-
8/2/2019 Doaa Doctor Paper
1/12
ABSTRACT
Introduction: Anthracyclines repre-
sent one of the most important
chemotherapeutics in breast cancer.
However, they cause cardiac damage
besides some tumors might be anthra-
cycline-resistant.
Aim of the work: The aim of the pre-
sent work was to study the predictive
value of human epidermal growth fac-
tor receptor 2 (HER2/neu) protein,
state (positive or negative) and score
(0,1+,2+,3+), for the outcome of 5-
fluorouracil / Adriamycin / cyclophos-
phamide (FAC) adjuvant chemother-
apy in Egyptian high risk female
breast cancer patients.
Subjects & Methods: The present ret-
rospective cohort study was conducted
in Alexandria Main University Hospi-tal, Egypt. It included
fifty high risk
female breast cancer patients
(according to St Gallen guidelines
2007) with operable breast cancer. All
of them have received FAC adjuvant
chemotherapy between January 2007
and December 2007 and were followed
for 2 years. Pretreatment breast tu-
mor samples were obtained from for-
malin fixed/paraffin-embedded tissue
blocks where HER2/neu protein was
assessed by immunohistochemistry
(IHC).
Results: Kaplan-Meier survival analy-
sis showed that positive HER2/neustate was associated with
superior 2-
year disease free survival (DFS) and
overall survival (OS) rates to negative
HER2/neu state but this difference
was statistically insignificant (log rank
p=0.08 and 0.24 respectively). On the
other hand, there was a statistically
significant difference between 2-year
DFS rate of different HER2/neu pro-
tein score categories (log rank
p=0.001*). Although being statistically
significant, there was no pattern be-
tween HER2/neu protein scoring andDFS where score 0 showed
intermedi-
ate DFS rate between scores 2+ and
3+. Moreover, Cox regression analysis
showed that HER2/neu protein score
couldnt be an independent predictor
for the outcome (DFS) of FAC adju-
vant chemotherapy (p=0.66).
THE PREDICTIVE VALUE OF HUMAN EPIDERMAL GROWTH FACTOR
RECEPTOR 2 (HER2/neu) FOR THE OUTCOME OF ANTHRACYCLINE-
BASED ADJUVANT CHEMOTHERAPY IN EGYPTIAN HIGH RISK FEMALE
BREAST CANCER PATIENTS
Ahmed N. Abd El-Aal1, Nashaat S. Lotfy
2, Ehsan M. H. Abd Al-Rahman
1,
Suzan M. F. Helal3, Eman M. S. Kamha
1, Doaa A. Abd Al-Monsif
1,
Mohammed S. Shaat4, Ahmed S. Anan4.Departments of Medical
Biochemistry1, Clinical Oncology and Nuclear Medicine2,
Pathology3, andUndergraduate students
4, Faculty of Medicine,
Alexandria University, Egypt.
THE EGYPTIAN JOURNAL OF MEDICAL SCIENCES VOL. 32-No. 1 JUNE 2011
(ISSN: 1110-0540)
8. Egypt. J. Med. Sci. 32 (1) June 2011: 107-118.
-
8/2/2019 Doaa Doctor Paper
2/12
Conclusion: HER2/neu protein might-
nt be considered as a predictor for the
outcome of FAC adjuvant chemother-
apy in Egyptian high risk female
breast cancer patients. Consequently,
large-scale prospective studies will be
needed to clearly define its predictive
value.
INTRODUCTION
Breast cancer is the most com-
monly diagnosed cancer in womenworldwide and is the second
leading
cause of deaths in women after lung can-
cer (Jemal et al., 2009). In Egypt, breast
cancer is the most prevalent cancer
among women where it constitutes 29%
of the National Cancer Institute cases
(Omar et al., 2003). Breast cancer, like
all malignancies, arises as a result of the
accumulation of genetic alterations, espe-
cially deregulation of the expression ofoncogenes and tumor
suppressor genes
(Omar et al., 2003). One of the most im-
portant adjuvant chemotherapeutics usedin breast cancer are
anthracycline-based
combinations (Buzdar, 2006). A major
component of anthracycline cytotoxicity
is due to topoisomerase II (TOPOII) poi-
soning. Moreover, they intercalate into
double-stranded deoxyribonucleic acid
(dsDNA) and produce structural changes
that interfere with DNA and ribonucleic
acid (RNA) synthesis. Besides, anthracy-
clines generate reactive oxygen species
(ROS) that damage DNA, messenger
RNA (mRNA), proteins and lipids; the
peroxidation of lipids may account formuch of the cardiac
toxicity characteris-
tic of these drugs (Rubin and Hait, 2003).Several predictive
factors that
might affect the outcome of chemother-
apy in breast cancer were studied but
none of them was proved to have enough
predictive power (Tewari et al., 2008).
Consequently, the choice of chemothera-
peutic drugs in breast cancer is usually
empiric and 30%70% of patients with
measurable disease fail to respond
(Kennedy et al., 2004). Additionally,
financing cancer treatment is a major
challenge especially for developing coun-
tries (Boutayeb et al., 2010). From here
comes the importance of predictive fac-
tors in tailoring of chemotherapy.The human epidermal growth
factor
receptor 2 gene is localized to chromo-some 17q11.2-12. It
encodes a 185 kDa
transmembrane tyrosine kinase receptor
that is a member of the epidermal growth
factor receptor (EGFR) family (Siddig etal., 2008). These
proteins possess an ex-
tracellular ligand-binding domain, a
membrane-spanning region and a cyto-
plasmic domain with tyrosine kinase ac-
tivity (Duffy, 2005). After heterodimeri-
zation, HER2/neu complexes initiate
intracellular signaling via the Ras/
mitogen-activated protein kinase
(MAPK) pathway, the phosphatidylinosi-
tol 3-kinase (PI3K) pathway, the Janus
kinase (JAK)/signal transducer and acti-vator of transcription
(STAT) pathway
and the phospholipase C-gamma (PLC-)
pathway. Activation of the latter path-
ways ultimately promote cell prolifera-
tion, survival, motility and adhesion
(Duffy, 2005). HER2/neu is overex-pressed in 15-25% of patients
with breast
cancer and was reported to be an unfa-
vorable prognostic factor in breast cancer
(Tewari et al., 2008). Furthermore, the
possible relation between HER2/neu
overexpression and the outcome of an-
thracycline-based regimens in breast can-
cer was hypothesized (Zhang and Liu,
2008).
The aim of the present work was to
reveal the possible predictive value ofHER2/neu protein, state
(positive or
108 Abd El-Aal et al.
Egypt. J. Med. Sci. 32 (1) 2011
-
8/2/2019 Doaa Doctor Paper
3/12
negative) and score (0, 1+, 2+, 3+), for
the outcome of anthracyclinebased ad-
juvant chemotherapy in Egyptian high
risk female breast cancer patients. The
predictive value was assessed in terms of
disease free survival (DFS), overall sur-
vival (OS) as well as time of relapse and
type of relapse (local or distant). DFS
was defined as the time between the date
of randomization and the date of diseaserelapse and OS was
defined as the time
between randomization and death from
any cause. Cardiotoxicity from anthracy-
cline and mortality were recorded as
well.
SUBJECTS & METHODS
The present retrospective cohort
study was conducted in Alexandria Main
University Hospital, Egypt. It included
fifty high risk female breast cancer pa-
tients according to St Gallen guidelines2007 (Goldhirsch et al.,
2007). Patients
were randomly recruited from the Clini-cal Oncology Department.
All of them
have received anthracyclinebased
(FAC) adjuvant chemotherapy between
January 2007 and December 2007. Pre-treatment breast tumor
samples were
obtained from formalin fixed/paraffin-
embedded tissue blocks, in accordance
with the standard methods, from the ar-
chives of the Pathology Department.
Before starting the treatment, all patientsunderwent a complete
physical examina-
tion, laboratory and radiological investi-
gations. Diagnosis was confirmed by afine needle aspiration
(FNA) or a core
biopsy of the primary tumor. Modified
radical mastectomy was the standard line
of treatment. After surgery, all patients
received 6 cycles of FAC and postmas-
tectomy irradiation. In addition, hormone
receptors [estrogen receptors (ER) and/or
progesterone receptors (PR)] positive
cases were assigned to receive tamoxifen
for a period of 5 years. After finishing
FAC-adjuvant chemotherapy, patients
were followed every 2 months for a pe-
riod of 2 years to detect local recurrence
or distant metastasis. In addition, cardio-
toxicity from anthracycline and mortality
were recorded. During the follow-up
period, patients were subjected to: thor-ough clinical
examination, laboratory
investigations, periodic radiological ex-
amination, ejection fraction and electro-
cardiogram (ECG) when needed. An
informed consent was taken from every
patient and the study was approved bythe Institutional Ethics
Committee. All
breast cancer tumor samples were sub-
jected to full histopathological examina-
tion. ER and PR states were determined
as well (Tafjord et al., 2002). Further-
more, breast cancer tumor samples were
subjected to the following assay:
Immunohistochemical (IHC) stainingprotocol of HER 2/neu
protein
Human epidermal growth factor
receptor 2 overexpression was assessedby IHC using primary
monoclonal anti-
body for HER2/neu [LabVision Corpora-
tion (Neo Markers, Fremont, USA)
http://www.labvision.com]. Expression
of HER2/neu was visualized using the
streptavidin-biotin-immunoenzymaticantigen detection system
which was per-
formed in accordance to the manufac-
turer's protocol (Rocha et al., 2009). Posi-tive and negative
controls were included
in all runs. Positive HER2/neu immu-
nostaining was defined as brown cell
membrane staining of the breast cancer
tissue. The threshold for Her2/neu was
assessed as described: no staining at all
or membrane staining in
-
8/2/2019 Doaa Doctor Paper
4/12
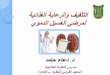
observed tumor cells was considered
negative (0). A faint/barely perceptible
membrane staining in >10% of tumor
cells or staining of part of their mem-
brane was scored as negative (1+). A
weak to moderate staining of the entire
membrane in >10% of the tumor cells
was considered weakly positive (2+). A
moderate to strong staining of the entire
membrane in >10% of the tumor cellswas scored as strongly
positive (3+)
(Orlando et al., 2008). HER2/neu protein
state was classified into negative (score 0
and 1+) and positive (score 2+ and 3+)
(Orlando et al., 2008) (Fig. 1).
Statistical Analysis
Demographic data including diag-
nosis details, tumor characteristics, che-
motherapy scheme, toxicity and outcome
were entered prospectively into a data-
base. Continuous data were expressed asmean (for normally
distributed data) or
median (for abnormally distributed data)and range between
parentheses. Qualita-
tive data were presented as absolute
numbers and percentages. Survival
curves were obtained by the KaplanMeier method. Differences
between the
survival curves were investigated using
the log-rank univariate analysis. A re-
gression analysis based on the Cox pro-
portional hazards model was conducted
using selected covariates to reveal thepossible independent
predictors for DFS
and OS. Mann-whitney test was used to
assess the possible effect of HER2/neuprotein on the time of
relapse. Chi-
square test was conducted to assess the
possible relation between HER2/neu
protein and the type of relapse. Data
were analyzed using SPSS software
package version 18.0. All statistical tests
were two sided and probability values of
p
-
8/2/2019 Doaa Doctor Paper
5/12
couldnt be an independent predictor for
better DFS after FAC therapy (p=0.66)
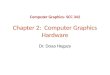
(Table 2). Positive HER2/neu protein
state was associated with a superior 2-
year OS rate (83.3%) which was statisti-
cally insignificant from negative HER2/
neu protein state (69.2%) (log rank
p=0.24) (Table 2, Fig. 2B). Furthermore,
there was a statistically insignificant
difference between 2-year OS rate ofdifferent HER2/neu protein
score catego-
ries (log rankp=0.31) (Table 2, Fig. 2B).
Among the relapsed patients, HER2/neu
failed to show a significant relation to
the type of relapse (p=0.11) (Table 3).
Moreover, it had no significant effect on
the time of relapse (HER2/neu positive
state: 10 cases, mean=10.95.32 months;
HER2/neu negative state: 18 cases,
mean=12.385.86 months; Mann-
whitneyp=0.48).
Figure 1.
A. Weak cytoplasmic positive stain with no membranous stain of
all tumor cells
[(negative score 0) immunostain HER2/neu (X40)].B. faint barely
perceptible membrane stain in more than 10% of cells [(negative
score 1+)
immunostain HER2/neu (X20)].
C. moderate stain of all membrane in 10% of cells [(weak
positive score 2+) immu-
nostain HER2/neu (X40)].
D. strong positive staining of the whole membrane, in all tumor
cells [(positive score 3+)
immunostain HER2/neu (X20)].
HER2/neu Value in Anthracycline Therapy in Breast Cancer 111
Egypt. J. Med. Sci. 32 (1) 2011
-
8/2/2019 Doaa Doctor Paper
6/12
Figure 2.
A. Kaplan-Meier disease free survival (DFS) curve for
FAC-treated breast cancer casesin Alexandria, Egypt, according
to:
A1. HER2/neu protein state.
A2. HER2/neu protein score.
B. Kaplan-Meier overall survival (OS) curve for FAC-treated
breast cancer cases in Al-
exandria, Egypt, according to:B1. HER2/neu protein state.
B2. HER2/neu protein score.
Kaplan-Meier curves were plotted in Harvard Graphics.
112 Abd El-Aal et al.
Egypt. J. Med. Sci. 32 (1) 2011
-
8/2/2019 Doaa Doctor Paper
7/12
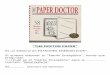
Table (1): Clinicopathological features of the studied
patients
Variable No. %
Age
-
8/2/2019 Doaa Doctor Paper
8/12
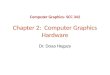
Table (2): Univariate (Log Rank) and multivariate (Cox
proportional hazards regression)
analysis for the HER2/neu protein state and score according to:
A. disease free survival(DFS) and B. overall survival (OS)
BiomarkerLog Rank Test
Cox Proportional Hazards
Regressiona
p valueb
p value Exp(B)c
A. DFS
HER2/neu Protein State 0.08 - -
HER2/neu Protein Score 0.001* 0.66 -
B. OS
HER2/neu Protein State 0.24 - -
HER2/neu Protein Score 0.31 - -
a. The significant parameters in log rank univariate analysis
were included in Cox pro-
portional hazards regression analysis to reveal the possible
independent predictorsfor DFS. By log rank test, except for tumor
type and ER protein state (log rank
p=0.001* and 0.000* respectively), none of the
clinicopathological characteristics of
patients were significantly related to DFS, so only tumor type
and ER state were
included in the regression analysis.
b. All statistical tests are two sided and probability (p) value
of
-
8/2/2019 Doaa Doctor Paper
9/12
DISCUSSION
Analysis of DFS curve for HER2/neu showed a discrepancy between
the
results of survival of HER2/neu protein
state and that of HER2/neu protein score
categories. Additionally, although the
latter was statistically significant, there
was no pattern between HER2/neu pro-tein scoring and DFS as
patients with
score 0 had intermediate DFS rate be-
tween scores 2+ and 3+. By Cox regres-sion analysis, HER2/neu
protein might-
nt be an independent predictor for better
DFS after FAC therapy. These discrep-ancies could probably be
explained by
the relatively small number of patients in
each HER2/neu protein score category
and/or possible IHC fallacies that might
be due to loss of HER2/neu protein as a
result of tissue storage and fixation
(Duffy, 2005). Regarding OS, although
positive HER2/neu protein state was
associated with a superior 2-year OS rate
to negative HER2/neu protein state, thisdifference was
statistically insignificant.Besides, there was a statistically
insig-
nificant difference between 2-year OS
rate of different HER2/neu protein score
categories. The latter results could be
explained by the relatively short duration
of follow-up and small number of pa-
tients in each HER2/neu protein score
category. In addition, Knoop et al.
(2005), had reported that recurrence is a
more precise measurement to outcome
than death as patients often have re-
ceived other treatment after their firstrelapse. Therefore, the
effect of treat-
ment would confound the true predictive
impact of the tested biomarker. Studies
reported the possible relation between
HER2/neu protein and the outcome ofanthracycline-based
chemotherapy
(Tubbs et al., 2009 & Konecny et al.,
2010). Additionally, HER2/neu-positive
tumors have been shown to have higherproliferation rate which
might make
these tumors more sensitive to chemo-
therapy (Paik et al., 2008). On the other
hand, other studies showed conflicting
results which led to the suggestion that
HER2/neu could be a surrogate marker
for the true predictor(s) of anthracycline
sensitivity (Bozzetti et al., 2006 &
Munro et al., 2010). The current results,
although statistically insignificant, sug-
gested that 30.8% of HER2/neu negative
patients had better outcome (no relapse)after FAC therapy,
making it difficult to
exclude FAC therapy in HER2/neu nega-
tive patients. This result is in agreement
to published reports (Esteva and Horto-
bagyi, 2009 and Miyoshi et al., 2010).
Furthermore, Miyoshi et al. (2010) ex-plained such observation
through a sub-
set of HER2/neu-negative tumors (triple-
negative and basal-like breast cancer
subtypes) that were proposed to possess
a specific molecular phenotype. Such
phenotypes might partially explain the
sensitivity of some HER2/neu-negative
tumors to anthracycline treatment. In
addition, there might be an interplay of
other factors which gives further support
to the use of a panel of predictive mark-ers, rather than a
single one, for tailoring
of chemotherapy. Among the relapsed
patients, HER2/neu failed to show a sig-
nificant relation to the type of relapse.
HER2/neu had no significant effect on
the time of relapse as well. In contrary tothese results,
Freudenberg et al. (2009)
reported the possible role of HER2/neu
in regulating different aspects of tumor
growth and progression possibly through
increasing motility of tumor cells, de-
creasing apoptosis, enhancing signaling
interactions with the tumor microenvi-
HER2/neu Value in Anthracycline Therapy in Breast Cancer 115
Egypt. J. Med. Sci. 32 (1) 2011
-
8/2/2019 Doaa Doctor Paper
10/12
ronment, regulating adhesion, as well as
a multitude of other functions. The cur-rent results could be
explained by the
limited number of the relapsed cases
and/or FAC therapy which might have
muffled the possible relation between
HER2/neu and each of time and type of
relapse.
In conclusion, HER2/neu protein
mightnt be considered as a predictor for
the outcome of FAC adjuvant chemo-therapy in Egyptian high risk
female
breast cancer patients. Consequently,
large-scale prospective studies will beneeded to clearly define
its predictive
value.
ACKNOWLEDGMENT
Special thanks go to Dr. Nadia
Abaas, Lecturer of Pathology, Faculty of
Medicine, University of Alexandria, for
her assistance in IHC work. We also
wish to thank Mrs. Safeya Abd Al-
Khalek, Pathology technician, for techni-cal assistance.
REFERENCES
1. Boutayeb, S.; Boutayeb, A.; Ahbed-
dou, N.; et al. (2010): Estimation of the
cost of treatment by chemotherapy for
early breast cancer in Morocco. Cost Eff
Resour Alloc, 8: 16.
2. Bozzetti, C.; Musolino, A.; Camisa,R.; et al. (2006):
Evaluation of HER-2/
neu amplification and other biological
markers as predictors of response toneoadjuvant
anthracycline-based chemo-
therapy in primary breast cancer: The
role of anthracycline dose intensity. Am
J Clin Oncol, 29 (2): 171-7.
3. Buzdar, A.U. (2006): Topoisomerase
II gene amplification and response to
anthracycline-containing adjuvant che-
motherapy in breast cancer. J Clin On-
col, 24 (16): 2409-11.
4. Duffy, M.J. (2005): Predictive mark-
ers in breast and other cancers: A re-
view. Clin Chem, 51 (3): 494-503.
5. Esteva, F.J. and Hortobagyi, G.N.
(2009): Topoisomerase II {alpha} ampli-
fication and anthracycline- based chemo-
therapy: The jury is still out. J Clin On-
col, 27 (21): 3416-7.
6. Freudenberg, J.A.; Wang, Q.; Ka-
tsumata, M.; et al. (2009): The role of
HER2 in early breast cancer metastasis
and the origins of resistance to HER2-
targeted therapies. Exp Mol Pathol, 87
(1): 1-11.
7. Goldhirsch, A.; Wood, W.C.; Gel-
ber, R.D.; et al. (2007): Progress and
promise: highlights of the international
expert consensus on the primary therapyof early breast cancer
2007. Ann Oncol,
18 (7): 1133-44.8. Jemal, A.; Siegel, R.; Ward, E.; et
al. (2009): Cancer Statistics, 2009. CA
Cancer J Clin, 59 (4): 225-49.
9. Kennedy, R.D.; Quinn, J.E.;
Mullan, P.B.; et al. (2004): The role of
BRCA1 in the cellular response to
chemotherapy. J Natl Cancer Inst, 96
(22): 1659-68.
10. Knoop, A.S.; Knudsen, H.; Balslev,
E.; et al. (2005): Retrospective analysis
of topoisomerase II amplifications and
deletions as predictive markers inprimary breast cancer patients
randomly
assigned to cyclophosphamide,
methotrexate and fluorouracil or
cyclophosphamide, epirubicin andfluorouracil: Danish breast
cancer
cooperative group. J Clin Oncol, 23 (30):
7483-90.
116 Abd El-Aal et al.
Egypt. J. Med. Sci. 32 (1) 2011
-
8/2/2019 Doaa Doctor Paper
11/12
11. Konecny, G.E.; Pauletti, G.;
Untch, M.; et al. (2010): Associationbetween HER2, TOP2A, and
response to
anthracycline-based preoperative chemo-
therapy in high-risk primary breast can-
cer. Breast Cancer Res Treat, 120
(2):481-9.
12. Miyoshi, Y.; Kurosumi, M.; Kure-bayashi, J.; et al. (2010):
The predictive
factors for anthracycline-based chemo-
therapy for human breast cancer. BreastCancer, 17 (2):
103-9.
13. Munro, A.F.; Cameron, D.A.;
Bartlett, J.M. (2010): Targeting anthra-cyclines in early breast
cancer: new can-
didate predictive biomarkers emerge.
Oncogene, 29 (38): 5231-40.
14. Omar, S.; Khaled, H.; Gaafar, R.;
et al. (2003): Breast cancer in Egypt: A
review of disease presentation and
detection strategies. East Mediterr
Health J, 9 (3): 448-63.
15. Orlando, L.; Del Curto, B.;
Gandini, S.; et al. (2008): Topoisom-
erase II gene status and prediction ofpathological complete
remission after
anthracycline-based neoadjuvant chemo-
therapy in endocrine non-responsive
Her2/neu-positive breast cancer. Breast,
17 (5): 506-11.
16. Paik, S.; Taniyama, Y.; Geyer,
C.E. Jr (2008): Anthracyclines in the
treatment of HER2 - negative breast can-
cer. J Natl Cancer Inst, 100 (1): 2-4.
17. Rocha, R.M.; Nunes, C.B.;
Sanches, F.S.; et al. (2009): Rabbit
antibodies for hormone receptors and
HER2 evaluation in breast cancer. Rev
Assoc Med Bras, 55 (2): 163-8.
18. Rubin, E.H.; Hait, W.N. (2003):
Chemotherapeutic Agents. Anthracy-clines and DNA Intercalators /
Epipodo-
phyllotoxins / Camptothecins / DNA
Topoisomerases. In: Kufe DW, Pollock
RE, Weichselbaum RR, Bast RC, Gan-
sler TS, Holland JF, Frei E (Eds). Hol-
land-Frei Cancer Medicine, 6th ed. BC
Decker Inc: Hamilton Canada., pp 781-
8.
19. Siddig, A.; Mohamed, A.O.; Kamal,H.; et al. (2008):
HER-2/neu Ile655Val
polymorphism and the risk of breast can-
cer. Ann N Y Acad Sci, 1138: 84-94.
20. Tafjord, S.; Bhler, P.J.; Risberg,
B.; Torlakovic, E. (2002): Estrogen and
progesterone hormone receptor status in
breast carcinoma: comparison of immu-
nocytochemistry and immunohistochem-
istry. Diagn Cytopathol, 26 (3): 137-41.
21. Tewari, M.; Krishnamurthy, A.;
Shukla, H.S. (2008): Predictive markers
of response to neoadjuvant chemother-apy in breast cancer. Surg
Oncol, 17
(4):301-11.
Tubbs, R.; Barlow, W.E.; Budd, G.T.;
et al. (2009): Outcome of patients with
early-stage breast cancer treated with
doxorubicin-based adjuvant chemother-
apy as a function of HER2 and TOP2A
status. J Clin Oncol, 27 (24): 3881-6.
22. Zhang, J.; Liu, Y. (2008): HER2
over-expression and response to differ-
ent chemotherapy regimens in breast
cancer. J Zhejiang Univ Sci B, 9 (1): 5-9.
HER2/neu Value in Anthracycline Therapy in Breast Cancer 117
Egypt. J. Med. Sci. 32 (1) 2011
-
8/2/2019 Doaa Doctor Paper
12/12
.
.
)/(
.
.
.
/
./
.
.
.)( : .
)/(
118 Abd El-Aal et al.
Egypt. J. Med. Sci. 32 (1) 2011