Embed Size (px)
Citation preview
“Tie Your Shoes Before You Trip!”
Prevention of Medical Errors
Arnold Mackles, MD, MBA, LHRM
St. Louis, MO
November 14, 2008 1:45 PM - 3:00 PM
Session 10: “Tie Your Shoes Before You Trip!” Prevention of Medical Errors Learning Objectives
• Describe the systems approach to medical error prevention. • Identify the drugs/drug classes that are at high risk for adverse drug events.
Faculty Arnold Mackles, MD, MBA, LHRM Physician Speaker, Licensed Health Care Risk Manager Palm Beach Gardens, Florida Dr Arnold Mackles has practiced hospital-based neonatal medicine in Florida for over 22 years since completing a fellowship in neonatology at the Cornell University Medical Center in New York. In addition to receiving an MBA from Nova Southeastern University, he obtained his license as a health care risk manager through studies at the University of South Florida. Currently, Dr Mackles devotes full time to risk management and patient safety issues. Faculty Financial Disclosure Statement The presenting faculty report the following: Dr Mackles has no relationships to disclose. Drug List Generic Trade amino acids various ampicillin various dexamethasone various enteric coated aspirin various furosemide Lasix heparin sodium various insulin various metronidazole various oxycodone OxyContin, Roxicodone penicillin various potassium chloride various potassium phosphate various warfarin sodium Coumadin, Jantoven Suggested Reading List Condition H phone line provides last chance to prevent serious errors. J Healthcare Risk Manage. 2006;28(2):13-24. Death of young girl prompts Condition H program. J Healthcare Risk Manage. 2006;28(2):13-24. Risk Management Pearls for Physicians. Chicago: American Society for Healthcare Risk Management (American Hospital Association); 2003. Risk Management Pearls for Medication Error Reduction. Chicago, IL: American Society for Healthcare Risk Management (American Hospital Association); 2001. Bates DW, Cullen DJ, Laird N, et al; ADE Prevention Study Group. Incidence of adverse drug events and potential adverse drug events. JAMA. 1995;274(1):29-34. Johns Hopkins Hospital. Children’s Medical and Surgical Center. Harriet Lane Handbook: A Manual for Pediatric House Officers. 16th ed. St Louis, MO: CV Mosby; 2002.
Session 10
Session 10
Kohn LT, Corrigan JM, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Committee on Quality of Health Care in America; Institute of Medicine. Washington, DC: National Academy Press; 2000. The Joint Commission. Official “Do Not Use” List. http://www.jointcommission.org/NR/rdonlyres/2329F8F5-6EC5-4E21-B932-54B2B7D53F00/0/06_dnu_list.pdf. Accessed March 17, 2008. The Joint Commission. Sentinel Event Policy and Procedures. http://www.jointcommission.org/SentinelEvents/PolicyandProcedures/se_pp.htm. Updated July 2007. Accessed March 17, 2008. The Joint Commission. Sentinel Event Statistics: As of December 31, 2007. http://www.jointcommission.org/NR/rdonlyres/D7836542-A372-4F93-8BD7-DDD11D43E484/0/SE_Stats_12_07.pdf. Accessed March 17, 2008. The Joint Commission. 2008 National Patient Safety Goals. http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. Accessed March 17, 2008. The Joint Commission. Root Causes of Sentinel Events. http://www.jointcommission.org/NR/rdonlyres/FA465646-5F5F-4543-AC8F-E8AF6571E372/0/root_cause_se.jpg. Accessed March 17, 2008. The Joint Commission. Sentinel Event Trends: Medication Error Events Reported by Year. http://www.jointcommission.org/NR/rdonlyres/61A7E8CF-2B0F-423A-ACA4-76F0A5EF37E7/0/se_trends_med_errors.gif. Accessed March 17, 2008. The Joint Commission. Sentinel Event Trends: Wrong-site Surgeries Reported by Year. http://www.jointcommission.org/NR/rdonlyres/6F94288C-EC8E-4B95-91F6-0A1C96C09708/0/se_trends_wss_reported.gif. Accessed March 17, 2008. Leape LL, Bates DW. Cullen DJ, et al; ADE Prevention Study Group. Systems analysis of adverse drug events. JAMA. 1995;274(1);35-43. Rothschild JM, Landrigan CP, Cronin JW, et al. The Critical Care Safety Study: The incidence and nature of adverse events and serious medical errors in intensive care. Crit Care Med. 2005;33(8):1694-1700. State of Florida. Agency for Health Care Administration. Division of Health Quality Assurance. Adverse Incident Reporting Guide. http://ahca.myflorida.com/MCHQ/Health_Facility_Regulation/Risk/documents/adverse_incident_reporting_guide_062006.pdf. Accessed March 17, 2008.
®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
1
?How confident are you in your ability to incorporate the Joint Commission patient
safety goals into your practice?
1) Very uncertain2) _3) _4) _5) _6) _7) Very confident
According to the Joint Commission, what is the most common root cause of sentinel events in
the hospital setting?
1) Staffing2) Continuum of care3) Organization culture4) Communication5) Not sure
What is the most common cause of medication errors in the hospital setting?
1) Ordering2) Transcription3) Dispensing4) Administration5) Not sure
Which of the following is recommended by the Joint Commission when writing
medication orders?
1) Abbreviate microgram “µg”2) Abbreviate once daily “qd”3) Use trailing zeros (eg, 2.0)4) Use leading zeros (eg, 0.2) 5) Not sure
Prevention of Medical ErrorsPrevention of Medical Errors
By Arnold MacklesMD,MBA,LHRM
“Tie your shoes before you trip…”
2
Our Medical TrainingOur Medical Training
• Taught diagnosis and treatment
• No formal training in preventing errors
Our Medical TrainingOur Medical Training
•• Forced long and exhausting Forced long and exhausting hours hours ““on callon call””
•• Putting us at risk for making Putting us at risk for making errorserrors
As Health Care ProvidersAs Health Care Providers
• We are expected to diagnose and treat without error
As Health Care ProvidersAs Health Care Providers
• We are held accountable
• Not only for our errors… but for systemic problems
As Health Care ProvidersAs Health Care Providers
• The system still permits us to perform surgery, deliver babies, place epidurals, care for preemies…
As Health Care ProvidersAs Health Care Providers
• At 5:30 AM after being “on call”and awake for 22 hours!
3
The Traditional Culture of The Traditional Culture of MedicineMedicine
• Has not been very successful in the prevention of medical errors
The Traditional Culture of The Traditional Culture of MedicineMedicine
• Until recently systemic problems often went unnoticed
• No changes made
A Broken SystemA Broken System
Broken SystemBroken System
We all need to participate in the repair
So We WonSo We Won’’t Trip !t Trip !
“To err is humanTo err is human……..
……to forgive divineto forgive divine””
4
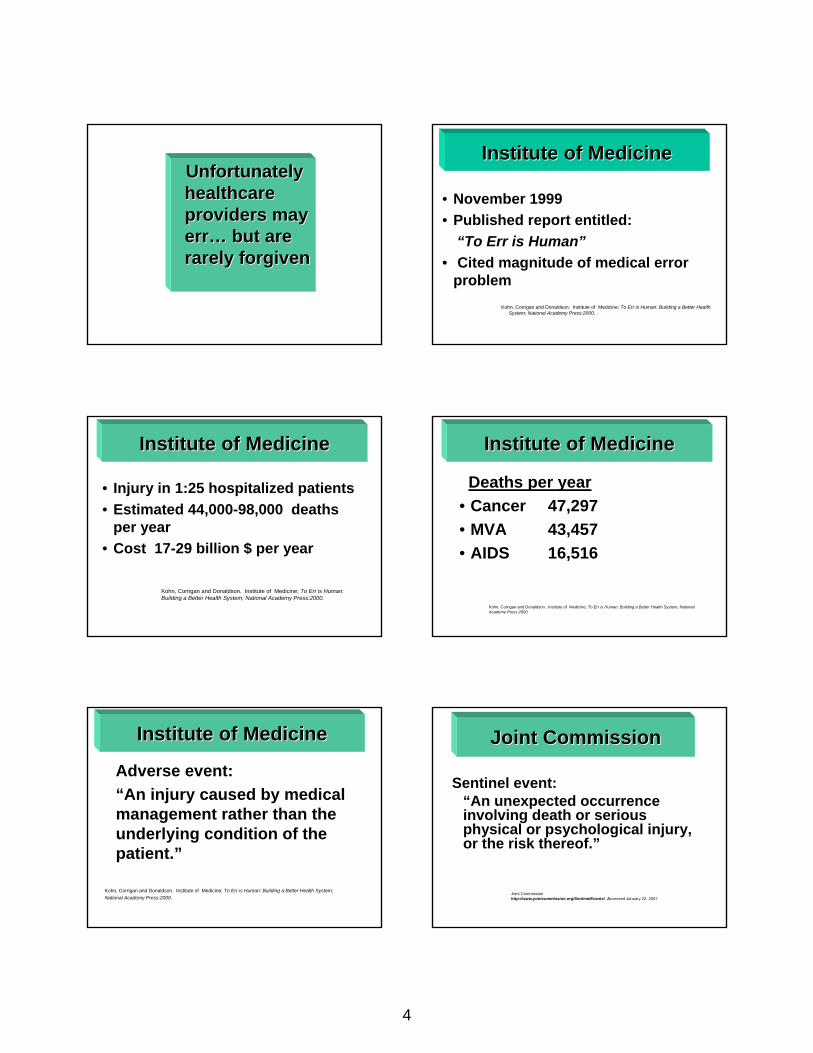
Unfortunately Unfortunately healthcare healthcare providers may providers may errerr…… but are but are rarely forgivenrarely forgiven
Institute of MedicineInstitute of Medicine
• November 1999• Published report entitled:
“To Err is Human”• Cited magnitude of medical error
problemKohn, Corrigan and Donaldson. Institute of Medicine; To Err is Human: Building a Better Health
System; National Academy Press:2000.
• Injury in 1:25 hospitalized patients• Estimated 44,000-98,000 deaths
per year• Cost 17-29 billion $ per year
Kohn, Corrigan and Donaldson. Institute of Medicine; To Err is Human: Building a Better Health System; National Academy Press:2000.
Institute of MedicineInstitute of Medicine Institute of MedicineInstitute of Medicine
Deaths per year• Cancer 47,297• MVA 43,457• AIDS 16,516
Kohn, Corrigan and Donaldson. Institute of Medicine; To Err is Human: Building a Better Health System; National Academy Press:2000.
Institute of MedicineInstitute of Medicine
Adverse event: “An injury caused by medical management rather than the underlying condition of the patient.”
Kohn, Corrigan and Donaldson. Institute of Medicine; To Err is Human: Building a Better Health System;National Academy Press:2000.
Joint CommissionJoint Commission
Sentinel event:“An unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof.”
Joint Commissionhttp://www.jointcommission.org/SentinelEvents/ Accessed January 22, 2007
5
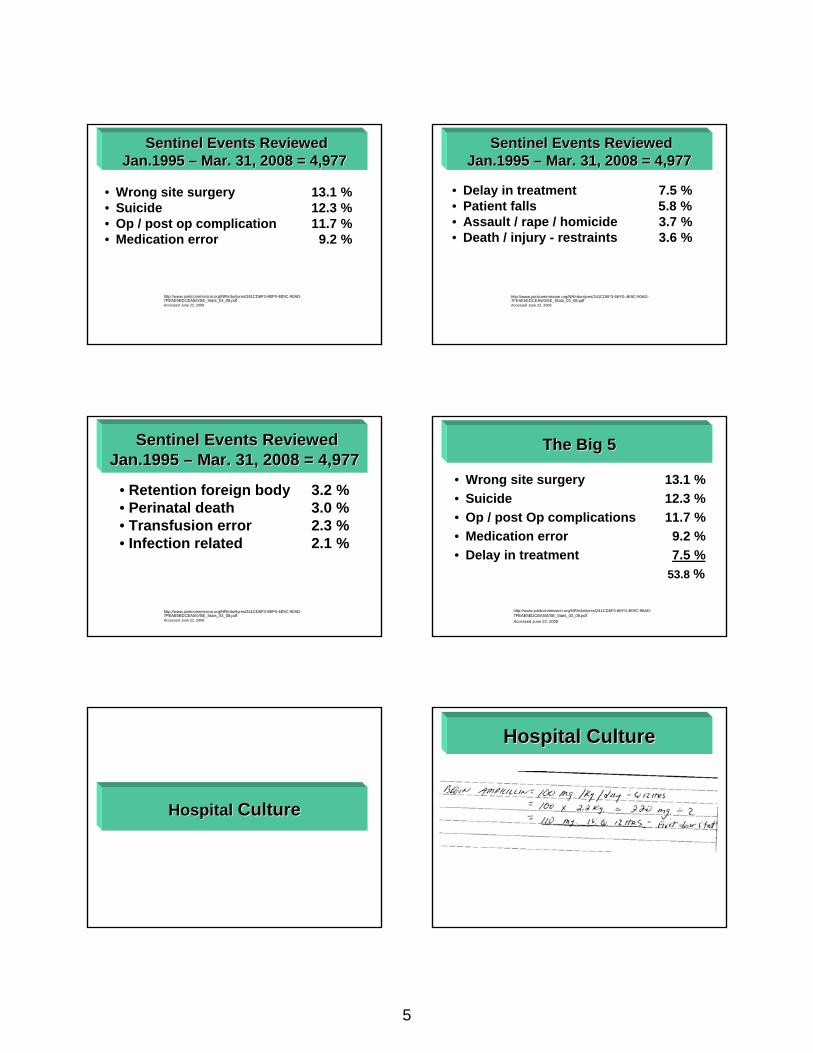
• Wrong site surgery 13.1 %• Suicide 12.3 %• Op / post op complication 11.7 %• Medication error 9.2 %
http://www.jointcommission.org/NR/rdonlyres/241CD6F3-6EF0-4E9C-90AD-7FEAE5EDCEA5/0/SE_Stats_03_08.pdfAccessed June 22, 2008
Sentinel Events Reviewed Sentinel Events Reviewed Jan.1995 Jan.1995 –– Mar. 31, 2008 = 4,977Mar. 31, 2008 = 4,977
Sentinel Events Reviewed Sentinel Events Reviewed Jan.1995 Jan.1995 –– Mar. 31, 2008 = 4,977Mar. 31, 2008 = 4,977
• Delay in treatment 7.5 %• Patient falls 5.8 %• Assault / rape / homicide 3.7 %• Death / injury - restraints 3.6 %
http://www.jointcommission.org/NR/rdonlyres/241CD6F3-6EF0-4E9C-90AD-7FEAE5EDCEA5/0/SE_Stats_03_08.pdfAccessed June 22, 2008
• Retention foreign body 3.2 % • Perinatal death 3.0 %• Transfusion error 2.3 %• Infection related 2.1 %
http://www.jointcommission.org/NR/rdonlyres/241CD6F3-6EF0-4E9C-90AD-7FEAE5EDCEA5/0/SE_Stats_03_08.pdfAccessed June 22, 2008
Sentinel Events Reviewed Sentinel Events Reviewed Jan.1995 Jan.1995 –– Mar. 31, 2008 = 4,977Mar. 31, 2008 = 4,977
The Big 5The Big 5
• Wrong site surgery 13.1 %• Suicide 12.3 %• Op / post Op complications 11.7 %• Medication error 9.2 %• Delay in treatment 7.5 %
53.8 %
http://www.jointcommission.org/NR/rdonlyres/241CD6F3-6EF0-4E9C-90AD-7FEAE5EDCEA5/0/SE_Stats_03_08.pdfAccessed June 22, 2008
Hospital Hospital CultureCulture
Hospital CultureHospital Culture
6
Hospital CultureHospital Culture
“Doctor… can’t I trust you”?
Hospital CultureHospital Culture
“…Just write the order !”
Airline CultureAirline Culture
Airline SafetyAirline Safety
• Systems approach to safety• Pilot checks aircraft• Checklists prior to takeoff
Airline SafetyAirline Safety
• Limited flying hours for flight crew
Old School Vs. New SchoolOld School Vs. New School
7
Old School Old School ––Traditional ViewTraditional View
• Blame individual responsible for error
• Usually person closest to incident
• Identify and Punish individual responsible
Leape, LL, Bates, DW. Cullen, DJ et al. Systems Analysis of Adverse Drug Events. JAMA 1995; 274(1); 35-43
• Leaves dangerous system in place
• Gives those in charge false impression of solving problem
• Ignores the big pictureLeape, LL, Bates, DW. Cullen, DJ et al. Systems Analysis of Adverse Drug Events. JAMA 1995; 274(1); 35-43
Old School Old School -- DrawbacksDrawbacks
New School New School –– Systems ViewSystems View
• Error viewed as problem with system
• Focus on cause of error…• Not on individual
Leape, LL, Bates, DW. Cullen, DJ et al. Systems Analysis of Adverse Drug Events. JAMA 1995; 274(1); 35-43
New School New School -- GoalsGoals
• Find specific error in system • Correct error• Care improved as dangerous
system corrected
Leape, LL, Bates, DW. Cullen, DJ et al. Systems Analysis of Adverse Drug Events. JAMA 1995; 274(1); 35-43
New School New School -- DrawbacksDrawbacks
• Creation of new bureaucracy? • Responsibility for change?• Paper trails?• Flexibility?
Analysis Analysis of of
ErrorsErrors
8
Root Cause AnalysisRoot Cause Analysis
Root Cause AnalysisRoot Cause Analysis
“A process for identifying the basic or causal factors that underlie variation in performance, including the occurrence or possible occurrence of a sentinel event.”
- The Joint Commission
http://www.jointcommission.org/SentinelEvents/se_glossary.htm?HTTP___JCSEARCH.The Joint Commission.ORG_CGI_BIN_MSMFIND.EXE?RESMASK=MssResEN.mskhttp%3A//jcsearch.The Joint Commission.org/cgi-bin/MsmFind.exe%3Fhttp%3A//jcsearch.The Joint Commission.org/cgi-bin/MsmFind.exe%3FRESMASK%3DMssResEN.msk accessed January 23, 2007
httphttp://://www.jointcommission.org/NR/rdonlyres/74540565www.jointcommission.org/NR/rdonlyres/74540565--4D0F4D0F--49924992--863E863E--8F9E949E6B56/0/SE_Stats_12_06.pdf8F9E949E6B56/0/SE_Stats_12_06.pdf
Accessed May 3, 2007Accessed May 3, 2007
““Identify That OrderIdentify That Order””
Identify That Order #1 ?
1) Ampicillin2) Amlodipine3) Albumin4) Amikacin5) None of the above
Identify That Order #2 ?
1) D5 NS + 20 meq. KCL per L at 35 cc/hr2) D5 ½ NS + 2 meq. KCL per L at 35 cc/hr3) D5 ½ NS + 20 meq. KCL per L at 75 cc/hr4) D5 ½ NS + 20 meq. KCL per L at 35 cc/hr5) None of the above
9
Identify That Order #3 ?
1) Labetalol2) Lactulose3) Levalbuterol4) Lamivudine5) None of the above
Identify That Order #4 ?
1. Acetaminophen2. EDTA 3. Enteric coated aspirin4. Acetylcysteine5. None of the above
Identify That Order #5 ?
1. Alternate KCL and NACL 40 meq.2. Alternate KCL and K phosphate 40 meq.3. Advance to KCL and K phosphate 40 meq.4. Alternate KCL and K phosphate/NACL 40 meq.5. None of the above
Error ReductionError Reduction
Medication ErrorsMedication Errors
The Joint Commission http://www.jointcommission.org/NR/rdonlyres/61A7E8CF-2B0F-423A-ACA4-76F0A5EF37E7/0/se_trends_med_errors.gif accessed January 22,2007
10
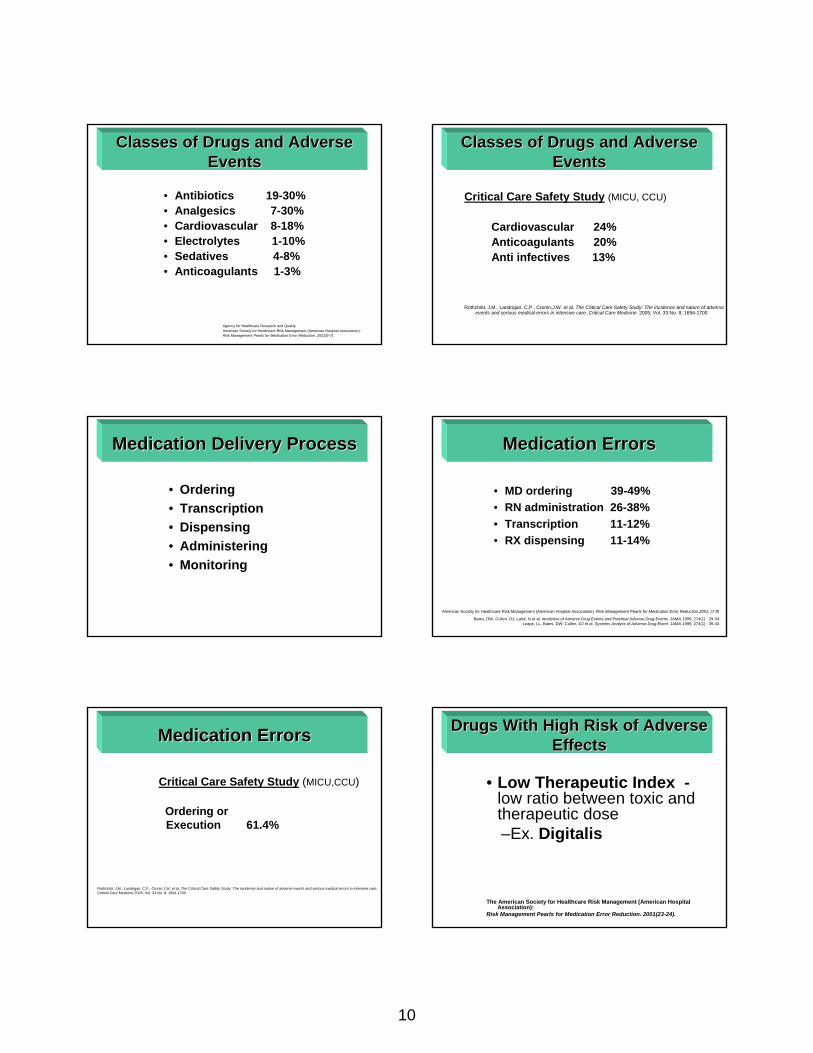
Classes of Drugs and Adverse Classes of Drugs and Adverse EventsEvents
• Antibiotics 19-30%• Analgesics 7-30%• Cardiovascular 8-18%• Electrolytes 1-10% • Sedatives 4-8%• Anticoagulants 1-3%
Agency for Healthcare Research and QualityAmerican Society for Healthcare Risk Management (American Hospital Association): Risk Management Pearls for Medication Error Reduction. 2001(6-7)
Classes of Drugs and Adverse Classes of Drugs and Adverse EventsEvents
Critical Care Safety Study (MICU, CCU)
Cardiovascular 24%Anticoagulants 20%Anti infectives 13%
Rothchild, J.M., Landrigan, C.P., Cronin,J.W. et al. The Critical Care Safety Study: The incidence and nature of adverse events and serious medical errors in intensive care. Critical Care Medicine. 2005; Vol. 33 No. 8; 1694-1700.
Medication Delivery ProcessMedication Delivery Process
• Ordering• Transcription• Dispensing• Administering• Monitoring
Medication ErrorsMedication Errors
• MD ordering 39-49%• RN administration 26-38%• Transcription 11-12%• RX dispensing 11-14%
American Society for Healthcare Risk Management (American Hospital Association): Risk Management Pearls for Medication Error Reduction.2001. (7-8)
Bates, DW, Cullen, DJ, Laird, N et al. Incidence of Adverse Drug Events and Potential Adverse Drug Events. JAMA 1995; 274(1) : 29-34 Leape, LL, Bates, DW. Cullen, DJ et al. Systems Analyss of Adverse Drug Event JAMA 1995; 274(1) ; 35-43
Medication ErrorsMedication Errors
Critical Care Safety Study (MICU,CCU)
Ordering orExecution 61.4%
Rothchild, J.M., Landrigan, C.P., Cronin,J.W. et al. The Critical Care Safety Study: The incidence and nature of adverse events and serious medical errors in intensive care. Critical Care Medicine 2005; Vol. 33 No. 8; 1694-1700
Drugs With High Risk of Adverse Drugs With High Risk of Adverse EffectsEffects
• Low Therapeutic Index -low ratio between toxic and therapeutic dose–Ex. Digitalis
The American Society for Healthcare Risk Management (American Hospital Association):
Risk Management Pearls for Medication Error Reduction. 2001(23-24).

11
Drugs With High Risk of Adverse Drugs With High Risk of Adverse EffectsEffects
• Concentrated Electrolytes– Ex. KCL– Ex. NACL
The American Society for Healthcare Risk Management (American Hospital Association): Risk Management Pearls for Medication Error Reduction. 2001(23-24).
Drugs With High Risk of Adverse Drugs With High Risk of Adverse EffectsEffects
• I.V. Anticoagulants–Heparin
• Warfarin
The American Society for Healthcare Risk Management (American Hospital Association): Risk Management Pearls for Medication Error Reduction. 2001(23-24).
Drugs With High Risk of Adverse Drugs With High Risk of Adverse EffectsEffects
• Narcotics, PCA– In combination with other meds:
• Benzodiazepines• Sedative/hypnotics
American Society for Healthcare Risk Management (American Hospital Association): Risk Management Pearls for Medication error Reduction.
Drugs With High Risk of Adverse Drugs With High Risk of Adverse EffectsEffects
• Insulin-Various Types• onset• duration • Concentrations
The American Society for Healthcare Risk Management (American Hospital Association): Risk Management Pearls for Medication Error Reduction. 2001(23-24).
Drugs With High Risk of Adverse Drugs With High Risk of Adverse EffectsEffects
• Chemotherapy–Highly Toxic Agents
The American Society for Healthcare Risk Management (American Hospital Association):
Risk Management Pearls for Medication Error Reduction. 2001(23-24).
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
12
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Fatigue
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Alcohol and Drugs
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Illness
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Inattention / Distraction
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Emotions
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Unfamiliar Situations
13
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Equipment Design / Flaws
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
• Inadequate labeling / Instructions
Increased Risk of Errors Increased Risk of Errors --FactorsFactors
“Hey…Who’s On First?”
CommunicationProblems
Confusion CornerConfusion Corner
To ensure patient safety…
@
…write out the word:
“At”
”The Joint Commission “Do Not Use” List
To ensure patient safety…
D/C
…write out the word:
“Discontinue” or “Discharge”
The Joint Commission “Do Not Use” List

14
To ensure patient safety…
U
…write out the word:
“Units”
The Joint Commission “Do Not Use” List
To ensure patient safety…
IU
…write out the words:
“International Units”
J CAHO has in st itu ted a Nat ional Pa t ient Safety Goa l rela ted to the u se of danger ous abbrevia t ions. To avoid t he r isk of poten tia l er r ors due to abbrevia t ions being misread or
misin terpr eted, MMH S request s tha t medica l st a ff r efra in from using unsafe a bbrevia t ion s.
To ensure patient safety…
MgS04
…write out the words:
“Magnesium Sulfate”
J CAHO has inst it u ted a N at ional Pa t ien t Safety Goa l r ela ted to the use of dangerous abbrevia t ions. To avoid the r isk of pot en tia l error s du e to abbrevia t ions being misread or
misin terpret ed, MMHS requests t ha t medica l st a ff r efr a in from using unsa fe abbrevia t ions. The Joint Commission “Do Not Use” List
To ensure patient safety…
MS04
…write out the words:
“Morphine Sulfate”
J CAHO ha s in st itu ted a Nat ional Pa tien t Safety Goal r ela ted to th e use of dangerous abbr evia t ion s. To avoid t he r isk of poten t ia l er rors due to abbrevia t ion s being misr ead or
misin terpreted, MMHS requ est s tha t medica l sta ff r efra in from using un safe abbreviat ion s. The Joint Commission “Do Not Use” List
To ensure patient safety…
MS
…write out the words:
“Morphine Sulfate”
J CAHO has inst itu ted a Na tiona l Pa t ient Safety Goal rela ted to the u se of danger ou s abbrevia tions. To avoid t he r isk of poten tia l er rors due to abbrevia t ions being misread or
misin terpr eted, MMH S requests th a t medica l s taff r efra in fr om using unsafe abbrevia t ion s. The Joint Commission “Do Not Use” List
To ensure patient safety…
μg
…write out:
“mcg” or “microgram”
J CAH O h as in st itu ted a Nat iona l Pa t ient Safety Goal r elated to the use of dan gerous abbr evia t ions. To avoid the r isk of potent ia l er ror s du e to abbrevia t ions bein g misr ead or
misin ter preted, MMH S requ est s tha t medica l s taff r efr a in from using unsafe a bbr evia t ion s. The Joint Commission “Do Not Use” List
15
To ensure patient safety…
QD
…write out the words:
“EVERY DAY”
J CAHO has in st itu ted a Nat ional Pa t ien t Safety Goa l r ela ted to the use of da ngerous a bbrevia t ions. To avoid t he r isk of poten t ia l error s due to abbrevia t ions being m isread or
misin terpreted, MMHS request s tha t medical staff r efr a in from using unsafe a bbrevia t ions.
The Joint Commission “Do Not Use” List
To ensure patient safety…
QID
…write out the words:
“Four Times Daily”
J CAHO h as in st itu ted a Na t iona l Pa tien t Safety Goal r ela ted to the u se of dan gerous abbrevia t ions. To avoid t he r isk of potent ia l er rors due to abbrevia t ions being misr ead or
misin terpreted, MMH S request s tha t medica l s ta ff r efra in from using unsafe abbr evia t ions. The Joint Commission “Do Not Use” List
To ensure patient safety…
QOD
…write out the words:
“Every Other Day”
J CAHO has in st itu ted a Nat ional Pa t ien t Safety Goal r ela ted to the use of danger ous abbr evia t ion s. To avoid the r isk of poten t ial er rors due to abbreviat ions being m isread or
m isin terpreted, MMHS request s tha t m edica l s ta ff refra in from using unsa fe abbrevia tions. The Joint Commission “Do Not Use” List
Use Leading Zeros Before a Decimal Point
Example:0.2 mg.
The Joint Commission “Do Not Use” List
Do Not Use Trailing Zeros
Example:Do not write 2.0 mg.
The Joint Commission “Do Not Use” List
16
Patient SafetyPatient Safety The Joint Commission The Joint Commission National Patient Safety GoalsNational Patient Safety Goals
GOALGOAL: Improve Accuracy of Patient : Improve Accuracy of Patient IdentificationIdentification.
• Use 2 patient identifiers for:– Obtaining blood– Giving meds– Procedures– Treatments
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ Accessed January 18, 2007
Hey, who’s on first ?
CommunicationCommunication
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/National
PatientSafetyGoals/ Accessed January 18, 2007
GOALGOAL: Improve the Effectiveness of : Improve the Effectiveness of Communication Among CaregiversCommunication Among Caregivers
• “Read back” phone, verbal orders
• “Read back” test results
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ Accessed January 18, 2007
GOALGOAL: Improve the Effectiveness of : Improve the Effectiveness of Communication Among CaregiversCommunication Among Caregivers
• Standardize list of abbreviations, acronyms not to be used
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ Accessed January 18, 2007
17
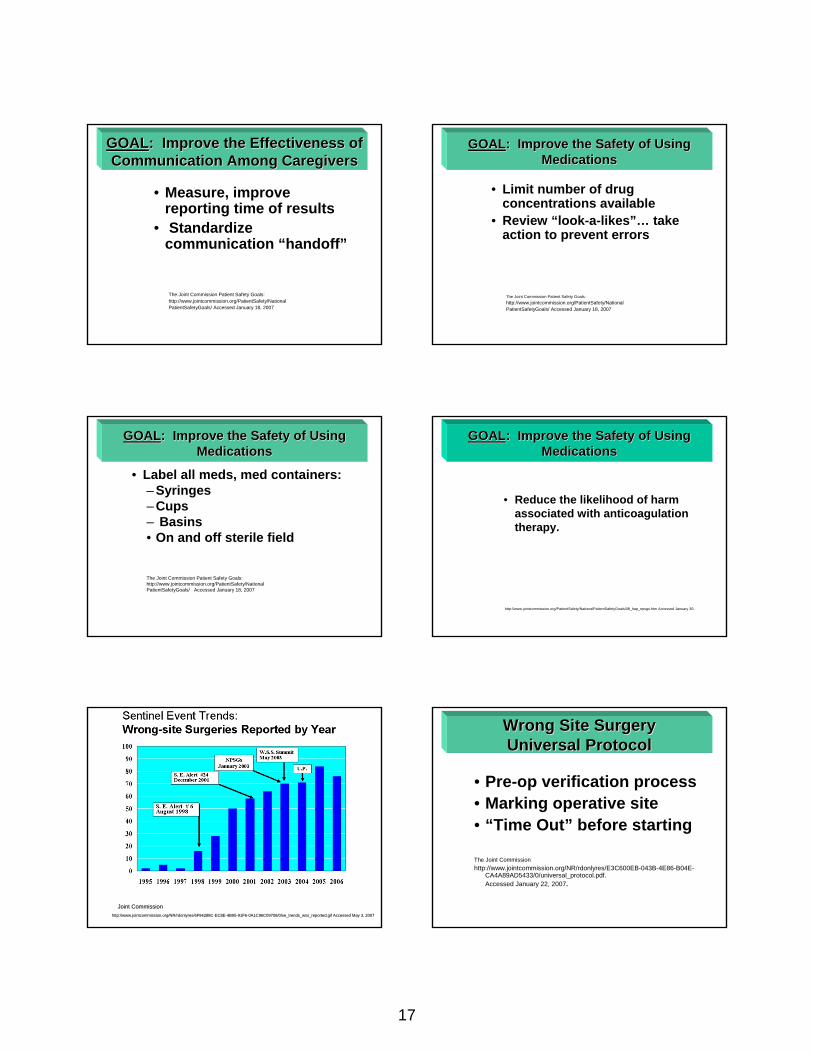
GOALGOAL: Improve the Effectiveness of : Improve the Effectiveness of Communication Among CaregiversCommunication Among Caregivers
• Measure, improve reporting time of results
• Standardize communication “handoff”
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ Accessed January 18, 2007
GOALGOAL: Improve the Safety of Using : Improve the Safety of Using MedicationsMedications
• Limit number of drug concentrations available
• Review “look-a-likes”… take action to prevent errors
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ Accessed January 18, 2007
GOALGOAL: Improve the Safety of Using : Improve the Safety of Using Medications Medications
• Label all meds, med containers:– Syringes– Cups– Basins • On and off sterile field
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ Accessed January 18, 2007
GOALGOAL: Improve the Safety of Using : Improve the Safety of Using MedicationsMedications
• Reduce the likelihood of harm associated with anticoagulation therapy.
http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/08_hap_npsgs.htm Accessed January 30,
http://www.jointcommission.org/NR/rdonlyres/6F94288Chttp://www.jointcommission.org/NR/rdonlyres/6F94288C--EC8EEC8E--4B954B95--91F691F6--0A1C96C09708/0/se_trends_wss_reported.gif Accessed May 3, 20070A1C96C09708/0/se_trends_wss_reported.gif Accessed May 3, 2007
Joint CommissionJoint Commission
Wrong Site Surgery Wrong Site Surgery Universal ProtocolUniversal Protocol
• Pre-op verification process• Marking operative site• “Time Out” before starting
The Joint Commissionhttp://www.jointcommission.org/NR/rdonlyres/E3C600EB-043B-4E86-B04E-
CA4A89AD5433/0/universal_protocol.pdf. Accessed January 22, 2007.
18
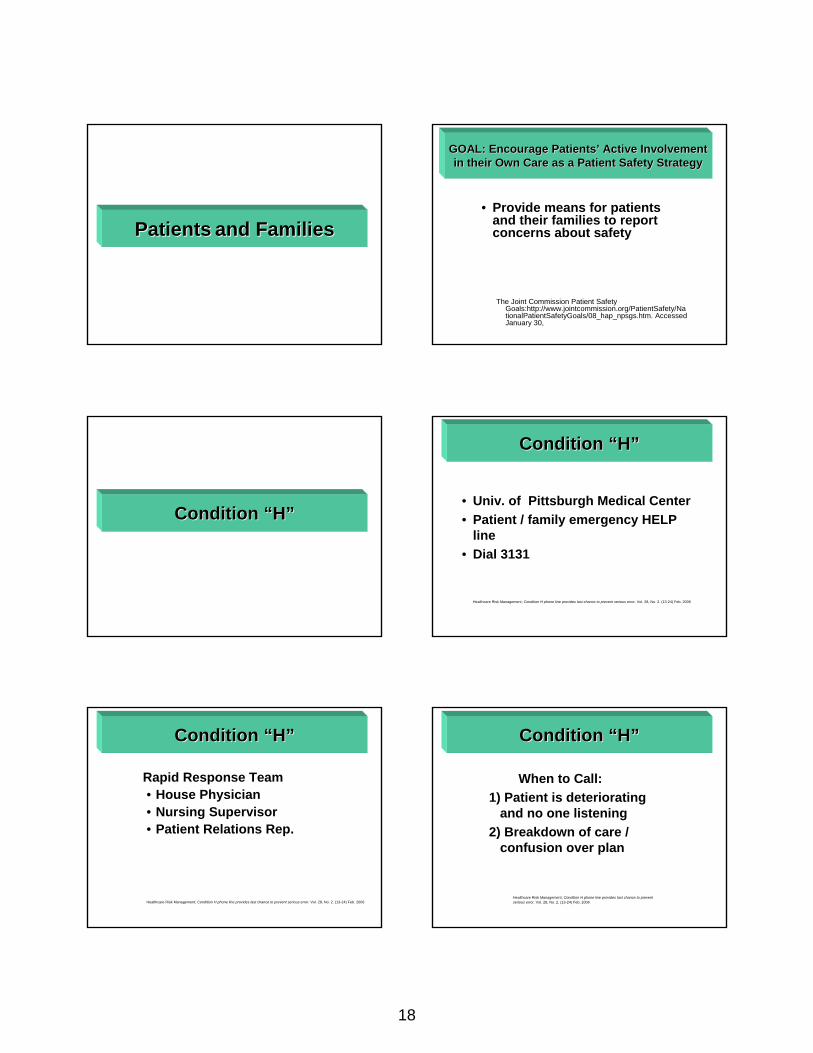
PatientsPatients and Familiesand Families
GOAL: Encourage PatientsGOAL: Encourage Patients’’ Active Involvement Active Involvement in their Own Care as a Patient Safety Strategyin their Own Care as a Patient Safety Strategy
• Provide means for patients and their families to report concerns about safety
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/08_hap_npsgs.htm. Accessed January 30,
Condition Condition ““HH””
Condition Condition ““HH””
• Univ. of Pittsburgh Medical Center• Patient / family emergency HELP
line• Dial 3131
Healthcare Risk Management; Condition H phone line provides last chance to prevent serious error. Vol. 28, No. 2. (13-24) Feb. 2006
Condition Condition ““HH””
Rapid Response Team• House Physician• Nursing Supervisor• Patient Relations Rep.
Healthcare Risk Management; Condition H phone line provides last chance to prevent serious error. Vol. 28, No. 2. (13-24) Feb. 2006
Condition Condition ““HH””
When to Call:1) Patient is deteriorating
and no one listening2) Breakdown of care /
confusion over plan
Healthcare Risk Management; Condition H phone line provides last chance to prevent serious error. Vol. 28, No. 2. (13-24) Feb. 2006
19
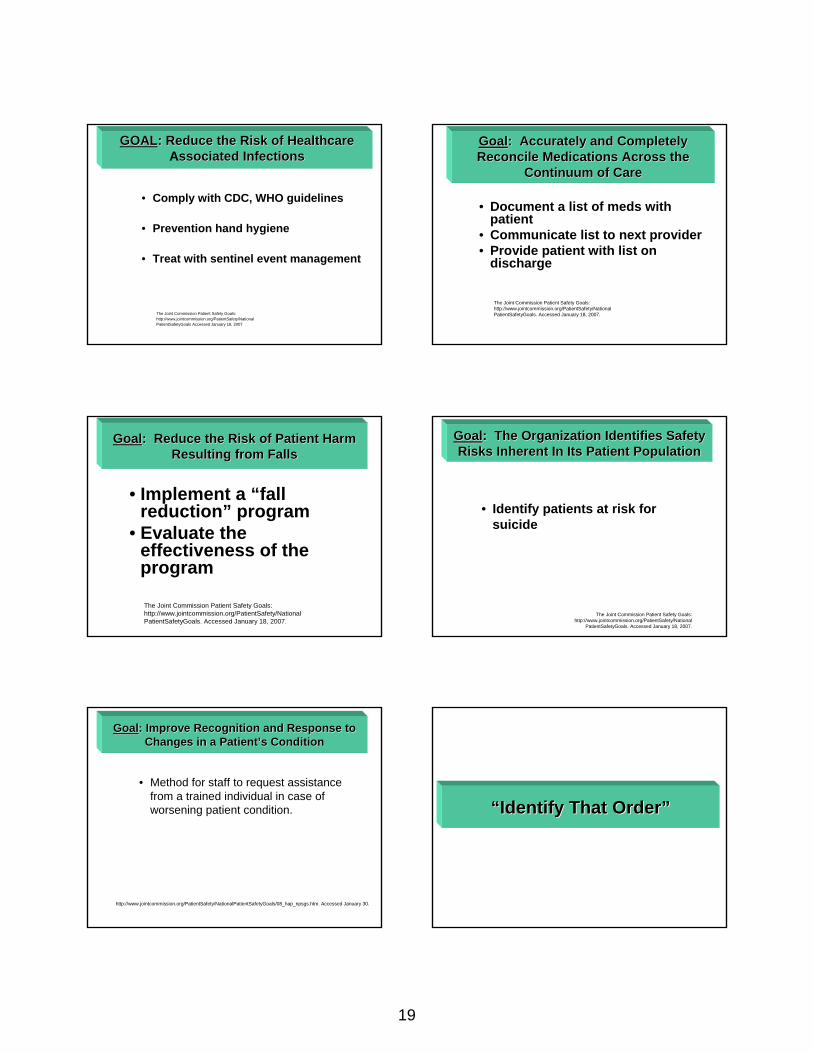
GOALGOAL: Reduce the Risk of Healthcare: Reduce the Risk of HealthcareAssociated Infectionsssociated Infections
• Comply with CDC, WHO guidelines
• Prevention hand hygiene
• Treat with sentinel event management
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals Accessed January 18, 2007
GoalGoal: Accurately and Completely : Accurately and Completely Reconcile Medications Across the Reconcile Medications Across the
Continuum of CareContinuum of Care
• Document a list of meds with patient
• Communicate list to next provider• Provide patient with list on
discharge
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals. Accessed January 18, 2007.
• Implement a “fall reduction” program
• Evaluate the effectiveness of the program
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals. Accessed January 18, 2007.
GoalGoal: Reduce the Risk of Patient Harm : Reduce the Risk of Patient Harm Resulting from FallsResulting from Falls
GoalGoal: The Organization Identifies Safety : The Organization Identifies Safety Risks Inherent In Its Patient PopulationRisks Inherent In Its Patient Population
• Identify patients at risk for suicide
The Joint Commission Patient Safety Goals:http://www.jointcommission.org/PatientSafety/National
PatientSafetyGoals. Accessed January 18, 2007.
GoalGoal: Improve Recognition and Response to : Improve Recognition and Response to Changes in a PatientChanges in a Patient’’s Conditions Condition
• Method for staff to request assistance from a trained individual in case of worsening patient condition.
http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/08_hap_npsgs.htm. Accessed January 30.
““Identify That OrderIdentify That Order””
20
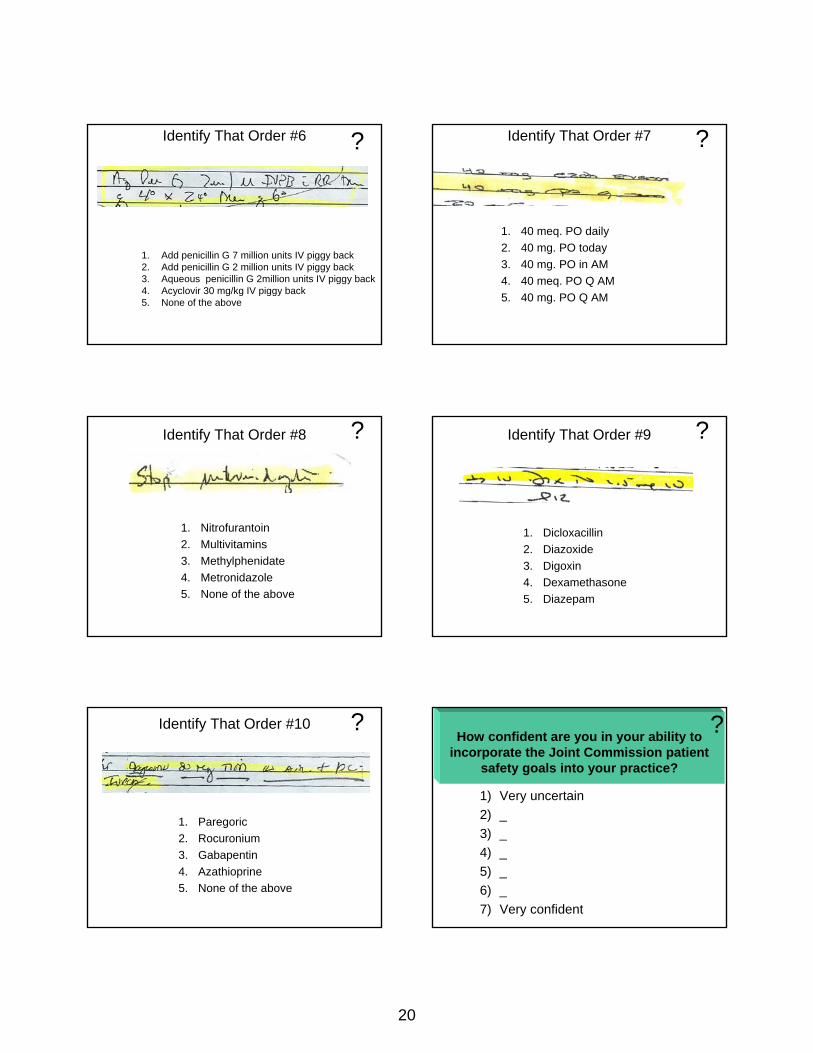
Identify That Order #6 ?
1. Add penicillin G 7 million units IV piggy back2. Add penicillin G 2 million units IV piggy back3. Aqueous penicillin G 2million units IV piggy back4. Acyclovir 30 mg/kg IV piggy back5. None of the above
Identify That Order #7 ?
1. 40 meq. PO daily2. 40 mg. PO today3. 40 mg. PO in AM4. 40 meq. PO Q AM5. 40 mg. PO Q AM
Identify That Order #8 ?
1. Nitrofurantoin2. Multivitamins3. Methylphenidate4. Metronidazole5. None of the above
Identify That Order #9 ?
1. Dicloxacillin2. Diazoxide3. Digoxin4. Dexamethasone5. Diazepam
Identify That Order #10 ?
1. Paregoric2. Rocuronium3. Gabapentin4. Azathioprine5. None of the above
?How confident are you in your ability to incorporate the Joint Commission patient
safety goals into your practice?
1) Very uncertain2) _3) _4) _5) _6) _7) Very confident
21
According to the Joint Commission, what is the most common root cause of sentinel events in
the hospital setting?
1) Staffing2) Continuum of care3) Organization culture4) Communication5) Not sure
What is the most common cause of medication errors in the hospital setting?
1) Ordering2) Transcription3) Dispensing4) Administration5) Not sure
Which of the following is recommended by the Joint Commission when writing
medication orders?
1) Abbreviate microgram “µg”2) Abbreviate once daily “qd”3) Use trailing zeros (eg, 2.0)4) Use leading zeros (eg, 0.2) 5) Not sure
Thank You For Your AttentionThank You For Your AttentionBefore Leaving Before Leaving –– Be Sure Your Be Sure Your
Shoes Are Tied !!Shoes Are Tied !!
By Arnold MacklesMD,MBA,LHRM