Embed Size (px)
Citation preview

Does Renal Failure Cause an Atherosclerotic Milieuin Patients with End-Stage Renal Disease?
Robert Kennedy, BSc (Hons), Colin Case, MSc, Robert Fathi, MBBS,David Johnson, MBBS, PhD, Nicole Isbel, MBBS, Thomas H. Marwick, MBBS, PhD
PURPOSE: Atherosclerotic vascular disease is the main causeof morbidity and mortality in patients with end-stage renal dis-ease, but the independent contribution of renal failure ratherthan associated risk factors is unclear. We sought to examine therelative contribution of these factors to the severity of athero-sclerosis by measuring intima-medial thickness and brachial ar-tery reactivity in uremic patients and controls.SUBJECTS AND METHODS: Cardiovascular risk factors, in-cluding lipid and homocysteine levels, were evaluated in 213patients (69 on hemodialysis, 60 on peritoneal dialysis, and 82nonuremic controls). High-resolution B-mode ultrasonogra-phy with automated off-line analysis was used to measure theintima-medial thickness in the common carotid artery and tomeasure the lumen diameter of the brachial artery at rest, dur-ing reactive hyperemia, and after sublingual nitroglycerine. Thecorrelations of risk factors with intima-medial thickness and
brachial reactivity were examined using a general linear regres-sion model.RESULTS: Patients with renal failure had a greater mean (6SEM) maximum intima-medial thickness than controls (0.83 60.02 mm versus 0.70 6 0.02 mm, P ,0.05), but the brachialartery response to reactive hyperemia was not significantly dif-ferent between the renal failure patients and the control group(4.7% 6 6.1% versus 6.1% 6 8.6% dilatation, P .0.05). Theuremic state was an independent predictor of intima-medialthickness (r2 5 0.16, P ,0.001) but not of brachial artery reac-tivity (P 5 0.99).CONCLUSION: The atherosclerotic burden in patients withrenal failure, as indicated by an increased intima-medial thick-ness, may reflect effects of uremia that are independent of car-diovascular risk factors. Am J Med. 2001;110:198 –204. q2001by Excerpta Medica, Inc.
Atherosclerotic cardiovascular disease is the lead-ing cause of morbidity and mortality in patientswith end-stage renal disease, accounting for 50%
of all deaths (1). It is unclear, however, whether end-stagerenal disease per se promotes an accelerated atherogenicstate or whether this simply reflects a greater prevalenceof cardiac risk factors (2,3). Both classic and new riskfactors for atherosclerosis (4,5) are prevalent in dialysispatients (6), and many of these factors can be modifiedsuccessfully.
Atherosclerosis leads to alterations in the structure andfunction of the arterial wall, resulting in thickening of theintima (4) and reduced endothelium-dependent vasodi-latation (7). Intima-medial thickness can be reliably andnoninvasively quantified by off-line automated digitalanalysis of high-frequency ultrasound images (8). Thisparameter is rapidly becoming accepted in nonuremicpatients as a noninvasive marker for following the pro-gression of atherosclerosis (9), such as when lipid-lower-ing agents are used (10). Endothelial dysfunction, a pre-cursor of atherogenesis that is reflected by abnormal bra-
chial artery reactivity, may also be used as a marker ofearly atherosclerosis (11). We used these tools to investi-gate the relative contribution of risk factors and the ure-mic state to atherosclerosis in patients with end-stage re-nal disease.
METHODS
Study DesignThis cross-sectional study involved patients with end-stage renal disease on peritoneal dialysis (n 5 60) or he-modialysis (n 5 69), and nonuremic control patients(n 5 82). The sample size was chosen to have an 80%power to detect an intima-medial thickness differencegreater than 0.10 mm (12), assuming a standard devia-tion of 0.18 mm (13) between uremic patients and con-trols, which required at least 50 subjects in the controland end-stage renal disease groups. For a power of 80% todetect a difference of 2% (14) with an assumed standarddeviation of 4.5% (15) in brachial artery reactivity, werequired at least 80 subjects in each group. There were noexclusion criteria, and all available dialysis patients wereapproached for study. The control patients were selectedfrom patients with one or more risk factors who attendedthe investigators’ outreach clinic for cardiovascularscreening or attended the investigators’ outpatient clinicor echocardiography laboratory for medical conditionsother than end-stage renal disease. Other than the pres-ence of risk factors, there were no selection criteria apart
From the University of Queensland, Brisbane, Queensland, Australia.Supported in part by a grant in aid from the Australian Kidney Foun-
dation and the National Health and Medical Research Council of Aus-tralia.
Requests for reprints should be addressed to Thomas H. Marwick,MBBS, PhD, University of Queensland Department of Medicine, Prin-cess Alexandra Hospital, Brisbane, Queensland 4102, Australia.
Manuscript submitted December 3, 1999, and accepted in revisedform October 4, 2000.
198 q2001 by Excerpta Medica, Inc. 0002-9343/01/$–see front matterAll rights reserved. PII S0002-9343(00)00695-1

from the availability of an investigator and machine toperform the imaging studies. All patients underwent clin-ical evaluation, biochemical testing, and quantitative ul-trasound measurements. For hemodialysis patients, allmeasurements were performed before dialysis. Writteninformed consent was obtained from all patients, and thestudy was approved by the Hospital Research EthicsCommittee.
Clinical CharacteristicsAll patients completed a questionnaire about risk factorsand their personal and family history of cardiovasculardisease. Risk factors included age, sex, smoking status,hypertension (systolic blood pressure .140 mm Hg ordiastolic blood pressure .90 mm Hg), presence and typeof diabetes, hyperhomocysteinemia (homocysteine level.15 mmol/L), hypercholesterolemia (total cholesterollevel .5.5 mmol/L), body mass index, previous cardio-vascular events, menopausal status, and estrogen use.
Biochemical AnalysisTotal cholesterol, high-density lipoprotein (HDL) cho-lesterol, and triglyceride levels in fasting venous sampleswere determined by standard enzymatic methods. HDL
cholesterol was separated by selective polyanion precipi-tation of apoprotein-B containing lipoproteins with dex-tran sulfate/magnesium chloride (16). Low-density li-poprotein (LDL) cholesterol levels were calculated ac-cording to Friedewald’s formula, and very low densitylipoprotein (VLDL) cholesterol levels were calculatedfrom the remaining fraction. Homocysteine levels weredetermined by a standard chromatography method (17).
Carotid ImagingIntima-medial thickness was measured with a high-reso-lution B-mode ultrasound HDI 5000 scanner (AdvancedTechnology Laboratories, Bothell, Washington)equipped with a 12.5 MHz linear transducer. The systemprovides an optimal axial resolution of 0.07 mm. Both theright and left common carotid arteries were examinedlongitudinally in the anterolateral, lateral, and posterolat-eral planes (18). Only the common carotid was exam-ined, as this gives more reliable and reproducible imagesthan the external and internal carotid arteries (19). Eachview was imaged 10 mm proximal from the bifurcation(20). All settings were kept constant, although the gainsetting was varied to provide the best image quality. One
Table 1. Clinical Characteristics of Patients with End-Stage Renal Disease and Control Patients
Risk Factor
Group
PValue
Control(n 5 84)
End-StageRenal Disease
(n 5 129)Mean 6 SD or Number (%)
Age (years) 58 6 13 54 6 15 0.04Male sex 45 (54) 65 (50) 0.68Premenopausal* 12 (31) 13 (20) 0.38Body mass index (kg/m2) 27.5 6 4.9 25.7 6 5.6 0.008Current smoker 11 (13) 22 (17) 0.45Former smoker 22 (26) 41 (32) 0.38Previous cardiac history 30 (36) 43 (33) 0.77History of hypertension 43 (51) 78 (60) 0.20Systolic blood pressure (mm Hg) 130 6 20 143 6 25 ,0.001Diastolic blood pressure (mm Hg) 78 6 11 82 6 13 0.01Hypercholesterolemia 40 (48) 26 (20) ,0.001Cholesterol (mmol/L) 5.3 6 1.0 4.9 6 1.0 0.02
Total high-density lipoprotein 1.14 6 0.4 1.14 6 0.3 0.99Low-density lipoprotein 3.2 6 0.8 2.8 6 0.9 0.005Very low density lipoprotein 0.80 6 0.4 0.77 6 0.35 0.67Low-density/high-density lipoprotein ratio 3 2.6 6 1.1 0.005
3.3 6 1.4 1.9 6 1.1 0.47Triglyceride (mmol/L) 2.1 6 2.1Diabetes 14 (17) 36 (28) 0.07Hyperhomocysteinemia 17 (22)† 83 (64) ,0.001Homocysteine (mmol/L) 12.9 6 4.9† 29.2 6 20.0 ,0.001Current medications
For hypertension 43 (51) 94 (73) 0.002For hypercholesterolemia 33 (39) 47 (36) 0.77Hormone replacement therapy* 12 (31) 10 (16) 0.08
* Among women only.† Measured in 79 patients.
Vascular Structure and Function in End-Stage Renal Disease/Kennedy et al
February 15, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 199

cine loop was recorded for each plane from both the leftand right common carotid vessels and stored digitally ona magneto-optical disc. The same operator performedboth the scan and the analysis (21) to minimize interop-erator variability. The operator was blinded to patienthistory and laboratory results.
Digital images were analyzed off line, using an auto-mated, computer edge-detection software developed forintima-medial thickness measurement (HDI Lab V1.5;Advanced Technology Laboratories). This edge-detec-tion software automatically identifies the relevant inter-faces on both the far and near walls from the region andtime of interest as identified by the observer. For eachview we selected the peak systolic frame to minimize vari-ability in intima-medial thickness during the cardiac cy-cle (8). Automated intima-medial thickness measure-ments were obtained from the near wall (from the “trail-ing” edge of the media-adventitia interface to thelumen-intima interface) and far wall (measured from lu-men-intima interface to the “leading” edge of the media-adventitia interface) (22). Results were recorded as themean intima-medial thickness (6 SEM) for both the farand near wall for each view; the maximum and average ofthe mean intima-medial thickness from each of the threeplanes was calculated for each artery (left and right) (23).Thus, intima-medial thickness was calculated as themean and maximum intima-medial thickness for the farwall for each patient. Visible plaques, as identified by afocal widening relative to adjacent segments with protru-sion into the lumen of either calcified deposits or a com-bination of calcification and noncalcified material, wereexcluded from the area analyzed (24).
Interobserver and intraobserver errors for intima-me-dial thickness were studied in 144 images that were ran-domly chosen and reanalyzed off line. Measurements ofthe far wall were conducted by the original reader (in-
traobserver error) and an independent expert reader (in-terobserver error), both blinded to the original and theother reader’s results (8). Scans were performed by thesame sonographer, and the images were stored digitallyand analyzed as previously stated. The use of the auto-mated software for measurement of far wall intima-me-dial thickness gave a high level of reproducibility of thismeasurement, with an intraobserver variation of 0.01 60.06 mm and a coefficient of variation of 6.7% (Cron-bach’s alpha 5 0.84). The interobserver difference was0.02 6 0.06 mm with a coefficient of variation of 6.8%(Cronbach’s alpha 5 0.81).
Brachial ImagingBrachial artery reactivity was assessed using the samehigh-resolution B-mode ultrasound HDI 5000 scannerand 12.5 MHz linear transducer with color Doppler (608angle to the vessel, with the 1.5 mm range gate in thecenter of the artery). Cine loops were stored digitally foroff-line analysis. The right brachial artery was scanned inlongitudinal section directly below the pressure cuff usedto induce reactive hyperemia. The pressure cuff was ap-plied to the right arm as high as possible above the elbow.Flow velocity and lumen diameter of the brachial arterywere measured after 10 minutes’ rest and before inflationof the cuff to a pressure of 300 mm Hg for 4.5 minutes.Reactive hyperemia (endothelial-dependent flow-medi-ated dilatation) was induced by deflation; flow velocitywere measured within 15 seconds, and lumen diameterwas measured 90 seconds after cuff deflation. A furtherresting scan was taken after 10 minutes to confirm vesselrecovery. Sublingual glyceryl trinitrate (Anginine, 0.4mg) was then administered and the final scan taken after3 minutes (25).
Reproducibility of brachial artery reactivity was also
Table 2. Mean and Maximum Intima-Medial Thickness of the Common Carotid Artery andBrachial Artery Reactivity to Reactive Hyperemia and Nitroglycerin
Measurement
Control(n 5 68)
End-StageRenal Disease
(n 5 128) PValueMean 6 SD*
Intima-medial thickness (mm)Mean 0.61 6 0.10 0.70 6 0.15 0.72Adjusted mean 0.58 6 0.02 0.72 6 0.2 ,0.001Maximum 0.71 6 0.13 0.81 6 0.22 0.05Adjusted maximum 0.70 6 0.02 0.83 6 0.02 ,0.001
Brachial artery reactivity (% dilation) (n 5 81) (n 5 127)To hyperemia 5.1 6 6.0 5.0 6 6.4 0.92To hyperemia reactivity (adjusted) 5.1 6 0.7 4.8 6 0.8 0.78To nitroglycerin 11.3 6 9.1 8.6 6 9.1 0.07To nitroglycerin (adjusted) 10.9 6 1.3* 7.0 6 0.8* 0.013
* Adjusted values are mean 6 SEM.
Vascular Structure and Function in End-Stage Renal Disease/Kennedy et al
200 February 15, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110

assessed for interobserver and intraobserver variation.Thirty-eight randomly selected images were reanalyzedoff line using the same method as for the intima-medialthickness measurements (HDI Lab V1.5 with the LumenDiameter Over Time V1.15 plug-in). Intraobserver vari-ation for brachial artery reactivity measurements was1.1% 6 5.3%, with a coefficient of variation of 43%(Cronbach’s alpha 5 0.90). Variation between observerswas 2.2% 6 6.8% with a coefficient of variation of 68%(Cronbach’s alpha 5 0.85). The use of the automatedsoftware reduced variation to 0.1% 6 3.4%, with a coef-ficient of variation of 38% (Cronbach’s alpha 5 0.91).
Statistical AnalysisAll data are expressed as mean 6 SD, apart from the datafrom the automated measurement package, which aremean 6 SEM. Univariate comparisons were performedusing Student’s t test or one-way analysis of variance(ANOVA). A general linear model was used to examinethe contribution of cardiovascular risk factors and end-stage renal disease to the variance of mean intima-medialthickness and brachial reactivity, and to estimate adjusted
measurements. Statistical significance was set at P ,0.05(two-sided). All statistical analyses were performed usingSPSS for Windows 9.0 (SPSS Inc., Chicago, Illinois).
RESULTS
The mean age of the patients with end-stage renal diseasewas less than that of controls, and hypertension and dia-betes were more common in the renal disease group (Ta-ble 1). The renal disease group also had significantly moreprevious cardiac events. Patients on hemodialysis wereyounger (49.4 6 14.7 versus 58.4 6 12.8 years, P ,0.01),had a greater systolic blood pressure (152 6 27 versus135 6 21 mm Hg, P ,0.001), and a greater prevalence ofhypertension (72% [50 of 69] versus 47% [28 of 60], P 50.004) than patients on peritoneal dialysis. Diabetes wasless prevalent in the hemodialysis group (20% [14 of 69]versus 37% [22 of 60], P 5 0.05). The peritoneal dialysisgroup had undergone dialysis for a shorter duration thanthe hemodialysis group (2.0 6 2.4 versus 4.3 6 5.9 years,P 5 0.005).
Table 3. Factors (Either Presence of Categoric or Increasing Levels of Continuous Variables) That Correlate Positively with Intima-Medial Thickness and Brachial Artery Reactivity in Patients and Controls
Risk Factor
Intima-Medial Thickness Brachial Artery Reactivity
UnivariateModel
MultivariateModel
UnivariateModel
MultivariateModel
r2 P Value r2 P Value r2 P Value r2 P Value
Age 0.12 ,0.001 0.18 ,0.001 0.01 0.12 — —Male gender 0.01 0.14 — — 0.01 0.10 — —Postmenopausal status without
hormone replacement0.07 0.004 — — 0.02 0.30 — —
Body mass index 0.002 0.53 — — 0.004 0.40 — —Smoking history 0.03 0.02 — — 0.004 0.39 — —Hypertension 0.00 0.95 — — 0.01 0.09 — —Systolic blood pressure 0.00 0.09 — — 0.01 0.24 — —Diastolic blood pressure 0.00 0.43 — — 0.00 0.53 — —Hypercholesterolemia 0.03 0.03 — — 0.00 0.62 — —Medication for
hypercholesterolemia0.01 0.25 — — 0.03 0.02 — —
Total cholesterol level 0.002 0.57 — — 0.01 0.18 — —High-density lipoprotein level 0.01 0.16 — — 0.03 0.04 — —Low-density lipoprotein level 0.00 0.73 — — 0.01 0.19 — —Very low density lipoprotein level 0.00 0.81 — — 0.04 0.02 — —Low-density/high-density
lipoprotein ratio0.00 0.92 — — 0.05 0.2 — —
Triglycerides 0.01 0.37 — — 0.03 0.05 — —Hyperhomocysteinemia 0.00 0.70 — — 0.01 0.52 — —Homocysteine level 0.01 0.30 — — 0.00 0.76 — —Diabetes 0.04 0.003 — — 0.03 0.07 — —Cardiac history 0.01 0.19 — — 0.01 0.27 — —Number of risk factors 0.14 0.00 0.043 0.34 0.08 0.01 0.08 0.001Renal disease 0.10 ,0.001 0.158 0.000 0.00 0.72 0.00 0.99Risk factor number by renal disease
(interaction)0.08 0.008
Vascular Structure and Function in End-Stage Renal Disease/Kennedy et al
February 15, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 201

Patients with end-stage renal disease had lower totaland LDL cholesterol levels than control patients (Table1).Defining an abnormal lipid profile as the presence of atotal cholesterol level .5.5 mmol/L, HDL cholesterollevel ,1.0 mmol/L, or an LDL cholesterol level .2.6mmol/L, 49% (63) of the 129 patients with end-stage re-nal disease and 63% (53) of the 84 patients in the controlgroup (P 5 0.05) met those criteria. Hyperhomocys-teinemia (.15 mmol/L) was much more common in thepatients with end-stage renal disease than in the controls(Table 1).
Hypercholesterolemia (.5.5 mmol/L) was more com-mon in patients on peritoneal dialysis than in those onhemodialysis (35% [16 of 46] versus 18% [10 of 55], P 50.07), as was use of lipid-lowering agents (55% [33 of 60]versus 20% [14 of 69], P , 0.001). Mean total cholesterol(5.4 6 1.0 versus 4.6 6 1.0 mmol/L, P 5 0.001) andtriglyceride levels (2.5 6 1.5 versus 1.7 6 0.9 mmol/L,P 5 0.001) were higher in patients on peritoneal dialysiscompared with the hemodialysis patients; there were nosignificant differences in the other lipid fractions.
Carotid UltrasoundPatients with end-stage renal disease had about a 15%greater mean and maximum intima-medial thicknesscompared with the nonuremic controls (Table 2). Ad-justment for other risk factors had only a modest effect.
Brachial ReactivityThere were no significant differences in the response toreactive hyperemia between the end-stage renal diseasegroup and the controls (Table 2). Patients with end-stagerenal disease had a diminished reactivity to nitroglycerinthat was statistically significant after adjustment for othercardiovascular risk factors.
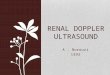
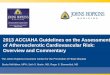
Relation among Cardiovascular Risk Factors,Renal Failure, and Noninvasive MeasuresAge, use of estrogen, hypercholesterolemia, diabetes,number of risk factors and end-stage renal disease wereassociated with mean intima-medial thickness in multi-variate analyses (Table 3). In a multivariate linear regres-sion model, age (r2 5 0.11, P ,0.011) and the uremicstate (r2 5 0.16, P ,0.011) were independent predictorsof intima-medial thickness. The number of cardiovascu-lar risk factors was associated with intima-medial thick-ness in controls and in patients with end-stage renal dis-ease (Figure 1). In univariate analyses, only diabetes andnumber of cardiovascular risk factors were associatedwith reduced reactivity to hyperemia (Table 3). In a mul-tivariate model, only the number of risk factors was anindependent predictor of decreased brachial artery reac-tivity (r2 5 0.08, P 5 0.3) (Figure 2). The uremic state wasnot associated with brachial artery reactivity (P 5 0.99).
Effects of Type of DialysisAmong patients with end-stage renal disease, peritonealdialysis was associated with a greater intima-medialthickness (Table 4). Mode of dialysis was not an indepen-dent predictor of reduced brachial artery reactivity.
DISCUSSION
Although atherosclerosis is common in patients withend-stage renal disease, it is unclear whether this is theresult of an independent effect of end-stage renal diseaseon the vasculature or merely reflects the high prevalenceof traditional cardiovascular risk factors such as diabetesand hypertension in these patients. The results of thepresent study confirm that patients with end-stage renaldisease have greater anatomic (intima-medial thickness)and functional (brachial reactivity) evidence of athero-
Figure 1. Relation of intima-medial thickness (mean 6 SD) tothe number of risk factors in patients with end-stage renal dis-ease and control patients.
Figure 2. Relation of brachial artery reactivity (mean 6 SD) tothe number of risk factors in patients with end-stage renal dis-ease and control patients.
Vascular Structure and Function in End-Stage Renal Disease/Kennedy et al
202 February 15, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110

sclerosis than people without end-stage renal disease. Al-though other studies have shown that patients with end-stage renal disease have diminished brachial artery reac-tivity (26,27), these changes as well as the greater intima-medial thickness that we observed might simply reflectthe greater prevalence of hypertension, hyperhomocys-teinemia, and diabetes in patients with end-stage renaldisease (6). Our results, however, indicate that end-stagerenal disease is independently associated with intima-medial thickness.
High resolution B-mode ultrasonography can be usedto visualize the intima-medial thickness of the commoncarotid artery (9,18,19), which correlates with histologicand angiographic evidence of atherosclerosis, and hasbeen used as a surrogate endpoint to measure atheroscle-rotic regression (12,28). Reductions in vasodilator re-sponsiveness reflect endothelial dysfunction, which hasbeen associated with aging, atherosclerotic risk factors,and the presence of atherosclerosis (11,25,29). Brachialartery reactivity measures the vasodilator response to me-chanically induced reactive hyperemia, which causesshear stress on the vessel wall and the release of nitricoxide, promoting flow-mediated vasodilatation. In thisstudy, endothelial dysfunction was abnormal in many pa-tients with end-stage renal disease as well as in many con-trol patients who had cardiovascular risk factors. Al-though brachial artery reactivity of patients with renaldisease was more abnormal than that of controls, the dif-ferences between the two groups of patients seemed to berelated to the greater prevalence of cardiovascular riskfactors among the patients with end-stage renal disease.
We sought to examine whether treatable risk factors ex-plained the greater prevalence of vascular disease in patientswith renal failure. Therefore, of the “new” risk factors foratherosclerosis, we measured only homocysteine levels. Li-poprotein (a), which consists of a low-density lipoproteinparticle with an apo (a) protein, is elevated threefold in pa-tients on dialysis (30) and may at least be partly responsiblefor the greater prevalence of atherosclerosis in patients withend-stage renal disease. There is also a strong associationwith fibrinogen levels, which are increased in patients ondialysis (31). Potential markers of vascular inflammation,such as serum levels of C-reactive protein, are both elevated
and associated with cardiovascular risk in patients with renalfailure (32). Future studies should address the relation ofthese factors to the anatomic and structural markers used inthis study.
It remains possible that the risk conferred by renal fail-ure is a marker for a more severe risk factor profile. Al-though renal failure was an independent predictor of in-tima-medial thickness after adjustment for blood pres-sure and levels of lipids and homocysteine, the durationof those risk factors was unknown. Moreover, standardlipid analyses may neglect important differences in lipidsubfractions. Nevertheless, our findings suggest that con-ventional intervention on modifiable cardiac risk factorssuch as dyslipidemia, hypertension, and hyperhomocys-teinemia may not be sufficient to normalize the cardio-vascular morbidity and mortality in patients with end-stage renal disease.
ACKNOWLEDGMENTSWe gratefully acknowledge the assistance of the staff and nursesof the Princess Alexandra Hospital Renal and Dialysis Unit.
REFERENCES1. ANZData Registry Report. Adelaide, South Australia: Australian
Kidney Foundation; 1998.2. Roh DD. Is atherogenesis accelerated in hemodialysis patients? Int J
Artif Organs. 1992;15:323–326.3. Charney DI, Walton DF, Cheung AK. Atherosclerosis in chronic
renal failure. Curr Opin Nephrol Hypertens. 1993;2:876 – 882.4. Ross R. The pathogenesis of atherosclerosis: a perspective for the
1990’s. Nature. 1993;362:801– 809.5. Gensini GF, Comegilo M, Colella A. Classical risk factors and
emerging elements in the risk profile for coronary artery disease.Eur Heart J. 1998;19:A53– 61.
6. Huysmans K, Lins R, Daelemans R, et al. Hypertension and accel-erated atherogenesis in endstage renal disease. J Nephrol. 1998;11:185–195.
7. Celermajer D. Endothelial dysfunction: does it matter? Is it revers-ible? J Am Coll Cardiol. 1997;30:325–333.
8. Wendelhag I, Liang Q, Gustavsson T, Wikstrand J. A new auto-mated computerized analyzing system simplifies readings and re-duces the variability in ultrasound measurement of intima-mediathickness. Stroke. 1997;28:2195–2200.
9. Pignoli P, Tremoli E, Poli A, et al. Intimal plus medial thickness ofthe arterial wall: a direct measurement with ultrasound imaging.Circulation. 1986;74:1399 –1406.
10. Hodis H. Reversibility of atherosclerosis— evolving perspectivesfrom two arterial imaging clinical trials: the cholesterol loweringatherosclerosis regression study and the monitored atherosclerosisregression study. J Cardiovasc Pharmacol. 1995;25:S25–S31.
11. Anderson T. Assessment and treatment of endothelial dysfunctionin humans. J Am Coll Cardiol. 1999;34:631– 638.
12. De Groot E, Jukema JW, van Swjndregt M, et al. B-Mode ultra-sound assessment of pravastatin treatment effect on carotid andfemoral artery walls and its correlations with coronary arterio-graphic findings: a report of the Regression Growth Evaluation Sta-tin Study (REGRESS). J Am Coll Cardiol. 1998;31:1561–1567.
13. Bots M, de Jong P, Hofman A, Grobbee D. Left, right, near or farwall common carotid intima-media thickness measurements: asso-
Table 4. Factors that Correlate with Increasing Intima-MedialThickness and Brachial Artery Reactivity among Patients withEnd-Stage Renal Disease
Risk Factor
Intima-MedialThickness
Brachial ArteryReactivity
r2 P r2 P
Age 0.19 ,0.001 — —Diabetes 0.07 0.003 0.06 0.004Peritoneal dialysis 0.05 0.02 0.01 0.37
Vascular Structure and Function in End-Stage Renal Disease/Kennedy et al
February 15, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 203

ciations with cardiovascular disease and lower extremity arterialatherosclerosis. J Clin Epidemiol. 1997;50:801– 807.
14. Sorensen K, Celermajer D, Spiegelhalter D, et al. Non-invasivemeasurement of human endothelium dependent arterial responses:accuracy and reproducibility. Br Heart J. 1995;74:247–253.
15. Atkov OY, Balahonova TV, Pogorelova OA. Non-invasive ultra-sound detection of endothelial dysfunction. Eur J Ultrasound. 1998;7:37– 45.
16. Kakuyama T, Kimura S, Hashiguchi Y. Fully automated determi-nation of HDL-cholesterol from human serum with Hitachi 911.Clin Chem. 1994;40:1104.
17. Araki A, Sako Y. Determination of free and total homocysteine inhuman plasma by high-performance liquid chromatography withfluorescence detection. J Chromatogr. 1987;422:43–52.
18. Adams M, Nakagomi A, Keech A, et al. Carotid intima-media thick-ness is only weakly correlated with the extent and severity of coro-nary artery disease. Circulation. 1995;92:2127–2134.
19. Hulthe J, Wikstrand J, Emanuelsson H, et al. Atheroscleroticchanges in the carotid artery bulb as measured by B-mode ultra-sound are associated with the extent of coronary atherosclerosis.Stroke. 1997;28:1189 –1194.
20. Mykkanen L, Zaccaro D, O’Leary D, et al. Microalbuminuria andcarotid artery intima-media thickness in nondiabetic and NIDDMsubjects. Stroke. 1997;28:1716.
21. Wikstrand J, Wendelhag I. Methodological considerations of ultra-sound investigation of intima-media thickness and lumen diame-ter. J Intern Med. 1994;236:555–559.
22. Salonen J, Salonen R. Ultrasound B-mode imaging in observationalstudies of atherosclerotic progression. Circulation. 1993;87:II-56 –II-65.
23. Bots M, Mulder P, Hofman A, et al. Reproducibility of carotid
vessel wall thickness measurements. The Rotterdam study. J ClinEpidemiol. 1994;47:921–930.
24. Touboul PJ, Prati P, Scarabin PY, et al. Use of monitoring softwareto improve the measurement of carotid wall thickness by B-modeimaging. J Hypertens. 1992;10:S37–S41.
25. Celermajer D, Sorensen K, Gooch V, et al. Non-invasive detectionof endothelial dysfunction in children and adults at risk of athero-sclerosis. Lancet. 1992;340:1111–1115.
26. van Guldener C, Lambert J, Janssen M, et al. Endothelium-depen-dent vasodilatation and distensibility of large arteries in chronichemodialysis. Nephrol Dial Transplant. 1997;12:14 –18.
27. Thambyrajah G, Landray MJ, McGlynn FJ, et al. Abnormalities ofendothelial function in patients with predialysis renal failure.Heart. 2000;83:205–209.
28. Hodis H, Mack W, Dunn M, et al. Intermediate-density lipopro-teins, and progression of carotid artery wall intima-media thick-ness. Circulation. 1997;95:2022–2026.
29. Megnien J, Simon A, Andriani A, et al. Cholesterol lowering therapy
inhibits the low-flow mediated vasoconstriction of the brachial ar-
tery in hypercholesterolaemic subjects. Br J Clin Pharmacol. 1996;
42:187–193.30. Parra HJ, Mezdour H, Cachera C, et al. Lp(a) lipoprotein in patients
with chronic renal failure treated by hemodialysis. Clin Chem. 1987;33:721.
31. Vaziri ND, Gonzales EC, Wang J, Said S. Blood coagulation, fi-brinolytic, and inhibitory proteins in end-stage renal disease: effectof hemodialysis. Am J Kidney Dis. 1994;23:828 – 835.
32. Westhuyzen J, Healy H. Biology and relevance of C-reactive proteinin cardiovascular and renal disease. Ann Clin Lab Sci. 2000;30:133–143.
Vascular Structure and Function in End-Stage Renal Disease/Kennedy et al
204 February 15, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110