Embed Size (px)
Citation preview
Opioids in persistent, non-cancer pain
Dr Angus RobinBradford VTS Feb 18th 2014
(with some slides from Dr Tim Williams and Dr F Cole)

WHO pain ladder
Was designed for cancer pain.Methadone was initially planned, morphine in
the end....Gives us ‘permission’ to escalate doses v
quickly – or so it seems.Doesn’t remind us about topical things or
neuropathic agents.

“But the drugs don’t work Dr...”

Expect analgesic failure; pursue analgesic success (BMJ 8th June 2013, page 19-21)
Most analgesics don’t work for most people, when you define ‘work’ as a 50% reduction (NNT...)
Most studies in acute post-op pain...so useless in the vast majority of patients.
Very few studies beyond 12 weeks.
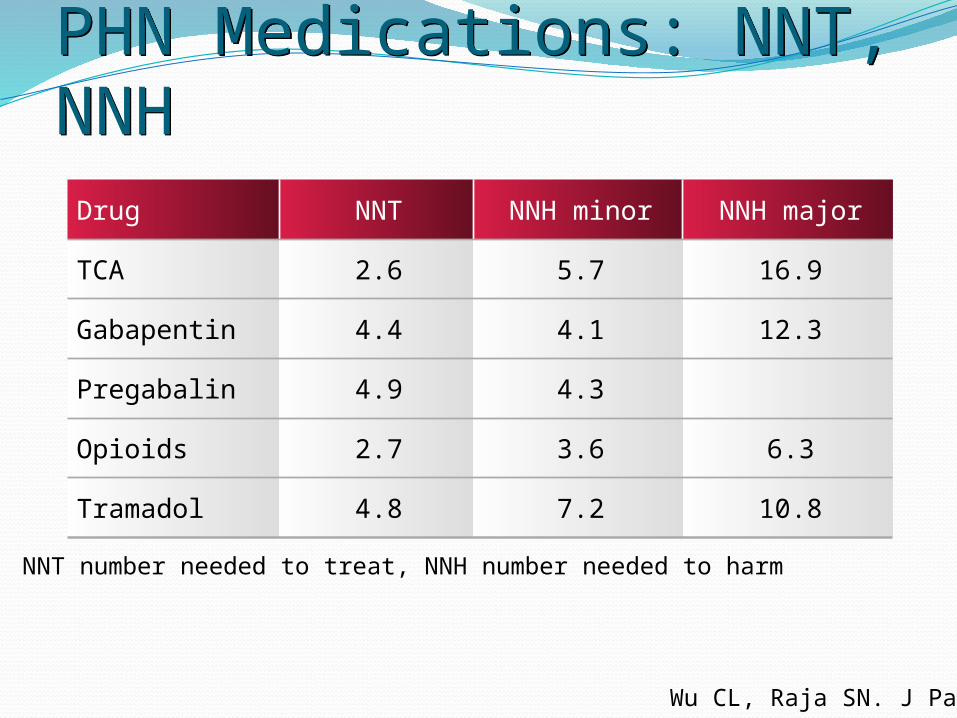
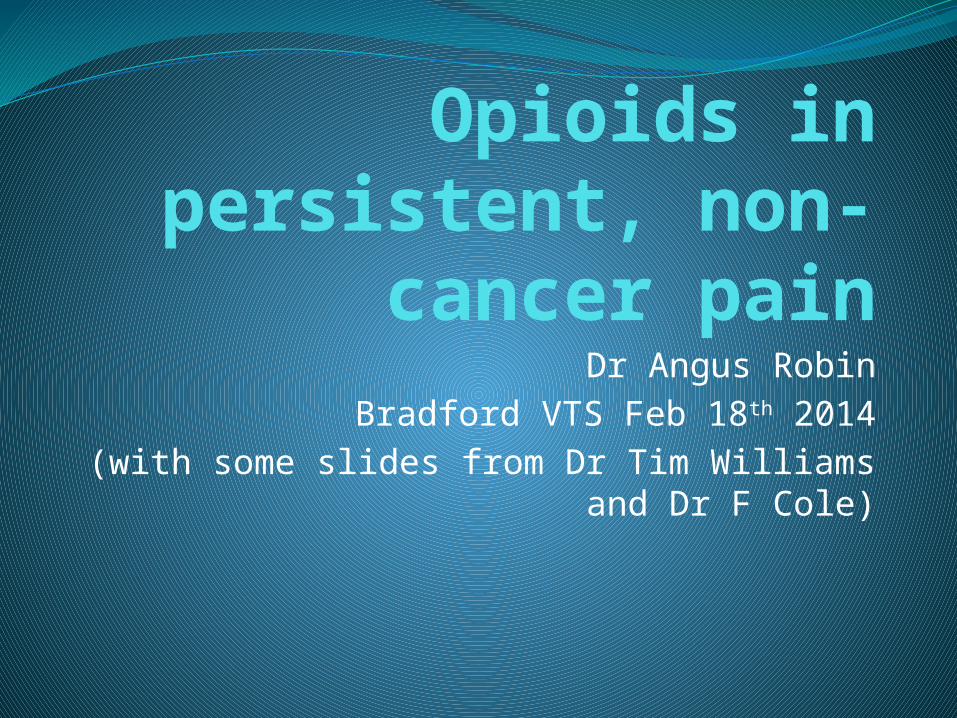
Drug NNT NNH minor NNH major
TCA 2.6 5.7 16.9
Gabapentin 4.4 4.1 12.3
Pregabalin 4.9 4.3
Opioids 2.7 3.6 6.3
Tramadol 4.8 7.2 10.8
PHN Medications: NNT, NNHPHN Medications: NNT, NNH
NNT number needed to treat, NNH number needed to harm
Wu CL, Raja SN. J Pain 2008

In low back pain tapentadol has a 90% failure rate (to give 50% relief) and oxycodone has a 100% failure rate.
This is consistent with observations of other opioids and what we see in the pain rehab ‘living with pain’ team.

When they do work they improve sleep, mood, fatigue, QoL, etc (unsurprisingly).
If one drug in a class fails, others may not, so we don’t know the best order to try drugs which mainly fail.
Due to low success rates, is polypharmacy the answer? (can of worms time....serotonin syndrome, etc).
A 50% pain reduction in a small group of patients is worth seeking out....
Expect modest benefits and frame patient expectations of analgesia benefits more realistically
Mention relaxation therapies as useful tools in setbacks / flare-ups
All the meds can help, but nowhere near as much as pharma wants us to think
Before you start opioids
Be aware safety and efficacy of long term opiates is uncertain.
Be aware of BPS guidance.Do a comprehensive Pain assessment
Including ……. The meds they’ve tried (and how long for – actually go through the records)
Co-morbid conditionsGOALS and WIDER
PLAN
There is no evidence from RCTs to support that benefits of long term opioid therapy outweigh the risks.

Starting OpioidsDiscuss well established side effects Appropriate preparation
Long-acting Dose Never injectable (rarely short-act)
Start low and go slow (<120mg/day)Co prescribe anti-emetic + laxative Agree follow up interval (1-2 weeks, then
monthly) Same prescriber ideallyConsider a contract
Opiate Adverse Effects80% will experience side effects
constipationnausea/vomitingitchdizzinesssedation (driving?) ...anecdote re: bus driver
Long term immunological/endocrine effectAddiction, dependence. “Using for sleep Dr”Withdrawal (sweat/cramps/yawn/tremor)Opioid induced hyperalgesia is rare, but
real.
Hormonal disturbanceGnRH reduced and subsequent effects on
FSH/LH levels.Leads to androgen/oestrogen level changes.Prolactin possibly increased.TFTs seem unaffected.Worsens diabetes, worsens obesity
(multifactoral).

Mortality data
In the US opioid related deaths rose from 4041 in 1999 to 14459 in 2007.
This is more than road traffic accidents.
In the UK deaths from prescribed opioids roughly doubled between 2005-09.

Approximate equivalent dosesN.B. There is no universal agreement
24 hour dose Morphine equivalent per day
Codeine 240 mg 40mg (26 – 60)
Dihydrocodeine 240 mg 50mg
Tramadol 400 mg Up to 120mg
Oxycodone 20mg 40mg
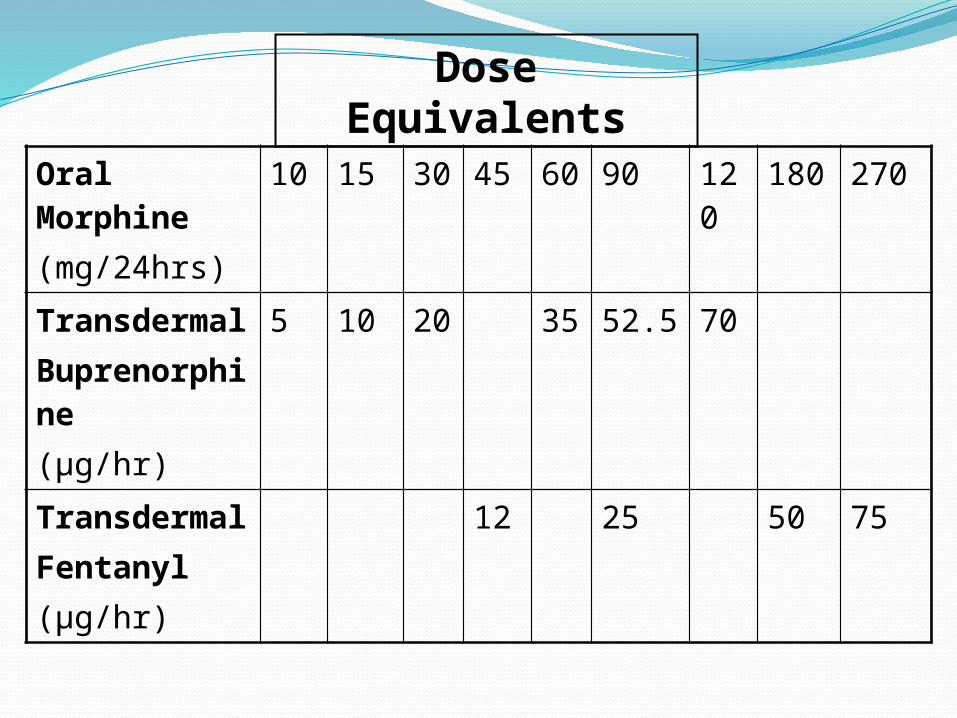
Oral Morphine(mg/24hrs)
10 15 30 45 60 90 120 180 270
TransdermalBuprenorphine(µg/hr)
5 10 20 35 52.5 70
TransdermalFentanyl(µg/hr)
12 25 50 75
Dose Equivalents
Managing established patientsRegular review (monthly/6monthly)
to include….. effectivenessside effectsplan complianceprogression to goalsclear documentation
Alternatives for ‘flare-up’ management. Ideally this is where ‘compassion days’ come in....pacing skills.
Flare-Up ManagementEstablish ‘flare-up’ and not new painRe-assurance that will settleConsider short- term changes to other
analgesics or use of alternatives E.g. TNS, relaxation techniques, pacing activities, self-compassion!(DWP not keen on this)
Avoid dose escalation....A&E struggle with this.

Stopping Opiates – When and HowWhen? Patient’s pain and function not
improved, or is worse.Concerns over addictive
behaviour.Unacceptable adverse effects.Patient preference.
How? Slow/gradual dose reductionConsider other pain relieving
strategies.

The future of opioid management (is it nearly now?)

So what about GP now?Tramadol KPPI in Bradford and Airedale
Tramadol is an opioid analgesic indicated for moderate tosevere pain. Tramadol is a potent drug; at 200mg/day it isequivalent to 40mg of oral morphine in 24hrs.Tramadol is available as 12-hourly and 24-hourly modifiedrelease preparations. These preparations are significantlymore expensive than the immediate release formulations andrestrict the up or down titration of the analgesicaccording to the patient’s symptoms.
All patients who are prescribed analgesics should havetheir pain symptoms and treatment reassessed on a regularbasis.

SummaryWe need patients to know that the medicines
will probably help less than we thought.We need to give them more information and
review pain medicines better.We need to believe that other methods of
dealing with chronic pain help and take the time to encourage a patients to engage with this.
BPS guidanceSummary page:
http://www.britishpainsociety.org/book_opioids_recommendations.pdf
Patients version: http://www.britishpainsociety.org/book_opioid_patient.pdf