Embed Size (px)
Citation preview
Staying out of Trouble in Outpatient Musculoskeletal Problems
PRESENTED BY: Scott Yang MD, Assistant Professor, Pediatric Orthopaedic Surgery Doernbecher Children’s Hospital, OHSU
Doernbecher Children’s HospitalOHSU
2
No disclosures for this presentationOHSU
Physical examination – diagnostic tools to stay out of troubleOHSU
4
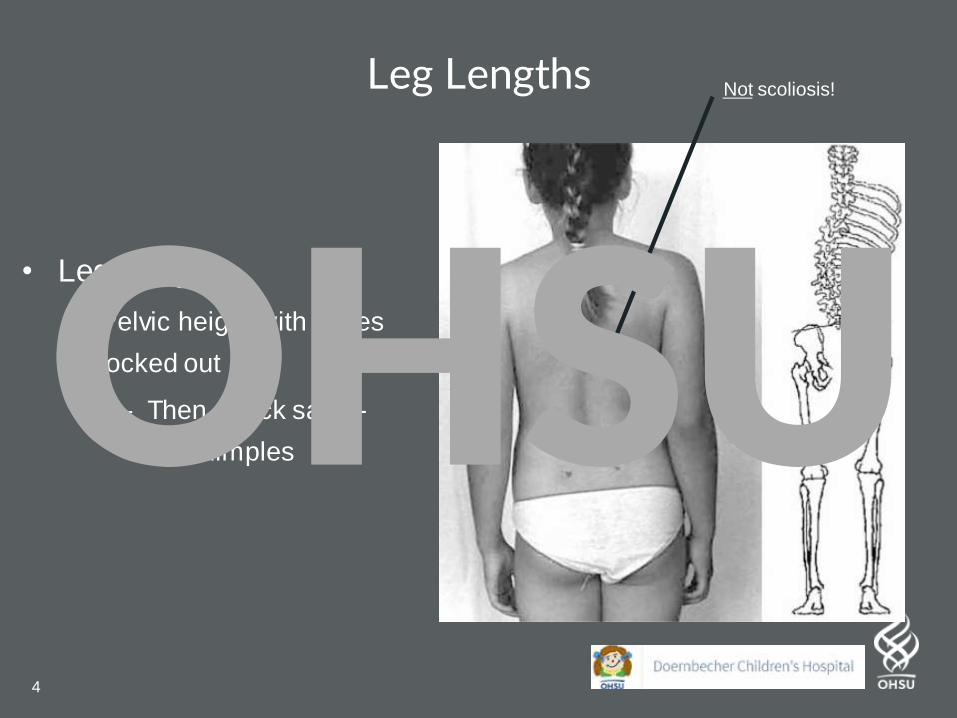
Leg Lengths
• Leg Lengths
– Pelvic height with knees
locked out
– Then check sacro-
iliac dimples
Not scoliosis!
OHSU
5
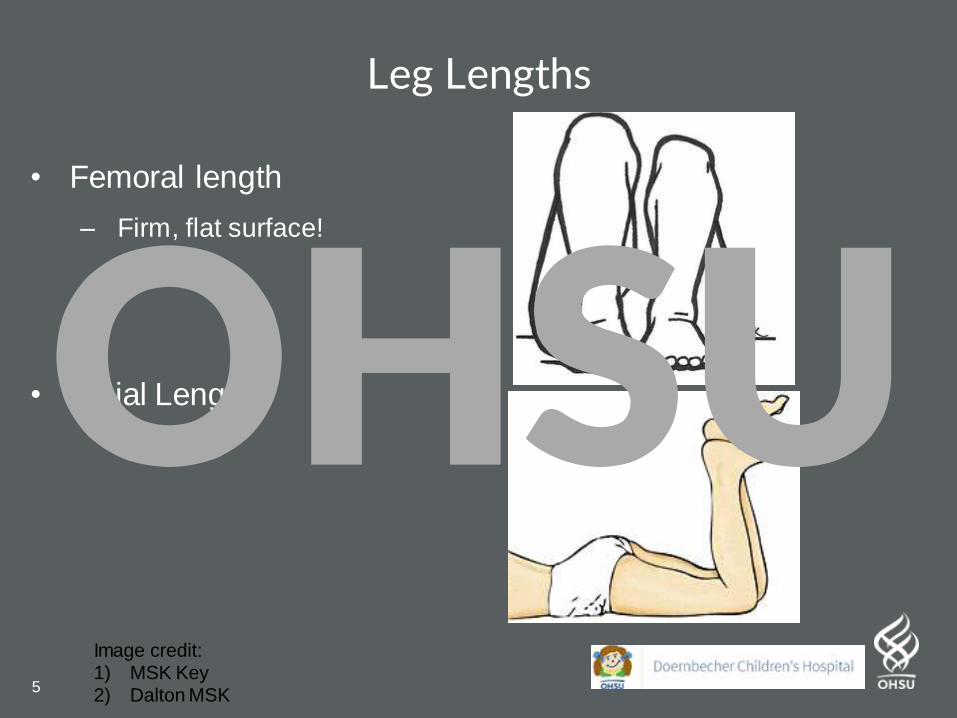
Leg Lengths
• Femoral length
– Firm, flat surface!
• Tibial Length
Image credit: 1) MSK Key2) Dalton MSK
OHSU
6
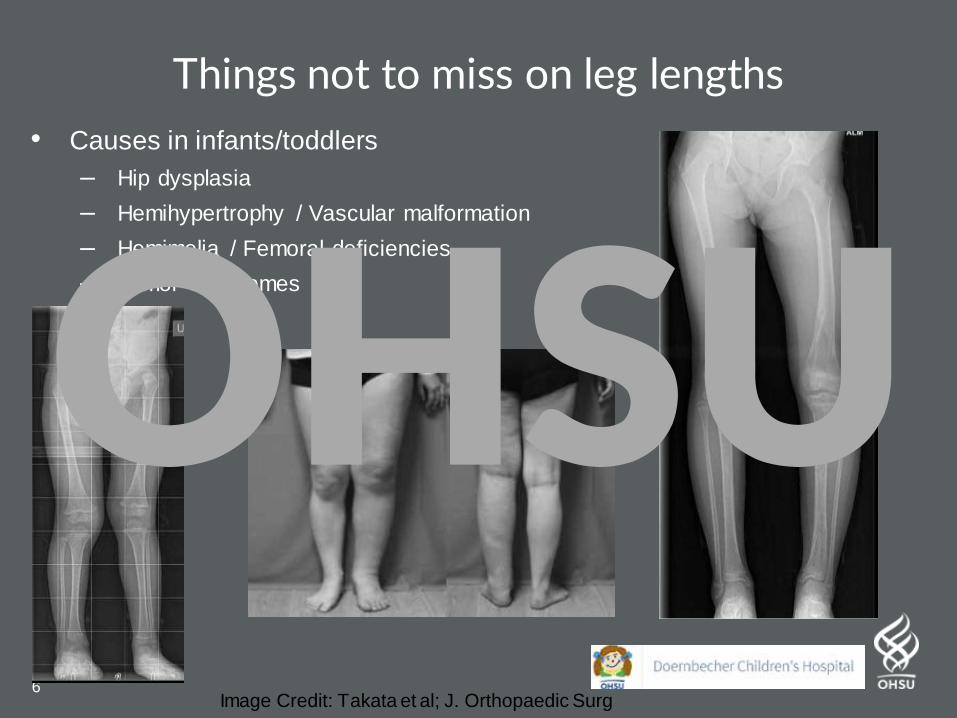
Things not to miss on leg lengths
• Causes in infants/toddlers
– Hip dysplasia
– Hemihypertrophy / Vascular malformation
– Hemimelia / Femoral deficiencies
– Tumor Syndromes
Image Credit: Takata et al; J. Orthopaedic Surg
OHSU
7
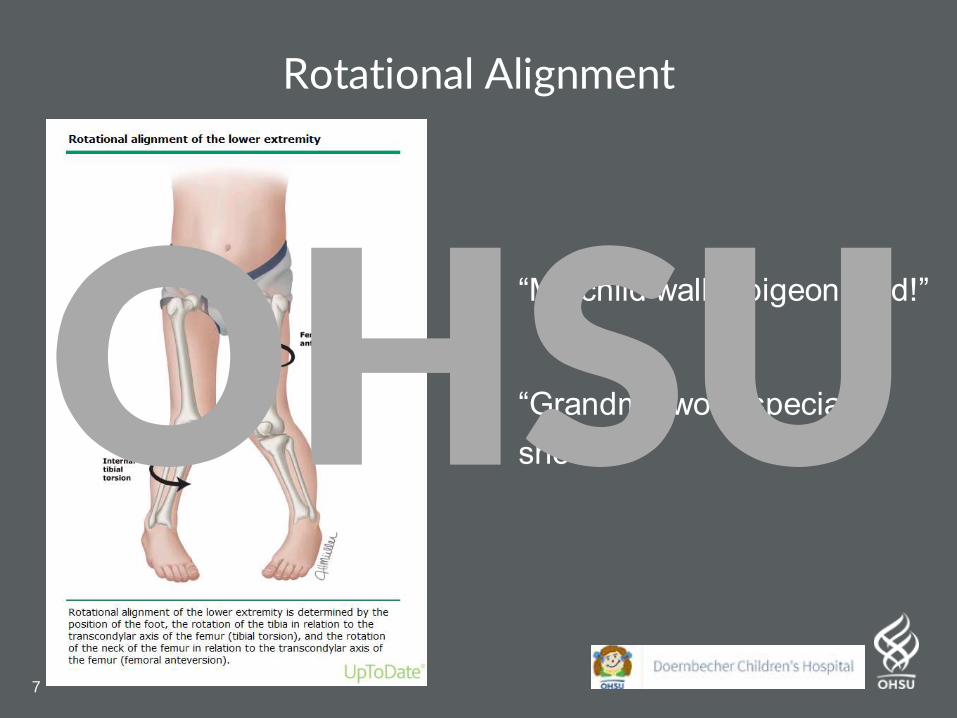
Rotational Alignment
• “My child walks pigeon toed!”
• “Grandma wore special
shoes”OHSU
8
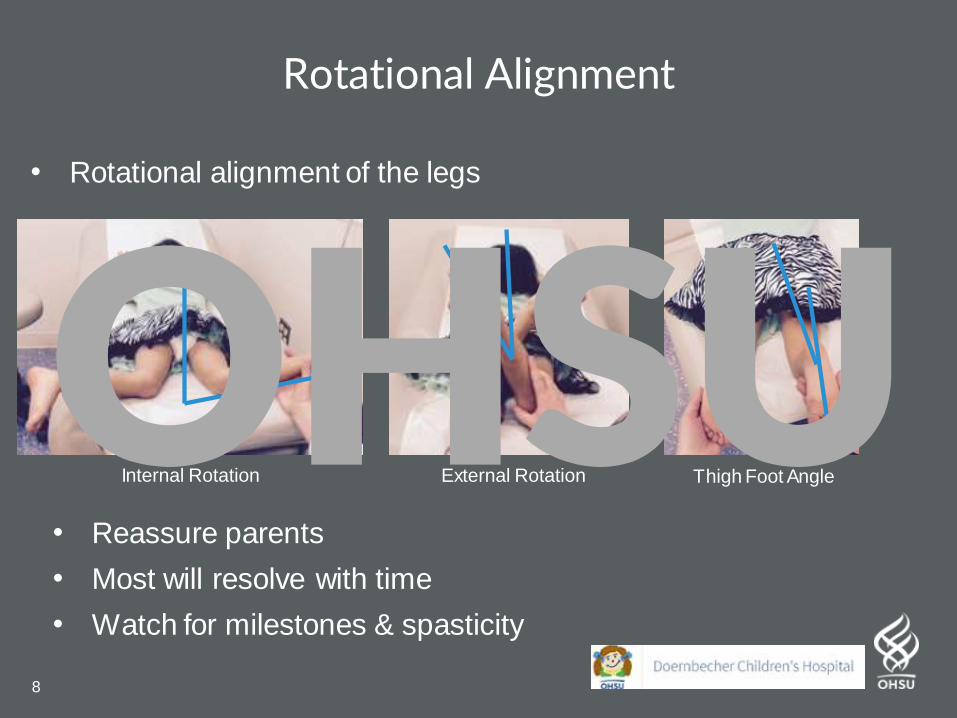
Rotational Alignment
• Rotational alignment of the legs
• Reassure parents
• Most will resolve with time
• Watch for milestones & spasticity
Internal Rotation External Rotation Thigh Foot AngleOHSU
9
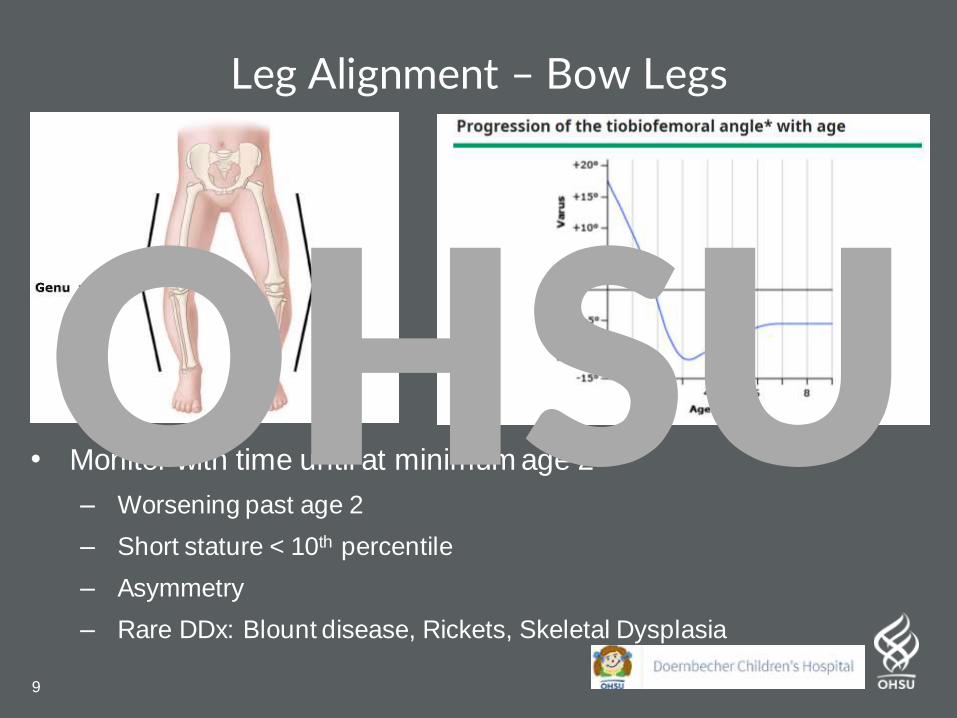
Leg Alignment – Bow Legs
• Monitor with time until at minimum age 2
– Worsening past age 2
– Short stature < 10th percentile
– Asymmetry
– Rare DDx: Blount disease, Rickets, Skeletal Dysplasia
OHSU
10
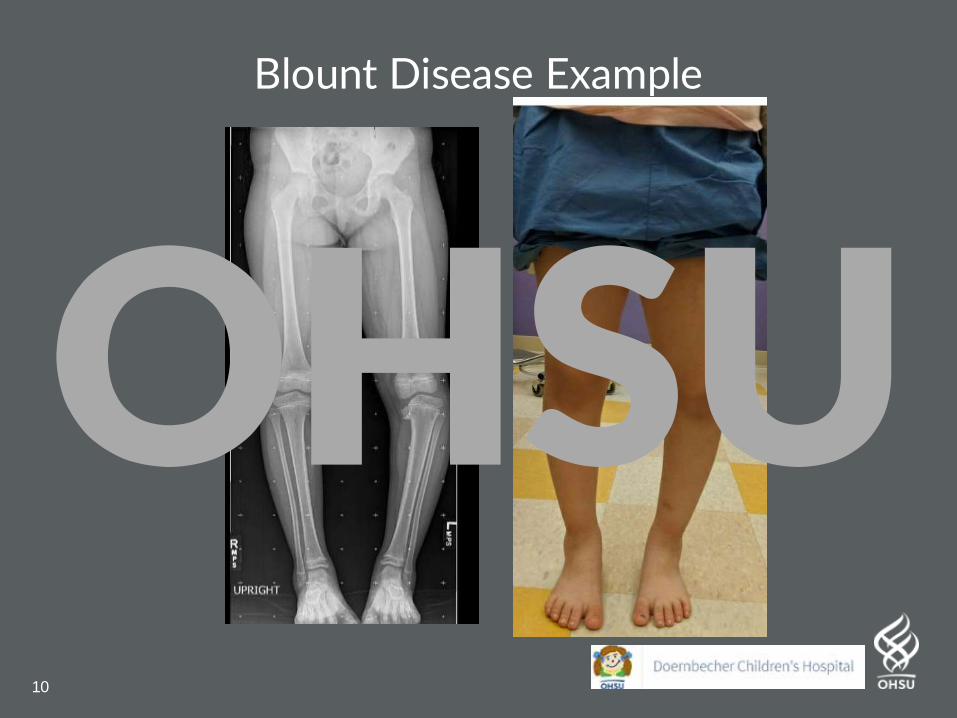
Blount Disease Example
OHSU
11
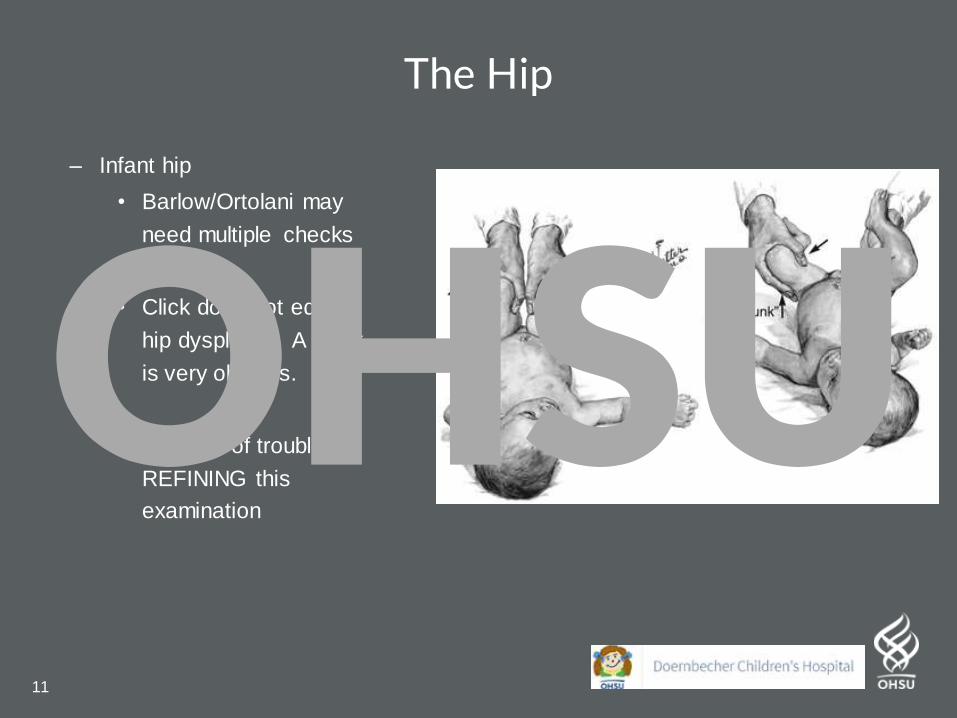
The Hip
– Infant hip
• Barlow/Ortolani may
need multiple checks
• Click does not equal
hip dysplasia. A clunk
is very obvious.
• Stay out of trouble by
REFINING this
examination
OHSU
12
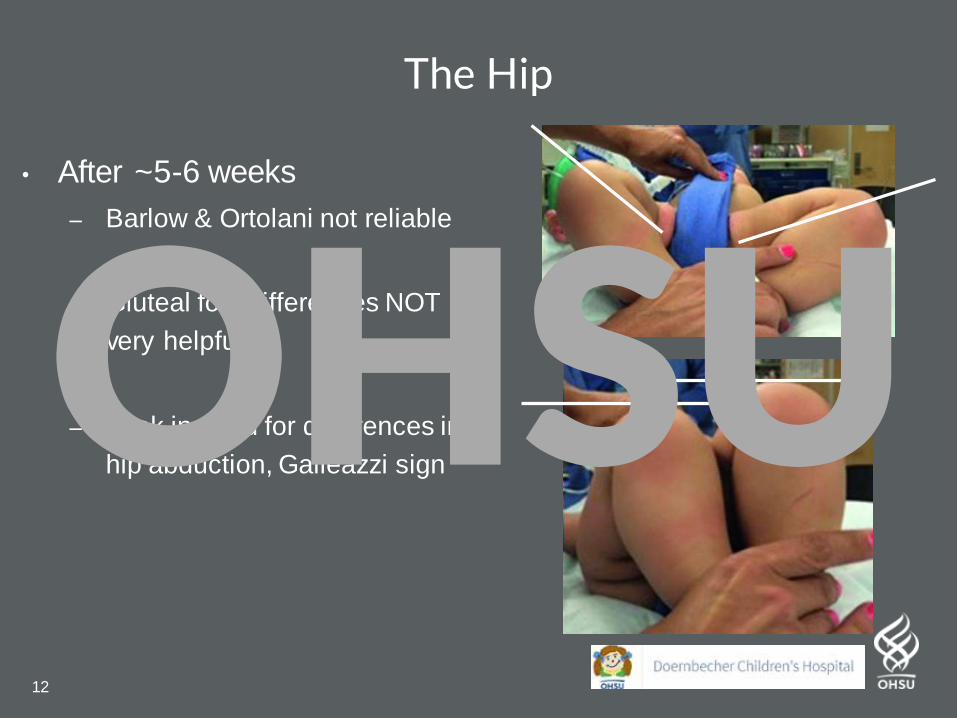
The Hip
• After ~5-6 weeks
– Barlow & Ortolani not reliable
– Gluteal fold differences NOT
very helpful
– Look instead for differences in
hip abduction, Galleazzi signOHSU
13
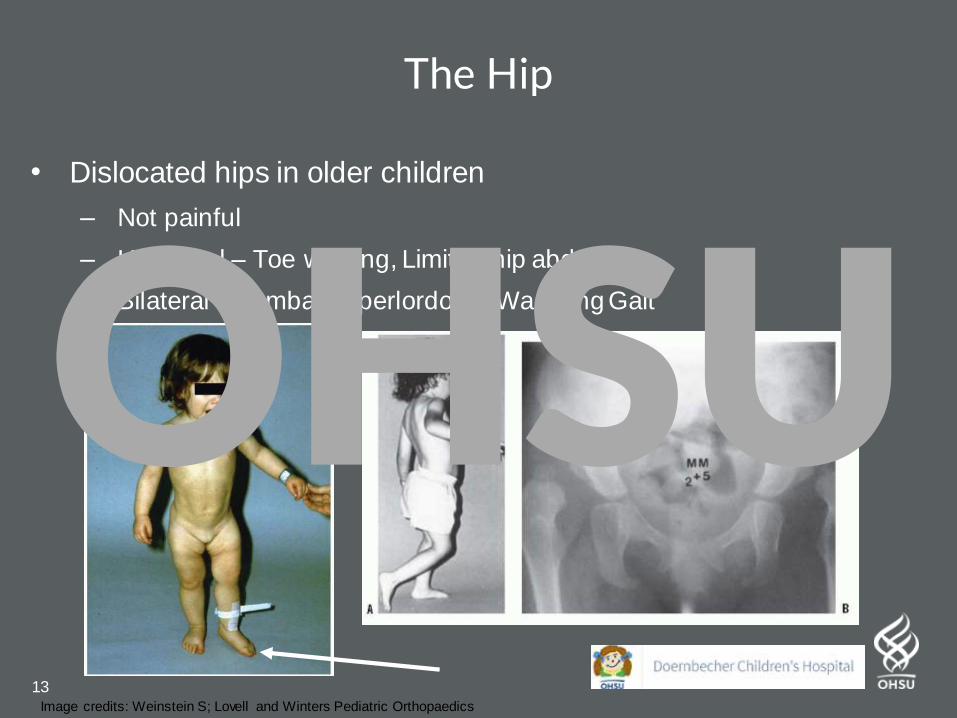
The Hip
• Dislocated hips in older children
– Not painful
– Unilateral – Toe walking, Limited hip abduction
– Bilateral – Lumbar hyperlordosis, Waddling Gait
Image credits: Weinstein S; Lovell and Winters Pediatric Orthopaedics
OHSU
14
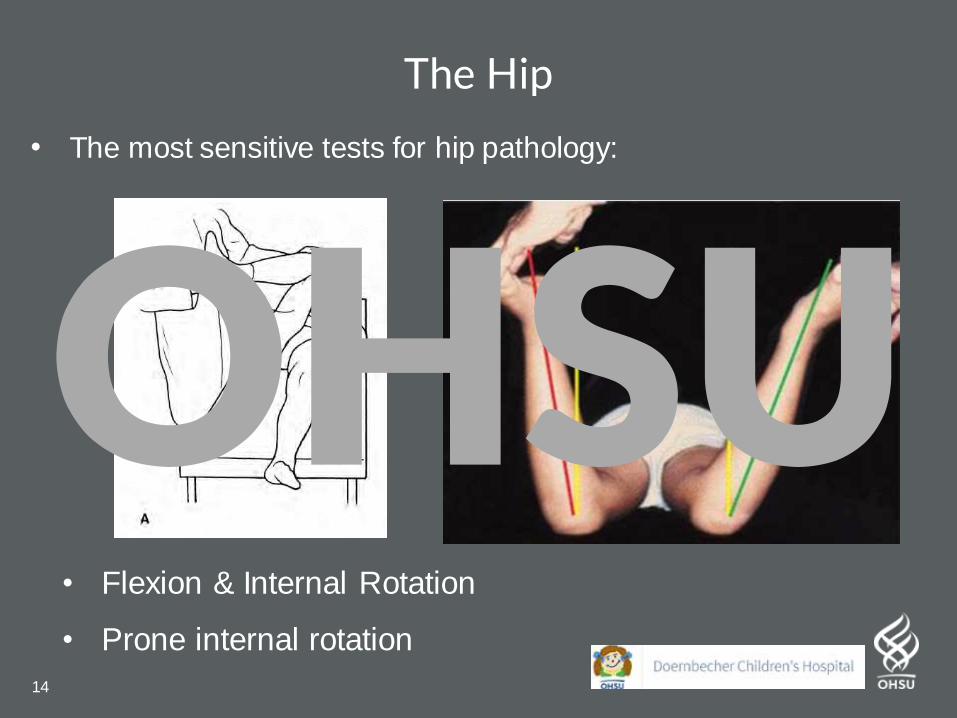
The Hip
• The most sensitive tests for hip pathology:
• Flexion & Internal Rotation
• Prone internal rotation
OHSU
15
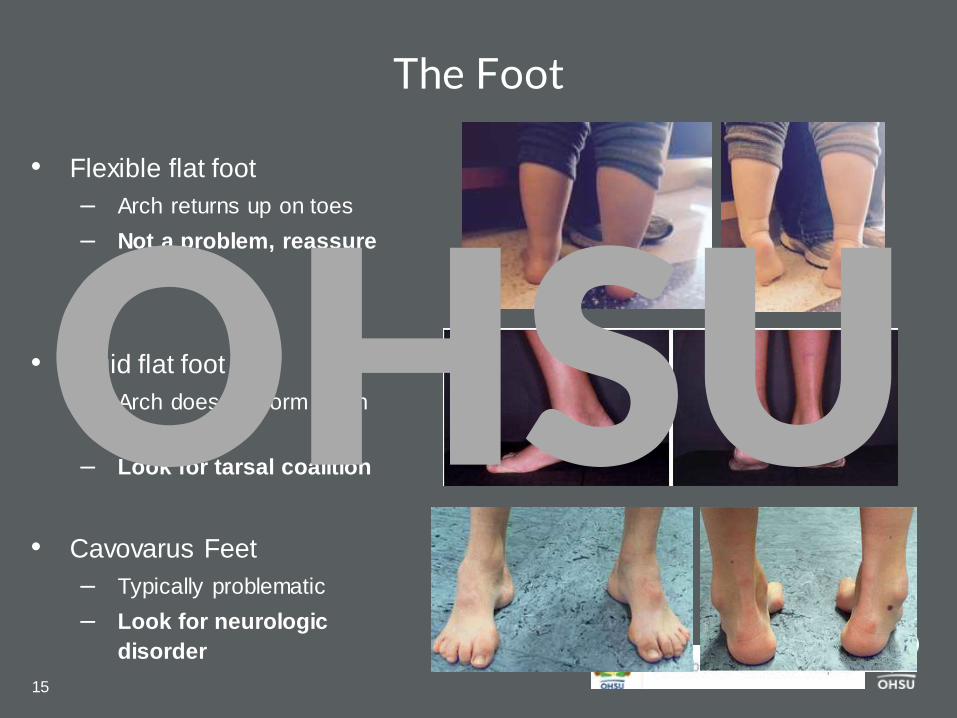
The Foot
• Flexible flat foot
– Arch returns up on toes
– Not a problem, reassure
• Rigid flat foot
– Arch does not form when
up on toes
– Look for tarsal coalition
• Cavovarus Feet
– Typically problematic
– Look for neurologic
disorder
OHSU
16
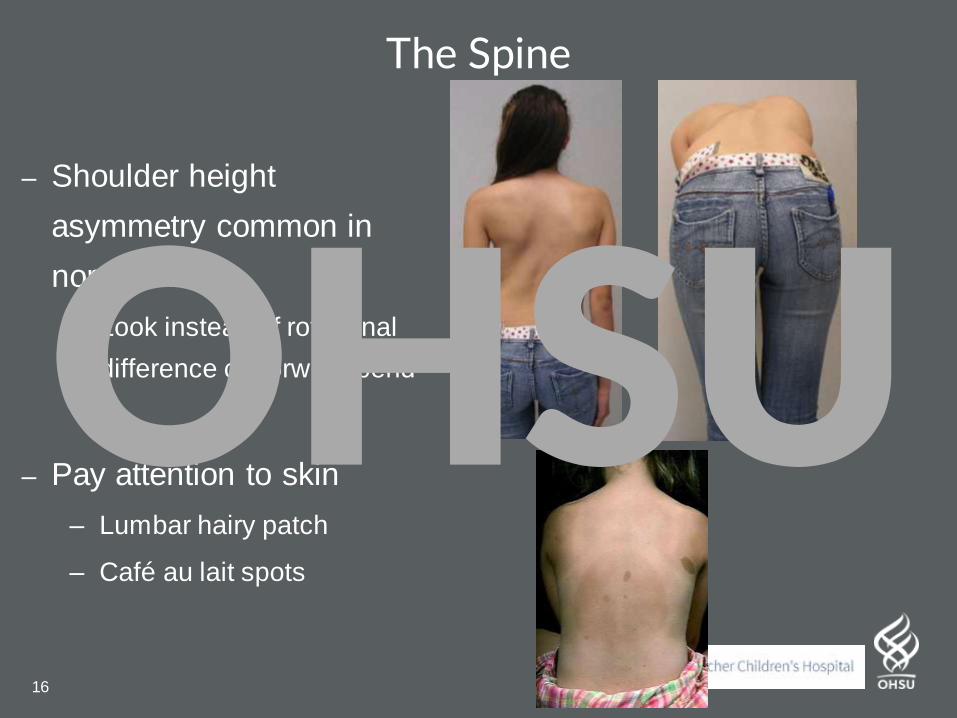
The Spine
– Shoulder height
asymmetry common in
normal kids
– Look instead of rotational
difference on forward bend
– Pay attention to skin
– Lumbar hairy patch
– Café au lait spots
OHSU
17
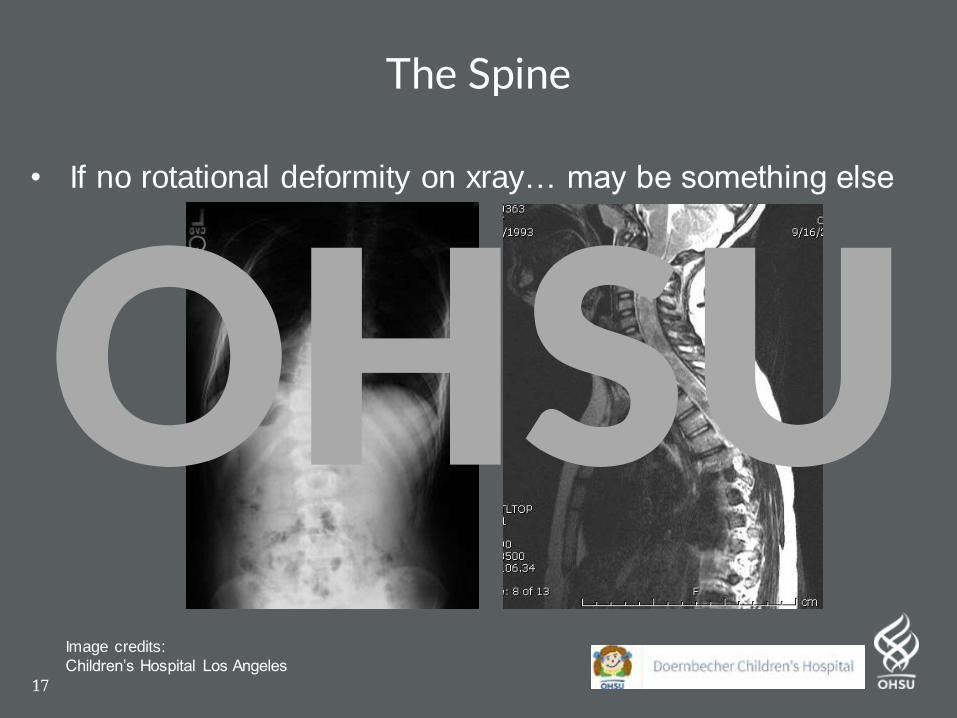
The Spine
• If no rotational deformity on xray… may be something else
Image credits:
Children’s Hospital Los Angeles
OHSU
18
“My child’s legs hurt”
• Simple tests to rule out growing pains from real pathology
• Tumors hurt. Infection hurts. Stress fractures hurt.
– Look for clear physical findings
– Single leg hop / jump x 5
– Squat jump x 10
– Then go for a walk & jog to look for limpOHSU
19
The Fresh NewbornOHSU
20
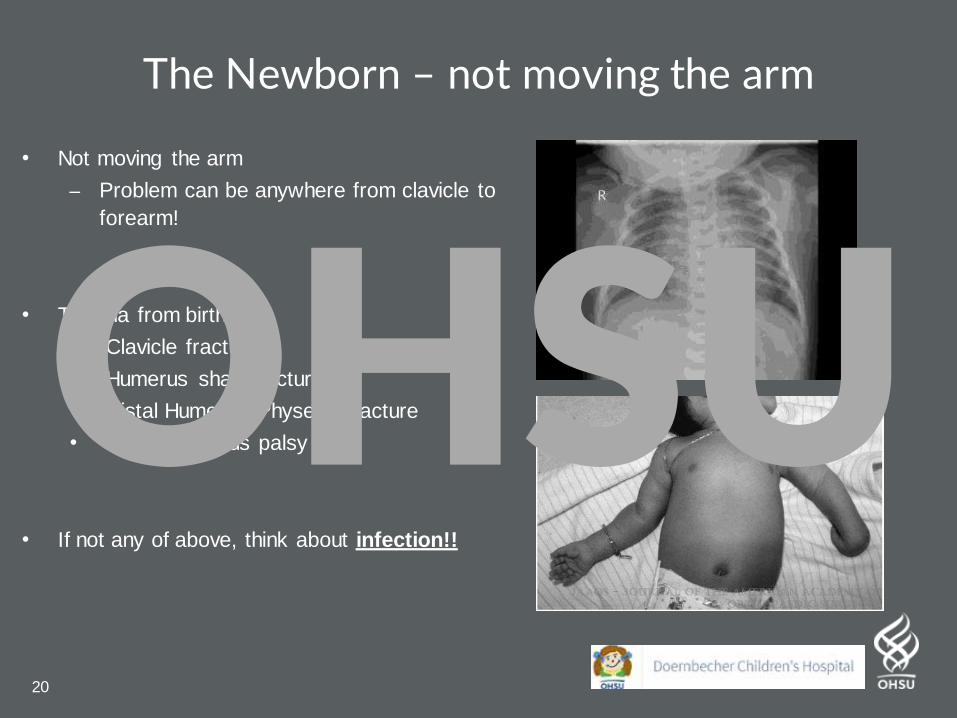
The Newborn – not moving the arm
• Not moving the arm
– Problem can be anywhere from clavicle to
forearm!
• Trauma from birth
• Clavicle fracture
• Humerus shaft fracture
• Distal Humerus Physeal Fracture
• Brachial Plexus palsy
• If not any of above, think about infection!!
OHSU
21
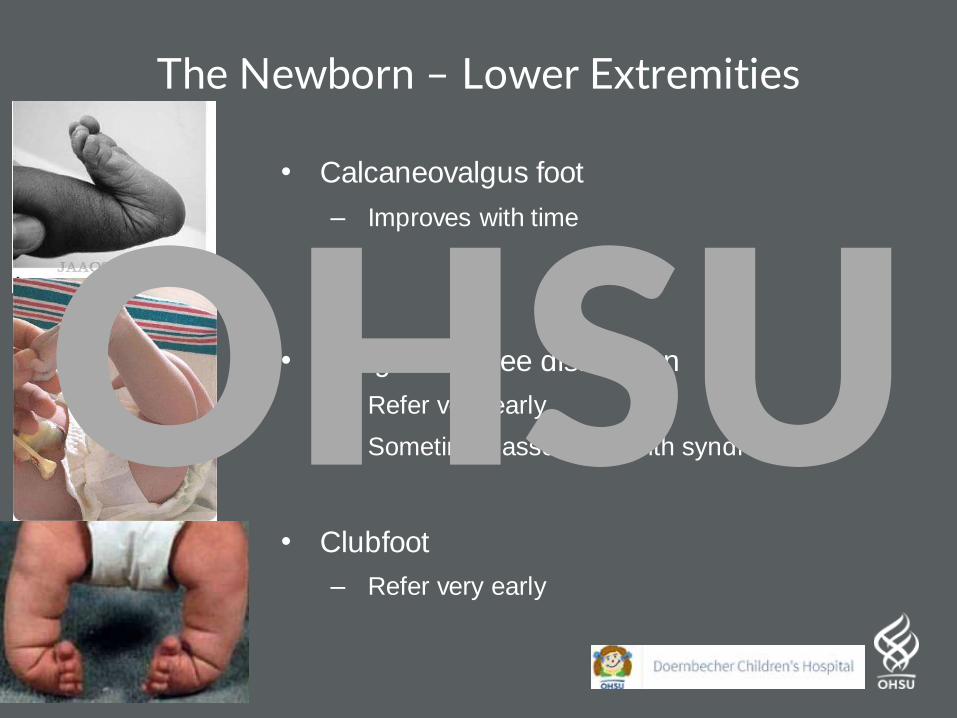
The Newborn – Lower Extremities
• Calcaneovalgus foot
– Improves with time
• Congenital knee dislocation
– Refer very early
– Sometimes associated with syndromes
• Clubfoot
– Refer very early
OHSU
22
Skeletal Injury from Child AbuseOHSU
23
Case ExampleHPI:
2 month old F brought in to PCP
for not moving left arm. Mother
unclear on traumatic event.
Conflicting history with Father.
Exam:
Guards left arm
Moves other limbs
spontaneously. No major
swelling or bruising
OHSU
24
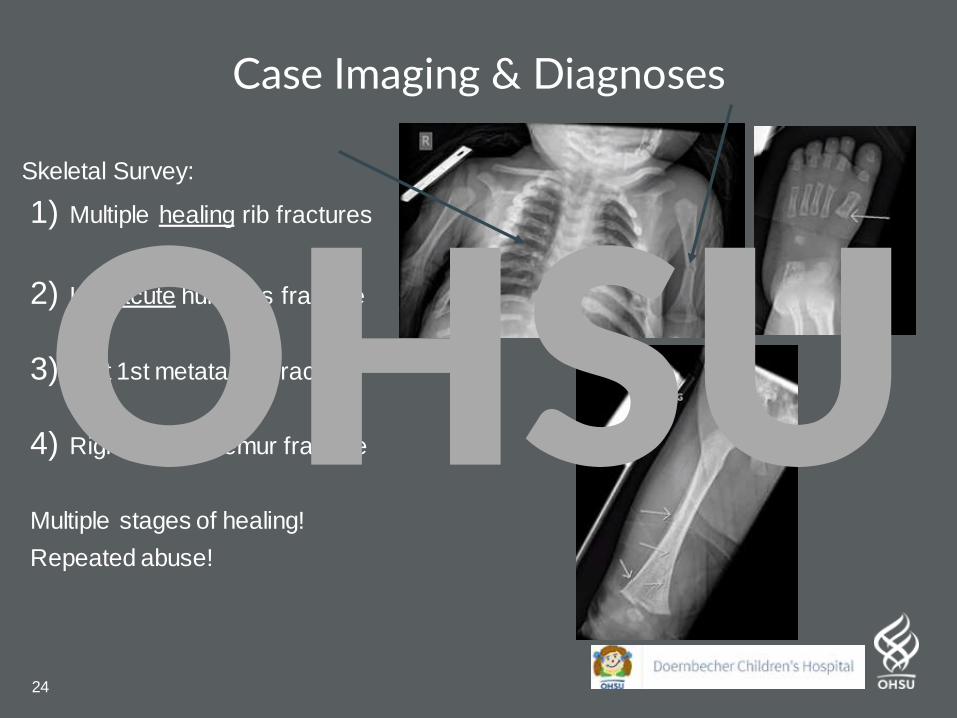
Case Imaging & Diagnoses
Skeletal Survey:
1) Multiple healing rib fractures
2) Left acute humerus fracture
3) Left 1st metatarsal fracture
4) Right healing femur fracture
Multiple stages of healing!
Repeated abuse!
OHSU
25
Case Treatment
• Hospitalize, Report to Social Work/DHS ASAP
• Treat injuries as appropriate, remove from current
situation
Learning Point: Very young non mobile children (< 1 year old) cannot easily hurt themselves
If presenting with pain or extremity splinting, they need you to advocate for them to look for injury, for which you may find many.
OHSU
26
The Pediatric HipOHSU
27
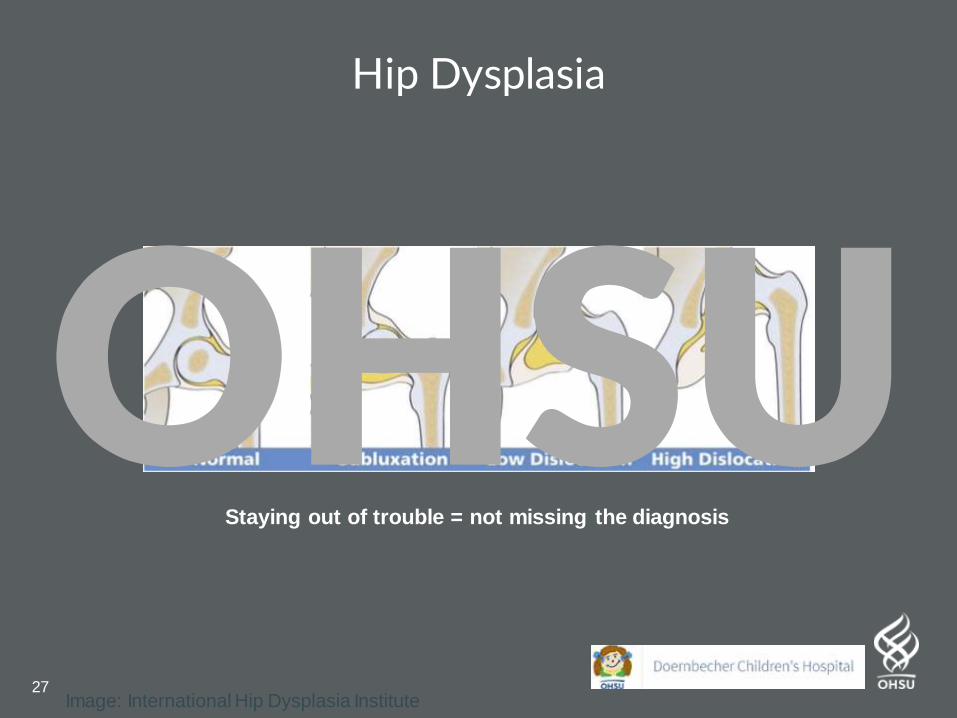
Hip Dysplasia
Image: International Hip Dysplasia Institute
Staying out of trouble = not missing the diagnosis
OHSU
28
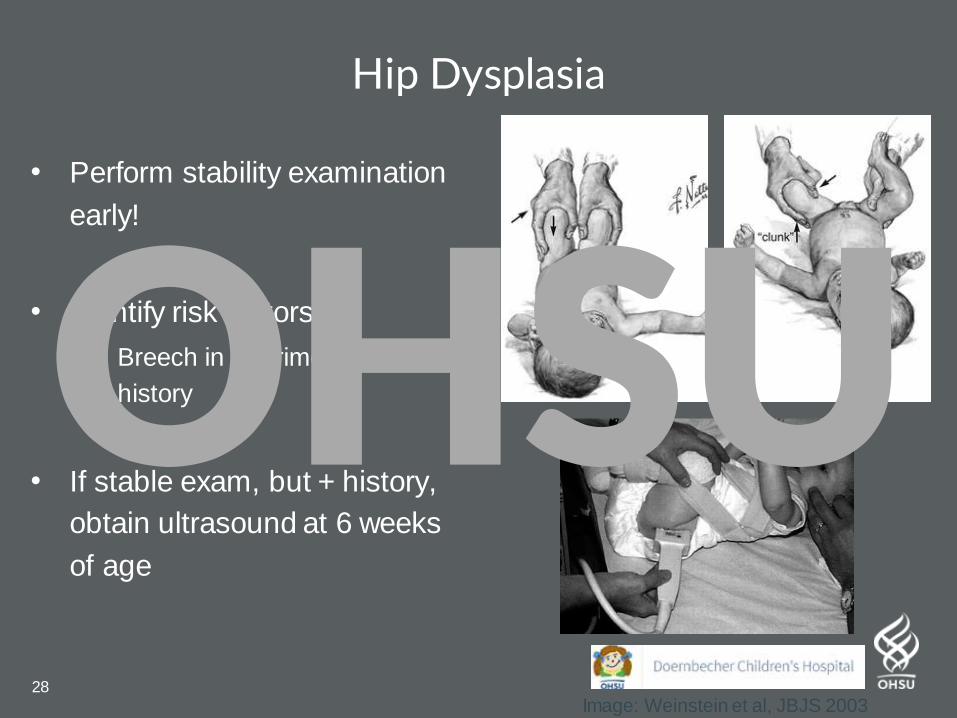
Hip Dysplasia
• Perform stability examination
early!
• Identify risk factors
– Breech in 3rd trimester; Family
history
• If stable exam, but + history,
obtain ultrasound at 6 weeks
of age
Image: Weinstein et al, JBJS 2003
OHSU
29
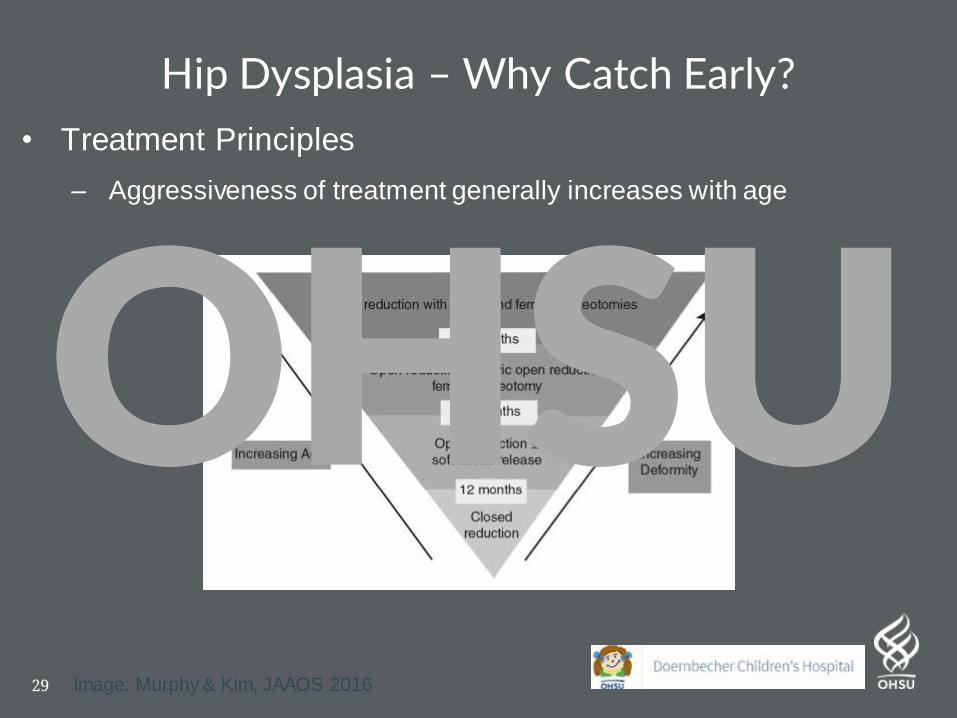
• Treatment Principles
– Aggressiveness of treatment generally increases with age
Hip Dysplasia – Why Catch Early?
Image: Murphy & Kim, JAAOS 2016
OHSU
30
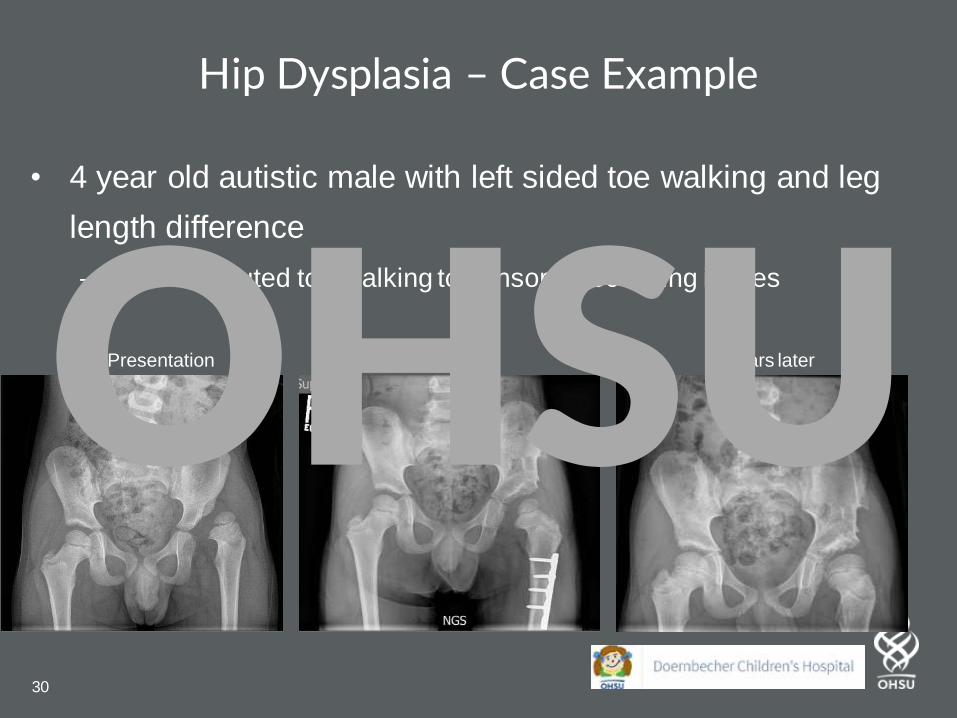
Hip Dysplasia – Case Example
• 4 year old autistic male with left sided toe walking and leg
length difference
– PCP attributed toe walking to sensory processing issues
Initial Presentation Surgery 2 years laterOHSU
31
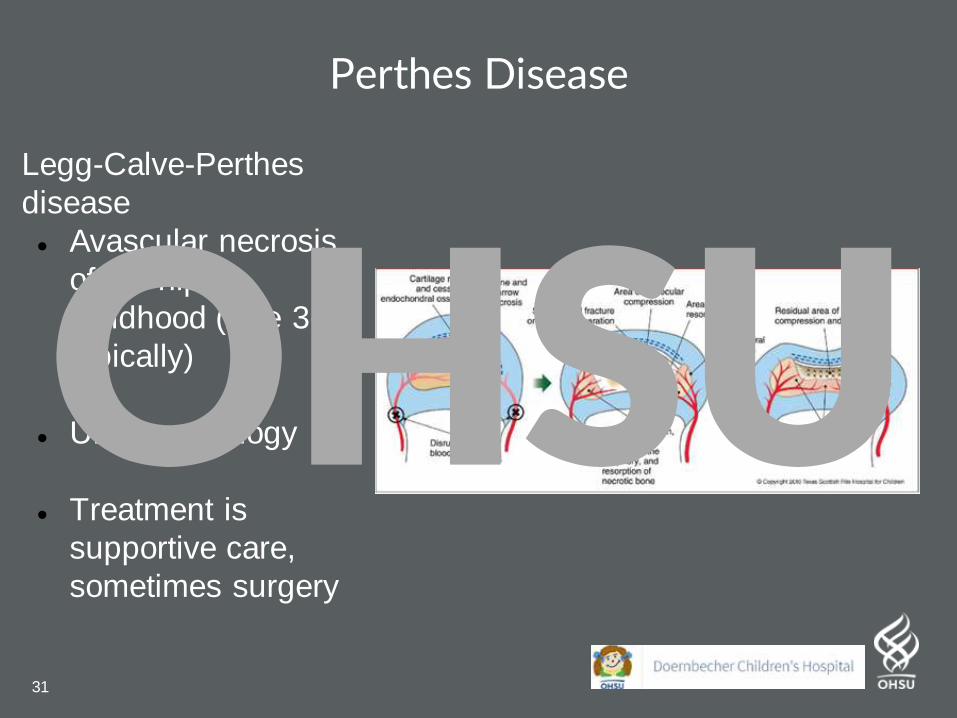
Perthes Disease
Legg-Calve-Perthes
disease
● Avascular necrosis
of the hip in
childhood (Age 3-9
typically)
● Unclear etiology
● Treatment is
supportive care,
sometimes surgery
OHSU
32
Perthes Disease – Case ExampleHPI:
5 year old male presents with
intermittent limping, and mild hip pain
for past 6 months. No fevers/malaise.
Able to jog with a limp
-Otherwise plays well, can go to school,
no malaise
PEX:
Well appearing
Slight trendelenburg limp
Difficulty running / jumping
Slightly decreased left hip abduction
range of motion
OHSU
33
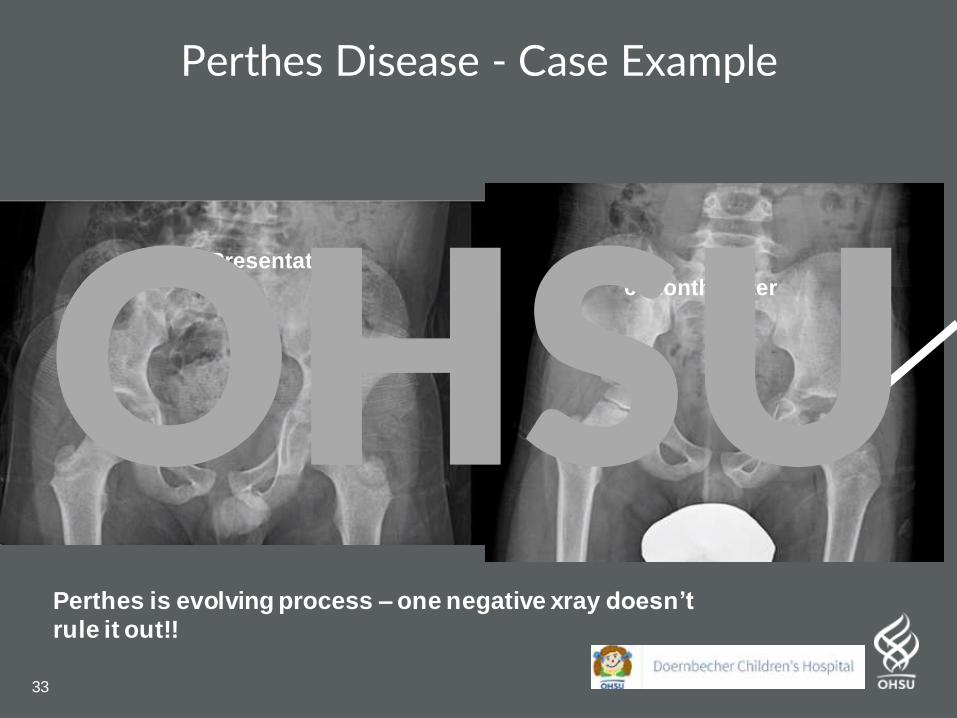
Perthes Disease - Case Example
6 months later
Initial Presentation
Perthes is evolving process – one negative xray doesn’t
rule it out!!
OHSU
34
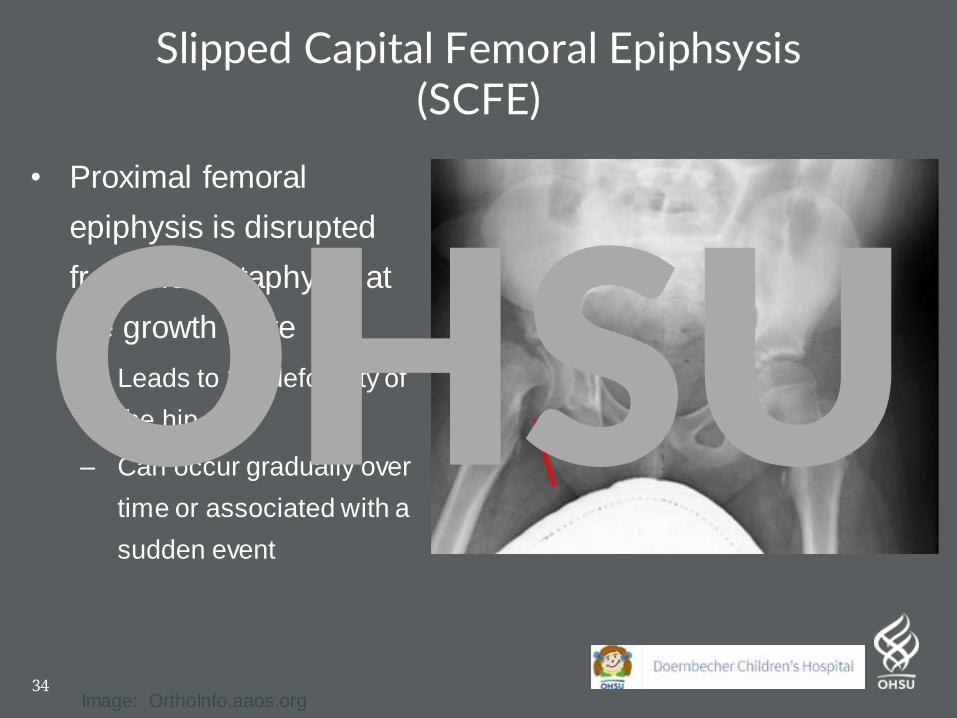
Slipped Capital Femoral Epiphsysis(SCFE)
• Proximal femoral
epiphysis is disrupted
from the metaphysis at
the growth plate
– Leads to 3D deformity of
the hip
– Can occur gradually over
time or associated with a
sudden event
Image: OrthoInfo.aaos.org
OHSU
35
SCFE Epidemiology
• Age 9-13
• 10.8/100,000 children
annually in USA
• Associated with obesity
– >50% of SCFE patients are
>95th percentile for weight
OHSU
36
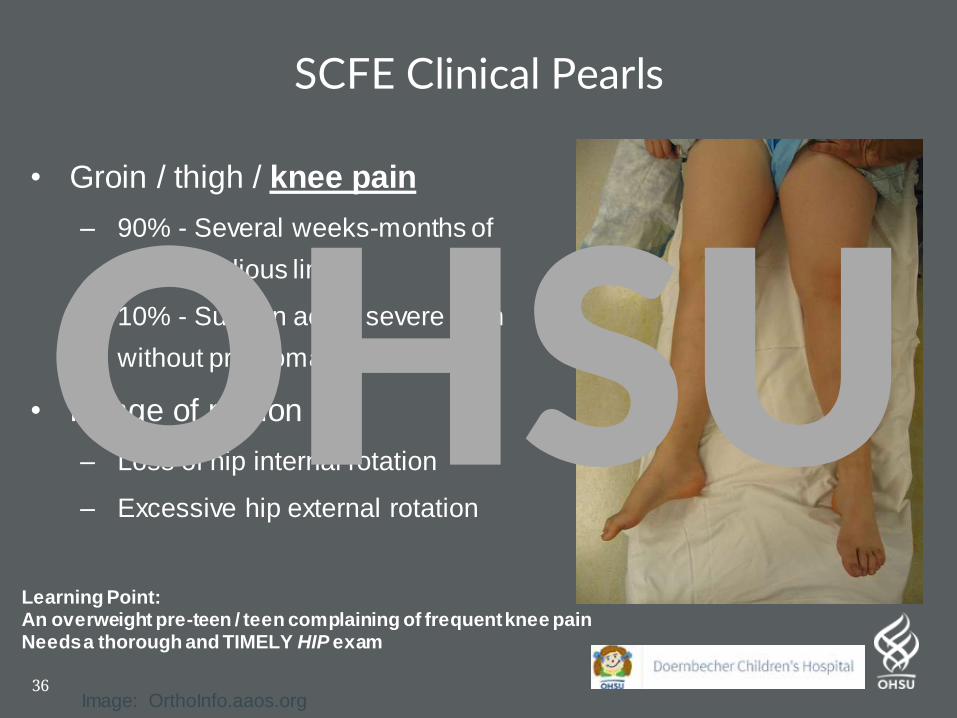
SCFE Clinical Pearls
• Groin / thigh / knee pain
– 90% - Several weeks-months of
pain, insidious limp
– 10% - Sudden acute severe pain
without prodromal symptoms
• Range of motion
– Loss of hip internal rotation
– Excessive hip external rotation
Image: OrthoInfo.aaos.org
Learning Point: An overweight pre-teen / teen complaining of frequent knee painNeeds a thorough and TIMELY HIP exam
OHSU
37
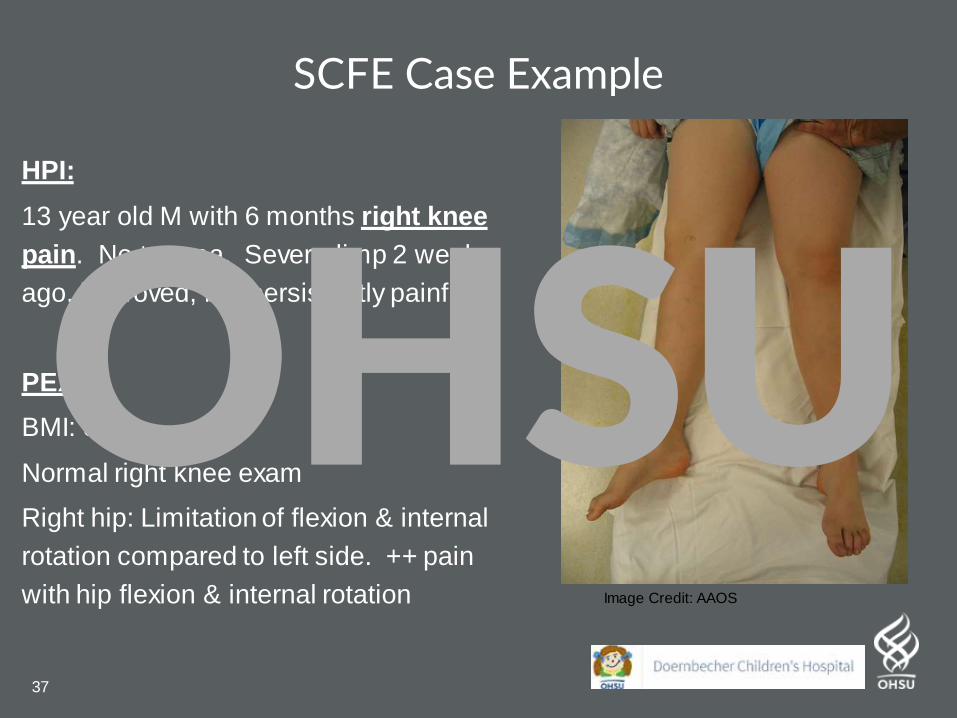
SCFE Case Example
HPI:
13 year old M with 6 months right knee
pain. No trauma. Severe limp 2 weeks
ago, improved, but persistently painful
PEX:
BMI: 31
Normal right knee exam
Right hip: Limitation of flexion & internal
rotation compared to left side. ++ pain
with hip flexion & internal rotation Image Credit: AAOS
OHSU
38
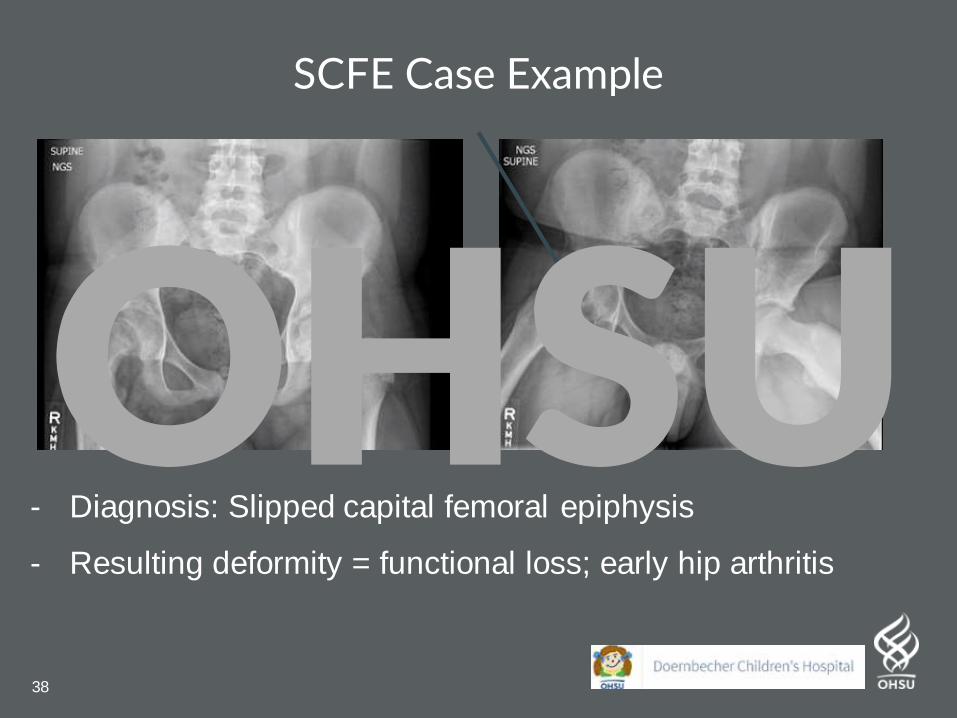
SCFE Case Example
- Diagnosis: Slipped capital femoral epiphysis
- Resulting deformity = functional loss; early hip arthritis
OHSU
39
The SpineOHSU
40
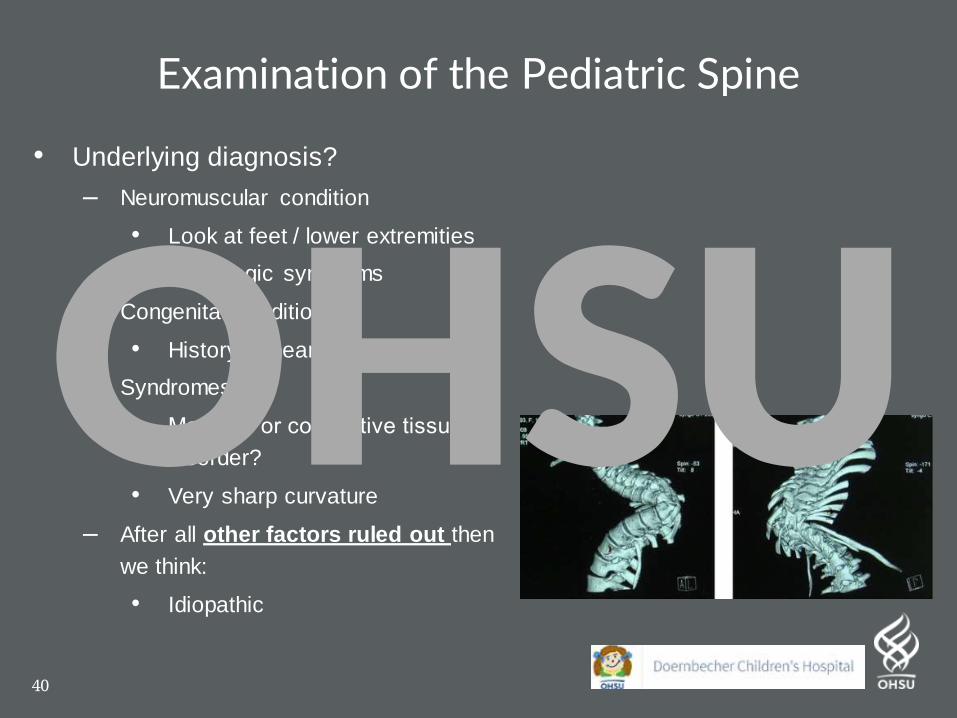
Examination of the Pediatric Spine
• Underlying diagnosis?
– Neuromuscular condition
• Look at feet / lower extremities
• Neurologic symptoms
– Congenital conditions
• History of heart / renal problems?
– Syndromes
• Marfan’s or connective tissue
disorder?
• Very sharp curvature
– After all other factors ruled out then
we think:
• Idiopathic
OHSU
41
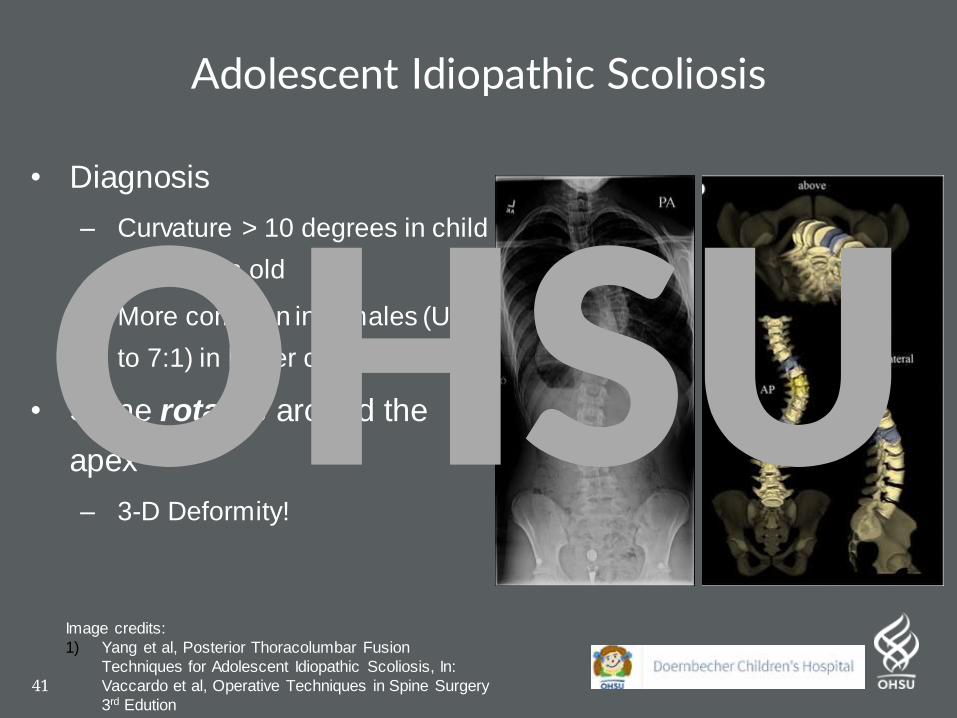
Adolescent Idiopathic Scoliosis
• Diagnosis
– Curvature > 10 degrees in child
> 10 years old
– More common in females (Up
to 7:1) in larger curves
• Spine rotates around the
apex
– 3-D Deformity!
Image credits:
1) Yang et al, Posterior Thoracolumbar Fusion
Techniques for Adolescent Idiopathic Scoliosis, In:
Vaccardo et al, Operative Techniques in Spine Surgery
3rd Edution
OHSU
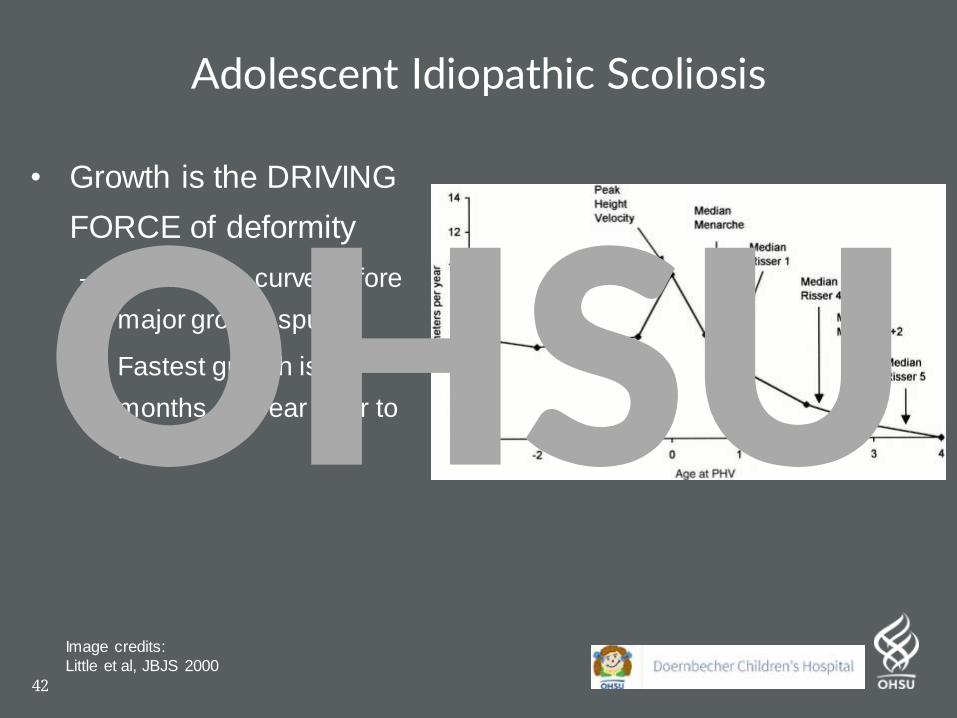
42
• Growth is the DRIVING
FORCE of deformity
– Control the curve before
major growth spurt
– Fastest growth is 6
months – 1 year prior to
menses
Adolescent Idiopathic Scoliosis
Image credits:
Little et al, JBJS 2000
OHSU
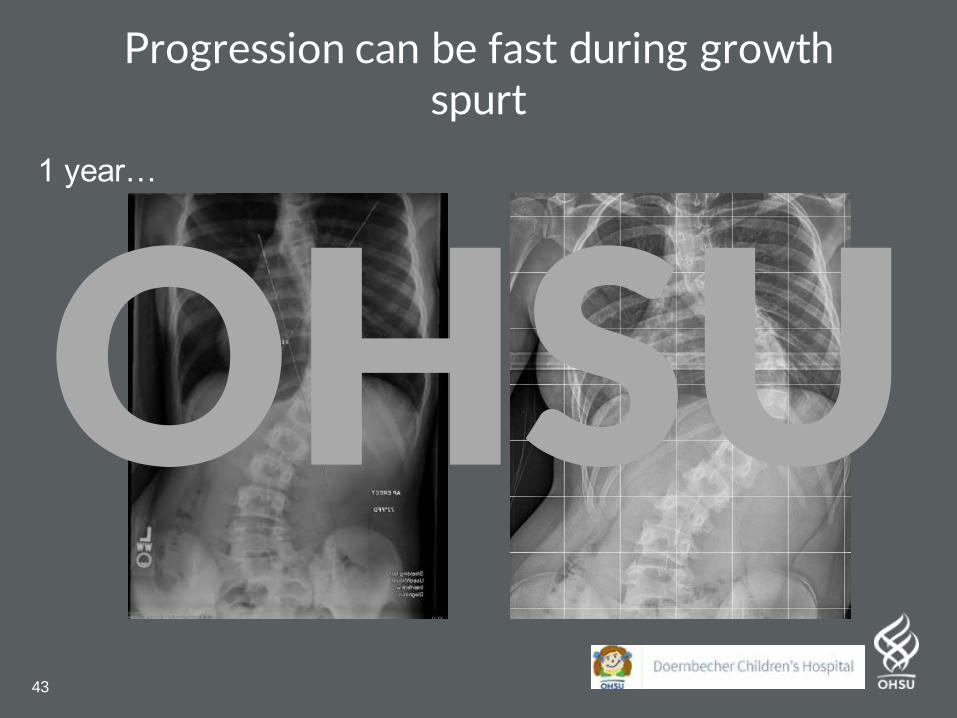
43
Progression can be fast during growth spurt
1 year…
OHSU
44
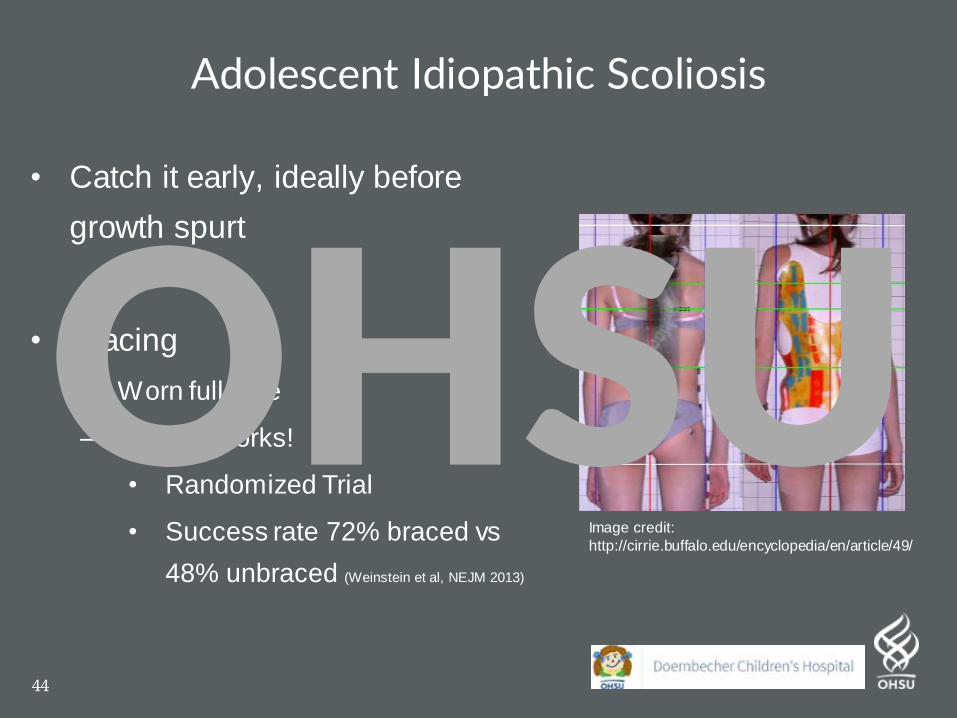
• Catch it early, ideally before
growth spurt
• Bracing
– Worn full time
– Bracing works!
• Randomized Trial
• Success rate 72% braced vs
48% unbraced (Weinstein et al, NEJM 2013)
Adolescent Idiopathic Scoliosis
Image credit:
http://cirrie.buffalo.edu/encyclopedia/en/article/49/
OHSU
The Adolescent AthleteOHSU
46
The Adolescent Athlete
Sporting or activity demands
may lead to stress injuries
- Year-round sports
common
- More competition /
intensityImage Credit: LariatonlineOHSU
47
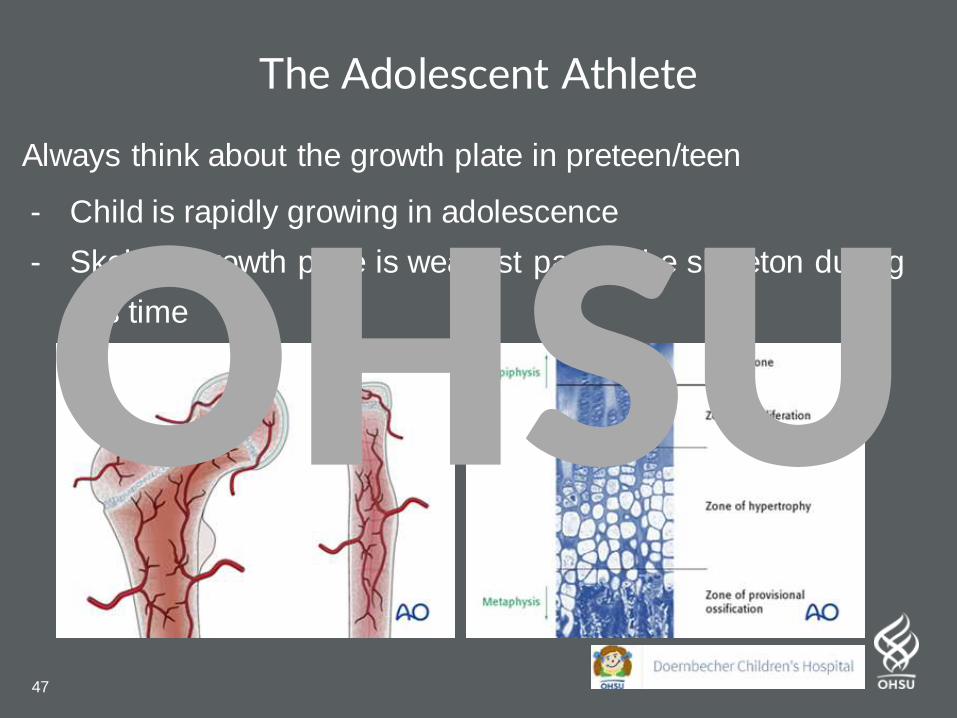
The Adolescent Athlete
Always think about the growth plate in preteen/teen
- Child is rapidly growing in adolescence
- Skeletal growth plate is weakest part of the skeleton during
this timeOHSU
48
Typical Case
HPI:
13 year old competitive soccer star
complains of activity related anterior
right > left knee pain
Worse with jumping or after soccer
practice
PEX:
- Tenderness along bilateral tibial
tubercle
- Pain with resisted knee extension,
pain with squat jumps
OHSU
49
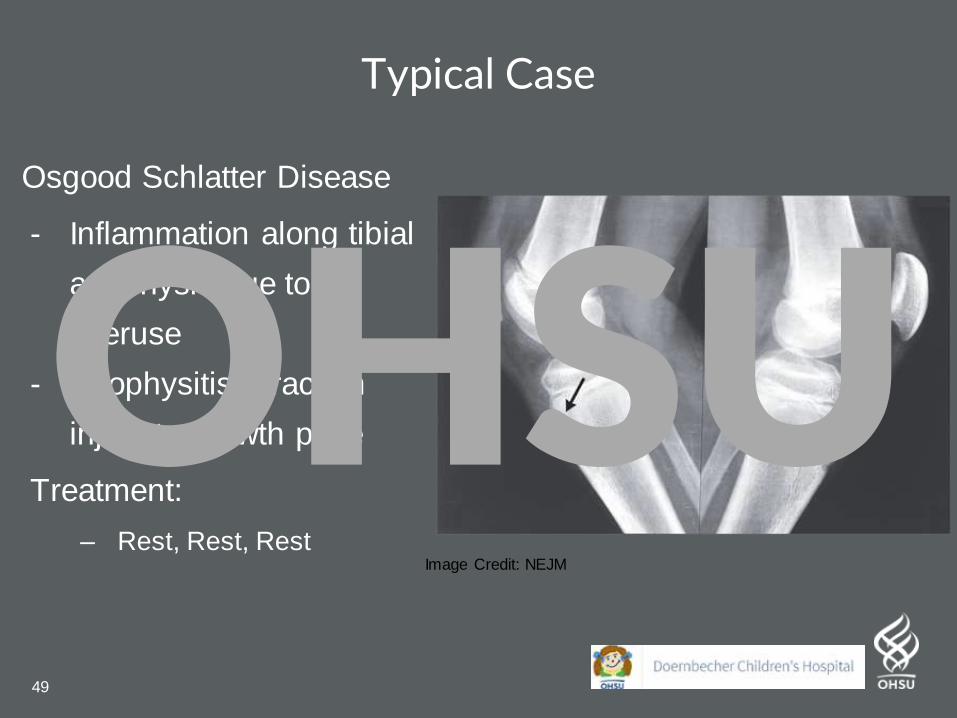
Typical Case
Osgood Schlatter Disease
- Inflammation along tibial
apophysis due to
overuse
- Apophysitis: Traction
injury to growth plate
Treatment:
– Rest, Rest, RestImage Credit: NEJM
OHSU
50
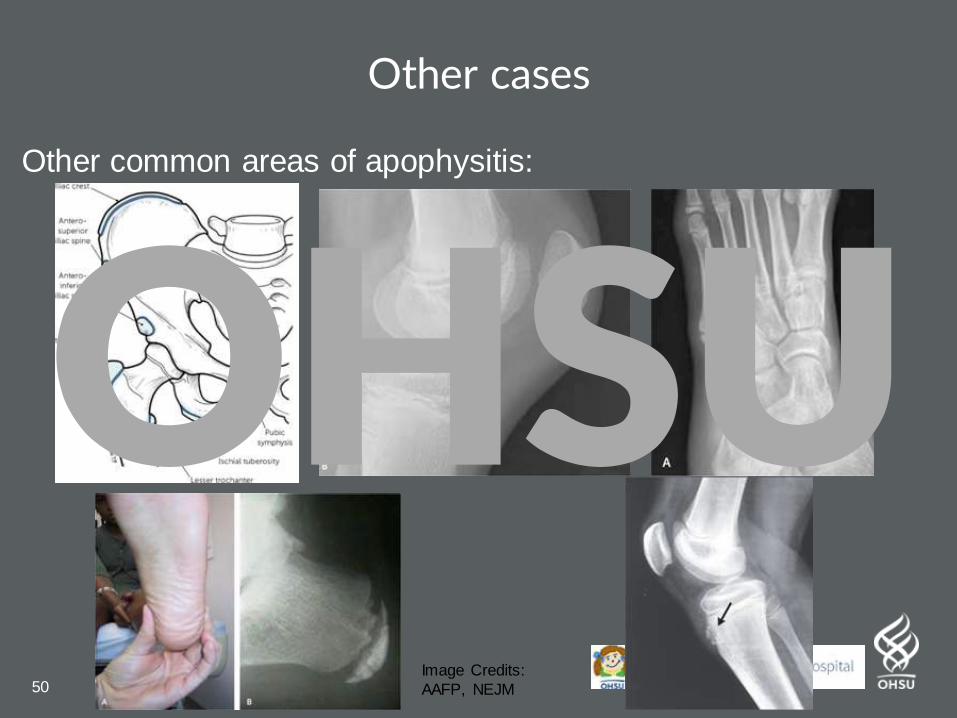
Other cases
Other common areas of apophysitis:
Image Credits:
AAFP, NEJM
OHSU
51
The Acutely Limping ChildOHSU
52
The Acutely Limping Child
– FIRST, rule out:
– Trauma
– (Fractures, growth plate injuries
including SCFE)
– Infection
– Can be from spine to foot!
– Tumor
Staying out of trouble =
don’t give up until you
find the causeOHSU
53
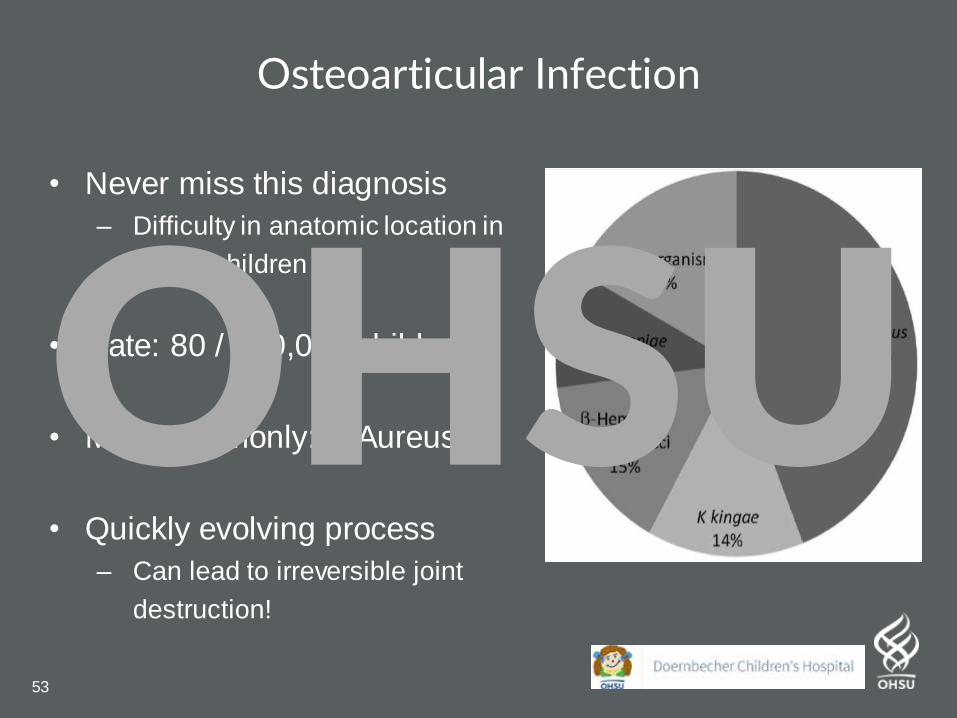
Osteoarticular Infection
• Never miss this diagnosis
– Difficulty in anatomic location in
young children
• Rate: 80 / 100,000 children
• Most commonly: S Aureus
• Quickly evolving process
– Can lead to irreversible joint
destruction!
OHSU
54
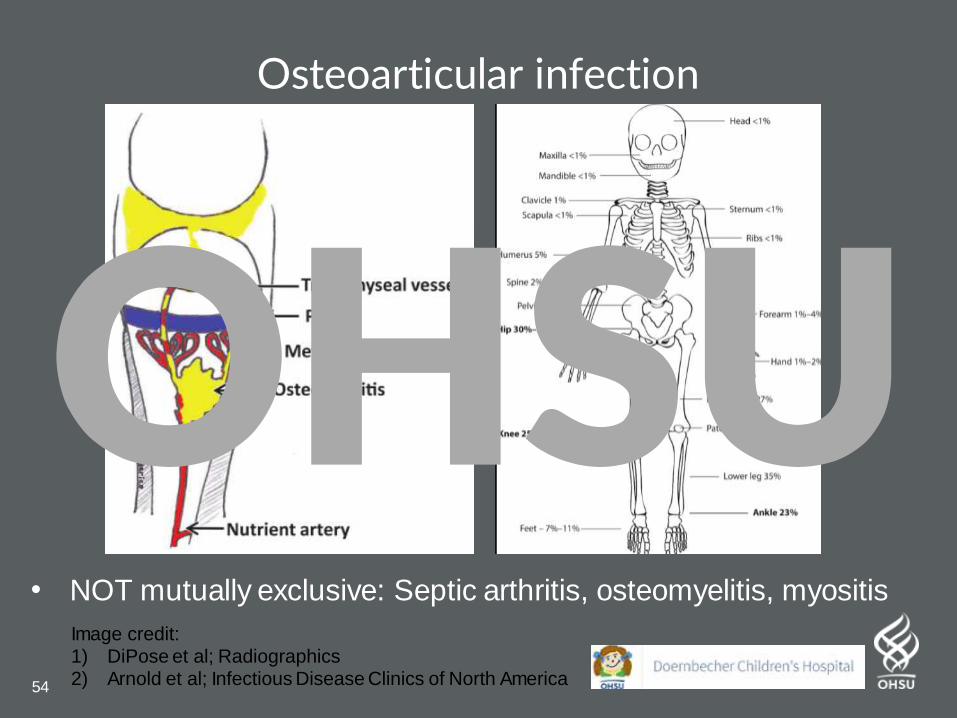
Osteoarticular infection
• NOT mutually exclusive: Septic arthritis, osteomyelitis, myositis
Image credit: 1) DiPose et al; Radiographics2) Arnold et al; Infectious Disease Clinics of North America
OHSU
55
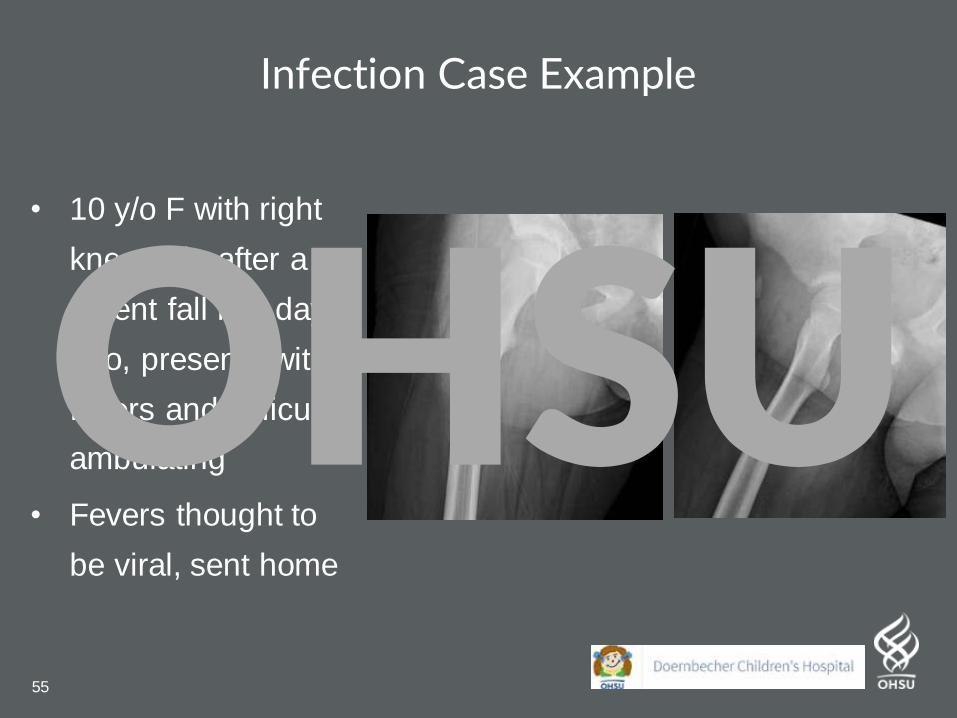
Infection Case Example
• 10 y/o F with right
knee pain after a
recent fall few days
ago, presents with
fevers and difficulty
ambulating
• Fevers thought to
be viral, sent home
OHSU
56
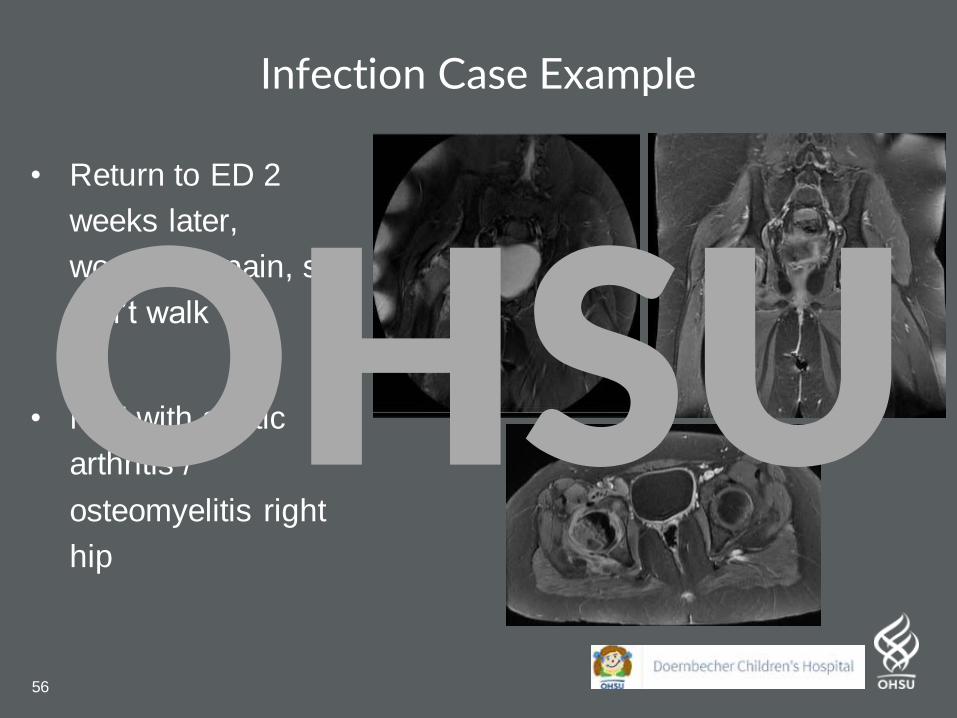
Infection Case Example
• Return to ED 2
weeks later,
worsening pain, still
can’t walk
• MRI with septic
arthritis /
osteomyelitis right
hip
OHSU
57
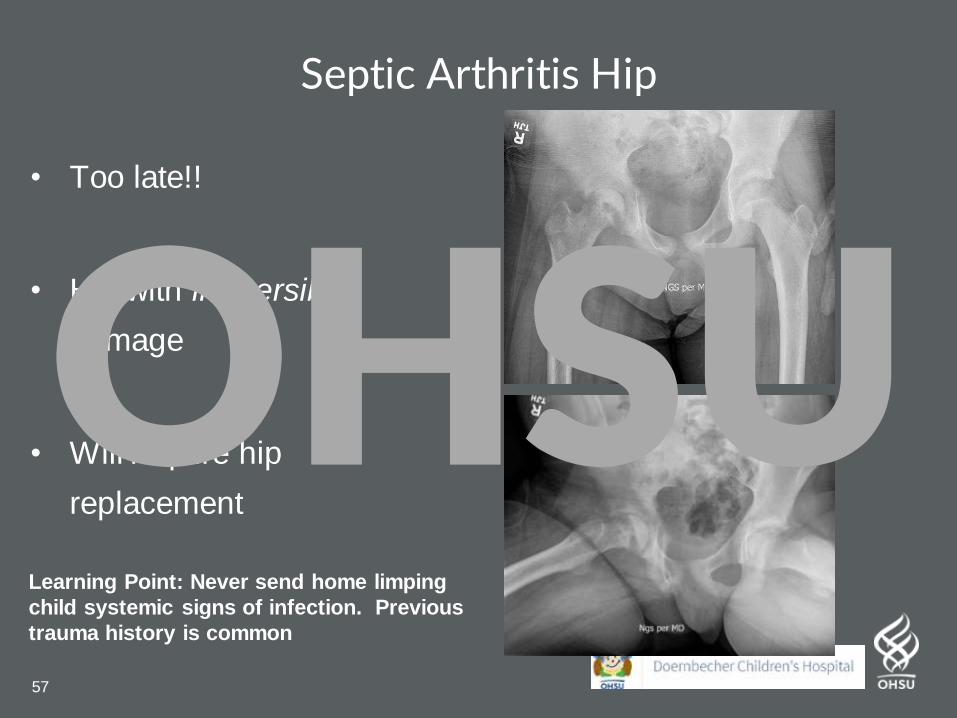
Septic Arthritis Hip
• Too late!!
• Hip with irreversible
damage
• Will require hip
replacement
Learning Point: Never send home limping
child systemic signs of infection. Previous
trauma history is common
OHSU
58
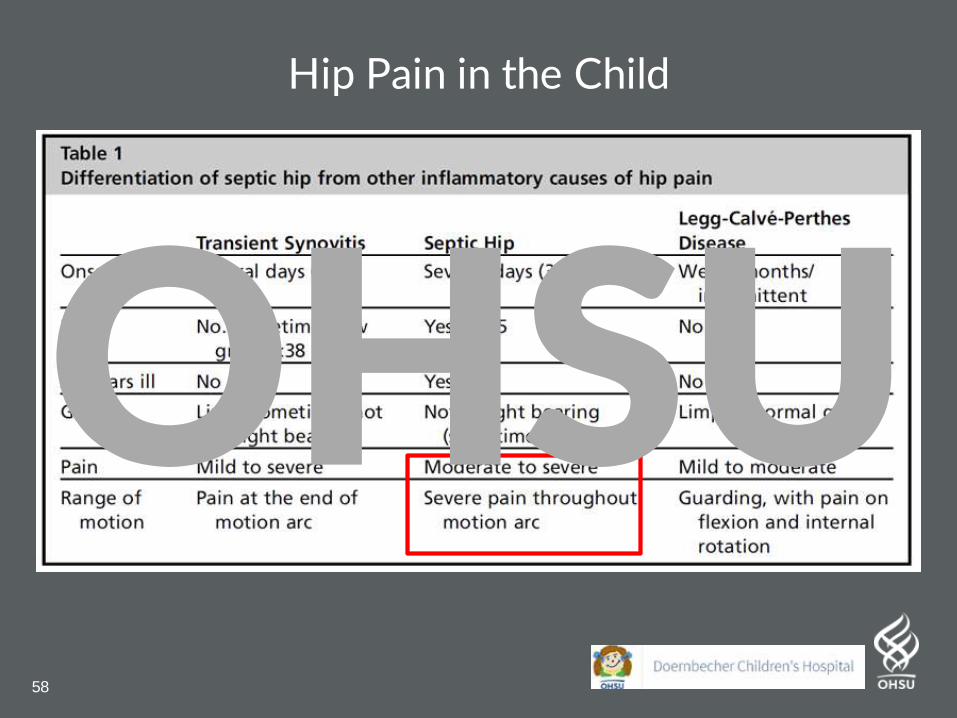
Hip Pain in the Child
OHSU
59
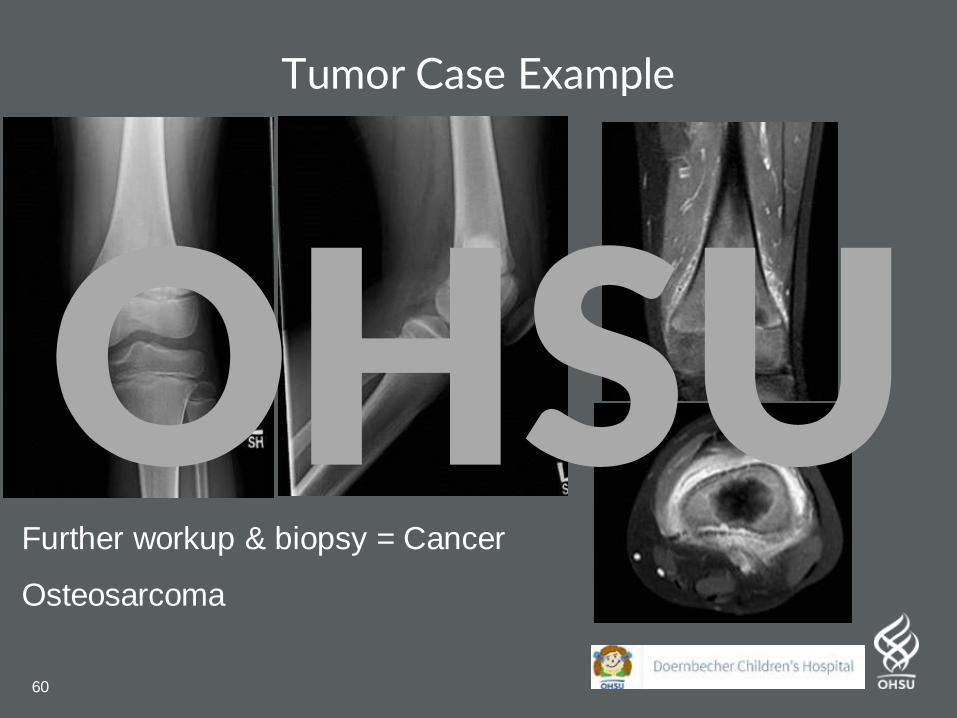
Tumor Case Example
HPI:
10 y/o M with 1 month left atraumatic knee pain. Hurts at rest,
wakes him at night, and painful every time he walks.
PEX:
Full range of motions left knee, no palpable masses
Antalgic gait, walks with clear limp
Learning Point: Persistent pain, frequent night pain, that is ALWAYS reproduceable, with limping = something is wrong!!
OHSU
60
Tumor Case Example
Further workup & biopsy = Cancer
Osteosarcoma
OHSU

61
Fractures / Injuries: Casting & SplintingOHSU
62
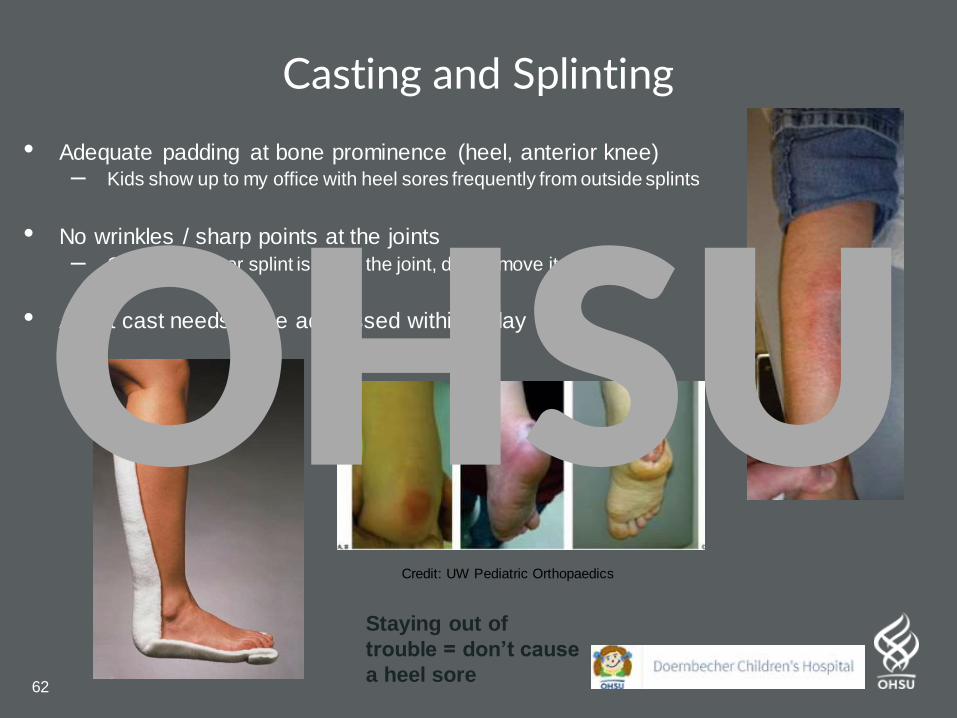
Casting and Splinting
• Adequate padding at bone prominence (heel, anterior knee)– Kids show up to my office with heel sores frequently from outside splints
• No wrinkles / sharp points at the joints
– Once the cast or splint is set at the joint, do not move it anymore!
• A wet cast needs to be addressed within a day
Credit: UW Pediatric Orthopaedics
Staying out of
trouble = don’t cause
a heel sore
OHSU
63
Fractures / Injuries: Do NOT miss these injuriesOHSU
64
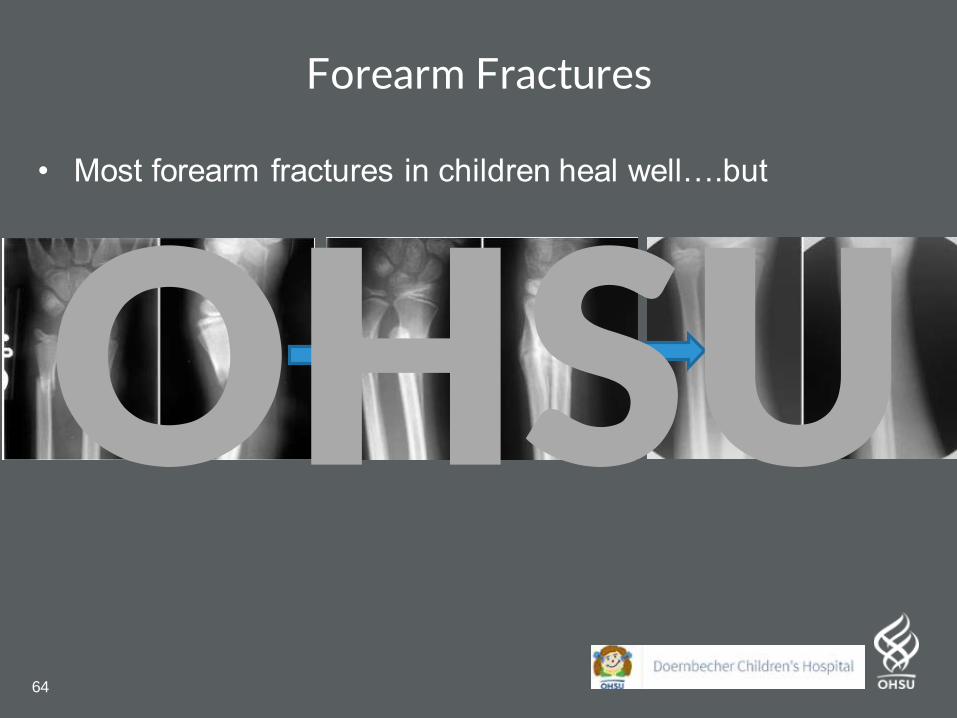
Forearm Fractures
• Most forearm fractures in children heal well….but
OHSU
65
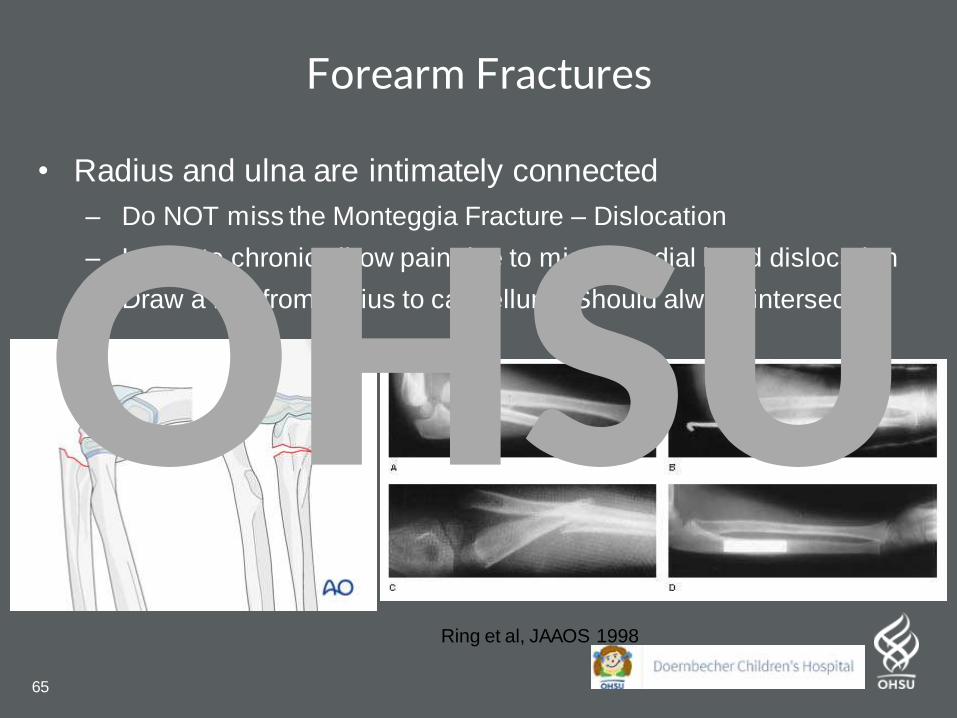
Forearm Fractures
• Radius and ulna are intimately connected
– Do NOT miss the Monteggia Fracture – Dislocation
– Leads to chronic elbow pain due to missed radial head dislocation
– Draw a line from radius to capitellum. Should always intersect.
Ring et al, JAAOS 1998
OHSU
66
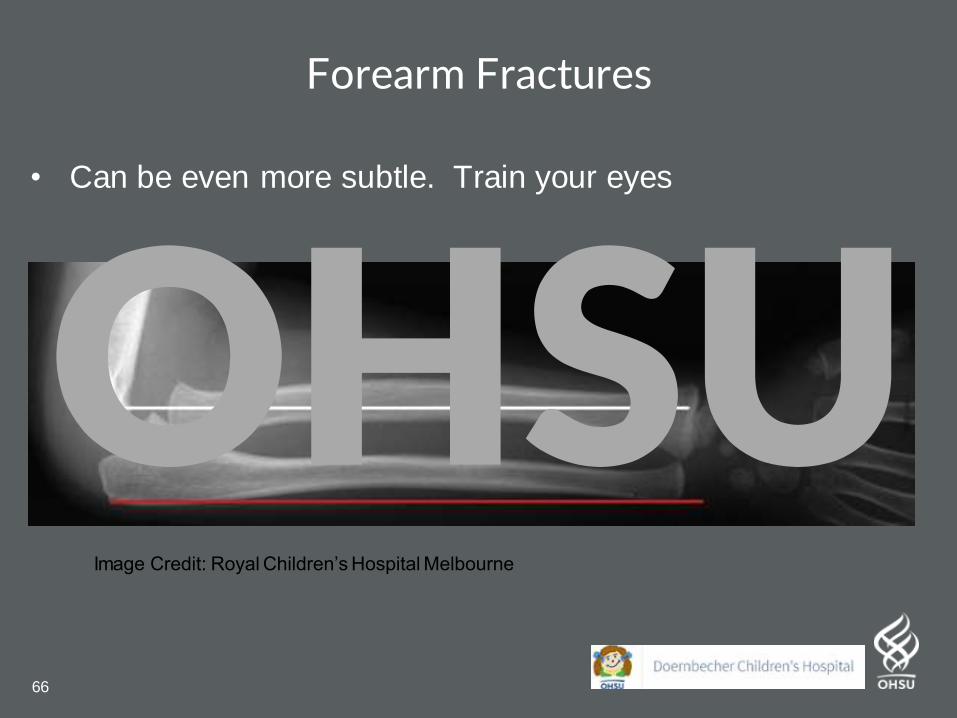
Forearm Fractures
• Can be even more subtle. Train your eyes
Image Credit: Royal Children’s Hospital Melbourne
OHSU
67
• Supracondylar humerus
fracture
– Most common elbow
fracture in children
– Can be very severe with
regards to loss of limb
function
Supracondylar Humerus Fractures
OHSU
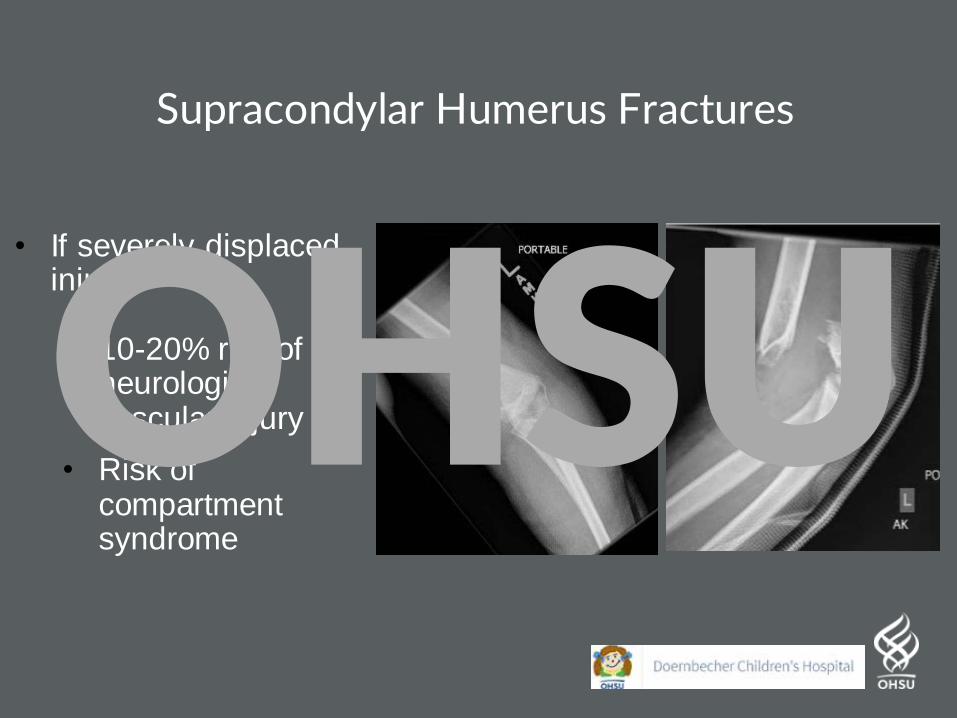
Supracondylar Humerus Fractures
• If severely displaced injury:
• 10-20% risk of neurologic / vascular injury
• Risk of compartment syndrome
OHSU
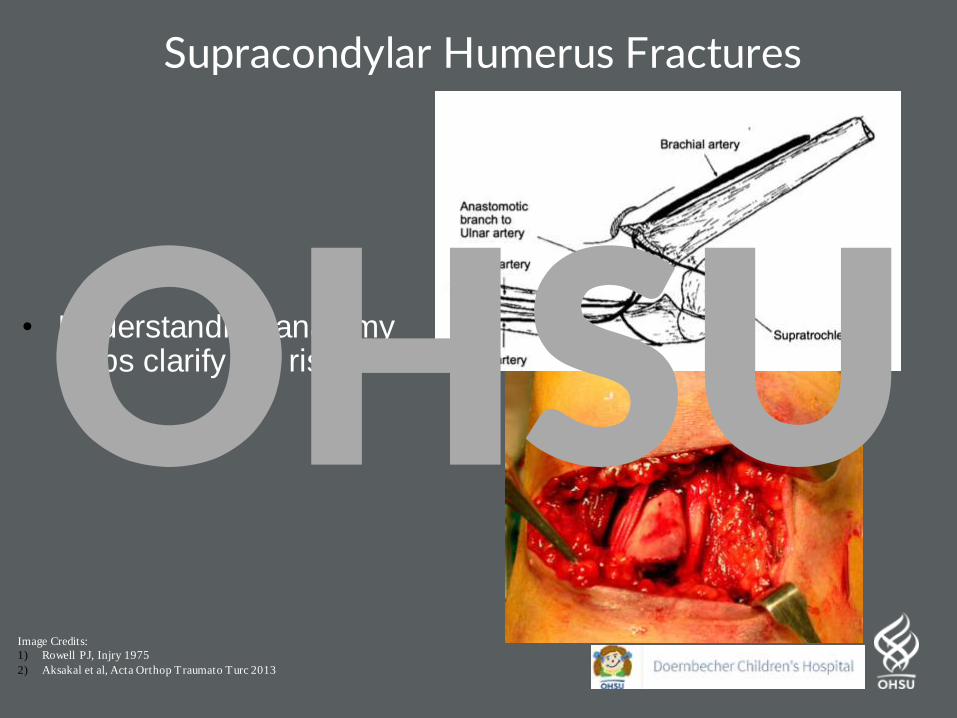
Supracondylar Humerus Fractures
Image Credits:
1) Rowell PJ, Injry 1975
2) Aksakal et al, Acta Orthop Traumato Turc 2013
• Understanding anatomy helps clarify the riskOHSU

Be on alert if you see this!!
OHSU
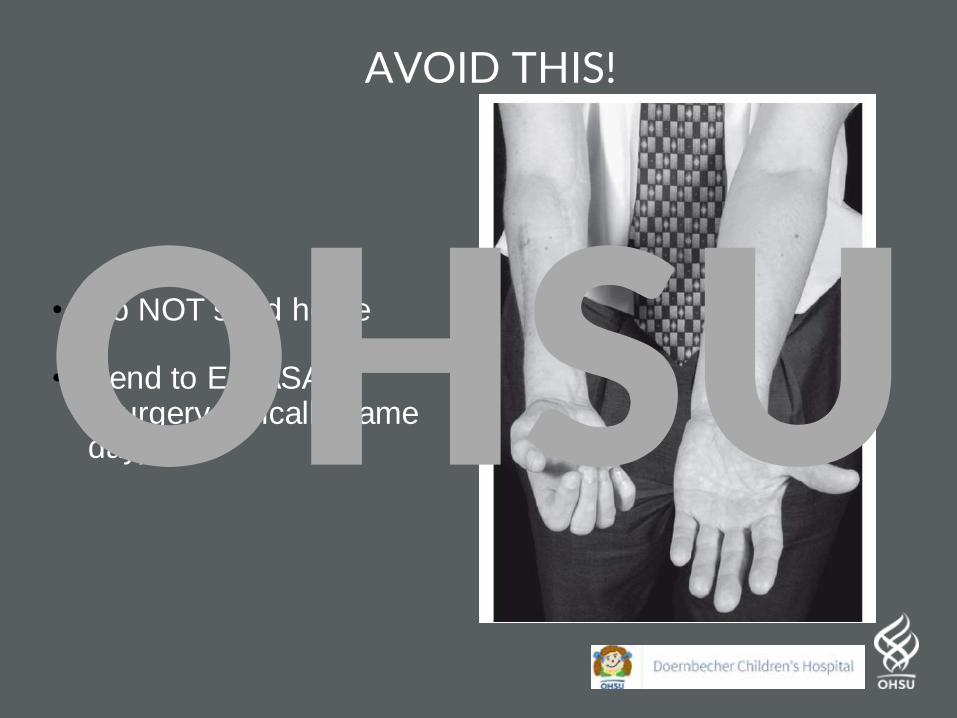
AVOID THIS!
• Do NOT send home
• Send to ED ASAP (Surgery typically same day)OHSU

Fractures / Injuries: Preventative Guidance
Please help prevent catastrophiesOHSU
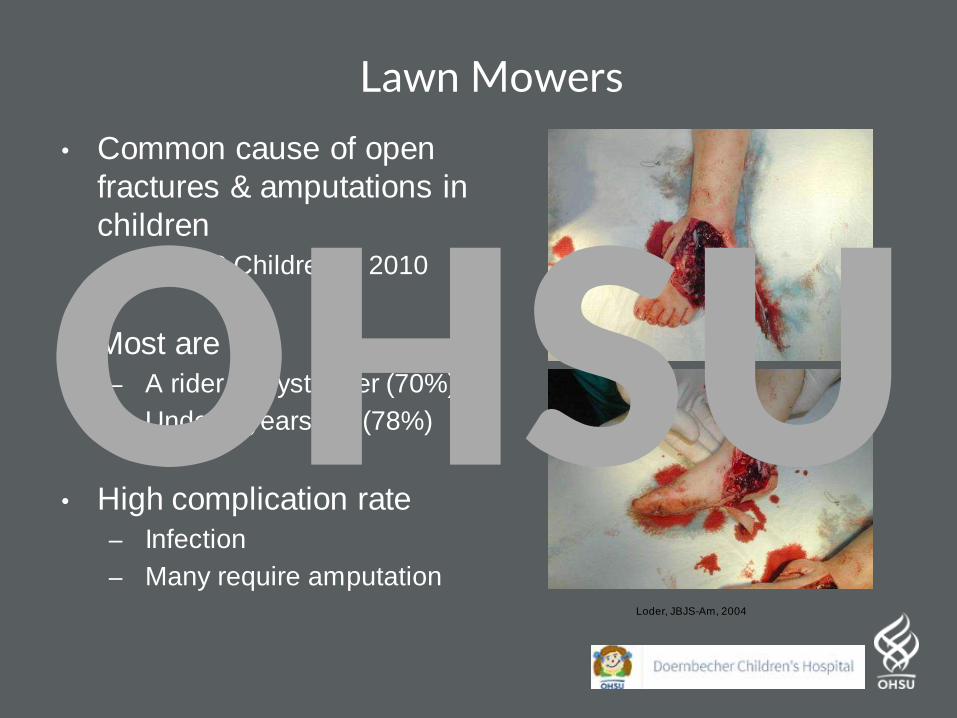
Lawn Mowers
• Common cause of open
fractures & amputations in
children
– 17,000 Children in 2010
• Most are
– A rider or bystander (70%)
– Under 5 years old (78%)
• High complication rate
– Infection
– Many require amputationLoder, JBJS-Am, 2004
OHSU
Lawn Mowers
• Tell your patients:
– Children < 14 should NOT operate power lawn mowers
– No riders other than the operator in a riding mower
– Secure lawn mowers in safe place, AWAY from children
– Caution with hills/slopes, especially when wet
OHSU
Trampolines
• AAOS Guidelines– No one under 6
– Always netted
– Always adult supervision
– One participant at a time
– Somersaults or high-risk maneuvers avoided
– Trampoline-jumping surface should be placed at ground level.
– Well padded bars
– Checked regularly
OHSU

Window Safety
• >5,000 falls from windows yearly– Age < 5 years old
– Serious head injuries / skeletal injuries
• No play near windows
• No furniture near by
• Install window stops / guards to limit opening to 4 inches
• Screens are not safety guards
OHSU
Thank YouOHSU