Embed Size (px)
Citation preview

Documented and Designed by SAATHII
in association with
New Concept Information Systems Pvt. Ltd.
Website: www.newconceptinfo.com
Copyright: 2009 TANSACS & SAATHII
ACKNOWLEDGEMENTS
1. I-TECH team
2. ART medical officers
3. TNFCC programme partners
4. TNFCC clients
5. TANSACS and SAATHII team
In the fight against HIV/AIDS, Tamil Nadu has achieved a significant reduction in the prevalence, providing an example to other states of how well-planned and comprehensive programmes can help control the epidemic. One such effort is the Clinical Mentorship Programme implemented by Tamil Nadu AIDS Control Society (TANSACS) as part of the 3-year (2005-08) Tamil Nadu Family Care Continuum Programme, in three government hospitals.
The technical assistance and capacity building inputs from SAATHII were crucial to the success of the programme. I-TECH, added to the quality of the training and mentorship component.
The aim of the clinical mentorship programme was to significantly increase the skills of medical officers in the management of HIV/AIDS; the approach was participatory, based on the principles of adult learning. Highly skilled and experienced clinicians were designated as mentors to guide the ART medical officers. Programme components which ensured effectiveness were needs assessment, training, both face-to-face and distance mentoring, and on-going monitoring and evaluation.
The programme has been remarkably successful in ensuring the mentees’ improved skills. Evaluation has demonstrated improved learning’s, improved clinical outcomes and improved documentation. Successful clinical mentorship has been followed by three other programmes: counseling mentorship for hospital and field counselors; home-based care mentorship for outreach workers; and child services mentorship for child counselors.
TANSACS acknowledges SAATHII for its technical assistance to the program, Duke University for monitoring and evaluation, The Children’s Investment Fund Foundation for funding support, and all the TNFCC-associated ART centers, field NGOs and hospital NGOs for effective implementation.
On behalf of TANSACS, I take this opportunity to express our appreciation of hospitals and the Medical Officers contribution to the success of the clinical mentorship programme.
Dr S. Vijayakumar, IAS
Project Director
fOrEWOrD

1. HIV Prevention, Care and Support in India 1
2. Tamil Nadu Family Care Continuum (TNFCC) Programme 4
3. TNFCC - Technical Assistance and Capacity Building 7
4. The Clinical Mentorship Programme - Overview 9
5. The Clinical Mentorship Programme - Training Needs Assessment 12
6. The Clinical Mentorship Programme - Learning Methodology 15
7. The Clinical Mentorship Programme – Findings, Feedback and Outcomes 19
Annexure I - I-TECH Clinical Mentors’ Training Curriculum 24
Annexure II - Tool for Mentorship Assessment 25
Annexure III - Sample Mentorship Report 43
Annexure IV - Case Sheet Documentation for treatment failure 48
CONTENTS

HIV Clinical Mentorship - In a public health context 1
Overview
The revised estimate of people living with HIV in
India (July 2007) puts India in third place in the list
of countries with the largest number of people living
with HIV. Of the estimated 2-3.1 million people
with HIV in India 39% are women and 3.8 % are
children.
The transmission route is predominantly sexual
(87.4%) from high-risk groups to bridge populations
(clients of sex workers, truckers) and then to the
general population.
Globally, the availability of new resources has
accompanied a push for greater access to treatment,
care and support. Never before has the world
attempted, on such a large scale, to bring broad-based
chronic disease management to resource-limited
settings. India, like other countries, has embarked
on aggressive campaigns to control the epidemic.
National response to the AIDS epidemic has been to
decentralize the programme to the state and district
levels to enhance commitment, coverage, and
effectiveness. The goal is to reverse the HIV epidemic
by 2015, and to improve quality of life for people
living with HIV/AIDS (PLHIV) through increased
access to care and support services and, in particular,
Anti Retroviral Therapy (ART).
The national response also recognizes the importance
of maintaining strong prevention efforts. Prevention is
critical in countries, like India, where HIV prevalence
remains low in the wider population and where
opportunities still exist to prevent an exponential rise
in transmission. Where transmission occurs mainly
through risky behaviors, it is critical to continue to
employ robust behavior change intervention efforts
to stem the epidemic.
Care and Treatment Models
Family-centered and comprehensive care models are
recognized as appropriate strategies for mitigating
the impact of AIDS. Access to therapy, nutrition
assistance, and treatment for Opportunistic Infections
(OI) and other health issues that complicate or
exacerbate HIV infection are all integral components
of a comprehensive care model.
It is thus recognized that medical treatment alone is
not sufficient. Programmes offering care and support
to HIV-affected families should integrate psychosocial
services in the treatment process, as well as supportive
services such as financial support, family counselling,
nutritional aids, and palliative care where necessary.
ART programmes should also address the mental
health-related aspects of disease management, and
HIV Prevention, Care and Support in India 1
2 HIV Clinical Mentorship - In a public health context
provide access to psychotropic medications where
possible. Palliative care—in combination with and as
an adjunct to home-based care— also has a role to
play in improving medical care, symptom control, and
mortality from the disease. Appropriate palliative care
also addresses psychosocial issues experienced by
families and surviving children, supports care givers
and communities, and encourages future patients to
come forward earlier in the disease.
National Strategy
Following the detection of the first case of AIDS in
India in 1986, several measures, both governmental
and non-governmental, were taken throughout the
country to curtail the spread of HIV and protect
the rights of People Living with HIV/AIDS (PLHIV).
At present, the National AIDS Control Organisation
(NACO) provides leadership to HIV/AIDS control
programmes in India through 35 HIV/AIDS Prevention
and Control Societies.
The overall goals of NACP-III (National AIDS Control
Programme) is to halt and reverse the epidemic
in India over the next five years by integrating
programmes for prevention, care and support, and
treatment [2]. This will be achieved through a four-
pronged strategy:
l Prevent infections through saturation of coverage
of high-risk groups with targeted interventions
(TIs) and scaled up interventions in the general
population.
l Provide greater care, support, and treatment to
larger numbers of PWLHA.
l Strengthen the infrastructure, systems, and
human resources in prevention, care, support,
and treatment programmes at district, state, and
national levels.
l Strengthen the nationwide Strategic Information
Management System.
The specific target of NACP-III is to reduce the rate
of incidence by 60 percent in the first year of the
programme in high prevalence states to obtain the
reversal of the epidemic, and by 40 percent in the
vulnerable states to stabilise the epidemic.
Care, Support, and Treatment under NACP-III
NACP–III seeks to implement HIV services across the
continuum of care. Accordingly, prevention will go
hand-in-hand with access to prophylaxis, management
of opportunistic infections, and ART. Given the low
levels of coverage, focus will also be on assuring

3HIV Clinical Mentorship - In a public health context
universal access to first line Anti Retroviral drugs
(ARVs) in the first instance. To ensure drug adherence,
the Community Care Centers will be reconfigured as a
bridge between the patient and the ART centers and
provide psychosocial support, counselling through
strong outreach services, referrals, and palliative
care. Home-based care will be an integral part of this
strategy.
Care, support, and treatment services include
management of opportunistic infections including
control of TB in PLHIV, ART, safety measures, positive
prevention, and impact mitigation. By 2011, the
programme will be able to treat 320,000 OI episodes
in a year, provide TB referrals to 2.8 million PLHIV,
and ART treatment to 300,000 PLHIV, including
39,000 children. The component related to Care,
Support, and Treatment is proposed to be allocated
an amount of Rs. 1953 crores accounting for 16.9%
of the total project outlay.

4 HIV Clinical Mentorship - In a public health context
Overview
Tamil Nadu Family Care Continuum (TNFCC) Programme for HIV+ Families is a 3-year programme (September
2005 to August 2008) being implemented by Tamil
Nadu State AIDS Control Society (TANSACS) in
partnership with Solidarity and Action Against the
HIV Infection in India (SAATHII). SAATHII, a non-
profit agency headquartered in Chennai, India,
provides technical assistance and capacity-building
to government and non-government HIV service
providers, and has been helping strengthen and scale
up services in the country since 2000.
In 2005, The Children’s Investment Fund Foundation,
UK (CIFF, UK) awarded funding to TANSACS to expand
ART, with SAATHII designated as the provider of
technical, operational, and logistical assistance.
Tamil Nadu Family Care Continuum (TNFCC) Programme 2
Clinical Mentorship is being carried out in partnership
with International Training and Education Center on
HIV/AIDS (I-TECH). External Monitoring and Evaluation
is being conducted by Duke University, USA.
TNFCC is one of the first and largest public-
private partnerships for HIV care in India. It
serves approximately 14,178 PLHIV, 9,393 families
with children, 13,104 adults, and 1,074 infected
and 10,253 affected children at the end of three
years (September 2005 to August 2008). It has
demonstrated success in reducing HIV-related
morbidity and mortality, and improving quality-
of-life, by providing ART to children and families
infected and affected by HIV/AIDS in the urban and
rural areas of Tamil Nadu.
Of particular note is the fact that TNFCC is one of the
first government programmes to give free 2nd line ART
drugs. Out of the 65,000 PLHIV in Tamil Nadu, around
3–5% requires 2nd line ART. Second line ART is more
expensive (Rs. 6,000–12,000, averaging 10,000 per
month) than 1st line ART (Rs. 650–2,000, depending
on regimen, government procurement rates may
be between Rs. 500–1,500). One of the biggest
achievements of the TNFCC clinical mentorship
programme is streamlined 2nd line initiation. This
process will be discussed later in the document.
TNfCC Programme Objectives:l To develop and evaluate a multi-sectoral model
involving government hospitals, NGOs, CBOs, and
positive networks in providing a comprehensive
continuum of care and treatment to include
medical, psychosocial and nutrition services,
treatment of opportunistic infections, and
provision of ART.
5HIV Clinical Mentorship - In a public health context
l To develop and evaluate an integrated family-
centred continuum of care and treatment model
for HIV positive families.
l To develop successful linkages through
partnerships among various stakeholders
including government, NGOs, CBOs, and PLHIV.
l To integrate community-led treatment
preparedness and literacy programmes with care,
support, and services.
l To evaluate the impact of nutrition support and
counselling on morbidity and mortality in children
and adults.
Expected Outcomes:l Prevent children being orphaned.
l Reduce HIV related mortality and morbidity
among families.
l Achieve 90% adherence among adults receiving
ARV therapy.
l Improve quality of life among families.
Programme Overview
SitesThree hospital sites cater to ten districts:l Kilpauk Medical College Hospital (Chennai
cluster) - Chennai, Tiruvallur, Kanchipuram and
Villupuram.
l Govt. Mohan Kumaramangalam Medical College
Hospital (Salem cluster) - Salem, Erode,
Dharmapuri, and Perambalur.
l Govt. Medical College Hospital (Tirunelveli
cluster) - Tirunelveli, and Tuticorin.
Hospital Activities
The three government medical college hospitals
function as hospital programme sites and are responsible
for coordinating and providing comprehensive care,
support, and treatment services.
The hospital-based services are provided by
hospital staff, government appointed doctors, and
representatives of community based organizations.
Hospital and NGO Partners of the TNfCC programme
Hospital Districts covered Hospital NGO field NGOs, CBOs and Positive Networks
Government Kilpauk
Medical College
Hospital, Chennai
Chennai, Tiruvallur,
Kanchipuram, and
Villupuram
Community Health
Education Society (CHES)
SIP+, MSDS, and ACD
Government Mohan
Kumaramangalam
Medical College
Hospital, Salem
Salem, Erode,
Dharmapuri, and
Perambalur
Young Women
Christian Association
(YWCA), Salem
YWCA, HILLS,
SEARCH, and INDO
Government Medical
College Hospital,
Tirunelveli
Tirunelveli, Tuticorin,
and Kanniyakumari
Gramodhaya Social
Service Society
PWST+, St. Joseph
Leprosy Hospital
6 HIV Clinical Mentorship - In a public health context
For each ART Center, TANSACS has recruited and
trained 2 ART medical officers, 1–2 counsellors,
1 lab technician, 1 pharmacist, 1 community care
coordinator, and 1 data entry operator. While this
staffing pattern is similar to that of ART Centers
across the country, TNFCC sites were established with
supplemental staffing in the form of a trained NGO
support team, consisting of the following personnel:
l 1 Project Coordinator
l 1–2 Counsellors
l 1–2 Nutritionists
l 1–2 Nurse Case Mangers
l 2 Nursing Aides
l 1 Pharmacist
l 1 Accountant/Data Entry Operator
l 1 Sanitary Worker
After the second year of operation, the NGO staff were
slowly phased out once the ART staff were added, as
per the revisions in national ART centre operational
guidelines. The NGO staff numbers have varied across
the three centers, in accordance with the prevailing
client load.
field Activities
Community services provided by NGOs in each of
these ten districts are as follows:
l Identification of HIV clients and motivation of
patients for hospital registration and monthly
follow-up visits
l Conducting support groups near the patient’s
residence
l Identification and training of peer educators and
care givers
l Provision of home-based care that includes
opportunistic infections diagnosis and referrals,
as well as ongoing adherence counselling
l Referrals and linkages to various services like
housing, income generation, legal services, etc.
l Child counselling and related services
All services are provided by the Project Coordinator,
Child Counsellor, Community Health Nurse, and 8–10
Outreach Workers of the field NGOs affiliated with the
respective ART Centers.

7HIV Clinical Mentorship - In a public health context
SAATHI (Solidarity and Action Against The HIV Infection in India) has served as technical assistance
partner for TNFCC, providing training, support visits,
coordination, networking, ongoing technical updates,
and mentorship.
Training
TANSACS and SAATHII conducted training for various
stakeholders on the following topics (target trainee
population shown in parentheses):
l Clinical Management of HIV/AIDS (counsellors, lab
technicians, nutritionists, pharmacists, sanitary
workers, project coordinators, community health
nurses, child counsellors, and outreach workers)
l Home-based Care (nurses, counsellors, project
coordinators, nutritionists, outreach workers,
community health nurses)
l Adherence Counselling (hospital and field
counsellors and coordinators, community health
nurses, and outreach workers)
l Child Counselling (ART counsellors and field child
counsellors)
l Life-skills Training (field project coordinators,
child counsellors)
l Financial Management (project head, project
coordinators, accountants)
l Training on Organization Development/
Management, Leadership, and Communication
(NGO heads and project coordinators)
l Induction and advanced training for
nutritionists
l Training and mentorship to hospital and field
counsellors and outreach workers on general
counselling with a component on HIV/AIDS
(disclosure, safe sex, and stigma)
TNFCC - Technical Assistance and Capacity Building 3
l Home-based care mentorship training for
community project coordinator, child counsellors,
and community health nurse for mentoring
outreach workers
l Child Services training for the community child
counsellors
l Training for ART medical officers (see below).
ART medical officers were trained at the start of the
TNFCC programme—four days in Tambaram Sanatorium
and six days in YRG Care. The Tambaram training
complied with NACO Guidelines and covered OI, ART,
side effects, documentation and reporting, monitoring,
clinical rounds, and pediatric HIV care. The training
at YRG covered second line drugs, system-wide HIV
clinical management, hospital-waste management,
universal work precautions, clinical rounds, and case
studies. Tools were adapted from the Clinical Mentoring
Toolkit developed by the International Training and
Education Center on HIV (I-TECH).
The contents of induction training were repeated
during Years II and III because of high staff

8 HIV Clinical Mentorship - In a public health context
turnover. The training was made specific and target-
focused in order to ensure that participants attained
the necessary level of competence. All training
programmes were conducted within the first three
years since TNFCC’s inception.
SAATHII provides technical updates during support
visits and programme coordination meetings at ART
centers where hospital ART team and community
NGO teams interface. Discussions focus on the issues
arising out of the daily work of programme staff,
especially outreach workers. Technical assistance
to NGOs helps in identifying field-based solutions
through monthly monitoring visits and ongoing need-
based support. For instance, several outreach workers
have difficulties in talking about sex, ART treatment,
and disclosure so SAATHII conducts regular follow-up
on the trainings provided.
Mentorship Initiatives
There are four Mentorship programmes under the
TNFCC:
l Clinical Mentorship to ART medical officers
(provided by SAATHII and I-TECH)
l Counselling Mentorship to hospital and field
counsellors (SAATHII)
l Home-based Care Mentorship to outreach workers
(SAATHII and Field NGO Core Team: Project
Coordinator, Child Counsellor, Community Health
Nurse)
l Child Services Mentorship to child counsellors
(SAATHII)
The clinical mentorship programme was the first
of its kind in the programme, and in the country,
and its success resulted in launching of mentorship
initiatives in the other domains listed above. The
clinical mentorship programme will be presented in
detail in the following section.
For the counselling mentorship programme, four days
of training were provided (two days each, in two
rounds from January to March 2008). In addition,
one-day visits were made twice to the hospitals.
These visits involved counselling and observations
in the morning, and case study discussions among
hospital and field counsellors, in the afternoon. The
mentorship activities were implemented by SAATHII
with initial assistance from external experts.
Initial home-based care mentorship was provided by
SAATHII. However, due to an increased number of
outreach workers in the third year (around 100), a
mentorship training was conducted by SAATHII for
selected field staff (20–25 total, two to three from
each community NGO) who then constituted the core
field team. This helped broaden and decentralize the
pool of mentors.
The child services mentorship was provided by SAATHII
to the community NGO-based child counsellors.
Training covered life skills education, recreation,
education and referrals, and linkages to additional
services.

9HIV Clinical Mentorship - In a public health context
Background and Partners
A significant need addressed through the TNFCC
programme was capacity enhancement of the local
health institutions in HIV care and treatment,
especially in management of complicated and
challenging cases in relation to OIs, and ART (first
and second line drugs). SAATHII identified clinical mentoring as an appropriate strategy to develop
this expertise among local health care providers.
Structured clinical mentoring, using adult learning
principles, helped bridge the training gap between
traditional didactic trainings and practice in the
clinical setting.
SAATHII identified the International Training and
Education Center on HIV/AIDS (I-TECH) as the
technical partner to develop the Clinical Mentorship
Programme for TNFCC. I-TECH is a global AIDS training
programme working at the invitation of ministries of
health and the U.S. government to increase human
and institutional capacity for care and treatment in
countries hardest hit by the HIV and AIDS epidemic.
The Clinical Mentorship Programme – Overview 4
I-TECH is collaboration between the University of
Washington, Seattle, and University of California,
San Francisco.
I-TECH’s model of Clinical Mentorship
I-TECH’s primary objectives for clinical
mentoring are consistent with the World Health
Organization’s public health approach to scaling
up HIV care and ART. These objectives include:
lSupporting decentralized delivery of HIV care,
ART and prevention, as well as continuous
improvement of patient outcomes at all ART
delivery sites.
lPromoting application of classroom learning
to clinical settings.
lImproving the quality of clinical care and
patient outcomes in resource-constrained
settings.
lBuilding capacity of primary care providers
to provide comprehensive and integrated
care using on-site clinical collaboration,
consultation, and directed support
SAATHII collaborated with I-TECH in curriculum
adaptation, mentor programme design and
implementation.
Geographical SitesThe Clinical Mentorship Programme has been implemented
in ART centers in three districts—Government Kilpauk
Medical College Hospital in Chennai, Government Mohan
Kumaramangalam Medical College Hospital in Salem,
and Government Medical College Hospital in Tirunelveli.
These three sites cater to families from three focal and
seven surrounding districts.

10 HIV Clinical Mentorship - In a public health context
Who is a Clinical Mentor?As defined by WHO: “A clinical mentor in the
antiretroviral therapy context is a clinician with
substantial expertise in antiretroviral therapy and
opportunistic infections who can provide ongoing
mentoring to less-experienced HIV clinical providers
by responding to questions, reviewing clinical cases,
providing feedback and assisting in case management.
This mentoring occurs during site visits as well as
via ongoing phone and e-mail consultation. Clinical
mentoring is critical to building successful district
networks of trained health care workers for HIV care
and treatment in resource-constrained settings.”
The Clinical Mentorship Programme involves two mentors
from I-TECH, one mentor from SAATHII, and seven
mentees, who are medical officers at the ART Centers
that were included in the TNFCC programme. When
mentorship was initiated in April 2007, the mentees
already had a case load of around 12,000 HIV/AIDS
patients altogether at three sites, including over 4,000
patients on ART, of whom 80 are on 2nd line drugs.
The mentors possess clinical knowledge, training and
interpersonal communication skills. Key mentoring
strategies included building rapport, giving feedback
effectively, identifying teaching moments, teaching
at the bedside, and addressing systemic issues.
For greater details on the Clinical Mentors’ Training
Curriculum, refer to www.go2itech.org
Mentorship Methodology
Mentorship is an ongoing process whereby the
mentor assists and assesses the patients’ condition
and line of treatment both directly during visits and
through distance mentorship to ART medical officers
based on details provided via email or telephone.
Mentorship includes, at a minimum, the following
components:
l Orientation of external mentor by SAATHI
mentor
l Planning and tool development by mentors
l Training and needs assessment of the ART medical
officers by SAATHII mentor
l Reliance on adult learning principles
l On-site two-day hospital visits by mentors to
each of the hospitals every three months
l Long-distance mentorship
Onsite MentorshipThe mentor makes quarterly visits to the hospitals
and engages directly with the doctors and the
patients identified by the mentee as case studies. In
addition, the mentor examines individual patients as
requested by the mentee. Onsite mentorship entails
the following:
lOnsite review of medical practices at the hospitals
with the doctors
lIdentifying training needs and areas for
strengthening
lMentoring the doctors by the various methods
elaborated below:
lModeling
lFacilitation of various case studies and
discussions
lHands-on training
lAdditional clinical training using adult learning
principles
lSharing of supplementary reading materials from
peer-reviewed journals.
lAdvocacy with mentees for systematized case-
management, laboratory investigations and
documentation
lFacilitating data collection, best practices
sharing, and clinical research
11HIV Clinical Mentorship - In a public health context
Distance MentorshipThis component of the mentorship programme is
probably the most pragmatic, as it ensures continuous
and adaptive learning. The mentees call or email
the mentors periodically, enabling timely treatment
of patients, and establishing open communication
between mentor and mentee.
Distance Mentorship entails the following:
lOngoing consultation with doctors by phone and
lExchange of case sheets, scans, and other relevant
documents
lSharing of reference material to enhance
learning
Focus Areas of Mentor Involvement lRoutine clinical care for HIV and associated
medical conditions
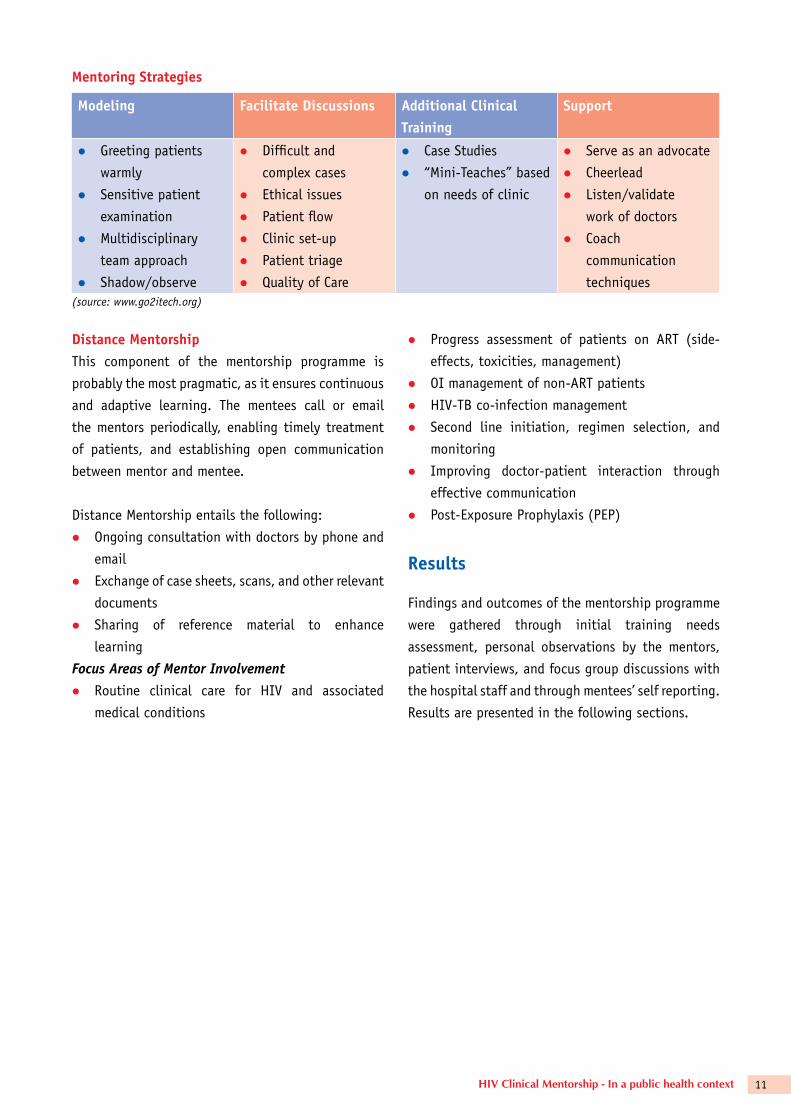
Mentoring Strategies
Modeling facilitate Discussions Additional Clinical Training
Support
l Greeting patients
warmly
l Sensitive patient
examination
l Multidisciplinary
team approach
l Shadow/observe
l Difficult and
complex cases
l Ethical issues
l Patient flow
l Clinic set-up
l Patient triage
l Quality of Care
l Case Studies
l “Mini-Teaches” based
on needs of clinic
l Serve as an advocate
l Cheerlead
l Listen/validate
work of doctors
l Coach
communication
techniques(source: www.go2itech.org)
lProgress assessment of patients on ART (side-
effects, toxicities, management)
lOI management of non-ART patients
lHIV-TB co-infection management
lSecond line initiation, regimen selection, and
monitoring
lImproving doctor-patient interaction through
effective communication
lPost-Exposure Prophylaxis (PEP)
results
Findings and outcomes of the mentorship programme
were gathered through initial training needs
assessment, personal observations by the mentors,
patient interviews, and focus group discussions with
the hospital staff and through mentees’ self reporting.
Results are presented in the following sections.
12 HIV Clinical Mentorship - In a public health context
The Mentees
A needs-assessment of the seven mentees was conducted
at the beginning of the mentorship. The following
synopsis reflects the experience in all three centers:
1. Prior experience in the HIV/AIDS fieldWork experience varied among doctors, with two
having less than two years of experience, and the
rest five either 2–4 years, 4–6 years, or 8–10 years.
All but one had previous AIDS-related work experience
in hospitals, private clinics, or with NGOs.
2. Patients treated per month
Hospital PLHIV PLHIV on ArT
Tirunelveli 1,000 250–300
Kilpauk Medical
College Hospital
2,100 530
Salem 4,500 1,500
Average 2,533 768
3. Previous trainingsAll of the doctors had attended previous HIV-related
trainings. These include:
lGHTM – NACO – 4 attendees
lYRG Care – 4 attendees
lHIV-TB/ATT-RNTCP – 4 attendees
lDr. MGR Medical University – 1 attendee
lInternational Conference, University of
Hyderabad – 1 attendee
lCME, Karigiri – 1 attendee
lCME, YRG – 2 attendees
lWHO IMAI training, St. John’s Bangalore –
1 attendee
lClinton Foundation – IMA doctors training
– 1 attendee
Clinical Mentorship Programme – Training Needs Assessment5
4. Training formatslThe most preferred training formats were:
t Conferences
t Printed materials (journals, newsletters, etc.)
t Skill building workshops
t Case presentation seminars
lThe least preferred training format was weekend
case discussions.
lEach doctor listed a separate preference for
frequency of ongoing trainings.
lMost of the doctors agreed that one working day
a month could be dedicated to training, either as
four hours each day for two days, or one day of
eight hours.
lInternet access: Tirunelveli and Salem had
unrestricted access to internet use, but KMCH
only received access towards the mid-mentorship
period.
13HIV Clinical Mentorship - In a public health context
5. Barriers to traininglThe most commonly cited barrier to training was
long travel times to Chennai.
Suggested solutions:
tMake Madurai or Tiruchi the centre for
trainings
tConduct trainings at all three sites, on a
rotating basis
lSalem indicated that both ART medical officers
could not attend at the same time.
Suggested solution: Assign an alternate/additional
ART medical officer
lKMCH cited lack of access to internet as a
barrier.
Suggested solution: Printed materials and CDs
Training Needs Assessment
Doctors were presented with a set of HIV-related
topics, and asked to indicate their level of skill in
each and their learning interest (as high, medium
or low).
The doctors expressed the highest learning interest in
topics listed below. Items that are starred are those
in which they also indicated low levels of skill.
1. Lab Diagnosis of HIV Infection – Therapeutic diagnoseslHIV RNA PCR
lCD4 Count testing
lOther markers*
lCulture and resistance*
2. Opportunistic Infections and Co-InfectionslClinical presentation
lLab and clinical diagnosis of OIs
lDifferential diagnosis
lTreatment
lGIT manifestations
lDental manifestations*
lOphthalmic manifestations*
lNeurological manifestations
lTuberculosis*
3. Pediatric HIVlGrowth and development parameters
lLab diagnosis (<18 months)
lART
lSecond line regimen
lART and ATT
lART in women (pregnancy and PMTCT)
lImmune Reconstitution Syndrome
lWhen to change treatment (resistance and
treatment failures)
5. HIV and Psychiatry
6. HIV Virology lMechanism of resistance
7. HIV and Gynecology*
8. HIV and Wasting*
9. HIV and Nutrition* lNutritional counselling
10. Legal, Ethical, Cultural Issues*
The doctors expressed low skill but only moderate
learning interest in the following:
lEconomic, health care, and socio-cultural issues
impacting patients.
lCurrent trends in epidemiology – India, Global
lPalliative care
lStructured treatment interruptions
14 HIV Clinical Mentorship - In a public health context
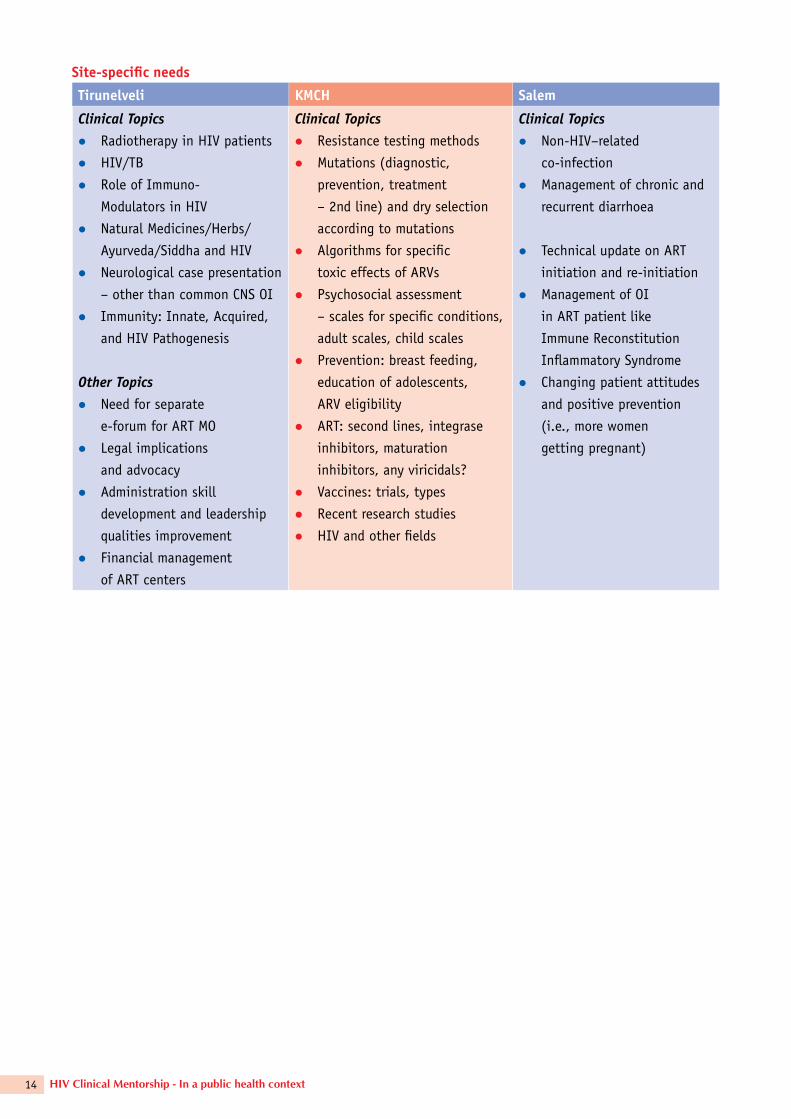
Site-specific needs
Tirunelveli KMCH Salem
Clinical TopicslRadiotherapy in HIV patients
lHIV/TB
lRole of Immuno-
Modulators in HIV
lNatural Medicines/Herbs/
Ayurveda/Siddha and HIV
lNeurological case presentation
– other than common CNS OI
lImmunity: Innate, Acquired,
and HIV Pathogenesis
Other TopicslNeed for separate
e-forum for ART MO
lLegal implications
and advocacy
lAdministration skill
development and leadership
qualities improvement
lFinancial management
of ART centers
Clinical TopicslResistance testing methods
lMutations (diagnostic,
prevention, treatment
– 2nd line) and dry selection
according to mutations
lAlgorithms for specific
toxic effects of ARVs
lPsychosocial assessment
– scales for specific conditions,
adult scales, child scales
lPrevention: breast feeding,
education of adolescents,
ARV eligibility
lART: second lines, integrase
inhibitors, maturation
inhibitors, any viricidals?
lVaccines: trials, types
lRecent research studies
lHIV and other fields
Clinical TopicslNon-HIV–related
co-infection
lManagement of chronic and
recurrent diarrhoea
lTechnical update on ART
initiation and re-initiation
lManagement of OI
in ART patient like
Immune Reconstitution
Inflammatory Syndrome
lChanging patient attitudes
and positive prevention
(i.e., more women
getting pregnant)

15HIV Clinical Mentorship - In a public health context
As described in Section IV, Overview, the TNFCC
Clinical Mentorship Programme incorporates three
primary learning components – use of adult learning
principles, onsite and Distance Mentorship. Training
tools were adapted from the Clinical Mentoring
Toolkit developed by I-TECH. (For additional
information on the I-TECH training curriculum, see
Annexure - I)
The following section explores these components in
greater detail.
Adult Learning as Basic Approach
The clinical mentorship programme is designed
on the premise that adult learning techniques are
the most effective in skills transfer. Adult learning
principles emphasize that adults come to learning
environments with:
ltheir own experience and expertise
lan expectation that they will be respected and
guided
land a focused motivation to learn based on
specific needs to accomplish job-related tasks
more effectively
The experience at Tirunelveli provides a case study on
the use of these learning principles within the clinical
mentorship programme. Dr. Narayana Srinivasan,
Senior Medical Officer at the Government Medical
College Hospital, Tirunelveli, calls this a unique
programme because it was developed in response to a
personal needs-assessment. The mentor’s first question
was ‘what are your expectations?’ The mentor seeks
to identify strengths and weaknesses and provides
assistance accordingly. The mentors work ‘beside’ the
doctors and not above them. The center has a case
load of 250 patients a day. The mentor recognizes the
The Clinical Mentorship Programme – Learning Methodology 6
challenges faced by the doctors and the staff, as well
as the demands made upon them.
The mentors have been very willing to share
information. The doctor calls the mentor everyday on
the I-TECH hotline to discuss any problems or doubts
he may have. These conversations cover a range of
issues including drug adjustment, availability of
drugs, and drug dosage. A recent example is that
of a patient with renal failure – the mentee sought
guidance regarding on how to assess changing levels
of kidney functions, and the need to adjust ARV
dosages accordingly.
Moreover, the mentorship is not purely clinical -- the
mentors urge the doctors to use interpersonal skills
which enhance their role as a doctor, such as how to
elicit information from reluctant/hesitant patients or
how to counsel them on behavior change.
16 HIV Clinical Mentorship - In a public health context
Mentorship through On-Site Visits
The first round of On-site Mentorship for the ART medical
officers of three TNFCC centers was implemented during
the first quarter of the grant period. This round followed
a tools development for mentors and training needs
assessment of the ART medical officers (mentees). On-
site visits proceeded as follows:
(a) The mentor outlined the objectives/purpose of
the visit to the medical officer: to improve the
skills of the ART medical officer. The mentor also
reviewed the principles of mentorship and the
specifics of the two-day schedule.
(b) On the first day’s morning session, observation
was used to assess the medical officer’s clinical
knowledge, skills, attitudes, and practices. Mentors
sat with the medical officers at the ART clinic.
(c) In the afternoon, discussions/trainings were
conducted to share observations, explore
challenging cases, review national guidelines,
and discuss the feasibility of implementation.
Mentors also shared their work experiences in
other settings as a way to discuss ‘best practices’.
In addition, the following issues were covered in
detail: ART toxicities, substitution of ARVs, privacy
of examination, flow of patients at the ART centre,
the role of the nurse case manager at the ART
centre, and HIV/TB co-infection management.
(d) On the second day, apart from mentoring in the
outpatient department, the mentor:
lPerformed ward rounds and hands-on-training
on the wards
lled detailed case discussions on second line
drugs using actual case studies from the ART
centre
laddressed gaps in case management and in
the documentations of second line cases;
and, made suggestions as to how to rectify
the problems using the check list, a draft
copy of which was handed out
ldemonstrated how to use the Stanford guide
in interpreting the genotype resistance study
results using the appropriate web site
lusing case records, stressed how important it
is for the medical officer to examine patients
on second line drugs
lexplained the importance of documentation
related to death and other interesting cases
lgave the medical officers important web sites
for reference, and shared articles related to
areas of interest
Recommendations were made to all three sites based
on the first round of visits. See box below. The tool for
mentorship assessment is provided in Annexure - II
Distance Mentorship
Distance Mentorship in this programme has been
actively encouraged and a ‘hotline’ between the
doctors and the mentor allows for open and regular
communication. Several doctors said that they would
call the mentors 3–4 times a day. Distance Mentorship
included:
(e) Ongoing consultation with the doctors through
various communication modes like phone calls
and e-mails
(f) Monthly follow-up meetings with Technical
Assistance (TA) and Implementer
(g) Quarterly field visits by the mentor. On these
occasions, special cases are directly presented
to the mentor. In addition, observations and
discussions with mentees give the mentor an
opportunity to observe any other infrastructure
needs doctors may have. (See more about On-Site
mentorship above).
17HIV Clinical Mentorship - In a public health context
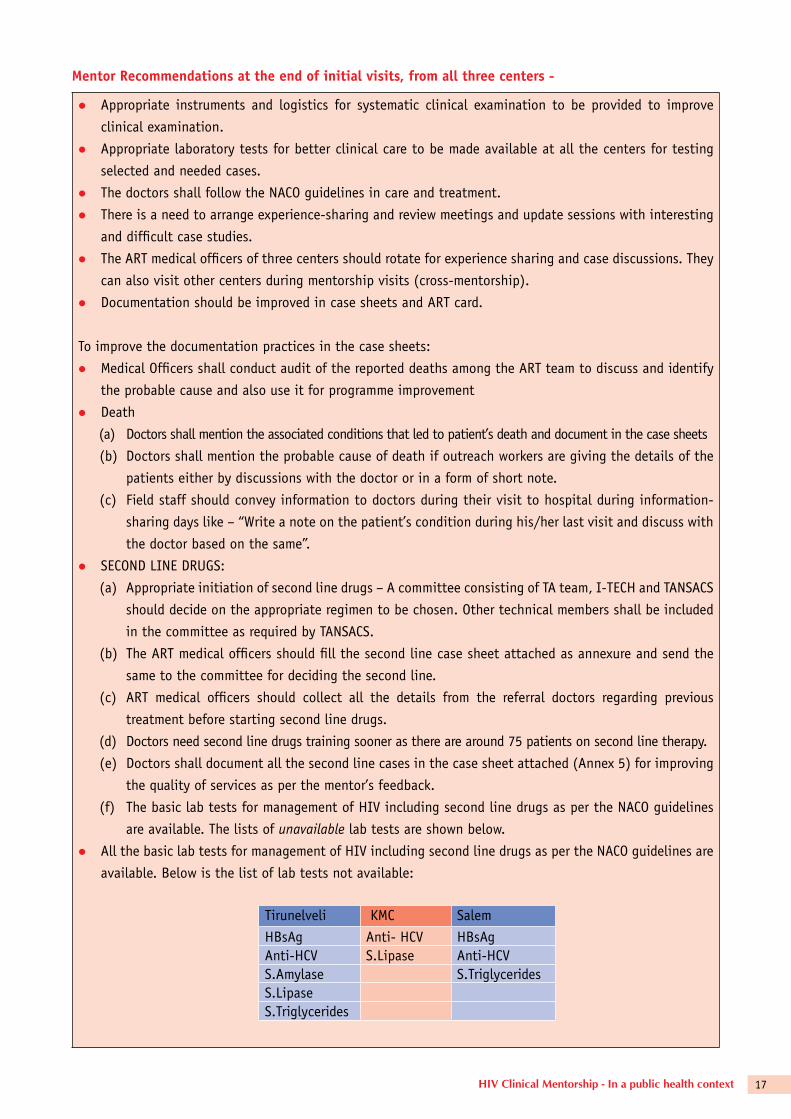
Mentor recommendations at the end of initial visits, from all three centers -
lAppropriate instruments and logistics for systematic clinical examination to be provided to improve
clinical examination.
lAppropriate laboratory tests for better clinical care to be made available at all the centers for testing
selected and needed cases.
lThe doctors shall follow the NACO guidelines in care and treatment.
lThere is a need to arrange experience-sharing and review meetings and update sessions with interesting
and difficult case studies.
lThe ART medical officers of three centers should rotate for experience sharing and case discussions. They
can also visit other centers during mentorship visits (cross-mentorship).
lDocumentation should be improved in case sheets and ART card.
To improve the documentation practices in the case sheets:
lMedical Officers shall conduct audit of the reported deaths among the ART team to discuss and identify
the probable cause and also use it for programme improvement
lDeath
(a) Doctors shall mention the associated conditions that led to patient’s death and document in the case sheets
(b) Doctors shall mention the probable cause of death if outreach workers are giving the details of the
patients either by discussions with the doctor or in a form of short note.
(c) Field staff should convey information to doctors during their visit to hospital during information-
sharing days like – “Write a note on the patient’s condition during his/her last visit and discuss with
the doctor based on the same”.
lSECOND LINE DRUGS:
(a) Appropriate initiation of second line drugs – A committee consisting of TA team, I-TECH and TANSACS
should decide on the appropriate regimen to be chosen. Other technical members shall be included
in the committee as required by TANSACS.
(b) The ART medical officers should fill the second line case sheet attached as annexure and send the
same to the committee for deciding the second line.
(c) ART medical officers should collect all the details from the referral doctors regarding previous
treatment before starting second line drugs.
(d) Doctors need second line drugs training sooner as there are around 75 patients on second line therapy.
(e) Doctors shall document all the second line cases in the case sheet attached (Annex 5) for improving
the quality of services as per the mentor’s feedback.
(f) The basic lab tests for management of HIV including second line drugs as per the NACO guidelines
are available. The lists of unavailable lab tests are shown below.
lAll the basic lab tests for management of HIV including second line drugs as per the NACO guidelines are
available. Below is the list of lab tests not available:
Tirunelveli KMC Salem
HBsAg Anti- HCV HBsAgAnti-HCV S.Lipase Anti-HCVS.Amylase S.TriglyceridesS.LipaseS.Triglycerides
18 HIV Clinical Mentorship - In a public health context
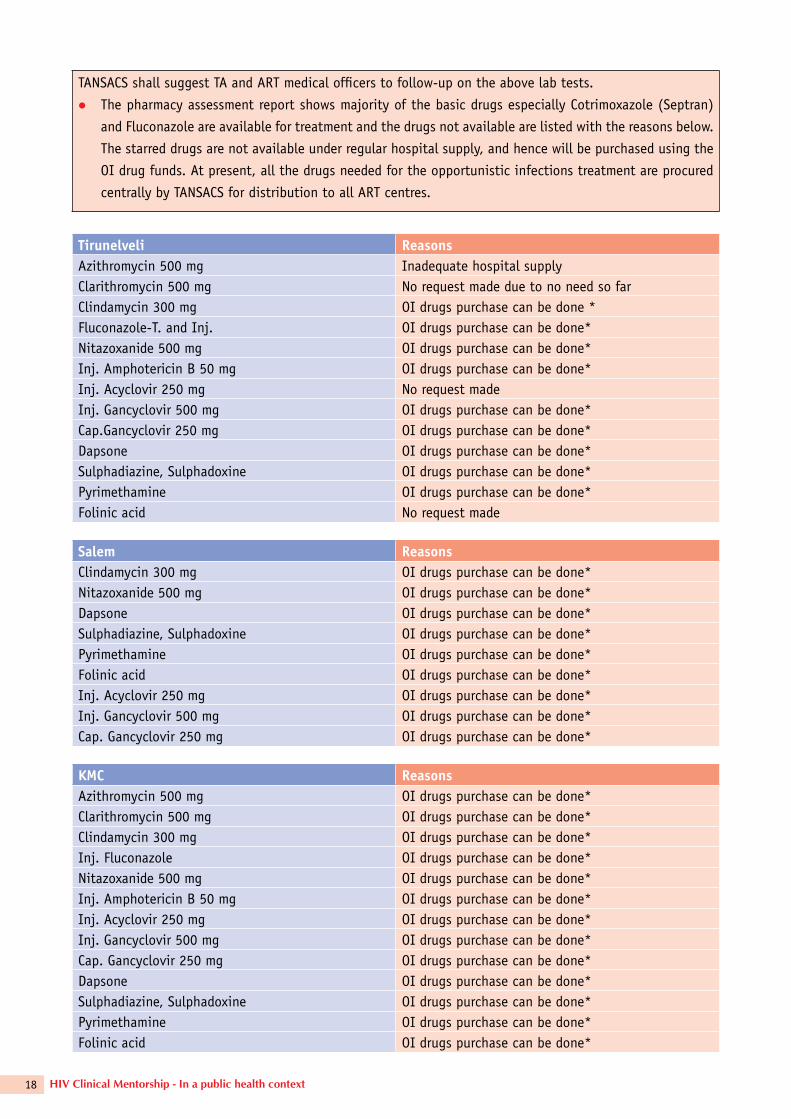
TANSACS shall suggest TA and ART medical officers to follow-up on the above lab tests.
lThe pharmacy assessment report shows majority of the basic drugs especially Cotrimoxazole (Septran)
and Fluconazole are available for treatment and the drugs not available are listed with the reasons below.
The starred drugs are not available under regular hospital supply, and hence will be purchased using the
OI drug funds. At present, all the drugs needed for the opportunistic infections treatment are procured
centrally by TANSACS for distribution to all ART centres.
Tirunelveli reasonsAzithromycin 500 mg Inadequate hospital supplyClarithromycin 500 mg No request made due to no need so farClindamycin 300 mg OI drugs purchase can be done *Fluconazole-T. and Inj. OI drugs purchase can be done*Nitazoxanide 500 mg OI drugs purchase can be done*Inj. Amphotericin B 50 mg OI drugs purchase can be done*Inj. Acyclovir 250 mg No request madeInj. Gancyclovir 500 mg OI drugs purchase can be done*Cap.Gancyclovir 250 mg OI drugs purchase can be done*Dapsone OI drugs purchase can be done*Sulphadiazine, Sulphadoxine OI drugs purchase can be done*Pyrimethamine OI drugs purchase can be done*Folinic acid No request made
Salem reasonsClindamycin 300 mg OI drugs purchase can be done*Nitazoxanide 500 mg OI drugs purchase can be done*Dapsone OI drugs purchase can be done*Sulphadiazine, Sulphadoxine OI drugs purchase can be done*Pyrimethamine OI drugs purchase can be done*Folinic acid OI drugs purchase can be done*Inj. Acyclovir 250 mg OI drugs purchase can be done*Inj. Gancyclovir 500 mg OI drugs purchase can be done*Cap. Gancyclovir 250 mg OI drugs purchase can be done*
KMC reasonsAzithromycin 500 mg OI drugs purchase can be done*Clarithromycin 500 mg OI drugs purchase can be done*Clindamycin 300 mg OI drugs purchase can be done*Inj. Fluconazole OI drugs purchase can be done*Nitazoxanide 500 mg OI drugs purchase can be done*Inj. Amphotericin B 50 mg OI drugs purchase can be done*Inj. Acyclovir 250 mg OI drugs purchase can be done*Inj. Gancyclovir 500 mg OI drugs purchase can be done*Cap. Gancyclovir 250 mg OI drugs purchase can be done*Dapsone OI drugs purchase can be done*Sulphadiazine, Sulphadoxine OI drugs purchase can be done*Pyrimethamine OI drugs purchase can be done*Folinic acid OI drugs purchase can be done*

19HIV Clinical Mentorship - In a public health context
The Clinical Mentorship Programme, implemented by
I-TECH and SAATHII, in partnership with TANSACS,
has demonstrated success in
1. Improved learning;
2. Improved clinical outcomes;
3. Improved documentation.
1. Improved Learning
The most significant emerging practice in the Clinical
Mentorship Programme is the culture of new and
continued learning for the entire team of health care
professionals in the three hospitals:
(a) Government Kilpauk Medical College Hospital,
Chennai
(b) Government Mohan Kumaramangalam Medical
College Hospital, Salem
(c) Government Medical College Hospital, Tirunelveli
Based on the pedagogical principles of adult learning,
the programme has made a significant impact on
the approach to HIV care and treatment, and laid a
strong foundation for continuous and renewed adult
learning.
Dr.Thennarasu from Kilpauk Medical Hospital affirms,
“The Clinical Mentorship has shaped me!” The
mentorship programme has brought him in contact
with senior professionals and has improved his
knowledge and skills in dealing with patients. A
focus group discussion with the project coordinator,
nutritionist, nurse, and lab technician at Government
Mohan Kumaramangalam Medical College Hospital
in Salem revealed that even though they have not
interacted with Dr. Manoharan (the mentor) directly,
they are aware of his expertise and knowledge. The
process of continuous learning has had a ripple
The Clinical Mentorship Programme – Findings, Feedback and Outcomes 7
effect. They have learnt when to change the regimen
and are more comfortable with preparing nutrients
for special cases, and making home visits. Health care
professionals in Salem indicate that their knowledge
of HIV has increased not only in care and treatment,
but in counselling as well.
Mentorship programme enhances the mentees’ existing expertise This enhanced expertise translates into higher job
satisfaction for doctors and, ultimately, into higher
patient satisfaction rates. For example, Mr.Rajan
(name changed)—a 35-year-old lorry driver who has
been coming to Tirunelveli since 2005—was aware
that when the new drug prescribed did not agree
with him, it was changed in consultation with an
‘external’ doctor.
This alternative route to learning has set a precedent
in the programme to foster an open environment
where there is easy access to information and
enhanced communication and collaboration at all
20 HIV Clinical Mentorship - In a public health context
levels. Besides this, the process of continued learning
is a new experience for the doctors who are used to
attending trainings that are either too didactic or
too short to address the complexities of HIV care and
treatment. Simple standardized guidelines for care
do not fit in many cases. The nuances of managing
drug interactions and toxicities against the backdrop
of underlying liver disease and co-infections are
challenges the medical world is trying to meet at
every turn. It requires expertise and a progressive
approach, which a mentorship programme provides
for both the mentor and the mentee.
Clinical mentors help the mentees translate theoretical knowledge into practical clinical skills Dr. Thennarasu at Kilpauk Medical Hospital admits
that his knowledge of HIV/AIDS prior to the launch of
mentorship was quite limited. His specialization is in
ophthalmology, and there was no component of HIV/
AIDS in his medical curriculum. It was only through
the Clinical Mentorship programme that he became
aware of diagnostic challenges and other clinical
considerations that steer the line of treatment. The
mentor advises him on when to run viral load and
resistance tests, and when to start 2nd line ART. Dr.
Sentha Krishna from Salem Government Hospital
explains, “I am more confident about handling cases
now.” She now treats complications like Cryptococcal
meningitis and Zidovudine anemia (caused by ART
toxicity) because of the knowledge she gained
through mentorship.
The mentors have been very willing to share
information, and they give the doctor tips on how to
elicit information from reticent patients. The doctors
call the mentors regularly on the I-TECH hotline for
advice on drug adjustment, dosage, and availability.
Detailed case histories are sent through email, while
X-rays, CT scans, and photographs are couriered at
least 2–3 times a month.
2. Improved Clinical Outcomes
Key outcomes of the clinical mentorship programme
have included streamlining of 2nd line ART initiation
and improved management of complicated cases
including kidney, liver and CNS issues.
TNFCC was one of the first initiatives in the country to
make 2nd line ART drugs available. Out of the 65,000
PLHIV in Tamil Nadu, around 5% require 2nd line ART.
NACO started 2nd line ART recently.
As Dr Sathish puts it, “one of the biggest
achievements of clinical mentorship is streamlined
2nd line initiation.” The complexity of managing
difficult cases means that standard protocols and
straightforward algorithms cannot always be applied.
Individual clinical judgment needs to be supported
through mentoring, referral, and consultation support
until clinicians become comfortable in knowing when
to start, stop or change therapies. The mentorship
programme enhances the quality of both short-term
and long-term patient care and health outcomes.
Prior to the mentorship programme, complicated
cases were referred to other hospitals or sent to
larger towns. Dr Sentha Krishna, from Salem, says
that referrals to Tambaram have come down and the
patients reiterate it, “Tambaram care is available
here!” The programme has also raised the hospital’s
profile in the eyes of patients. Patients from other
districts have also started visiting these hospitals
because of accessibility and quality treatment.
Complicated cases are treated in the hospital either
through electronic or telephonic consultations or
the case is presented to the mentor on the day of
his visit.
Another significant clinical outcome of this programme
is the timely intervention in peripheral and symptomatic
conditions like kidney and liver malfunction, central
nervous system problems. Earlier these cases were
referred to other departments or hospitals causing
delays in the patients’ treatment, which in some cases
were fatal. For instance, a patient with Zidovudine
anemia in Salem hospital showed no improvement
even after eight bottles of blood transfusion. On
mentor’s suggestion, an erythropoietin injection was
administered and the patient, who had severe anemia

21HIV Clinical Mentorship - In a public health context
with heart failure, improved dramatically and his
hemoglobin, is now 12%.
3. Documentation
In many healthcare programmes implemented by the
government and NGOs, documentation processes and
quality are compromised due to a high patient load,
lack of documenting skills, and a single-minded focus
on care and treatment. Although doctors are fully
aware that documentation is a critical contributor
to assessment and follow-up in patient care, the
documents they produce are usually perfunctory and
sketchy. The mentorship programme is based on long
distance communication and quarterly visits, making
accurate and detailed case studies imperative in order
to determine the line of treatment and follow-up.
The programme’s well-defined documentation processes
are now being followed by all the staff. Reports,
detailed records, maintaining registers, death analysis,
2nd line ART documentation, and pediatric records
have improved and mentors have been extremely
encouraging in teaching new documentation skills.
In addition, the mentors have introduced the doctors
to some online learning models to expose them to
international formats and even shared a model of the
Stanford Guide from their curriculum.
Bridging Gaps in the Mentorship Programme
Though there has been a significant scaling up of HIV
care and treatment through the clinical mentorship
programme, there are still some gaps that need to be
addressed.
The mentors are well respected doctors and their
commitment to the programme has helped make it a
success. But the mentees did not have exposure to all
the mentors because there was no rotation, and some
of the doctors felt that they would have benefitted from
other mentors. Successful mentoring involves a dynamic
process and it is often wise to consider establishing
a discrete time period as a trial basis to determine
whether the mentoring relationship is working. This
22 HIV Clinical Mentorship - In a public health context
may help minimize any misunderstandings. It is
important to match the mentees expectations in order
to foster an effective mentoring relationship. There
were cases where a mentee would have preferred a
more senior mentor who better matched his own
considerable experience and knowledge.
The mentorship programme needs to focus beyond
clinical management of HIV. The spectrum of HIV
related care is much broader and the patient load in
some of these centers is very high (the doctors are
treating around 12,750–13,000 HIV/AIDS patients
at three sites, more than 4,300 of whom are on
ART, including 100 on 2nd line drugs). Counselling,
stigmatization, and behavioral changes are some of
the issues that need to be addressed.
The mentorship programme is too focused on clinical
care and management of HIV/AIDS. It should include
counselling, nutrition and home based care.
Some doctors felt that the mentors’ quarterly visits
were not enough, especially if they delayed/missed a
visit. A more flexible itinerary may be more effective.
Most doctors felt that it would be a good idea to
institutionalize the mentorship programme.
Mentorship outcomes and findings
Mentorship’s Positive Impact on Care as per Mentor’sOobservationslComprehensive medical assessment
lImproved safer sex education and family
counselling
lPrivacy during medical examination and
counselling
lDiagnosis and treatment of complex medical
conditions including crypotococcal meningitis,
TB meningitis, TB pleural effusion, AZT-induced
chronic diarrhoea and ascites among others
lTimely initiation of ART for TB co-infected
patients
lUse of correct dosages of ART for children
lDiagnosis and treatment of co-morbidities such
as diabetes, hypercholesterolemia, and liver
disease
lAccurate identification and treatment of failure
cases
lReferral to appropriate medical services which are
available onsite
lFrequent referencing to national guidelines and
protocols
lQuality of care documentation
lReduction of overcrowding at the clinics by
shifting certain tasks to nurse managers
lDiagnosis of various medical conditions through
use of medical equipment that was previously not
available onsite
In the course of a focus group discussion with
ART team other than doctors, to share and analyze
outcomes of the mentorship programme, points
discussed included:
l Paramedical staff (excluding the Project
Coordinator) knew about the mentor’s visits.
l There is not enough space and time to control the
high patient turn over. Given the opportunity, they
would like to spend more time on counselling.
l Improvement in infrastructure, like provision
of generators, would facilitate the free flow of
services, especially in the labs.
l To help practice universal precautions, coats,
shoes, and gloves have been provided and are
available.
feedback from Different Stakeholders:
The clinical mentorship programme has been received
favourably in all the centers and feedback reflects
this. Its reach has, in some cases, extended to
persons not directly participating in the programme.
For example, at one ART centre, staff who had not
interacted directly with the mentor was familiar with
his work in the hospital.
Direct feedback obtained from the different groups
reflects a generally favorable reaction to the
mentorship programme.
23HIV Clinical Mentorship - In a public health context 23
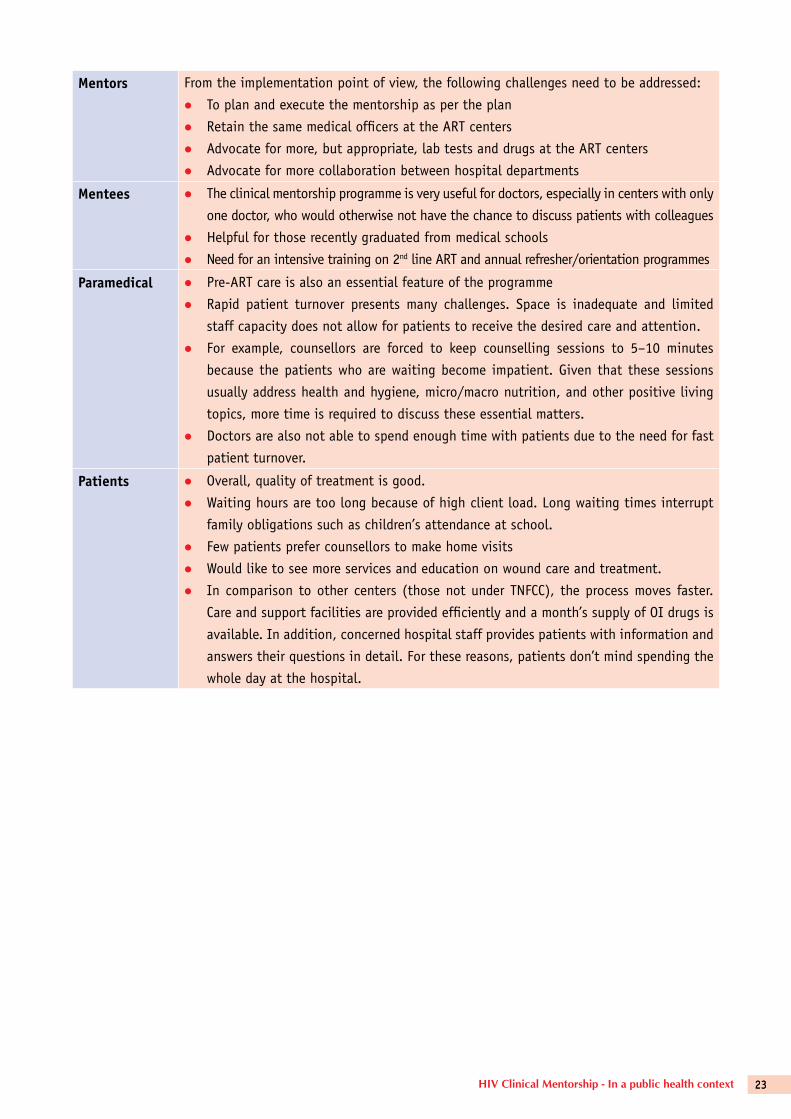
Mentors From the implementation point of view, the following challenges need to be addressed:
l To plan and execute the mentorship as per the plan
l Retain the same medical officers at the ART centers
l Advocate for more, but appropriate, lab tests and drugs at the ART centers
l Advocate for more collaboration between hospital departments
Mentees l The clinical mentorship programme is very useful for doctors, especially in centers with only
one doctor, who would otherwise not have the chance to discuss patients with colleagues
l Helpful for those recently graduated from medical schools
l Need for an intensive training on 2nd line ART and annual refresher/orientation programmes
Paramedical l Pre-ART care is also an essential feature of the programme
l Rapid patient turnover presents many challenges. Space is inadequate and limited
staff capacity does not allow for patients to receive the desired care and attention.
l For example, counsellors are forced to keep counselling sessions to 5–10 minutes
because the patients who are waiting become impatient. Given that these sessions
usually address health and hygiene, micro/macro nutrition, and other positive living
topics, more time is required to discuss these essential matters.
l Doctors are also not able to spend enough time with patients due to the need for fast
patient turnover.
Patients l Overall, quality of treatment is good.
l Waiting hours are too long because of high client load. Long waiting times interrupt
family obligations such as children’s attendance at school.
l Few patients prefer counsellors to make home visits
l Would like to see more services and education on wound care and treatment.
l In comparison to other centers (those not under TNFCC), the process moves faster.
Care and support facilities are provided efficiently and a month’s supply of OI drugs is
available. In addition, concerned hospital staff provides patients with information and
answers their questions in detail. For these reasons, patients don’t mind spending the
whole day at the hospital.
24 HIV Clinical Mentorship - In a public health context
reference:
To equip the mentors with mentoring skills the three-
day training focuses on:
relationship Building
A trusting, two-way relationship between the mentor
and mentee is the foundation of effective mentoring
practice. This section includes suggestions on how
to initiate and build a strong relationship of mutual
respect between the mentor and the mentee, and how
to provide constructive feedback and encouragement
within the mentoring relationship.
Strategies for Mentoring
Mentors work in a variety of settings in which they
face a wide range of constraints and challenges.
Developing strategies and approaches to effectively
carry out mentoring activities within different settings
presents a unique set of challenges. The documents
in this section provide mentors with suggestions and
ideas on various approaches to mentoring, including
how to conduct bedside teaching, conduct site visits,
mentoring in the face of heavy patient loads, and
strategies for addressing a wide range of systems
issues.
Monitoring and Evaluation Tools
This section includes tools and resources for a
mentor to use to assess the skills of providers and
to assess facility issues. Observation checklists
in this section help the mentor to track providers’
I-TECH Clinical Mentors’ Training CurriculumAnnexure - I
improvement in their delivery of clinical care over
time. Facility checklists enable monitoring of systems
improvements at a site. The tools included have been
developed by I-TECH projects around the world, and
can be adapted to fit a mentor’s particular situation
and area of focus.
Training Health Care Workers
The ultimate goal of a clinical mentoring programme is
to build the skills of local clinicians. Clinical mentors
may provide one-on-one mentoring to a health care
provider during a patient consultation, conduct stand-
alone sessions for clinical staff on various clinical
topics, lead discussions highlighting the management
of complex cases, and accompany staff on rounds.
This section includes resources for mentors on how to
use case studies and clinical vignettes to guide the
training of health care workers.
I-TECH Curricula
This section contains I-TECH training curricula on a
variety of topics related to HIV and AIDS that can
be used by a clinical mentor to conduct more formal,
classroom-based training of health care workers.
Each curriculum includes sets of PowerPoint slides,
facilitator guides, and participant handbooks. Clinical
mentors are free to adapt and change these materials
as needed. This section includes twelve complete
curricula (multiday trainings with several slide sets)
and four workshops (shorter sessions appropriate for
an hour or two of training on a focused topic). All of
the curricula included here have been pilot tested by
I-TECH country programmes.
25HIV Clinical Mentorship - In a public health context
Tool for mentoship assessmentAnnexure - II
Clinical Mentorship - Assessment Questionnaire
Date: ______________________________________________
Site: _______________________________________________
Site Reviewer: ________________________________________
I. STAFFING
What types and numbers of providers do you have at this clinic?
Number Number
Physician ______ Nurse case manager ______ Lab technician ______ Nurse aid/assistant ______ Pharmacist ______ Nutritionist ______
Councelor ______ Project coordinator ______ Data entry operator ______ Sanitary worker ______ Pharmacist ______ Other (specify) ______
1. How would you describe your overall staffing level?
Very well staffed Adequately staffed Understaffed
2. How much staff turnover do you experience? High turnover Moderate turnover Low turnover
Where among your staff is the greatest turnover? Comments:
26 HIV Clinical Mentorship - In a public health context
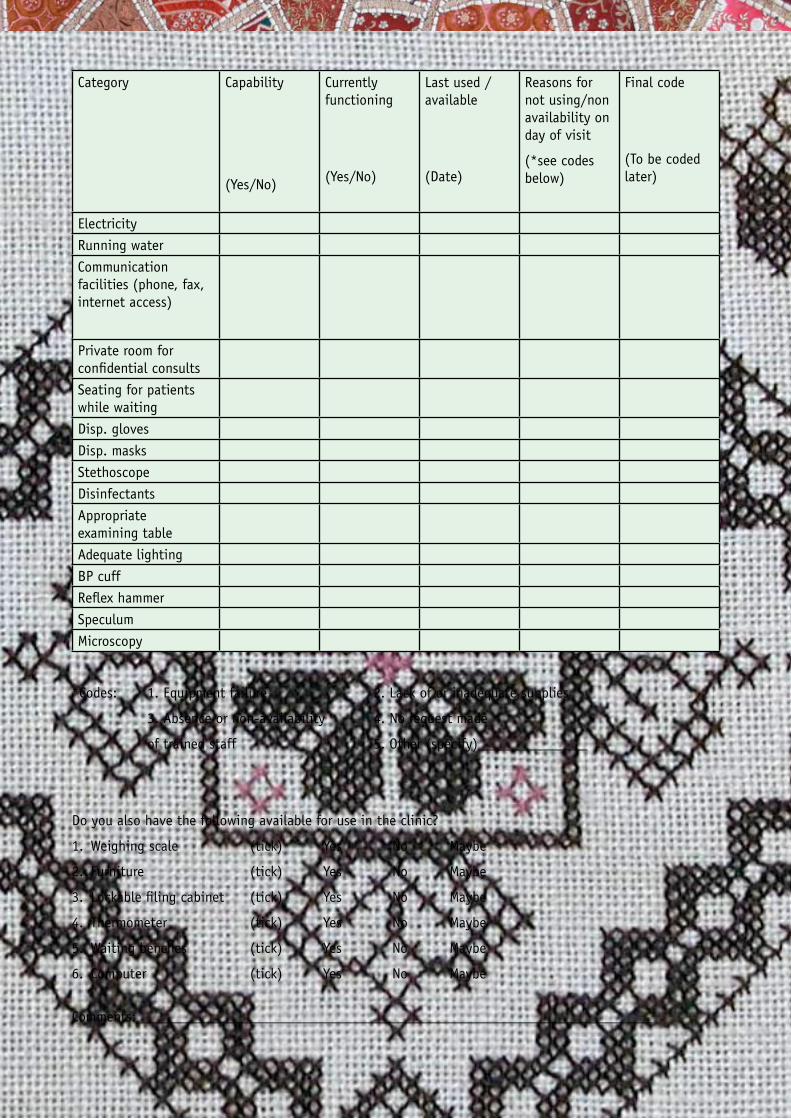
II. SPACE AND EQUIPMENT
How many consulting or counseling rooms are present in the centre? _____
Facilities and supplies (Tick all that apply)
1. Injection material:
1.1 Multiple use needles provided
1.2 Single use disposable needles
provided
If YES
1.2.1 Needles recapped before disposal
1.2.2 Needles recapped one handed
1.2.3 Needles deposited directly
1.2.4 Needle cutter used
1.2.5 Sharps containers available
2. Methods for disinfecting reusable
medical equipment:
2.1 Autoclave
2.2 Steam sterilization
2.3 Boiling and chemicals
2.4 Chemicals only
2.5 Boiling only
2.6 Other ____________________
2.7 Use disposables only
3. Disposal of contaminated items:
3.1 Burned in incinerator
3.2 Burned in open pit
3.3 Burned and buried
3.4 Thrown in trash/open pit
3.5 Thrown in pit latrines
3.6 Removed off site
3.7 Other ______________________________
4. Record keeping:
4.1 Record HIV-related illnesses in register
4.2 Patient medical records kept by patient
4.3 Paper patient medical records kept on-site
4.4 Electronic medical records
5. Availability of written material/posters on HIV/AIDS/STDs to educate patients:
Yes
No
6. Material/internet access for doctors on:
6.1 NACO ART adult guidelines
6.2 Paediatric guidelines
6.3 OI guidelines
6.4 PEP
6.5 PPTCT guidelines
6.6 Second line drugs
6.7 Others
27HIV Clinical Mentorship - In a public health context
Category Capability
(Yes/No)
Currently functioning
(Yes/No)
Last used / available
(Date)
Reasons for not using/non availability on day of visit
(*see codes below)
Final code
(To be coded later)
Electricity
Running water
Communication facilities (phone, fax, internet access)
Private room for confidential consults
Seating for patients while waiting
Disp. gloves
Disp. masks
Stethoscope
Disinfectants
Appropriate examining table
Adequate lighting
BP cuff
Reflex hammer
Speculum
Microscopy
*Codes: 1. Equipment failure 2. Lack of or inadequate supplies
3. Absence or non-availability 4. No request made
of trained staff 5. Other (specify)_______________
Do you also have the following available for use in the clinic?
1. Weighing scale (tick) Yes No Maybe
2. Furniture (tick) Yes No Maybe
3. Lockable filing cabinet (tick) Yes No Maybe
4. Thermometer (tick) Yes No Maybe
5. Waiting benches (tick) Yes No Maybe
6. Computer (tick) Yes No Maybe
Comments: ______________________________________________________________________
28 HIV Clinical Mentorship - In a public health context
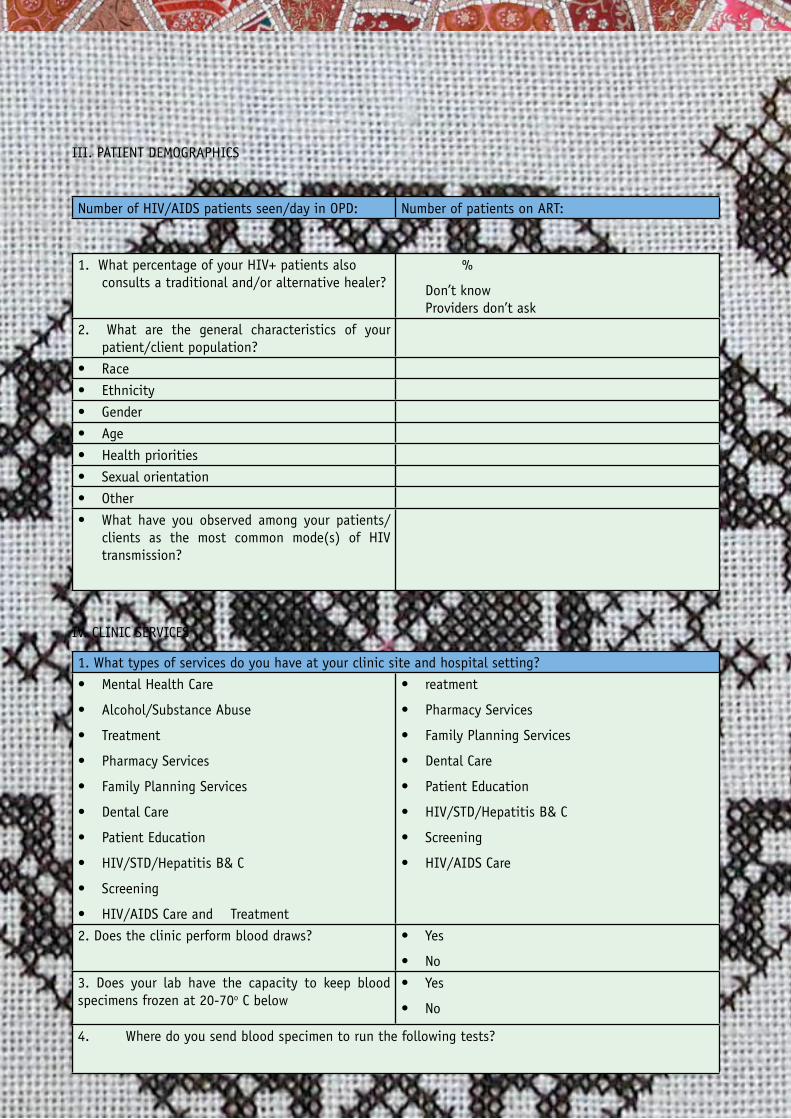
III. PATIENT DEMOGRAPHICS
Number of HIV/AIDS patients seen/day in OPD: Number of patients on ART:
1. What percentage of your HIV+ patients also consults a traditional and/or alternative healer?
%
Don’t know Providers don’t ask
2. What are the general characteristics of your patient/client population?
Race•
Ethnicity•
Gender•
Age•
Health priorities•
Sexual orientation•
Other•
What have you observed among your patients/•clients as the most common mode(s) of HIV transmission?
IV. CLINIC SERVICES
1. What types of services do you have at your clinic site and hospital setting?
Mental Health Care•
Alcohol/Substance Abuse •
Treatment•
Pharmacy Services•
Family Planning Services•
Dental Care•
Patient Education•
HIV/STD/Hepatitis B& C•
Screening •
HIV/AIDS Care and Treatment•
reatment•
Pharmacy Services•
Family Planning Services•
Dental Care•
Patient Education•
HIV/STD/Hepatitis B& C•
Screening •
HIV/AIDS Care •
2. Does the clinic perform blood draws? Yes•
No•
3. Does your lab have the capacity to keep blood specimens frozen at 20-70o C below
Yes•
No•
4. Where do you send blood specimen to run the following tests?
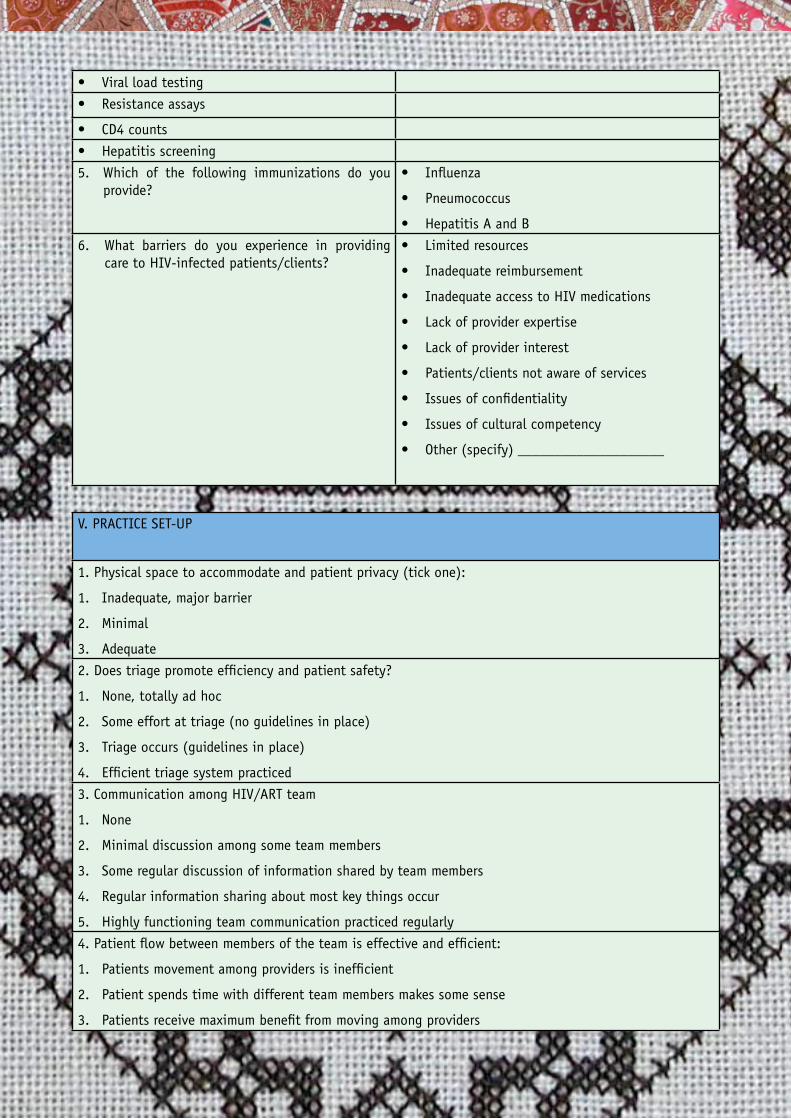
29HIV Clinical Mentorship - In a public health context
Viral load testing•
Resistance assays•
CD4 counts•
Hepatitis screening•
5. Which of the following immunizations do you provide?
Influenza•
Pneumococcus•
Hepatitis A and B•
6. What barriers do you experience in providing care to HIV-infected patients/clients?
Limited resources•
Inadequate reimbursement•
Inadequate access to HIV medications •
Lack of provider expertise•
Lack of provider interest•
Patients/clients not aware of services•
Issues of confidentiality•
Issues of cultural competency•
Other (specify) ____________________•
V. PRACTICE SET-UP
1. Physical space to accommodate and patient privacy (tick one):
Inadequate, major barrier1.
Minimal2.
Adequate3.
2. Does triage promote efficiency and patient safety?
None, totally ad hoc 1.
Some effort at triage (no guidelines in place) 2.
Triage occurs (guidelines in place) 3.
Efficient triage system practiced 4.
3. Communication among HIV/ART team
None1.
Minimal discussion among some team members2.
Some regular discussion of information shared by team members3.
Regular information sharing about most key things occur4.
Highly functioning team communication practiced regularly5.
4. Patient flow between members of the team is effective and efficient:
Patients movement among providers is inefficient1.
Patient spends time with different team members makes some sense2.
Patients receive maximum benefit from moving among providers3.
30 HIV Clinical Mentorship - In a public health context
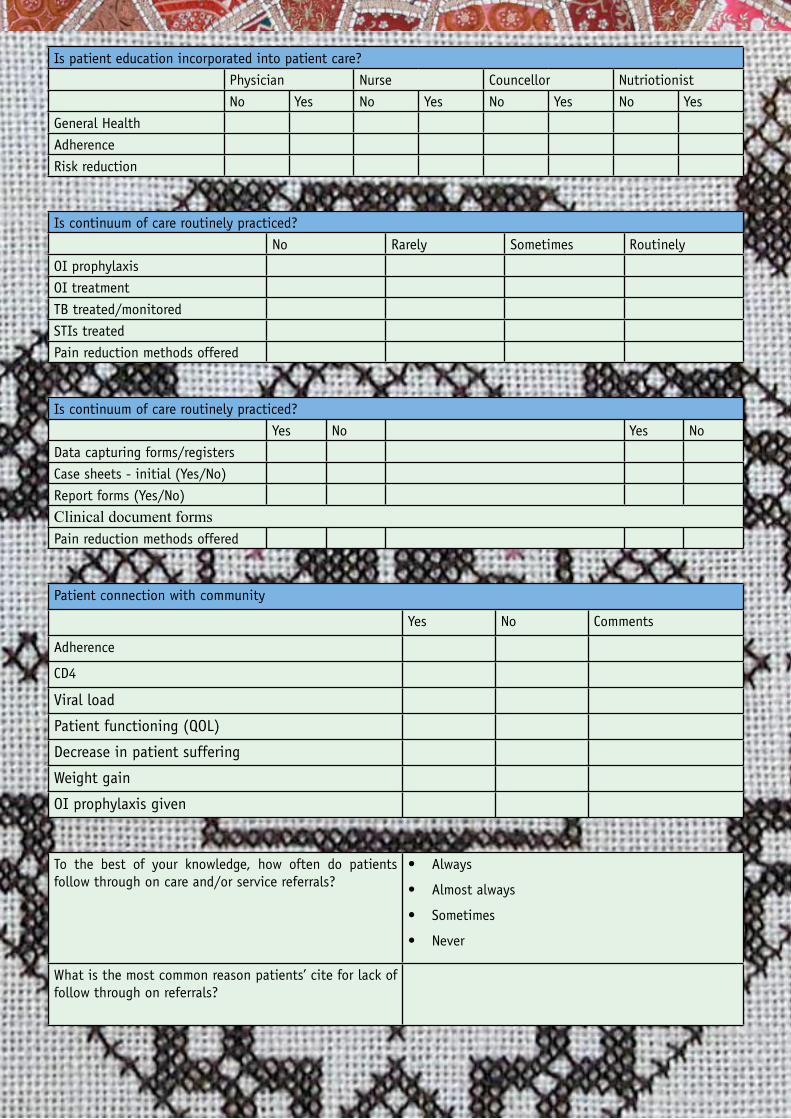
Is patient education incorporated into patient care?
Physician Nurse Councellor Nutriotionist
No Yes No Yes No Yes No Yes
General Health
Adherence
Risk reduction
Is continuum of care routinely practiced?
No Rarely Sometimes Routinely
OI prophylaxis
OI treatment
TB treated/monitored
STIs treated
Pain reduction methods offered
Is continuum of care routinely practiced?
Yes No Yes No
Data capturing forms/registers
Case sheets - initial (Yes/No)
Report forms (Yes/No)
Clinical document formsPain reduction methods offered
Patient connection with community
Yes No Comments
Adherence
CD4
Viral load
Patient functioning (QOL)
Decrease in patient suffering
Weight gain
OI prophylaxis given
To the best of your knowledge, how often do patients follow through on care and/or service referrals?
Always •
Almost always•
Sometimes•
Never•
What is the most common reason patients’ cite for lack of follow through on referrals?
31HIV Clinical Mentorship - In a public health context
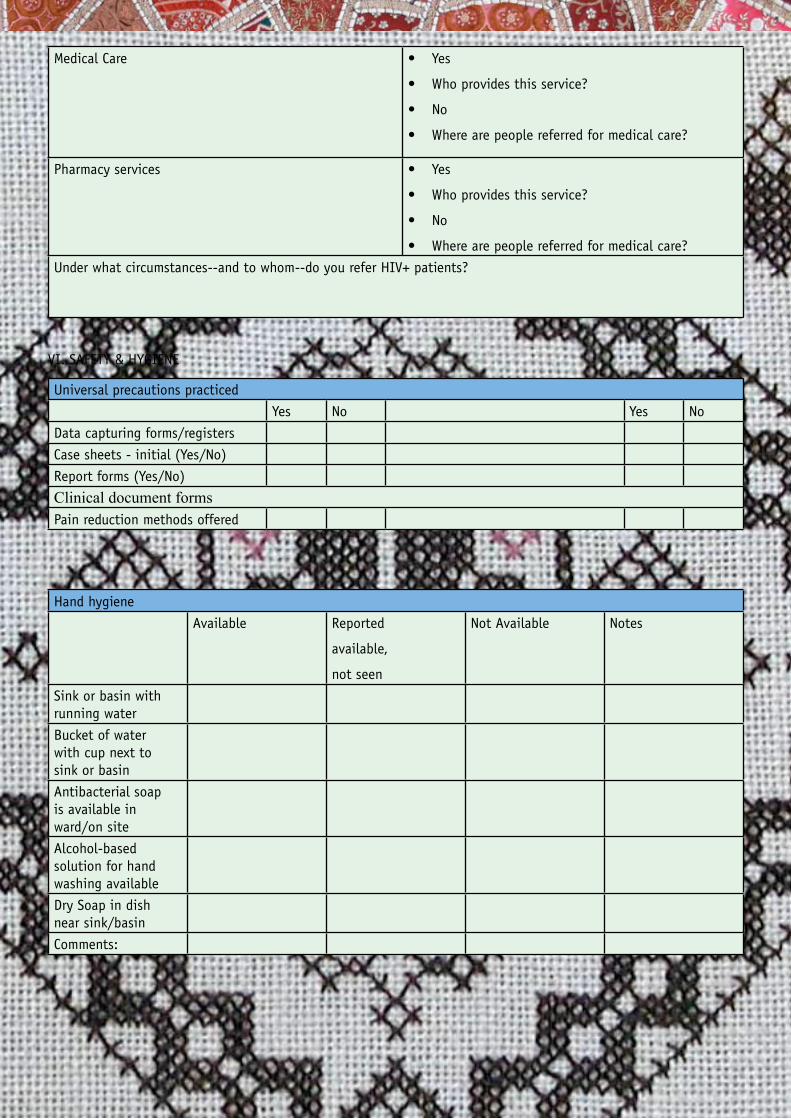
Medical Care Yes•
Who provides this service?•
No•
Where are people referred for medical care?•
Pharmacy services Yes•
Who provides this service?•
No•
Where are people referred for medical care?•
Under what circumstances--and to whom--do you refer HIV+ patients?
VI. SAFETY & HYGIENE
Universal precautions practiced
Yes No Yes No
Data capturing forms/registers
Case sheets - initial (Yes/No)
Report forms (Yes/No)
Clinical document formsPain reduction methods offered
Hand hygiene
Available Reported
available,
not seen
Not Available Notes
Sink or basin with running water
Bucket of water with cup next to sink or basin
Antibacterial soap is available in ward/on site
Alcohol-based solution for hand washing available
Dry Soap in dish near sink/basin
Comments:
32 HIV Clinical Mentorship - In a public health context
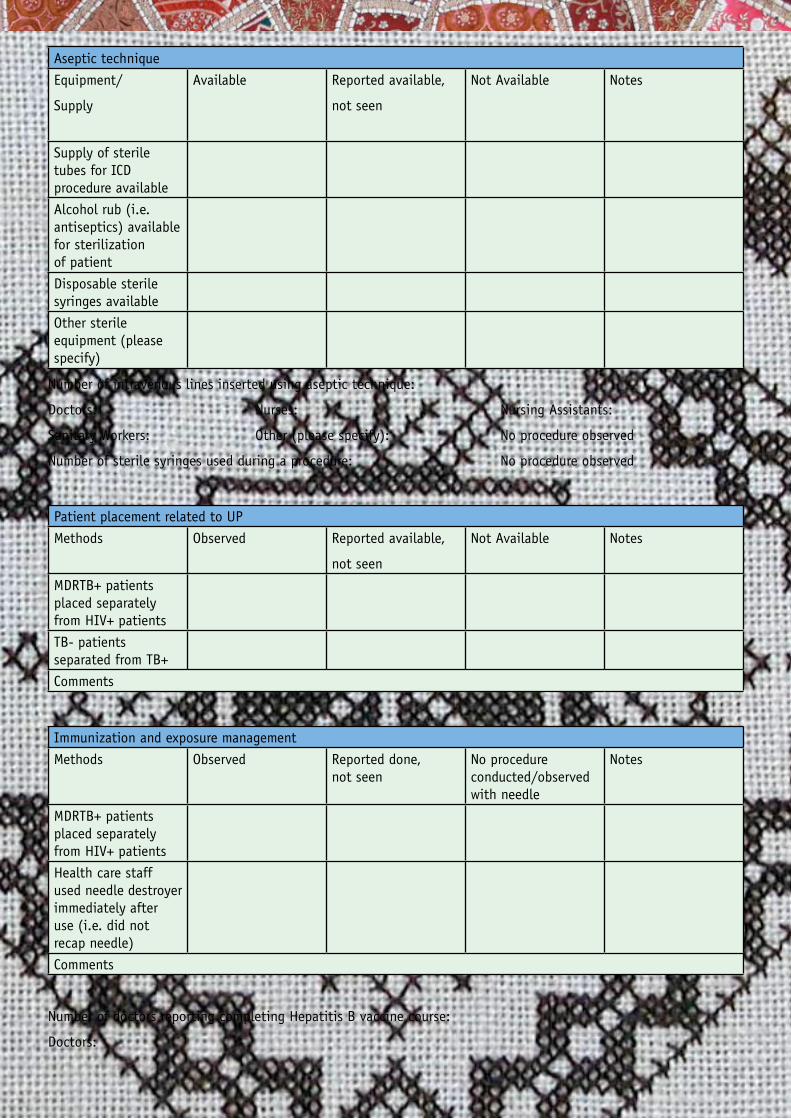
Aseptic technique
Equipment/
Supply
Available Reported available,
not seen
Not Available Notes
Supply of sterile tubes for ICD procedure available
Alcohol rub (i.e. antiseptics) available for sterilization of patient
Disposable sterile syringes available
Other sterile equipment (please specify)
Number of intravenous lines inserted using aseptic technique:
Doctors: Nurses: Nursing Assistants:
Sanitary Workers: Other (please specify): No procedure observed
Number of sterile syringes used during a procedure: No procedure observed
Patient placement related to UP
Methods Observed Reported available,
not seen
Not Available Notes
MDRTB+ patients placed separately from HIV+ patients
TB- patients separated from TB+
Comments
Immunization and exposure management
Methods Observed Reported done, not seen
No procedure conducted/observed with needle
Notes
MDRTB+ patients placed separately from HIV+ patients
Health care staff used needle destroyer immediately after use (i.e. did not recap needle)
Comments
Number of doctors reporting completing Hepatitis B vaccine course:
Doctors:
33HIV Clinical Mentorship - In a public health context
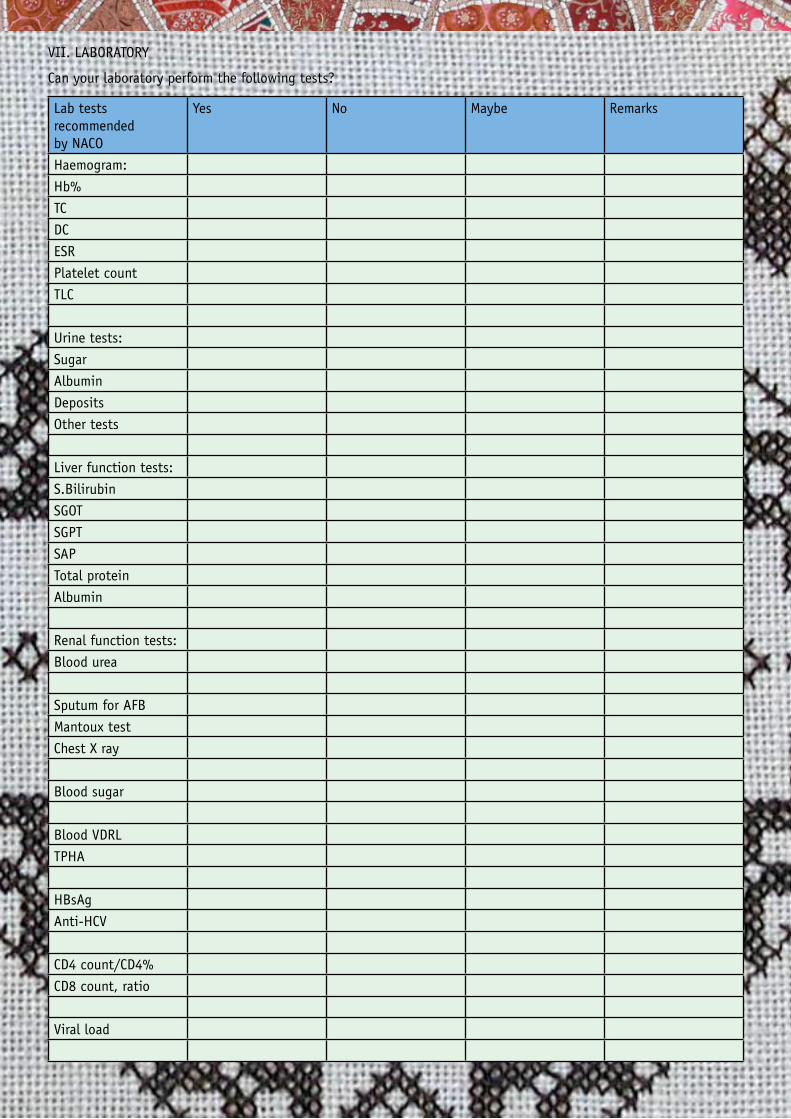
VII. LABORATORY
Can your laboratory perform the following tests?
Lab tests recommended by NACO
Yes No Maybe Remarks
Haemogram:
Hb%
TC
DC
ESR
Platelet count
TLC
Urine tests:
Sugar
Albumin
Deposits
Other tests
Liver function tests:
S.Bilirubin
SGOT
SGPT
SAP
Total protein
Albumin
Renal function tests:
Blood urea
Sputum for AFB
Mantoux test
Chest X ray
Blood sugar
Blood VDRL
TPHA
HBsAg
Anti-HCV
CD4 count/CD4%
CD8 count, ratio
Viral load
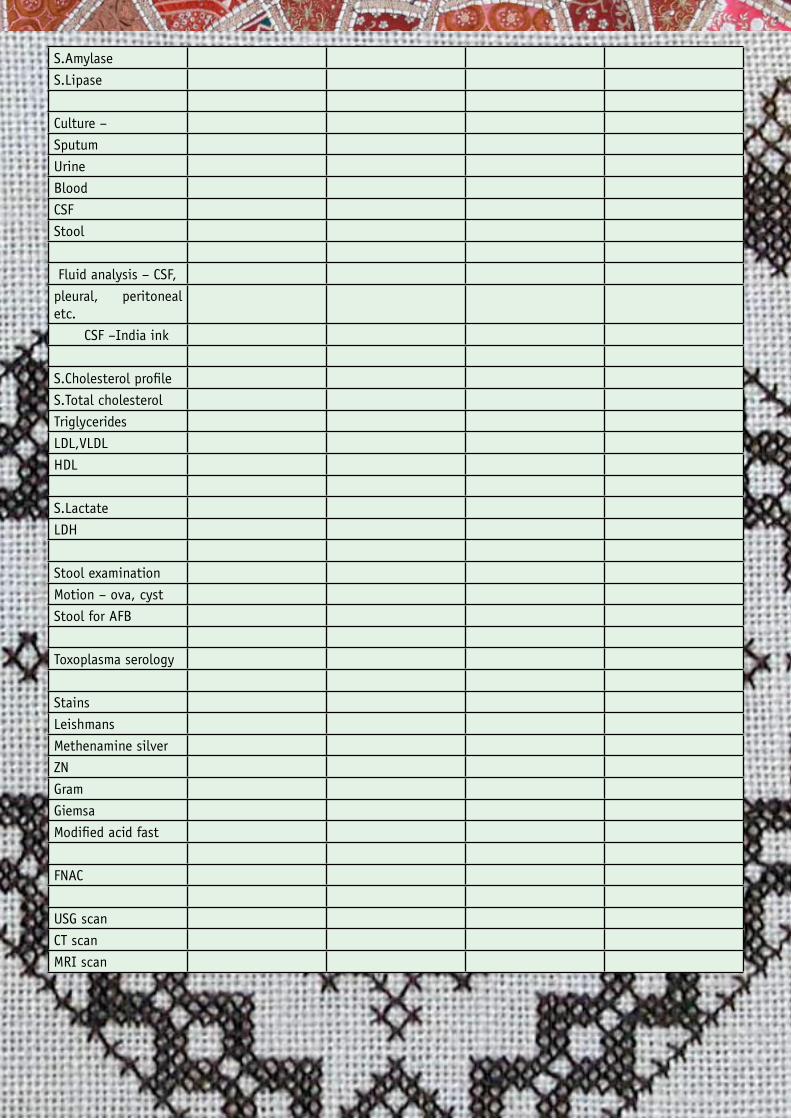
34 HIV Clinical Mentorship - In a public health context
S.Amylase
S.Lipase
Culture –
Sputum
Urine
Blood
CSF
Stool
Fluid analysis – CSF,
pleural, peritoneal etc.
CSF –India ink
S.Cholesterol profile
S.Total cholesterol
Triglycerides
LDL,VLDL
HDL
S.Lactate
LDH
Stool examination
Motion – ova, cyst
Stool for AFB
Toxoplasma serology
Stains
Leishmans
Methenamine silver
ZN
Gram
Giemsa
Modified acid fast
FNAC
USG scan
CT scan
MRI scan
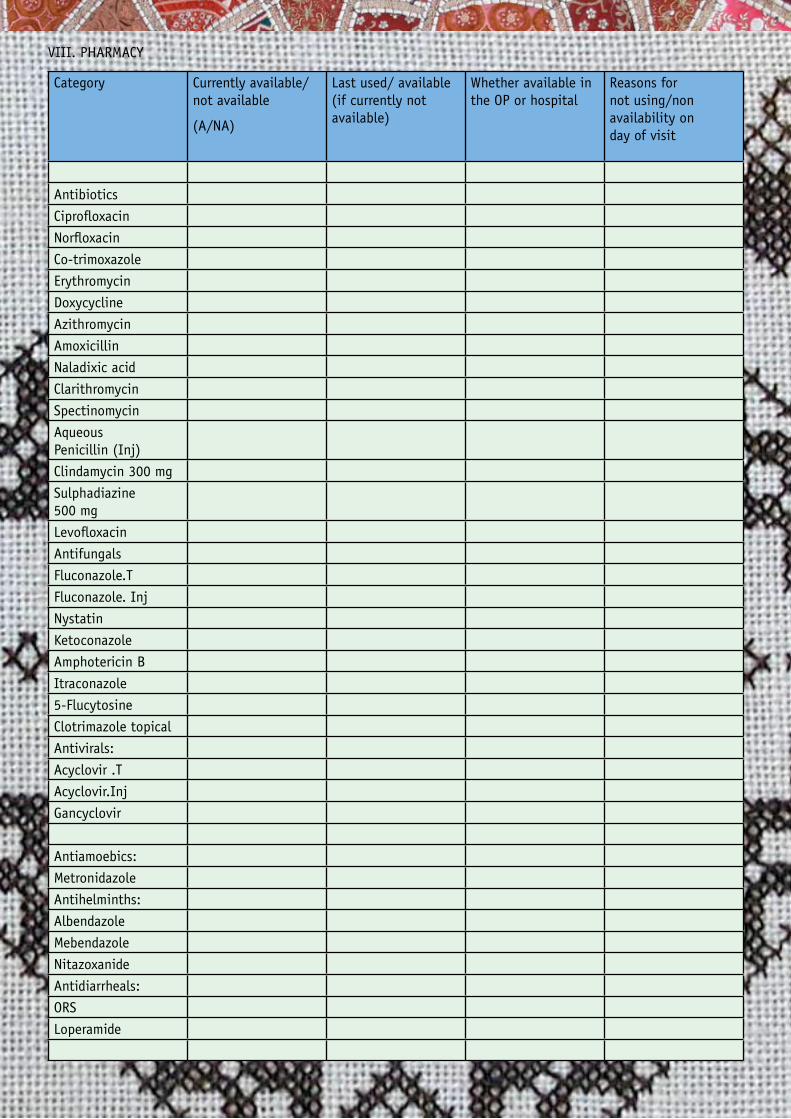
35HIV Clinical Mentorship - In a public health context
VIII. PHARMACY
Category Currently available/not available
(A/NA)
Last used/ available (if currently not available)
Whether available in the OP or hospital
Reasons for not using/non availability on day of visit
Antibiotics
Ciprofloxacin
Norfloxacin
Co-trimoxazole
Erythromycin
Doxycycline
Azithromycin
Amoxicillin
Naladixic acid
Clarithromycin
Spectinomycin
Aqueous Penicillin (Inj)
Clindamycin 300 mg
Sulphadiazine 500 mg
Levofloxacin
Antifungals
Fluconazole.T
Fluconazole. Inj
Nystatin
Ketoconazole
Amphotericin B
Itraconazole
5-Flucytosine
Clotrimazole topical
Antivirals:
Acyclovir .T
Acyclovir.Inj
Gancyclovir
Antiamoebics:
Metronidazole
Antihelminths:
Albendazole
Mebendazole
Nitazoxanide
Antidiarrheals:
ORS
Loperamide
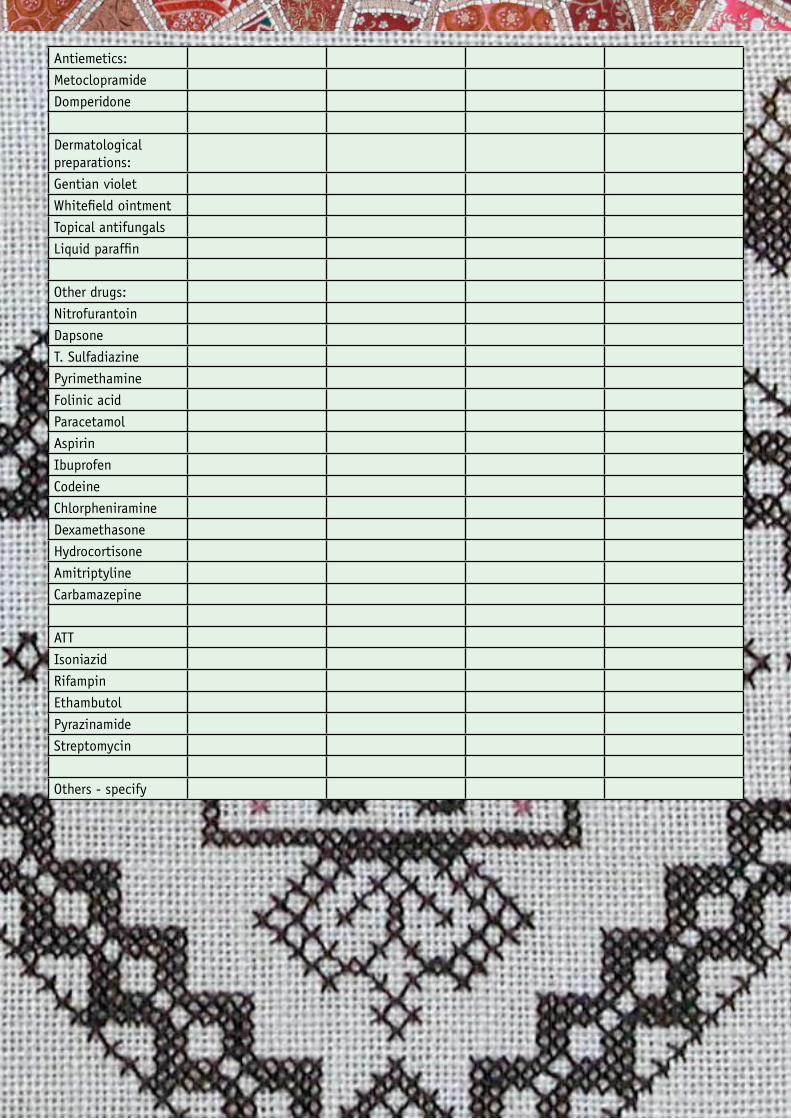
36 HIV Clinical Mentorship - In a public health context
Antiemetics:
Metoclopramide
Domperidone
Dermatological preparations:
Gentian violet
Whitefield ointment
Topical antifungals
Liquid paraffin
Other drugs:
Nitrofurantoin
Dapsone
T. Sulfadiazine
Pyrimethamine
Folinic acid
Paracetamol
Aspirin
Ibuprofen
Codeine
Chlorpheniramine
Dexamethasone
Hydrocortisone
Amitriptyline
Carbamazepine
ATT
Isoniazid
Rifampin
Ethambutol
Pyrazinamide
Streptomycin
Others - specify
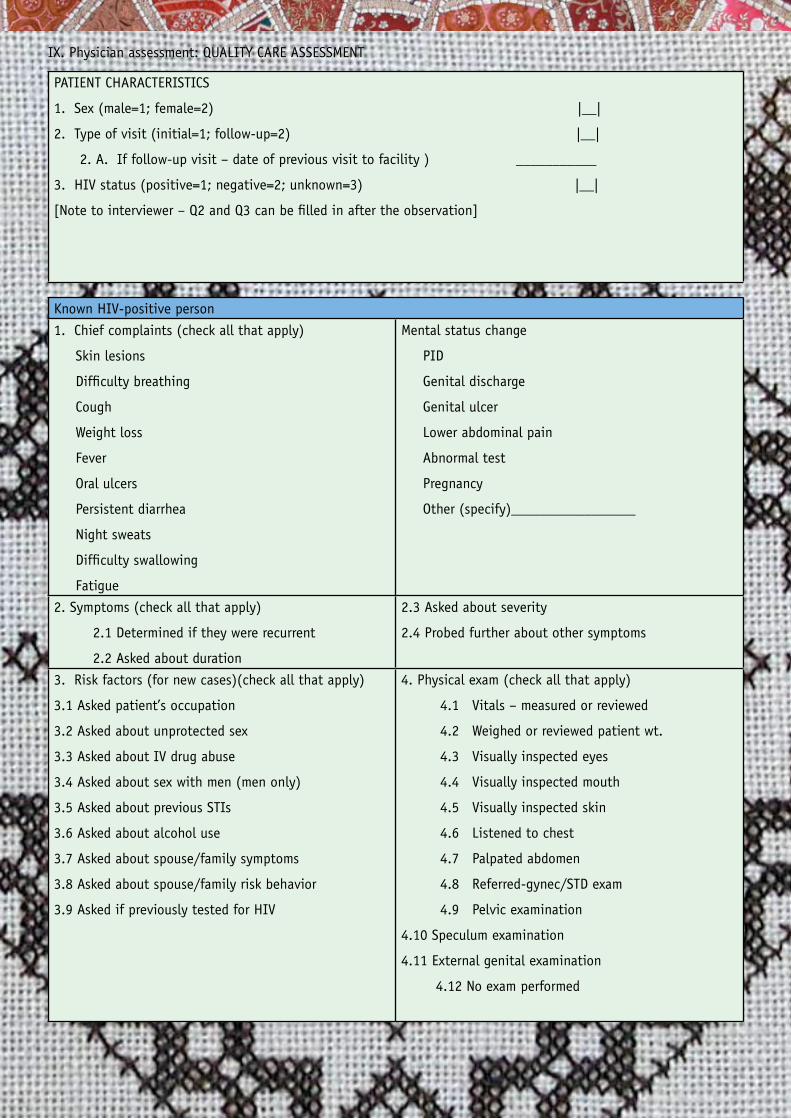
37HIV Clinical Mentorship - In a public health context
IX. Physician assessment: QUALITY CARE ASSESSMENT
PATIENT CHARACTERISTICS
1. Sex (male=1; female=2) |__|
2. Type of visit (initial=1; follow-up=2) |__|
2. A. If follow-up visit – date of previous visit to facility ) ___________
3. HIV status (positive=1; negative=2; unknown=3) |__|
[Note to interviewer – Q2 and Q3 can be filled in after the observation]
Known HIV-positive person
1. Chief complaints (check all that apply)
Skin lesions
Difficulty breathing
Cough
Weight loss
Fever
Oral ulcers
Persistent diarrhea
Night sweats
Difficulty swallowing
Fatigue
Mental status change
PID
Genital discharge
Genital ulcer
Lower abdominal pain
Abnormal test
Pregnancy
Other (specify)_________________
2. Symptoms (check all that apply)
2.1 Determined if they were recurrent
2.2 Asked about duration
2.3 Asked about severity
2.4 Probed further about other symptoms
3. Risk factors (for new cases)(check all that apply)
3.1 Asked patient’s occupation
3.2 Asked about unprotected sex
3.3 Asked about IV drug abuse
3.4 Asked about sex with men (men only)
3.5 Asked about previous STIs
3.6 Asked about alcohol use
3.7 Asked about spouse/family symptoms
3.8 Asked about spouse/family risk behavior
3.9 Asked if previously tested for HIV
4. Physical exam (check all that apply)
4.1 Vitals – measured or reviewed
4.2 Weighed or reviewed patient wt.
4.3 Visually inspected eyes
4.4 Visually inspected mouth
4.5 Visually inspected skin
4.6 Listened to chest
4.7 Palpated abdomen
4.8 Referred-gynec/STD exam
4.9 Pelvic examination
4.10 Speculum examination
4.11 External genital examination
4.12 No exam performed
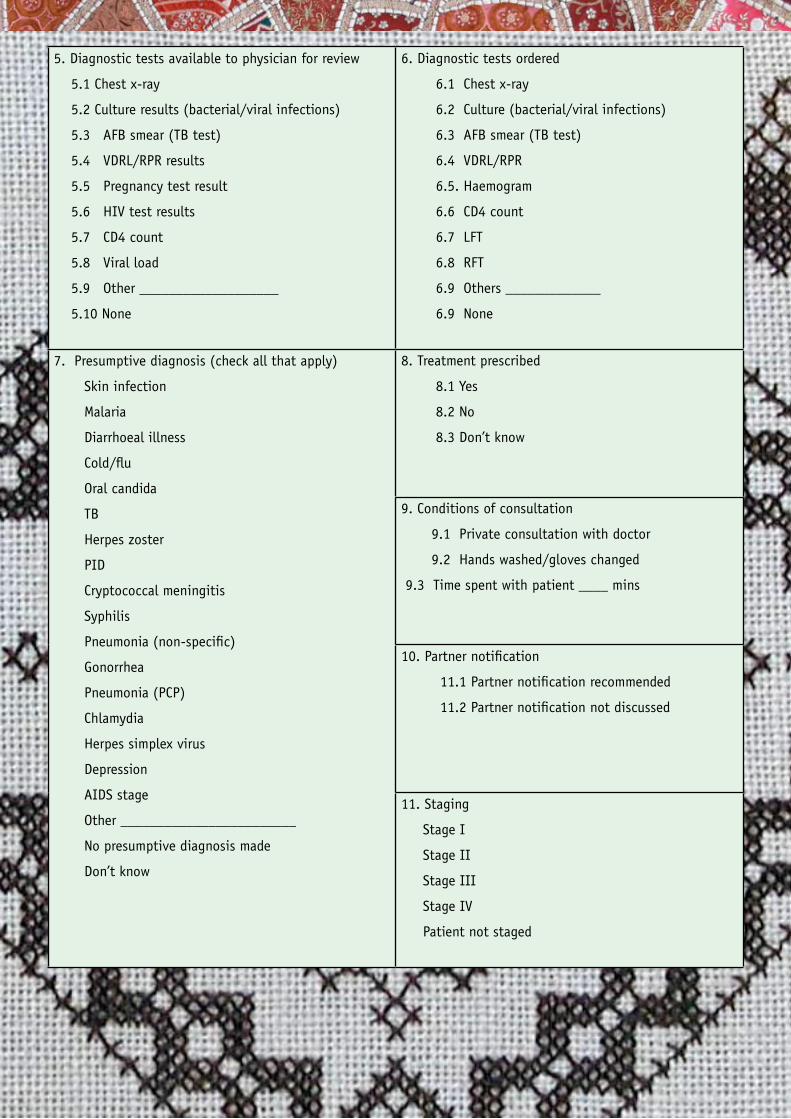
38 HIV Clinical Mentorship - In a public health context
5. Diagnostic tests available to physician for review
5.1 Chest x-ray
5.2 Culture results (bacterial/viral infections)
5.3 AFB smear (TB test)
5.4 VDRL/RPR results
5.5 Pregnancy test result
5.6 HIV test results
5.7 CD4 count
5.8 Viral load
5.9 Other ___________________
5.10 None
6. Diagnostic tests ordered
6.1 Chest x-ray
6.2 Culture (bacterial/viral infections)
6.3 AFB smear (TB test)
6.4 VDRL/RPR
6.5. Haemogram
6.6 CD4 count
6.7 LFT
6.8 RFT
6.9 Others _____________
6.9 None
7. Presumptive diagnosis (check all that apply)
Skin infection
Malaria
Diarrhoeal illness
Cold/flu
Oral candida
TB
Herpes zoster
PID
Cryptococcal meningitis
Syphilis
Pneumonia (non-specific)
Gonorrhea
Pneumonia (PCP)
Chlamydia
Herpes simplex virus
Depression
AIDS stage
Other ________________________
No presumptive diagnosis made
Don’t know
8. Treatment prescribed
8.1 Yes
8.2 No
8.3 Don’t know
9. Conditions of consultation
9.1 Private consultation with doctor
9.2 Hands washed/gloves changed
9.3 Time spent with patient ____ mins
10. Partner notification
11.1 Partner notification recommended
11.2 Partner notification not discussed
11. Staging
Stage I
Stage II
Stage III
Stage IV
Patient not staged
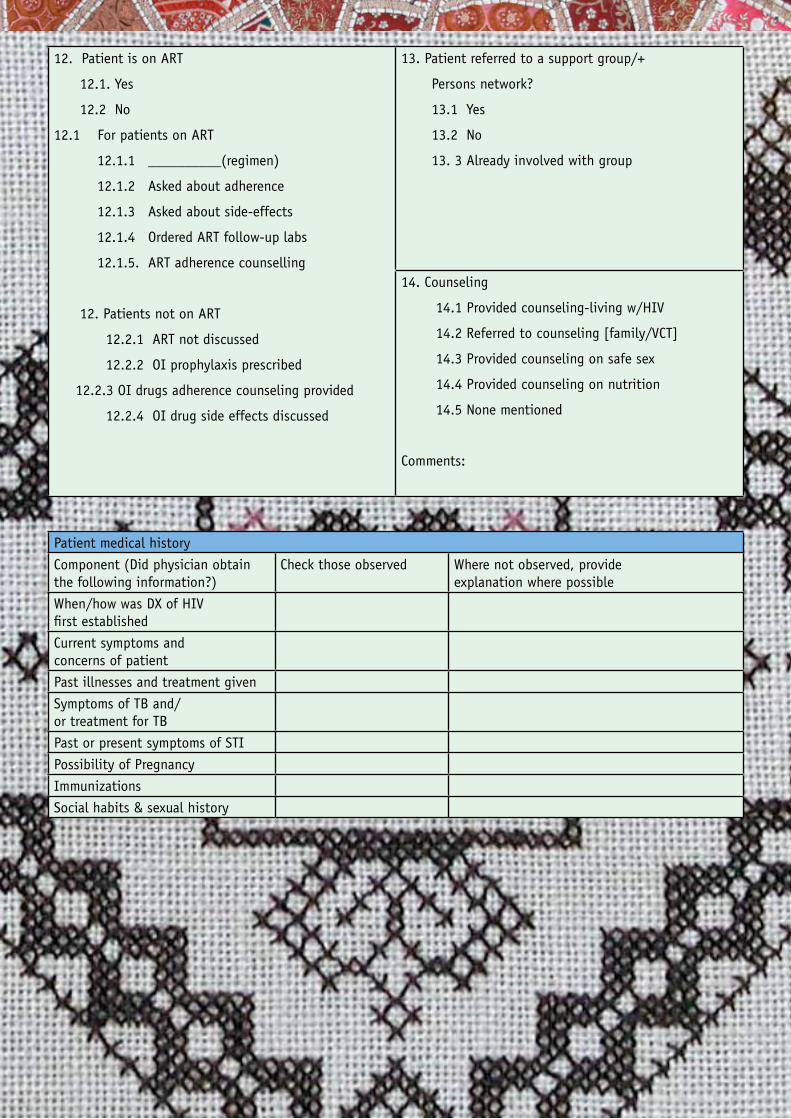
39HIV Clinical Mentorship - In a public health context
12. Patient is on ART
12.1. Yes
12.2 No
12.1 For patients on ART
12.1.1 __________(regimen)
12.1.2 Asked about adherence
12.1.3 Asked about side-effects
12.1.4 Ordered ART follow-up labs
12.1.5. ART adherence counselling
12. Patients not on ART
12.2.1 ART not discussed
12.2.2 OI prophylaxis prescribed
12.2.3 OI drugs adherence counseling provided
12.2.4 OI drug side effects discussed
13. Patient referred to a support group/+
Persons network?
13.1 Yes
13.2 No
13. 3 Already involved with group
14. Counseling
14.1 Provided counseling-living w/HIV
14.2 Referred to counseling [family/VCT]
14.3 Provided counseling on safe sex
14.4 Provided counseling on nutrition
14.5 None mentioned
Comments:
Patient medical history
Component (Did physician obtain the following information?)
Check those observed Where not observed, provide explanation where possible
When/how was DX of HIV first established
Current symptoms and concerns of patient
Past illnesses and treatment given
Symptoms of TB and/or treatment for TB
Past or present symptoms of STI
Possibility of Pregnancy
Immunizations
Social habits & sexual history
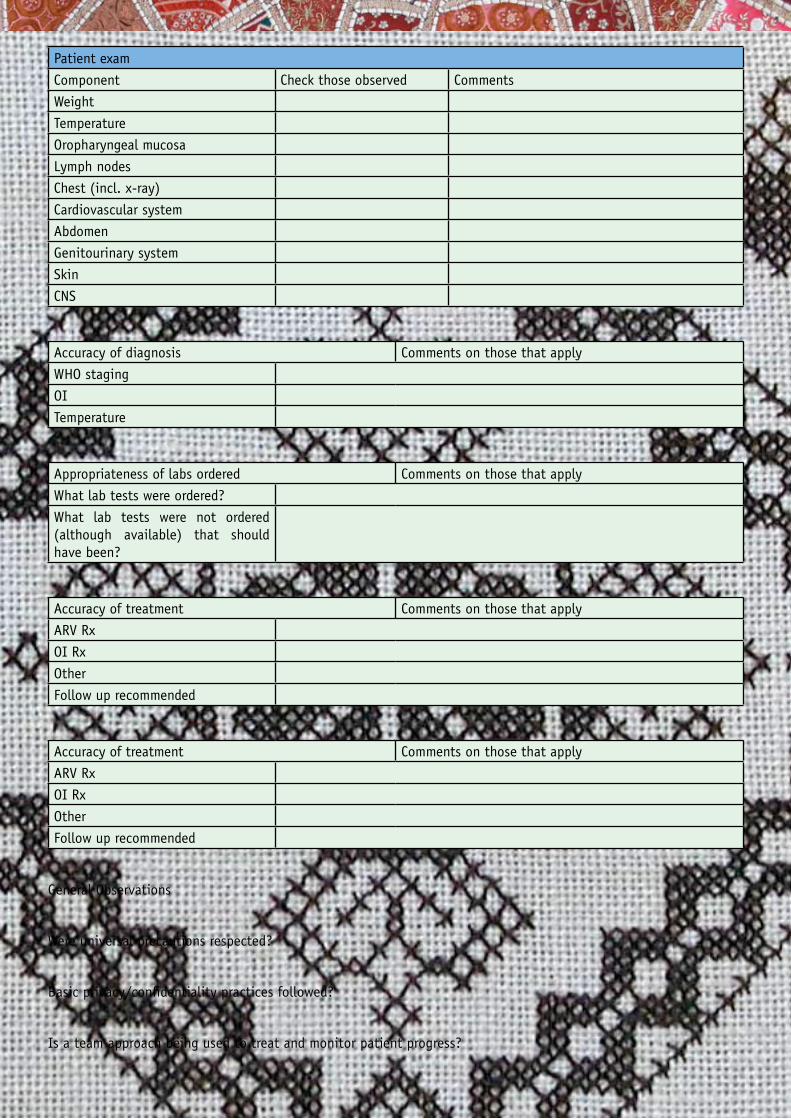
40 HIV Clinical Mentorship - In a public health context
Patient exam
Component Check those observed Comments
Weight
Temperature
Oropharyngeal mucosa
Lymph nodes
Chest (incl. x-ray)
Cardiovascular system
Abdomen
Genitourinary system
Skin
CNS
Accuracy of diagnosis Comments on those that apply
WHO staging
OI
Temperature
Appropriateness of labs ordered Comments on those that apply
What lab tests were ordered?
What lab tests were not ordered (although available) that should have been?
Accuracy of treatment Comments on those that apply
ARV Rx
OI Rx
Other
Follow up recommended
Accuracy of treatment Comments on those that apply
ARV Rx
OI Rx
Other
Follow up recommended
General Observations
Were universal precautions respected?
Basic privacy/confidentiality practices followed?
Is a team approach being used to treat and monitor patient progress?
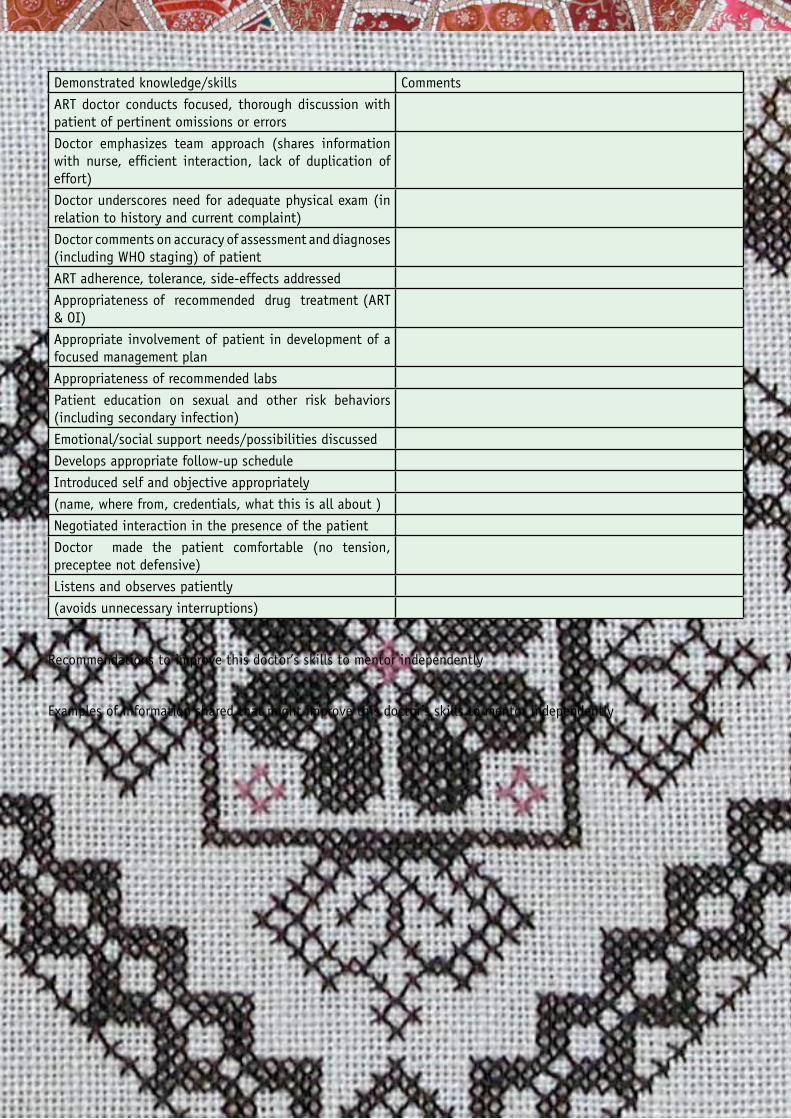
41HIV Clinical Mentorship - In a public health context
Demonstrated knowledge/skills Comments
ART doctor conducts focused, thorough discussion with patient of pertinent omissions or errors
Doctor emphasizes team approach (shares information with nurse, efficient interaction, lack of duplication of effort)
Doctor underscores need for adequate physical exam (in relation to history and current complaint)
Doctor comments on accuracy of assessment and diagnoses (including WHO staging) of patient
ART adherence, tolerance, side-effects addressed
Appropriateness of recommended drug treatment (ART & OI)
Appropriate involvement of patient in development of a focused management plan
Appropriateness of recommended labs
Patient education on sexual and other risk behaviors (including secondary infection)
Emotional/social support needs/possibilities discussed
Develops appropriate follow-up schedule
Introduced self and objective appropriately
(name, where from, credentials, what this is all about )
Negotiated interaction in the presence of the patient
Doctor made the patient comfortable (no tension, preceptee not defensive)
Listens and observes patiently
(avoids unnecessary interruptions)
Recommendations to improve this doctor’s skills to mentor independently
Examples of information shared that might improve this doctor’s skills to mentor independently
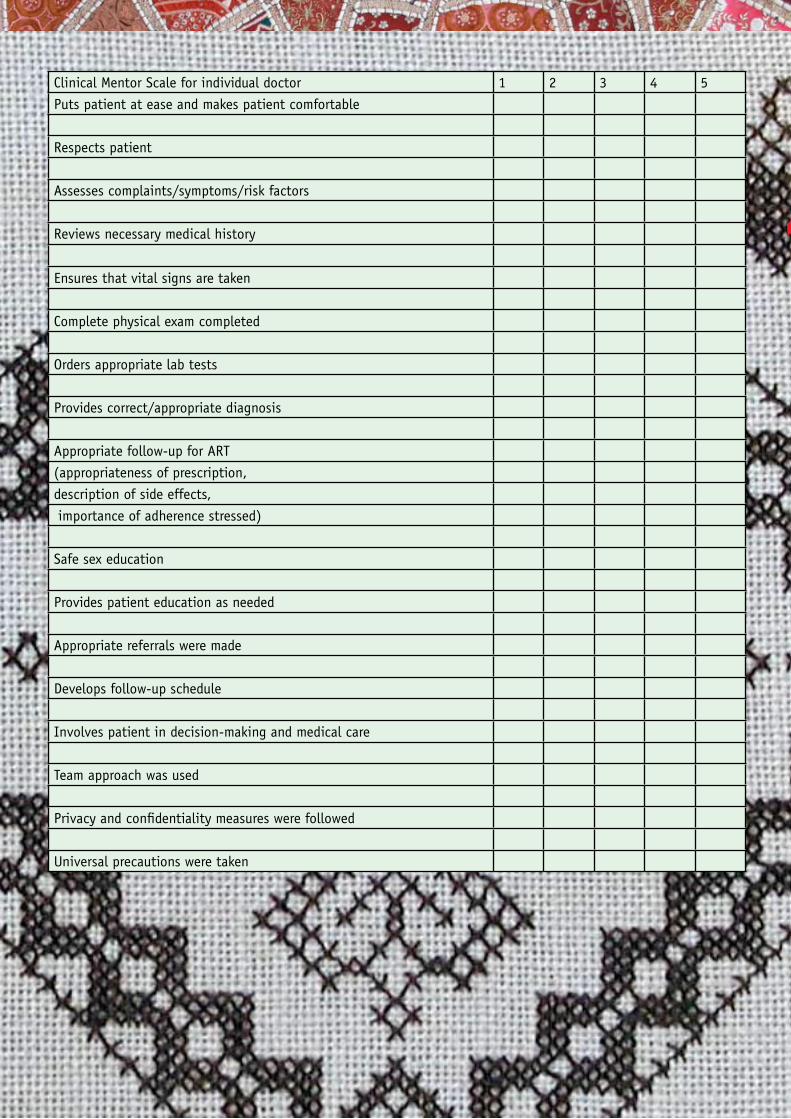
42 HIV Clinical Mentorship - In a public health context
Clinical Mentor Scale for individual doctor 1 2 3 4 5
Puts patient at ease and makes patient comfortable
Respects patient
Assesses complaints/symptoms/risk factors
Reviews necessary medical history
Ensures that vital signs are taken
Complete physical exam completed
Orders appropriate lab tests
Provides correct/appropriate diagnosis
Appropriate follow-up for ART
(appropriateness of prescription,
description of side effects,
importance of adherence stressed)
Safe sex education
Provides patient education as needed
Appropriate referrals were made
Develops follow-up schedule
Involves patient in decision-making and medical care
Team approach was used
Privacy and confidentiality measures were followed
Universal precautions were taken
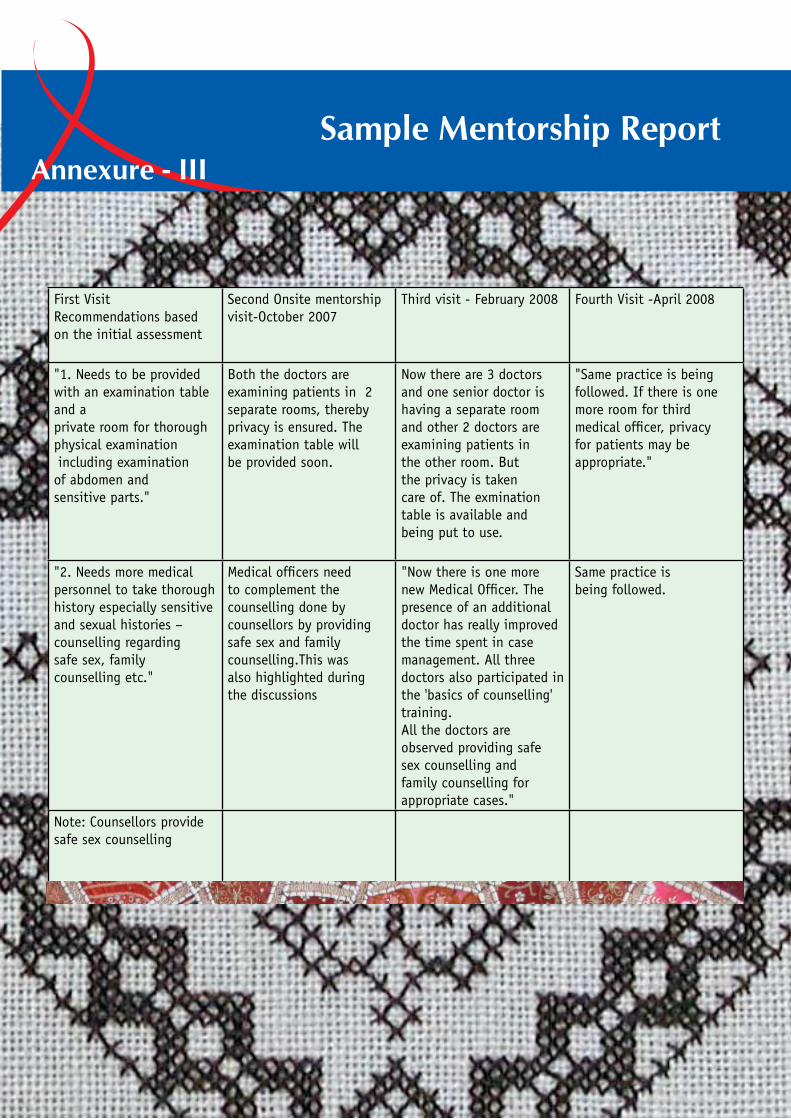
43HIV Clinical Mentorship - In a public health context
First Visit Recommendations based on the initial assessment
Second Onsite mentorship visit-October 2007
Third visit - February 2008 Fourth Visit -April 2008
"1. Needs to be provided with an examination table and a private room for thorough physical examination including examination of abdomen and sensitive parts."
Both the doctors are examining patients in 2 separate rooms, thereby privacy is ensured. The examination table will be provided soon.
Now there are 3 doctors and one senior doctor is having a separate room and other 2 doctors are examining patients in the other room. But the privacy is taken care of. The exmination table is available and being put to use.
"Same practice is being followed. If there is one more room for third medical officer, privacy for patients may be appropriate."
"2. Needs more medical personnel to take thorough history especially sensitive and sexual histories – counselling regarding safe sex, family counselling etc."
Medical officers need to complement the counselling done by counsellors by providing safe sex and family counselling.This was also highlighted during the discussions
"Now there is one more new Medical Officer. The presence of an additional doctor has really improved the time spent in case management. All three doctors also participated in the 'basics of counselling' training. All the doctors are observed providing safe sex counselling and family counselling for appropriate cases."
Same practice is being followed.
Note: Counsellors provide safe sex counselling
Sample Mentorship ReportAnnexure - III
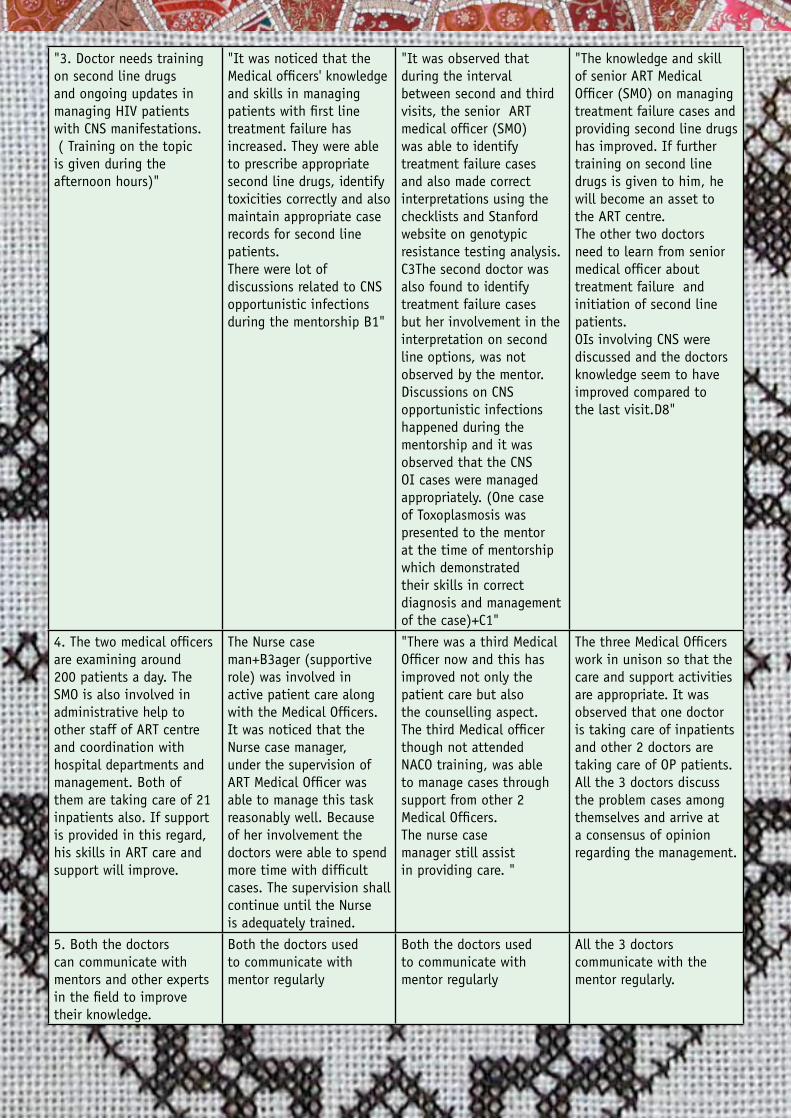
44 HIV Clinical Mentorship - In a public health context
"3. Doctor needs training on second line drugs and ongoing updates in managing HIV patients with CNS manifestations. ( Training on the topic is given during the afternoon hours)"
"It was noticed that the Medical officers' knowledge and skills in managing patients with first line treatment failure has increased. They were able to prescribe appropriate second line drugs, identify toxicities correctly and also maintain appropriate case records for second line patients. There were lot of discussions related to CNS opportunistic infections during the mentorship B1"
"It was observed that during the interval between second and third visits, the senior ART medical officer (SMO) was able to identify treatment failure cases and also made correct interpretations using the checklists and Stanford website on genotypic resistance testing analysis. C3The second doctor was also found to identify treatment failure cases but her involvement in the interpretation on second line options, was not observed by the mentor. Discussions on CNS opportunistic infections happened during the mentorship and it was observed that the CNS OI cases were managed appropriately. (One case of Toxoplasmosis was presented to the mentor at the time of mentorship which demonstrated their skills in correct diagnosis and management of the case)+C1"
"The knowledge and skill of senior ART Medical Officer (SMO) on managing treatment failure cases and providing second line drugs has improved. If further training on second line drugs is given to him, he will become an asset to the ART centre. The other two doctors need to learn from senior medical officer about treatment failure and initiation of second line patients. OIs involving CNS were discussed and the doctors knowledge seem to have improved compared to the last visit.D8"
4. The two medical officers are examining around 200 patients a day. The SMO is also involved in administrative help to other staff of ART centre and coordination with hospital departments and management. Both of them are taking care of 21 inpatients also. If support is provided in this regard, his skills in ART care and support will improve.
The Nurse case man+B3ager (supportive role) was involved in active patient care along with the Medical Officers. It was noticed that the Nurse case manager, under the supervision of ART Medical Officer was able to manage this task reasonably well. Because of her involvement the doctors were able to spend more time with difficult cases. The supervision shall continue until the Nurse is adequately trained.
"There was a third Medical Officer now and this has improved not only the patient care but also the counselling aspect. The third Medical officer though not attended NACO training, was able to manage cases through support from other 2 Medical Officers. The nurse case manager still assist in providing care. "
The three Medical Officers work in unison so that the care and support activities are appropriate. It was observed that one doctor is taking care of inpatients and other 2 doctors are taking care of OP patients. All the 3 doctors discuss the problem cases among themselves and arrive at a consensus of opinion regarding the management.
5. Both the doctors can communicate with mentors and other experts in the field to improve their knowledge.
Both the doctors used to communicate with mentor regularly
Both the doctors used to communicate with mentor regularly
All the 3 doctors communicate with the mentor regularly.
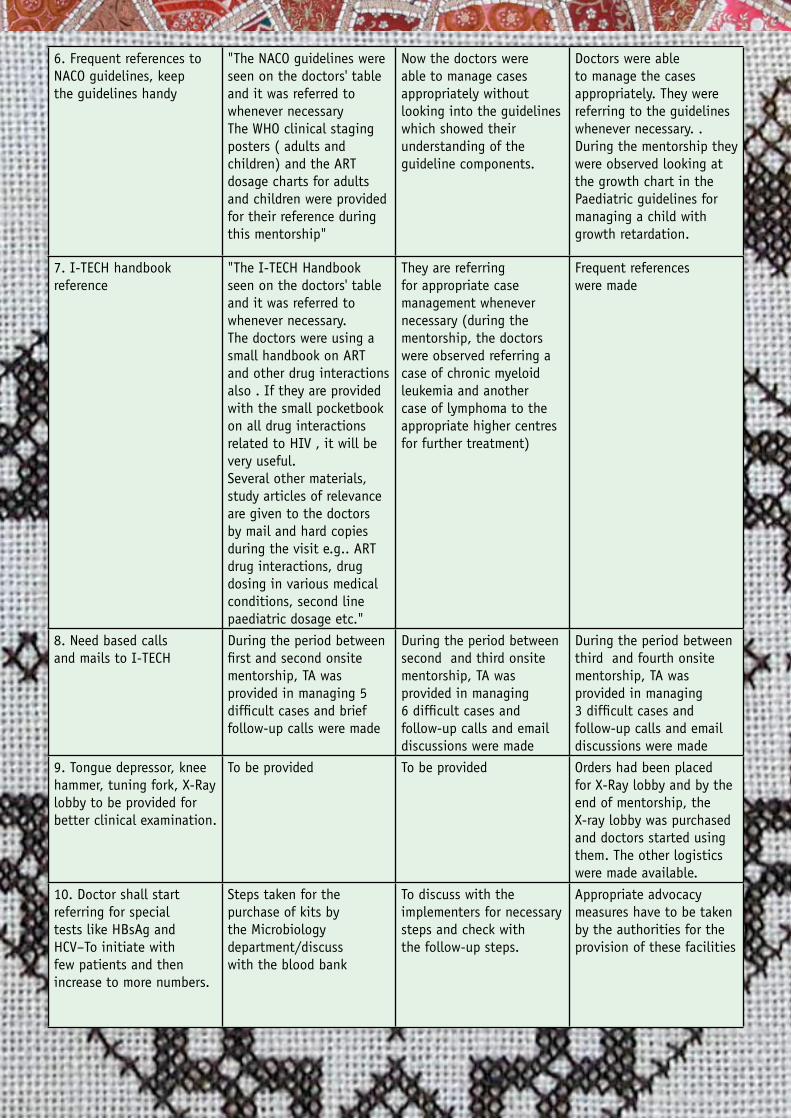
45HIV Clinical Mentorship - In a public health context
6. Frequent references to NACO guidelines, keep the guidelines handy
"The NACO guidelines were seen on the doctors' table and it was referred to whenever necessary The WHO clinical staging posters ( adults and children) and the ART dosage charts for adults and children were provided for their reference during this mentorship"
Now the doctors were able to manage cases appropriately without looking into the guidelines which showed their understanding of the guideline components.
Doctors were able to manage the cases appropriately. They were referring to the guidelines whenever necessary. . During the mentorship they were observed looking at the growth chart in the Paediatric guidelines for managing a child with growth retardation.
7. I-TECH handbook reference
"The I-TECH Handbook seen on the doctors' table and it was referred to whenever necessary. The doctors were using a small handbook on ART and other drug interactions also . If they are provided with the small pocketbook on all drug interactions related to HIV , it will be very useful. Several other materials, study articles of relevance are given to the doctors by mail and hard copies during the visit e.g.. ART drug interactions, drug dosing in various medical conditions, second line paediatric dosage etc."
They are referring for appropriate case management whenever necessary (during the mentorship, the doctors were observed referring a case of chronic myeloid leukemia and another case of lymphoma to the appropriate higher centres for further treatment)
Frequent references were made
8. Need based calls and mails to I-TECH
During the period between first and second onsite mentorship, TA was provided in managing 5 difficult cases and brief follow-up calls were made
During the period between second and third onsite mentorship, TA was provided in managing 6 difficult cases and follow-up calls and email discussions were made
During the period between third and fourth onsite mentorship, TA was provided in managing 3 difficult cases and follow-up calls and email discussions were made
9. Tongue depressor, knee hammer, tuning fork, X-Ray lobby to be provided for better clinical examination.
To be provided To be provided Orders had been placed for X-Ray lobby and by the end of mentorship, the X-ray lobby was purchased and doctors started using them. The other logistics were made available.
10. Doctor shall start referring for special tests like HBsAg and HCV–To initiate with few patients and then increase to more numbers.
Steps taken for the purchase of kits by the Microbiology department/discuss with the blood bank
To discuss with the implementers for necessary steps and check with the follow-up steps.
Appropriate advocacy measures have to be taken by the authorities for the provision of these facilities
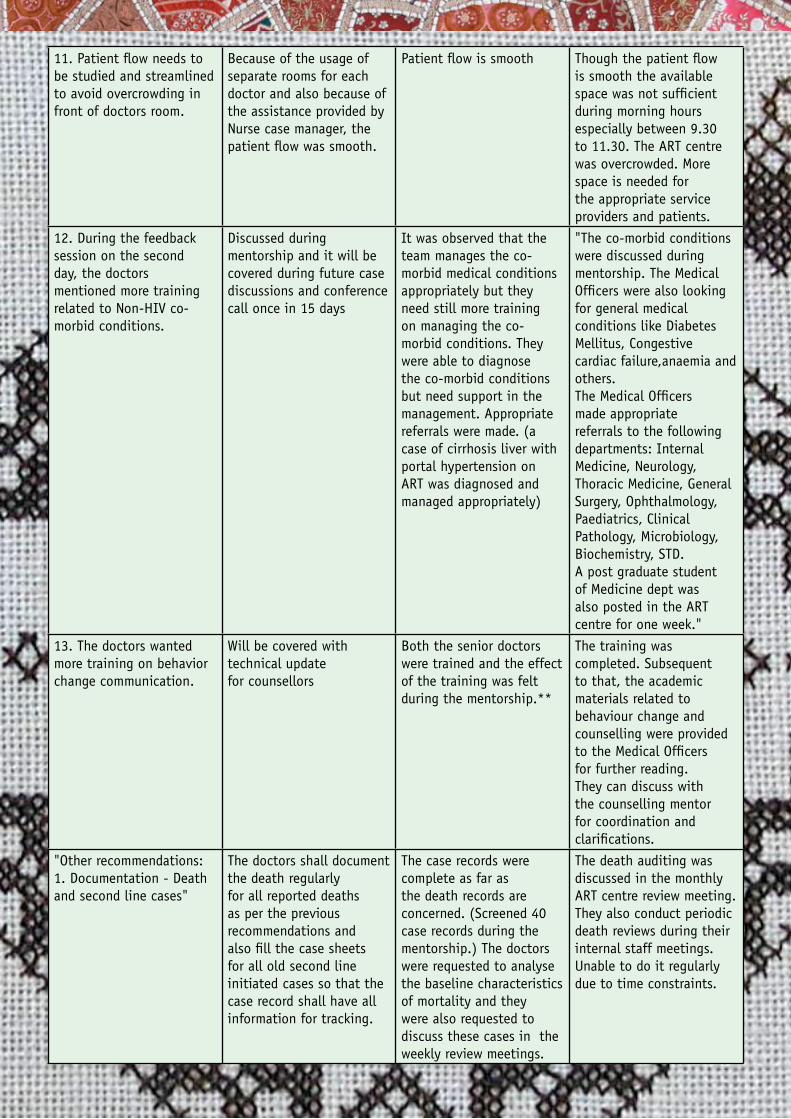
46 HIV Clinical Mentorship - In a public health context
11. Patient flow needs to be studied and streamlined to avoid overcrowding in front of doctors room.
Because of the usage of separate rooms for each doctor and also because of the assistance provided by Nurse case manager, the patient flow was smooth.
Patient flow is smooth Though the patient flow is smooth the available space was not sufficient during morning hours especially between 9.30 to 11.30. The ART centre was overcrowded. More space is needed for the appropriate service providers and patients.
12. During the feedback session on the second day, the doctors mentioned more training related to Non-HIV co-morbid conditions.
Discussed during mentorship and it will be covered during future case discussions and conference call once in 15 days
It was observed that the team manages the co-morbid medical conditions appropriately but they need still more training on managing the co-morbid conditions. They were able to diagnose the co-morbid conditions but need support in the management. Appropriate referrals were made. (a case of cirrhosis liver with portal hypertension on ART was diagnosed and managed appropriately)
"The co-morbid conditions were discussed during mentorship. The Medical Officers were also looking for general medical conditions like Diabetes Mellitus, Congestive cardiac failure,anaemia and others. The Medical Officers made appropriate referrals to the following departments: Internal Medicine, Neurology, Thoracic Medicine, General Surgery, Ophthalmology, Paediatrics, Clinical Pathology, Microbiology, Biochemistry, STD. A post graduate student of Medicine dept was also posted in the ART centre for one week."
13. The doctors wanted more training on behavior change communication.
Will be covered with technical update for counsellors
Both the senior doctors were trained and the effect of the training was felt during the mentorship.**
The training was completed. Subsequent to that, the academic materials related to behaviour change and counselling were provided to the Medical Officers for further reading. They can discuss with the counselling mentor for coordination and clarifications.
"Other recommendations: 1. Documentation - Death and second line cases"
The doctors shall document the death regularly for all reported deaths as per the previous recommendations and also fill the case sheets for all old second line initiated cases so that the case record shall have all information for tracking.
The case records were complete as far as the death records are concerned. (Screened 40 case records during the mentorship.) The doctors were requested to analyse the baseline characteristics of mortality and they were also requested to discuss these cases in the weekly review meetings.
The death auditing was discussed in the monthly ART centre review meeting. They also conduct periodic death reviews during their internal staff meetings. Unable to do it regularly due to time constraints.
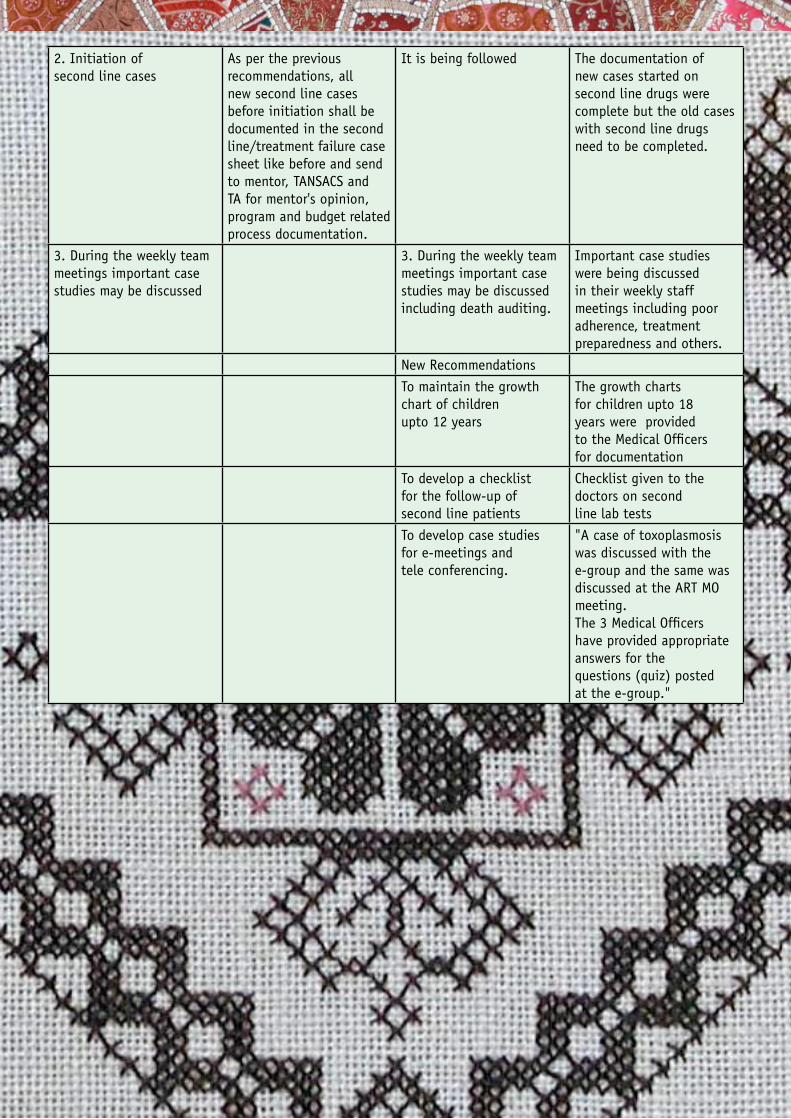
47HIV Clinical Mentorship - In a public health context
2. Initiation of second line cases
As per the previous recommendations, all new second line cases before initiation shall be documented in the second line/treatment failure case sheet like before and send to mentor, TANSACS and TA for mentor's opinion, program and budget related process documentation.
It is being followed The documentation of new cases started on second line drugs were complete but the old cases with second line drugs need to be completed.
3. During the weekly team meetings important case studies may be discussed
3. During the weekly team meetings important case studies may be discussed including death auditing.
Important case studies were being discussed in their weekly staff meetings including poor adherence, treatment preparedness and others.
New Recommendations
To maintain the growth chart of children upto 12 years
The growth charts for children upto 18 years were provided to the Medical Officers for documentation
To develop a checklist for the follow-up of second line patients
Checklist given to the doctors on second line lab tests
To develop case studies for e-meetings and tele conferencing.
"A case of toxoplasmosis was discussed with the e-group and the same was discussed at the ART MO meeting. The 3 Medical Officers have provided appropriate answers for the questions (quiz) posted at the e-group."
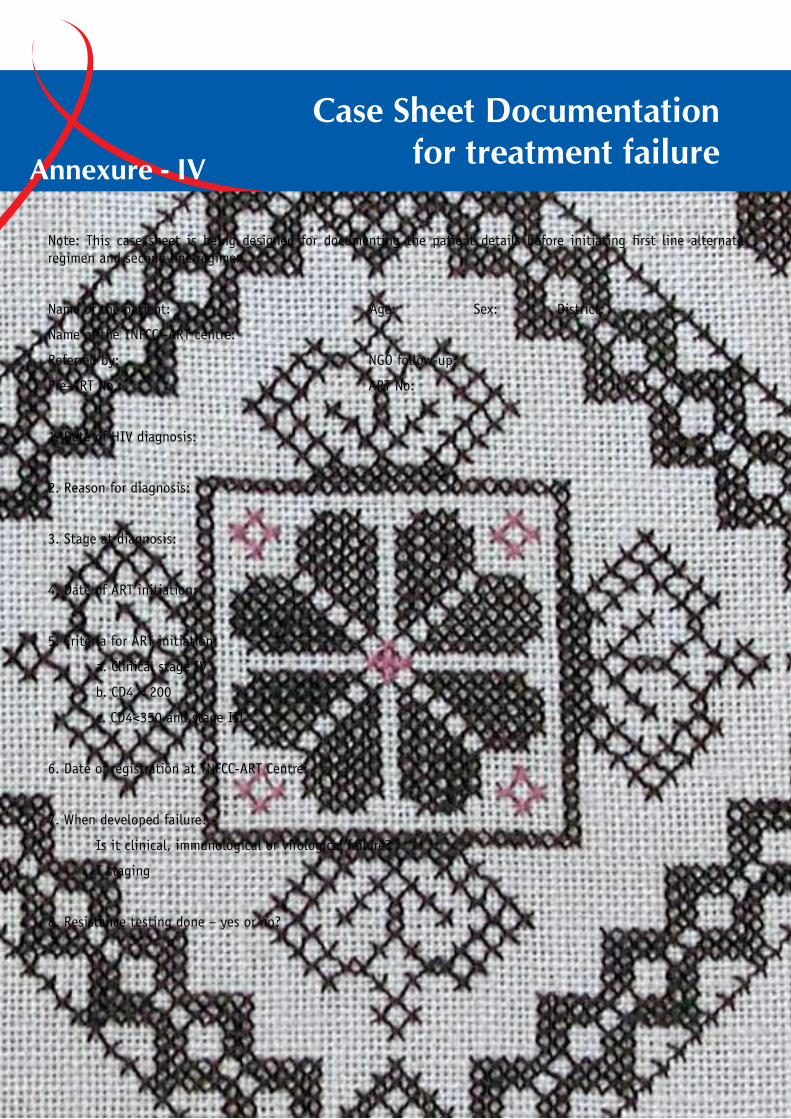
48 HIV Clinical Mentorship - In a public health context
Note: This case sheet is being designed for documenting the patient details before initiating first line alternate regimen and second line regimen.
Name of the patient: Age: Sex: District:
Name of the TNFCC -ART centre:
Referred by: NGO follow-up:
Pre-ART No.: ART No:
1. Date of HIV diagnosis:
2. Reason for diagnosis:
3. Stage at diagnosis:
4. Date of ART initiation:
5. Criteria for ART initiation:
a. Clinical stage IV
b. CD4 < 200
c. CD4<350 and stage III
6. Date of registration at TNFCC-ART Centre:
7. When developed failure? -
Is it clinical, immunological or virological failure?
T staging
8. Resistance testing done – yes or no?
Case Sheet Documentation for treatment failureAnnexure - IV

49HIV Clinical Mentorship - In a public health context
9. A
RT t
reat
men
t de
tails
: S.No
Period*
Regimen with duration ( … months)
Place of treatment
CD4 count/% with date
Viral load with date
Cause for change in regimen**
Adh %
T Stage
Wt
Ht (in children)
OIs
Drug side effects
Imp. lab values
Remarks***
1
2
3
4
5
6
7
* -
If d
ate
not
avai
labl
e, p
leas
e m
enti
on m
onth
and
yea
r or
yea
r on
ly.
•**
- AR
V dr
ug s
ide
effe
cts/
toxi
city
/ s
ubst
itut
ion
/ st
oppe
d Rx
/ t
reat
men
t fa
ilure
- im
mun
olog
ical
/clin
ical
/viro
logi
cal f
ailu
re e
tc.
***
-Rem
arks
- p
leas
e m
enti
on r
easo
ns f
or p
oor
adhe
renc
e, d
rug/
Rx s
topp
ed,
any
med
ical
and
soc
ial f
acto
rs w
hich
are
app
ropr
iate
.Pl
ease
go
thro
ugh
priv
ate
doct
or’s
pres
crip
tion
s (i
f pa
tien
t is
tak
ing
ART
wit
h pr
ivat
e do
ctor
) fo
r ad
here
nce
and
regi
men
typ
e (m
ono/
dual
/tri
ple
•dr
ug a
nd na
me
of d
rugs
)

50 HIV Clinical Mentorship - In a public health context
10. If done, resistance testing reports (provided resistance testing is done when the patient is on ART drugs)
11. Analysis of resistance testing and interpretation of resistance test report:
12. Appropriate second line drug regimen:
13. Appropriate lab tests done before second line ART initiation – Yes/No If yes, please mention the lab values.

51HIV Clinical Mentorship - In a public health context
52 HIV Clinical Mentorship - In a public health context





























