Dr.Yvon C. Chagnon, who studiesobesity genes, says that most obesitytoday is the result of “a bad geneticpackage made worse by our way oflife.” She notes, “When you have easyaccess to food and don’t burn whatyou eat, obesity results.” (GenomeNews Network, June 13, 2003;www.genomenewsnetwork.org/articles/06_03/obesity.shtml)

ing; they take elevators instead of the stairs; they use vacuum cleaners rather thanbrooms; and they cut the lawn with riding rather than push mowers. All of these simplechanges reduce the amount of energy expended to perform the tasks of daily living. Atypical office worker today walks only about 3000 to 5000 steps in their daily activities.In contrast, in the Amish community—where driving automobiles and using electricalappliances and other modern conveniences are not allowed—a typical adult takes14,000 to 18,000 steps a day. The overall incidence of obesity in the group is only 4%.40
In addition to less active jobs, busy schedules and long days at work and commut-ing make people feel they have no time for active recreation. Instead, at the end of theday, Americans sit in front of televisions, electronic games, and computers—all seden-tary ways to spend leisure time.
The reduction in physical activity is not restricted to adults. American children arealso less active. Many schools have reduced or even eliminated physical education pro-grams in trying to find more time for academics. Social conditions that have increasedcrime have forced children to stay inside after school. In the 1960’s kids spent their after-school hours outdoors with bikes, balls, and friends. Today they are more likely to spendit indoors with video games and computers. The end result is that they burn fewer calo-ries and have more opportunities to consume more, and consequently they gain weight.
To be healthy, Americans need to eat less and move moreAccording to the U.S. Surgeon General’s Call to Action to Prevent and Decrease Over-weight and Obesity, to improve our health we need to eat less and/or move more.1 Thisreport recommends a number of strategies aimed at improving food choices and in-creasing physical activity. It suggests that the public and food manufacturers work to-gether to offer smaller portion sizes so that we eat less. It suggests that communitieswork to provide recreational facilities for people of all ages and employers offer moreopportunities for physical activity at the workplace. It also emphasizes that thesechanges be implemented among America’s youth by improving the diets and increas-ing the activity of children and young adults. The changes recommended are not largebut need to be consistent in order to arrest the increase in obesity in the population. Ithas been estimated that a population-wide shift in energy balance of only 100 Caloriesa day, the equivalent of walking a mile or cutting out a scoop of ice cream, would pre-vent further weight gain in 90% of the population.41
Managing Your Weight Means Keeping It Healthy 209
Managing Your Weight Means Keeping It Healthy
Are you one of the 64% of Americans who are overweight? Do you want to avoid be-coming one? Managing your weight is a lifestyle choice. It involves maintaining a bal-ance of intake and exercise that will bring your weight in the healthy range and keep itthere. For some people weight management may mean avoiding weight gain as theyage by making healthy food choices, controlling portion size, and maintaining an ac-tive lifestyle. For others, it may mean developing a meal and exercise plan that willallow their weight to decrease (or increase). The goal is getting to a healthy weight andstaying there (Figure 7.16).
Assessing your health risks determines if you should lose weightDo you need to lose weight? Answering this question starts with an evaluation of yourcurrent weight and weight history along with a review of your medical history. Startby determining your BMI. In general, a BMI above the healthy range means thatweight loss would improve long-term health, but this is not always the case. Somepeople with high BMIs, such as weight lifters, may have a greater muscle mass but notmore body fat than is recommended. If, in addition to a high BMI, body fat is ele-vated or waist circumference is increased, weight loss is usually recommended. Age is
Obesity is a preventable diseaseif lifestyle changes are made toincrease activity and decreasefood intake before the effects of energy imbalance cause too much weight gain. Thisapproach can stop weight gainin individuals and can helpstop the obesity epidemic fromexpanding further.
Aim for a healthy weight
F I G U R E 7 . 1 6
The Dietary Guidelines for Americans, 2000,advises us to “Aim for a healthy weight.”

210 Chapter 7 Managing Your Weight
also important because extra weight may be less of a health risk at certain times in life.For example, in a teen who is still growing, an increase in body weight may be fol-lowed by a growth spurt that puts BMI back in the healthy range. In older adults afew extra pounds may provide a reserve that is beneficial in the event of a long-termillness.
A key factor in whether or not weight loss is recommended is the presence of dis-eases and abnormalities associated with excess body fat (see Table 7.1). For example,blood pressure, blood sugar, and blood cholesterol levels all increase with body weight,and with them the risk of heart disease and diabetes. A person whose BMI is above thehealthy range and has two or more of these conditions will probably benefit fromweight loss. A family history of these conditions is also a consideration in determiningwhether or not weight loss is recommended. On the basis of these criteria, not every-one who is a few pounds over ideal body weight needs to lose the extra weight. Peoplewho have a BMI in the overweight range (25–29.9 kg/m2) but have none of thehealth conditions associated with excess body fat and have a healthy lifestyle may notbenefit from weight loss. For example, a person with a BMI of 28 kg/m2 whose bloodpressure and cholesterol are normal and who exercises regularly would not reduce hisor her health risks by losing weight. For persons such as this, weight management maymean simply preventing further weight gain. For others, this risk assessment may indi-cate that body weight is a health risk and that a weight loss plan should be developed.For example, weight loss would be recommended for a person with a BMI of 28kg/m2 who has high blood pressure and high blood cholesterol levels.
Even losing a small amount of weight can decrease dis-ease risk The medical goal for weight loss in an overweight person is to reducethe health risks associated with being overweight. For most people, a loss of 5 to 15%of body weight will significantly reduce disease risk.42 The initial goal of weight lossshould therefore be to reduce body weight by about 10% over a period of about 6months.43 After this initial weight loss, risks can be reassessed to determine if addi-tional weight loss would be beneficial. A slow loss of 10% of body weight is consid-ered achievable for most people and is easier to maintain than larger weight losses.Most people who lose large amounts of weight or lose weight rapidly eventually regainall that they have lost. Repeated cycles of weight loss and regain, referred to as weightcycling or yo-yo dieting, increase the proportion of body fat with each successiveweight regain and cause a decrease in BMR, making subsequent weight loss more dif-ficult (Figure 7.17).44 Even if an individual has lost and regained weight in the past,weight loss is recommended if they are still obese or overweight and have two or moreconditions that increase the health risks associated with obesity.42
New determinationto diet
DIE
TING
OVE
RE
ATIN
G
DIETIN
G
Shame
Guilt
Rapid weight gain
Return to formereating habits
Food cravings
Decrease in BMR
Rapid weight loss
Fatigue and decrease in activity
Bodyweight
F I G U R E 7 . 1 7
Weight cycling, commonly known as yo-yo dieting, is the repeated lossand subsequent regain of body weight.
Weight cycling or yo-yo dieting Thecycle of repeatedly losing and regainingweight.
�*
Twenty-ounce soda bottles havereplaced the old 12-ounce cans inmost vending machines. Every timeyou drink a bottle you are consuming100 more calories than you did withthe 12-ounce can.

Weight loss is not recommended at all life stages Obesity isa growing problem among children (Figure 7.18). However, strict weight-loss diets aregenerally not recommended for children or adolescents, because a severe reduction inintake can interfere with growth. A better approach is to encourage physical activity,along with a moderate energy-intake restriction, allowing the child to grow in heightwith little additional weight gain (see Chapter 13).
Weight-loss diets are also not recommended during pregnancy. Even women whoare overweight at the start of pregnancy should gain at a slow, steady rate to accumu-late about 15 to 25 pounds over the course of pregnancy. A weight-loss program canbe initiated after the baby is born and the mother has recovered (see Chapter 12).Slow weight loss is appropriate during lactation, but rapid weight loss can decreasemilk production.
For older adults, the risks associated with excess body fat are lower than they are foryounger adults.45 However, the decision to treat obesity should not be based on agealone. Weight loss can enhance day-to-day functioning and improve cardiovasculardisease risk factors at all ages.43 Older people tend to lose muscle and replace it withfat; therefore, weight-training activities are an important part of a weight-loss programfor the elderly (see Chapter 13).
Weight loss involves reducing intake,increasing activity, and changing behaviorLosing weight requires tipping the energy balance scale: eating less or exercising more(Figure 7.19). A pound of body fat provides about 3500 Calories. Therefore, to lose apound of fat, you need to decrease your intake or increase your expenditure by thisamount. To lose a pound in a week, you would need to tip your energy balance by
Managing Your Weight Means Keeping It Healthy 211
1963–70
Age in years
Prevalence of overweight amongchildren and adolescents ages 6-19 years
12-196-11
1971–74 1976–80
(year)
1988–94 1999–000%
5%
10%
15%
20%
F I G U R E 7 . 1 8
The prevalence of obesity among children and adolescents in the United States hasincreased over the last 30 years. (National Center for Health Statistics. Prevalenceof Overweight Among Children and Adolescents: United States, 1999–2000,www.cdc.gov/nchs/products/pubs/pubd/hestats/overwght99.htm)
F I G U R E 7 . 1 9
What you weigh is a balance between how manycalories you eat and how many you expend.

212 Chapter 7 Managing Your Weight
about 500 Calories per day. This could mean adding 500 Calories of exercise, sub-tracting 500 Calories from your food intake, or some combination of the two. Weightloss should be kept at between 1/2 and 2 pounds per week to ensure that most of whatyou lose is fat and not lean tissue. If weight is lost more rapidly, the loss is less likely tobe maintained, and the additional loss will be from fluid, glycogen, and muscle protein.
Although the arithmetic is simple, achieving and maintaining weight loss is noteasy. There are regulatory mechanisms at work to keep body weight stable. There areenvironmental and emotional motivators to increase food intake and reduce the incli-nation to exercise. Nonetheless, reductions in intake, increases in activity, and changesin behavior can promote weight loss and long-term weight management.
Decrease energy intake by choosing low-calorie, nutrient-dense foods In order to lose weight without compromising nutrient intake,your diet must be low in energy but provide for all the body’s nutrient needs. Nutrientdensity becomes more important as energy intake is reduced; choosing foods that arelow in fat and added sugars will increase nutrient density. Even when choosing nutri-ent dense foods, it is difficult to meet nutrient needs with intakes of less than 1200Calories per day; therefore, dieters consuming less than this should take a multivita-min and mineral supplement. Medical supervision is recommended if intake is 800Calories per day or less.
Your Choice: How Much Food is 1500 Calories?
A 1500-Calorie diet will promote weight loss in most people,but how much food can you eat for 1500 Calories? Theanswer depends on which foods you choose. Your choices canmean the difference between feeling hungry all day andfeeling satisfied so you can stick with the low-calorie diet andlose the weight. In terms of weight loss, it doesn’t matter ifthe calories are from a few high-calorie foods or many low-calorie choices. If your energy intake is less than your output,you will lose weight. But if you choose nutrient-dense foods,
you will have more to choose from. For example, a breakfastof two eggs fried in butter and two breakfast sausagesprovides about 350 Calories. If instead you choose a bowl ofoatmeal with raisins and a glass of skim milk, you would beeating 100 fewer Calories. This translates into a banana, someyogurt, or another 100-calorie snack that can be eaten laterin the day. The two diets shown below each provide 1500Calories, but one has a lot more food and nutrients than theother. Which diet would you rather eat?
Meal More Nutrient Dense Less Nutrient DenseBreakfast Cheerios Fried eggs
Skim milk Sausage
Banana Toast with butter
Orange Juice
Coffee Coffee
Lunch Turkey sandwich with lettuce, Hamburger on bun with lettuce, tomato, ketchup, mustard,tomato, and mustard and mayonnaise
Apple
Skim milk Soda
Dinner Baked chicken breast Fried chicken breast
Baked potato with butter
Green salad with dressing
BrownieSkim milk
Trying to lose weight? Drink yourmilk. We all know it is a good sourceof calcium, which keeps your boneshealthy, but studies now indicatethat it may also make it easier tolose weight.

Increase physical activity to increase energy expendi-ture and reduce stress Physical activity is an important component of anyweight-management program. Exercise promotes fat loss and weight maintenance. Itincreases energy expenditure, so if intake remains the same, energy stored as fat is usedfor fuel. An increase in activity of 200 Calories five times a week will result in the lossof a pound in about 3 1/2 weeks. In addition to increasing energy expenditure, exer-cise also promotes muscle development. This is important for promoting weight lossbecause muscle is metabolically active tissue. Increasing muscle mass helps to preventthe drop in calorie needs that occurs as body weight decreases. Weight loss is bettermaintained when physical activity is included.46 In addition, physical activity im-proves overall fitness and relieves boredom and stress. The benefits of exercise are dis-cussed in Chapter 11.
Change behavior to promote weight loss and mainte-nance People tend to think of weight loss as something they can accomplish bygoing on a diet. When the weight is lost, they go off the diet. The problem is thatwhen their eating patterns return to what they were previously, they regain the weight.This “on a diet, off a diet” pattern may allow you to look good for the prom, but itisn’t what is needed for long-term weight management. To manage your weight at ahealthy level, you need to establish a pattern of food intake and exercise that allowsyou to enjoy foods and activities you like without your weight climbing. It should be apattern that you can comfortably adapt for life.
Changing food consumption and exercise patterns requires identifying the oldpatterns that led to weight gain and replacing them with new ones to promote andmaintain weight loss. This can be accomplished through a process called behaviormodification, which is based on the theory that behaviors involve (1) antecedents orcues that lead to the behavior, (2) the behavior itself, and (3) consequences of the be-havior. These are referred to as the ABCs of behavior modification.
The first step in a behavior modification program is to identify cues that lead toeating. You can do this by keeping a log of everything you eat or drink, where youwere when you ate, what else you were doing at the time, and what motivated you toeat at that time. Then by analyzing this log, you can see what prompted you to eat ex-cessive amounts of high-calorie foods. For instance, sitting in front of the televisionand mindlessly demolishing a bag of potato chips may cause you to overeat and thenfeel bad because you consumed the extra calories. In this case, the antecedent is watch-ing TV, the behavior is mindlessly eating the chips, and the consequence is feeling re-morse and gaining weight. The key to modifying this behavior is to recognize theantecedent, change the behavior, and replace the negative consequence with a positiveone. In this example, not taking food with you to the television, or taking only theportion of food you want to consume, eliminates the antecedent and the behavior.The consequence is that you have consumed only the food you planned, you do notgain weight, and you feel a sense of accomplishment. Applying behavior modificationtechniques to change eating behaviors has been shown to improve long-term weightmaintenance.
Weight gain can be achieved by increasingintake and weight trainingAs difficult as weight loss is for some people, weight gain can be equally elusive for un-derweight individuals. The first step toward weight gain is a medical evaluation to ruleout medical reasons for low body weight. This is particularly important when weightloss occurs unexpectedly. If the low body weight is due to low intake or high expendi-ture, gradually increasing consumption of energy-dense foods is suggested. More fre-quent meals and high-calorie snacks such as nuts, peanut butter, or milkshakesbetween meals can help increase energy intake. Replacing low-calorie fluids like waterand diet beverages with fruit juices and milk may also help. To encourage a gain inmuscle rather than fat, strength-training exercise should be a component of anyweight gain program. This approach requires extra calories to fuel the activity needed
Managing Your Weight Means Keeping It Healthy 213
Behavior modification A process usedto gradually and permanently changehabitual behaviors.
�*
If you lose weight you need to eatless to stay at the lower weight.For example, a 30-year-old 5�4�woman who weighs 170 poundsand is “low active” requires about2400 Calories a day to maintain herweight. If she loses 40 pounds butdoes not change her activity level,she will need to consume onlyabout 2100 Calories to maintainher healthier reduced weight.

214 Chapter 7 Managing Your Weight
to build muscles. These recommendations apply to individuals who are naturally thinand have trouble gaining weight on the recommended energy intake. This dietary ap-proach may not promote weight gain for those who limit intake because of an eatingdisorder.
So, What Should I Eat?
Watch your serving size• Pour your chips into a one-serving bowl rather than eating right from the big bag• Fill your plate once; skip the seconds• Check labels to see if your serving matches the label• Don’t supersize—choose a small drink and a small order of fries• Have a plain old burger, not one with a special sauce or extra-large patty• When you eat out, share an entrée with a friend or take some home for lunch the next day
Cut down on high-calorie foods• Have 1 scoop of ice cream rather than 2• Skip dessert• Bring your own lunch instead of having hot lunch at school• Have an apple with lunch instead of a candy bar• Have water instead of soda• Switch to low-fat milk
Don’t get too hungry• Eat breakfast—you’ll eat less later in the day• Increase your vegetable servings• Plan your snacks; you will probably choose more nutrient-dense food• Keep cut-up veggies and fruit available for snacks
If you want to eat more, exercise more• Go for a bike ride• Try bowling instead of watching TV on Friday nights• Take a walk during your lunch break or after dinner• Play tennis; you don’t have to be good to get plenty of exercise• Shoot some hoops• Get off the bus one stop early
There Are Many Diets; All Depend on Reducing Intake
Want to lose 10 pounds in just 5 days? What dieter wouldn’t? People desperate to loseweight are prey to all sorts of diets that promise quick fixes. They willingly eat a singlefood for days at a time, select foods on the basis of special fat-burning qualities, andconsume odd combinations at specific times of the day. Most diets, no matter howoutlandish, will promote weight loss because they reduce energy intake. Even dietsthat focus on modifying fat or carbohydrate intake or promise to allow unlimitedamounts of certain foods work because intake is reduced. The effectiveness of aweight-loss diet becomes evident when you evaluate long-term success.
When selecting a weight-management program, look for one that is based onsound nutrition and exercise principles, suits your individual food preferences, pro-motes long-term lifestyle changes, and meets your needs in terms of cost, conve-

nience, and time commitment (Table 7.8). An ideal diet is one that is part of aweight-management program that allows weight loss and then maintenance of thatloss over the long term. To be successful it needs to promote changes in the lifestylepatterns that led to weight gain. While quick fixes are tempting, if the program’s ap-proach is not one that can be followed for a lifetime, it is unlikely to promote success-ful weight management.
The following sections discuss some of the more common methods for reducingcalorie intake. The advantages and disadvantages of a number of popular diets andcommercial weight-management programs are given in Table 7.9.
Some weight-loss programs use exchangesand points to help you choose foodsFor breakfast, choose one food from group A, one from group B, and two from groupC. The foods in these groups or exchanges are similar in their energy and nutrientcontent, so they can be exchanged for one another. Diets that are based on such ex-changes recommend certain numbers of servings from specific food groups in order tolimit calorie intake but provide an adequate balance of nutrients. Some diet plans usethe Exchange Lists established by the American Diabetes and American Dietetic Asso-ciations (see Table 7.4 and Appendix I). Others, such as Weight Watchers, have devel-oped their own point system from which to choose foods. These programs offervariety from meal to meal and from day to day and are likely to meet nutrient needs.In addition, they teach meal-planning skills that are easy to apply away from homeand can be used over the long term.
There Are Many Diets; All Depend on Reducing Intake 215
T A B L E 7 . 8Rate Your Weight-Loss Program Before You Start
Does it promote a healthy dietary pattern that can be followedfor life?• Does it meet your nutrient needs?• Does it include enough variety to not become boring over time?• Does it fit your health needs? For example, would it be healthy for someone
who has high blood cholesterol?• Does it suit your food preferences?• Is the diet plan flexible enough to follow when eating away from home?• Does it include foods that you can easily obtain?
Does it promote a reasonable rate of weight loss?• Does it provide a reasonable number of calories (not less than 1200)?• Does it recommend realistic weight-loss goals (1/2 to 2 pounds per week)?
Does it promote physical activity?• Does it include an increase in activity?• Is the activity plan one you can follow?
Does it promote a change in behavior?• Does it provide the social support you need?• Does it promote changes in behavior that you can maintain over the long
term?• Does it help you learn healthy eating habits?
Is it scientifically sound?• Is the program based on sound scientific principles?• Are the personnel monitoring the weight-management program health
professionals?
Adapted from the American Heart Association’s Web site atwww.amhrt.org/Health/Risk_Factors/Overweight/Fad_Diets/fadguide.html.
For more informationon evaluating weight-loss programs, go to
the American DieteticAssociation at
www.eatright.org/and search for weight loss.

216 Chapter 7 Managing Your Weight
Some programs use packaged meals and drinks to limit portions and eliminate decisionsWhether you have a personal chef or buy frozen meals, it is easier to eat less whensomeone else decides what you’re having and puts that food in front of you. This isthe idea behind diet plans that sell prepackaged meals designed to replace some or all
T A B L E 7 . 9So Many Diets: Pros and Cons
Diet Approach Pros Cons
Weight Watchers Low energy, social support Safe, inexpensive, flexible Requires group participation
Jenny Craig Low energy Safe, convenient Expensive; relies on purchaseof special foods
SlimFast Low energy Safe Does not promote long-termbehavior change
The New Beverly Specific timing and Inexpensive Based on unsound principles;Hills Diet combinations of foods does not promote long-term
behavior change; nutritionally unsound
Optifast Very-low-calorie formula Rapid weight loss Expensive; dangerous if doesnot include medicalsupervision
Fit or Fat Increased exercise Safe, inexpensive No social support
The Zone (and Low carbohydrate (40% Inexpensive, flexible Based on questionableMastering the Zone) of energy) principles; no social supportDiet
Eating Thin for Life Moderation—written as Inexpensive No social supportweight-loss success stories, recipes, and menu ideas
Dieting with the Simple nutrition and Inexpensive, flexible No social supportDuchess exercise tips
Cabbage soup diet Unlimited amounts of Rapid weight loss No social support; does notcabbage soup, fruit, promote long-term behaviorcoffee, and tea change; lacks variety
Grapefruit diet Some foods have special Inexpensive Based on unsound principlesqualities that burn fat
Sugar Busters Eliminates sugar; low Inexpensive No social support; based oncalorie—1200 Cal a day unsound principles;
insufficient carbohydrate
Volumetrics Weight Emphasizes foods high in Safe, inexpensive No social support or exerciseControl Plan water, fiber, and air to component
promote fullness with few calories
Atkins’ Diet Very low carbohydrate Inexpensive; Difficult to follow in the longrapid initial term; no social supportweight loss
South Beach Initially very low carbohydrate, Safe, inexpensive, Initial weight loss is mostly Diet then more healthy heart-healthy water; no social support
carbohydrates are allowed

of your usual meals. These diets are easy to follow as long as you are not traveling oreating out, but they can be expensive and are not practical in the long term. Becauseall meals are provided, they do not teach the food selection skills needed to make along-term lifestyle change.
Over-the-counter diet drinks can help reduce calorie in-take Rather than pre-packaged meals, many diet plans replace some or all of yourmeals with special beverages (Figure 7.20). They can make reducing intake easy be-cause they eliminate the problem of choosing low-calorie foods. Many of the liquidweight-loss diets that are available over-the-counter recommend a combination offood and formula to provide about 800 to 1200 Calories per day. These formula planspromote weight loss as long as the foods eaten with them are low in calories. They areeasy to use and relatively inexpensive, but they do little to change eating habits for life.Most diet programs that rely exclusively on liquid formulas have high dropout ratesand poor long-term weight-maintenance results. These are not recommended withoutmedical supervision.
Very-low-calorie diets cause rapid weight loss but canincrease risks A very-low-calorie diet is defined as one with fewer than 800Calories per day. These diets are generally a variation of the protein-sparing modifiedfast, which is a diet providing a high proportion of protein but little energy. The con-cept behind this is that the protein in the diet will be used to meet the body’s proteinneeds and therefore will prevent excessive loss of body protein. Frequently, very-low-calorie diets are offered as a liquid formula. These formulas provide from 300 to 800Calories and 50 to 100 g of protein per day and meet all other nutrient needs.
These diets will cause you to lose fast; initial weight loss is 3 to 5 pounds per week.This can provide a psychological boost and motivate the dieter to continue losingweight; however, in most cases, almost 75% of this initial weight loss is from waterloss. Once the initial water loss ends, weight loss slows. The dieter’s basal metabolismslows to conserve energy, and physical activity decreases because the dieter often doesnot have the energy to continue his or her typical level of activity.
Very-low-calorie diets are no more effective than other methods in the long termand carry more risks. At these low-energy intakes, body protein is broken down andpotassium is excreted. Depletion of potassium can result in an irregular heartbeat andis potentially deadly. Other side effects include gallstones, fatigue, nausea, cold-intol-erance, light-headedness, nervousness, constipation or diarrhea, anemia, hair loss, dryskin, and menstrual irregularities. These diets are not recommended for people whoare less than 30 to 40% above their healthy body weight, for pregnant or breast-feed-ing women, or for children, adolescents, or those with severe medical problems.47
Since 1984, the FDA has required that all very-low-calorie diet formulas carry awarning that they can cause serious illness and should be used only under medicalsupervision.
Low-fat diets are not necessarily low in caloriesIf a food is low in fat, is it low in calories? The answer is sometimes yes, but not al-ways. Because fat is high in calories, consuming a low-fat diet typically reduces energyintake. Low-fat diets provide more food for the same amount of energy than high-fatdiets and may satisfy hunger after less energy is consumed. Differences in the way di-etary fat and dietary carbohydrate are used by the body also explain why low-fat dietsare effective for weight loss. Excess calories from dietary fat are stored more efficientlythan excess calories from carbohydrate, so consuming excess energy from fat leads to agreater accumulation of body fat than consuming excess energy as carbohydrate.48
Problems with low-fat diets occur when people think they can eat low-fat foods inunlimited quantities. This is not too much of a problem if the low-fat food is broccoli,but problems emerged in the 1990’s when the food industry flooded the market withlow-fat cookies and cakes. These foods were low in fat but not in energy. When con-sumed in large amounts they cause weight gain. Even a diet low in fat will result in
There Are Many Diets; All Depend on Reducing Intake 217
F I G U R E 7 . 2 0
Liquid diet products are easy to use becausethey eliminate food choices, but they donothing to change eating habits. (Julie Toy/The Image Bank/Getty Images)
Does cabbage soup or grapefruitstimulate the breakdown of bodyfat? Unfortunately not; the weightloss caused by such diets is due toa reduction in energy intake andnot the magical properties of thefoods. Diets based on single foodsdo not encourage the changes ineating behavior that are needed to maintain a healthy weight.
Very-low-calorie diet A weight-lossdiet that provides fewer than 800 Caloriesper day.
�*
Protein-sparing modified fast A very-low-calorie diet of high protein contentdesigned to maximize the loss of fat andminimize the loss of protein from the body.
�*

218 Chapter 7 Managing Your Weight
weight gain if energy intake exceeds energy output. This is illustrated by the fact thatthe percent of calories as fat in the typical American diet has decreased, while thenumber of people who are overweight continues to increase.49
Low-carbohydrate diets vary in the amount of carbohydrate allowedIf you cut out the pasta and potatoes you will lose weight, right? The Atkin’s diet,South Beach diet, Sugar-busters, Calories Don’t Count, the Scarsdale diet, and theZone are just a few of the low-carbohydrate weight-loss diets that have been promotedover the last 30 years. In addition to promising weight loss, these diets claim to im-prove athletic performance and promote overall health. They are all based on thepremise that a high carbohydrate intake causes an increase in insulin levels, which pro-motes the storage of body fat. Restricting carbohydrate intake is hypothesized to re-duce insulin, thereby reducing fat storage and promoting fat loss. Unfortunately, therelationship between carbohydrate intake, insulin levels, and body fat is not that sim-ple. Some of these diets severely restrict carbohydrate intake, while others are less re-strictive and are more concerned with the type of carbohydrate.
Very-low-carbohydrate diets cause ketosis and weightloss Very restrictive low-carbohydrate diets prohibit foods such as breads, grains,and fruits, and limit vegetable intake while allowing unlimited quantities of meat andhigh-fat foods that are low in carbohydrate. These diets cause a rapid initial weightloss, most of which is water. This occurs because when carbohydrate intake is verylow, glycogen stores, along with the water they hold, are lost quickly. Ketones are pro-duced because fat is not completely broken down in the absence of carbohydrate. Ex-cretion of these ketones causes further water loss. In addition, there is evidence thatketones in the blood suppress appetite, making it easier to reduce food intake. Theappetite-suppressing effect of ketones is not unique to low-carbohydrate diets. Ketonelevels increase on any low-calorie diet and suppress appetite.
Although these diets do promote weight loss, more research is needed to determinethe health consequences of long-term consumption of very-low-carbohydrate diets.These diets are higher in fat and protein than is recommended. High intakes of satu-rated fat and cholesterol increase the risk of high blood cholesterol and gallbladderdisease. They are also lower in fruits, vegetables, whole grains, and milk than is recom-mended. Low intakes of these will reduce intakes of essential nutrients, phytochemi-cals, and fiber.
The type of carbohydrate is more important than theamount Not all low-carbohydrate diets severely restrict the amount of carbohy-drate, and most allow an increase in some types of carbohydrate over time. The carbo-hydrates that are allowed are those from unrefined sources such as vegetables andwhole grains. These foods are high in fiber and do not increase insulin nearly as muchas refined carbohydrates such as white flour and sugar. Including whole grains andvegetables increases the intake of fiber, phytochemicals, and micronutrients and hasonly a modest effect on insulin levels.
Low-carbohydrate diets reduce energy intake Weight loss oc-curs on low-carbohydrate diets because total energy intake is reduced. After all, if youremove the bun from your burger and take the baked potato away from your steakdinner, you have cut the calories in the overall meal. But if you replace the bun withsome low-carbohydrate bread and substitute some low-carbohydrate pasta for thepotato, you may have more trouble losing pounds. As with special low-fat products,low-carbohydrate foods are not necessarily low in calories and cannot be eaten liber-ally without affecting energy balance (Figure 7.21).
F I G U R E 7 . 2 1
Consuming a low-carbohydrate diet canpromote weight loss, but just because a food is labeled low-carbohydrate doesn’t mean itcan be eaten liberally without concern for itscalories. The food industry is rapidly developinglow-carbohydrate foods, but they are not all lowin calories. (© AP/Wide World Photos)
Low-carbohydrate diets are notnew. In 1864 William Bantingpublished a book called Letter onCorpulence, which promoted a high-protein, high-fat, low-carbohydratediet. The first three editions sold63,000 copies in Britain alone.

Drugs and Surgery May Help When Conventional Approaches Fail
Drugs and Surgery May Help When Conventional 219
P I E C E I T T O G E T H E R
Choosing a Weight Loss Plan that Works for YouMark is 40 pounds overweight. He has high blood pressure andhigh blood cholesterol levels. Given his BMI of 28 kg/m2 andhis other risk factors, his doctor advises him to lose weight. Heresearches a number of weight-loss programs and finally narrowshis choices down to three. He lists these below with the reasonshe is considering them.
• Low-carbohydrate plan—Many of his friends have usedthis to shed pounds and say they were never hungry
• Liquid formula that replaces two meals a day—Easybecause he doesn’t need to do much meal planning andhe can still eat dinner with his family
• Exchange plan run through his community center—Lots of social support and includes a walking group that meets 5 days a week
To decide which is best for him, he considers the advantagesand disadvantages of each plan in terms of the nutritionalsoundness of the diet, variety, ease, expense, and how it willaffect his exercise level.
ARE THE DIETS NUTRITIONALLY SOUND?
• Low-carbohydrate plan—The diet is too low incarbohydrate to prevent ketosis, low in fiber, and low in calcium because milk is restricted
• Liquid formula—Seems alright as long as the meal isnutritionally sound
• Exchange plan—This is nutritionally sound because itincludes choices from all food groups
HOW WOULD YOU RATE THESE DIETSIN TERMS OF VARIETY?
Your answer:
�
�
HOW EASY ARE THESE DIETS TO FOLLOW?
At first the liquid diet seems easiest because he needs toworry about only one meal a day. But then he realizes hestill has to cook for his family. The only diet that will allowhim to prepare a meal that will fit into his diet and workfor the whole family is the exchange plan.
HOW DO THESE PLANS COMPARE IN COST?
All three are equal in cost. The extra cost of the moreexpensive meats included in the high-carbohydrate diet issimilar to the extra cost of the liquid formula. The exchangeplan involved a monthly fee to the community center.
HOW DO THEY RATE IN TERMS OF EXERCISE?
Your answer:
WHICH PLAN DO YOU THINK WOULD WORK BESTFOR MARK OVER THE LONG TERM? WHY?
Your answer:
�
�
�
�
Drugs and surgery can help promote weight loss but these drastic measures are not foreveryone. They can be acceptable weight-management tools however for obese indi-viduals when diet and exercise alone are not enough.

220 Chapter 7 Managing Your Weight
An ideal weight-loss drug would promotelong-term weight loss without side effectsSome of the drugs available to promote weight loss are well studied and offer legiti-mate aids to weight loss; others offer little more than water loss. An ideal drug for thetreatment of obesity would permit an individual to lose weight and maintain the loss,be safe when used for long periods of time, have no side effects, and not be addictive.Many attempts have been made to develop such a drug, but weight-loss drugs stillcarry risks. In 1997, a prescription drug combination called fen-phen (fenfluramineand phentermine) that was being used to reduce food intake was linked to seriousheart valve damage. As a result, fenfluramine and the related drug dexfenfluraminewere withdrawn from the market.50
There are only a few drugs that promote weight loss Pre-scription drugs available for the treatment of obesity include those that reduce ap-petite by affecting the activity of brain neurotransmitters (sibutramine, brand nameMeridia) and those that decrease the absorption of fat in the intestine (orlistat, brandname Xenical). Prescription drugs such as these are recommended only for thosewhose health is seriously compromised by their body weight: those with a BMI greaterthan 30 kg/m2 and those with a BMI greater than or equal to 27 kg/m2 who have riskfactors or diseases.43 One of the major disadvantages of drug treatment is that even ifthe drug promotes weight loss in the short term, the weight is regained when thedrugs are discontinued.
There are also some nonprescription medications sold over-the-counter to promoteweight loss. Most contain either caffeine, which promotes water loss, or fiber, whichincreases satiety. These are regulated by the FDA and must adhere to strict guidelinesregarding the dose per pill and the effectiveness of the ingredients. Some may be mod-erately effective, but, as with prescription medications, the weight is usually regainedwhen the product is no longer taken.
Weight-loss supplements are not regulated by the FDAWeight-loss supplements often include herbal sources of compounds contained inprescription medications. Some of these are powerful drugs with dangerous side ef-fects. The FDA does not regulate dietary supplements for weight loss unless theyclaim to be a substitute for a drug or claim to perform a drug action or therapy (seeChapter 10). Because they are not strictly regulated, their safety and effectiveness maynot have been carefully tested, and doses may vary from tablet to tablet and brand tobrand. It cannot be assumed that a product is safe simply because it is labeled “herbal”or “all natural.” Common ingredients in weight-loss dietary supplements include theamino acids arginine and ornithine, chromium, and a variety of herbs. Arginine andornithine are hypothesized to burn fat during sleep because they stimulate the releaseof growth hormone. Although growth hormone promotes fat loss and muscle growth,research has not found any relationship between body weight and the levels of growthhormone. The mineral chromium is usually included as chromium picolinate. Adver-tisements claim that chromium picolinate will decrease body fat and increase the pro-portion of lean tissue, but human trials have not consistently demonstrated an effecton body composition or body weight.
Herbal products marketed for weight loss also include teas and supplements thatcontain plant-derived laxatives such as senna, aloe, buckthorn, rhubarb root, cascara,and castor oil. Cascara, senna, and castor oil are approved by the FDA and regulatedas drugs for use in nonprescription laxatives. These cause weight loss by inducing diar-rhea, which causes water loss. They don’t lead to fat loss, however, because they do notsignificantly reduce nutrient absorption. This is because they act in the colon, not inthe small intestine, where most absorption occurs. Overuse of herbal laxatives cancause serious side effects, including nausea, diarrhea, vomiting, stomach cramps,chronic constipation, fainting, and severe electrolyte imbalances leading to cardiac ar-rhythmia and death.51
Ephedra, an ingredient that wasused in weight-loss supplementscalled fat burners, was banned bythe FDA in 2004. Fat burners aresupplements that claim to increasemetabolism. Ephedra did increaseenergy expenditure somewhat, butit also caused increases in heartrate and blood pressure, which ledto serious side effects.

Weight-loss surgery reduces the amount of food that can be eaten and absorbedThere are a number of surgical procedures that reduce body weight by altering the GItract to reduce food intake and absorption. These surgical approaches are recom-mended only in cases where the risk of dying from obesity and its complications isgreat. It is appropriate only for individuals with a BMI greater than or equal to 40kg/m2 (extreme obesity) and in those with a BMI between 35 and 40 kg/m2 who haveother life-threatening conditions that could be remedied by weight loss. Each casemust be evaluated individually to assess the potential risks and benefits of the surgery.
Currently, the most popular surgical approach to treat obesity is gastric bypass.Gastric bypass involves bypassing part of the stomach by connecting the intestine tothe upper portion of the stomach. Food intake is reduced because the now-smallerstomach becomes full with less food and absorption is reduced because the small in-testine is shortened. Significant weight loss is usually achieved 18 to 24 months aftersurgery (Figure 7.22). Some weight regain is common after 2 to 5 years. Anothersurgery, gastroplasty, involves stapling off a section of the top of the stomach to limitthe amount of food that can be consumed at any given time. The success rate is lowerwith gastroplasty because the staples can be broken by consumption of large meals.Both of these procedures have short-term surgical risks and a long-term risk of nutri-ent deficiencies, particularly of vitamin B12, folate, and iron.52 Even after surgery, it isnecessary to limit the types and amounts of food consumed in order to allow weightloss and maintenance.
Eating Disorders Involve an Abnormal Concern with Body Weight and Shape 221
F I G U R E 7 . 2 2
Gastic bypass surgery is not without risks, but it can bevery effective in promoting weight loss. NBC’s Today Showweather anchor Al Roker lost 100 pounds after undergoingthe procedure. (a: Nick Elgar/Getty Images; b: GregoryPace/Corbis)
(b)(a)
Eating Disorders Involve an Abnormal Concern with Body Weight and Shape
On some days, you may eat twice as much as other days. One day you may stuff your-self at lunch and indulge in a rich dessert at dinner and on the next skip lunch alto-gether. Some days you may survive on snack foods while on others you eat threebalanced meals. Is this normal? Yes, normal eating patterns are flexible; sometimespeople overeat, and sometimes they undereat. Normal eating may involve limitingwhat you eat in order to manage your weight and meet recommendations for ahealthy diet. It can also mean eating more than you need at a party or other special oc-casion. What and how much people eat vary in response to social occasions, personal
Fat can be removed from specificlocations on the body by liposuction.This procedure involves inserting alarge hollow needle under the skininto a localized fat deposit andliterally vacuuming out the fat.Liposuction does not significantlyreduce overall body weight.
Some people go to great extremesto limit their food intake. Oneprocedure wires the jaw shut sointake is restricted to liquids thatcan be taken through a straw. Jawwiring is not effective for maintainingweight loss in the long term becauseit does not help change the eatinghabits that led to weight gain.

222 Chapter 7 Managing Your Weight
emotions, time limitations, hunger, and the availability of food, but generally peopleeat when they are hungry, choose foods they enjoy, and stop eating when they aresatisfied.
Abnormal eating occurs when someone becomes overly concerned with food, eat-ing, and body size and shape. If the emotional aspects of food and eating overpowerthe role of food as nourishment, an eating disorder may develop. The term “eatingdisorder” is somewhat of a misnomer because it implies that the problem is a nutri-tional one. In fact, eating disorders are primarily psychological disorders that involvenutrition-related behaviors; they have nutritional and physiological complications.According to mental health guidelines, there are three categories of eating disorders:anorexia nervosa, bulimia nervosa, and a third category called “eating disorders nototherwise specified” (EDNOS) that includes abnormal eating behaviors that don’t fitthe other two categories. Binge-eating disorder is included in the EDNOS category(Table 7.10).53
Anorexia nervosa is characterized by self-starvationAnorexia nervosa is a life-threatening disorder. “Anorexia” means lack of appetite, butin the case of the eating disorder anorexia nervosa it is a desire to be thin, rather than alack of appetite, that causes individuals to decrease their food intake (Figure 7.23).Anorexia nervosa was first recognized by physicians in the second half of the 19th cen-tury, but the characteristics they described are still true of the syndrome today: severeweight loss, amenorrhea, constipation, and restlessness. Anorexia nervosa affects 1%of female adolescents in the United States.54 The average age of onset is 17 years.
T A B L E 7 . 1 0Distinguishing Eating Disorders
Binge-Eating Factor Anorexia Bulimia Disorder
Body weight Below normal Usually normal Above normal(less than 85% ofrecommendedweight)
Binge eating Possibly Yes, at least twice Yes, at least twicea week for 3 a week for 6months months
Purging Possibly Yes, at least twice Noa week for 3months
Restricts food Yes Yes Yes
intake
Body image Dissatisfaction Dissatisfaction Dissatisfactionwith body and with body and with bodydistorted image distorted image of body size of body size
Fear of being fat Yes Yes Not excessive
Self-esteem Low Low Low
Menstrual Absence of at least No Noabnormalities three consecutive
periods
For more informationon eating disorders,go to the NationalEating Disorders
Association, atwww.nationaleatingdisorders.org/,or to the National Institutes of MentalHealth at www.nimh.nih.gov/
Eating disorder A persistentdisturbance in eating behavior or otherbehaviors intended to control weight thataffects physical health and psychosocialfunctioning.
�*
Anorexia nervosa An eating disordercharacterized by self-starvation, a distortedbody image, and low body weight.
�*
Bulimia nervosa An eating disordercharacterized by the consumption of largeamounts of food at one time (binge eating),followed by purging behaviors such asvomiting and the use of laxatives toeliminate food or energy from the body.
�*
Binge-eating disorder An eatingdisorder characterized by recurrent episodesof binge eating in the absence of purgingbehavior.
�*
Amenorrhea Delayed onset ofmenstruation or the absence of three or more consecutive menstrual cycles.
�*

There is a 5% death rate in the first 2 years, and this can reach 20% in untreated indi-viduals.55 Anorexia is a psychological disorder that has a behavioral component andphysical and nutritional consequences that can be life-threatening.
The fear of being fat dominates anorexia The psychologicalcomponent of anorexia nervosa revolves around an overwhelming fear of gainingweight, even in those who are already underweight. It is not uncommon for individu-als with anorexia to feel that they would rather be dead than fat. Anorexia is also char-acterized by disturbances in body image or perception of body size that prevent thoseaffected from seeing themselves as underweight even when they are dangerously thin.Those with this disorder may use body weight and shape as a means of self-evaluation:“If I weren’t so fat then everyone would like and respect me and I wouldn’t have otherproblems.” However, no matter how much weight they lose they do not gain self-respect, inner assurance, or the happiness they seek. Therefore, they continue to restricttheir intake, overexercise, or use purging behaviors in order to lose weight.
People with anorexia restrict food intake The most obviousbehavioral component of anorexia nervosa is a restriction in food intake. Food andeating become an obsession. In addition to restricting the total amount of foodconsumed, anorexics develop personal diet rituals, limiting certain foods and eatingthem in specific ways. Although they do not consume very much food, they are preoc-cupied with food and spend an enormous amount of time thinking about food, talk-ing about food, and preparing food for others. Instead of eating, they move the foodaround the plate and cut it into tiny pieces. Although anorexics keep their weight lowby restricting intake, it is estimated that 50% of people with anorexia also use purgingas a means of weight control.56
Another behavior that is typical of anorexia is hyperactivity and overactivity. This isin contrast to the decrease in activity and fatigue that characterizes other starvationstates associated with weight loss. Many anorexics exercise excessively to burn calories.Sometimes the activity is surreptitious, such as going up and down stairs repeatedly orgetting off the bus a few stops too early. For others the activity takes the form of stren-uous physical exercise. They may become fanatical athletes. The exercise is typicallydone alone and is performed as a regular rigid routine. They feel guilty if they cannotexercise and may link exercise and eating, so a certain amount of exercise earns themthe right to eat and if they eat too much they must pay the price by adding extra exer-cise. Those who use exercise to increase energy expenditure do not stop when they aretired; instead, they train compulsively beyond reasonable endurance.
Eating Disorders Involve an Abnormal Concern with Body Weight and Shape 223
Dear Diary,
For breakfast today I had a cup of tea. For
lunch I ate some lettuce and a slice of tomato, but
no dressing. I cooked dinner for my family. I love to
cook, but it is hard not to taste. I tried a new
chicken recipe and served it with rice and
asparagus. I even made a chocolate cake for dessert
but I didn’t even lick the bowl from the frosting.
When it came time to eat, I only took a little. I told
my mom I nibbled while cooking. I pushed the food
around on my plate so no one would notice that I
only ate a few bites. I was good today – I kept my
food intake under control. The scale says I have lost
20 pounds but I still look fat.
F I G U R E 7 . 2 3
Persons with anorexia nervosa carefullyregulate what they eat to maintain a very lowbody weight. (David Young Wolff/PhotoEdit)
Eating disorders can be life-threatening, particularlyanorexia. If untreated, peoplewith this disorder may starvethemselves to death.
Body image The way you perceive and imagine your body.�*
Purging Behaviors such as self-induced vomiting and misuse of laxativesand diuretics to rid the body of energy.
�*

224 Chapter 7 Managing Your Weight
The physical symptoms of anorexia are those of starva-tion The first obvious physical symptom of anorexia is weight loss. As weight lossbecomes severe, symptoms of starvation begin to appear. Starvation affects mentalfunction, causing anorexics to become apathetic, dull, exhausted, and depressed.Physical symptoms include depletion of fat stores; wasting of muscles; inflammationand swelling of the lips; flaking and peeling of skin; growth of fine hair on the body,and dry, thin, brittle hair on the head that may fall out. In females, estrogen levelsdrop, and menstruation becomes irregular or stops.6 This can delay sexual maturationand can have long-term effects on bone density. In males, testosterone levels decrease.In the final stages of starvation, symptoms include abnormalities in electrolyte bal-ance, dehydration, edema, cardiac abnormalities, absence of ketones due to fat-storedepletion, and infection, which further increases nutritional needs.
Treatment of anorexia nervosa must restore nutritionalhealth The goal of treatment for anorexia nervosa is to help resolve the psychologi-cal and behavioral problems while providing for physical and nutritional rehabilita-tion. Early treatment of anorexia is important because starvation may causeirreversible damage. The goal of nutrition intervention is to promote weight gain byincreasing energy intake and expanding dietary choices.57 Nutritional rehabilitation inmild cases involves learning about nutrition and meal planning in order to develophealthy eating patterns. In more severe cases, anorexics are hospitalized, and their foodintake and exercise behaviors are carefully controlled. Intravenous nutrition may benecessary to keep the individual alive. Some anorexics make full recoveries but abouthalf have poor long-term outcomes—remaining irrationally concerned about weightgain and never achieving normal body weight.
Bulimia nervosa is characterized by cycles of bingeing and purging“Bulimia” is from the Greek bous (ox) and limos (hunger), denoting hunger of such in-tensity that a person could eat an entire ox. The modern concept of bulimia nervosa asan eating disorder arose in the early 1970’s, when a set of symptoms was identifiedand distinguished from anorexia and obesity. Many different names were used for thisdisorder, including dysorexia, bulimarexia, thin-fat syndrome, binge/purge syndrome,and dietary chaos syndrome. The term bulimia nervosa was coined in 1979 by aBritish psychiatrist who suggested that bulimia consisted of powerful urges to overeatin combination with a morbid fear of becoming fat and the avoidance of the fatteningeffects of food by inducing vomiting or abusing purgatives or both.58 It currently oc-curs in 2 to 5% of the population.59 Bulimia nervosa is a disorder that involves fre-quent episodes of binge eating or bingeing that are almost always followed by purgingand other inappropriate compensatory behaviors. A diagnosis of bulimia is based onthe frequency with which episodes of binge eating and inappropriate compensatorybehaviors occur. Bulimia is subdivided into nonpurging and purging types. Nonpurg-ing bulimics use behaviors such as fasting or excessive exercise to prevent weight gain.Purging bulimics regularly engage in behaviors that may include self-induced vomit-ing and misuse of enemas, laxatives, diuretics, or other medications.
Preoccupation with body weight dominates bulimia ner-vosa As with anorexia, people with bulimia have an intense fear of becoming fat.They have a negative body image accompanied by a distorted perception of their bodysize. Their self-esteem is highly tied to their impressions of their body shape andweight. They are preoccupied with the fear that once they start eating they will not beable to stop. They may engage in continuous dieting, which leads to a preoccupationwith food.
People with bulimia blame all of their problems on their appearance; this allowsthem to avoid things that are real problems. A bulimic also thinks he or she is the onlyperson in the world with this problem. As a result they are often socially isolated.They may avoid situations that will expose them to food, such as going to parties orout to dinner, further isolating them socially.
Binge eating or bingeing The rapidconsumption of a large amount of food in a discrete period of time associated with a feeling that eating is out of control.
�*

The binge/purge behavior distinguishes bulimia Bulimiatypically begins with dieting that is motivated by the desire to be thin. Overwhelminghunger may finally cause the dieting to be interrupted by a period of overeating. Even-tually a pattern develops involving semi-starvation interrupted by periods of gorging.During a food binge, a bulimic experiences a sense of lack of control. The amount offood consumed during a binge varies but is typically on the order of 3400 Calories—as much as many teenagers eat in an entire day. One study found that bulimics con-sumed an average of about 7000 Calories in a 24-hour period.60 Binges usually lastless than 2 hours and occur in secrecy. They stop when the food runs out or whenpain, fatigue, or an interruption intervenes (Figure 7.24).
After these binge episodes, most bulimics use purging techniques such as vomitingor abuse of laxatives or diuretics to eliminate the excess calories from their bodies. Themost common behavior is self-induced vomiting. It is used at the end of a binge butalso after normal eating to eliminate food before it is absorbed and the energy it pro-vides can cause weight gain. Laxatives are taken to induce diarrhea. Although the pa-tients believe the diarrhea prevents calories from being absorbed, in fact, nutrientabsorption is almost complete before food enters the colon where laxatives work. Theweight loss associated with laxative abuse is due to dehydration. Diuretics also causewater loss, but via the kidney. They do not cause fat loss. A smaller number of bulimiasufferers resort to other methods of eliminating these excess calories, such as extremeexercise or fasting. A few bulimics use a combination of purging and non-purgingmethods.
Purging can damage the gastrointestinal tract It is the purg-ing of the binge-purge cycle that is most hazardous to health in bulimia nervosa. Purg-ing by vomiting brings stomach acid into the mouth. Frequent vomiting affects thegastrointestinal tract by causing tooth decay, sores in the mouth and on the lips,swollen jaws and salivary glands, irritation of the throat, esophageal inflammation,and changes in stomach capacity and stomach emptying.61 It also causes broken bloodvessels in the face from the force of vomiting, electrolyte imbalance, dehydration,muscle weakness, and menstrual irregularities. Laxative and diuretic abuse can alsocause dehydration and electrolyte imbalance. Rectal bleeding may occur from laxativeoveruse.
Treatment of bulimia nervosa must separate eatingfrom emotions The overall goal of therapy for people with bulimia nervosa isto separate eating from their emotions and from their perceptions of success and topromote eating in response to hunger and satiety. Psychological issues related to body
Eating Disorders Involve an Abnormal Concern with Body Weight and Shape 225
Dear Diary, Today started well. I stuck to my diet through breakfast, lunch, and dinner, but by 8 PM I was feeling depressed and bored. I thought food would make me feel better. Before I knew it I was at the convenience store buying two pints of ice cream, a large bag of chips, a one pound package of cookies, half dozen candy bars, and a quart of milk. I told the clerk I was having a party. But it was a party of one. Alone in my dorm room I started by eating the chips, then polished off the cookies and the candy bars, washing them down with milk and finishing with the ice cream. Luckily no one was around so I was able to vomit without anyone hearing. I feel weak and guilty but also relieved that I got rid of all those calories. Tomorrow, I will start a new diet.
F I G U R E 7 . 2 4
Bulimia is characterized by binge eatingfollowed by purging. (David Young Wolff/PhotoEdit)
In a study that measured the foodfrom a binge that remained in thestomach after vomiting, it wasfound that on average 1209Calories were retained after abinge containing 3530 Calories.

226 Chapter 7 Managing Your Weight
image and a sense of lack of control overeating must be resolved. Nutritional therapymust address physiological imbalances caused by purging episodes as well as provideeducation on nutrient needs and how to meet them. Antidepressant medications havealso been shown to reduce the frequency of binge episodes. Treatment has been foundto speed recovery, but for some women this disorder may remain a chronic problemthroughout life.62
Binge-eating disorder is characterized by bingeing without purgingBinge-eating disorder is probably the most common eating disorder. According to theNational Institutes of Health, it affects up to 4 million Americans. Binge-eating disor-der affects 2 to 3% of the total adult population and about 8% of the obese popula-tion. Unlike anorexia and bulimia, binge-eating disorder is not uncommon in men; itoccurs in a female to male ratio of about 1.5 to 1. Compared to anorexia or bulimia,binge-eating disorder occurs in an older population, being most common in those be-tween 30 and 50 years of age. Individuals who suffer from binge-eating disorder en-gage in recurrent episodes of binge eating but do not regularly engage in purgingbehaviors such as vomiting, fasting, or excessive exercise (Figure 7.25). These individ-uals may range from normal weight to obese but are likely to have above-normal bodyweights and may seek help for treatment of obesity rather than for their binge-eatingbehavior.59 About one-quarter to one-third of individuals who attend weight-loss clin-ics meet the criteria for binge-eating disorder.
Treatment of this disorder involves counseling to improve body image and self-acceptance, a healthy nutritious diet, and increased exercise to promote weight loss,along with behavior therapy to reduce bingeing.
Genetic, psychological, and socioculturalfactors increase the risk of eating disordersEating disorders occur in people of all ages, races, and socioeconomic backgrounds,but some groups are at a greater risk than others. In the United States, anorexia, bu-limia, and binge-eating disorder affect about 5% of girls and women and 1% of boys
Your Choice: Can You Help aFriend with an Eating Disorder?
The physical consequences of eating disorders are verysevere, and people with them usually do not get better bythemselves. It is therefore important that they get help. Youcan’t provide the medical and psychological treatment afriend or relative with an eating disorder needs, but you can help them.
If you suspect a friend has an eating disorder, alert aparent, teacher, coach, pastor, school nurse, or other trustedadult about your concerns or confront your friend yourselfand express your concern. If you choose to approach themyourself, you need to be firm but supportive and caring. The first reaction of someone confronted about an eatingdisorder is often to deny that they have a problem. Supportyour suspicions with examples of things you have seen that
make you believe your friend has a problem. You should be prepared for all possible reactions. People with eatingdisorders are good at hiding their behaviors and denyingthe problem, so it is traumatic for them when someone hasdiscovered their secret. One person may be relieved that youare concerned and willing to help, whereas another may beangry and defensive.
The goal in discussing a person’s eating disorder is toencourage him or her to seek help. But help is effective onlyif it is desired. People with eating disorders are likely torefuse help initially; it is therefore important that you makeit clear that you are not forcing them to do anything theydon’t want to do. Continued encouragement can help somepeople to seek professional help.

and men.59 Eating disorders most commonly begin in adolescence, when physical,psychological, and social development are occurring rapidly. We do not know whatcauses eating disorders, but genetic, psychological, and social and cultural factors con-tribute to their development.
Genetics contributes to the development of eating dis-orders You don’t necessarily inherit an eating disorder, but the genes you inheritcontribute to personality traits and other biological characteristics that predispose youto developing an eating disorder. For example, inherited abnormalities in the levels ofneurotransmitters such as serotonin, which affects food intake, and in levels of thehormone leptin, which helps regulate body weight, have been hypothesized to con-tribute to the behaviors typical of anorexia and bulimia.64 Binge-eating disorder maybe linked to a defect in a gene called the melanocortin 4 receptor gene. The proteinmade by this gene helps control hunger and satiety. If this gene is abnormal andmakes too little of this protein, the body feels too much hunger. In one study, all carri-ers of the mutant gene were binge eaters and mutations were found in 5% of obesesubjects.65 Genes such as this contribute to eating disorders, but a single gene is notlikely to be the sole cause. These are complex diseases that are the result of the interac-tion of multiple genes with the environment. When placed in the right environment,an individual who carries such genes will be more likely to develop an eating disorder.
Low self-esteem is common among people with eatingdisorders Certain personality characteristics and psychological problems are com-mon among individuals with eating disorders. Often people with eating disordershave a low self-esteem. Self-esteem refers to the judgments people make and maintainabout themselves—a general attitude of approval or disapproval that indicates if theythink they are worthy and capable. Eating disorders are also rooted in the need forself-control. Those with eating disorders are often perfectionists who set very highstandards for themselves and others. In order to be perfect they strive to be in controlof their bodies and their lives. They view everything as either a success or a failure.Being fat is seen as failure, thin as success, and thinner as even more successful. Inspite of their many achievements, those with eating disorders feel inadequate, defec-tive, and worthless.
Eating Disorders Involve an Abnormal Concern with Body Weight and Shape 227
Dear Diary,
I got on the scale today. What a mistake!
My weight is up to 180 pounds. I hate myself for
being so fat. Just seeing that I gained more weight
made me feel ashamed – all I wanted to do was
bury my feelings in a box of cookies or a carton of
ice cream. Why do I always think the food will
help? Once I started eating I couldn’t stop. When
I finally did I felt even more disgusted, depressed,
and guilty. I am always on a diet but it is never
long before I lose control and pig out. I know my
eating and my weight are not healthy but I just
can’t seem to stop.
F I G U R E 7 . 2 5
People with binge-eating disorder binge but do not purge and are typically overweight. (Ken Ross/Taxi/Getty Images)
There are many people in theUnited States who are overweight,but there are also an alarmingnumber who just think they are. Onestudy reported that half of womensurveyed thought they were too fat,but only 17% of them wereoverweight.

228 Chapter 7 Managing Your Weight
People with eating disorders often try to use their relationship with food to gain con-trol over their lives and boost their self-esteem. They believe that controlling their foodintake and weight demonstrates their ability to control other aspects of their lives. Theirfixation with food and weight loss and their ability to control their intake and weighthelp them to feel better about themselves. Unfortunately, rather than solving the prob-lem this control of food intake creates additional physical and psychological problems.
Societal messages about the ideal body may promoteeating disorders While genetic and psychological issues may predispose anindividual to an eating disorder, societal and cultural factors are an important triggerfor the onset of these problems. Eating disorders occur in societies where food isabundant and the body ideal is thin. They do not occur where food is scarce and peo-ple must worry about where their next meal is coming from. Cultural ideals aboutbody size are linked to body image and the incidence of eating disorders.
Thinness is the ideal in American culture From television andmovies to magazines, advertisements, and even toys, messages about what societyviews as a perfect body are constantly delivered to us. The perfect body is long, lean,and muscled. The tall, dark, muscular man gets the girl; the thin, athletic woman getsher man. Thin fashion models slink down the runway to show off the latest clothes.These messages about how we should look are difficult to ignore and can create pres-sure to work toward this ideal body. But striving for this ideal can contribute to dis-turbances in body image and eating behavior. This is illustrated by the fact that as thebodies of female models, actresses, and other cultural icons have become thinner overthe last several decades, the incidence of eating disorders has increased (Figure 7.26).
Poor body image contributes to eating disorders Your bodyimage is the picture of your body that you form in your mind. It is how you perceiveand imagine yourself. When you look in the mirror you compare what you see withwhat you think you should look like (Table 7.11). Your definition of what you thinkyou should look like or wish you would look like is affected by the ideals of your cul-ture and society. Many women and girls, particularly teenagers, are not happy withtheir body because it looks different than what they see as ideal; for some this becomes
1900 – Actress Lillian Russell is considered a beauty at about 200 pounds
1920s – The thinner flapper look becomes popular
1950s – The curvy figure of Marilyn Monroe becomes the beauty standard
1960s – Twiggy, who weighs less than 100 pounds, is leading model
1980s – Jane Fonda’s workout book is a best seller
Today – The fashion ideal today is thin but well muscled
F I G U R E 7 . 2 6
Thinness has not always been the beauty standard in America. This timelineshows how the female body ideal has changed over the years. (top three photos:© Bettman/Corbis; bottom photo: Corbis Sygma)
After the introduction of Westernmedia to the Pacific Island of Fiji,the rates of body-image and eatingdisturbances increased. Beforethis, Fiji had had no thin-idealbody images.
Social pressures to have an idealbody aren’t limited to women. Formen a body ideal that is muscular,moderate in weight, and low in bodyfat is portrayed in action toys andsuper-hero cartoons. To look thetypical super-hero, the averagehealthy male would need to be 20inches taller, make his chest 11inches larger, and make his neck7.9 inches larger.

a pathological concern with body weight and shape, and their body image becomesdistorted. A distorted body image means you are unable to judge the size of your ownbody and do not see yourself as you really are. Distorted body image is common witheating disorders, so even if a young woman achieves a body weight comfortable to thatof a fashion model, she may continue to see herself as fat and strive to lose more weight.
Eating disorders are more common in groups concernedwith body weight Eating disorders are more prevalent in groups concernedwith weight and body image.66 For example, they are more common in professionaldancers and models and are on the rise among athletes, especially those involved insports that require the athlete to be thin, such as gymnastics and figure skating, or tofit into a particular weight class, such as wrestling. Eating disorders are far more com-mon in women than men. Only an estimated 5 to 15% of people with anorexia or bu-limia and an estimated 35% of those with binge-eating disorder are male.67
Identifying risks can help prevent eating disordersTo prevent eating disorders, it is important to first recognize factors that increase risk.Excessive concerns about body weight, having friends that are preoccupied withweight, being teased by peers about weight, and problems with one’s family all predis-pose people to eating disorders. There is an association between parental criticism andchildren’s weight preoccupation. Dieting also increases risk. Girls and women whodiet are more likely to develop an eating disorder than those who don’t diet. Thosewho have a mother, sister, or friend who diets are also at increased risk. Exposure tomedia pressure to be thin is also associated with the development of eating disorders.
Those who are at risk for eating disorders should be targeted for intervention. Forteens, parents play an important role. Arranging an evaluation with a physician and amental health specialist when risk factors, such as preoccupation with weight, are firstrecognized may help prevent the development of an eating disorder. More widespreadinterventions to prevent eating disorders can target the elimination of weight-relatedteasing and criticism from peers and family members. Another important target is themedia. If the unrealistically thin body ideal presented by the media could be altered,the incidence of eating disorders would likely decrease. Education through schoolsand communities about the symptoms and complications of eating disorders can helppeople identify friends and family members at risk and persuade those with earlysymptoms to seek help. Eating disorders are easier to prevent than to cure.
Eating Disorders Involve an Abnormal Concern with Body Weight and Shape 229
T A B L E 7 . 1 1Don’t Fall into the Body Image Trap
Try to• Accept that healthy bodies come in many shapes and sizes• Recognize your positive qualities• Remember that you can be your worst critic• Explore your internal self, as well as your external appearance• Spend your time and energy enjoying the positive things in your life• Be aware of your own weight prejudice; explore how those feelings may
affect your self-esteem.
And try not to• Let your body define who or what you are• Judge others on the basis of appearance, body size, or shape• Forget that society changes its ideas of beauty over the years• Forget that you are not alone in your pursuit of self-acceptance• Be afraid to enjoy life
Adapted from: www.mckinley.uiuc.edu/Handouts/bodyimage.htm.
Who are we modeling ourselvesafter? The fashion models womenwant to emulate are thinner than98% of American women. Theaverage American woman is 5�4�inches tall and weighs 140 pounds.The average fashion model is 5�11�inches tall and weighs 117 pounds.Medically, the typical fashion modelis in a weight range that is belowwhat is recommended for optimalhealth. The difference has beenincreasing. The average weight of amodel is 23% lower than that of anaverage woman; 40 years ago, thedifferential was only 8%.
To see if you are at riskfor an eating disorder,take the self-test at
Anorexia and RelatedEating Disorders, Inc., at
www.anred.com/slf_tst.html/

230 Chapter 7 Managing Your Weight
S U M M A R Y
1. The incidence of overweight and obesity in America hasrisen so much over the last 30 years that is has beencalled an epidemic. Excess body fat increases the risk ofchronic diseases such as diabetes, heart disease, highblood pressure, and certain types of cancer.
2. The risks associated with body weight can be assessedby determining Body Mass Index, body composition,and the location of body fat. Body fat located in theabdominal region (visceral fat) is a greater health riskthan subcutaneous fat in the hips and thighs.
3. The genes you inherit affect how much you weigh bycoding for proteins that help regulate how much youeat from meal to meal and the amount of fat you storeover the long term. Signals from the gastrointestinal(GI) tract, hormones, and circulating nutrients regulateshort-term hunger and satiety. Signals from fat cells,such as the release of leptin, regulate long-term energyintake and expenditure. Defects in one or more of thegenes that regulate body weight (called obesity genes)could lead to the storage of too much body fat.
4. Although what we weigh is greatly affected by genetics,environmental factors such as the availability of high-calorie foods and labor-saving devices, as well as
personal choices concerning the amount and type offood consumed and activity level, also affect bodyweight.
5. The principle of energy balance states that if energyintake equals energy needs, body weight will remainconstant. Energy is provided to the body by thecarbohydrate, fat, and protein in the food we eat. Thisenergy is used for basal metabolism, activity, and thethermic effect of food (TEF). Basal metabolism is theenergy needed to maintain body functions that keep usalive and is usually the largest component of energyexpenditure. The amount of energy expended foractivity can vary a great deal from person to person.TEF is the energy needed to digest and metabolizefood.
6. When excess energy is consumed, it is stored for lateruse. Fat is preferentially stored, while carbohydrate isused for energy and amino acids are used to meetprotein needs. When energy in the diet does not meetneeds, body energy stores are used.
7. The energy needs of healthy people can be predicted bycalculating estimated energy requirements (EER). YourEER depends on your gender, age, life stage, height,
T H I N K I N G F O R Y O U R S E L F
1. Are you in the healthy weight range?a. Use Figure 7.3 to determine if your BMI falls in the
healthy range.b. If your BMI is greater than 25, measure your waist
circumference. Does it indicate a risk due to visceralfat storage?
c. Even if you are not overweight, answer the followingquestions to see how many factors you have that mayincrease your risk of obesity-related complications ifyou become overweight.1. Do you have a personal or family history of heart
disease?2. Are you a male older than 45 years?3. Are you a postmenopausal female?4. Do you smoke cigarettes?5. Do you have a sedentary lifestyle?6. Do you have high blood pressure?7. Do you have high LDL cholesterol, low HDL
cholesterol, or high triglycerides?8. Do you have diabetes?
2. Are you in energy balance?a. Use the 3-day food record you kept in Chapter 2 to
calculate your average daily energy intake.
b. Keep an activity log for several days. Use Tables 7.5and 7.6 to determine your physical activity level andPA value. Calculate your EER. (See Table 7.7.)
c. How does your EER compare with your energy intake?d. If you consumed and expended this amount of energy
every day, would your weight increase, decrease, orstay the same?
e. If your intake does not equal your EER, how muchwould you gain or lose in a month? (Assume that apound of fat is equal to 3500 Calories)
f. If your energy intake does not equal your EER, listsome specific changes you could make in your diet orthe amount of activity you get to make the two balance.
3. How useful are low-calorie products?a. Go to the grocery store and select five to ten products
labeled “light,” “reduced-calorie,” “low-calorie,” or“calorie-free.” Record the number of Calories perserving.
b. Would any of these products be useful for someone ona weight-loss diet?
c. Can they be consumed in unlimited amounts withoutsignificantly increasing energy intake?
d. Rate these foods in terms of their nutrient density.

weight, and level of physical activity. As your level ofphysical activity increases, so does the number ofcalories you need to maintain your weight.
8. More Americans are overweight today because as apopulation we are taking in more calories, due to poorfood choices and larger portion sizes, and moving less,due to modern lifestyles that include computers, cars,and other conveniences that reduce energy expended inwork and play.
9. Weight management involves adjusting energy intakeand expenditure and modifying long-term behaviors tokeep weight in a healthy range. Whether you need tolose weight depends on how much body fat you have,where that fat is located, and what your health risks are.To lose a pound of fat, expenditure must be increased orintake decreased by approximately 3500 Calories. Slow,steady weight loss of 1/2 to 2 pounds per week is morelikely to be maintained than rapid weight loss.
10. There are thousands of diets that promise weight loss.All cause short-term weight loss because they decreaseenergy intake. A good weight-loss diet is one that allows
a wide variety of food choices, does not require thepurchase and consumption of special foods orcombinations of foods, and can be followed for life.
11. Drug therapy and surgery may be effective approachesto weight management in certain obese individuals.However, to be effective they must be accompanied bylong-term changes in diet and lifestyle.
12. Eating disorders are psychological disorders that involvedissatisfaction with body weight. Anorexia involves self-starvation resulting in an abnormally low body weight.Bulimia nervosa is characterized by repeated cycles ofbinge eating followed by purging and other behaviors toprevent weight gain. Binge-eating disorder ischaracterized by bingeing without purging, and peoplewith this disorder are typically overweight.
13. Eating disorders are caused by a combination of genetic,psychological, and sociocultural factors. The lean bodyideal in the United States is believed to contribute toeating disorders. Treatment involves psychologicalcounseling to change attitudes about body size andimprove eating habits while supplying an adequate diet.
References 231
R E V I E W Q U E S T I O N S
1. What health problems are associated with excess body fat?
2. Is Body Mass Index a measure of body composition?3. How does the distribution of body fat affect the risks
of excess weight?4. Define what is meant by a healthy weight.5. What is EER and what factors are used in its
calculation?6. What is energy balance?7. Which nutrients provide energy? How much does
each provide?
R E F E R E N C E S
1. Office of the Surgeon General. The Surgeon General’s Call toAction to Prevent and Decrease Overweight and Obesity. Rockville,MD: U.S. Department of Health and Human Services, 2001.Available online at www.surgeongeneral.gov/topics/obesity/Accessed March 4, 2004.
2. Mokdad, A. H., Marks, J. S., Stroup, D. F., and Gerberding, J. L. Actual causes of death in the United States. JAMA291:1238–1245, 2004.
3. National Institutes of Diabetes and Digestive and KidneyDiseases, Weight Control Information Network. Statistics Relatedto Overweight and Obesity. Available online at www.niddk.nih.gov/health/nutrit/pubs/statobes.htm#cost/Accessed April 1, 2002.
4. Centers for Disease Control and Prevention. Prevalence ofOverweight and Obesity Among Adults: United States 1999–2000.Available online at www.cdc.gov/nchs/releases/02news/obesityonrise.htm/ Accessed March 16, 2004.
5. American Obesity Association. Obesity—A Global Epidemic.Available online at www.obesity.org/subs/fastfacts/obesity_global_epidemic.shtml/ Accessed July 15, 2004.
6. Wang, Y., Monteiro, C., and Popkin, B. Trends of obesity andunderweight in older children and adolescents in the UnitedStates, Brazil, China, and Russia. Am. J. Clin. Nutr. 75:971–977,2002.
7. International Union of Nutritional Scientists. The Global Challengeof Obesity and the International Obesity Task Force Obesity Epidemic.Available online at www.iuns.org/ Accessed July 15, 2004.
8. Eisenberg, M. E., Neumark-Sztainer D., and Story, M. Associationsof weight-based teasing and emotional well-being amongadolescents. Arch. Pediatr. Adolesc. Med. 157:733–738, 2003.
9. Strauss, R. S., and Pollack, H. A. Social marginalization ofoverweight children. Arch. Pediatr. Adolesc. Med. 157:746–752,2003.
10. Onyike, C. U., Crum, R. M., Lee, H. B., et. al. Is obesityassociated with major depression? Results from the ThirdNHANES. Am. J. Epidemiol. 158:1139–1147, 2003.
11. Gallagher, D., Heymsfield, S., Heo, M., et al. Healthy percentagebody fat ranges: an approach for developing guidelines based onbody mass index. Am. J. Clin. Nutr. 72:694–701, 2000.
8. List three components of energy expenditure.9. What is basal metabolic rate?
10. List some environmental factors that affect energybalance. How might these affect an individual’s geneticpredisposition to a particular weight?
11. Discuss the advantages and disadvantages of threedifferent approaches to reducing energy intake.
12. What is the best approach to weight management? Why?13. What are the characteristics of anorexia nervosa?14. What are the differences between bulimia nervosa
and binge-eating disorder?

232 Chapter 7 Managing Your Weight
12. National Institutes of Health, National Heart, Lung, and BloodInstitute. The Practical Guide: Identification, Evaluation andTreatment of Overweight and Obesity in Adults. NIH publicationno. 02-4084. Bethesda, MD: National Institutes of Health, 2002.
13. Bosello, O., Armellini, S., Zamboni, M., and Fitchet, M. Thebenefits of modest weight loss in type II diabetes. Int. J. Obes.Relat. Metab. Disord. 21(Suppl):S10–S13, 1997
14. Katzmarzyk, P. T., Craig, C. L., and Bouchard, C. Underweight,overweight and obesity: Relationships with mortality in the 13-year follow-up of the Canada Fitness Survey. J. Clin. Epidemiol.54:916–920, 2001.
15. Bouchard, C., Tremblay, A., Després, J.-P., et al. The response to long term feeding in identical twins. N. Engl. J. Med.322:1477–1482, 1990.
16. Conway, J. M. Ethnicity and energy stores. Am. J. Clin. Nutr.62(Suppl):1067S–1071S, 1995.
17. Albu, J., Allison, D., Boozer, C. N., et al. Obesity solutions:Report of a meeting. Nutr. Rev. 55:150–156, 1997.
18. Chagnon, Y. C., Rankinen, T., Snyder, E. E., et al. The humanobesity gene map: the 2002 update. Obes. Res. 11:313–367,2003.
19. Schwartz, M. W., Baskin, D. G., Kaiyala, K. J., and Woods, S. C.Model for the regulation of energy balance and adiposity by thecentral nervous system. Am. J. Clin. Nutr. 69:584–596, 1999.
20. Cummings, D. E., Weigle, D. S., Frayo, R. S., et al. Plasmaghrelin levels after diet-induced weight loss or gastric bypasssurgery. N. Engl. J. Med. 346:1623–1630, 2002.
21. Batterham, R.L., Cowley, M.A., Small, C.J., et al. Gut hormonePYY(3-36) physiologically inhibits food intake. Nature418(6898):650–654, 2002.
22. Friedman, J. M. The alphabet of weight control. Nature385:119–120, 1997.
23. Peters, J. C., Kriketos, A. D., and Hill, J. O. Control of energybalance. In Biochemical and Physiological Aspects of HumanNutrition. Stipanuk, M. H., ed. Philadelphia: WB Saunders,2000: 425–438.
24. Tsigos, C., Kyrou, I., and Raptis, S. A. Monogenic forms ofobesity and diabetes mellitus. J. Pediatr. Endocrinol. Metab.15:241–253, 2002.
25. Schoeller, D. A. Recent advances from application of doubly-labeled water to measurement of human energy expenditure. J. Nutr. 129:1765–1768, 1999.
26. Diaz, E. O., Prentice, A. M., Goldberg, G. R., et al. Metabolicresponse to experimental overfeeding in lean and overweighthealthy volunteers. Am. J. Clin. Nutr. 56:641–655, 1992.
27. Gura, T. Uncoupling proteins provide new clues to obesity’scauses. Science 280:1369–1370, 1998.
28. Lisette, C. P., de Groot, G. M., and van Staveren, W. A. Reducedphysical activity and its association with obesity. Nutr. Rev.53:11–18, 1995.
29. Levine, J. A., Eberhardt, N. L., and Jensen, M. D. Role ofnonexercise activity thermogenesis in resistance to fat gain inhumans. Science 283:212–214, 1999.
30. Bouchard, C. Genetics of human obesity: Recent results fromlinkage studies. J. Nutr. 127:1887S–1890S, 1997.
31. Norman, R. A., Thompson, D. B., Foroud, T., et al. Genomewidesearch for genes influencing percent body fat in Pima Indians:Suggestive linkage at chromosome 11q21-q22. Am. J. HumanGenet. 60:166–173, 1997.
32. Esparza, J., Fox, C., Harper, I. T., et al. Daily energy expenditurein Mexican and USA Pima Indians: Low physical activity as apossible cause of obesity. Int. J. Obes. Relat. Metab. Discord.24:55–59, 2000.
33. Institute of Medicine, Food and Nutrition Board. DietaryReference Intakes for Energy, Carbohydrate, Fiber, Fat, Protein andAmino Acids. Washington, DC: National Academy Press, 2002.
34. Wadden, T. A., Foster, G. D., Letizia, K. A., and Muller, J. L.Long-term effects of dieting on resting metabolic rate in obesepatients. JAMA 264:707–711, 1990.
35. Horten, T. S., Drougas, H., Brachey, A., et al. Fat andcarbohydrate overfeeding in humans: Different effects on energy storage. Am. J. Clin. Nutr. 62:19–29, 1995.
36. Hellerstein, M. K. De novo lipogenesis in humans: metabolicand regulatory aspects. Eur. J. Clin. Nutr. 53 (Suppl. 1):S53–S65,2000.
37. Hill, J. O., and Peters, J. C. Environmental contributions to theobesity epidemic. Science 280:1371–1374, 1998.
38. Young, L. R., and Nestle, M. The contribution of expandingportion size to the obesity epidemic. Am. J. Public Health92:246–249, 2002.
39. Rolls, B. J., Morris, E. L., and Roe, L. S. Portion size of foodaffects energy intake in normal-weight and overweight men andwomen. Am. J. Clin. Nutr. 76:1207–1213, 2002.
40. Bassett, D. R., Schneider P. L., and Huntington, G.E. Physicalactivity in an Old Order Amish community. Med. Sci. SportsExerc. 36:79–85, 2004.
41. Hill, J. O., Wyatt, H. R., Reed, G. W., and Peters, J. C. Obesityand the environment: where do we go from here? Science299:853–855, 2003.
42. U.S. Department of Agriculture, U.S. Department of Health andHuman Services. Nutrition and Your Health: Dietary Guidelinesfor Americans, 5th ed. Home and Garden Bulletin no. 232.Hyattsville, MD: U.S. Government Printing Office, 2000.
43. National Institutes of Health, National Heart, Lung, and BloodInstitute. Clinical Guidelines on the Identification, Evaluation, andTreatment of Overweight and Obesity in Adults. Executivesummary, June 1998. Available online at www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm/ Accessed January 5, 2001.
44. American Dietetic Association. Position of the American DieteticAssociation: Weight management. J. Am. Diet. Assoc. 97:71–74,1997.
45. Stevens, J., Cai, J., Pamuk, E. R., et al. The effect of age on theassociation between body mass index and mortality. N. Engl. J.Med. 338:1–7, 1998.
46. Wilmore, J. H. Increasing physical activity: alterations in bodymass and composition. Am. J. Clin. Nutr. 63(suppl):456S–460S,1996.
47. American Dietetic Association. Position of the American DieteticAssociation: very-low-calorie weight-loss diets. J. Am. Diet. Assoc.94:722–726, 1990.
48. Horten, T. S., Drougas, H., Brachey, A., et al. Fat andcarbohydrate overfeeding in humans: Different effects on energystorage. Am. J. Clin. Nutr. 62:19–29, 1995.
49. Willett, W .C. Dietary fat plays a major role in obesity: no. Obes.Rev. 3:59–68, 2002.
50. Frackelmann, K. Diet drug debacle: How two federally approvedweight-loss drugs crashed. Science News 152:252–253, 1997.
51. Kurtzweil, P. Dieter’s brews make tea time a dangerous affair. FDAConsumer 31: July–August, 1997. Available online atwww.fda.gov/fdac/features/1997/597_tea.html/ AccessedFebruary 18, 2004.
52. Flancbaum, L., and Choban, P. S. Surgical implications of obesity.Ann. Rev. Med. 49:214–234, 1998.
53. American Psychiatric Association. Diagnostic and StatisticalManual, 4th ed. Washington, DC: American PsychiatricAssociation, 1994.
54. Anorexia Nervosa and Related Eating Disorders, Inc. (ANRED).Statistics: How many people have eating disorders? Availableonline at www.anred.com/stats.html/ Accessed April 2, 2002.
55. Foreyt, J. P., Poston, W. S. C., II, and Goodrick, G. K. Futuredirections in obesity and eating disorders. Addict. Behav.21:767–778, 1996.

56. Medical Sciences Bulletin. Serotonin and eating disorders.Available online at www.pharminfo.com/pubs/msb/serotonin.html/ Accessed April 18, 2000.
57. Rock, C. L., and Curran-Celentano, J. Nutritional managementof eating disorders. Psychiatr. Clin. North Am. 19:701–713, 1996.
58. Vandereycken, W. History of anorexia nervosa and bulimianervosa. In Eating Disorders and Obesity: A ComprehensiveHandbook, 2nd ed. Fairburn, C. G., and Brownell, K. D, eds.New York: The Guilford Press, 2002:151–154.
59. American Dietetic Association. Position of the AmericanDietetic Association. Nutrition intervention in the treatment of anorexia nervosa, bulimia nervosa, and eating disorders nototherwise specified (EDNOS). J. Am. Diet. Assoc.101:810–819, 2001.
60. Kaye, W. H., Weltzin, T. E., McKee, M., et al. Laboratoryassessment of feeding behavior in bulimia nervosa and healthywomen. Methods of developing a human feeding laboratory. Am.J. Clin. Nutr. 52:8000–8007, 1992.
61. Anderson, L., Shaw, J. M., and McCargar, L. Physiological effectsof bulimia nervosa on the gastrointestinal tract. Can. J.Gastroenterol. 11:451–459, 1997.
62. Keel, P. K., and Mitchell, J. E. Outcome in bulimia nervosa. Am. J. Psychiatry 154:313–321, 1997.
63. National Eating Disorders Association. Statistics: Eating disordersand their precursors. Available online atwww.edap.org/edinfo/stats2.html/ Accessed March 2, 2004.
64. Walsh, B. T., and Devlin, M. J. Eating disorders: progress andproblems. Science 280:1387–1390, 1998.
65. Branson, R., Potoczna, N., Kral, J. G. et al. Binge eating as amajor phenotype of melanocortin 4 receptor gene mutations. N. Engl. J. Med. 348:1096–1103, 2003.
66. Hsu, L. K. Epidemiology of the eating disorders. Psychiatr. Clin.North Am. 19:681–700, 1996.
67. American Psychiatric Association. Practice Guidelines for theTreatment of Patients with Eating Disorders, 2000. Available onlineat www.psych.org/clin_res/guide.bk42301.cfm.
References 233