Embed Size (px)
Citation preview

Doctor, I Can't See
27th May 2016
Dr Lai Ee Ling
Hospital Sultan Ismail Johor Bahru

First presentation - 12/2015
• Madam A • 33 years old • 6 months post-partum • Onset of symptoms - 3 months post partum • Presented with
– Constitutional sx • Prolonged intermittent fever
– Mucocutaneous sx • Malar rash, photosensitivity, oral ulcer & alopecia
– Arthalgia

Eye Symptoms
• Bilateral blurring of vision for 1 month • Painless • Gradual Onset • Progressively worsening

• Obstetric history: – Para 3, delivered full term – No h/o miscarriage – No h/o PIH
• FH : No h/o CTD • Drug history: No h/o traditional medicine or
other drug history

Physical Examination
• General examination: Alert, GCS 15/15 • BP : 101/64 mmHg • HR : 134 bpm • T : 39.3 • Lung : Clear • CVS : S1S2 • P/A : Soft, no hepatosplenomegaly

First presentation -12/2015


Opthalmologist review
• Bilateral pupils round and reactive • Bilateral eye EOM full • RAPD negative • Visual Acuity
- R finger counting - L hand movement

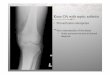
Fundoscope: Right Eye

Fundoscope: Left Eye

Purtscher's Like Retinopathy - Rare disease

Progress in Ward
• Developed acute confusion & psychosis in ward – auditory hallucination – delusion – disorientated to time
• CECT brain : Normal • LP : Not suggestive of intra-cranial infection • Metabolic cause excluded (except the
hypothyroid)

Blood Investigation
30/12/2015
WCC 3.2Hb 9.4Plt 86Urea 2.3Crea4nine 48AST 95ALT 30T.Bilirubin 7FT4 6.7TSH 8.9

• PBF : No evidence of hemolysis • UFEME: Protein 2+, Blood negative • 24 Hour urine protein : 0.47g/day • Serum albumin : 19 g/L • Serum amylase : 31 u/L (normal) • Hep B & C : negative • HIV : Negative

Immunology Investigations
• Positive Result
• ANA 1:1280 (speckled) • Anti-Sm >600u/mL • Anti U1RNP 125u/mL • Anti SSA > 600u/mL • C3 : 0.59 (↓) • C4 : 0.224 (↓) • Anti-thyroglobulin Ig :
Positive (169 )
• Negative Result
• Anti SSB Negative • Anti Scl 70 Negative • Anti Centromere
Negative • LA: Negative • ACA : Rejected

CSF result
• Opening pressure: 12cmH2O • Clear and colorless • No cell seen • Indian Ink : negative • Latx agglutinan : negative • AFB direct smear & PCR : Negative • C&S : negative

(1) SLE with mucocutananeous, joint, renal, hematological & CNS lupus (2) Purtscher's Like Retinopathy secondary to SLE (3) Autoimmune hypothyroidism

SLEDAI score
Descriptor ScoreOrganicbrainsyndrome 8Psychosis 8
Visual 8Vasculi4s 8Newmalarrash 4Oralulcer 4Alopecia 4Lowcomplement 4Thrombocytopenia 4TOTAL 60

Treatment
• IV methylprednisolone 500mg OD for 3 days
• Tapering dose of prednisolone • Antibiotic for sepsis • Refuse IV Cyclophosphamide

Clinic Review

5/2016 - Clinic Follow up 5 months later

Visual Progress
VisualAcuityatPresenta:on
VisualAcuityAt5months
RightEye FingerCoun4ng Fingercoun4ng
LePEye Handmovement 6/60

Right Eye Fundoscope After 5 month

Left eye fundoscope

Clinic Review
• On tapering prednisolone dose • Still refuse Cyclophosphamide • Started on azathioprine in view of active
disease and Purtscher retinopathy – Developed azthioprine induced hepatitis

Investigation during follow up
30/12/2015 15/3/2016 17/5/2016WCC 3.2 6.0 5.4Hb 9.4 12.7 13.6Plt 86 237 246Urea 2.3 2.7 2.1Crea4nine 48 58 59AST 95 23 282ALT 30 32 426T.Bilirubin 7 5 102(DIrect
predominant)FT4 6.7 15.9TSH 8.9 1.06
Started AZA

Purtscher's Retinopathy
Purtscher-like Retinopathy

Purtscher's Retinopathy
• First described by Otmar Purtscher in
1910 in a patient with head trauma • Similar retinal appearance also descibe in
other conditions, eg pancreatitis

Epidemiology
• Incidence: - 0.24 person per million per year (Including Purtscher and Purtscher's like retinopathy)
• Prevalance in SLE :
- 0.14% Miguel et al 2013 Chan Wu et al 2014

Pathogenesis
• Vaso-oclussive retinopathy • Pre-capillary occlusion
– Emboli (Fat, air, amniotic fluid) – Vasculitis – Leukoaggregation by complement activation – Vascular endothelial dysregulation, follow by
endothelin induced vasculopathy
• Microvascular infarct of retinal nerve fiber layer

Causes of Purtscher's Retinopathy
• TRAUMATIC – Head Trauma – Chest compression – Long bone #/Crush
injury – Weight lifting – Battered baby
syndrome – Barotrauma – Orthopaedic surgery
• NON TRAUMATIC – Acute pancreatitis – Connective Tissue
Disease (SLE, SSc, Dermatomyositis)
– Cryoglobulinemia – Chronic renal failure – TTP/HUS – Pre-eclampsia – HELLP – Embolism (fat, air,
amniotic fluid)

Symptoms
• Loss of visual acuity • Loss of visual field
– Central – Paracentral – Arcuate scotoma – Peripheral field usually preserved
• Combination loss of visual acuity AND visual field

Bilateral Vs Unilateral Eye
• Bilateral(60%)> Unilateral • Bilateral > common in cases precipitated
by systemic illness • Unilateral > common in cases of chest
compression and trauma
• No different in the extent of retina involvement

Diagnosis
• Made on clinical ground – Sudden visual loss after the causal pathology – Fundoscopic signs
• Typically in posterior pole of eye • Cotton wool spots • Intra-retinal haemorrhage • Purtscher flecken (pathognomic)


Diagnosis
• Supported by Intravenous flourescein angiography – Arteriolar obstruction – Leakage of dye from retinal arteriole, capillary
and venules

Flourescein Angiography
Arteriolar occlusion in right eye (arrow) Area of capillary leakage in the macule of left eye

Diagnosis Criteria
• Migual et al • At least 3 of 5 criteria
– Purstcher flecken – Retinal haemorrhage in low to moderate
number – Cotton wool spots (confine to posterior pole) – Probable explanatory etiologies – Complementary investigation compatible with
diagnosis

Acute Retinal Signs
• Cotton wool spot (93%) • Retinal haemorrhage (65%) • Purtscher flecken (63%) • Pseudo cherry red spot (26%) • Macula edema (22%) • Optic disc swelling (16%)
AIM Minguel et al 2013

Purtscher Flecken
• Polygonal patches of retinal whitening • Between affected retinal arterioles and
venules • Characteristic clear zone • 50um unaffected on either side of retinal
arteries and pre-capillary arterioles

Purstcher Flecken
Clear zone between flecken and arterial wall

Chronic Retinal Signs
• Optic atrophy (64%) • Normalization of retinal appearnce (40%) • Mottling of retinal pigment epithelium
(23%) • Narrowing of retinal arterioles (4%)
AIM Miguel et al 2013

Chronic Retinal Changes
Pale optic disc Retinal pigment epithelial changes in macular

Treatment
• No proven beneficial therapy • Spontaneous visual improvement (variable
degree) even without therapy • Steroid thereotically beneficial in systemic
vasculitis disease

Prognosis
• Visual prognosis is variable

Purtscher's and Purtsher Like Retinopathy


Prognostic Factors
• Visual Acuity Improvement – Male gender – Etiology : Trauma and acute pancreatitis – Absence of macular edema – Absence of pseudo cherry red spot
– No statistically significant difference in VA improvement between those reveived corticosteroid Vs NO corticosteroid

Purtscher-like Retinopathy in SLE


Conclusion
• In SLE patient with purtscher's retinopathy – CNS lupus more common – SLEDAI on initial presentation is significant
higher (>20) – No different in prevalance of lupus nephritis – No different in prevalance of APS

Conclusion
• POOR visual prognsis despite aggressive treatment (High dose steroid + CYC/MTX) – At 6/12 of treatment, 67% had optic atrophy – Pseudo-cherry spot at presentation had the
worse VA at 6/12 – Retinal neovascularization, require laser
therapy

Summary
• Our patient had features that consistent with report by Chan wu et al – CNS lupus – High SLEDAI score – Poor visual prognosis

Reference
(1) Chan Wu, Rongping D, Fangtian D, Qian W. Purtscher-like Retinopathy in Systemic Lupus Erythematosus. American Journal of Ophthalmology 2014;158(6): 1335-1341.
(2) Agrawal A, McKibbin M. Purtscher's retinopathy:
epidemiology, cinical features and outcome. Br J Ophthalmol2007; 91(11):1456-1459
(3) Miguel AI, Henriques F, Azevedo LFR, Loureiro AJR,
Maber;ey DAL. Systemic review of Purtscher's and Purtscher like retinopathies. Eye (I.orul) 2013;19(6):512-518

Thank You