Embed Size (px)
DESCRIPTION
Timeline & Milestones: Certification & Standards NPRM Stage 2 Health IT Standards Committee, March 29, 2011. Doug Fridsma, MD, PhD Director Office of Interoperability & Standards. Agenda. Key Milestones and Timeline Strategic Principles for Standards and Certification - PowerPoint PPT Presentation
Citation preview

Timeline & Milestones:
Certification & Standards NPRM Stage 2
Health IT Standards Committee, March 29, 2011
Doug Fridsma, MD, PhD
DirectorOffice of Interoperability & Standards
1

2
Agenda
• Key Milestones and Timeline
• Strategic Principles for Standards and Certification
• Draft Core Themes for Standards and Certification
• Discussion

3
TIMELINE AND MILESTONES

4
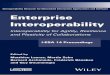
Key Milestones and Timelines
Q22011
Q32011
Q42011
Q12012
Q22012
Q32012
Q42012
Q12013
Final Rule Published
NPRM Published
NPRM Drafted

5
Key Timeline Constraints
• NPRM must be drafted and undergo regulatory clearance well before publication
• Publication of final rule must allow for– Comment period– Analysis of comments– Rule drafting and regulatory clearance
• Certification tests must be developed, vetted and implemented by ONC-ACB
• EHRs and EHR modules must have lead-time for– Software development– Certification– Upgrade/installation and training

6
STRATEGIC PRINCIPLES

7
The best way to predict the future is to invent it
Alan Kay
The future is already here – it's just not very evenly distributed
William Gibson
The problem with the future is that it keeps turning into the present
Calvin and Hobbes
Quotes

8
Key Principles for Standards and Certification Criteria
• Standards and Certification for the sake of– Meaningful use– Improved care, improved health,
decreased costs– Confidence and trust– Individual empowerment– Rapid learning and innovation
• Standards and Criteria should couple low regret and high leverage

9
For Discussion: Core Themes
• Pragmatic vocabulary– Reduce alternatives in vocabularies– Code subsets that drive 95% of volume and value– Inclusive of laboratory reports, care transitions, public health, quality measures
• Upgrade from paper to electronic data transmission– Reduce alternatives and increase specificity of data transmission standards– Health Information Exchange– Lab, individual engagement, public health– Major focus on standards for care transitions
• Down-payment on transport for PCAST, query/retrieve
• Update NWHIN specifications to include content and transport standards for MU

10
VOCABULARY

11
For Discussion: Philosophy for Vocabulary
• Work with HITSC and NLM on pragmatic subsets for– Problems– Medications and medication reactions/allergies– Results
• Constrain for success– Converge to a single vocabulary for a particular purpose– Focus on ambulatory domain, quality reporting and public health– Focus on interoperability only, not internal representation– Work to address 95% most commonly used elements and certify on that 95% subset– Certify on ability to consume data where EHR does not understand the code
• Name the standard in rulemaking, “late bind” the 95% subset in testing

12
UPGRADE TO ELECTRONIC

13
For Discussion: Core specifications needed
• Directed Exchange Bundle– Transport– Certificates– Directories
• Lab Results– Ambulatory results IG– Associated vocabulary
• Public Health (ELR, VXU/Q/R, reportable conditions)– Refined IGs + vocabulary subsets

14
For Discussion: Core Specifications Needed
• Transitions of Care– Directed Exchange– Content vocabularies for
• Medications• Medication reactions/allergies• Problems• Results
– Common content sections + transition specific content sections
– Refinement/updates to existing content standards
• Include the individual (publish to PCHR as core transition)

15
DOWNPAYMENTON THE FUTURE

16
For Discussion: Query/Retrieve, PCAST
• Need to explore “low regret” standards for future information exchange needs to support innovation and a learning healthcare system
• Candidates include:– Synchronous secure transport (e.g., SOAP + TLS + WS-Security
and HTTP + TLS + OAuth2)– Subset of current NWHIN specifications for exchange– Metadata for a universal exchange language derived from existing
exchange standards– Distributed queries to support risk adjustment, quality reporting,
public health

17
DISCUSSION