Embed Size (px)
Citation preview
1
TB Prevention, innovating an old idea to reach a new target:
TB Elimination
Davide Manissero, MD
Senior Director, Medical and Scientific Affairs
QuantiFERON, EMEA & APAC
DISCLOSURE
I am currently a QIAGEN employee.
The information and opinions provided hereby are b ased
solely on my personal experience and judgment and d o not
represent QIAGEN’s opinion.
TB PREVENTION BIAS
4
LTBI Screening Tools
Targeted Testing – Migrant Case Study
TB Prevention – global policy breakthrough
Targeted Testing – HCW Case Study
Thanks to two innovators:
………. but the world has changed.
Robert KochRobert KochRobert KochRobert Koch
Karel StybloKarel StybloKarel StybloKarel Styblo
“….for the control of the disease, the sources from which the infectious
material flows must be closed as far as is humanly possible……
the most essential one, is thesputum of consumptives .”
70% case detection
85% treatment success
Georges CanettiGeorges CanettiGeorges CanettiGeorges Canetti
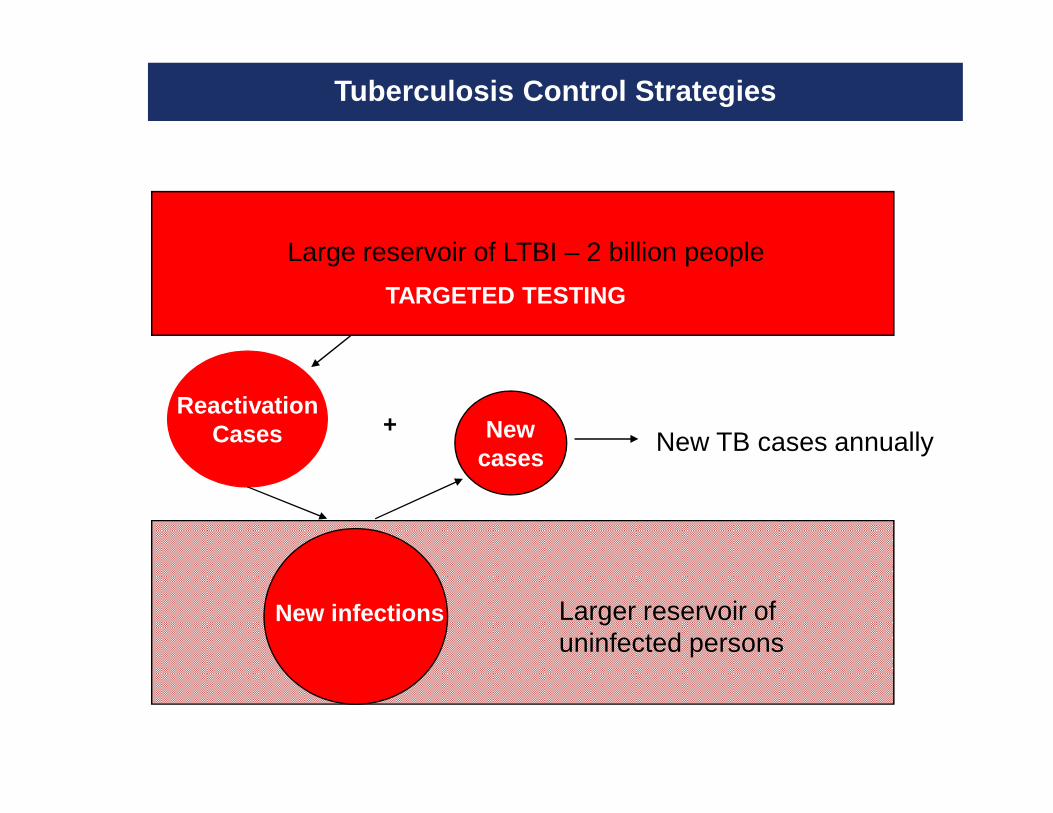
Tuberculosis Control Strategies
ReactivationCases
Large reservoir of LTBI – 2 billion people
Larger reservoir of uninfected persons
Newcases
New infections
+New TB cases annually
TARGETED TESTING
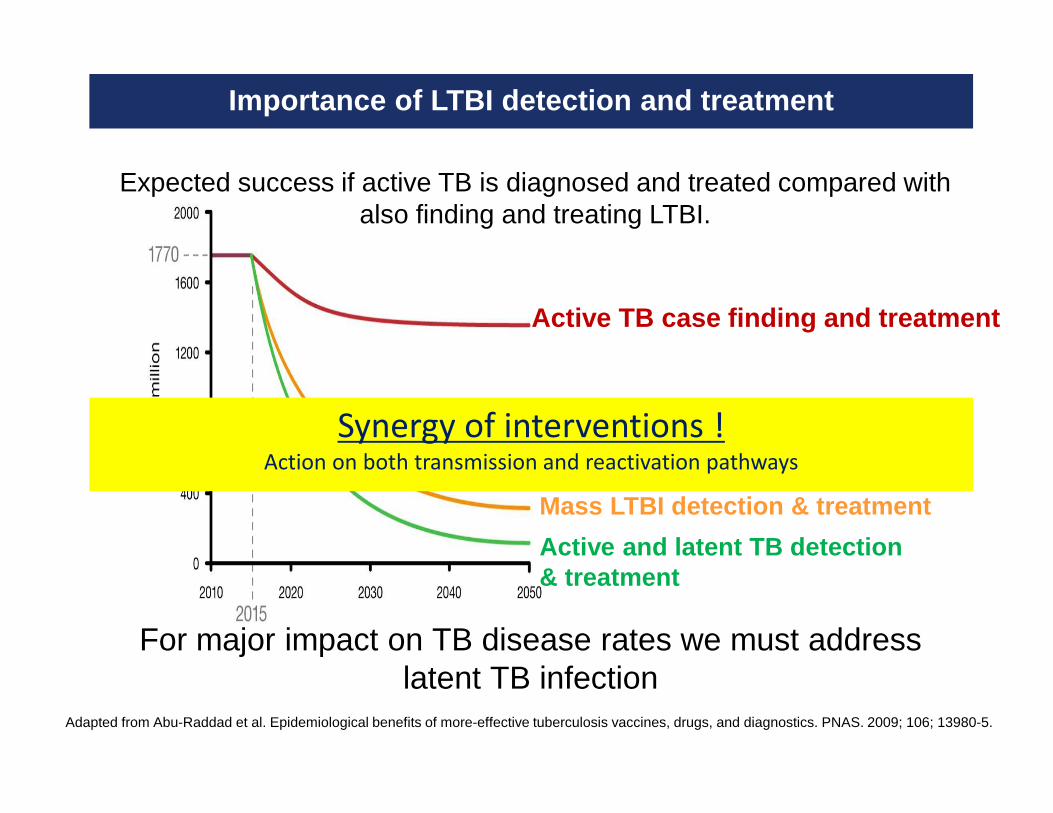
Importance of LTBI detection and treatment
Active TB case finding and treatment
Mass LTBI detection & treatment
Active and latent TB detection& treatment
Expected success if active TB is diagnosed and treated compared with also finding and treating LTBI.
For major impact on TB disease rates we must address latent TB infection
Adapted from Abu-Raddad et al. Epidemiological benefits of more-effective tuberculosis vaccines, drugs, and diagnostics. PNAS. 2009; 106; 13980-5.
Synergy of interventions !Action on both transmission and reactivation pathways
2 new policies and a guideline
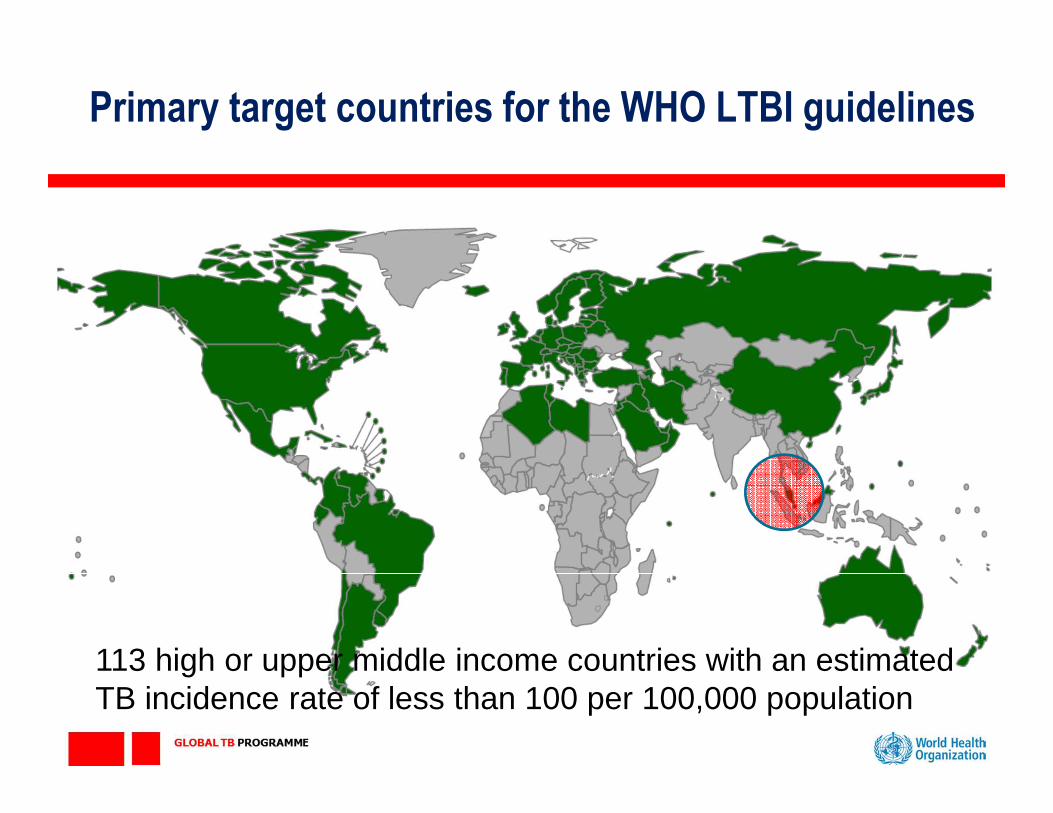
Primary target countries for the WHO LTBI guidelines
113 high or upper middle income countries with an estimated TB incidence rate of less than 100 per 100,000 population
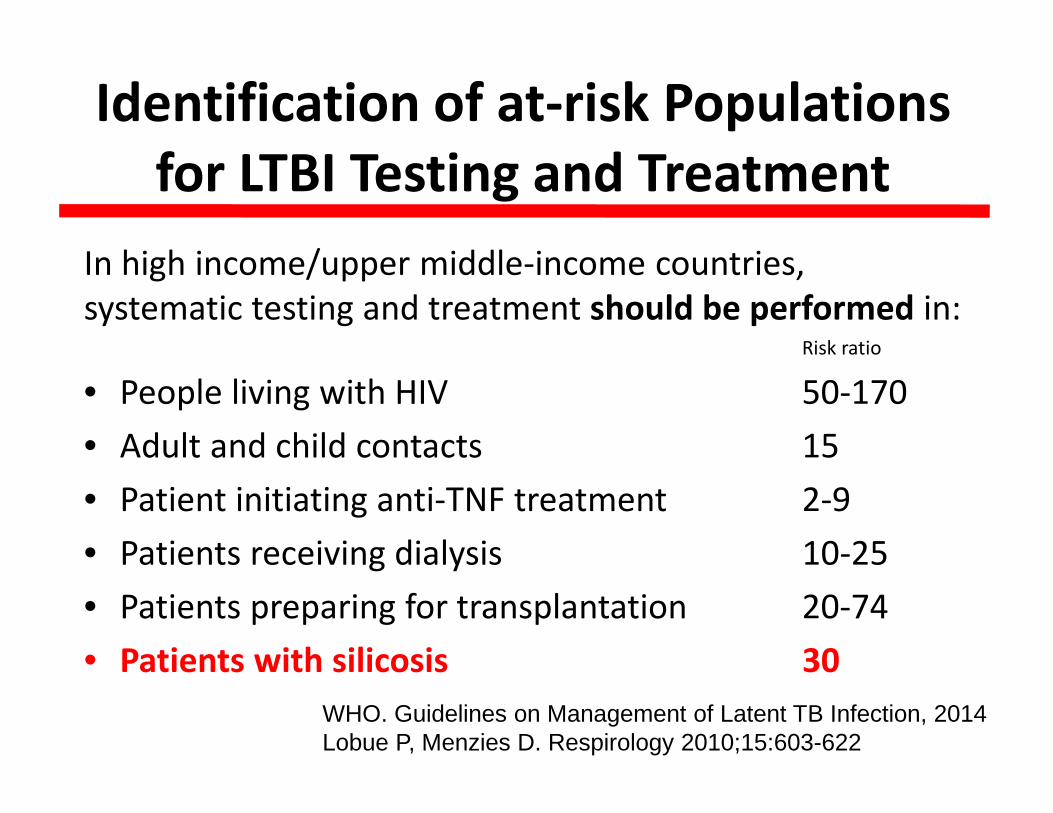
Identification of at-risk Populations
for LTBI Testing and Treatment
In high income/upper middle-income countries,
systematic testing and treatment should be performed in:Risk ratio
• People living with HIV 50-170
• Adult and child contacts 15
• Patient initiating anti-TNF treatment 2-9
• Patients receiving dialysis 10-25
• Patients preparing for transplantation 20-74
• Patients with silicosis 30
WHO. Guidelines on Management of Latent TB Infection, 2014Lobue P, Menzies D. Respirology 2010;15:603-622
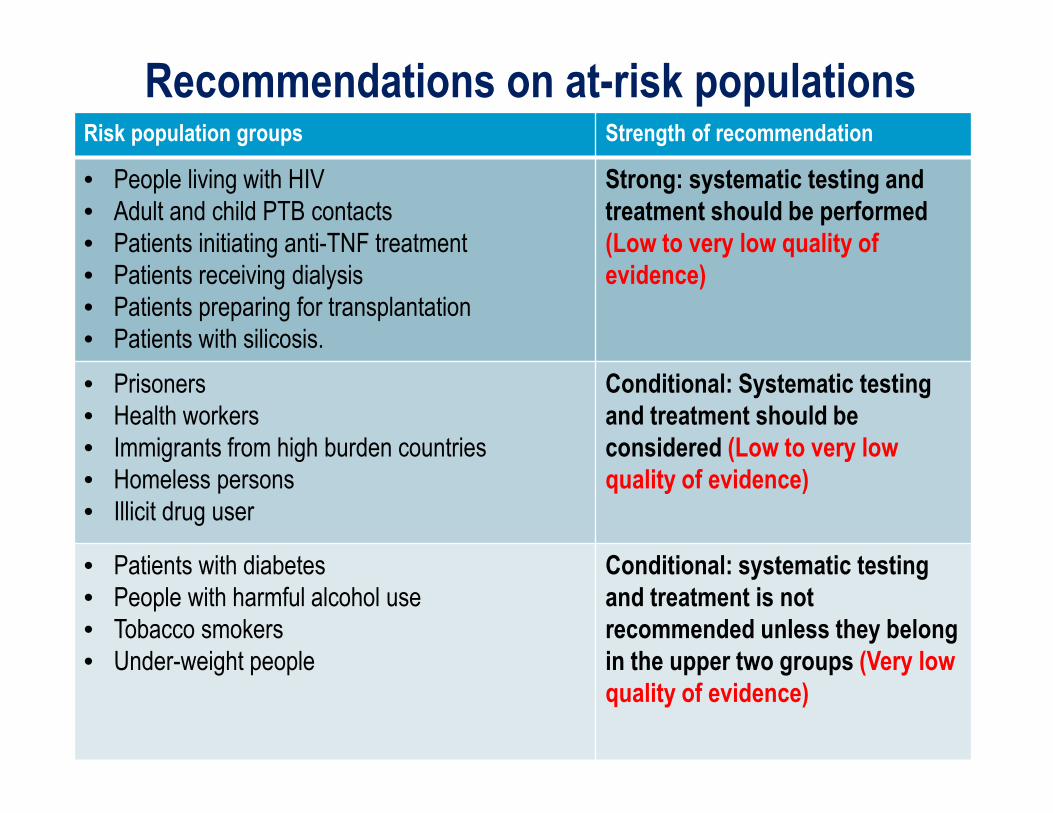
Recommendations on at-risk populationsRisk population groups Strength of recommendation
• People living with HIV
• Adult and child PTB contacts
• Patients initiating anti-TNF treatment
• Patients receiving dialysis
• Patients preparing for transplantation
• Patients with silicosis.
Strong: systematic testing and
treatment should be performed
(Low to very low quality of
evidence)
• Prisoners
• Health workers
• Immigrants from high burden countries
• Homeless persons
• Illicit drug user
Conditional: Systematic testing
and treatment should be
considered (Low to very low
quality of evidence)
• Patients with diabetes
• People with harmful alcohol use
• Tobacco smokers
• Under-weight people
Conditional: systematic testing
and treatment is not
recommended unless they belong
in the upper two groups (Very low
quality of evidence)
Either TST or IGRA can be used to test for latent TB infection.
IGRA should not replace TST in low and middle income
countries1.
(Strong recommendation, very low quality of evidence)
Recommendation on ruling in latent TB infection
1 Use of tuberculosis interferon-gamma release assays (IGRAS) in low- and middle-income countries. Policy
statement. Geneva: World Health Organization; 2011.
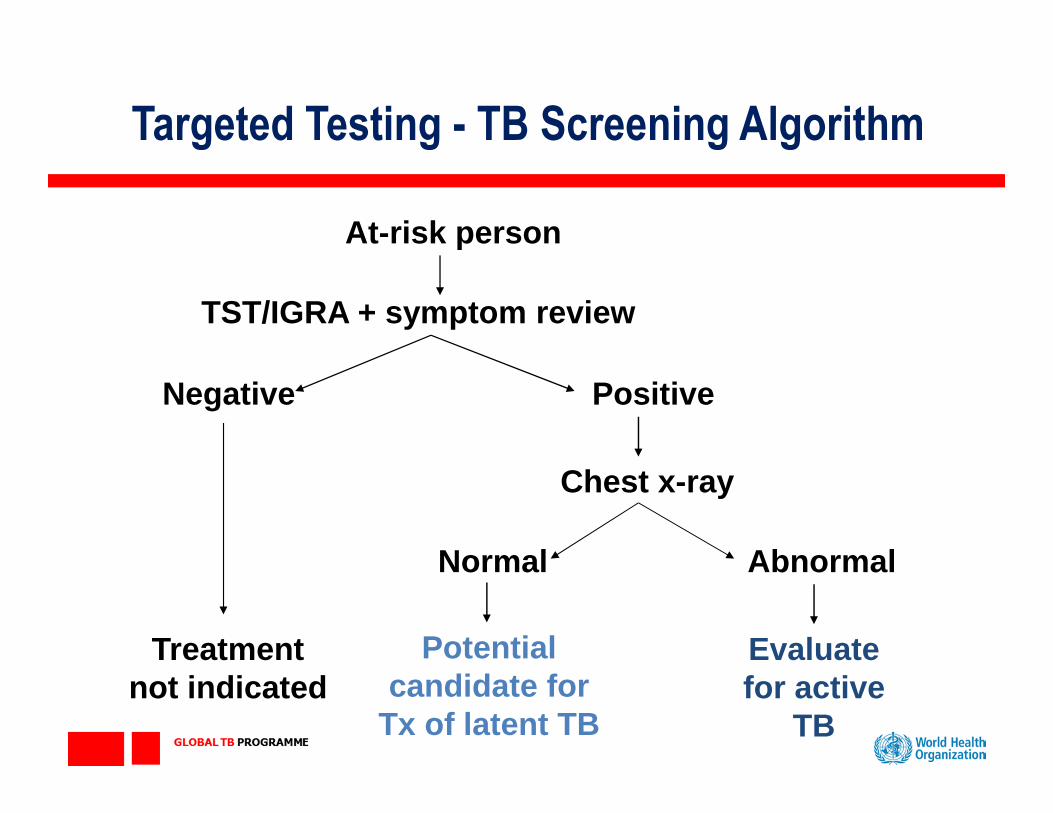
Targeted Testing - TB Screening Algorithm
Evaluate for active
TB
At-risk person
TST/IGRA + symptom review
Negative Positive
Chest x-ray
Normal Abnormal
Treatmentnot indicated
Potential candidate for
Tx of latent TB
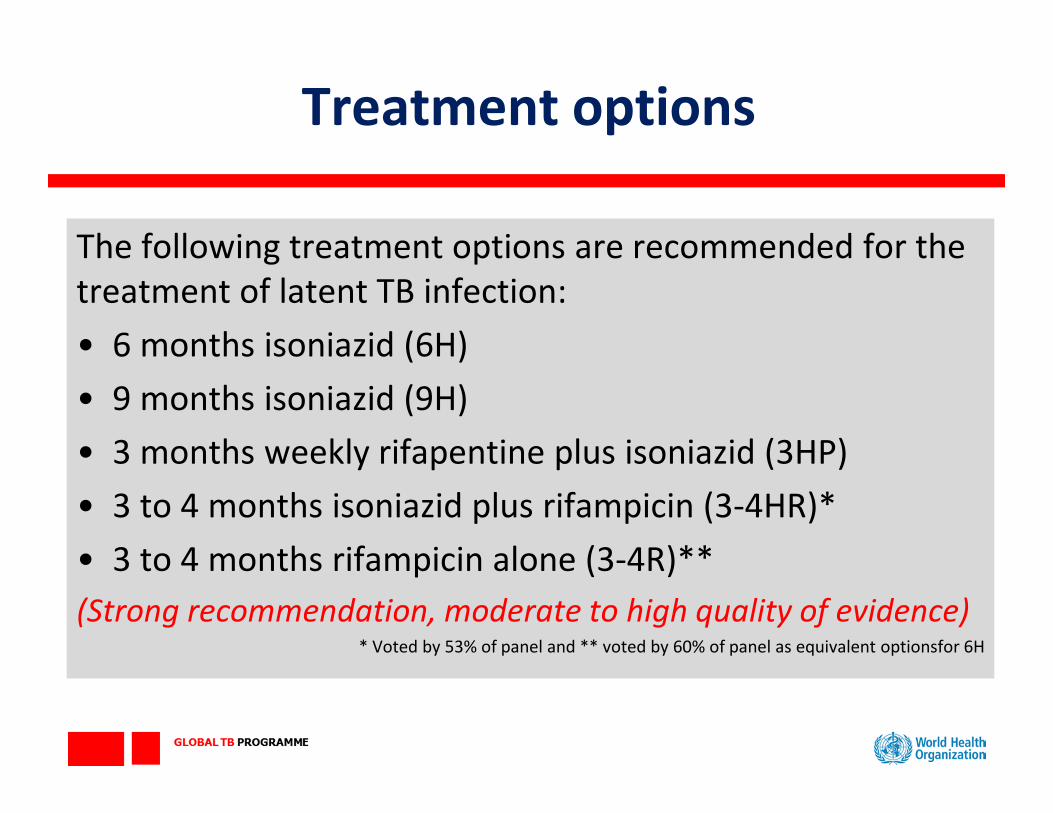
The following treatment options are recommended for the
treatment of latent TB infection:
• 6 months isoniazid (6H)
• 9 months isoniazid (9H)
• 3 months weekly rifapentine plus isoniazid (3HP)
• 3 to 4 months isoniazid plus rifampicin (3-4HR)*
• 3 to 4 months rifampicin alone (3-4R)**
(Strong recommendation, moderate to high quality of evidence) * Voted by 53% of panel and ** voted by 60% of panel as equivalent optionsfor 6H
Treatment options
17
LTBI Screening Tools
Targeted Testing – Migrant Case Study
TB Prevention – global policy breakthrough
Targeted Testing – HCW Case Study
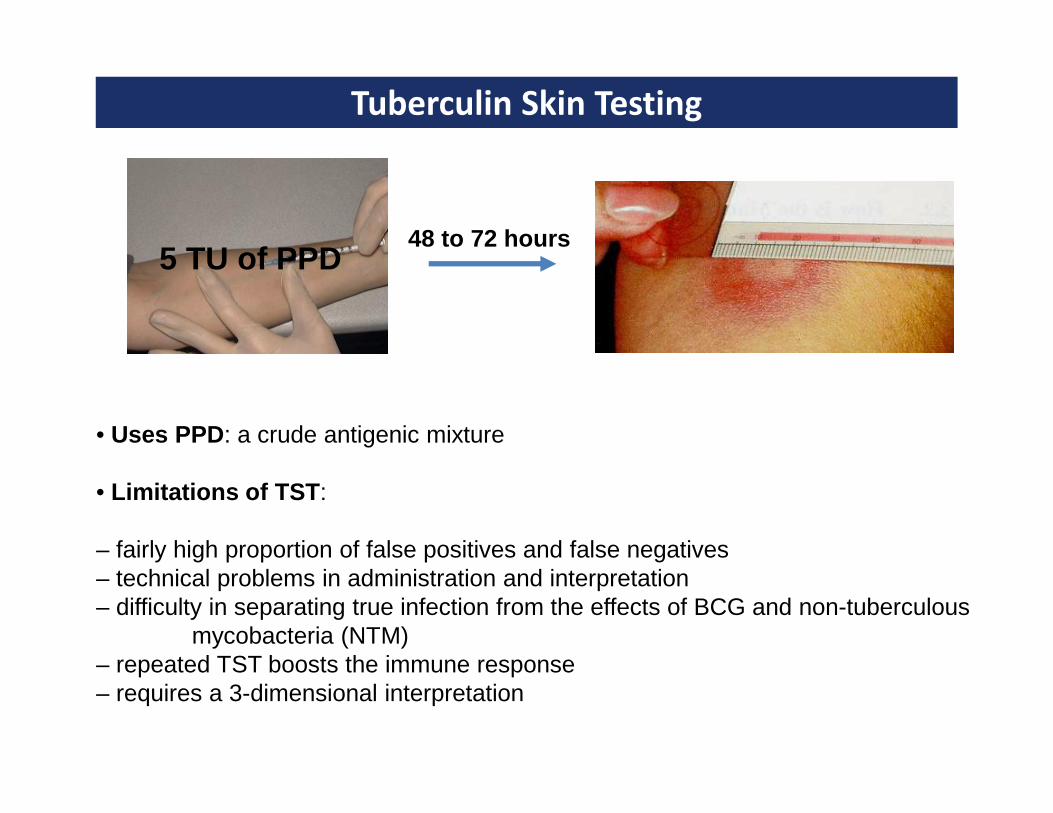
Tuberculin Skin Testing
48 to 72 hours5 TU of PPD
• Uses PPD : a crude antigenic mixture
• Limitations of TST :
– fairly high proportion of false positives and false negatives– technical problems in administration and interpretation– difficulty in separating true infection from the effects of BCG and non-tuberculous
mycobacteria (NTM)– repeated TST boosts the immune response– requires a 3-dimensional interpretation
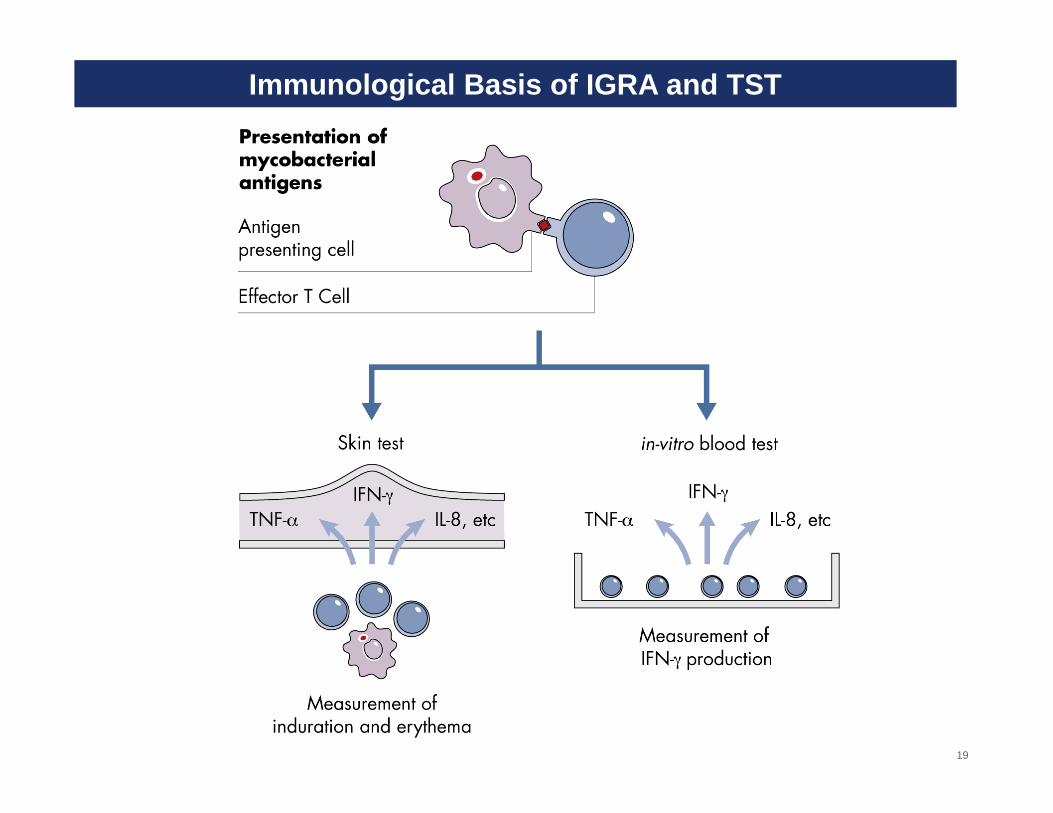
Immunological Basis of IGRA and TST
19

QuantiFERON-PLUS exploring CD8 response
20
21
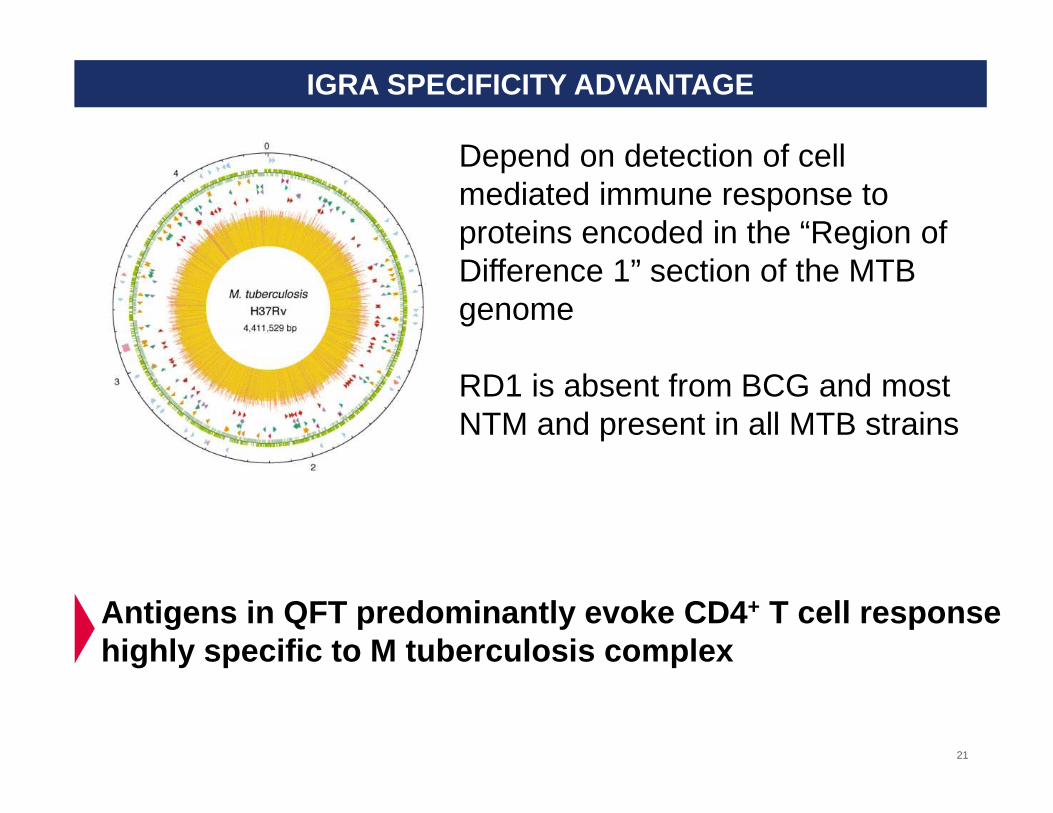
Depend on detection of cell mediated immune response to proteins encoded in the “Region of Difference 1” section of the MTB genome
RD1 is absent from BCG and most NTM and present in all MTB strains
IGRA SPECIFICITY ADVANTAGE
Antigens in QFT predominantly evoke CD4 + T cell response highly specific to M tuberculosis complex
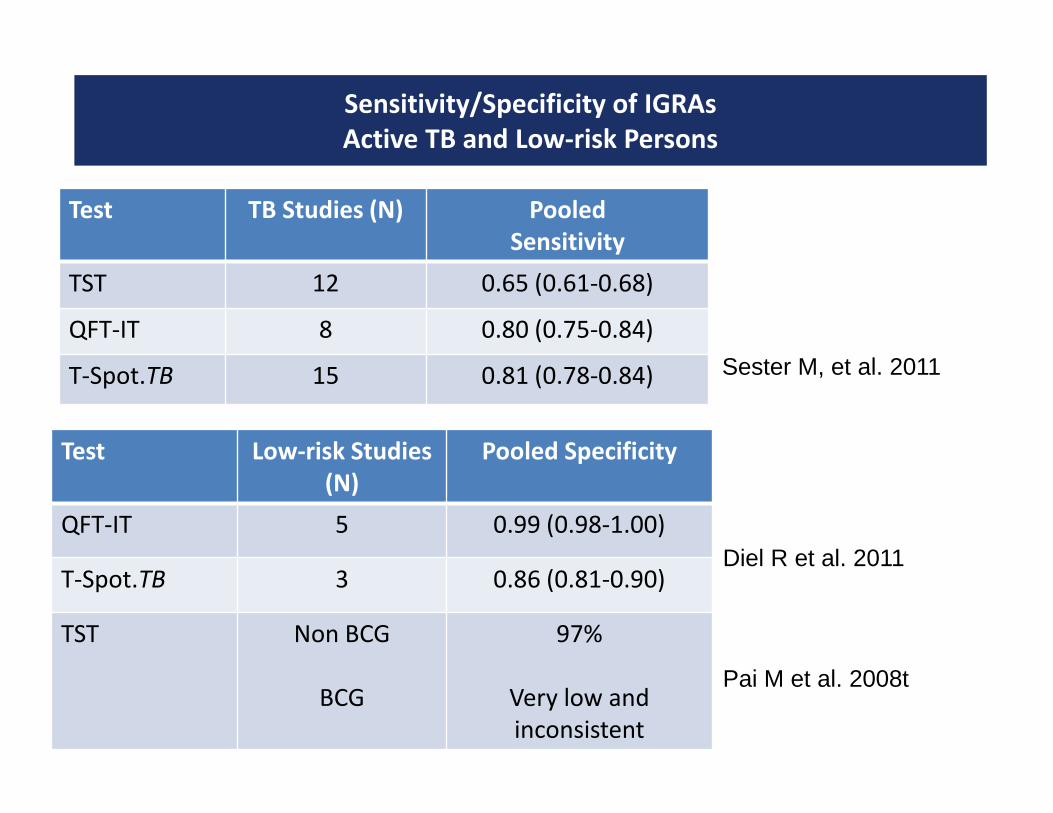
Sensitivity/Specificity of IGRAs
Active TB and Low-risk Persons
Test TB Studies (N) Pooled
Sensitivity
TST 12 0.65 (0.61-0.68)
QFT-IT 8 0.80 (0.75-0.84)
T-Spot.TB 15 0.81 (0.78-0.84) Sester M, et al. 2011
Test Low-risk Studies
(N)
Pooled Specificity
QFT-IT 5 0.99 (0.98-1.00)
T-Spot.TB 3 0.86 (0.81-0.90)
TST Non BCG
BCG
97%
Very low and
inconsistent
Diel R et al. 2011
Pai M et al. 2008t
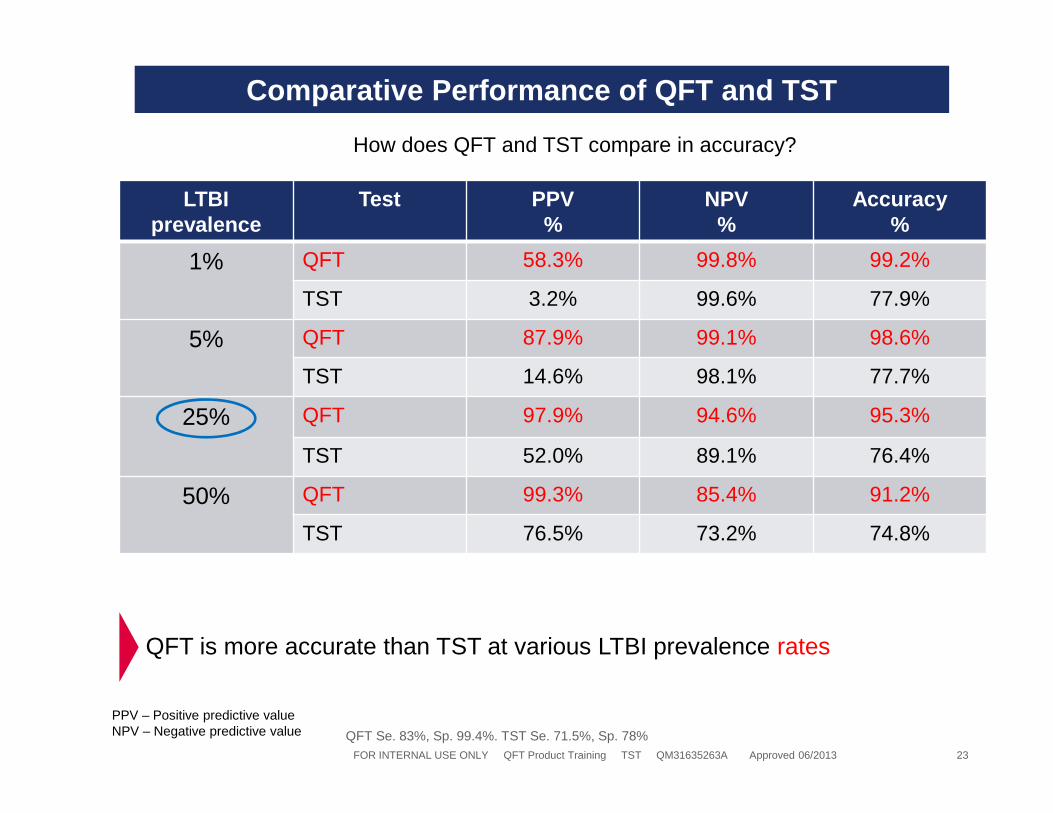
Comparative Performance of QFT and TST
LTBIprevalence
Test PPV%
NPV %
Accuracy%
1% QFT 58.3% 99.8% 99.2%
TST 3.2% 99.6% 77.9%
5% QFT 87.9% 99.1% 98.6%
TST 14.6% 98.1% 77.7%
25% QFT 97.9% 94.6% 95.3%
TST 52.0% 89.1% 76.4%
50% QFT 99.3% 85.4% 91.2%
TST 76.5% 73.2% 74.8%
FOR INTERNAL USE ONLY QFT Product Training TST QM31635263A Approved 06/2013 23
How does QFT and TST compare in accuracy?
QFT Se. 83%, Sp. 99.4%. TST Se. 71.5%, Sp. 78%
PPV – Positive predictive valueNPV – Negative predictive value
QFT is more accurate than TST at various LTBI prevalence rates
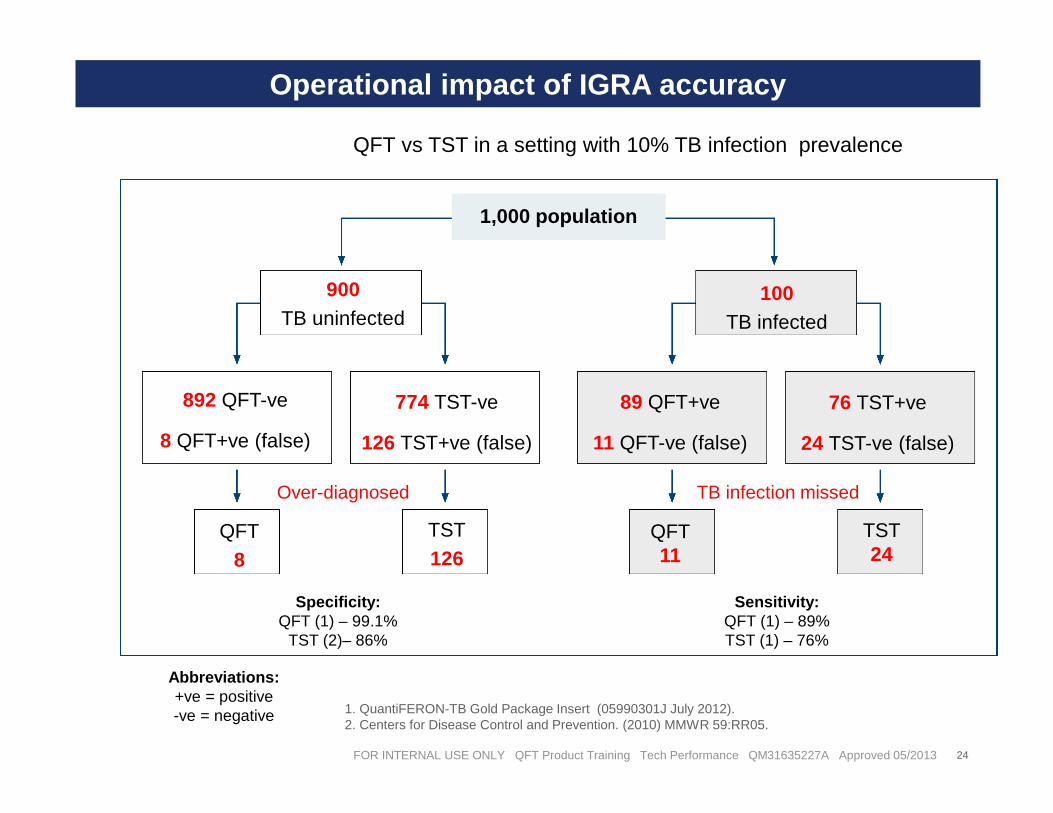
Specificity:QFT (1) – 99.1%
TST (2)– 86%
Sensitivity:QFT (1) – 89%TST (1) – 76%
Over-diagnosed TB infection missed
Operational impact of IGRA accuracy
FOR INTERNAL USE ONLY QFT Product Training Tech Performance QM31635227A Approved 05/2013 24
QFT vs TST in a setting with 10% TB infection prevalence
1,000 population
900TB uninfected
100TB infected
892 QFT-ve
8 QFT+ve (false)
774 TST-ve
126 TST+ve (false)
89 QFT+ve
11 QFT-ve (false)
76 TST+ve
24 TST-ve (false)
QFT8
TST126
QFT11
TST24
Abbreviations:+ve = positive-ve = negative 1. QuantiFERON-TB Gold Package Insert (05990301J July 2012).
2. Centers for Disease Control and Prevention. (2010) MMWR 59:RR05.
25
LTBI Screening Tools
Targeted Testing – Migrant Case Study
TB Prevention – global policy breakthrough
Conclusions
One third of the world population is infected with TB
26
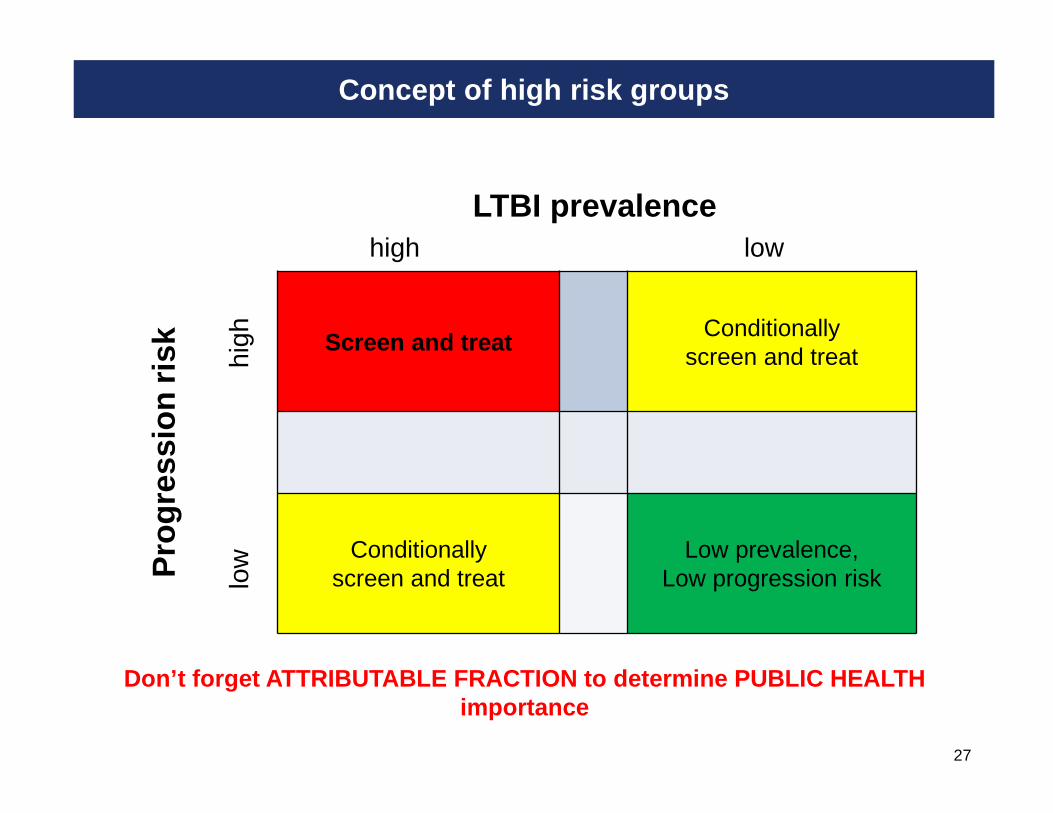
Concept of high risk groups
27
Screen and treatConditionally
screen and treat
Conditionallyscreen and treat
Low prevalence,Low progression risk
LTBI prevalencehigh low
Pro
gres
sion
risk hi
ghlo
w
Don’t forget ATTRIBUTABLE FRACTION to determine PUB LIC HEALTH importance
28CONFIDENTIAL
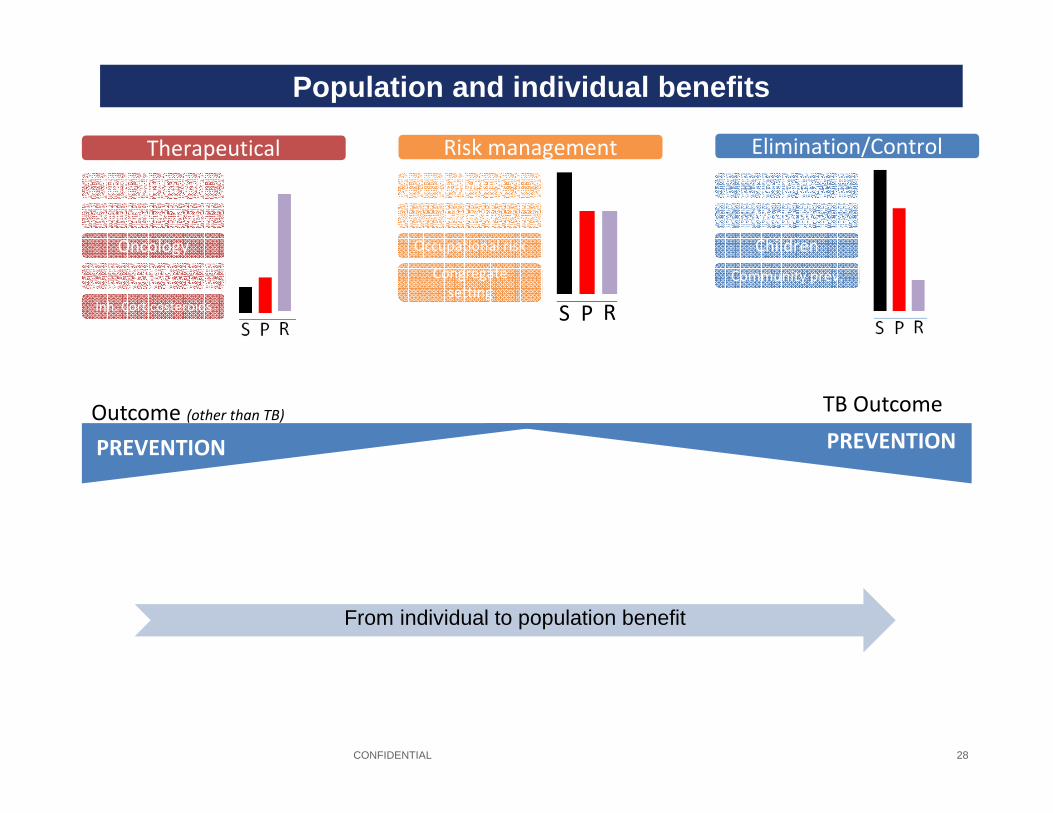
Risk management Elimination/Control
Diabetes
Occupational risk
Elderly
Congregate
setting
Contacts
Children
Migrants
Community prev.
S RP
Therapeutical
TNF-alpha inh
Oncology
Solid Organ Trans.
Inh. Corticosteroids
ESRD
Outcome (other than TB)
PREVENTION PREVENTION
TB Outcome
Public Health Marketing
Population and individual benefits
From individual to population benefit
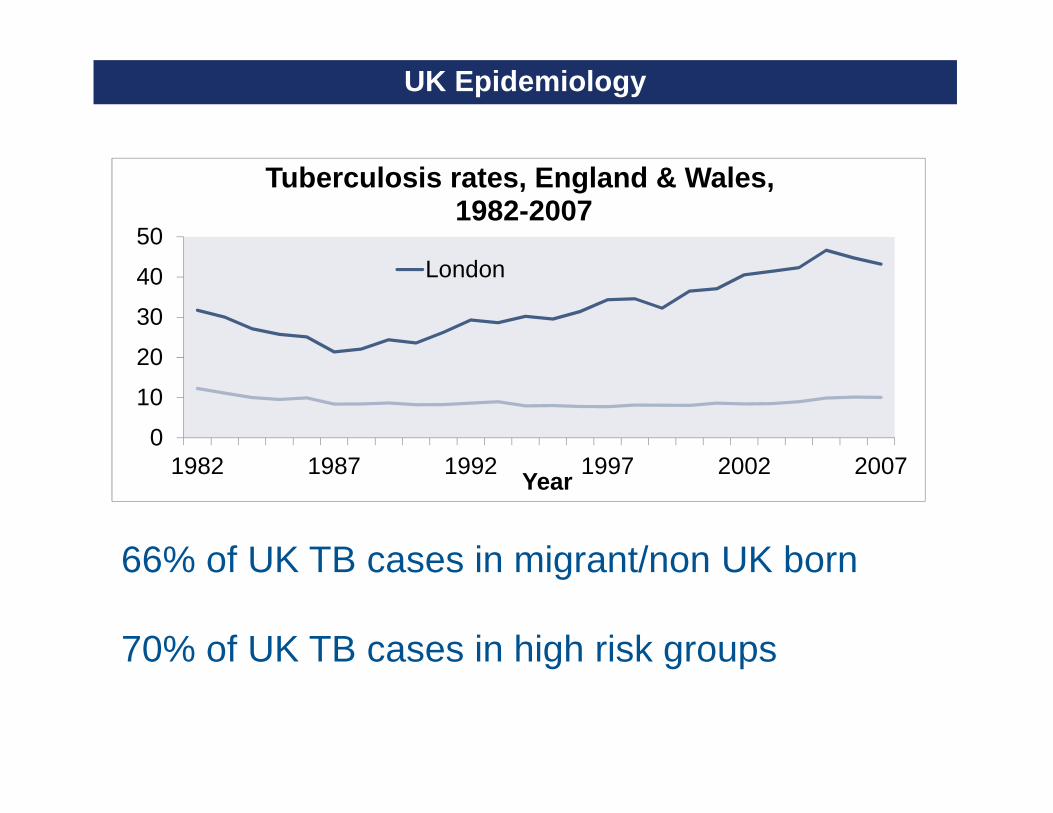
UK Epidemiology
0
10
20
30
40
50
1982 1987 1992 1997 2002 2007Year
Tuberculosis rates, England & Wales,1982-2007
London
Sources: Statutory notifications of infectious diseases (NOIDs) 1982-1998, Enhanced Tuberculosis Surveillance 1999-2007, Office for National Statistics mid-year population estimates, Enhanced Surveillance of Mycobacterial Infections
66% of UK TB cases in migrant/non UK born
70% of UK TB cases in high risk groups
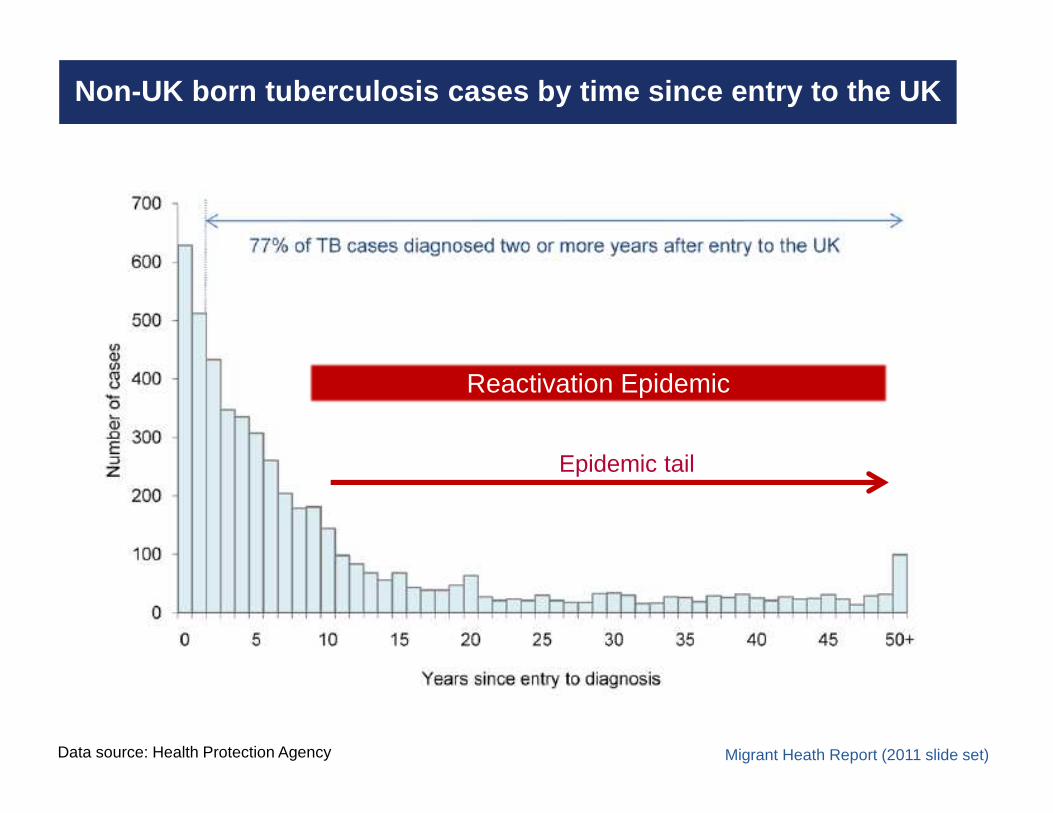
Non-UK born tuberculosis cases by time since entry to the UK
Migrant Heath Report (2011 slide set)Data source: Health Protection Agency
Reactivation Epidemic
Epidemic tail
31
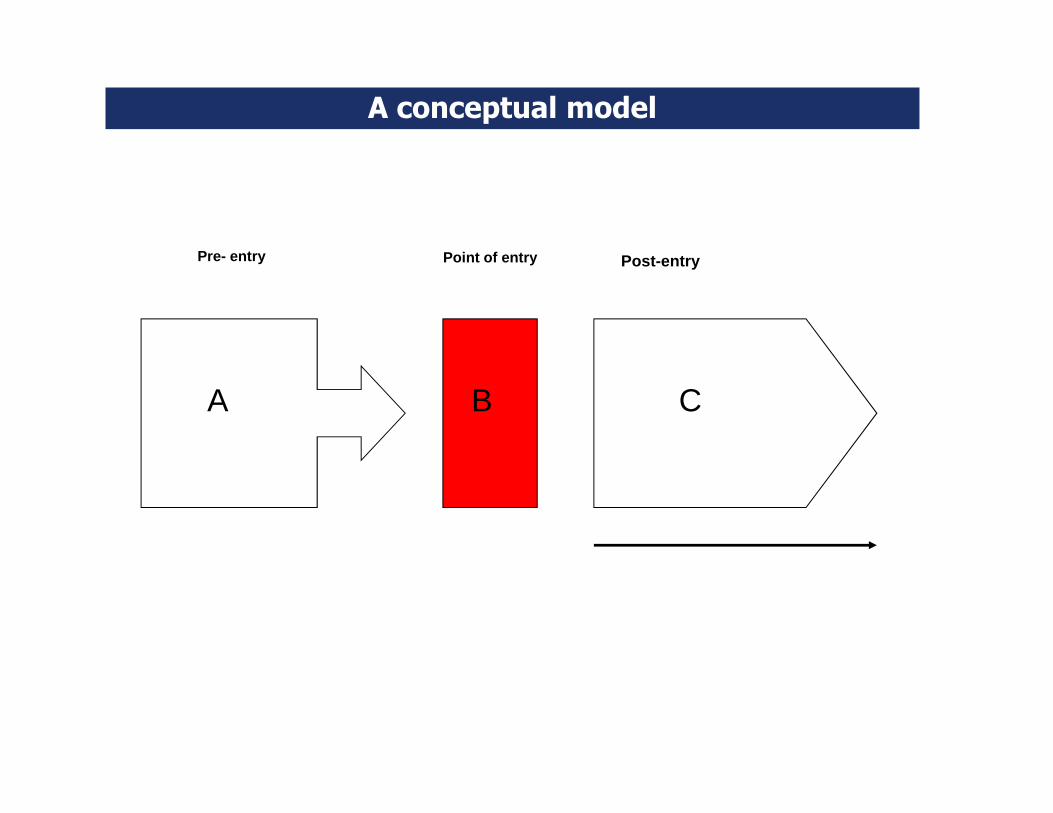
Point of entry
A B C
A conceptual model
Post-entryPre- entry
Forecasting tuberculosis in migrants :
Sake de Vlas
Bram Meima
Gerard Borsboom
Davide Manissero (ECDC)
Department of Public Health, Erasmus MC, Rotterdam
33
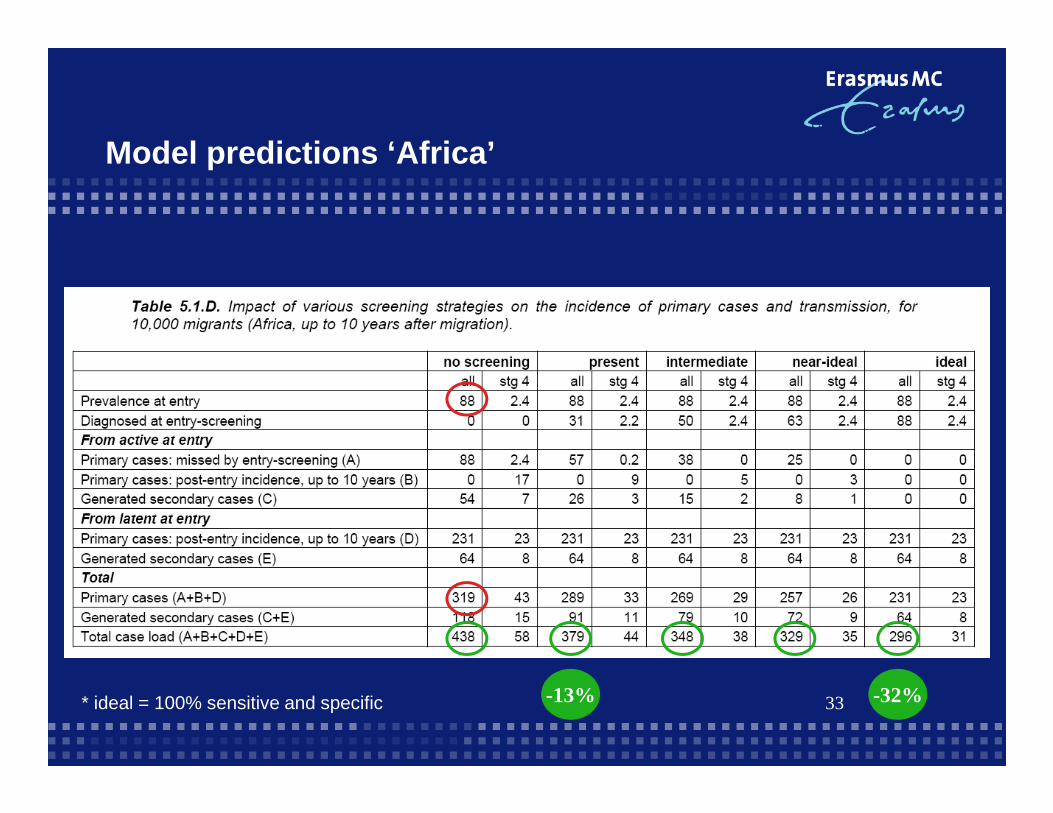
Model predictions ‘Africa’
-13% -32%* ideal = 100% sensitive and specific
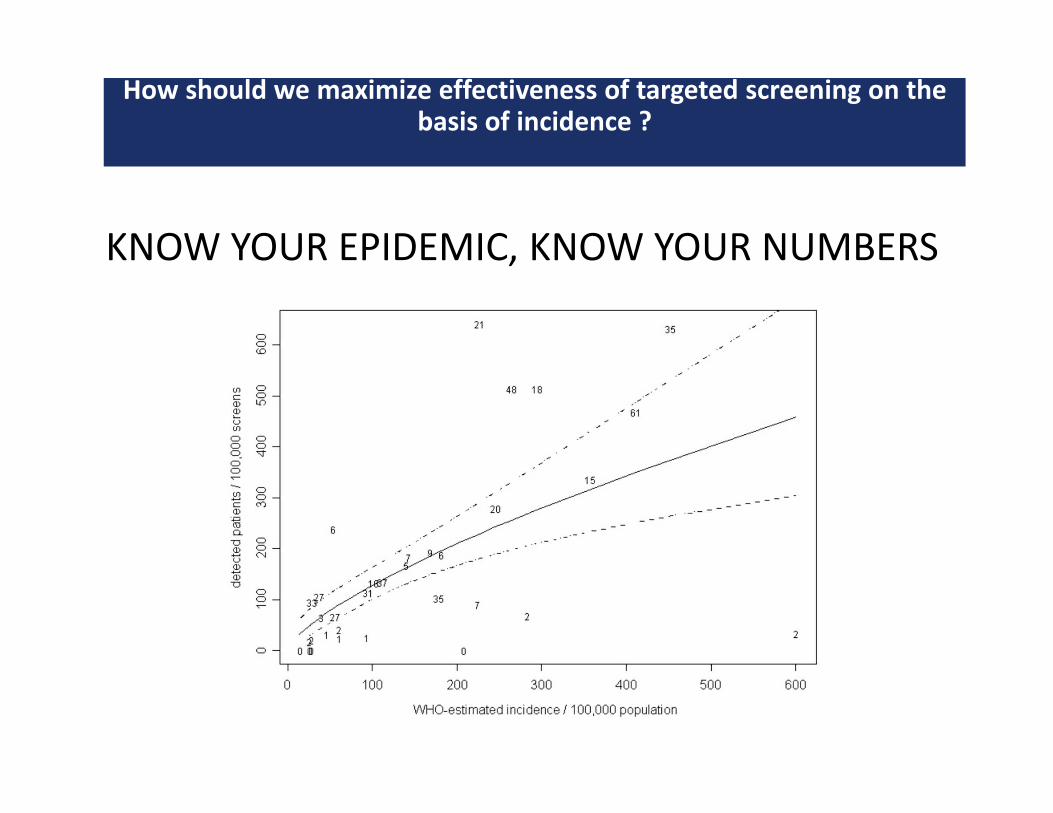
How should we maximize effectiveness of targeted screening on the basis of incidence ?
KNOW YOUR EPIDEMIC, KNOW YOUR NUMBERS
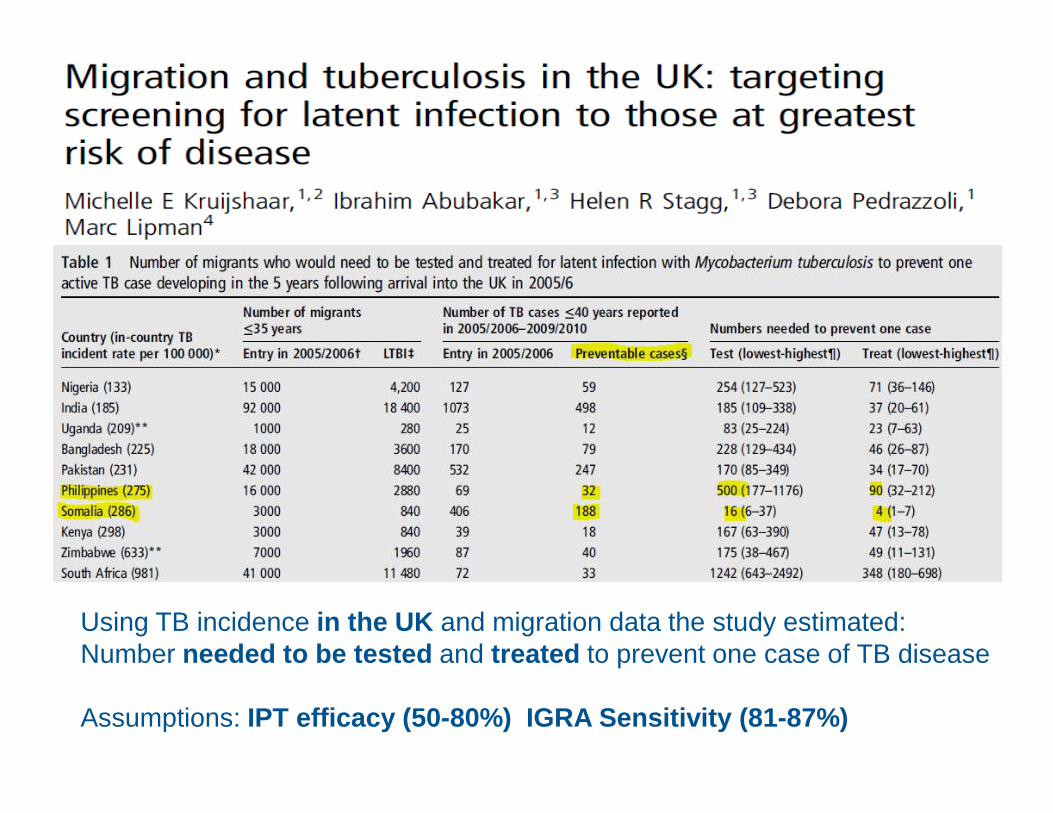
Using TB incidence in the UK and migration data the study estimated:Number needed to be tested and treated to prevent one case of TB disease
Assumptions: IPT efficacy (50-80%) IGRA Sensitivity (81-87%)

36
LTBI Screening Tools
Targeted Testing – Migrant Case Study
TB Prevention – global policy breakthrough
Conclusions
37
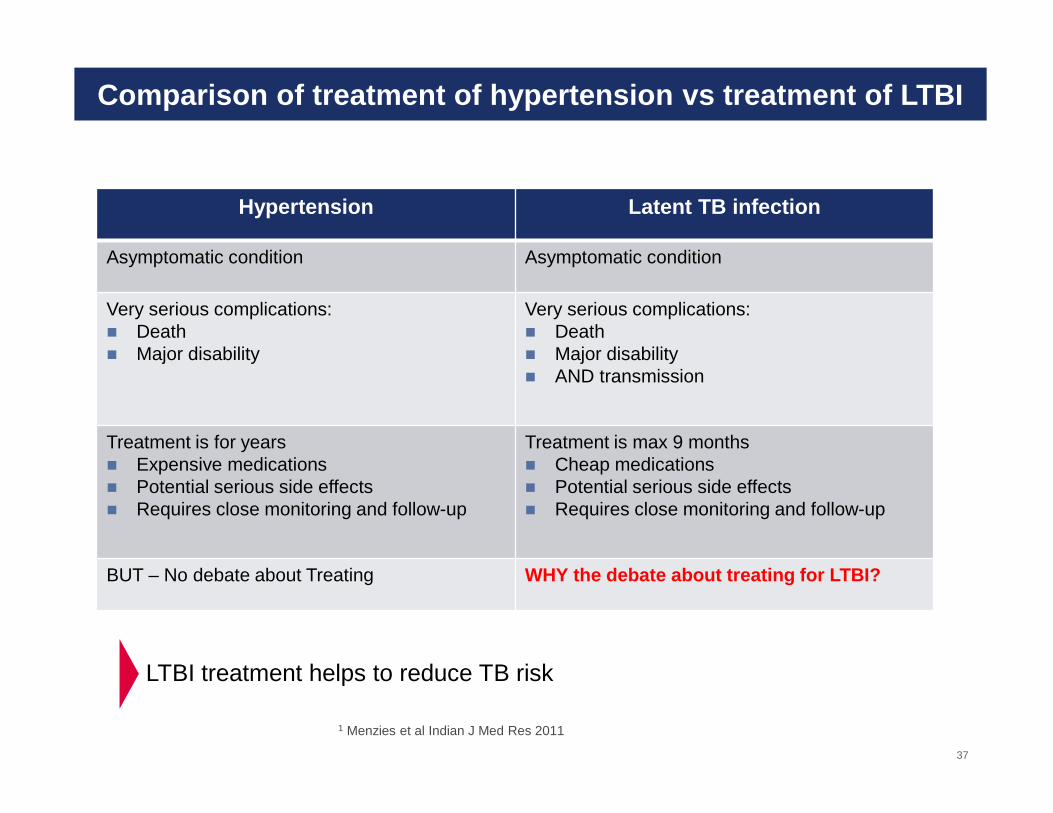
Comparison of treatment of hypertension vs treatmen t of LTBI
Hypertension Latent TB infection
Asymptomatic condition Asymptomatic condition
Very serious complications:� Death � Major disability
Very serious complications:� Death � Major disability� AND transmission
Treatment is for years� Expensive medications� Potential serious side effects� Requires close monitoring and follow-up
Treatment is max 9 months� Cheap medications� Potential serious side effects� Requires close monitoring and follow-up
BUT – No debate about Treating WHY the debate about treating for LTBI?
LTBI treatment helps to reduce TB risk
1 Menzies et al Indian J Med Res 2011
HIV RETHINKING PREVENTIONTB NOT THINKING AT ALL?
The formula of TB Elimination
TB Control= diagnosis + treatment of infectious cases
TB Elimination= TB Control + TB prevention== TB Control + (LTBI diagnosis + LTBI treatment)
Courtesy Prof. GB Migliori





























