Embed Size (px)
Citation preview

Down on the Farm: PreventingFarm Accidents in ChildrenAlice E. ConwayAmyJ. McClunePatricia Nosel
The sun peeks its head abovethe horizon, casting its firstrays upon acres of lush greenfields, glistening from the
morning dew. A rooster crows, markingthe advent of a new day. The air is fra-grant with fresh soil and warm home-made bread. These tranquil images arewhat we associate with farm life. Itseems like a Utopia, a close knit familyworking side by side for the bettermentof the farm and ultimately each other.Unfortunately farm life is far from aUtopia.
SignificanceAgriculture continues to rank as the
most dangerous industry in the UnitedStates, with an accidental work- relateddeath rate six times that of all otherindustries combined (DeMuri &Purschwitz, 2000). It is a unique indus-try, in that it is often a family business,where parents and children both liveand work. In 1999. according to theNational Agricultural Statistics Service(rSASS) (n.d.), there were more than 2million farms in the United States, with1.5 million children and adolescentsliving and/or working on farms. In theUnited States, tOO children die andmore than 100.000 are injured eachyear on these farms where they live,work, and play.
With 23% of its citizens residing inrural areas. Pennsylvania ranks 6'̂ inthe nation in total population and ranksI" in rural population (The Center forRural Pennsylvania, 2000). The Centerfor Rural Pennsylvania defines rural andurban based on population density.
Alice E. Conway, PhD. CRMP. APRN-BC.is Professor. Department of Nursing,Edinboro (Jniversily of Pennsylvania,Edinboro, PA.
Amy J. McClune. PhD. RN. BC, isAssistant Professor, Department of Nurs-ing, Edinboro University of Pennsylvania.Edinboro, PA.
Patricia Nosel, MN. RN, D.Ed(C), isAssociate Professor, Department of Nurs-ing, Edinboro University of Pennsylvania,Edinboro, PA.
Agriculture continues to rank as the most dangerous industry in theUnited States. The objectives of this pilot study were to identify theincidence of care provided to children involved in farm accidents,examine barriers to utilization of farm safety materials by primaryhealth care practitioners (PHCPs), and determine the percentage ofPHCPs who provide anticipatory guidance related to farm safety.Pender's revised Health Promotion Model (2006) was used, A surveywas developed and mailed to 110 PHCPs of all levels in Morth WestPennsylvania. The return rate was 20%. Types of injuries identified bythe PHCPs included lacerations and musculosketal injuries caused byanimals and farm equipment. Forty-five percent of the PHCPs report-ing asked new patients/families if their children lived or worked on afarm. Eighteen percent specifically focused on farm-related injury pre-vention. Fourteen percent were aware of farm injury prevention mate-rials and 73% were interested in receiving such materials. A largerstudy needs to be conducted to validate these findings.
Rural population refers to a municipali-ty, either a county or school district,that has less than 274 persons persquare mile, or a municipality whosepopulation is less than 2500 persons.Forty-eight of Pennsylvania's 67 coun-ties fall into the rural category (TheCenter for Rural Pennsylvania, 2000).
Between 1982 and 1996. Penn-sylvania ranked 3rd in the nation,behind Texas and North Carolina, forfatal farm-related injuries in childrenunder 20 years of age. Nationwide, thegroup most likely to experience nonfa-tal farm accidents is adolescents(Reed, Westneat. & Kidd, 2003); how-ever, in Pennsylvania [with] 40% offarm fatalities occurred in childrenunder 5 years of age (Adekoya & Pratt.2001). Between 2000 and 2002, a totalof 82 farm-related fatalities werereported across the Commonwealth;27% involved children 19 years of ageor younger. Of the 22 child fatalities, 14(63.6%) involved children under theage of 5 years. Of the total of 82 farm-related fatalities that occurred in thatsame time period, 27% involved chil-dren 19 years of age or younger (seeTable I).
Various groups, including theNational Committee for ChildhoodAgricultural Injury Prevention (NCAIP.
1996) and Farm Safety 4 Just Kids(n.d.), provide resources for farm safe-ty education. These resources includea Farm Safety Day Camp; age-appro-priate publications such as story booksand coloring books featuring the char-acter Cawshus the Crow; DVDs; and arural health and safety kit that includesgames, puzzles, and brochures on top-ics such as food safety, sun safety, andhearing protection. Still, farm-relatedinjuries and fatalities continue to occur.Many factors have been proposed ascontributing to this problem: the lack ofparental supervision, operator fatigue.children performing tasks inappropri-ate for age. and the purposeful dis-abling of safety devices (DeMuri &Purschwitz. 2000).
PurposeThe purpose of this pilot study was
to identify health promotion proceduresthat primary health care practitioners(PHCPs) use to educate children andtheir families about farm safety.Pender's model was used in this studyto describe how PHCPs used the oppor-tunity in their practice to engagepatients in health-promoting behaviorsrelated to farm safety. Specifically, theproject sought to (a) identify the num-ber of farm accidents involving children,
PEDIATRIC NURSING/Janaury-February 2007/Vol. 33/No. 1
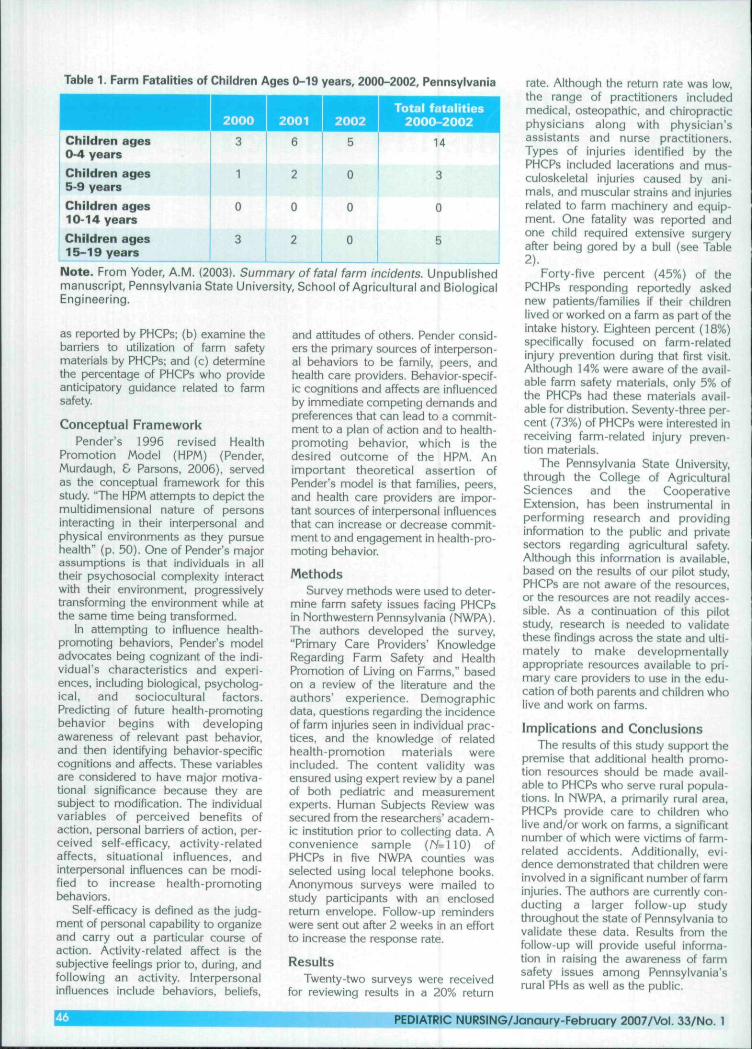
Table 1. Farm Fatalities of Children Ages 0-19 years, 2000-2002, Pennsylvania
Children ages0-4 yearsChildren ages5-9 yearsChildren ages10-14 yearsChildren ages15-19 years
Note. From Yoder, A.M. (2003). Summary of fatal farm incidents. Unpublishedmanuscript, Pennsylvania State University, School of Agricultural and BiologicalEngineering.
2002
5
0
0
0
Total fatalities2000-2002
14
3
0
5
as reported by PHCPs; (b) examine thebarriers to utilization of farm safetymatenals by PHCPs; and (c) determinethe percentage of PHCPs who provideanticipatory guidance related to farmsafety.
Conceptual FrameworkPender's 1996 revised Health
Promotion Model (HPM) (Pender,Murdaugh, & Parsons, 2006), servedas the conceptual framework for thisstudy. "The HPM attempts to depict themultidimensional nature of personsinteracting in their interpersonal andphysical environments as they pursuehealth" {p. 50). One of Pender's majorassumptions is that individuals in alltheir psychosocial complexity interactwith their environment, progressivelytransforming the environment while atthe same time being transformed.
In attempting to influence health-promoting behaviors, Pender's modeladvocates being cognizant of the indi-vidual's characteristics and experi-ences, including biological, psycholog-ical, and sociocultural factors.Predicting of future health-promotingbehavior begins with developingawareness of relevant past behavior,and then identifying behavior-specificcognitions and affects. These variablesare considered to have major motiva-tional significance because they aresubject to modification. The individualvariables of perceived benefits ofaction, personal barriers of action, per-ceived self-efficacy, activity-relatedaffects, situational influences, andinterpersonal influences can be modi-fied to increase health promotingbehaviors.
Self-efficacy is defined as the judg-ment of personal capability to organizeand carry out a particular course ofaction. Activity-related affect is thesubjective feelings prior to, during, andfollowing an activity. Interpersonalinfluences include behaviors, beliefs,
and attitudes of others. Pender consid-ers the primary sources of interperson-al behaviors to be family, peers, andhealth care providers. Behavior-specif-ic cognitions and affects are influencedby immediate competing demands andpreferences that can lead to a commit-ment to a plan of action and to health-promoting behavior, which is thedesired outcome of the HPM. Animportant theoretical assertion ofPender's model is that families, peers,and health care providers are impor-tant sources of interpersonal influencesthat can increase or decrease commit-ment to and engagement in health-pro-moting behavior.
MethodsSurvey methods were used to deter-
mine farm safety issues facing PHCPsin Northwestern Pennsylvania (MWPA),The authors developed the survey,"Primary Care Providers' KnowledgeRegarding Farm Safety and HealthPromotion of Living on Farms," basedon a review of the literature and theauthors' experience. Demographicdata, questions regarding the incidenceof farm injuries seen in individual prac-tices, and the knowledge of relatedhealth-promotion materials wereincluded. The content validity wasensured using expert review by a panelof both pediatric and measurementexperts. Human Subjects Review wassecured from the researchers' academ-ic institution prior to collecting data. Aconvenience sample (/V= 110) ofPHCPs in five MWPA counties wasselected using local telephone books.Anonymous surveys were mailed tostudy participants with an enclosedreturn envelope. Follow-up reminderswere sent out after 2 weeks in an effortto increase the response rate.
ResultsTwenty-two surveys were received
for reviewing results in a 20% return
rate. Although the retum rate was low,the range of practitioners includedmedical, osteopathic, and chiropracticphysicians along with physician'sassistants and nurse practitioners.Types of injuries identified by thePHCPs included lacerations and mus-culoskeletal injuries caused by ani-mals, and muscular strains and injuriesrelated to farm machinery and equip-ment. One fatality was reported andone child required extensive surgeryafter being gored by a bull (see Table2).
Forty-five percent (45%) of thePCHPs responding reportedly askednew patients/families if their childrenlived or worked on a farm as part of theintake history. Eighteen percent (18%)specifically focused on farm-relatedinjury prevention during that first visit.Although 14% were aware of the avail-able farm safety materials, only 5% ofthe PHCPs had these materiais avail-able for distribution. Seventy-three per-cent (73%) of PHCPs were interested inreceiving farm-related injury preven-tion materials.
The Pennsylvania State University,through the College of AgriculturalSciences and the CooperativeExtension, has been instrumental inperforming research and providinginformation to the public and privatesectors regarding agricultural safety.Although this information is available.based on the results of our pilot study,PHCPs are not aware of the resources,or the resources are not readily acces-sible. As a continuation of this pilotstudy, research is needed to validatethese findings across the state and ulti-mately to make developmentallyappropriate resources available to pri-mary care providers to use in the edu-cation of both parents and children wholive and work on farms.
Implications and ConclusionsThe results of this study support the
premise that additional health promo-tion resources should be made avail-able to PHCPs who serve rural popula-tions. In MWPA, a primarily rural area,PHCPs provide care to children wholive and/or work on farms, a significantnumber of which were victims of farm-related accidents. Additionally, evi-dence demonstrated that children wereinvolved in a significant number of farminjuries. The authors are currently con-ducting a larger follow-up studythroughout the state of Pennsylvania tovalidate these data. Results from thefollow-up will provide useful informa-tion in raising the awareness of farmsafety issues among Pennsylvania'srural PHs as well as the public.
PEDIATRIC NURSING/Janaury-February 2a07/Vol. 33/No. 1
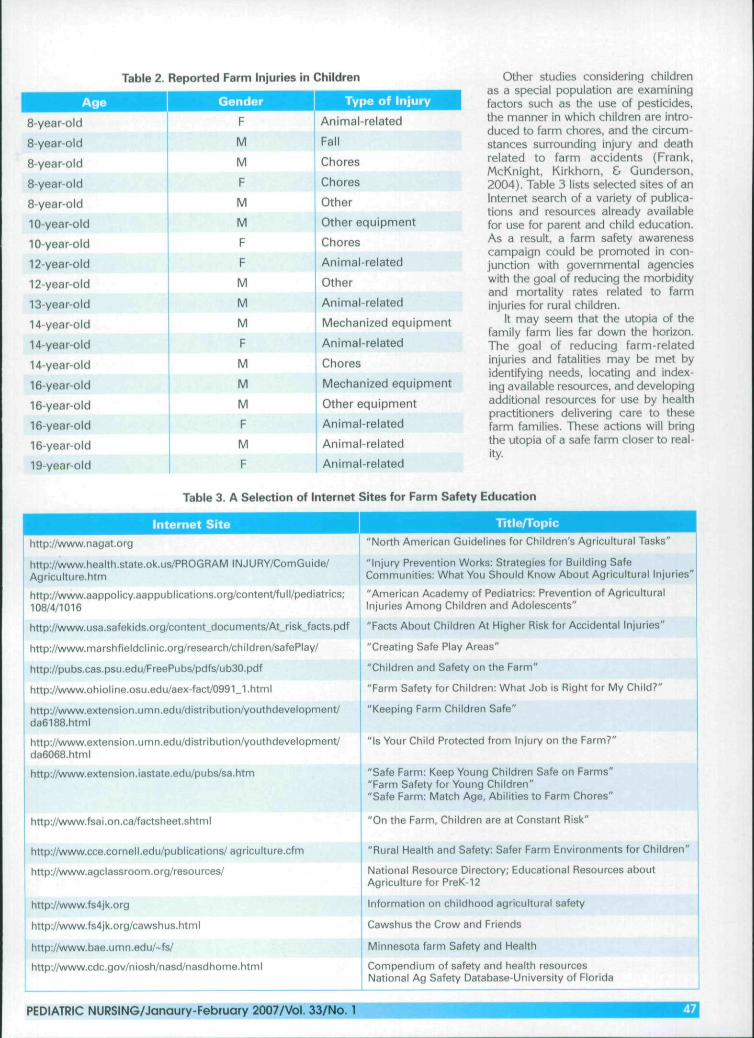
Table 2. Reported Farm Injuries in Children
8-year old
8-year-old
8-year-old
8-year-old
8-year-old
10-year-old
10-year-old
12-year-old
12-year-old
13-year-old
14-year-old
14-year-old
14-year-old
16-year-old
16-year-old
16-year-old
16-year-old
19-year-old
nder Type of Injury
F
M
M
F
M
M
F
F
M
M
M
F
M
M
M
F
M
F
Animal-related
Fall
Chores
Chores
Other
Other equipment
Chores
Animal-related
Other
Animal-related
Mechanized equipment
Animal-related
Chores
Mechanized equipment
Other equipment
Animal-related
Animal-related
Animal-related
Other studies considering childrenas a special population are examiningfactors such as the use of pesticides,the manner in which children are intro-duced to farm chores, and the circum-stances surrounding injury and deathrelated to farm accidents (Frank,McKnight. Kirkhorn, & Gunderson,2004). Table 3 lists selected sites of anInternet search of a variety of publica-tions and resources already availablefor use for parent and child education.As a result, a farm safety awarenesscampaign could be promoted in con-junction with governmental agencieswith the goal of reducing the morbidityand mortality rates related to farminjuries for rural children.
It may seem that the Utopia of thefamily farm lies far down the horizon.The goal of reducing farm-relatedinjuries and fatalities may be met byidentifying needs, locating and index-ing available resources, and developingadditional resources for use by healthpractitioners delivering care to thesefarm families. These actions will bringthe Utopia of a safe farm closer to real-ity.
Table 3. A Selection of Internet Sites for Farm Safety Education
Internet Sitehttp://www.nagat.org
http://www.health.state.ok.us/PROGRAM INJURY/ComGuide/Agriculture.htm
http://www.aappolicy.aappublications.org/content/full/pediatrics;108/4/1016
http://www,usa.safekids.org/content_documents/At_risk_facts.pdf
http://www.marshfieldclinic.org/research/children/safePtay/
http://pubs.cas.psu.edu/FreePubs/pdfs/ub30.pdf
http://www.ohioline.osu.edu/aex-fact/0991_1.html
http://www.extension.umn.edu/distribution/youthdevelopment/da6188.html
http://www.exlension.umn.edu/distribution/youthdevelopment/da6068.html
http://www.extension.iastate.edu/pubs/sa.htm
http://www,fsai.on.ca/factsheet.shtml
http://wvi'w.cce.cornell.edu/publications/agriculture.cfm
http://www.agclassroom.org/resources/
http://www,fs4jk.org
http://www.fs4jk.org/cawshus.html
http://www.bae.umn.edu/-fs/
http://www.cdc.gov/niosh/nasd/nasdhome.html
Title/Topic"North American Guidelines for Children's Agricultural Tasks"
"Injury Prevention Works: Strategies for Building SafeCommunities: What You Should Know About Agricultural Injuries*
"American Academy of Pediatrics: Prevention of AgriculturalInjuries Among Children and Adolescents"
"Facts About Children At Higher Risk for Accidental Injuries"
"Creating Safe Play Areas"
"Children and Safety on the Farm"
"Farm Safety for Children: What Job is Right for My Child?"
"Keeping Farm Children Safe"
"Is Your Child Protected from Injury on the Farm?"
"Safe Farm: Keep Young Children Safe on Farms""Farm Safety for Young Children""Safe Farm: Match Age, Abilities to Farm Chores"
"On the Farm, Children are at Constant Risk"
"Rural Health and Safety: Safer Farm Environments for Children"
National Resource Directory; Educational Resources aboutAgriculture for PreK-12
Information on childhood agricultural safety
Cawshus the Crow and Friends
Minnesota farm Safety and Health
Compendium of safety and health resourcesNational Ag Safety Database-University of Florida
PEDIATRIC NURSING/Janaury-February 2007/Vol. 33/No. 1

ReferencesAdekoya, N., & Pratt, S.G. (2001). Fata! intentional farm injuries
among persons less than 20 years of age in the United States:Geographic profiles. Washington, DC: Department of Healthand Human Services. Retrieved January 2, 2007 fromhttp:/Aflrt'vw.CDC.gov/niosh/chlldag.
DeMuri, G.R, & Purschwitz, M,A, (2000, December). Farm Injuries inchildren: A review, Wisconsin MedicaiJournal, 99(9), 51-55.
Frank, A.L, McKnight, R., Kirkhorn, S.R., & Gunderson, P. (2004).Issues of agricultural safety and health. Annual Review ofPublic Heaith. 25(1), 225-245.
National Agricultural Statistics Service, (n.d.). 1998 childhood agri-cultural injuries. Retrieved October 18, 2003, fromhtp://osda.mannlib.cornell.edu/reports/nassr/other/injury/injr1099.pdf
National Committee for Childhood Agricultural Injury Prevention(1996). Childrend and agriculture: opportunities for safety andhealth. Marshfield, WI: Marshfield Clinic.
Pender, N,J., Murdaugh, C.L., & Parsons, M.A. (2006). Health pro-motion in nursing practice. (5"' ed.). Upper Saddle River, NJ:Pearson Pentice Hall.
Reed, D.B., Westneat, S.C, & Kidd, P. (2003) Observation study ofstudents who completed a high school agricultural safety edu-cation program. Journal of Agricultural Safety and Heaith, 9(4),275-283.
The Center for Rural Pennsylvania (2000). Demographics:Rural/Urban PA. Retrieved October 18, 2003 from http://rural-pa.org/about.html
Yoder, A.M., (2003). Summary of fatal farm incidents. Unpublishedmanuscript. Pennsylvania State University, School ofAgricultural and Biological Engineering.
PNP Care Coordinator Modelcotitinued from page 34
Bender, N.L. (2003). An analysis ofthe processes and outcomes ofcoordination of care: A home care organization initiated casemanagement intervention in a Medicare population.Unpublished doctoral dissertation. University of Rochester,Rochester, New York.
King, L., Lee, J.L., & Henneman, E. (1993). A collaborative practicemodel for critical care. American Journai of Critical Care, 2(6),444-449.
Lindeke, L.L., Leonard, B.J., Presler, B., & Garwick, A. (2002).Family-centered care coordination for children with specialneeds across multiple settings. Journal of Pediatric HealthCare, 16{6), 290-297.
McPherson, M., Arango, P., Fox, H., Lauver, C, McManus. M,,Newacheck, P.W., Perrin, J.M., Shonkoi^, J.P, & Strickland. B.(1998). A new definition of children with special health careneeds. Pediatrics, /02(1), 137- 139.
Stille, C. J., & Antonelli, R.C. (2004), Coordination of care for chil-dren with special health care needs. Current Opinions inPediatrics, 76(6), 700-705.
Strickland, B., McPherson, M,, Weissman, G., VanDyck, P., Huang,Z.J., & Newacheck, P (2004). Access to the medical home:Results of the national survey of children with special careneeds. Pediatrics, 77.3(5), 1485-1492.
Whitcomb, R., Wilson, S., Chang-Dawkins, S., Durand, J., Pitcher,D., Lauzon, C, & Aleman, D. (2002). Advanced practice nuris-ng: Acute care modal in progress. Journai of Nursing Admi-nistration, 52(3), 123-125.
^ FOR THECOUNTLESS
LITTLEREASONS
H you got into nursing.
CHRISTUS Santa Rosa Children's Hospital is seeking a DIRECTOR OF PATIENT CARE SERVICES for its 200+ bed academicchildren's hospital. This position will direct, supervise and coordinate all nursing personnel, functions and activities in patientcare areas and as.signed areas of responsibility. Candidates must have a bachelor's degree in nursing, master's preferred, licenseby the State of Texas and a min. of 3-5 years demonstrated satisfactory performance as a director or manager.
CHRISTUS Santa Rosa Children's Hospital is located in beautiful San Antonio, TX and is thecity's only pediatric academic hospital, Recently rated in tbe top 10% nationally for patientsatisfaction its renov f̂ned services include a dedicated ER, enhanced NICU and PICU.national Congenital Heart Program as well as future plans for trauma and transplant services.
To learn more or to apply online, visit www. heavenly careers.com
As a faith-based organization. CHRISTUS Santa Rosa believes in the value and dignity of each individual. We i^edge tn evaliiate allcandidates based solely on their talents, regardless cif racr. rdigiiin or disabilily. Pre-placement ph)-sical ajid drug screening rfquiri'd
CHRISTUS.SANTA ROSAChildren's Hospital
Work at CSR. The Remmis Are Eternal.
San Antonio, Texas | 800-880-NURSwww.heavenlycareers.coni
PEDIATRIC NURSING/Janaury-February 2007/Vol. 33/No. 1