Bone consists of : a protein matrix: osteoid a mineral phase,
principally composed of calcium and phosphate: hydroxyapatite
Slide 3
Osteomalacia: Inadequate mineralization of bone osteoid; in
children or adults Rickets: a disease of growing bone, due to
unmineralized matrix at the growth plates.
Slide 4
. VITAMIN D PHYSIOLOGY
Slide 5
Cutaneous synthesis The most important source of vitamin D
Conversion of 7-dehydrochlesterol to vitamin D 3
(3-cholecalciferol) by ultraviolet B radiation from the sun.
Covering the skin with clothing or applying sunscreen, also
decrease vitamin D synthesis. Children who spend less time outside
have reduced vitamin D synthesis.
Slide 6
dietary sources Fish liver oils have a high vitamin D content.
Other good dietary sources include fatty fish and egg yolks.
Vitamin D fortified foods, especially formula Supplemental vitamin
D may be vitamin D 2 (which comes from plants or yeast) or vitamin
D 3 ; they are biologically equivalent. Breast milk has a low
vitamin D content, approximately 1260 IU/L.
Slide 7
Metabolism of Vit.D Vitamin D is transported to the liver and
converts to 25-hydroxyvitamin D (25-D), the most abundant
circulating form of vitamin D. In the kidney, 1-hydroxylase adds a
second hydroxyl group, resulting in 1,25- dihydroxyvitamin D
(1,25-D). The 1-hydroxylase activity is regulated by PTH,
phosphate, and 1,25-D levels.
Slide 8
Action of Vit. D On GI: marked increase in calcium absorption,
which is highly dependent on 1,25-D. phosphorus absorption, most
dietary phosphorus absorption is vitamin Dindependent. On bone,
mediating resorption. Suppresses PTH secretion 1,25-D inhibits its
own synthesis in the kidney.
Slide 9
Etiology of Rickets
Slide 10
Slide 11
Causes of rickets
Slide 12
Clinical Manifestations
Slide 13
Slide 14
Slide 15
The chief complaint in a child with rickets: skeletal
deformities difficulty walking due to a combination of deformity
and weakness. failure to thrive symptomatic hypocalcemia.
Slide 16
Clinical Manifestations Most manifestations of rickets are due
to skeletal changes. Craniotabes, occiput or parietal Craniotabes
may also be secondary to osteogenesis imperfecta, hydrocephalus,
and syphilis. It is a normal finding in many newborns, but
disappears within a few months of birth.
Slide 17
Clinical Manifestations Thickening of growth plate, causing
widening of the wrists and ankles. general softening of the bones
that causes them to bend easily when subject to
Slide 18
Clinical Manifestations Widening of the costochondral junctions
results in a rachitic rosary; along the costochondral
junctions
Slide 19
Slide 20
Growth plate widening causes enlargement at the wrists and
ankles. Harrison groove: The horizontal depression along the lower
anterior chest; occurs due to pulling of the softened ribs by the
diaphragm during inspiration
Slide 21
Slide 22
Clinical Manifestations Softening of the ribs also impairs air
movement and predisposes patients to atelectasis. The risk of
pneumonia is elevated.
Slide 23
Clinical Manifestations There is some variation in the clinical
presentation of rickets based on the etiology. Changes in the lower
extremities tend to be the dominant feature in X-linked
hypophosphatemic rickets. Symptoms secondary to hypocalcemia occur
only in those forms of rickets associated with decreased serum
calcium.
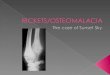
Radiology Rachitic changes are most easily visualized on
posteroanterior radiographs of the wrist: The edge of the
metaphysis loses its sharp border, which is described as fraying.
The edge of the metaphysis changes from a convex or flat surface to
a more concave surface. This is termed cupping.
Slide 35
Slide 36
Slide 37
Laboratory findings Alk.ph is always elevated, except in zinc
def. or protein def. Ph. is always decreased, except in renal
failure. Ca. is always normal or decreased
Slide 38
Slide 39
Diagnosis Diagnosis is based on the presence of classic
radiographic abnormalities, supported by physical examination and
history and laboratory results.
Slide 40
Vit.D Deficient Rickets
Slide 41
. Vit.D deficient Rickets The most common cause of rickets
globally and is prevalent, even in industrialized countries.
Slide 42
Vit.D deficient Rickets Etiology: Most commonly occurs in
infancy due to a combination of poor intake and inadequate
cutaneous synthesis. Transplacental transport of 25-D provides
enough vitamin D for the 1st 2 mo of life unless there is severe
maternal vitamin D deficiency.
Slide 43
Vit.D deficient Rickets Infants who receive formula receive
adequate vitamin D, even without cutaneous synthesis. Breast-fed
infants, because of the low vitamin D content of breast milk, rely
on cutaneous synthesis or vitamin supplements.
Slide 44
Laboratory Findings. Hypocalcemia is a variable finding due to
elevated PTH. Hypophosphatemia is due to increased PTH and
decreased vit.D. Wide variation in 1,25-D levels (low, normal, or
high) Some patients have a metabolic acidosis secondary to
PTH-induced renal bicarbonate-wasting. There may also be
generalized aminoaciduria.
Slide 45
Diagnosis and Differential Diagnosis Based on the combination
of History of poor vitamin D intake and risk factors for decreased
cutaneous synthesis, Radiographic changes consistent with rickets
typical laboratory findings
Slide 46
Treatment 2 strategies for administration of vitamin D. Stoss
therapy, 300,000600,000 IU of vitamin D are administered orally or
intramuscularly as 24 doses over 1 day. Alternative is daily,
high-dose vitamin D, with doses ranging from 2,0005,000 IU/day over
46 wk. Either strategy should be followed by daily vitamin D intake
of 400 IU/day, as a multivitamin. Adequate dietary calcium and
phosphorus; by milk, formula, and other dairy products.
Slide 47
Treatment Symptomatic hypocalcemia need intravenous calcium
acutely, followed by oral calcium supplements, which typically can
be tapered over 26 wk in children who receive adequate dietary
calcium.
Slide 48
Prognosis Excellent response to treatment Radiologic healing
within a few months, first finding is Z-P line. Normalization of
laboratory test results : Ca and Ph after 5 to 7 days, Alk-ph after
a few weeks
Slide 49
Prevention Daily multivitamin containing 200400 IU of vitamin D
to children who are breast-fed. For other children, the diet should
be reviewed to ensure that there is a source of vitamin D.
Slide 50
SECONDARY VITAMIN D DEFICIENCY Etiology: inadequate absorption,
decreased hydroxylation in the liver, and increased degradation in
patients with liver and gastrointestinal diseases
Slide 51
SECONDARY VITAMIN D DEFICIENCY phenobarbital, phenytoin,
isoniazid and rifampin increase degradation of vitamin D by
inducing the P450 system.
Slide 52
VITAMIN DDEPENDENT RICKETS, TYPE 1
Slide 53
VITAMIN DDEPENDENT RICKETS, TYPE 1. Mutations in the gene
encoding renal 1- hydroxylase, preventing conversion of 25-D into
1,25-D. Present during the 1st 2 yr of life
Slide 54
Laboratory Findings. Most lab. Findings are similar to Vit. D
def. rickets: Hypocalcemia is a variable finding due to elevated
PTH. Hypophosphatemia is due to increased PTH and decreased vit.D.
Wide variation in 1,25-D levels (low, normal, or high) Some
patients have a metabolic acidosis secondary to PTH-induced renal
bicarbonate-wasting. There may also be generalized aminoaciduria.
But 1,25 D level is decreased.
Slide 55
VITAMIN DDEPENDENT RICKETS, TYPE 1 Treatment: Long-term
treatment with 1,25-D (calcitriol)
Slide 56
VITAMIN DDEPENDENT RICKETS, TYPE 2
Slide 57
VITAMIN DDEPENDENT RICKETS, TYPE 2. mutations in the gene
encoding the vitamin D receptor, preventing a normal physiologic
response to 1,25-D. Levels of 1,25-D are extremely elevated.
Present during infancy 5070% of children have alopecia.
Slide 58
VITAMIN DDEPENDENT RICKETS, TYPE 2 Treatment Some respond to
extremely high doses of vitamin D 2, 25-D, or 1,25-D, due to a
partially functional vitamin D receptor.
X-LINKED HYPOPHOSPHATEMIC RICKETS Clinical Manifestations:
These patients have rickets, but abnormalities of the lower
extremities and poor growth are the dominant features.
Slide 62
CHRONIC RENAL FAILURE Decreased activity of 1-hydroxylase in
the kidney, leading to diminished production of 1,25- D. unlike the
other causes of vitamin D deficiency, patients have
hyperphosphatemia as a result of decreased renal excretion
Slide 63
Clinical Evaluation Initial evaluation should focus on a
dietary history, emphasizing intake of vitamin D and calcium. ask
about time spent outside, sunscreen use, and clothing.
Slide 64
Clinical Evaluation when a neonate or young infant has rachitic
findings: Consider maternal risk factors for nutritional vitamin D
deficiency, including diet and sun exposure.
Slide 65
Clinical Evaluation Take history of anticonvulsants use
(phenobarbital and phenytoin), and aluminum- containing
antacids.
Slide 66
Clinical Evaluation History of liver or intestinal disease,
although occasionally, rickets may be the presenting
complaint.
Slide 67
Clinical Evaluation A history of renal disease (proteinuria,
hematuria, urinary tract infections.
Slide 68
Clinical Evaluation The family history is critical. Inquire
about leg deformities, difficulties with walking, or unexplained
short stature because some parents may be unaware of their
diagnosis.
Slide 69
Clinical Evaluation Physical examination: Observe the child's
gait, auscultate the lungs to detect atelectasis or pneumonia, and
plot the patient's growth. Alopecia suggests vitamin D dependent
rickets type 2.
Slide 70
Clinical Evaluation The initial laboratory tests in a child
with rickets should include: serum calcium; phosphorus; alkaline
phosphatase; parathyroid hormone (PTH); 25- hydroxyvitamin D;
1,25-dihydroxyvitamin D 3 ; creatinine; and electrolytes.
Urinalysis is useful for detecting the glycosuria and
aminoaciduria.