Embed Size (px)
Citation preview
Do you need a cuppa?
Dr. Anushma Sharma
ST5 Paediatrics
Department of Community Paediatrics Salford
AIM
1. Present an interesting case
2. Discuss the outcome
3. Discuss the causes of the presenting symptoms
Admission 1
1 year old
Vomiting, loose stools, unwell
Tachycardiac, irrtable, breathless
Metabolic acidosis – pH 7.13, pCO2 2.2, BE -23 , Lac 27, Glu 5.3
Improved quickly within 12 hours with ventilatory support and fluids + sodium bicarbonate correction
Metabolic disorder suspected
Investigations
ammonia
acyl carnitine
plasma amino acids
free fatty acids
urine organic and amino acids
LFT and renal funtions
salicylate levels
Admission 2
13 months
Had been well
Found unresponsive on bedroom floor at 0800
No hypoglycaemia
Severe metabolic acidosis pH 6.91, pCO2 2.96, Bicarb 4.3, BE -27.9, lactate>30
Sent to PICU and recovered in 12 hours
Skin biopsy and toxicology investigations
Previously.....
Parents 18 years old, both unemployed, separated
H/o domestic violence
Good pregnancy
NVD
No significant neonatal diagnoses
Satisfactory growth and development
Previously............
7 weeks old
Unwitnessed fall from sofa while being watched by mother's friend
Attended A+E promptly
Parietal skull fracture
Discharged back to mother after child protection investigations
11th admission
Recent Burn????
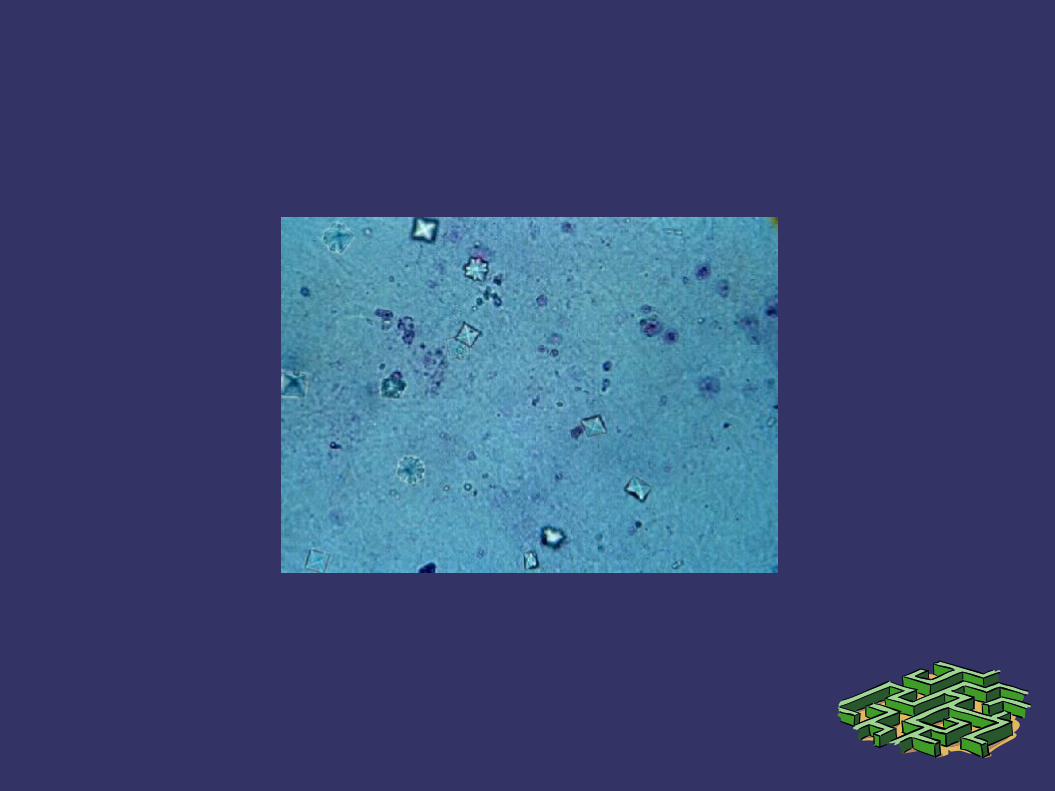
Toxicology
Urine positive for Glycolate
Antifreeze= Ethylene Glycol
Colourless
Odourless
Very sweet
Present in Radiator fluid, Deicer, Wind screen wash, Window cleaning fluid

Fake vodka health warning in UK
ingestion.
Counterfeit vodka seized by council trading standard teams. Photograph: Nottinghamshire County Council/PA
The Guardian, Saturday 31 December 2011
Ethylene Glycol Toxicity
Toxic dose requiring medical trematment is 0.1ml/kg body weight or 4 ml for 20 Kg child
Lethal dose in humans is 1.4ml/kg or 56 ml for a 20 kg child
Ethylene glycol does not evaporate so inhalational exposure is unlikelyEthylene glycol is not absorbed through skin so dermal exposure is also uncommon
OutcomeOutcome
Forensic samples obtained
Police investigations started and mother was taken in custody
BC and sister 10 months old in foster care
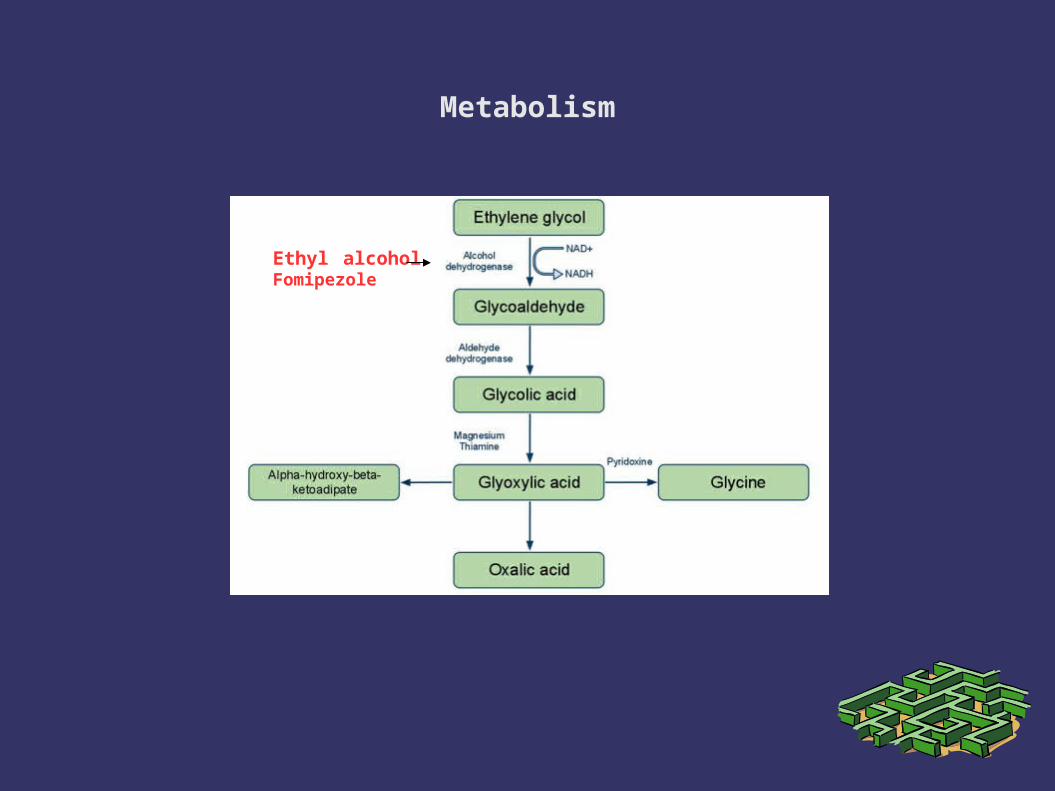
Metabolism
Ethyl alcoholFomipezole
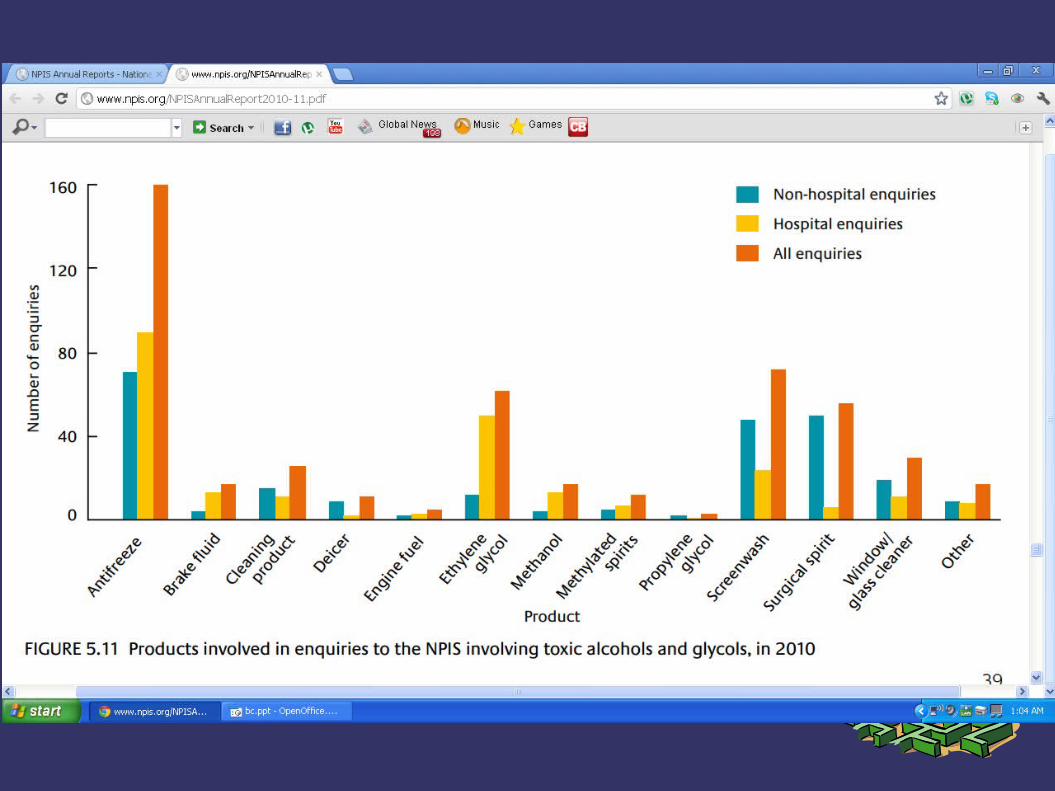
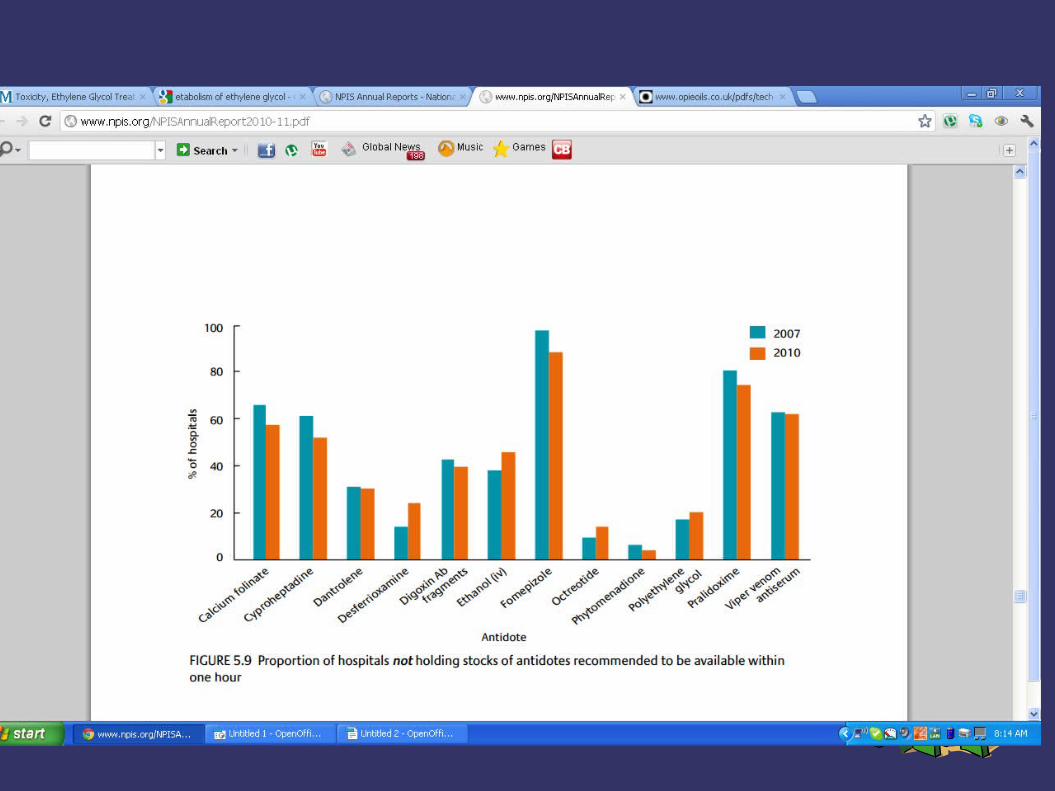
NPIS annual Report 2010-2011
➲ Prospective audit➲ Toxic alcohol and glycol cases reported through telephone
enquiries to the NPIS in 2010➲ Aim: 1. To provide information on the frequency, current
management and outcomes of systemic toxic alcohol poisoning.2. To provide information on which to base the planning of clinical services for this type of poisoning, including appropriate availability of assays and antidotes.
Results
➲ 488 individual exposures➲ 250 in non hospital sourced
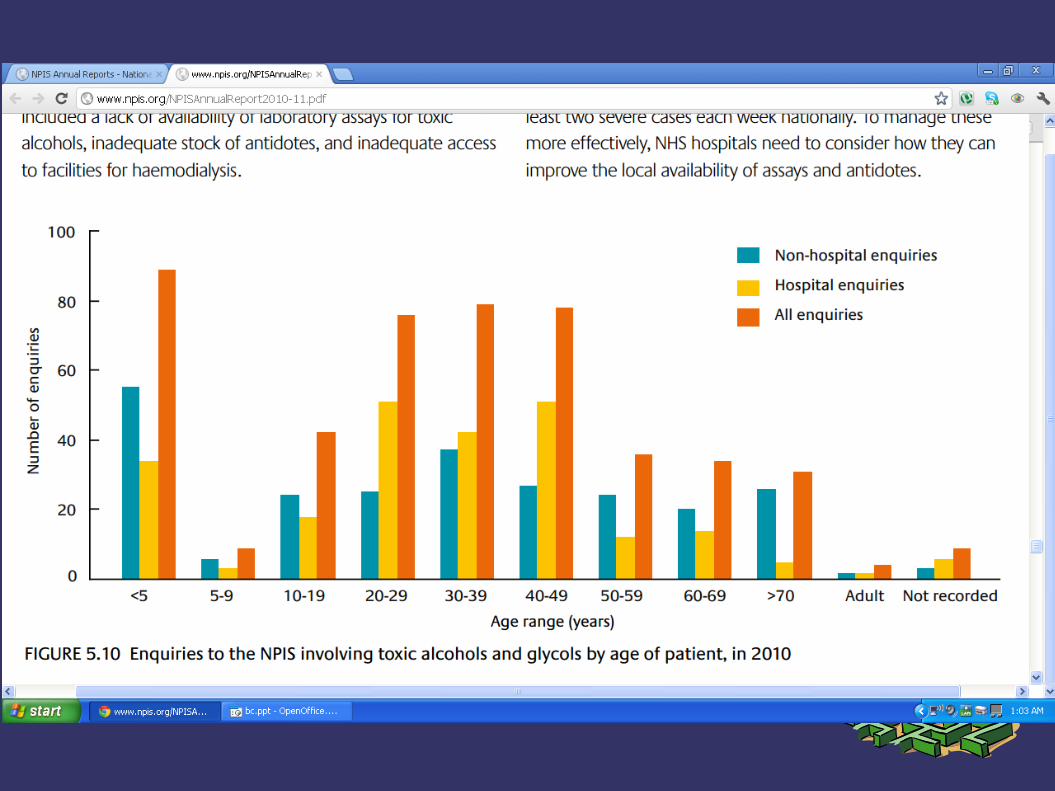
➲ 89 (18%) cases less than 5 years old➲ 238 in hospital sources➲ 182 potentially systemic exposures
➲ 99 (20%) reqiured treartment with antidotes➲ 33 haemodialysis, heamofiltration➲ At least 2 severe cases each week nationally
➲ Main difficulty in management is unavailability of lab assayand inadequate stock of antidote
Summary
➲ Glycol and Toxic alcohol toxicity though less common in UK is a significant differntial diagnosis to consider especially in cases of disproportionate metabolic acidosis
➲ It is important to plan and consider how we can treat such a case in our unit, especially when most of us donot stock any of the antidotes
Questions?






























