Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, and Psychiatry 1996;61:485-490
Two domains of anosognosia in Alzheimer'sdisease
Sergio E Starkstein, Liliana Sabe, Erain Chemerinski, Laura Jason, Ramon Leiguarda
AbstractObjective-To examine the presence ofdifferent dimensions of unawareness inpatients with probable Alzheimer's dis-ease.Methods-A consecutive series of 170patients with probable Alzheimer's dis-ease were assessed with the anosognosiaquestionnaire-dementia (AQ-D) whichincludes items related to cognitive deficitsand behavioural problems.Results-A factor analysis of the AQ-Dproduced two factors: a "cognitiveunawareness" factor, which loaded onitems of memory, spatial and temporalorientation, calculation, abstract reason-ing, and praxis, and a "behaviouralunawareness" factor which loaded onitems of irritability, selfishness, inappro-priate emotional display, and instinctivedisinhibition. A stepwise forward regres-sion analysis showed significant correla-tions between the cognitive unawarenessfactor and more severe cognitive deficits,delusions, and apathy, but less depres-sion. On the other hand, the behaviouralunawareness factor correlated signifi-cantly with higher mania and pathologicallaughing scores. Whereas the cognitiveunawareness factor showed a significantcorrelation with cognitive tests assessingverbal comprehension and long termmemory, and was significantly associatedwith a longer duration of illness, no sig-nificant correlations were found betweenthe behavioural unawareness factor andthe neuropsychological tasks.Conclusion-Unawareness of cognitivedeficits and unawareness of behaviouralproblems may constitute independentphenomena in Alzheimer's disease.Whereas unawareness ofcognitive deficitsis related to the severity of intellectualimpairment and the presence of delu-sional apathetic mood, unawareness ofbehavioural problems may be part of adisinhibition syndrome.
(7 Neurol Neurosurg Psychiatry 1996;61:485-490)
Keywords: anosognosia; dementia; behaviour
Unawareness or the explicit denial of cognitivedeficits has often been reported in patientswith probable Alzheimer's disease. In a recentstudy that included a consecutive series of 103patients with Alzheimer's disease we found
that 20% had anosognosia, and a similarprevalence was reported by other authors."-5Most studies divided patients with Alzheimer'sdisease into groups with or without anosog-nosia based on the presence of unawarenessfor the cognitive (mainly memory) deficits.Whereas behavioural problems such as depres-sion, irritability, emotional lability, disinhibi-tion, and apathy are often found inAlzheimer's disease, whether patients withAlzheimer's disease may also show unaware-ness of behavioural problems has rarely beenexamined.
In a recent study, Vasterling et al6 reportedthat unawareness (measured as patient minuscare giver disagreement) was most prominentin ratings of memory and self care, less promi-nent in ratings of anxiety and irritability, andabsent in ratings of depression and health sta-tus. Whereas these findings suggest a dissocia-tion between unawareness of cognitive deficitsand unawareness of behavioural problems,Vasterling et al used an anosognosia instru-ment with unknown validity and reliability,cognitive and behavioural domains were arbi-trarily defined, and the low depression ratingsproduced by patients with Alzheimer's diseasemay have produced a "floor" effect thatexplains the low correlation between depres-sion and anosognosia scores.The mechanism of anosognosia in
Alzheimer's disease still remains unknown.Several studies showed that patients withAlzheimer's disease with anosognosia had sig-nificantly more severe deficits on "frontal loberelated" neuropsychological tests (such asset alternation tasks) compared with non-anosognosic patients with Alzheimer's dis-ease,7-8 but other studies could not replicatethose findings'5 One possibility is that anosog-nosia for cognitive deficits and anosognosia forbehavioural problems have different neuropsy-chological and psychiatric correlates. In thiscase, the association between anosognosia anddeficits in specific cognitive tasks may be pri-marily related to the prevalence of differentdomains of anosognosia within theAlzheimer's disease sample.The aim of this study was to determine the
presence of different domains of anosognosiain Alzheimer's disease. For this purpose weexamined a large sample of consecutivepatients with Alzheimer's disease using theanosognosia questionnaire-dementia (AQ-D).The AQ-D is a quantified scale with estab-lished reliability and validity in Alzheimer'sdisease, which includes questions about differ-ent cognitive deficits and behavioural prob-
Department ofBehavioral Neurologyand Neuropsychiatry,Raril Carrea InstituteofNeurologicalResearch, BuenosAires, ArgentinaS E StarksteinL SabeE ChemerinskiL JasonR LeiguardaCorrespondence to:Dr S E Starkstein,Rail Carrea Institute ofNeurological Research,Montafneses 2325, 1428Buenos Aires, Argentina.Received 4 December 1995and in final revised form3 July 1996Accepted 4 July 1996
485
on 3 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.5.485 on 1 N
ovember 1996. D
ownloaded from
Starkstein, Sabe, Chemerinski, Jason, Leiguarda
lems. ' To determine specific correlates ofanosognosic domains, patients were alsoassessed with a comprehensive neuropsycho-logical battery and a structured psychiatricevaluation.
Materials and methodsPATIENTSWe examined a consecutive series of 186patients who attended the neurology clinic ofour institute due to progressive cognitivedecline. The inclusion criteria were the follow-ing: (1) NINCDS-ADRDA criteria for proba-ble Alzheimer's disease,9 (2) normal results onlaboratory tests, (3) no history of closed headinjuries with loss of consciousness, strokes, orother neurological disorders with CNSinvolvement, (4) no focal lesions on CT orMRI, and (5) a Hachinski ischaemic score< 4.
PSYCHIATRIC EXAMINATIONAfter informed consent, patients were assessedby a psychiatrist with a comprehensive psychi-atric evaluation, which provided measure-ments of different behavioural domains suchas depression, anxiety, anosognosia, apathy,irritability, pathological affect, disinhibition,and delusions.
Structured clinical interview for DSM-III-R(SCID) "The SCID is a semistructured diagnosticinterview for making the major axis I DSM-III-R'2 diagnoses. The SCID was administeredby a psychiatrist blind to the remaining clinicaldata, and the interview was carried out withthe patient and at least one first degree rela-tive. Based on the SCID responses, DSM-III-Raxis I diagnoses were made.
Hamilton depression scale (HAM-D)"The HAM-D is a 17 item interviewer ratedscale that measures psychological and auto-nomic symptoms of depression.
Hamilton anxiety scale (HAM-A)'4The HAM-A is an 11 item interviewer ratedscale that measures the severity of generalisedor persistent anxiety.
Anosognosia questionnaire-dementia (AQ-D)'This instrument consists of 30 questionsdivided into two sections. The first sectionassesses intellectual functioning (for example,Do you have problems remembering dates?Do you have problems remembering tele-phone calls? etc), and the second sectionexamines changes in interests and personality(for example, Do you get easily irritated? Haveyou lost interest in things?) Each answer israted as never, 0 points; sometimes, 1 point;usually, 2 points; and always present, 3 points.Thus higher scores indicate more severeimpairments. Form A is answered by thepatient alone, and form B, a similar question-naire written in the third person, is answeredby the patient's care giver blind to the patient'sanswers in form A. The final score is the sub-
traction between scores in forms B and A.Thus positive scores indicate that the care-taker rated the patient as more impaired thanthe patient's own evaluation (the patient wasless aware of his or her cognitive or emotionaldeficits). We have demonstrated the reliabilityand validity of this scale in Alzheimer's dis-ease. I
Bech mania scale'5This scale assesses the severity of disinhibitionsymptoms.
Pathological laughing and crying scale(PLACS) 16This instrument is an interviewer rated scalethat quantifies aspects of pathological affect,including the duration of the episodes, theirrelation to external events, degree of voluntarycontrol, inappropriateness in relation to emo-tions, and degree of resultant distress. Boththe reliability and validity of this scale havebeen previously demonstrated. The scale isadministered to the patient and at least onefirst degree relative or care giver in close con-tact with the patient. The scale consists of 16items, eight assessing pathological laughter(PLACS-L) and eight assessing pathologicalcrying (PLACS-C), which are scored from 0to 3 points.
Apathy scale'7This scale includes 14 items which are scoredby the patient's relative or care giver. Eachquestion has four possible answers, which arescored from 0 to 3. Thus the apathy scalescore ranges from 0 to 42 points; and higherscores indicate more severe apathy. We havedemonstrated the reliability and validity of theapathy scale in Alzheimer's disease.'8
Irritability scale'8This is a 14 item scale which is rated by thepatient's relative or a care giver. Scores rangefrom 0 to 42, and higher scores indicate moresevere irritability. We have demonstrated thevalidity and reliability of this scale inAlzheimer's disease.'8
Dementia psychosis scale (DPS) 19This is an 18 item scale which quantifies theseverity and types of delusions in dementedpatients at the time of the psychiatric evalua-tion. This scale was rated by a psychiatristwith the patient and at least one close relativeor care giver
Functional independence measure (FIM)"'This instrument assesses self care, sphinctercontrol, mobility, locomotion, communica-tion, and social cognition on a low level scale.Higher scores indicate less impairments inactivities of daily living (ADLs).
NEUROPSYCHOLOGICAL EXAMINATIONThe neuropsychological evaluation was car-ried out by a neuropsychologist who was blindto the psychiatric data. The neuropsychologi-cal battery included tests that measureddeficits in different cognitive domains, such as
486
on 3 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.5.485 on 1 N
ovember 1996. D
ownloaded from
Two domains of anosognosia in Alzheimer's disease
verbal and visual memory, language, abstractreasoning, auditory attention, praxis, set alter-nation, and planning.
Mini mental state examination (MMSE)2'The MMSE is an 11 item examination thathas been found to be reliable and valid inassessing a limited range of cognitive func-tions.
Raven's progressive matrices (RPM)22The RPM assesses reasoning in the visualmodality. Patients are presented with a patternproblem with one part removed and severalpictured inserts, one of which contains thecorrect pattern. The patient has to select themissing piece to complete the pattern.
Wisconsin card sorting test23This test measures the ability to develop newconcepts and shift sets, and also requires thesubject to suppress a previously correctresponse and produce a new one. Assessmentof the overall proficiency of the test was judgedby the number of categories achieved (maxi-mum = 6).
Controlled oral word association test24This test examines access to semantic infor-mation with time constraint. Patients wereinstructed to name as many words beginningwith the letter F as they could in one minute.People's names and proper nouns were notpermitted. The letters A and S were then pre-sented successively, one minute being allowedfor each letter. The score was the number ofwords produced in one minute.
Digit span25This test examines auditory attention, andconsists of two parts. Both consist of sevenpairs of random sequences that the examinerpresents at the rate of one per second. In thefirst part (digits forward) the patient is askedto repeat a string of numbers exactly as it isgiven, and in the second (digits backwards)the patient is asked to repeat a string of num-bers in reversed order.
Buschke selective reminding test26This test measures verbal learning and mem-ory during a multiple trial list learning task.The patient listens to a list of words and has torecall as many words as possible. Each subse-
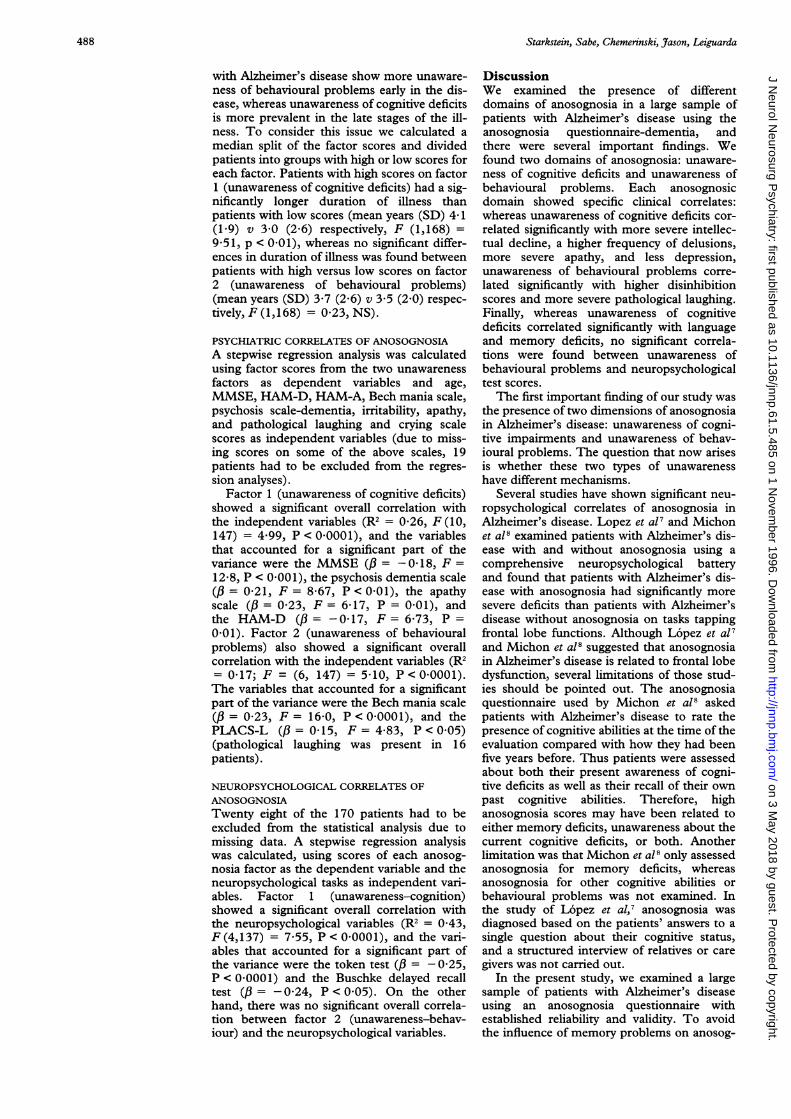
Anosognosia questionnaire-dementia: factor loadings (varimax normalised)
Item Factor I Factor 2
Recall of dates 0 75 0 01Orientation in new places 0-72 0 09Recall of telephone calls 0-62 0-08Recall of location of objects 0-67 0-18Handling money 0-69 0-18Recall of appointments 0-68 0-16Practice of hobbies 061 0-12Mental calculations 069 0-24Recall of shopping lists 070 0-06Understanding a movie 062 0-27Performance of household chores 066 0-17Performance of clerical work 0-65 0-23Increased selfishness 0-19 061Increased irritability 0-06 0-71Laughing inappropriately 0-12 0-60Increased sexual interest - 0-22 0-60
quent learning trial involves the selectivepreservation of only those words that were notrecalled on the immediately preceding trial.The final score was the delayed recall.
Token test27This test examines verbal comprehension ofsentences of increasing complexity.
Block design25This test examines the presence of construc-tional apraxia. Patients are presented with redand white blocks and are asked to constructreplicas of printed designs.
Similarities25This test provides a measure of abstract rea-soning.
STATISTICAL ANALYSISStatistical analysis was carried out usingmeans and SDs, multivariate analysis of vari-ance (ANOVA), and post hoc planned com-parisons. Frequency distributions werecompared using x2, Fisher tests, and contin-gency tables. A principal components factoranalysis for the AQ-D items was carried outusing varimax rotation. All P values are twotailed.
ResultsDue to lack of a care giver or relative whocould complete the AQ-D, 16 patients had tobe excluded from the study. Thus our sampleconsisted of 170 patients (1 14 women and 56men) with a mean age (SD) of 705 (5 4)years, a mean duration of illness (SD) of 3-6(2 3) years, a mean MMSE score (SD) of 18-8(6 6) points, and a mean (SD) AQ-D score of15-4 (21-0) points.The AQ-D items of the 170 patients were
entered into a principal factor analysis and atwo factor solution was derived. Factor 1 hadan eigenvalue of 9 34 and accounted for31 1% of the variance. This factor heavilyloaded on the following items (> 0 60): diffi-culties remembering dates, orienting to newplaces, remembering telephone calls, remem-bering location of objects in the house, han-dling money, remembering appointments,doing hobbies, performing mental calcula-tions, remembering a shopping list, under-standing the plot of a movie, carrying outhousehold chores, and carrying out clericalwork (table). Factor 2 had an eigenvalue of2-15 and accounted for 7-1% of the variance.This factor loaded on the following items(> 0.60): increased selfishness, increased irri-tability, laughing inappropriately, andincreased interest in sexual subjects (table).Thus whereas factor 1 may be construed as anunawareness of cognitive deficit factors includ-ing memory, temporal and spatial orientation,calculation, abstract reasoning, and praxis,factor 2 may be construed as an unawarenessof behavioural problem factors including self-ishness, irritability, inappropriateness of emo-tional display, and instinctive disinhibition.One important question is whether patients
487
on 3 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.5.485 on 1 N
ovember 1996. D
ownloaded from
Starkstein, Sabe, Chemerinski, Jrason, Leiguarda
with Alzheimer's disease show more unaware-ness of behavioural problems early in the dis-ease, whereas unawareness of cognitive deficitsis more prevalent in the late stages of the ill-ness. To consider this issue we calculated amedian split of the factor scores and dividedpatients into groups with high or low scores foreach factor. Patients with high scores on factor1 (unawareness of cognitive deficits) had a sig-nificantly longer duration of illness thanpatients with low scores (mean years (SD) 4 1(1 9) v 3 0 (2.6) respectively, F (1,168) =9-51, p < 0-01), whereas no significant differ-ences in duration of illness was found betweenpatients with high versus low scores on factor2 (unawareness of behavioural problems)(mean years (SD) 3-7 (2.6) v 3-5 (2 0) respec-tively, F (1,168) = 0 23, NS).
PSYCHIATRIC CORRELATES OF ANOSOGNOSIAA stepwise regression analysis was calculatedusing factor scores from the two unawarenessfactors as dependent variables and age,MMSE, HAM-D, HAM-A, Bech mania scale,psychosis scale-dementia, irritability, apathy,and pathological laughing and crying scalescores as independent variables (due to miss-ing scores on some of the above scales, 19patients had to be excluded from the regres-sion analyses).
Factor 1 (unawareness of cognitive deficits)showed a significant overall correlation withthe independent variables (R2 = 0-26, F (10,147) = 4 99, P < 0-0001), and the variablesthat accounted for a significant part of thevariance were the MMSE (, = -0 18, F =12.8, P < 0-001), the psychosis dementia scale(/3 = 0-21, F = 8-67, P < 0 01), the apathyscale (/ = 0-23, F= 6-17, P = 0-01), andthe HAM-D (/ = -0-17, F = 6-73, P =0-01). Factor 2 (unawareness of behaviouralproblems) also showed a significant overallcorrelation with the independent variables (R2= 0-17; F = (6, 147) = 5-10, P< 00001).The variables that accounted for a significantpart of the variance were the Bech mania scale(/3 = 0-23, F = 16-0, P < 0-0001), and thePLACS-L (/3 = 0 15, F = 4-83, P < 0 05)(pathological laughing was present in 16patients).
NEUROPSYCHOLOGICAL CORRELATES OFANOSOGNOSIATwenty eight of the 170 patients had to beexcluded from the statistical analysis due tomissing data. A stepwise regression analysiswas calculated, using scores of each anosog-nosia factor as the dependent variable and theneuropsychological tasks as independent vari-ables. Factor 1 (unawareness-cognition)showed a significant overall correlation withthe neuropsychological variables (R2 = 0.43,F (4,137) = 7-55, P < 0-0001), and the vari-ables that accounted for a significant part ofthe variance were the token test (/3 = - 025,P < 0 0001) and the Buschke delayed recalltest (/3 = -0-24, P < 0-05). On the otherhand, there was no significant overall correla-tion between factor 2 (unawareness-behav-iour) and the neuropsychological variables.
DiscussionWe examined the presence of differentdomains of anosognosia in a large sample ofpatients with Alzheimer's disease using theanosognosia questionnaire-dementia, andthere were several important findings. Wefound two domains of anosognosia: unaware-ness of cognitive deficits and unawareness ofbehavioural problems. Each anosognosicdomain showed specific clinical correlates:whereas unawareness of cognitive deficits cor-related significantly with more severe intellec-tual decline, a higher frequency of delusions,more severe apathy, and less depression,unawareness of behavioural problems corre-lated significantly with higher disinhibitionscores and more severe pathological laughing.Finally, whereas unawareness of cognitivedeficits correlated significantly with languageand memory deficits, no significant correla-tions were found between unawareness ofbehavioural problems and neuropsychologicaltest scores.The first important finding of our study was
the presence of two dimensions of anosognosiain Alzheimer's disease: unawareness of cogni-tive impairments and unawareness of behav-ioural problems. The question that now arisesis whether these two types of unawarenesshave different mechanisms.
Several studies have shown significant neu-ropsychological correlates of anosognosia inAlzheimer's disease. Lopez et al7 and Michonet al8 examined patients with Alzheimer's dis-ease with and without anosognosia using acomprehensive neuropsychological batteryand found that patients with Alzheimer's dis-ease with anosognosia had significantly moresevere deficits than patients with Alzheimer'sdisease without anosognosia on tasks tappingfrontal lobe functions. Although Lopez et a17and Michon et a18 suggested that anosognosiain Alzheimer's disease is related to frontal lobedysfunction, several limitations of those stud-ies should be pointed out. The anosognosiaquestionnaire used by Michon et al8 askedpatients with Alzheimer's disease to rate thepresence of cognitive abilities at the time of theevaluation compared with how they had beenfive years before. Thus patients were assessedabout both their present awareness of cogni-tive deficits as well as their recall of their ownpast cognitive abilities. Therefore, highanosognosia scores may have been related toeither memory deficits, unawareness about thecurrent cognitive deficits, or both. Anotherlimitation was that Michon et al8 only assessedanosognosia for memory deficits, whereasanosognosia for other cognitive abilities orbehavioural problems was not examined. Inthe study of L6pez et al,7 anosognosia wasdiagnosed based on the patients' answers to asingle question about their cognitive status,and a structured interview of relatives or caregivers was not carried out.
In the present study, we examined a largesample of patients with Alzheimer's diseaseusing an anosognosia questionnaire withestablished reliability and validity. To avoidthe influence of memory problems on anosog-
488
on 3 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.5.485 on 1 N
ovember 1996. D
ownloaded from

Two domains of anosognosia in Alzheimer's disease
nosia ratings, we asked our patients to ratetheir cognitive and behavioural problems asthey were at the time of the evaluation. Wecould not find a significant correlationbetween domains of anosognosia and frontallobe related tasks such as the Wisconsin cardsorting test or a verbal fluency task. In a recentstudy, Dalla Barba et al28 were also unable tofind a significant association between deficitson frontal lobe related tasks and anosognosiain Alzheimer's disease. However, we did find asignificant association between unawareness ofcognitive impairments and both the token testand the Buschke selective reminding test, aswell as a longer duration of illness, suggestingthat deficits of verbal memory and verbal com-prehension may play an important part in theproduction of this type of unawareness. Onthe other hand, there were no significant cor-relations between unawareness for behaviouralproblems and cognitive impairments, showingthat neuropsychological deficits may onlyaccount for some aspects of the anosognosiasyndrome in Alzheimer's disease.
Another important finding was that bothtypes of unawareness were significantly associ-ated with specific behavioural problems.Whereas unawareness of cognitive deficits wassignificantly correlated with more severe delu-sions and apathy and less depression,unawareness of behavioural problems was sig-nificantly correlated with more severe disinhi-bition and pathological laughing. In the past,anosognosia in Alzheimer's disease has beenvariably construed as the product of a defencemechanism protecting patients withAlzheimer's disease from depressive symp-toms,2 or as a behavioural manifestation of aspecific brain dysfunction.' The first theorywas based on significant, albeit mild, inversecorrelations between anosognosia and depres-sion scores-that is, less anosognosia withhigher depression scores-but other studiescould not replicate this correlation.' In arecent study we found that patients withAlzheimer's disease with dysthymia had signif-icantly lower anosognosia scores than non-depressed patients with Alzheimer's diseasesuggesting a greater association between rela-tively preserved awareness and more depres-sion.' However, we also found that patientswith Alzheimer's disease with major depres-sion had similar anosognosia scores that non-depressed patients with Alzheimer's disease,suggesting that some depressions inAlzheimer's disease are not related to thedegree of awareness. In the present study wefound a significant correlation betweenunawareness of cognitive deficits and depres-sion scores-that is, higher anosognosia withlower depression scores-suggesting a role fordepression in this type of anosognosia.However, depression did not account for a sig-nificant part of the variance in the correlationwith unawareness of behavioural problems,suggesting that anosognosia and depressionare not causally related.
Apathetic patients may be less reactive totheir surroundings as well as to their needs andemotions,29 and this decreased reactivity may
play a part in the production of anosognosia inAlzheimer's disease. Delusions are false beliefsthat are held despite contextual evidence tothe contrary, and constitute a frequent findingamong patients with Alzheimer's disease.'0Delusions in Alzheimer's disease may resultfrom dysfunction of polymodal associationareas involved in the assessment of thepatient's context,'0 and anosognosia mayoccur with further disruption of brain areasrelated to self assessment.We also found that unawareness of behav-
ioural problems was significantly correlatedwith higher disinhibition scores and moresevere pathological laughing. Thus unaware-ness of behavioural problems may be part of adisinhibition syndrome characterised by therelease of inappropriate behaviours such asgrandiose ideas, irritability, hyperactivity, andinappropriate emotional display. It is possiblethat the brain mechanism that controls theinhibition of behaviours may at the same timeactivate brain areas that mediate awarenessabout released or inhibited behaviours.Disruption of this system may result in a disin-hibition syndrome and anosognosia for behav-ioural problems.
There are clinical implications of our find-ings. Johnson and Orrell3" suggested thatpatients' perceptions about their illness maybe influenced by their own perception of thedisease, the treatment they receive, and thequality of psychiatric services and social sup-ports available to them. These importantissues should be considered in future studies.In a recent study that assessed insight in schiz-ophrenic patients, David et al32 suggested anindirect approach to help patients recognisetheir illness. Future studies should assess theutility of these techniques in patients withAlzheimer's disease, as these interventionsmay improve their quality of life and lessen thecare givers' burden.
In conclusion, we identified two domains ofanosognosia in Alzheimer's disease: unaware-ness of cognitive deficits and unawareness ofbehavioural problems, and we demonstrateddifferent cognitive and psychiatric correlatesfor these disorders. Future studies shouldexamine neuroradiological and neurometa-bolic correlates of these anosognosic domainsin Alzheimer's disease.
This study was partially supported by a grant from the RaulCarrea Institute of Neurological Research and the FundacionPerez Companc. We thank Dr J Paul Fedoroff for his mosthelpful comments.
1 Migliorelli R, Teson A, Sabe L, et al. Anosognosia inAlzheimer's disease: a study of associated factors. 7Neuropsychiatry Clin Neurosci 1995;7:338-44.
2 Reisberg B, Gordon B, McCarthy M. Insight and denialaccompanying progressive cognitive decline in normalaging and Alzheimer's disease. In: Stanley B, ed. Geriatricpsychiatry: ethical and legal issues. Washington, DC:American Psychiatric Press, 1985:19-39
3 Feher EP, Mahurin RK, Inbody SB, Crook TH, PirozzoloFJ. Anosognosia in Alzheimer's disease. Neuropsychiatry,Neuropsychology and Behavioral Neurology 199 1;4: 13646.
4 Sevush S, Leve N. Denial of memory deficit in Alzheimer'sdisease. Am Jf Psychiatry 1993;150:748-5 1.
5 Reed BR, Jagust WJ, Coulter L. Anosognosia inAlzheimer's disease: relationships to depression, cogni-tive function, and cerebral perfusion. J7 Clin ExpNeuropsychol 1993;15:231-44.
6 Vasterling JF, Seltzer B, Foss JF, Vanderbrook V.Unawareness of deficit in Alzheimer's disease: domain-specific differences and disease correlates. Neuro-
489
on 3 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.5.485 on 1 N
ovember 1996. D
ownloaded from

Starkstein, Sabe, Chemerinski, J3ason, Leiguarda
psychiatry, Neuropsychology, and Behavioral Neurology1995;8:26-32.
7 L6pez OL, Becker JT, Somsak D, Dew MA, DeKosky ST.Awareness of cognitive deficits in probable Alzheimer'sdisease. Eur Neurol 1993;34:277-82.
8 Michon A, Deweer B, Pillon B, Agid Y, Dubois B. Relationof anosognosia to frontal lobe dysfunction in Alzheimer'sdisease. _7 Neurol Neurosurg Psychiatry 1994;57:805-9.
9 McKhann G, Drachman D, Folstein MF, Katzman R,Price D, Stadlan EM. Clinical diagnosis of Alzheimer'sdisease: report of the NINCDS-ADRDA Work Groupunder the auspices of Department of Health and HumanServices Task Force on Alzheimer's Disease. Neurology1984;34:939-44.
10 Hachinski VC, Iliff LD, Zilhka L, et el. Cerebral blood flowin dementia. Arch Neurol 1975;40:97-103.
11 Spitzer RL, Williams JBW, Gibbon M, First MB. Thestructured clinical interview for DSM-III-R SCID. I: his-tory, rationale, and description. Arch Gen Psychiatry1992;49:624-9.
12 American Psychiatric Press. Diagnostic and statistical manualof mental disorders. 3rd ed, revised. Washington, DC:APA, 1987.
13 Hamilton MA. A rating scale for depression. Neurol
Neurosurg Psychiatry 1960;23:56-62.14 Hamilton MA. The assessment of anxiety states by rating.
BrJMed Psychol 1959;32:50-5.15 Bech P, Kastrup M, Rafaelsen OJ. Mini-compendium of
rating scales for states of anxiety, depression, mania,schizophrenia, with corresponding DSM-III syndromes.Acta Psychiatr Scand 1986;73(suppl 236):29-31.
16 Robinson RG, Parikh RM, Lipsey JR, Starkstein SE, PriceTR. Pathological laughing and crying following stroke:validation of measurement scale and double blind treat-ment study. AmJ7Psychiatry 1993;150:286-93.
17 Starkstein SE, Mayberg HS, Preziosi TJ, AndrezejewskiMA, Leiguarda R, Robinson RG. Reliability, validity,and clinical correlates of apathy in Parkinson's disease.Neuropsychiatry Clin Neurosci 1992;4: 134-9.
18 Starkstein SE, Migliorelli R, Manes F, et al. The prevalence
and clinical correlates of apathy and irritability inAlzheimer's disease. Journal of European Neurology 1995;2:540-6.
19 Migliorelli R, Petracca G, Teson A, Sabe L, Leiguarda R,Starkstein SE. Neuropsychiatric and neuropsychologicalcorrelates of delusions in Alzheimer's disease. PsycholMed 1995;25:505-13.
20 Granger CV, Hamilton BB, Kayton R. Guide for use of theuniform data set for medical rehabilitation. Unifornm data sys-
tem for medical rehabilitation. Buffalo: 1986.21 Folstein MF, Folstein SE, McHugh PR. Mini-mental state:
a practical method for grading the cognitive state ofpatients for the clinician. J Psychiatr Res 1975;12:189-98.
22 Raven JC, Court JH, Raven J. Manual for Raven's progres-sive matrices and vocabulary scales. London: HK Lewis,1986.
23 Nelson HE. A modified card sorting test sensitive to frontallobe defects. Cortex 1976;12:313-24.
24 Benton AL. Differential behavioral effects in frontal lobedisease. Neuropsychology 1968;6:53-60.
25 Wechsler D. Wechsler adult intelligence scale manual. NewYork: Psychological Corporation, 1955.
26 Buschke H, Fuld PA. Evaluating storage, retention, andretrieval in disordered memory and learning. Neurology1974;24:1019-25.
27 De Renzi E, Faglioni P. Development of a shortened ver-sion of the token test. Cortex 1978;14:41-9.
28 Dalla Barba G, Parlato V, Iavarone A, Boller F. Anosog-nosia, intrusions and 'frontal' functions in Alzheimer'sdisease and depression. Neuropsychology 1995;33:247-59.
29 Marin RS. Apathy: a neuropsychiatric syndrome. .7
Neuropsychiatry Clin Neurosci 1991;3:243-54.30 Starkstein SE, Vazquez S, Petracca G, Teson A, Migliorelli
R, Leiguarda R. A SPECT study of delusions inAlzheimer's disease. Neurology 1994;44:2055-9.
31 Johnson S, Orrell M. Insight: a social perspective. PsycholMed 1995;25:515-20.
32 David A, Buchanan A, Ried A, Almeida 0. The assessmentof insight in psychosis. Br _7 Psychiatry 1992;161:599-602.
490
on 3 May 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.61.5.485 on 1 N
ovember 1996. D
ownloaded from