Embed Size (px)
Citation preview

IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Hemorrhage: Severe and fatal hemorrhages occurred with CABOMETYX. The incidence of Grade 3 to 5 hemorrhagic events was 5% in CABOMETYX patients. Discontinue CABOMETYX for Grade 3 or 4 hemorrhage. Do not administer CABOMETYX to patients who have a recent history of hemorrhage, including hemoptysis, hematemesis, or melena.
Please see additional Important Safety Information throughout and full Prescribing Information.
Dosing andAdministration GuideFind the right dose for your patients when needed
FIRST- AND SECOND-LINE aRCC CABOMETYX® (cabozantinib) is indicated for the treatment of patients with advanced renal cell carcinoma (RCC).
SECOND-LINE HCC CABOMETYX® (cabozantinib) is indicated for the treatment of patients with hepatocellular carcinoma (HCC) who have been previously treated with sorafenib.
Dose ad
justments
and m
anagem
entD
ose experience
in clinical trialsD
rug interactions/
Specifi
c pop
ulationsA
dm
inistration/ Storag
e and hand
lingIm
portant Safety
Information
Summ
ary

2
Please see additional Important Safety Information throughout and full Prescribing Information.
Dose ad
justments
and m
anagem
entD
ose experience
in clinical trialsD
rug interactions/
Specifi
c pop
ulationsA
dm
inistration/ Storag
e and hand
lingIm
portant Safety
Information
Summ
ary
You may need to adjust the CABOMETYX dose based on individual patient safety and tolerability1
WithholdCABOMETYX
RestartFor patients who previously received 60 mg or 40 mg: RESTART CABOMETYX at a dose reduced by 20 mg
ResumeFor patients who previously received 20 mg: RESUME CABOMETYX at 20 mg if tolerated; otherwise, DISCONTINUE
Waituntil improvement or resolution (return to baseline or resolution to Grade 1)
If ARs occur, consider supportive care and/or adjust the dose
FOR INTOLERABLE GRADE 2 ARs, OR GRADE 3-4 ARs
AR=adverse reaction; GI=gastrointestinal; ONJ=osteonecrosis of the jaw.
Permanently discontinue CABOMETYX for severe hemorrhage, development of a GI perforation or unmanageable fistula, serious thromboembolic event, hypertensive crisis or severe hypertension despite optimal medical management, nephrotic syndrome, or reversible posterior leukoencephalopathy syndrome
Tablets shown are not actual size.
60 mg dailyRecommended starting dose
40 mg dailyFirst reduction
Second reduction 20 mg daily
Available in 3 strengths to help you find the right dose for your patients when needed1
Pharmacokinetics1
The predicted terminal half-life is approximately 99 hours ONJ occurred in <1% of patients treated with CABOMETYX. Withhold CABOMETYX for development of ONJ until complete resolution

204060
4
Please see additional Important Safety Information throughout and full Prescribing Information.
Dose ad
justments
and m
anagem
entD
ose experience
in clinical trialsD
rug interactions/
Specifi
c pop
ulationsA
dm
inistration/ Storag
e and hand
lingIm
portant Safety
Information
Summ
ary
Modifying the CABOMETYX dose can help to manage ARs1
The overall efficacy results in the CABOMETYX trials were achieved in the context of dose modifications1
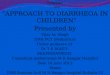
Clinical trials in advanced RCC
CABOSUN was a randomized (1:1), open-label, multicenter trial of CABOMETYX vs sunitinib in 157 first-line patients with aRCC. The starting dose for CABOMETYX was 60 mg, administered orally once daily, and for sunitinib was 50 mg, administered orally once daily on a schedule of 4 weeks on treatment followed by 2 weeks off. The trial included patients who had to have intermediate- or poor-risk disease as defined by IMDC risk categories, clear-cell component, measurable disease, and ECOG PS 0-2. The primary endpoint was PFS. Secondary endpoints included OS and ORR.1,2,4
Clinical trial in HCC
CELESTIAL was a randomized (2:1), double-blind, phase 3 trial of CABOMETYX vs placebo in 707 patients with Child-Pugh A HCC who had previously received sorafenib. The starting dose for CABOMETYX was 60 mg, administered orally once daily. The trial had a broad range of patients who received 1-2 prior systemic therapies, with progression following at least 1, and did not exclude patients based on main portal vein invasion, use of prior immunotherapy, >50% liver involvement, bile duct invasion, sorafenib intolerance, AFP level, or viral load. The primary endpoint was OS. Secondary endpoints included PFS and ORR.1,6
METEOR was a randomized (1:1), double-blind, phase 3 trial of CABOMETYX vs everolimus in 658 patients with aRCC who had previously received at least one prior anti-angiogenic treatment. The starting dose for CABOMETYX was 60 mg, administered orally once daily, and for everolimus was 10 mg, administered orally once daily. The trial included patients who had to have had received prior therapy, clear-cell component, and measurable disease. The primary endpoint was PFS. Secondary endpoints included OS and ORR.1,5
1L(CABOSUN)vs sunitinib
2L(METEOR)
vs everolimus
2L+(CELESTIAL)
vs placebo
Dose withholds1,2 73%71%
70%59%
84%37%
Median duration of each dose withhold2 NA 7 days 9 days
Dose reductions1,3 46%35%
60%24%
62%13%
Discontinuations1,3 21%22%
10%10%
16%3%
Mean average daily dose2 49 mg 45 mg 37 mg
aRCC HCC
Patients who require a dose reduction will receive a free 15-tablet supply of CABOMETYX in the new lower dose. Additional restrictions and eligibility rules apply
To obtain a Dose Exchange Program Form, contact your sales representative, call EASE at 1-844-900-EASE (3273), or visit www.EASE.us
Dose Exchange Program: Supporting your patients who require a dose modification during CABOMETYX treatment
NA=not available.
AFP=alpha-fetoprotein tumor marker; ECOG=Eastern Cooperative Oncology Group; IMDC=International Metastatic Renal Cell Carcinoma Database Consortium; ORR=objective response rate; OS=overall survival; PFS=progression-free survival.

6
Please see additional Important Safety Information throughout and full Prescribing Information.
Dose ad
justments
and m
anagem
entD
ose experience
in clinical trialsD
rug interactions/
Specifi
c pop
ulationsA
dm
inistration/ Storag
e and hand
lingIm
portant Safety
Information
Summ
ary
Drug interactions1
When strong CYP3A4 inhibitors cannot be avoided
When strong CYP3A4 inducers cannot be avoided
Resume CABOMETYX at the dose that was used prior to initiating the strong CYP3A4 inhibitor 2 to 3 days after discontinuation of the strong inhibitor
Examples of strong CYP3A4 inhibitors
Boceprevir, clarithromycin, conivaptan, grapefruit juice, indinavir/ritonavir, itraconazole, ketoconazole, lopinavir/ritonavir, nefazodone, nelfinavir, posaconazole, ritonavir, saquinavir/ritonavir, and voriconazole.
Resume CABOMETYX at the dose used prior to initiating the strong CYP3A4 inducer 2 to 3 days after discontinuation of the strong inducer
— Do not exceed a daily dose of 80 mg
Examples of strong CYP3A4 inducers
Rifampin, phenytoin, carbamazepine, and St. John’s wort.
Reduce the daily dose of CABOMETYX if concomitant use with strong CYP3A4 inhibitors cannot be avoided.
Increase the daily dose of CABOMETYX if concomitant use with strong CYP3A4 inducers cannot be avoided.
REDUCE DOSE BY20 mg
INCREASE DOSE BY20 mg
Specific populations1
Renal impairment Dose adjustment is not required in patients with mild to moderate renal impairment
There is no experience with CABOMETYX in patients with severe renal impairment
Hepatic impairment Reduce the CABOMETYX dose in patients with moderate hepatic impairment (Child-Pugh B)
Avoid CABOMETYX in patients with severe hepatic impairment (Child-Pugh C), since it has not been studied in this population
Pediatrics The safety and effectiveness of CABOMETYX in pediatric patients have not been established
Geriatrics No dose modification required
Surgery For patients undergoing surgery, stop treatment with CABOMETYX at least 28 days prior to scheduled surgery, including dental surgery
Lactation Advise women not to breastfeed during treatment with CABOMETYX and for 4 months after the final dose
Females and males of reproductive potential Verify the pregnancy status of females of reproductive potential prior to initiating CABOMETYX and advise them to use effective contraception during treatment and for 4 months after the final dose
Based on findings in animals, CABOMETYX may impair fertility in females and males of reproductive potentialFor more information about CYP3A4 inhibitors and inducers, visit
https://www.fda.gov/drugs/developmentapprovalprocess/developmentresources/druginteractionslabeling/ucm093664.htm

+
8
Please see additional Important Safety Information throughout and full Prescribing Information.
Dose ad
justments
and m
anagem
entD
ose experience
in clinical trialsD
rug interactions/
Specifi
c pop
ulationsA
dm
inistration/ Storag
e and hand
lingIm
portant Safety
Information
Summ
ary
Strength NDC
60 mg, 30 tablets 42388-023-26
40 mg, 30 tablets 42388-025-26
20 mg, 30 tablets 42388-024-26
Storage and handling1
Store CABOMETYX at room temperature: 20°C to 25°C (68°F to 77°F); excursions are permitted from 15°C to 30°C (59°F to 86°F)
Keep CABOMETYX and all medications out of the reach of children
CABOMETYX tablets are not scored
Recommended administration of CABOMETYX1
Do not substitute CABOMETYX tablets with cabozantinib capsules
Do not ingest food (eg, grapefruit or grapefruit juice) or nutritional supplements (eg, St. John’s wort) that are known to strongly induce or inhibit cytochrome P450 during CABOMETYX treatment
A high-fat meal increased Cmax and AUC values by 41% and 57%, respectively, relative to fasting conditions in healthy subjects administered a single oral dose of a cabozantinib capsule formulation
For more information on drug interactions, see page 6.
If your patients miss a dose
IF THE NEXT SCHEDULED DOSE IS:
in less than 12 hours in 12 hours or more
Do not make up the missed dose
Take the next dose at the usual time
Take the missed dose as soon as possible
Take the next dose at the usual time
DO NOT TAKE CABOMETYX WITH FOODTake CABOMETYX at least 1 hour before or at least 2 hours after eating
8 oz of water
Swallow tablet wholeDO NOT CRUSH

10 Please see full Prescribing Information.
Dose ad
justments
and m
anagem
entD
ose experience
in clinical trialsD
rug interactions/
Specifi
c pop
ulationsA
dm
inistration/ Storag
e and hand
lingIm
portant Safety
Information
Summ
ary
Indications and Important Safety InformationINDICATIONSCABOMETYX® (cabozantinib) is indicated for the treatment of patients with advanced renal cell carcinoma (RCC).
CABOMETYX® (cabozantinib) is indicated for the treatment of patients with hepatocellular carcinoma (HCC) who have been previously treated with sorafenib.
IMPORTANT SAFETY INFORMATIONWARNINGS AND PRECAUTIONSHemorrhage: Severe and fatal hemorrhages occurred with CABOMETYX. The incidence of Grade 3 to 5 hemorrhagic events was 5% in CABOMETYX patients. Discontinue CABOMETYX for Grade 3 or 4 hemorrhage. Do not administer CABOMETYX to patients who have a recent history of hemorrhage, including hemoptysis, hematemesis, or melena.
Perforations and Fistulas: GastrointestinaI (GI) perforations, including fatal cases, occurred in 1% of CABOMETYX patients. Fistulas, including fatal cases, occurred in 1% of CABOMETYX patients. Monitor patients for signs and symptoms of perforations and fistulas, including abscess and sepsis. Discontinue CABOMETYX in patients who experience a fistula that cannot be appropriately managed or a GI perforation.
Thrombotic Events: CABOMETYX increased the risk of thrombotic events. Venous thromboembolism occurred in 7% (including 4% pulmonary embolism) and arterial thromboembolism in 2% of CABOMETYX patients. Fatal thrombotic events occurred in CABOMETYX patients. Discontinue CABOMETYX in patients who develop an acute myocardial infarction or serious arterial or venous thromboembolic event requiring medical intervention.
Hypertension and Hypertensive Crisis: CABOMETYX can cause hypertension, including hypertensive crisis. Hypertension occurred in 36% (17% Grade 3 and <1% Grade 4) of CABOMETYX patients. Do not initiate CABOMETYX in patients with uncontrolled hypertension. Monitor blood pressure regularly during CABOMETYX treatment. Withhold CABOMETYX for hypertension that is not adequately controlled with medical management; when controlled, resume at a reduced dose. Discontinue CABOMETYX for severe hypertension that cannot be controlled with anti-hypertensive therapy or for hypertensive crisis.
Diarrhea: Diarrhea occurred in 63% of CABOMETYX patients. Grade 3 diarrhea occurred in 11% of CABOMETYX patients. Withhold CABOMETYX until improvement to Grade 1 and resume at a reduced dose for intolerable Grade 2 diarrhea, Grade 3 diarrhea that cannot be managed with standard antidiarrheal treatments, or Grade 4 diarrhea.
Palmar-Plantar Erythrodysesthesia (PPE): PPE occurred in 44% of CABOMETYX patients. Grade 3 PPE occurred in 13% of CABOMETYX patients. Withhold CABOMETYX until improvement to Grade 1 and resume at a reduced dose for intolerable Grade 2 PPE or Grade 3 PPE.
Proteinuria: Proteinuria occurred in 7% of CABOMETYX patients. Monitor urine protein regularly during CABOMETYX treatment. Discontinue CABOMETYX in patients who develop nephrotic syndrome.
Osteonecrosis of the Jaw (ONJ): ONJ occurred in <1% of CABOMETYX patients. ONJ can manifest as jaw pain, osteomyelitis, osteitis, bone erosion, tooth or periodontal infection, toothache, gingival ulceration or erosion, persistent jaw pain, or slow healing of the mouth or jaw after dental surgery. Perform an oral examination prior to CABOMETYX initiation and periodically during treatment. Advise patients regarding good oral hygiene practices. Withhold CABOMETYX for at least 28 days prior to scheduled dental surgery or invasive dental procedures. Withhold CABOMETYX for development of ONJ until complete resolution.
Wound Complications: Wound complications were reported with CABOMETYX. Stop CABOMETYX at least 28 days prior to scheduled surgery. Resume CABOMETYX after surgery based on clinical judgment of adequate wound healing. Withhold CABOMETYX in patients with dehiscence or wound healing complications requiring medical intervention.
Reversible Posterior Leukoencephalopathy Syndrome (RPLS): RPLS, a syndrome of subcortical vasogenic edema diagnosed by characteristic finding on MRI, can occur with CABOMETYX. Evaluate for RPLS in patients presenting with seizures, headache, visual disturbances, confusion, or altered mental function. Discontinue CABOMETYX in patients who develop RPLS.
Embryo-Fetal Toxicity: CABOMETYX can cause fetal harm. Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Verify the pregnancy status of females of reproductive potential prior to initiating CABOMETYX and advise them to use effective contraception during treatment and for 4 months after the last dose.
ADVERSE REACTIONSThe most commonly reported (≥25%) adverse reactions are: diarrhea, fatigue, decreased appetite, PPE, nausea, hypertension, and vomiting.
DRUG INTERACTIONSStrong CYP3A4 Inhibitors: If coadministration with strong CYP3A4 inhibitors cannot be avoided, reduce the CABOMETYX dosage. Avoid grapefruit or grapefruit juice.
Strong CYP3A4 Inducers: If coadministration with strong CYP3A4 inducers cannot be avoided, increase the CABOMETYX dosage. Avoid St. John’s wort.
USE IN SPECIFIC POPULATIONSLactation: Advise women not to breastfeed during CABOMETYX treatment and for 4 months after the final dose.
Hepatic Impairment: In patients with moderate hepatic impairment, reduce the CABOMETYX dosage. CABOMETYX is not recommended for use in patients with severe hepatic impairment.
References: 1. CABOMETYX® (cabozantinib) Prescribing Information. Exelixis, Inc, 2019. 2. Data on file. Exelixis, Inc. 3. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. New Eng J Med. 2018;379:54-63. doi:10.1056/NEJMoa1717002. 4. Choueiri TK, Halabi S, Sanford BL, et al. Cabozantinib versus sunitinib as initial targeted therapy for patients with metastatic renal cell carcinoma of poor or intermediate risk: the Alliance A031203 CABOSUN trial. J Clin Oncol. 2017;35(6):591-597. 5. Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): final results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2016;17(7):917-927. 6. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. New Eng J Med. 2018;379:54-63. doi: 10.1056/NEJMoa1717002 [supplementary appendix].

204060
Patients who require a dose reduction will receive a free 15-tablet supply of CABOMETYX in the new lower dose. Additional restrictions and eligibility rules apply
To obtain a Dose Exchange Program Form, contact your sales representative, call EASE at 1-844-900-EASE (3273), or visit www.EASE.us
Find the right dose for your patients when needed1
© 2019 Exelixis, Inc. CA-1082 01/19
Convenient, once-daily oral dosing
CABOMETYX is available in 3 strengths
— Recommended starting dose: 60 mg daily — Dose after first reduction: 40 mg daily — Dose after second reduction: 20 mg daily
You may need to adjust the CABOMETYX dose based on individual patient safety and tolerability
Dose Exchange Program: Supporting your patients who require a dose modification during CABOMETYX treatment
IMPORTANT SAFETY INFORMATION (cont’d)
WARNINGS AND PRECAUTIONS
Perforations and Fistulas: GastrointestinaI (GI) perforations, including fatal cases, occurred in 1% of CABOMETYX patients. Fistulas, including fatal cases, occurred in 1% of CABOMETYX patients. Monitor patients for signs and symptoms of perforations and fistulas, including abscess and sepsis. Discontinue CABOMETYX in patients who experience a fistula that cannot be appropriately managed or a GI perforation.
Please see additional Important Safety Information throughout and full Prescribing Information.
Dose ad
justments
and m
anagem
entD
ose experience
in clinical trialsD
rug interactions/
Specifi
c pop
ulationsA
dm
inistration/ Storag
e and hand
lingIm
portant Safety
Information
Summ
ary