Embed Size (px)
Citation preview

Dose-Intensification of Procarbazine, CCNU (Lomustine), Vincristine (PCV)With Peripheral Blood Stem Cell Support in Young Patients With Gliomas
Regina I. Jakacki, MD,1* Cheryl Jamison, RN, CPNP,1 Vincent P. Mathews, MD,3
Douglas K. Heilman,4 Edward Dropcho, MD,5 Ken Cornetta, MD,6
David R. Macdonald, MD,7 and David A. Williams, MD1,2
Background. The regimen of procarbazine,CCNU, and vincristine is active against glio-mas. Previous attempts at dose-intensificationhave been unsuccesful because of delayed andcumulative myelosuppression. We sought todetermine whether peripheral blood stem cell(PBSC) infusions would allow dose-escalationand time compression. Procedure. Eleven pa-tients, age 2.8–35.9 years, with newly diag-nosed (n = 10) or recurrent (n = 1) gliomasunderwent PBSC harvesting after mobilizationwith G-CSF. Chemotherapy consisted of CCNU130 mg/m2 on day 0, vincristine 1.5 mg/m2 ondays 0 and 7, and procarbazine 150 mg/m2 ondays 1–7. PBSCs were reinfused on day 9 ofeach course. Four courses of chemotherapywere administered 28 days apart or whencounts recovered. Involved field radiation wasadministered to newly diagnosed high-grade
glioma patients following recovery from che-motherapy. Results. Compared to the standardPCV regimen given every 6 weeks, dose inten-sity received was 1.7- and 1.8-fold greater forCCNU and procarbazine. Chemotherapy wasdelivered on time in 33/41 (80.5%) courses.Four courses (9.8%) were complicated by ab-solute neutrophil counts <200/µL; platelet na-dirs < 50,000/µL occurred in two courses(4.9%). Fever with neutropenia complicatedthree courses. Eight of 9 patients with measur-able disease had an objective decrease in tu-mor size and/or decreased enhancement. Me-dian survival for patients with high-grade glio-mas (n = 6) was 13 months. Conclusions. Dose-intensification of PCV is possible using PBSCs.Med. Pediatr. Oncol. 31:483–490, 1998.© 1998 Wiley-Liss, Inc.
Key words: gliomas; procarbazine; CCNU; dose-intensity; peripheral blood stem cell
INTRODUCTION
A correlation between dose intensity (defined as theamount of drug delivered per unit time) and treatmentoutcome, in terms of both response and survival, hasbeen demonstrated in several clinical trials involvingvarious malignancies [1–3]. Greater dose intensity can beaccomplished not only by increasing dose, but by de-creasing the time interval between courses of chemo-therapy. Indeed, models of chemotherapy utility based onfractional cell kill predict increased efficacy with shortertime intervals between chemotherapy administrations [4].
The combination regimen of procarbazine, 1-(2-chloroethyl)-3-cyclohexyl-1-nitrosourea (CCNU) andvincristine (PCV) has been used for malignant brain tu-mors since the 1970s and is considered by many to bestandard chemotherapy for high-grade gliomas. PCV isthe only combination regimen shown to be more effec-tive than BCNU alone in a randomized clinical trial [5].The standard PCV regimen consists of 110 mg/m2 ofCCNU on day 1 followed by 60 mg/m2/d of procarbazineon days 8–21, with courses given every 6 to 8 weeks.Myelosuppression is dose-limiting for both chloroethyl-nitrosoureas (CENUs) and procarbazine [6]. The nadir inblood counts is later than with most other chemothera-
1Section of Pediatric Neuro-Oncology, Department of Pediatrics,James Whitcomb Riley Hospital for Children, Indianapolis, Indiana2Herman B.Wells Center for Pediatric Research, Indianapolis, Indiana3Department of Radiology, Indiana University Medical Center, India-napolis, Indiana4Department of Biostatistics, Indiana University Medical Center, In-dianapolis, Indiana5Department of Neurology, Indiana University Medical Center, India-napolis, Indiana6Division of Hematology/Oncology, Department of Medicine, IndianaUniversity Medical Center, Indianapolis, Indiana7Departments of Clinical Neurological Sciences and Oncology, Uni-versity of Western Ontario, London, Canada
Grant sponsor: NCI; Grant number: P01CA59348; Grant sponsor:Center of Excellence in Molecular Hematology; Grant number:NIDDK P50DK49218.
*Correspondence to: Regina I. Jakacki, M.D., Section of PediatricNeuro-Oncology, Riley Hospital for Children, Room 0903, 702 Barn-hill Dr., Indianapolis, IN 46202-5225.E-mail: [email protected]
Received 3 December 1997; Accepted 12 May 1998
Medical and Pediatric Oncology 31:483–490 (1998)
© 1998 Wiley-Liss, Inc.

peutic regimens and the marrow suppression becomesmore severe with each subsequent course of chemo-therapy. Cairncross et al. attempted to increase the dosesof CCNU (130 mg/m2) and procarbazine (75 mg/m2/d ×14 days) without growth factor support in patients witholigodendrogliomas [7]. There were frequent dose reduc-tions and delays for hematologic toxicity. Only 25% ofcourses were able to be administered on time (6 weeksapart) and the actual dose-intensity was no different thanthe standard PCV regimen.
The currently available growth factors shorten the du-ration of neutropenia but have little effect on plateletrecovery, thereby limiting the ability to increase dose-intensity [8,9]. Since CENUs appear to be extremelytoxic to primitive hematopoietic stem and progenitorcells [10], we sought to determine whether the use ofperipheral blood stem cells could reduce the hematologictoxicity associated with the intensified regimen used byCairncross et al. In addition, we sought to further inten-sify this regimen by administering the chemotherapycourses every 4 weeks rather than every 6 weeks.
METHODSPatient Selection
Study eligibility included the diagnosis of one of thefollowing: high-grade glial tumors, unresectable oligo-dendrogliomas, or brainstem tumors where the majorityof the tumor was intrinsic to the pons and/or medulla.Histologic verification was required unless the tumorwas entirely intrinsic to the brainstem. Patients were noteligible if they had received prior chemotherapy. Patientshad to have adequate renal, liver, and pulmonary func-tion. A minimum weight of 10 kg and an ECOG Perfor-mance Status of 0–2 was required. Patients and/or par-ents signed a written informed consent approved by theInstitutional Review Board of Indiana University.
Peripheral Blood Stem Cell Mobilization, Collection,and Storage
Upon study entry, G-CSF (10 mcg/kg) was give sub-cutaneously for 4 days prior to leukapheresis. Two pa-tients received less than 4 days of G-CSF priming be-cause of deteriorating clinical status. Leukapheresis wasperformed through a tunnelled double lumen venous di-alysis catheter. Peripheral blood stem cells were col-lected using the Cobe Spectra or the Baxter CS 3000machine. A minimum of 16 × 108 mononuclear cells(MNC)/kg were harvested. G-CSF was continued dailyuntil sufficient cells were collected. The pheresis ma-chine was primed with packed red blood cells for patientsweighing less than 25 kg. PBSCs were divided into ali-quots and cryopreserved in 10% dimethyl sulfoxide us-ing controlled-rate freezing at approximately one degree
centigrade/minute and stored at −196°C. The CD34+ cellcontent was determined by flow cytometric analysis.
Treatment Regimen
Chemotherapy was begun as soon as a minimum of 16× 108 MNC/kg were collected. Four courses of chemo-therapy were given 4 weeks apart and/or when the ANCwas >1000/mL and platelets >100,000/mL. Chemo-therapy consisted of CCNU (130 mg/m2) orally on day 0,vincristine (1.5 mg/m2, maximum 2.0 mg) intravenouslyon day 0 and 7, and procarbazine (150 mg/m2/day) orallyon days 1–7. No dose reductions for hematologic toxicitywere allowed. Vincristine was held or the dose reducedin the presence of foot drop, paresis or ileus. Procarba-zine-related rashes were treated with antihistamines andsteroids if necessary. Patients who developed a rash re-ceived diphenhydramine prior to subsequent doses ofprocarbazine, which was discontinued only if mucosalinvolvement developed. A minimum of 4 × 108 MNC/kgwas reinfused 36–48 hours following the last dose ofprocarbazine during each course. Intravenous hydrationwas administered for 4–6 hours following the reinfusionof PBSCs. Four weeks after the last course of chemo-therapy and following recovery of blood counts, newlydiagnosed patients with high-grade gliomas received in-volved field radiation therapy in 180 cGy fractions todoses ranging from 5,040–5,940 cGy.
Pre-treatment evaluation included an MRI scan withand without gadolinium; history and physical examina-tion with documentation of all neurologic deficits; bloodcounts, chemistries and urinalysis; pulmonary functiontesting and creatinine clearance. Decadron doses wererecorded at the time of all MRI scans and clinic visits.During treatment, CBCs were done twice weekly andchemistries done weekly. Following completion of alltherapy, patients were followed with serial MRI scansand physical and neurologic evaluations.
Supportive Care
Transfusions of irradiated, Pall-filtered blood productswere used to maintain a hemoglobin above 8.0 gm/dl andplatelets above 30,000–50,000/mL. Growth factor was tobe used only in the setting of serious infection and neu-tropenia. Antiemetics were given prior to each dose ofCCNU and procarbazine and as needed otherwise.Decadron was tapered as rapidly as possible after startingtreatment, and patients were maintained on the lowestdose possible.
Evaluation of Response
MRI scans with and without gadolinium were ob-tained prior to the third course of chemotherapy and 4weeks after the last course of chemotherapy. Tumor mea-surements and response designations were determined
484 Jakacki et al.

following completion of therapy by a neuroradiologist(VM) who was blinded to the clinical status of the pa-tients. Tumor size was determined by multiplying thelargest cross-sectional diameters in each dimension (an-terior-posterior, craniocaudal, and transverse). For brain-stem tumors, the T2-weighted abnormalities were used todetermine measurements, while the post-contrast imageswere used for tumors in other locations. Responses weredefined using the published guidelines for pediatric braintumors [11].
Statistical Analysis
The ability to receive chemotherapy on time (every 4weeks) in the study patients was compared to the abilityto receive chemotherapy every 6 weeks in the patientstreated by Cairncross et al. [7]. Data on the patientstreated by Cairncross et al. was provided by Dr. DavidMacdonald. The difference between the two groups inthe ability to receive the subsequent course of chemo-therapy on time was modeled using the generalized es-timating equations approach [12]. Outcome was classi-fied according to whether the patient was able to receivethe next course of therapy on time. Parameter estimatesfor the group effect as well as the course effect wereobtained. The analysis was carried out assuming no spe-cific structure to the correlation between courses. Theassociation between course outcome and the number ofCD34+ cells/kg was modeled using a similar generalizedestimating equations approach [12]. The difference be-tween the percentage of patients in the two groups whorecovered their counts on time after the first course ofchemotherapy was evaluated using the Fisher’s Exacttest.
RESULTSPatient Characteristics (Table I)
From June 1995 through May 1996, ten patients withnewly diagnosed tumors and one patient with a high-grade glioma that had recurred following radiationtherapy were treated on study. Two additional patientswith diffusely intrinsic brainstem gliomas were enrolledbut did not receive therapy as intended: one patient be-cause of third-party payor refusal to cover the PBSCportion of the protocol and the second because of rapidneurologic deterioration and death before apheresis couldbe undertaken.
The median age of the patient population was 10.3years (range 2.8 to 35.9 years). Four patients had dif-fusely intrinsic brainstem gliomas, one of which was abiopsy-proven glioblastoma. Three patients had focal in-trinsic brainstem tumors with at least two-thirds of thetumor within the pons and/or medulla. All three pre-sented with either long tract signs, cranial nerve deficitsand/or ataxia. Patient 6 had an 8 × 7 cm. extremelyvascular intraventricular/hemispheric tumor that was bi-opsied and originally diagnosed as an oligodendro-glioma. The patient was enrolled on study; subsequentlyan outside neuro-pathologic opinion diagnosed the tumoras a pilocytic astrocytoma. Patient 11 had an anaplasticastrocytoma that recurred 16 months after involved fieldradiation therapy.
PBSC Collection and Reinfusion
A median of six blood volumes were processed perday (range 2.5–6.6) and sufficient PBSCs were harvestedin 1–3 days (median 1 day). All aphereses and reinfu-sions were well tolerated. The median number of MNC/kg
TABLE I. Patient Characteristics and Outcome*
Patientnumber
Age atdiagnosis(years) Tumor location Pathology Surgery
Response tochemotherapy XRT
dose(cGy)
TTP(months)
Survival(months)R C
1 10.3 Pons/diffuse GBM Bx MR Y 5,940 8 92 13.1 Pons/diffuse PR Y 5,580 12 143 4.8 Pons/diffuse SD Y 5,940 10 124 6.0 Pons/diffuse PD N 5,040 1 55 11.4 Pons/focal PR Y 23+6 5.5 Pons/CP angle/focal Pilocytic Bx PR Y 25+7 2.8 Pons/medulla/focal PR Y 29+8 3.6 4th ventricle Anaplastic
ependymomaGTR 28+
9 24.6 Temporal lobe GBM GTR 5,600 15 1810 10.5 Lateral vantricle Pilocytic Bx SD Y 26+11a 35.9 Frontotemporal AA Bx PR Y 6 25+
*Bx, biopsy; GTR, gross total resection; GBM, glioblastoma; AA, anaplastic astrocytoma; TTP, time to progression; C, clinical responseincluding steroid taper (Y, yes, N, no); R, radiographic response; MR, minor response; SD, stable disease; PR, partial response; PD, progressivedisease.aPatient with recurrent disease.
Dose-Intensified PCV With PBSC Support 485

infused was 4.6 × 108 MNC/kg, range 3.8 to 6.3 × 108
MNC/kg. The median number of CD34+ cells/kg infusedwas 1.96 × 106/kg, ranging from 0.42 × 106/kg to 4.5 ×106/kg. The number of CD34 + cells/kg infused was notsignificantly associated with the ability to receive thenext course of chemotherapy on time (P > 0.7). In fact,the patient who received the lowest number of CD34+cells/kg after the fourth course of chemotherapy (0.42 ×106), never dropped her ANC <1000/mL or platelets<100,000/mL.
Chemotherapy Delivery (Table II)
Overall, there was recovery from all toxicity within 31days in 33 of 41 (80.5%) courses. There were no delaysfor hematologic toxicity in the first two courses (onepatient had a delay in order to recover from a woundinfection). Ten of 29 patients in the Cairncross et al. [7]study showed count recovery within 6 weeks after thefirst course of chemotherapy vs. 11 of 11 patients whorecovered their counts by 31 days following the firstcourse of chemotherapy with PBSC support (P < .001).The median dose intensity received (mg/m2/week) forboth CCNU and procarbazine was nearly twice that ofthe standard PCV regimen (Table II). The odds of re-ceiving any given course of therapy on time was 13.6(5.2–35.9; 95% confidence interval) times greater for pa-tients treated with the PBSC protocol than for patients onthe Cairncross et al. [7] study. There was also a signifi-cant course effect seen not only in the patients treated inthe Cairncross et al. [7] study, but in those treated withPBSCs as well, where each subsequent course was lesslikely to be given on time.
Hematologic Toxicity
Hematologic toxicity was mild. Fourteen of 41(34.2%) courses were complicated by ANC<500/mL(median 4 days, range 3–21 days) and in only four (9.8%)did the ANC fall below 200/mL (lasting 1, 2, 3, and 7days). The frequency of neutropenia (ANC <500) aftercourse 1 was no different than after course 4 despite nodose reductions. Three courses were complicated by fe-ver and neutropenia: one patient with documented Influ-enza A, one patient with negative cultures, and one pa-tient who developed aStaphylococcus aureuswound in-
fection. Platelets fell to <50,000/mL in only two courses(4.9%). The lowest platelet count during any course ofchemotherapy was 29,000/mL.
Non-Hematologic Toxicity
The only bacterial infection associated with neutrope-nia was a post-operativeStaphylococcus aureuswoundinfection requiring debridement and prolonged antibiotictherapy. There were five episodes of central line-associated bacteremia without neutropenia. Patient 3 de-veloped fever and respiratory distress 2 weeks after re-ceiving the fourth course of chemotherapy. Chest X-raysshowed progressively worsening bilateral infiltrates. Anopen lung biopsy revealed a lobular pattern of consoli-dation with alveolar accumulation of macrophages, fi-brin, lymphocytes, and hemorrhagic exudate without eo-sinophilia. All cultures were negative. The patient recov-ered rapidly without further intervention and thepresumed diagnosis was viral pneumonia.
Erythematous and/or urticarial rashes developed infive patients during nine courses (22% of all courses),presumably secondary to procarbazine. Three patientsdeveloped a rash during the first and/or second course ofchemotherapy but not during the last two courses (withantihistamine given prior to each procarbazine dose). Nopatient had mucosal involvement, although one patientdeveloped swelling of the face and lips which respondedto antihistamines and steroids. This patient, whose rashoccurred during courses 2, 3, and 4, also developed apulmonary hypersensitivity reaction 3 weeks after thefourth course of chemotherapy, presenting with worsen-ing dyspnea, cough, and an oxygen requirement. ChestX-ray showed subtle bilateral interstitial infiltrates. Sheresponded rapidly to steroids that were subsequently ta-pered without recurrence of symptoms.
Significant anorexia and weight loss were seen in pa-tients not on steroids. Three of the four patients who werenot on steroids during chemotherapy lost greater than10% of their body weight. One of seven patients on ste-roids lost 5–10% of their body weight.
Six of the ten patients who received all four courses ofchemotherapy required vincristine dose reductions/deletions for neurologic toxicity (distal weakness, ileus).Nine of the ten patients developed a severe post-
TABLE II. Chemotherapy Delivery and Intended Dose-Intensity
Coursesgiven on time
Procarbazine(mg/m2/week)
CCNU(mg/m2/week)
PCV with PBSC support(28–31 days) 33/41 (80.5%) 262.5 32.5
Dose escalated PCV(42–44 days)a 25/94 (26.6%) 175 21.6
Standard PCV 140 18.3
aData from Cairncross et al. [7].
486 Jakacki et al.

chemotherapy hyperesthesia syndrome consisting of hy-peresthesia to touch or pressure, particularly over thelateral rib cage. Younger children could not tolerate be-ing picked up underneath the arms. Symptoms typicallystarted 3 to 4 weeks after the fourth course of chemo-therapy and persisted for months. Administration of ste-roids usually resulted in some improvement but not com-plete resolution of symptoms.
Clinical and Radiographic Responses (Table I)
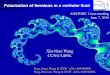
Three of four patients with diffuse, intrinsic brainstemgliomas showed dramatic clinical improvement withinthe first 2 weeks of starting chemotherapy, including twopatients who became bradycardic and/or somnolent be-fore chemotherapy was started and showed minimal tono improvement with steroids. One patient (no. 3), ini-tially showed clinical improvement, followed by neuro-logic worsening after the second course of chemo-therapy. MRI showed cystic degeneration of the enhanc-ing portion of the tumor with increased edema.Chemotherapy was continued and there was gradualclinical and radiographic improvement with a significantdecrease in the size and enhancement of the ring-enhancing component of the tumor by the end of che-motherapy. Figure 1 shows the MRI findings in Patient 1with biopsy-proven glioblastoma, before and after fourcourses of chemotherapy (prior to radiation).
The three patients with focal intrinsic brainstem le-sions showed a somewhat different clinical course. Clini-cal and radiographic improvement was delayed. Two pa-tients continued to show radiographic improvement forseveral months after chemotherapy was completed. Onepatient (no. 5) developed neurologic deterioration afterstarting treatment, with increased edema but decreasedenhancement of the tumor on MRI scan, followed bygradual but dramatic clinical and radiographic improve-ment.
Consolidation Therapy and Survival
The patients with diffuse intrinsic brainstem lesionsand the patient with the temporal lobe glioblastoma re-ceived involved field radiation therapy following thecompletion of chemotherapy. All five patients developedprogressive disease (median 9 months) and died 5–18months from diagnosis (median 11 months).
None of the patients with low-grade tumors or focalintrinsic brainstem tumors received radiation therapy af-ter completing chemotherapy and all remain clinicallywell and progression-free 23–29 months from diagnosis.Patient 10, whose tumor could not be safely resected atthe time of diagnosis because of extreme vascularity, wasable to undergo a radical resection following the comple-tion of chemotherapy.
DISCUSSION
The PCV regimen continues to be the mainstay ofadjuvant chemotherapy for malignant gliomas. A 32–44% response rate is reported in Phase II studies of pa-tients with newly diagnosed and/or recurrent malignantgliomas [13,14]. The original PCV regimen, first pre-scribed in 1972, attempted to give CCNU 75 mg/m2 day0, procarbazine 100 mg/m2 days 1–14, and vincristine1.4 mg/m2 days 0 and 8 every 4 weeks [14]. Bone mar-row toxicity necessitated modifying the regimen so thatcourses are now given 6 weeks apart and the CCNU (110mg/m2) and procarbazine (60 mg/m2/d × 14 days) areseparated by one week [15]. Even with these changes,significant cumulative myelotoxicity compromises drugdelivery. Recent attempts by Cairncross et al. to escalatethe doses of CCNU and procarbazine without growthfactors was unsuccesful [7]. Only 14% of patients whoresponded to the regimen were able to receive six coursesof full-dose chemotherapy and the actual dose-intensitywas no different than the standard PCV regimen.
Using peripheral blood stem cell technology, we haveshown that the PCV regimen can be successfully dose-intensified both by increasing doses and shortening thetime interval between chemotherapy courses. Patientswith brain tumors are ideal candidates for stem cell sup-port since there is a negligible risk of contamination withtumor cells. Eighty percent of courses were able to beadministered on time (i.e., every 4 weeks) as compared to27% of patients on the Cairncross et al. [7] study whowere able to receive an equal number of chemotherapycourses 6 weeks apart. If the dose reductions and intervaldelays typically required in patients receiving the PCVregimen are taken into account, the dose-intensity re-ceived by patients treated with PBSCs is more thandouble that of the standard regimen, since no dose re-ductions were allowed. Some PCV regimens prescribethe chemotherapy be given every 8 weeks, rather thanevery 6 because of the delays in count recovery. All ofour patients recovered their counts by 31 days followingthe first course of chemotherapy vs. 34% who recoveredwithin 6 weeks after the first course of chemotherapy inthe Cairncross et al. [7] study, consistent with successfulengraftment of the reinfused cells.
Thrombocytopenia was rare and short-lived in our pa-tients. Although the majority of our patients were chil-dren, there is no reason to believe that children handlethis regimen differently than adults. Previous experienceshows that children treated with standard PCV for ma-lignant gliomas require an average delay of 0.6 weeks/course due to hematologic toxicity and 3 of 12 childrenhad chemotherapy stopped due to persistent thrombocy-topenia [16]. There were two adults treated on our pro-tocol, who tolerated the therapy no differently than theyounger patients. In fact, the oldest patient encountered
Dose-Intensified PCV With PBSC Support 487

Fig. 1. Ten-year-old girl with a pontine glioblastoma (Patient 1).A: T2-weighted MR image shows a heterogeneously hyperintense mass withinthe pons extending into the right middle cerebellar peduncle.B: T1-weighted image at diagnosis shows heterogeneous contrast enhancement ofthe mass.C: T2-weighted MRI after completing chemotherapy shows significant reduction in the size of the brainstem mass. Note less masseffect on the fourth ventricle.D: T1-weighted image after completing chemotherapy shows decreased contrast enhancement.
488 Jakacki et al.

no hematologic toxicity during any of the four courses ofchemotherapy.
Chemotherapy administration, stem cell harvesting,and reinfusions were done as outpatients. Transfusionrequirements were minimal and the bulk of the toxicitywas non-hematologic and quite manageable. Most of thehospitalizations were for central line infections, none ofwhich were associated with neutropenia or clinical sep-sis.
Approximately half the patients who completedtherapy developed a procarbazine-associated rash, typi-cally during the first or second course of chemotherapy.Hypersensitivity reactions to procarbazine, most com-monly macular-papular rashes are well described in pa-tients with brain tumors [17,18] and there is controversyas to whether the drug should be continued once the rashdevelops [19]. Our patients continued receiving the drug,even if it necessitated using steroids. The patient with themost severe rash developed a delayed allergic pneumo-nitis which responded promptly to steroids. Interestingly,three patients developed rash during the first and/or sec-ond courses of chemotherapy but not during subsequentcourses, which is contrary to reports of prompt reoccur-rence with rechallenge [20,21], suggesting that antihis-tamine pre-treatment may be effective.
A post-chemotherapy hyperesthesia syndrome, whichwas often severe, developed in 9 of the 10 patients whocompleted chemotherapy. Both procarbazine and vincris-tine can cause peripheral neuropathy, particularly vin-cristine which has dose-limiting neurotoxicity [22]. Theincidence of procarbazine-assocated neuropathy is 20%or less, with a much higher incidence when the two drugsare administered together [16,22]. Many patients re-quired dose reductions in vincristine because of periph-eral neuropathy. This distal neuropathy was distinctlydifferent from the syndrome seen after completion ofchemotherapy where the hyperesthesia was predomi-nantly truncal.
The clinical and radiographic responses, particularlyin the patients with diffuse brainstem gliomas whoshowed no response to steroids, was encouraging. Pre-radiation cisplatinum and cyclophosphamide were givento patients with brainstem gliomas in a Pediatric Oncol-ogy Group study [23]. Three patients (9.4%) showed>50% decrease in the size of their tumor after 4 coursesof chemotherapy. Six patients progressed during chemo-therapy and only 16 (50%) completed all four courses ofchemotherapy. In comparison, of the six patients in ourstudy who would fulfill the entry criteria for the POGstudy, three had an objective radiographic response (P 4.039, Fisher’s Exact test) and five of the six showedclinical improvement.
In conclusion, we have shown that the dose intensityof procarbazine and CCNU in the PCV regimen can benearly doubled compared to the standard PCV regimen
through the use of peripheral blood stem cells. Toxicitywas quite manageable and the need for blood productsupport was minimal. Both clinical and radiographic re-sponses were seen, verifying the activity of this regimen.Further studies in larger numbers of patients are neces-sary to determine whether dose-intensification of PCVresults in improved survival compared to standard dosingand timing.
ACKNOWLEDGMENTS
The authors thank Pam Webb and Donna Fischer fortheir secretarial assistance, the staff in the Stem CellLaboratory and Apheresis Center at Riley Hospital forChildren, Indiana University, Melissa Lee for assistancewith data management, and Nancy Wainman of the Na-tional Cancer Institute of Canada Clinical Trials Groupfor providing data from the NCIC oligodendrogliomatrial.
REFERENCES
1. Hryniuk W: The importance of dose-intensity in the outcome ofchemotherapy. In: DeVita VT Jr, Helman S, Rosenberg SA (eds):‘‘Important Advances in Oncology.’’ Philadelphia: Lippincott,1989, pp. 121–141.
2. Gurney H, Dodwell D, Thatcher N, Tattersall MHN: Escalatingdrug delivery in cancer chemotherapy: A review of concepts andpractice. Part 2. Ann Oncol 4:103–115, 1993.
3. Wood WC, Budman DR, Korzun AH, et al: Dose and dose inten-sity of adjuvant chemotherapy for Stage II, node positive breastcarcinoma. N Engl J Med 330: 1253–1259, 1994.
4. Skipper HE: Kinetics of mammary tumor cell growth and impli-cations for therapy. Cancer 28:1479–1499, 1971.
5. Levin VA, Silver P, Hannigan J, et al: Superiority of postradio-therapy adjuvant chemotherapy with CCNU, procarbazine andvincristine (PCV) over BCNU for anaplastic gliomas: NCOG6G61 final report. Int J Radiat Oncol Biol Phys 18:321–324, 1990.
6. Hoagland HC: Hematologic complications of cancer chemo-therapy. In: Perry MC (ed): ‘‘The Chemotherapy Source Book.’’Baltimore, MD: Williams and Wilkins, 1992, pp. 498–502.
7. Cairncross G, Macdonald D, Ludwin S, et al: Chemotherapy foranaplastic oligodendroglioma. J Clin Oncol 12:2013–2021, 1994.
8. Seidman A, Scher H, Gabrilove J, et al: Dose-intensification ofMVAC with recombinant granulocyte colony-stimulating factoras initial therapy in advanced urothelial cancer. J Clin Oncol 11:408–414, 1993.
9. Rampling R, Steward W, Paul J, et al: rhGM-CSF amelioratesneutropenia in patients with malignant gioma treated with BCNU.Br J Cancer 69:541–545, 1994.
10. Maze R, Moritz T, Williams DA: Increased survival and multi-lineage hematopoietic protection from delayed and severe myelo-suppressive effects of a nitrosourea with recombinant interleukin-11 (IL-11). Cancer Res 54:4947–4951, 1994.
11. Gnekow AK: Recommendations of the brain tumor subcommitteefor the reporting of trials. Med Ped Oncol 24:104–108, 1995.
12. Zeger SL, Liang K-Y: Longitudinal data anlysis for discrete andcontinuous outcomes. Biometrics 42:121–130, 1986.
13. Avellanosa AM, West CR, Tsukada Y, et al: Chemotherapy ofnonirradiated malignant gliomas: Phase II study of the combina-
Dose-Intensified PCV With PBSC Support 489

tion of methyl-CCNU, vincristine and procarbazine. Cancer 44:839–846, 1979.
14. Gutin PH, Wilson CB, Kumar AR, et al: Phase II study of pro-carbazine, CCNU, and vincristine combination chemotherapy inthe treatment of malignant brain tumors. Cancer 35:1398–1404,1975.
15. Levin VA, Edwards MS, Wright DC, et al: Modified procarba-zine, CCNU, and vincristine (PCV 3) combination chemotherapyin the treatment of malignant brain tumors. Cancer Treat Rep64:237–241, 1980.
16. Michalski A, Needle M, Goldwein J, et al: Increased toxicity withthe use of procarbazine in addition to CCNU and vincristine inmalignant gliomas of childhood. Pediatr Neurosurg 21:211, 1994.
17. Coyle T, Bushunow P, Winfield J, et al: Hypersensitivity reactionsto procarbazine wtih mechlorethamine, vincristine and procarba-zine chemotherapy in the treatment of glioma. Cancer 69:2532–2540, 1992.
18. Green S, Byar D, Walker M, et al: Comparisons of carmustine,
procarbazine and high dose methylprednisolone as additions tosurgery and radiotherapy for the treatment of malignant glioma.Cancer Treat Rep 67:121–132, 1983.
19. Chabner B: Anticancer drugs. In: DeVita VT Jr, Hellman S,Rosenberg SA (eds): ‘‘Cancer: Principles and Practice of Oncol-ogy,’’ 4th ed. Philadelphia: Lippincott, 1993, p. 387.
20. Lokich J, Maloney W: Allergic reaction to procarbazine. ClinPharmacol Ther 13: 573–574, 1972.
21. Jones SE, Moore M, Blank N, Castellino RA: Hypersensitivity toprocarbazine manifested by fever and pleuropulmonary reaction.Cancer 29: 498–500, 1972.
22. Weiss R, Vogelzang N: Adverse effects of treatment. In: DeVitaVT, Hellman S, Rosenberg SA (eds): ‘‘Cancer: Principles andPractice of Oncology,’’ 4th ed. Philadelphia: Lippincott, 1993, p.2353.
23. Kretschmar CS, Tarbell NJ, Barnes P, et al: Pre-irradiation che-motherapy and hyperfractionated radiation therapy 66 Gy for chil-dren with brainstem tumors. Cancer 72:1404–1413, 1993.
490 Jakacki et al.