Embed Size (px)
Citation preview

University of Kentucky University of Kentucky
UKnowledge UKnowledge
DNP Projects College of Nursing
2018
Does a Nonstandardized Lactulose Administration Practice affect Does a Nonstandardized Lactulose Administration Practice affect
Hepatic Encephalopathy in Patients with Liver Disease in the Hepatic Encephalopathy in Patients with Liver Disease in the
Acute Care Setting? Acute Care Setting?
Mary Broadbent [email protected]
Right click to open a feedback form in a new tab to let us know how this document benefits you. Right click to open a feedback form in a new tab to let us know how this document benefits you.
Recommended Citation Recommended Citation Broadbent, Mary, "Does a Nonstandardized Lactulose Administration Practice affect Hepatic Encephalopathy in Patients with Liver Disease in the Acute Care Setting?" (2018). DNP Projects. 223. https://uknowledge.uky.edu/dnp_etds/223
This Practice Inquiry Project is brought to you for free and open access by the College of Nursing at UKnowledge. It has been accepted for inclusion in DNP Projects by an authorized administrator of UKnowledge. For more information, please contact [email protected].

Running head: LACTULOSE ADMINISTRATION
i
DNP Final Project
Does a Nonstandardized Lactulose Administration Practice affect Hepatic Encephalopathy in Patients with Liver Disease in the Acute Care Setting?
Mary B Broadbent
University of Kentucky
College of Nursing
Fall 2018
Melanie Hardin-Pierce DNP, APRN, ACNP-BC – Committee Chair
Karen Butler DNP, RN- Committee Member
Whitney Kirkpatrick, Pharm-D– Committee Member/Clinical Mentor

LACTULOSE ADMINISTRATION
ii
Dedication
This DNP project is dedicated to my husband and my children. My husband’s support
during my school career has been tremendous. For as long as I have known him, he has always
pushed me to do my best and be my best. He has supported me through the ups and the downs
during the last 4.5 years and he has always been there for me. He has given me the
encouragement to succeed in the program. I want to show my children that hard work is an
important quality to have in life and to never give up. I hope that I can show them that they
should always follow their dreams and goals in life, no matter what life throws them or
challenges that may come in their way. There is never an excuse for lack of time for anything in
life.
LACTULOSE ADMINISTRATION
iii
Acknowledgements
I would like to acknowledge my committee chair, Melanie Hardin-Pierce. She has been a
great resource to have for my time in the program and for this project. She has offered me
support and has guided me down the right path during the past 4.5 years. Her guidance for this
project has been very helpful and she has always provided a constant foundation for growth as I
transition from an RN to a DNP.
I would also like to acknowledge Karen Butler and Whitney Kirkpatrick who both served
as committee members on my project. They have supported me through the process of this
project and have been there for any problems/concerns. Lastly, I wanted to acknowledge
Amanda Wiggins for help on the statistical part of this study. She spent a lot of time helping me
with this paper and her knowledge has impacted my project greatly.

LACTULOSE ADMINISTRATION
iv
Table of Contents
Acknowledgements ........................................................................................................................ iii
List of Tables ................................................................................................................................. vi
Abstract ........................................................................................................................................... 1
Introduction ..................................................................................................................................... 3
Background ..................................................................................................................................... 6
Purpose .......................................................................................................................................... 10
Methods......................................................................................................................................... 11
Setting ........................................................................................................................................ 11
Sample ....................................................................................................................................... 12
Data Collection .......................................................................................................................... 12
Data Analysis ............................................................................................................................. 13
Results ........................................................................................................................................... 14
Sample Characteristics .............................................................................................................. 14
Bowel Movements ..................................................................................................................... 14
MELD Score .............................................................................................................................. 14
GCS Score ................................................................................................................................. 15
Discussion ..................................................................................................................................... 15
Limitations……………………………………………………………………………..………16
Recommendations for Future Studies ........................................................................................ 17
Conclusion .................................................................................................................................... 18

LACTULOSE ADMINISTRATION
v
References ..................................................................................................................................... 20

LACTULOSE ADMINISTRATION
vi
List of Tables
Table 1. List of Variables per Category ........................................................................................ 23
Table 2. Narcotics Administered in this Study .............................................................................. 24
Table 3.Demographics of patients in this study. (N=70)………………………………………………………..….….24
Table 4. Percentage of patients who met the goal of 2-4 bowel movements (BMs) each day for
the first five days of hospitalization…………………………………………………………..….24
Table 5: Chi square: Percentage of patients with a MELD score of ³ 25 who met the goal of 2-4
BM’s per day, received a PRN dose of lactulose, received a lactulose enema, and received a
narcotics each day for the first five days of hospitalization…………………………………..…25
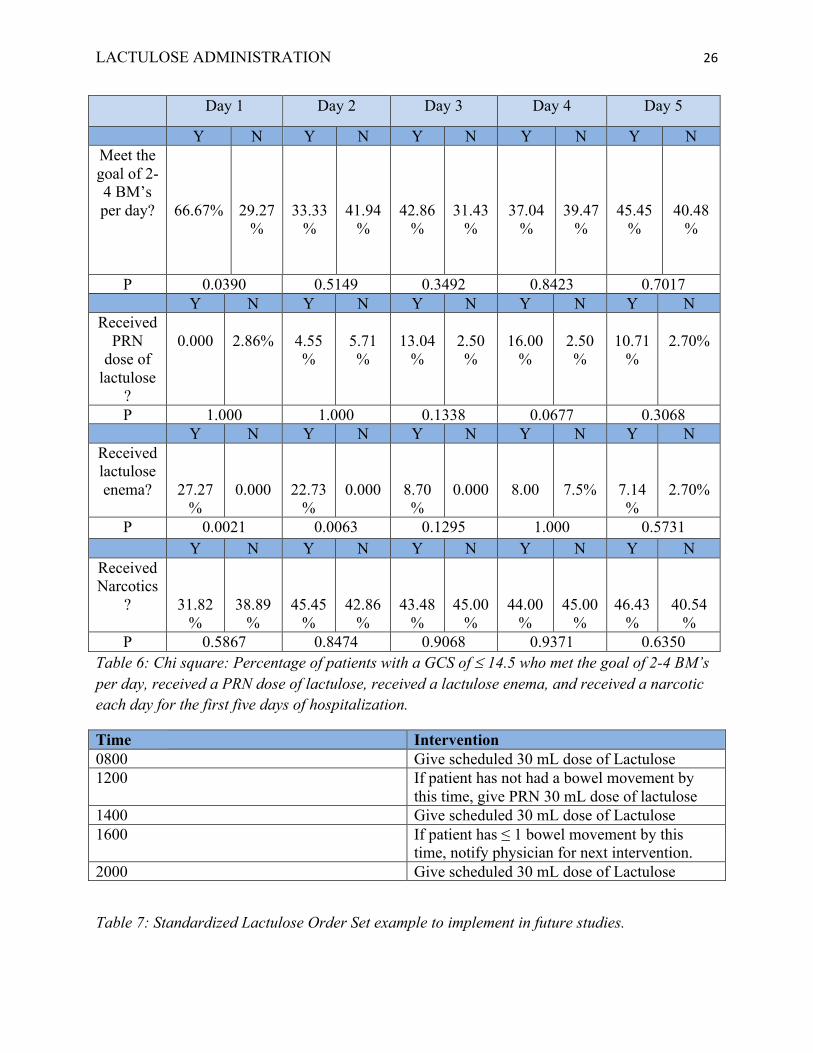
Table 6: Chi square: Percentage of patients with a GCS of £ 14.5 who met the goal of 2-4 BM’s
per day, received a PRN dose of lactulose, received a lactulose enema, and received a narcotic
each day for the first five days of hospitalization……………………………………………..…26
Table 7: Standardized Lactulose Order Set example to implement in future studies…….……..26

Running head: LACTULOSE ADMINISTRATION
1
Abstract
PURPOSE: The purpose of this study is to examine whether inpatients with liver disease at
University of Kentucky Hospital receiving lactulose are meeting the protocol of 2-4 bowel
movements per day. Research shows that lactulose is the medication of choice used to treat and
prevent hepatic encephalopathy (HE). Additional lactulose interventions, a patient’s MELD
score, and GCS score will be examined in this study as well. This information would be
beneficial to providers and nurses because it would provide data on patients who might require
more lactulose interventions than others.
METHODS: Retrospective chart reviews of 70 inpatients with liver disease receiving lactulose at
the University of Kentucky from January 1, 2017 to December 31, 2017 were performed.
Number of daily movements, MELD score, GCS score, PRN lactulose administration, lactulose
enema administration, and narcotic administration were examined during the first five days of
hospitalization.
RESULTS: In the sample, a higher percentage of patients (>50%) did not meet the protocol of 2-
4 daily bowel movements during the first five days of hospitalization. There was no association
shown for patients who had a higher MELD score ≥ 25 on whether or not they met the goal of 2-
4 bowel movements per day or received additional lactulose interventions. Those who had a
GCS of ≤ 14.5 were more likely to receive lactulose enemas on day 1 and 2 (p=0.0021, 0.0063)
and no significance was shown for the remaining days or PRN lactulose. Narcotic administration
did not affect this group, as there was no association shown between GCS and narcotic
administration.
CONCLUSIONS: More than 50% of patients were not meeting the goal of 2-4 daily bowel
movements during the first five days of hospitalization. Those who are confused seem to require

LACTULOSE ADMINISTRATION 2
additional lactulose during the early initial days of hospitalization. This information can help
nurses and physicians better understand lactulose titration and administration in the hospital
setting.

LACTULOSE ADMINISTRATION 3
Does a Nonstandardized Lactulose Administration Practice affect Hepatic Encephalopathy in Patients with Liver Disease in the Acute Care Setting?
Introduction
Liver disease is prevalent in the United States. In 2015, the number of adults diagnosed
with liver disease was 3.9 million (Centers for Disease Control and Prevention [CDC], 2017). In
2014, there were 38,170 deaths from liver disease (CDC, 2017). In the state of Kentucky, liver
disease falls in the top fifteen causes of death for patients aged 45 to 75 (Kentucky Life
Expectancy, 2017).
According to the American Liver Foundation (2017), over 17,000 Americans are on the
waiting list for a liver transplant. A patient’s Model for End-Stage Liver Disease (MELD) score
helps prioritize patients who are waiting for a liver transplant. The MELD score is numeric scale
that ranges from 6 (less ill) to 40 (severely ill) and the score determines how urgent the liver
transplant is needed within the next three months (Sutter Health, 2014). The Liver Specialists of
Texas (2011) stated that the higher the MELD score, the more ill the patient is. Most transplant
programs are performing liver transplants with a MELD score of >25. The components utilized
to measure a MELD score include whether or not a patient has had dialysis twice in the past
week and the specific lab values: creatinine (Cr), total bilirubin, sodium (Na), and the
international normalized ratio (INR), (MD Calc, 2016). The MELD score has been validated
since 2001 and applied to numerous clinical situations (Tsang & Admed, 2013). Since its
implementation, use of it has led to a sharp reduction in waiting list registrations and reduced
mortality on the liver transplant waiting list without affecting post-transplant outcomes (Tsang &
Admed, 2013).

LACTULOSE ADMINISTRATION 4
Patients with liver disease are at risk for developing hepatic encephalopathy (HE), which
causes changes in an individual’s mental status that can range from mild confusion to a comatose
state. Numerous factors contribute to the pathophysiology of HE, which plays a role in altering
the function of neuronal cells. The common agents that are thought to cause HE include
inflammatory cytokines, benzodiazepine-like compounds (i.e. gamma-amino butyric acid),
manganese deposition in the basal ganglia, and ammonia—the most studied agent. Ammonia, a
gut-derived nitrogenous toxin, is produced by bacterial metabolism of urea from proteins
ingested from an individual’s diet. The liver metabolizes ammonia and it is cleared by the
kidneys. When patients have liver damage, the metabolism of ammonia is impaired. Portal
hypertension causes shunting of ammonia rich blood to the systemic circulation without
detoxification. Ammonia crosses the blood brain-barrier and is metabolized in the astrocytes by
glutamine synthetase. As a result, ammonia and glutamate are converted to glutamine. The
increase of glutamine in the brain causes an osmotic gradient that produces astrocyte swelling
and generation of reactive oxygen species, which plays role in the cerebral dysfunction
associated with HE. (Elwir & Rahimi, 2017)
Diagnosis of HE can be challenging and tends to be a clinical diagnosis (Elwir & Rahimi,
2017). There are numerous tools that can be used to help diagnose HE including the West Haven
Criteria, the International Society for Hepatic Encephalopathy and Nitrogen Metabolism
(ISHEN), Full Outline of Unresponsiveness (FOUR), the Glascow Coma Scale (GCS), Hepatic
Encephalopathy Scoring Algorithm (HESA), Clinical Hepatic Encephalopathy Staging Scale
(CHESS), and the Spectrum of Neurocognitive Impairment in Cirrhosis (SONIC). The West
Haven Criteria is the most popular tool used for diagnosing HE. However, the GSC can be used
for individuals with severe encephalopathy. When diagnosing HE, a provider must rule out other

LACTULOSE ADMINISTRATION 5
causes such as medications, electrolyte disorders, infection, withdrawal, hypoglycemia, or
hypercapnia. (Hepatitis C Online)
HE treatment targets the gut bacteria due to the hyperammonia state in the body.
Lactulose, a nonabsorbable disaccharide, is used to prevent and treat HE. This drug is
metabolized by the colonic microbiota and forms short chains organic acids. The creation of an
acidic environment helps prevent the growth of ammonia producing bacteria and support the
growth of favorable microorganisms. In an acidic environment, ammonia converts to
ammonium, which is not absorbed and lowers the ammonia load. Lastly, the laxative effects of
lactulose help remove nitrogen-containing substances from the gastrointestinal tract. Lactulose
can be administered orally or rectally and needs to be titrated to a goal of 2-4 bowel
movements/day. (Elwir & Rahimi, 2017)
Lactulose is the drug of choice for preventing and treating HE. Research shows that
lactulose administration needs to be titrated for the patient to have 2-4 bowel movements a day.
In the hospital setting, some patients may not meet the goal of 2-4 bowel movements a day,
increasing their risk of becoming encephalopathic. Often times, an additional dose of lactulose or
a lactulose enema is ordered to promote a bowel movement. The purpose of this study is to
perform a retrospective chart review to examine whether or not inpatients with liver disease at
University of Kentucky Hospital receiving lactulose for liver disease etiologies are meeting the
protocol of 2-4 bowel movements per day. Additional lactulose interventions and a patient’s
MELD score and GCS score will be also be examined in this study. If these patients are not
meeting the protocol of 2-4 bowel movements per day, a standardized order set could be
beneficial in this patient population that would help improve nurse-provider communication
about titrating bowel movements to lactulose administration.

LACTULOSE ADMINISTRATION 6
This study is important because it will provide information regarding whether or not
patients with liver disease receiving lactulose are meeting the protocol of 2-4 bowel movements
per day in the hospital setting. Examining an individual’s MELD score could show that a higher
MELD score may require additional lactulose interventions. Examining an individual’s GCS
could show that a score ≤ 14.5 may require additional lactulose interventions. Providers at UK
hospital do not document the West Haven Criteria for diagnosing HE. Consequently, GCS will
be the variable used for assessing level of conscious (LOC) in this population because it is
assessed at least two times a day by the nursing staff at UK. This information would be
beneficial to providers because it would provide patients at risk for developing HE and those
who need more lactulose interventions than others.
Background
Lactulose is the primary drug used for preventing and treating HE in patients with liver
disease. HE occurs when ammonia levels rise due to diffuse brain edema and structural brain
injury resulting in neuronal dysfunction (Wijdicks, 2016). The rise of ammonia levels causes
mental status, behavioral, and motor changes (AACN, n.d.). Consequently, drug therapies to
prevent and treat HE are aimed toward lowering ammonia levels (Wijdicks, 2016). Lactulose
works by removing the nitrogen containing substances from the gastrointestinal tract and can be
given orally or rectally to achieve 2-4 bowel movements daily (Elwir & Rahimi, 2017). As a
result, ammonia is eliminated from the body through bowel movements. If an individual does not
have 2-4 bowel movements per day, ammonia levels can accumulate in the body and cause
mental status changes. The National Organization for Rare Disorders (2011) states that the exact
incidence of HE is unknown but it is most often associated with cirrhosis. The organization
found that 70% of individuals with cirrhosis develop symptoms of HE. In 2003, HE related

LACTULOSE ADMINISTRATION 7
hospitalizations cost over 930 million dollars (The Hepatology Center for Educational Expertise,
2012). Morgan, Jenkins-Johns, Radwan, Conway, and Currie (2014) found that HE increased the
mortality risk in patients with liver disease. The study found that in 551 patients with HE, 304
(55.2%) died during the follow up period.
Research indicates that lactulose is the gold standard of treatment for HE. A study by
Sharma, Sharma, Agrawal, and Sarin (2009) found that 19.6% of patients who were administered
lactulose suffered from HE while 46.8% of patients in the placebo group suffered from HE.
Sharma, Sharma, Agrawal, and Sarin (2012) showed that 6 (11%) out of 55 patients who
received lactulose developed HE while 14 (28%) out of 50 patients who did not receive lactulose
developed HE. This study also proved that lactulose improved minimal hepatic encephalopathy
(MHE) in 66% of patients who were given lactulose. Lactulose administration significantly
lowered abnormal neuropsychological tests, reduced the risk of no improvement, and decreased
the time to complete a number connection test when compared to a placebo or no intervention
(Luo, Li, Lu, & Cao, 2011). Similarly, Prasad et al. (2007) showed that the mean number of
neuropsychological tests decreased after a 3-month course of lactulose administration compared
to no lactulose treatment for 3 months. The mean number of abnormal psychometric tests
decreased significantly when patients were given lactulose compared to no lactulose
administration (Dhimen et al., 2000). The evidence shows that lactulose prevents HE from
occurring in patients with liver disease. Therefore, it is essential that all inpatients taking
lactulose are meeting the goal of 2-4 bowel movements per day.
When research was done about the role of lactulose and other drugs, most showed that
lactulose is the drug of choice of treatment for HE. Mittal, Sharma, Sharma, and Sarin (2011)
studied the effects of lactulose, probiotics, l-ornithine l-aspartate (LOLA) and no treatment on

LACTULOSE ADMINISTRATION 8
HE. They found that lactulose had the strongest results among the three interventions through
significance in neuropsychological test improvement, decreased blood ammonia levels, and the
SIP questionnaire (this tool assesses the effect of HE on daily functioning). Lactulose, either
alone or in combination with Rifaximin, is the treatment of choice for HE (Zhan & Stremmel,
2012). Tapper, Jiang, and Patwardhan (2015) examined the effects of existing and evolving
therapeutic treatment for HE and found that lactulose is the first line of therapy for HE compared
to other medications.
According to Kamath & Kim (2007), A patient’s MELD score can be used to predict survival
in patients with different levels of liver disease and their severity. MELD scores were initially
calculated to predict the patient survival rates following the placement of transjugular
intrahepatic portosystemic shunts (TIPS). However, the MELD score has become an acceptable
way to predict long-term survival in patients with cirrhosis, variceal bleeding, Hepatitis C-
cirrhosis, alcoholic hepatitis, fulminant hepatic failure, other chronic liver diseases, and hepatic
cellular carcinoma. MELD scores are also used for liver transplant purposes. According to the
United Network for Organ Sharing, the higher the MELD score, the more urgently a patient
needs a liver transplant. Patients with a higher MELD score will always be considered first
before those who have a lower MELD score, regardless of how long they have been on the
waiting list.
The GCS has been in healthcare since the 1980s. According to Nickson (2017), this scale is
the most widely recognized of all conscious level scoring systems in the world. The scale
measures the mental status of patients according to three categories: verbal response, motor
response, and eye response. For eye response, the patient is scored based on (1) no eye opening,
(2) eye opening to pain, (3) eye opening to verbal command, and (4) eyes opening

LACTULOSE ADMINISTRATION 9
spontaneously. For verbal response, the patient is scored based on (1) no verbal response, (2)
incomprehensible sounds, (3) inappropriate words, (4) confused, and (5) oriented. For motor
response, the patient is scored based on (1) no motor response, (2) abnormal extension to pain,
(3) abnormal flexion to pain, (4) withdrawal from pain, (5) localizing pain, and (6) obeys
commands. The GCS can range from 3-15 and the total of these scores add up to 15, which
indicates the patient is alert and oriented. Using GCS has been accepted as a mental status
assessment method in the hospital setting. For this study, GCS scores are used for the mental
status assessment in patients receiving lactulose. (Jain & Iverson, 2018)
Lactulose is given to inpatients at University of Kentucky of hospital that have liver disease
and it is important that they are meeting the protocol of 2-4 bowel movements per day to prevent
changes in mental status from occurring. If a patient becomes encephalopathic, additional
interventions are needed such as an additional dose of lactulose or a lactulose enema. This results
in increased costs and length of stay for patients. There is an economic burden associated with
HE. From 2005-2009, the total costs of hospitalizations increased by 55.1%. The average length
of stay increased from 8.1 days in 2005 to 8.5 days in 2009 for patients with HE. Patients who
had HE during hospitalization, had increased costs due to increased resource utilization,
increased number of inpatient procedures, and an increased average length of stay. The total
costs went from $4.68 billion in 2005 to $7.25 billion in 2009 for patients who suffered from HE
while hospitalized. (Flamm, 2018)
The conceptual framework guiding this study is the Logic Model. The purpose of the study is
to examine the number of bowel movements patients with liver disease who are receiving
lactulose are having each day and assess whether or not additional lactulose interventions are
required. The context of this study is to examine the Internal Medicine inpatient cohort at UK

LACTULOSE ADMINISTRATION 10
hospital. The inputs will be Sunrise Clinical Manager, which is the charting system at UK
hospital, to collect the raw data which will then be entered and stored on REDCap. The activities
will be statistical analysis on SPSS version 25 of data to see if the protocol of 2-4 daily bowel
movements is being met. The outputs will be the results of the study, specifically the percentage
of patients who are meeting the protocol of 2-4 daily bowel movements and whether or not they
required additional lactulose interventions. The effects of this study will be what the author does
with the results and what further studies can be performed to help meet this protocol in the
inpatient setting. (Community Tool Box, 2018)
Purpose
The literature shows that Lactulose is the drug of choice for prevention and treatment of HE
in patients with liver disease. The purpose of this study was to examine whether inpatients with
liver disease at University of Kentucky Hospital receiving lactulose are meeting the protocol of
2-4 bowel movements per day. Additional interventions (administration of PRN doses of
lactulose or lactulose enemas) and a patient’s MELD score and GCS score will be examined in
this study as well.
The specific objectives are:
OBJECTIVE 1: To determine the proportion of patients with liver disease receiving
lactulose at UK hospital are meeting the protocol of 2-4 bowel movements per day, and
examine the demographic differences among the sample population in the study.
OBJECTIVE 2: To assess if inpatients with liver disease receiving lactulose at UK
hospital with a MELD score ≥ 25 are meeting the goal of 2-4 bowel movements per day

LACTULOSE ADMINISTRATION 11
during the first five days of hospitalization and how often they are requiring additional
lactulose interventions.
OBJECTIVE 3: To assess if inpatients with liver disease receiving lactulose at UK
hospital with a GCS ≤14.5 are meeting the goal of 2-4 bowel movements per day during
the first five days of hospitalization, how often they are requiring additional lactulose
interventions, and whether or not they received narcotics.
Methods
A retrospective chart review was conducted including patients that were admitted to
University of Kentucky Hospital with a history of or diagnosis of HE on the Internal Medicine
service line. Data was collected through a sample from January 1, 2017 to December 31, 2017 of
75 randomly selected charts from the electronic medical records (EMR) gathered by the CCTS
from the KMSF database. The principle investigator (PI) collected data from the EMR and
entered and stored them on REDCap’s protected server. MRNs were entered on REDCap, but
not exported into SPSS for the data analysis. Once the data was collected and entered into the
data collection tool, the de-identified data was uploaded into SPSS version 25 statistical software
for data analysis with statistical significance to be a p-value of <0.05.
Setting
The study took place at University of Kentucky (UK) hospital in Lexington, Kentucky. UK
hospital is committed to the pillars of academic health care—research, education, and clinical
care (UK Healthcare). The hospital is dedicated to the health of Kentucky to provide the most
advanced patient care and serve as an information resource (UK Healthcare). The 9th and 10th

LACTULOSE ADMINISTRATION 12
floors in Pavilion A and the 5th floor and two wings on the 6th floor in Pavilion H make up the
Internal Medicine cohort at UK hospital with 122 beds.
Sample
Patient inclusion criteria were: 1) patients aged at least 18 years old; 2) patients with history
of or diagnosis of HE; 3) Length of stay ≥ 5 days. Patient exclusion criteria were: 1) patients
aged less than 18 years; 2) patients receiving lactulose for non-liver disease etiologies (i.e.
constipation); 3) Length of stay ≤ 5 days. Demographic variables will be extracted for each
individual in the study including age, sex, race, and admitting diagnosis. We reviewed all
patients’ charts that were identified with a history or diagnosis of hepatic encephalopathy from
January 1, 2017 to December 31, 2017. Seventy-five charts were reviewed. We excluded 5
patients as not meeting criteria leaving 70 patients who met the inclusion and exclusion criteria.
Data Collection
Approvals from the University of Kentucky Institutional Review Board (IRB) and the
University of Kentucky Nurse Research Board were obtained prior to the collection of data. This
study was based on a retrospective chart review. Patient charts were collected from the KSMF
electronic patient database. Seventy-five randomly selected charts were identified using the
ICD10 CM coding scheme with diagnosis or history of hepatic encephalopathy ICD-10 code
K72.90. During data collection, patient records were accessed using the patient medical record
number (MRN), data was abstracted based on listed variables in Table 1, and data was entered
stored on REDCap, a protected data collection server. Please refer to Table 1 for a list of
variables that were reviewed, which included demographic variables (length of stay, age, race,
sex, admitting diagnosis), the number of daily bowel movements in 24 hours for the first give

LACTULOSE ADMINISTRATION 13
days of hospitalization, daily PRN oral lactulose administration, daily lactulose enema
administration, admit MELD score, average daily GCS score, and daily narcotic administration.
Specific laboratory values were collected on day one of hospitalization to calculate the admit
MELD score: INR, Cr, Na, total bilirubin, and whether or not the patient received dialysis twice
in the past week. The MELD score was then calculated by using the MD Calc website. Please
see table 2 for the list of narcotics patients received in this study.
Data Analysis
Descriptive statistics, including frequency distributions, means, percentages and standard
deviations (SD) were used to describe patients’ demographic measures and whether or not the
protocol of 2-4 bowel movements were met. The chi-square test of association was used to test
for associations between categorical variables. The categorical variables in the study were:
patients with a MELD score ³ 25 and whether or not they met the criteria of 2-4 daily bowel
movements (yes/no), and whether or not they received additional lactulose interventions (yes/no
for lactulose enema or PRN lactulose administration) and patients with an GCS £ 14.5 and
whether or not they met the criteria of 2-4 daily bowel movements (yes/no), and whether or not
they received additional lactulose interventions (yes/no for lactulose enema or PRN lactulose
administration) and whether or not narcotics were administered (yes or no). All analysis was
conducted using SPSS version 25; an [alpha] level of .05 was used for statistical significance in
all analysis

LACTULOSE ADMINISTRATION 14
Results
Sample Characteristics
A total of 70 patients who met the inclusion/exclusion criteria were included in this
study. Five patients did not meet the criteria because lactulose was not ordered for them until
after five days of hospitalization. The average age of patients was 57.6 (SD=10.7; see Table 3),
with the majority of the patients being White (95.7%) and male (51.4%). The median length of
stay (LOS) was 11.5 days with a range of 6-20. The majority of patients had an admitting
diagnosis of non-liver disease etiology (62.9%).
Bowel Movements
Patients were defined as meeting the criteria each day if the number of daily bowel
movements was recorded as 2-4. Of the five days, the highest percentage of patients not meeting
the criteria was day 1 (77.36%; see Table 4). Greater than 50% of patients did not meet the
criteria on the four additional days.
MELD Score
Patients who presented with a MELD score ≥ 25 on the first day of admission were
analyzed specifically. There was no association between a higher MELD score and whether or
not the criteria of 2-4 bowel movements were met (see Table 5). Also, there was no association
among a higher MELD score and requiring additional lactulose interventions (PRN lactulose or
lactulose enema).

LACTULOSE ADMINISTRATION 15
GCS Score
Patients who had an average daily GCS score of ≤ 14.5 were analyzed specifically. On
day 1 and day 2 of hospitalization, significance was shown for lactulose enema administration
(p=0.0021, 0.0063 respectively, see Table 6). There was no association between a confused
patient and whether or not the criteria of 2-4 bowel movements were met. Also, there was no
association among a confused patient and requiring PRN lactulose or lactulose enemas on days
3, 4, and 5. There was no association between confusion and narcotic administration.
Discussion
This study aimed to better understand lactulose administration for patients with liver
disease in the hospital setting. Additional lactulose interventions were examined to see if those
with a higher MELD score or confusion required more lactulose. Understanding the findings in
this study will help nurses and physicians understand the importance of lactulose titration in the
hospital setting.
Research has shown that a goal of 2-4 bowel movements per day helps prevent and treat
HE. This study has shown that over half of the patients are not meeting the criteria of 2-4 daily
bowel movements during the first five days of hospitalization. Therefore, nurses may not be
titrating lactulose administration to bowel movements properly. As a result, patients are at an
increased for becoming encephalopathic because they are not clearing the ammonia through the
stool. Physicians may not be aware that they their patients have not the met the goal of 2-4 bowel
movements until the following day because the nurse did not inform them the prior day.
Therefore, better methods of communication need to be established among the nurses and
physicians about the number of bowel movements their patients are having.

LACTULOSE ADMINISTRATION 16
When examining a patient’s MELD score, the severity of a patient’s liver disease did not
seem to impact whether or not they were meeting the criteria of 2-4 bowel movements daily.
This patient population did not require additional lactulose interventions. This indicates that
although a patient may have a higher MELD score, lactulose titration does not need to be done
any differently.
When examining a patient’s GCS score, there was no significance shown for whether or
not they are meeting the criteria of 2-4 bowel movements per day. However, on day one and day
two of hospitalization, this population was requiring the additional intervention of lactulose
enemas. This indicates that upon admission, confused patients may need more lactulose
interventions due to their mental status. This allows physicians and nurses to be aware that close
titration of lactulose needs to be done for the first few days of hospitalization. Perhaps, ordering
a standing order of a lactulose enema would be beneficial for confused patients. Therefore, the
nurse could go ahead and administer the enema if the patient has not been stooling enough.
There was no significance for this population receiving a PRN lactulose dose or a lactulose
enema on days 3, 4, and 5. Lastly, there was no significance in this population among narcotic
use. This indicates that narcotic administration does not affect GCS score in this patient
population.
Limitations
There were limitations identified in the design of the study. Data was collected through a
retrospective chart review. Consequently, there was no way to verify the recorded results.
Patients who are independent may have gotten up alone and had a bowel movement without
reporting it to the nursing tech or registered nurse to enter into the chart. Nursing techs or

LACTULOSE ADMINISTRATION 17
registered nurses might not remember to record every bowel movement their patient has had that
day.
Some patients had to be excluded from the study because lactulose was not started until later
in their stay. When patients are first admitted, some health care providers do not start all the
home medications right away and wait until they are stable to resume home medications.
Therefore, some patients were not receiving lactulose until after five days of hospitalization, thus
causing them to be excluded and lowering the patient population for the study.
Calculating a MELD score involves getting specific lab values including INR, Cr, Na, and
total bilirubin. All of these values need to be collected at the same time to calculate a MELD
score. In some patients, the admit MELD score could not be calculated because some of the lab
components were missing, specifically the INR value. This resulted in a smaller number of
patients included for the MELD score analysis in this study.
Recommendations for Future Studies
Recommendations for future studies would include implementing a standardized lactulose
order set for this patient population. This would allow for effective nurse/physician
communication about the number of bowel movements the patients are having. The order set
would guide nurses throughout the day on when to give scheduled and PRN lactulose. It would
also tell nurses under what circumstances and when they should inform the physician if the
patient has only had ≤ 1 bowel movement that day. After implementing this order set, the
number of bowel movements could be analyzed to see if an increased number of patients are
meeting the criteria of 2-4 daily bowel movements. Results of implementation of a standardized

LACTULOSE ADMINISTRATION 18
lactulose order set could be compared to this study that does not have any standardization in
place. Please refer to Table 7 for an example of a potential standardized lactulose order set.
Another recommendation for future studies could be an assessment of nurse’s knowledge
when titrating lactulose administration. Surveys could be given to nurses to ask whether or not
they are paying attention to the number of bowel movements their patients are having, whether
or not they communicate effectively with the nursing techs about the number of bowel
movements their patients are having, and how they feel about communicating with the physician
regarding the titration of lactulose and number of bowel movements their patients are having.
These results could be beneficial to help find ways to improve patient outcomes in meeting the
specific criteria for lactulose administration.
Conclusion
The goal of this study was to examine whether or not patients with liver disease receiving
lactulose were meeting the goal of 2-4 bowel movements per day in the inpatient setting.
Additional factors were analyzed including PRN lactulose and lactulose enema administration.
The study population was broken down into those who had a MELD score ≥ 25 and those with
daily average GCS of ≤ 14.5. These groups were further analyzed to see if they required
additional lactulose interventions and narcotic administration was examined in the GCS group.
The study showed that higher percentages of patients were not meeting the criteria of 2-4 daily
bowel movements during the first five days of hospitalization. Patients with a MELD score of ≥
25 did not require additional lactulose interventions. Patients with a GCS of ≤ 14.5 required
lactulose enemas on days 1 and 2 of hospitalization, indicating these patients should be closely
monitored during the first few days of hospitalization. This knowledge lets physicians and nurses
LACTULOSE ADMINISTRATION 19
realize that those who are confused may require additional lactulose interventions upon
admission. Lastly, narcotic use was examined in those with a GCS ≤ 14.5 and it does not
correlate with their mental status.
This study can give providers a better understanding of lactulose titration and administration
in the inpatient healthcare setting and show that not all patients may be meeting the specific
protocol that the research proposes. Implementation of a standardized lactulose order set may
allow for better lactulose titration and could be examined in a future study. Reducing the rates of
HE in the hospital setting can reduce healthcare costs. It is important that nurses and doctors are
monitoring the number of daily bowel movements their patients are having to prevent further
complications from occurring.
LACTULOSE ADMINISTRATION 20
References
American Association of Critical-Care Nurses. (n.d.). AACN PCCN Review: Gastrointestinal. Retrieved from https://www.aacn.org/docs/OnDemand/PCCN2013/PCCNGastrointestinal/Gastrointestin al.pdf
American Liver Foundation. (July 2017). More about organ donation. Retrieved from http://www.liverfoundation.org/patients/organdonor/about/ Centers for Disease Control and Prevention. (2017). Chronic liver disease and cirrhosis. Retrieved from https://www.cdc.gov/nchs/fastats/liver-disease.htm’ Community Tool Box. (2018). Developing a logica model or theory of change. CTB. Retrieved
from https://ctb.ku.edu/en/table-of-contents/overview/models-for-community-health-and-
development/logic-model-development/main Dhiman, R. K., Sawhney, I. M. S., Chawla, Y. K., Das, G., Ram, S., & Dilawari, J. B. (2000).
Efficacy of lactulose in cirrhotic patients with subclinical hepatic encephalopathy. Digestive diseases and sciences, 45(8), 1549-1552.
Elwir, S. & Rahimi, R.S. (2017). Hepatic encephalopathy: An update on the pathophysiology
and therapeutic options. Journal of Clinical and Translational Hepatology, 5(2): 142-151.
Flamm, S.L. (2018). Considerations for the cost-effecitve management of hepatic encephalopathy. American Journal of Managed Care. Retrieved from
https://www.ncbi.nlm.nih.gov/books/NBK513298/ Galati, J.G. (2011). The MELD score and liver transplant: An update for patients. Liver
Specialists of Texas. Retrieved from https://blog.texasliver.com/2011/02/the-meld-score-and-liver-transplant-an-update-for-
patients/ Hepatitis C Online. Diagnosis and management of hepatic encephalopathy. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5472935/pdf/JCTH-5-142.pdf
Hepatology Centers of Educational Expertise. (2012). The multidimensional burden of hepatic encephalopathy.Retrieved from http://www.chronicliverdisease.org/disease_focus/enewsletters/HepCoEE_eNewsLetter_ Multidimensional_burden.pdf
Jain, S. & Iverson, L.M. (2018). Glascow Coma Scale. StatPearls. Retrieved from
https://www.ncbi.nlm.nih.gov/books/NBK513298/
Kamath, P.S. & Kim, R. (Mar 2007). The Model for End Stage Liver Disease (MELD). Hepatology, 45(3), 797-805. Retrieved from
LACTULOSE ADMINISTRATION 21
https://aasldpubs.onlinelibrary.wiley.com/doi/epdf/10.1002/hep.21563 Kentucky Life Expectancy. (2017). Kentucky causes of death by age and gender. Retrieved from http://www.worldlifeexpectancy.com/kentucky-cause-of-death-by-age-and-gender Luo, M., Li, L., Lu, C.-Z., & Cao, W.-K. (2011). Clinical efficacy and safety of lactulose for
minimal hepatic encephalopathy: a meta-analysis. European journal of gastroenterology & hepatology, 23(12), 1250-1257.
MD Calc. (2016). MELD Score (Model for End Stage Liver Disease) (12 and Older). Retreieved
from https://www.mdcalc.com/meld-score-model-end-stage-liver-disease-12-older Morgan, C.L., Jenkins-Johns, S., Radwan, A., Conway, P., & Currie, C.J. (2014). PTU-126
Mortality associated with hepatic encephalopathy in patients with severe liver disease. Gut, 63, A94.
National Organization for Rare Disorders. (2011). Hepatic encephalopathy. Retrieved from https://rarediseases.org/rare-diseases/hepatic-encephalopathy/
Nickson, C. (2017). Glascow coma scale (GCS). Life in the FASTLANE. Retrieved from
https://lifeinthefastlane.com/ccc/glasgow-coma-scale-gcs/=
Prasad, S., Dhiman, R. K., Duseja, A., Chawla, Y. K., Sharma, A., & Agarwal, R. (2007). Lactulose improves cognitive functions and health-related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy. Hepatology, 45(3), 549-559. Sutter Health. (2014). MELD and the waiting list for liver transplant. Retrieved from http://www.cpmc.org/advanced/liver/patients/topics/MELD.html
Sharma, B. C., Sharma, P., Agrawal, A., & Sarin, S. K. (2009). Secondary prophylaxis of hepatic encephalopathy: an open-label randomized controlled trial of lactulose versus placebo. Gastroenterology, 137(3), 885-891. e881.
Sharma, P., Agrawal, A., Sharma, B. C., & Sarin, S. K. (2011). Prophylaxis of hepatic
encephalopathy in acute variceal bleed: a randomized controlled trial of lactulose versus no lactulose. Journal of gastroenterology and hepatology, 26(6), 996-1003.
Sharma, P., Sharma, B. C., Agrawal, A., & Sarin, S. K. (2012). Primary prophylaxis of overt
hepatic encephalopathy in patients with cirrhosis: an open labeled randomized controlled trial of lactulose versus no lactulose. Journal of gastroenterology and hepatology, 27(8), 1329-1335.
Tapper, E. B., Jiang, Z. G., & Patwardhan, V. R. (2015). Refining the Ammonia Hypothesis: A
Physiology-Driven Approach to the Treatment of Hepatic Encephalopathy. Paper presented at the Mayo Clinic Proceedings.
Tsang, L. & Ahmed, J. (2013). Clinical applications of the Model for End-Stage Liver Disease

LACTULOSE ADMINISTRATION 22
(MELD) in hepatic medicine. Hepatic Medicine, 5, 1-10. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3953735/
UK HealthCare. About UK healthcare. Retrieved from
https://ukhealthcare.uky.edu/about
United Network for Organ Sharing. Questions & answers for transplant candidates about MELD
and PELD. UNOS. Retrieved from
https://www.unos.org/wp-content/uploads/unos/MELD_PELD.pdf
Wijdicks, E. (2016). Hepatic encephalopathy. The New England Journal of Medicine, 375, 1660-1670.
Zhan, T., & Stremmel, W. (2012). The diagnosis and treatment of minimal hepatic
encephalopathy. Deutsches Ärzteblatt International, 109(10), 180.

LACTULOSE ADMINISTRATION 23
List of Variables per Category Category Variables/Measures Demographic Measures
Age age of participants in years Race American Indian/Alaskan Native, Asian, Native Hawaiian or Other
Pacific Islander, Black or African American, White, Other, Unknown/not reported
Gender Male, female Admitting diagnosis Diagnosis upon admission to the hospital
Length of stay Number of days of hospitalization Process Measures Daily PRN oral lactulose
administration Yes or No daily for the first five days of hospitalization
Daily lactulose enema administration
Yes or No daily for the first five days of hospitalization
Admit MELD score Calculated with admit lab work (day 1 of hospitalization) using Creatinine, International normalized ratio, Sodium, Bilirubin and dialysis frequency; score ranges from 6-40
Average daily GCS score Average daily GCS for 0800 and 2000 for the first five days of hospitalization, 15 or ≤ 14.5
Daily narcotic administration
Yes or No daily for the first five days of hospitalization
Outcome Measures Daily number of bowel
movements Number of daily bowel movements for the first five days of hospitalization
Notes: Length of stay (LOS), Model for End Stage Liver Disease (MELD), Creatinine (Cr), International normalized ratio (INR), Sodium (Na), Bilirubin (bili), Glascow Coma Scale (GCS) Table 1: List of variables per category.

LACTULOSE ADMINISTRATION 24
Narcotics Administered in this Study Generic Name Brand Name Propofol Diprovan Oxycodone Oxycontin Morphine Duramorph Hydromorphone Dilaudid Hydrocodone/Acetaminophen
Norco
Tramadol Ultram
Table 2: Narcotics Administered in this Study
Mean (SD) or n (%) Age 57.6 (10.7) Sex Male Female
36 (51.4%) 34 (48.6%)
Ethnicity Black or African American White
3 (4.3%)
67 (95.7%)
Admitting Diagnosis Liver Disease Etiology Non-liver Disease Etiology
26 (37.1%) 44 (62.9%)
Length of Stay
Median (Range) 11.5 (6-20)
Table 3. Demographics of patients in the study. (N=70)
Day 1 Day 2 Day 3 Day 4 Day 5
Y N Y N Y N Y N Y N Meet the goal of 2-4 BM’s per day?
22.64%
77.36%
43.64%
56.36%
44.44%
55.56%
41.54%
58.46%
34.38%
65.63%
Table 4. Percentage of patients who met the goal of 2-4 bowel movements (BMs) each day for the first five days of hospitalization.

LACTULOSE ADMINISTRATION 25
Day 1 Day 2 Day 3 Day 4 Day 5
Y N Y N Y N Y N Y NMeet the goal of 2-4 BM’s per day?
22.22%
25.81%
52.63%
40.63%
36.36%
51.53%
43.48%
34.21%
43.48%
32.43%
P 1.000 0.4048 0.2638 0.4692 0.3880 Y N Y N Y N Y N Y NReceived PRN dose
of lactulose?
4.76%
0.00
14.29
%
0.00
9.09%
5.41%
8.70%
5.26%
8.70%
2.63%
P 0.3889 0.0536 0.6244 0.6282 0.5507 Y N Y N Y N Y N Y N
Received lactulose enema?
4.76%
15.15
%
4.76%
12.12
%
0.000
5.41%
13.04
%
5.26%
4.35%
5.26%
P 0.3863 0.6377 0.5243 0.3559 1.000 Table 5: Chi square: Percentage of patients with a MELD score of ³ 25 who met the goal of 2-4 BM’s per day, received a PRN dose of lactulose, received a lactulose enema, and received a narcotics each day for the first five days of hospitalization.
LACTULOSE ADMINISTRATION 26
Day 1 Day 2 Day 3 Day 4 Day 5
Y N Y N Y N Y N Y N Meet the goal of 2-4 BM’s per day?
66.67%
29.27%
33.33%
41.94%
42.86%
31.43%
37.04%
39.47%
45.45%
40.48%
P 0.0390 0.5149 0.3492 0.8423 0.7017 Y N Y N Y N Y N Y N Received
PRN dose of
lactulose?
0.000
2.86%
4.55%
5.71%
13.04
%
2.50%
16.00
%
2.50%
10.71
%
2.70%
P 1.000 1.000 0.1338 0.0677 0.3068 Y N Y N Y N Y N Y N
Received lactulose enema?
27.27%
0.000
22.73%
0.000
8.70%
0.000
8.00
7.5%
7.14%
2.70%
P 0.0021 0.0063 0.1295 1.000 0.5731 Y N Y N Y N Y N Y N
Received Narcotics
?
31.82%
38.89%
45.45%
42.86%
43.48%
45.00%
44.00%
45.00%
46.43%
40.54%
P 0.5867 0.8474 0.9068 0.9371 0.6350 Table 6: Chi square: Percentage of patients with a GCS of £ 14.5 who met the goal of 2-4 BM’s per day, received a PRN dose of lactulose, received a lactulose enema, and received a narcotic each day for the first five days of hospitalization.
Time Intervention 0800 Give scheduled 30 mL dose of Lactulose 1200 If patient has not had a bowel movement by
this time, give PRN 30 mL dose of lactulose 1400 Give scheduled 30 mL dose of Lactulose 1600 If patient has ≤ 1 bowel movement by this
time, notify physician for next intervention. 2000 Give scheduled 30 mL dose of Lactulose
Table 7: Standardized Lactulose Order Set example to implement in future studies.





























