Embed Size (px)
Citation preview

Dove siamo con l’epidemia: i casi e le previsioni
WHO Collaborating Center for clinical care, diagnosis, response and training on Highly Infectious Diseases
Giuseppe Ippolito National Institue for Infectious Diseases Lazzaro Spallanzani-Roma

Ringraziamenti
• Tutti i partecipanti • Effetti • I componenti della unità di crisi Ebola
dell’INMI • Tutto il personale dell’INMI

I numeri di Ebola al 7 novembre 2014 Country Total Cases Total Deaths
Liberia 6,525 2,697 Sierra Leone 4,759 1,070 Guinea 1,731 1,041 Nigeria 20 8 Senegal 1 0 Spain 1 0 USA 4 1 Mali 1 1 Total: 13,042 4,818
DR Congo 70 42

I numeri della epidemia in corso, rispetto alle epidemie precedenti, sono incredibilmente più alti

I casi fuori dall’Africa

How Many Ebola Patients Have Been Treated Outside of West Africa?
http://www.nytimes.com/interactive/2014/07/31/world/africa/ebola-virus-outbreak-qa.html?module=Search&mabReward=relbias%3As%2C%7B%222%22%3A%22RI%3A17%22%7D

How Many People Could Become Infected?
http://www.nytimes.com/interactive/2014/07/31/world/africa/ebola-virus-outbreak-qa.html?module=Search&mabReward=relbias%3As%2C%7B%222%22%3A%22RI%3A17%22%7D

Periodo di incubazione a fine settembre 2014

9
Estimating the Incubation Period Distribution
Figure S3: Gamma parametric fits to the distributions of incubation periods among confirmed and probable EVD cases reporting (A) single day and (B) multiday exposures.
WHO Ebola Response Team, NEJM 2014

Tasso di letalità 1976-2012
Lefebvre A. Med Mal Infect, 2014
Negli anni il tasso di mortalità è andato mediamente diminuendo (cure di base migliori?)

Letalità di EVD e confronto con altre infezioni
• EVD 54,9% (24-89%) • Media da comparsa sintomi alla
morte: 7 giorni ----------------------------------------- • Influenza Pandemica (1918) 4% • SARS 10% • Colera: 1-10%

Evoluzione di EVD
• Media da comparsa sintomi alla guarigione: 15 giorni
Fonte: WHO Data from Guinea, Liberia, and Sierra Leone (VSHOC Ebola database, 25 Aug 2014) Imperial College & University of Oxford (Database USCDC/WHO RO/WHO HQ, 27 Aug 2014)

Mortalità stimata a fine settembre 2014

14
Estimating the Case Fatality Rate Figure S6. Cumulative CFR estimate (95% CIs) of confirmed and probable cases over time by country. (A) based on definitive clinical outcome, dividing total deaths by total cases with known final outcome (death or recovery), (B) naïve estimate, dividing total deaths by total cases (irrespective of outcome), and (C) the naïve estimate adjusted for the delay between case and death reporting4.
WHO Ebola Response Team, NEJM 2014

15
WHO Ebola Response Team, NEJM 2014

Kaplan–Meier Estimate of the Probability of Survival among Patients with Ebola Virus Disease, by Age.
Elhadj Ibrahima Bah et al. NEJM October 29 2014,
RR 3.49 95% CI, 1.42 to 8.59; P = 0.007

Le previsioni

Case importation probability projection for 31 October 2014
Gomes MFC et al. PLOS Currents Outbreaks 2014 Sep 2
http://www.mobs-lab.org/ebola.html

http://www.mobs-lab.org/ebola.html

Assuming no change in control measures for the epidemic, there will be close to 20,000 cases by early November (conservative projection)
WHO Ebola Response Team, NEJM Sept 23,2014

Look to the future. There will be more epidemics and outbreaks of Ebola and other new or reemerging infections. Yet our response to such events remains slow, cumbersome, poorly funded, conservative, and ill prepared. We have been very lucky with SARS, H5N1 and H1N1 influenza, and possibly MERS-CoV, but this Ebola epidemic shows what can happen when luck escapes us.

Collegamenti aerei con l’Africa occidentale
Gomes MFC et al. PLOS Currents Outbreaks 2014 Sep 2
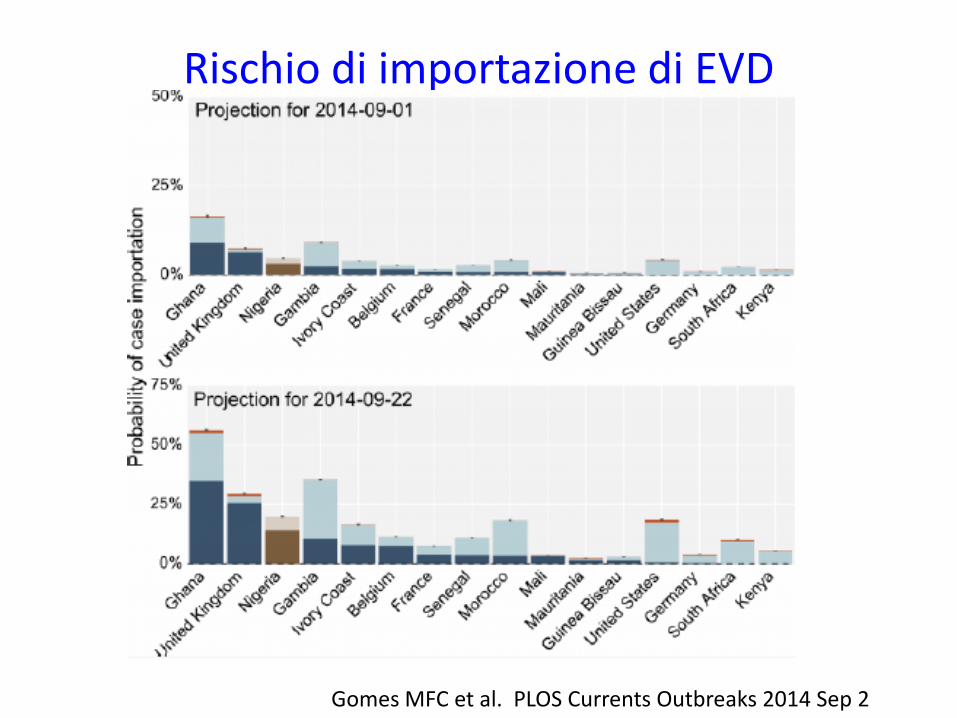
Rischio di importazione di EVD
Gomes MFC et al. PLOS Currents Outbreaks 2014 Sep 2

Parametri epidemiologici di riferimento
Gomes MFC et al. PLOS Currents Outbreaks 2014 Sep 2
Struttura della presentazione • Perché iniziamo dai DEA? • Ebola chi? • Epidemie da Malattia da Virus Ebola (EVD): uno sguardo al
passato • L’epidemia in corso in Africa Occidentale
– Origine – Numeri e parametri epidemiologici
• Una epidemia senza precedenti: perché? • Difficoltà, criticità e critiche nella risposta internazionale • Le possibilità e le speranze terapeutiche e vaccinali • Pazienti con EVD in Europa ed in Italia: dobbiamo
aspettarceli? • Le strategie di intervento

Ebola nei paesi occidentali


EVD in western countries: main criticisms Advantages Problems
Patients specifically evacuated in western countries
Pz already recognized, usually trasnferred to HLIU, limited need for contact tracing
Safety during the transport, limited bed capabilities

EVD in western countries: main criticisms Advantages Problems
Patients specifically evacuated in western countries
Pz already recognized, usually trasnferred to HLIU, limited need for contact tracing
Safety during the transport, limited bed capabilities
Patients newly diagnosed in western countries
- Early diagnosis, first contact in unprepared hospital, complex contact tracing

EVD in western countries: main criticisms Advantages Problems
Patients specifically evacuated in western countries
Pz already recognized, usually trasnferred to HLIU, limited need for contact tracing
Safety during the transport, limited bed capabilities
Patients newly diagnosed in western countries
- Early diagnosis, first contact in unprepared hospital, complex contact tracing
Secondary transmission
Easy to recognize because of the “medical” surveillance measures
Faults in procedures, anxiety among other HCWs

La crisi del paziente zero americano

The nightmare of the Texas Health Presbyterian Hospital

Texas health Presbyterian Hospital
• Duncan was released from the ER despite his having a fever and abdominal pain and telling a nurse that he had been in West Africa, where the Ebola virus was spreading.

• The hospital said late Thursday that a flaw with the electronic records system kept Thomas Eric Duncan’s travel history from being communicated to physicians.

• Under CDC guidelines issued in August, the hospital must consider isolating Duncan and testing him for the virus.

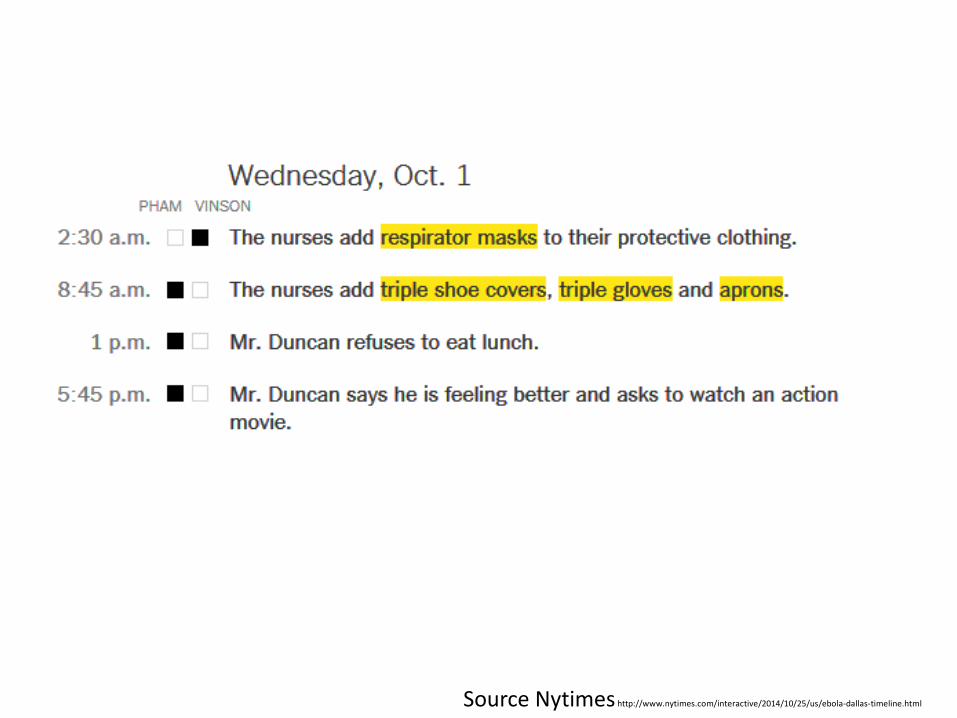
Reconstruction of management Details of Duncan’s Treatment Texas
Health Presbyterian Hospital in Dallas After being released from the emergency room on his first
visit, Thomas Eric Duncan was admitted to Texas Health Presbyterian Hospital in Dallas on a second visit. The handling of Mr. Duncan, the first person to test positive for Ebola in the United States, is detailed below, based on medical documents provided to The New York Times. OCT. 25, 2014



Sunday, Sept. 28
8:35 p.m. 9:40 p.m.
• Mr. Duncan is examined by an infectious-
disease specialist, who says Ebola “should be high on the list” of possible diagnoses.
• Mr. Duncan has explosive diarrhea and projectile vomiting.
Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html
Mr. Duncan is moved to a 24-bed intensive care unit
after all other patients are transferred out.

Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html
Mr. Duncan is moved to a 24-bed intensive care unit
after all other patients are transferred out.

Monday, Sept. 29-4:40 p.m. Mr. Duncan is moved to a 24-bed intensive care unit
after all other patients are transferred out.
Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html
Medical Intensive Care Unit
Mr. Duncan’s room

Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html
Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html

Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html

Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html

Source Nytimes http://www.nytimes.com/interactive/2014/10/25/us/ebola-dallas-timeline.html

http://www.nytimes.com/interactive/2014/07/31/world/africa/ebola-virus-outbreak-qa.html?module=Search&mabReward=relbias%3As%2C%7B%222%22%3A%22RI%3A17%22%7D

Analysis of the US response • Dallas also shattered the fundamental assumption
among most American health officials that almost any large American hospital could safely treat Ebola.
• Many of the procedures that have been put in place since Dallas reflect that change in thinking with the designation of specific hospitals as point places for Ebola treatment.
Modified from http://www.nytimes.com/2014/10/26/us/new-york-ebola-response-polar-opposite-of-dallas.html

Laboratories for testing patient samples and hospitals designated to accept Ebola patients
http://www.nytimes.com/interactive/2014/07/31/world/africa/ebola-virus-outbreak-qa.html?module=Search&mabReward=relbias%3As%2C%7B%222%22%3A%22RI%3A17%22%7D
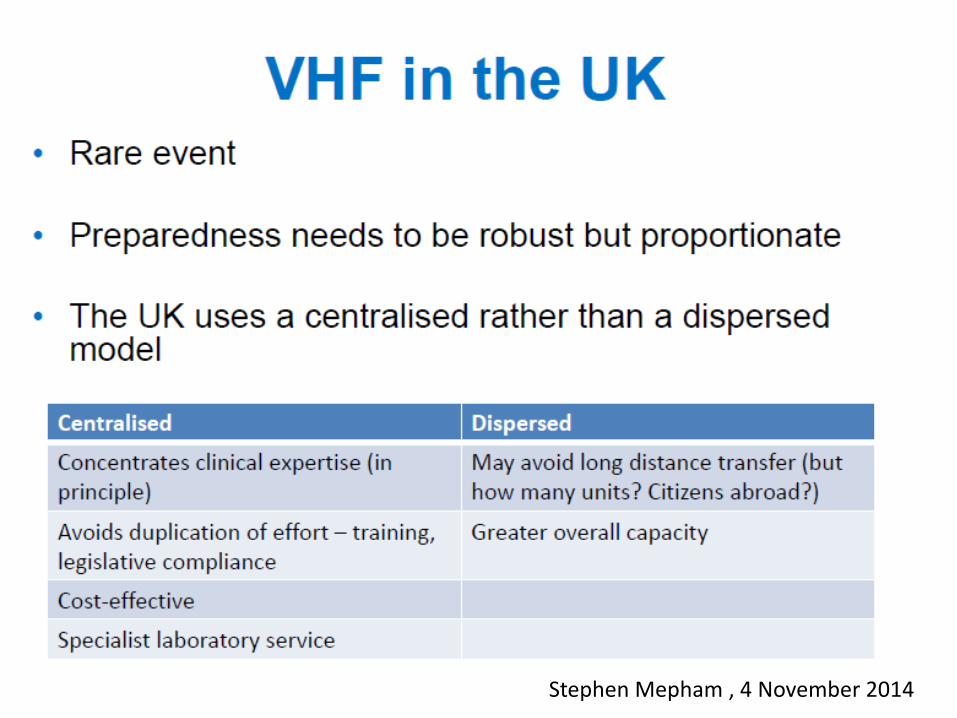
Stephen Mepham , 4 November 2014

Hospital preparedeness for EVD in EU
• Only available inventory: EuroNHID surveys in 2009-10;
• 16 countries, 48 isolation facilities visited;
• All facilities were identified by National Health Authorities as the referral hospital for Highly Infectious Diseases (HIDs).
You said it was ONLY a virus!
(Schilling et al. Plos One 2014)

4
4
3
2
2
Isolation facilities in 16 EU countries – 2009-10

Classification of Isolation Facilities
• Referral centres: hospitals identified by National Health Authorities for the management of HIDs, but not equipped with special technical features;
• Isolation Room: hospital rooms equipped with special technical features for the management of HID, usually part of Infectious Diseases or Intensive Care wards
• High-Level Isolation Unit (HLIU)

High-Level Isolation Unit (HLIU) - Definition
An HLIU is a health-care facility specifically designed to provide safe, secure, high-quality, and appropriate care, with optimal infection containment and infection prevention and control procedures, for a single patient or a small number of patients who have, or who may have, a highly infectious disease.
Comment: it perfectly fit with the current epidemiological
situation

EuroNHID project: HLIU in Europe

HLIU: specific safety and infection control issues for EVD
• Logistic, technical and engineering items; • Transport; • Staff: training and workplan; • Medical issues: special procedures; • PPE: selection, donning and doffing; • Management of diagnostic samples; • Disinfection and decontamination; • Waste management; • Management of human remains.

Logistic/Technical/Engineering issues for the safe management of a EVD patient
• EVD is transmitted by contacts/droplets; • Therefore items needed are:
– Anteroom for donning and removal of PPE; – Ideally a separate way-in and way-out; – Clear limits between clean and contaminated areas; – Material easy to be contaminated for ceiling, walls
and floor; • Items for air-handling (negative pressure, HEPA filtration,
windows sealed) are not strictly necessary during routine care of EVD patients, but are advisable during aerosol-generating procedures.

HLIU: specific safety and infection control issues for EVD
• Logistic, technical and engineering items; • Transport; • Medical issues: special procedures; • Staff: training and workplan; • PPE: selection, donning and removal; • Management of diagnostic samples; • Disinfection and decontamination; • Waste management; • Management of human remains.

Transport of EVD patients • Safe modalities for external and internal transport of EBV
patients should be planned; • Ambulances with special technical features are present in 4
countries; • Ideally, dedicated pathway should be identified for internal
transport; • An area for ambulance decontamination should be identified.

Transport of EVD patients • N36 stretcher largely available in Europe

HLIU: specific safety and infection control issues for EVD
• Logistic, technical and engineering items; • Transport; • Staff: training and workplan; • Medical issues: special procedures • PPE: selection, donning and removal; • Management of diagnostic samples; • Disinfection and decontamination; • Waste management; • Management of human remains.

Staff in HLIUs: specific requirements for EVD • Training, training, training, including periodical simulation; • Different specialties (at least Infectious Diseases, Intensive
Care and Infection Control) must be part of staff; • Pre-identified and trained consultants should be available; • Modalities for staff activation in short time; • Detailed workplan needed (short shifts).

HLIU: specific safety and infection control issues for EVD
• Logistic, technical and engineering items; • Transport; • Staff: training and workplan; • Medical issues: special procedures; • PPE: selection, donning and removal; • Management of diagnostic samples; • Disinfection and decontamination; • Waste management; • Management of human remains.

Medical issues: special procedures for EVD
• Limit procedures to those strictly mandatory only; • All procedures should be performed within HLIU; • Intensive Care should be provided inside isolation area by
portable equipments; • Similarly, all complex diagnostic and therapeutic procedures
(e.g. X-ray, endoschopy, dialysis) should be reduced to minimum and performed within isolation area;
• Keep special attention to aerosol-generating procedures.

HLIU: specific safety and infection control issues for EVD
• Logistic, technical and engineering items; • Transport; • Staff: training and workplan; • Medical issues: special procedures; • PPE: selection, donning and removal; • Management of diagnostic samples; • Disinfection and decontamination; • Waste management; • Management of human remains.

I tempi dele raccomandazioni

WHO PPE guidelines
Rationale, approach and summary recommendations
Constanza Vallenas WHO November 2014

PPE for EVD
• Probably the most discussed issue during this outbreak;
• Removal procedures are essential; • Mistakes in PPE removal are suggested to
be the origin of secondary cases in USA and Spain;
• Indications are continuosly evolving; • Recent new indications come from CDC
and WHO; • A comprehensive guidance about PPE
critical aspects has been recently released by ECDC.

PPE proposals for EVD
ECDC proposals CDC initial proposal and first modification

Changes to Ebola Protection Worn by U.S. Hospital Workers

HLIU: specific safety and infection control issues for EVD
• Logistic, technical and engineering items; • Transport; • Staff: training and workplan; • PPE: selection, donning and removal; • Management of diagnostic samples; • Disinfection and decontamination; • Waste management; • Management of human remains.

Management of diagnostic samples from EVD
• Maximize the use of Point-of-care systems; • Diagnostic tests may be performed in BSL-3 lab also, but
confirmatory test require a BSL-4 laboratory; • Routine tests may be safely performed in automated closed
systems; • QUANDHIP project developed a form with brief and operative
instructions for the managment of samples in EVD patients, available at: http://www.quandhip.info/Quandhip/EN/Home/Ebola_fever_instructions.pdf;jsessionid=4111EBD98C50C57A3EA338A79D718A7C.2_cid290?__blob=publicationFile

The main criticism for the management of EVD: unprepared hospitals!
• Establishment of contact isolation is not enough! • It is also needed:
– well-trained staff, – awareness about procedures, – experienced infection control experts, – adequate logistic (e.g. the presence of an anteroom,
materials easy-to-decontaminate within the room, dedicated pathways),
– availability of correct PPE and procedures for their use, donning and removal,
– presence of procedures for disinfection and waste management.
In one sentence, an established “infection control culture
and practice”.

A model for hospital management of EVD: why to use HLIU
• HLIUs only have this expertise; • The bed capacity of HLIU is enough to comply with EU need in
the current epidemiological context; • HLIUs staff is used to work at international level; • A univocal public health model for referral and care can be
used; • In HLIUs clinical research activities may be conducted in an
harmonized matter; • Trans-national agreements are possible for those countries
where HLIUs are not available.

Key problem to deal with the 2014 EVD outbreak
Conclusions

Problems often unresolved
• Incomplete understanding of threats • Decision making without data, plans and
programs • Coordination • Organization of public health infrastructure

Decision Making without Data
• Need to make decisions rapidly in the absence of data • Access to subject matter experts is required • No “textbook” experience to guide response • Understanding of “risk” evolved as outbreak unfolded • Need coherent, rapid process for addressing scientific
issues in midst of crisis
Michael Hopmeier, 2004





























