Embed Size (px)
Citation preview
Acta Obstet Gynecol Scand 2000; 79: 631–634 Copyright C Acta Obstet Gynecol Scand 2000
Printed in Denmark ¡ All rights reservedActa Obstetricia et
Gynecologica ScandinavicaISSN 0001-6349
ORIGINAL ARTICLE
Doppler ultrasound of the maternal uterinearteries: disappearance of abnormalwaveforms and relation to birthweight andpregnancy outcomeSTUART CAMPBELL1, REBECCA S. BLACK1, CHRISTOPH C. LEES2, VALERIE ARMSTRONG2 AND JANET L. PEACOCK3
From the Academic Departments of 1Obstetrics and Gynaecology and 3Public Health Sciences, St George’s Hospital MedicalSchool, London, and the 2Department of Obstetrics and Gynaecology, King’s College Hospital, London, United Kingdom
Acta Obstet Gynecol Scand 2000; 79: 631–634. C Acta Obstet Gynecol Scand 2000
Background. To assess whether the gestation at which abnormal uterine artery waveformsdisappear is related to birthweight and complications of pregnancy.Methods. A prospective study of outcome of pregnancy after a uterine artery Doppler screen-ing program set in an inner city teaching hospital. One thousand five hundred and twenty-four consecutive women attending the Obstetric Department for a routine anomaly scan atbetween 19 and 21 weeks gestation had maternal uterine arteries assessed using color waveDoppler. Those women in whom the flow was deemed abnormal were recalled for a furtherscan at 24–26 weeks gestation. The main outcome measures were birthweight, gestation atdelivery and incidence of pre eclampsia.Results. The women in whom the uterine artery blood flow was normal at 20 weeks hadbabies with significantly higher mean birthweight than those who normalized between 20 and24–26 weeks gestation (‘late normalizers’) after adjustment for confounding factors; ges-tational age, maternal height, parity, ethnic group and smoking (mean differenceΩ173 g, 95%confidence intervals 42 to 303 g).Conclusions. The timing of trophoblast invasion, as reflected by abnormal uterine arterywaveforms, may have an effect on birthweight.
Key words: birthweight; Doppler ultrasound; pre eclampsia; uterine artery
Submitted 15 April, 1999Accepted 28 September, 1999
Factors contributing to the weight of the fetus atbirth have been studied extensively (1–3). Themain variables affecting birthweight are consideredto be: gestational age at delivery, maternal height,sex of infant, parity, ethnic origin and smoking. Inthis study we investigate whether another mechan-ism could be added to this list: the timing of tro-phoblast invasion.
Abbreviations:IUGR: intra uterine growth restriction; Cauc: Caucasian; AC:Afro-Caribbean; s.d.: standard deviation; RI: resistance index;BW: birthweight; CI: confidence interval.
C Acta Obstet Gynecol Scand 79 (2000)
Invasion of maternal tissue by the fetal tropho-blast is essential for the establishment of a viablepregnancy. Normally, the trophoblast induces con-version of the maternal spiral arteries from theirnon-pregnant state in two stages. Decidual seg-ments are converted by a wave of endovascular tro-phoblast migration in the first trimester, and thenmyometrial segments by a subsequent wave in thesecond trimester (4). However, failure of adequatematernal spiral artery invasion is known to be as-sociated with an increased risk of diseases of thetrophoblast – pre eclampsia, IUGR and placentalabruption. Histological studies have shown that in
632 S. Campbell et al.
pregnancies where there is intra uterine growth re-striction, there is a marked decrease in the amountand quality of trophoblast invasion and a decreasein the feto-maternal surface area (5). Invading tro-phoblast cells from pre eclamptic pregnancies ap-pear to fail to express adhesion molecules presentin cells from normal pregnancies (6). The reasonsfor this abnormality of trophoblast invasion arestill unclear, but the resulting high resistance to ut-ero placental flow can be detected through Dopp-ler ultrasound of the maternal uterine arteries. Ahigh resistance index and bilateral early diastolicnotching at 24 weeks gestation, for example, had apositive predictive value of 50% for pre eclampsia(7).
At King’s College Hospital in 1995, all women at-tended for an ultrasound scan at 20 weeks gestation,and at this time continuous wave Doppler measure-ments of the uterine arteries were made. All womenin whom there was suboptimal Doppler velocimetrywere recalled for further assessment at 24–26 weeksgestation, by color and pulsed wave Doppler im-aging. Suboptimal blood flow patterns were definedas the existence of unilateral or bilateral notching,and/or a mean resistance index (RI) of greater than0.6, two standard deviations above the mean.
The aim of this study was to relate uterine arteryDoppler indices to pregnancy outcome. In particu-lar, we were interested in investigating the effect onbiological and clinical outcome for the group ofwomen in whom relatively later normalization ofthe uterine artery waveform occurred. We there-fore compared women who had abnormal Dopplerparameters at 20 weeks gestation, which had nor-malized by 24–26 weeks, with those in whom anormal blood flow pattern had already been estab-lished by 20 weeks of gestation, and those whoseparameters were persistently abnormal.
Materials and methods
One thousand five hundered and twenty-four con-secutive women attending King’s College Hospitalin 1995 for a routine anomaly scan at between 19and 21 weeks gestation were included in this study.At the time of the anomaly scan, continuous waveDoppler assessment of the maternal uterine arter-ies was also carried out with a 4MHz continuous-wave probe (Doptek Ltd, Chichester, UK). Thosewomen in whom the blood flow was deemed sub-optimal were recalled for a further scan at 24–26weeks gestation. The scans were performed by oneof two operators (RSB or CCL). On this occasion,color wave Doppler imaging (Acuson 128 5-MHzlinear transducer (Acuson, Mountain View, CA))of the uterine arteries was performed as previouslydescribed (8).
C Acta Obstet Gynecol Scand 79 (2000)
Once all the women had delivered, ultrasound,demographic and pregnancy outcome data werecollected from hospital records.
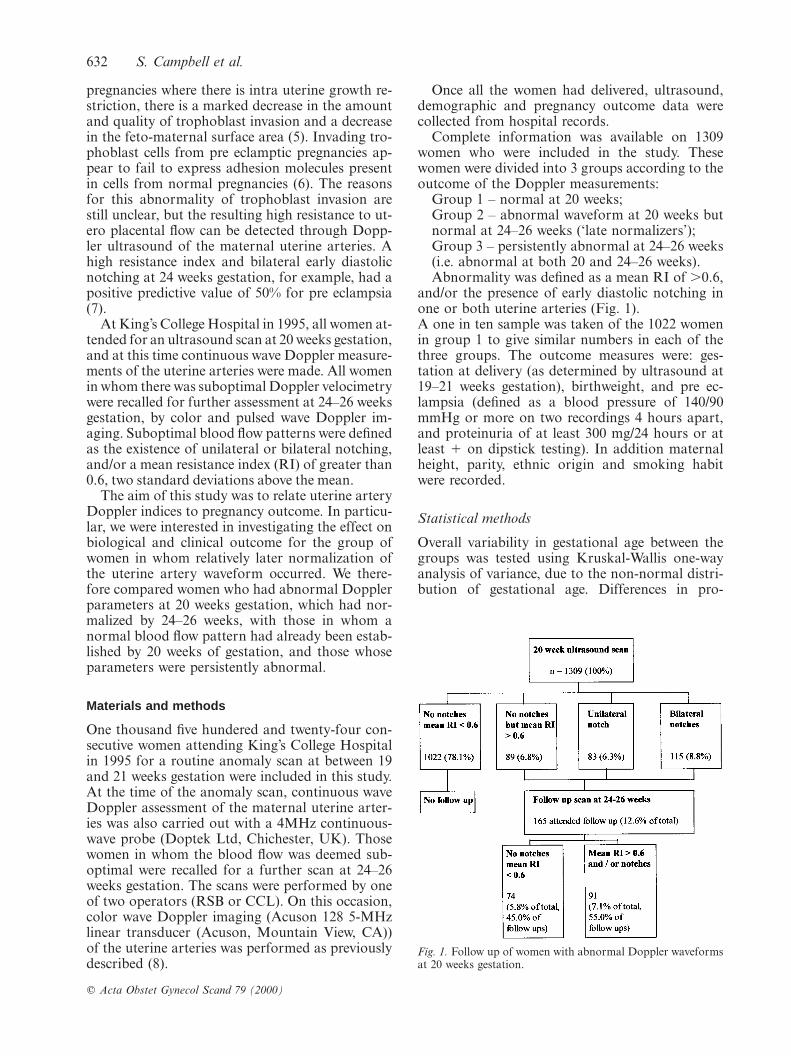
Complete information was available on 1309women who were included in the study. Thesewomen were divided into 3 groups according to theoutcome of the Doppler measurements:
Group 1 – normal at 20 weeks;Group 2 – abnormal waveform at 20 weeks butnormal at 24–26 weeks (‘late normalizers’);Group 3 – persistently abnormal at 24–26 weeks(i.e. abnormal at both 20 and 24–26 weeks).Abnormality was defined as a mean RI of .0.6,
and/or the presence of early diastolic notching inone or both uterine arteries (Fig. 1).A one in ten sample was taken of the 1022 womenin group 1 to give similar numbers in each of thethree groups. The outcome measures were: ges-tation at delivery (as determined by ultrasound at19–21 weeks gestation), birthweight, and pre ec-lampsia (defined as a blood pressure of 140/90mmHg or more on two recordings 4 hours apart,and proteinuria of at least 300 mg/24 hours or atleast π on dipstick testing). In addition maternalheight, parity, ethnic origin and smoking habitwere recorded.
Statistical methods
Overall variability in gestational age between thegroups was tested using Kruskal-Wallis one-wayanalysis of variance, due to the non-normal distri-bution of gestational age. Differences in pro-
Fig. 1. Follow up of women with abnormal Doppler waveformsat 20 weeks gestation.
Uterine artery Doppler and birthweight 633
Table I. Maternal characteristics for the three groups
EthnicityPrimi- Mean Mean
Cauc AC Other parae height weight SmokingGroup No. (%) (%) (%) (%) (cm) (kg) (%)
1 99 51 41 8 41 162.4 66.4 13.02 74 41 49 11 54 161.4 65.3 14.73 91 51 41 9 54 162.0 65.1 22.6
Group 1Ωnormal uterine artery blood flow at 20 weeks, Group 2Ωabnormalat 20 weeks but normal at 24–26 weeks, Group 3Ωpersistently abnormal at24–26 weeks. (CaucΩCaucasian, ACΩAfro-Caribbean).
Table II. Outcome measures for the three groups
Pre eclampsia Mean gestation Mean birthweightGroup No. (%) (s.d.)/weeks (s.d.)/g
Group 1 99 0 39.73 (1.89) 3446 (542)Group 2 74 0 39.74 (2.07) 3241 (530)Group 3 91 13 38.71 (3.13) 2892 (740)
p-value p,0.001 pΩ0.03 p,0.001(group 3 vs group 1)
portions (pre eclampsia) were compared usingFisher’s Exact Test. Mean (unadjusted) birthweightin the three groups was compared using analysisof variance. Multiple regression was used to com-pare the groups after adjusting for the five factorsknown to be related to birthweight. The factorswere: gestational age, maternal height, parity (pri-miparae/multiparae), ethnic origin (Caucasian/Afro-Caribbean/other) and smoking (non-smoker/smoker). Adjusted mean birthweights are pre-sented by adjusting to 40 weeks gestational age,160 cm maternal height, primiparity, Caucasian,non-smoker. Differences, 95% confidence intervalsand p-values are presented for mean birthweight inthe normal group (group 1) compared with theother two groups. Analyses were performed usingSTATA (STATA Corporation, Texas, USA) andepi-info V6 (CDC Atlanta, GA, USA).
Table III. Unadjusted and adjusted birthweights in the three groups. Adjustments were for gestational age, maternal height, parity, ethnic group and smoking
Mean BW Difference in BWGroup No. (g) from group 1 (g) 95% CI p value
1 99 unadjusted 3446 ª ª ªadjusted 3458 ª ª ª
2 74 unadjusted 3241 205 24 to 387 0.03adjusted 3285 173 42 to 303 0.01
3 91 unadjusted 2892 554 383 to 725 ,0.0001adjusted 3088 370 245 to 494 ,0.0001
(BWΩbirthweight)
C Acta Obstet Gynecol Scand 79 (2000)
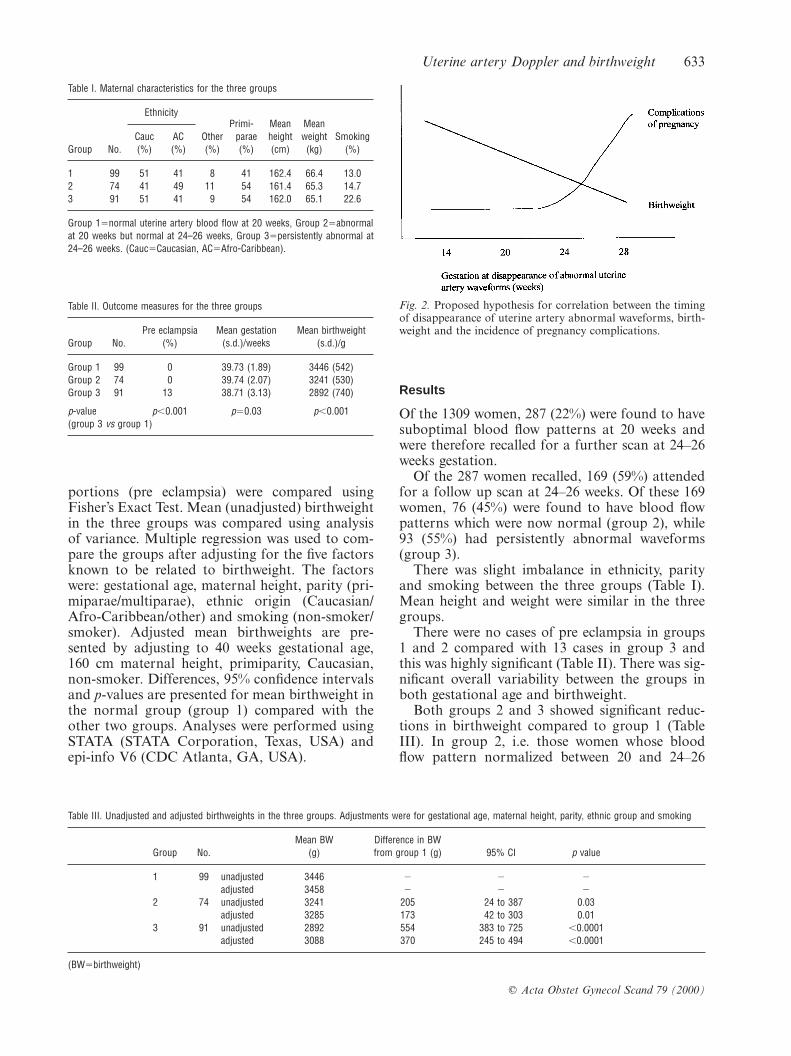
Fig. 2. Proposed hypothesis for correlation between the timingof disappearance of uterine artery abnormal waveforms, birth-weight and the incidence of pregnancy complications.
Results
Of the 1309 women, 287 (22%) were found to havesuboptimal blood flow patterns at 20 weeks andwere therefore recalled for a further scan at 24–26weeks gestation.
Of the 287 women recalled, 169 (59%) attendedfor a follow up scan at 24–26 weeks. Of these 169women, 76 (45%) were found to have blood flowpatterns which were now normal (group 2), while93 (55%) had persistently abnormal waveforms(group 3).
There was slight imbalance in ethnicity, parityand smoking between the three groups (Table I).Mean height and weight were similar in the threegroups.
There were no cases of pre eclampsia in groups1 and 2 compared with 13 cases in group 3 andthis was highly significant (Table II). There was sig-nificant overall variability between the groups inboth gestational age and birthweight.
Both groups 2 and 3 showed significant reduc-tions in birthweight compared to group 1 (TableIII). In group 2, i.e. those women whose bloodflow pattern normalized between 20 and 24–26

634 S. Campbell et al.
weeks (‘late normalizers’), the mean birthweightwas over 200 g lower than those with a normal 20week scan (group 1). When adjusted for con-founding factors, this was reduced to 173 g butremained significant (pΩ0.01).
Discussion
We were particularly interested in the outcomes ofthe uterine artery ‘late normalizers’ group (group2); their pregnancy course has to date not beenproperly characterized. In this group, the mean ad-justed birthweight was 173 g less than in group 1,in whom the uterine artery blood flow was alreadyentirely normal at 20 weeks gestation. This com-pares to the effects of other known factors affect-ing birthweight (adjusted for confounding vari-ables): a reduction of approximately 200–250 g forsmoking, an increase of 108–150 g for a parity ofbetween 1 and 4 compared to primiparity, and adecrease of up to 186 g for ethnic origins otherthan Caucasian (2, 3). The timing of the disappear-ance of abnormal uterine artery waveforms thusappears to be another important factor affectingbirthweight. It may be that in these ‘late normal-izers’ the second wave of trophoblast invasion isdelayed, resulting in less placental perfusion duringthe end of the second trimester, or is in some waydefective, leading to an impaired uteroplacentalcirculation for the remaining duration of gestation.Our study did not, however, demonstrate an effectof this ‘late normalization’ on the incidence of preeclampsia or the gestational age at delivery.
We have shown similar results in terms of thepercentage of women recalled for follow up, thosewith persistent abnormal uterine artery waveformsat 24–26 weeks and the subsequent development ofpre eclampsia as seen in previous studies (7, 8). Thelowest adjusted mean birthweight was found in thegroup with persistently abnormal Doppler wave-forms group (group 3).
It may be that there is a correlation betweennotch disappearance and birthweight over a muchwider range of gestation than we have demon-strated here. We have simply investigated the ges-tation range 20–26 weeks over which changes inthe uterine artery flow velocity waveform oc-curred. Furthermore, there may be a correlation
C Acta Obstet Gynecol Scand 79 (2000)
between notch disappearance and the likelihood ofpregnancy complications (Fig. 2). This may be acontinuum, or there may be a ‘cut-off point’ atwhich such problems are more likely. The gestationat which uterine artery waveforms ‘normalize’could be expected to be inversely correlated withbirthweight. A larger, prospective study is neededto investigate possible variations in the occurrenceof pre eclampsia and other diseases of the tropho-blast in relation to the timing of the disappearanceof abnormal waveforms.
References
1. Thomson AM, Billewicz WZ, Hytten FE. The assessmentof fetal growth. J Obstet Gynaecol Br Commonw 1968; 75:903–16.
2. Brooke OG, Anderson HR, Bland JM, Peacock JL, StewartCM. Effects on birth weight of smoking, alcohol, caffeine,socioeconomic factors, and psychosocial stress. Br Med J1989; 298: 795–801.
3. Gardosi J, Mongelli M, Wilcox M, Chang A. An adjustablefetal weight standard. Ultrasound Obstet Gynecol 1995; 6:168–74.
4. Khong TY, De Wolf F, Robertson WB, Brosens I. Inad-equate maternal vascular response to placentation in preg-nancies complicated by pre-eclampsia and by small-for-ges-tational-age infants. Br J Obstet Gynaecol 1986; 93: 1049–59.
5. Macara L, Kingdom JC, Kaufmann P, Kohnen G, Hair J,More IA et al. Structural analysis of placental terminal villifrom growth-restricted pregnancies with abnormal umbili-cal Doppler waveforms. Placenta 1996; 17: 37–48.
6. Zhou Y, Damsky CH, Fisher SJ. Pre eclampsia is associ-ated with failure of human cytotrophoblasts to mimic avascular adhesion phenotype. One cause of defective endo-vascular invasion in this syndrome? J Clin Invest 1997; 99:2152–64.
7. Harrington K, Cooper D, Lees C, Hecher K, Campbell S.Doppler ultrasound of the uterine arteries: the importanceof bilateral notching in the prediction of pre-eclampsia, pla-cental abruption or delivery of a small-for-gestational-agebaby. Ultrasound Obstet Gynecol 1996; 7: 182–8.
8. Bower S, Bewley S, Campbell S. Improved prediction of preeclampsia by two-stage screening of uterine arteries usingthe early diastolic notch and color Doppler imaging. ObstetGynecol 1993; 82: 78–83.
Address for correspondence:
R. S. Black, M.R.C.O.G.Academic Department of Obstetrics and GynaecologySt George’s Hospital Medical SchoolCranmer TerraceLondon SW17 0REUK.