Embed Size (px)
Citation preview

Dr J C D Wells Pain Research Institute,
Liverpool, UK President Elect, EFIC
Founder and honorary member of NeuPSIG Treasurer, WSPC Councillor, WIP

Pain Relief Foundation
Liverpool

E’un grande onore per affrontare l’incontro piu importante il trattamento del dolore a
Italia quest’anno

Neuropathic Pain : a wide variety of Aetiologies
Shingles
Surgery Radiculopathy Trauma
Syringomyelia

Pain initiated or caused by a primary lesion or dysfunction in the nervous system (IASP, 1994)
Definitions
Pain arising as a direct consequence of a lesion or disease affecting the somatosensory system (Treede et al.,Neurology 2008)
Pain quality, mixed pain, not taken into account

Both types of pain co- exist in
many conditions (mixed pain)
Neuropathic pain
Nociceptive pain
Webster LR. Am J Manag Care 2008;14 (5 Suppl 1):S116–22 Ross E. Expert Opin Pharmacother 2001;2:1529–30

Freynhagen R, Baron R. Curr Pain Headache Rep 2009;13:185–90

Lumbar vertebra
Disc herniation
Activation of peripheral nociceptors –cause of nociceptive pain component1
Compression and inflammation of nerve root – cause of neuropathic pain component2
1. Brisby H. J Bone Joint Surg Am 2006;88 (Suppl 2):68–71 2. Freynhagen R, Baron R. Curr Pain Headache Rep 2009;13:185–90

Lesion
Activation of local
nociceptors1
Constant ache, throbbing pain in the low back2
Patient presents with both types
of pain
Shooting, burning pain in the foot2,3
Ectopic discharges from nerve root lesion2
1. Brisby H. J Bone Joint Surg Am 2006;88 (Suppl 2):68–71 2. McMahon SB and Koltzenburg M. Wall and Melzack’s Textbook of Pain. 5th ed. London: Elsevier; 2006; pg 1032 3. Freynhagen R, Baron R. Curr Pain Headache Rep 2009;13:185–90

¨ “Pain can be more or less neuropathic” Rasmussen et al, 2004; Attal and Bouhassira, 2004; Bennett et al 2006
¡ Gradient of neuropathic characteristics with increasing diagnostic certainty (MPQ, NPS, DN4, S-LANSS)
¨ So neuropathic pain can be seen as a spectrum, not a dichotomy
¨ Which point on the spectrum do we use for epidemiological case definition?

¨ Common features among all causes ¡ Mechanisms, symptoms, signs ¡ HRQoL impact more dependent on intensity than cause Doth et al 2010
¨ Common response to some treatments ¡ Sindrup and Jensen, 1999; Hansson and Dickenson, 2005
¨ Not always possible to distinguish diagnosis ¡ Especially in primary care, also in epidemiology (eg ca, local)
¨ Specific treatments available for NeuP? ¡ Therefore important to try identify and target unclassified and
mixed cases, as well as classical syndromes ¡ Daniel et al (2008) – different treatment needs for NeuP than for
CLBP

¨ Obvious aetiological differences ¡ Eg, PDN, PHN, Postsurgical pain, central pain, HIV neuropathy
¨ With implications for prevention ¡ Eg treating hyperglycaemia, HZV immunisation, HIV prevention
¨ Emerging evidence of clinical differences ¡ Fields et al 1998: two distinct PHN subtypes ¡ Baron et al 2009: five distinct NeuP subtypes, frequencies vary in PHN and LBP ¡ Grémau-Richard et al 2010: different response to treatment in 2 BMS subtypes ¡ ?implications for treatment generally
¨ Most RCTs are condition-specific ¡ Evidence limited of application to different conditions ¡ Some evidence of condition-specific effects, eg HIV ú Amitriptyline and gabapentin ineffective (Kieburtz et al 1998; Hahn et al 2004; Shay et al 1998) ú Cannabis effective (Abrams et al 2007; Ellis et al 2008)

¨ Condition-specific estimates ¨ Prevalence of neuropathic pain ~1% Bowsher 1990
¨ Prevalence of neuropathic pain ~2% Bennett 1997
¨ “Thought to be more common than has been
generally appreciated…” Dworkin 2002

¨ S-LANSS Torrance et al 2006; Smith et al 2007
¡ “Pain of predominantly neuropathic origin” ¡ 8.2% (UK)
¨ DN4 Bouhassira et al 2008
¡ “Pain with neuropathic characteristics” ¡ 6.9% (France)
¨ Validated in pain clinic populations ¨ Validity and PPV unknown in general population
Therefore, this is not the prevalence of neuropathic pain Prevalence of “possible neuropathic pain? Treede et al 2008

¨ PHN ¡ Prevalence 2.6% to 10% of those who have had HZ ¡ Higher in older age-groups
¨ PDN ¡ Prevalence 8% to 20% of those with Type 2 diabetes
¨ Back pain neuropathy ¡ Prevalence 37% of those with CLBP (painDETECT) ¡ Population prevalence 0.75% to 14.5% !

¨ Poor health-related quality of life Schmader et al 2002; Smith et al 2007; Jensen et al 2007; Doth et al 2010
¨ HRQoL most dependent on pain intensity Doth et al 2010
¨ HRQoL scores equivalent to those found in ¡ Clinical depression ¡ Coronary artery disease ¡ Recent MI ¡ Poorly controlled diabetes
¨ Increasing impact on society ¡ Ageing population ¡ Increasing prevalence of DM ¡ Global burden of HIV (33.2 million have HIV; 35% have painful
neuropathy)

Patients with ‘moderate’ to ‘very severe’ discomfort (n=126)
40 20 70 60 0 50 30 10 Patients (%)
Difficulty sleeping
Lack of energy
Drowsiness
Difficulty concentrating
Depression
Anxiety
Poor appetite
Type
of f
unct
iona
l im
pairm
ent
Adapted from Meyer-Rosberg et al. Eur J Pain 2001;5:379–89 06-00306 Date of preparation March 2010
Pain In Practice - A medical education meeting initiated and funded by Pfizer

Available epidemiological evidence confirms that: ¨ Neuropathic pain is common ¨ Neuropathic pain is important, cost + QOL ¡ To individuals ¡ To society
¨ There is potential to target identification and treatment strategies
¨ There are opportunities for prevention ¨ More research is needed


Holistic Psychological Pharmacological Interventional (NeuPSIG guidelines for H+I)

0
10
20
30
40
50
60
70
80
ParacetamolNSAIDsAntidepressantsOpioidsAEDsAspirin
NSAIDs, non-steroidal anti-inflammatory drugs; AEDs, anti-epileptic drugs Adapted from Hans G et al. BMC Public Health 2007;7:170
Patie
nts
pres
crib
ed tr
eatm
ents
fo
r neu
ropa
thic
pai
n (%
)
Graph adapted from an observational study looking at neuropathic pain in daily practice in Belgium
*
*
* * Some Antidepressants, AEDS & Opioids have demonstrated efficacy.

PNS
C fibre
Ab fibre
Lesion
Phenotypic changes
Ectopic discharges
Ectopic discharges
Phenotypic changes Gene dysregulation
glutamate peptides
SP?
Alteration of inhibitory controls
Hyperexci- tability of nociceptive neurons
Neuropathic pain
Reduction of segmental inhibition GABA, KCC2, glycine
Microglial activation
CNS
In: Bouhassira and Attal, douleurs neuropathiques, 2007

PNS CNS
Gene regulation
Current therapeutic targets
Desensitization
Excitability
Central sensitization
Inhibition of the transmission
Segmental inhibition
Descending controls
Microglial activation
Alpha2delta agonists (gabapentin, pregabalin)
Antidepressants Alpha2delta agonists Opioids/tramadol
Tricyclic antidepressants Sodium channel blockers - Lidocaine - Antiepileptics
Opioids
Alpha2delta agonists (gabapentin, pregabalin)

Meta-analysis of neuropathic pain treatments
Finnerup et al. Pain 2005 NNT 50% pain relief
0 2 4 6 8 10 12
Topiramate SSRI
Capsaicin NMDA antagonists
Mexiletine
SRNI
Gabapentin / Pregabalin Tramadol
Opioids
Carbamazepine / Lamotrigine
Valproate
TCAs 397
389
120
420
1057
81
466
150
214
149
109
83
Peripheral NP
Adapted from C. Wells and G. Mick (with permission)

Finnerup et al 2005 Pain Current update
Attal et al 2006, 2010 Eur J Neurol
Gilron et al 2006 CMAJ
Dworkin et al 2007 Pain Summary of recommendations Mayo Clin Proc 2010
Treatment algorithm based on meta-analysis
EFNS guidelines (aetiology-based)
Practical guide Consensus based NeuPsig recommendations
131 refs 147 refs 138 refs 132 refs

Algorithm for peripheral neuropathic pain treatment: an evidence based proposal
Lidocaine plaster*
TCA (SNRI)
Gabapentin/ Pregabalin
Gabapentin/ Pregabalin
Postherpetic neuralgia and focal neuropathy
Peripheral neuropathic pain
yes
TCA (SNRI)
yes
Tramadol, Oxycodone
TCA contraindication
no yes TCA contra-indication
no
no
Finnerup et al. Pain 118 (2005) 289–305

Aetiology Recommendations for first line
Recommendations for Second / third line
Diabetic NP PHN Central NP
Duloxetine 60-120 mg/d Gabapentin 1200-3600 mg/d Pregabalin 300-600 mg/d TCA 25-150 mg/d Venlafaxine ER 150-225 mg/d Gabapentin Pregabalin TCA Lidocaine plasters 1 to 3/day Gabapentin Pregabalin TCA
Opioids (individual titration) Tramadol 200-400 mg/d Capsaicin cream 4 appl./day Opioids Lamotrigine 200-400 mg/day Opioids Tramadol (SCI)
Attal et al. Eur J Neurol 2010

EFNS guidelines
PHN with allodynia*
Lidocaine patches
Peripheral neuropathic pain
GBP/pregabalin TCA/SNRI**
Attal, et al EFNS guidelines Eur. J Neurol, 2010
No effect Side effects
Opioids Tramadol
NeuPsig recommendations
Dworkin et al Pain 2007
- Antidepressants (TCA/SNRI) - Gabapentin or pregabalin - Topical lidocaine (localized pain) - Opioids or tramadol (acute NP, cancer NP or episodic exacerbations of severe pain and when prompt pain relief is required)
* Particularly in the elderly ** first line in painful polyneuropathies

Moore et al. Cochrane database of Systematic Reviews 2009
Fibromyalgia
PDN
Central NP
PHN
1 2 4 6 8 10 12 14 16 18NNT (95% CI): at least 30% pain improvement at 12 weeks
Pregabalin in neuropathic pain
Pregabalin 600 mg daily moderate benefit or better at study end

Sultan et al. BMC Neurology 2008;8:29 Moore et al. Cochrane database of Systematic Reviews 2009
Moore et al, unpublished
Pregabalin 450/600 mg
Duloxetine 60/120 mg
Tramadol/acetaminophen 300/2600 mg
Amitriptyline 25/50 mg
1 2 4 6 8 10 12 14 16NNT for at least moderate benefit at 12 weeks (95% CI)
Fibromyalgia pain moderate benefit or better at study end

CLBP
Osteoarthritis
Fibromyalgia
PDN
1 2 4 6 8 10 12 14 16 18NNT (95% CI): at least 30% pain improvement at 12 weeks
Duloxetine in chronic pain
Duloxetine 60/120 mg daily
Various sources
moderate benefit or better at study end

Antidepressant Outcome Trials Patients Placebo Active NNT (95% CI)
Duloxetine 60/120 mg at least 50% pain relief 3 1024 27 47 5.1 (3.9 to 7.3)
Amitriptyline all doses global improvement 10 588 32 64 3.2 (2.6 to 4.2)
Other antidepressants global improvement 3 216 12 50 2.6 (2.0 to 3.7)
Venlafaxine all doses global improvement 3 200 25 57 3.1 (2.2 to 5.1)
Desipramine all doses global improvement 2 78 10 59 2.1 (1.5 to 3.3)
Imipramine all doses global improvement 2 58 5 97 1.1 (1.0 to 1.2)
Number of Percent with
Sultan et al. BMC Neurology 2008 8:29.

Sultan et al. BMC Neurology 2008;8:29 Moore et al. Cochrane database of Systematic Reviews 2009
Pregabalin 600 mg
Pregabalin 300 mg
Duloxetine 60/120 mg
Pregabalin 600 mg
Pregabalin 300 mg
Duloxetine 60/120 mg
1 2 4 6 8 10 12 14 16 18NNT (95% CI): pain improvement at 12 weeks
Moderate benefit
Substantial benefit
Painful diabetic neuropathy IMMPACT outcomes or better at study end

¨ CNP arises from damage to ascending spino-thalamo-cortical pathways, their relays, or end-stations in the spinal cord or brain.
¨ Usually a pain in an area of altered sensation
“pain arising as a direct consequence of a lesion or
disease affecting the somatosensory system” Treede et al, 2007

Same general principles as all NPP Worse results! Little clinical trial work ? small numbers ? –ve outcomes ? lack of interest
PNPP 76/101 +ve trials 68.5% CNPP 4/9 +ve trials 44.4%

in small trials only:-
TCA’s (Amit) ( Rintala) Gabapentin ( To, Siddall ) Pregabalin (Vranken, Siddall) Carbamazepine (Leijon, CPSP) Opioids (iv) (Attal) Lamotrigine (Vestergaard, Finnerup) Topiramate (Harden) Tramadol ( CNP) Cannabinoids ( Rog, Svendson,in MS) IV lignocaine (then carbamazepine?) Ketamine ( Eide, iv only)

Amitriptylene ( Cardenas ) Opioids Mexiletine Ketamine Lozenges Baclofen Valproate Trazodone

Agents Outcome
Amitriptyline vs acupuncture Negative Amitriptyline vs mexiletine Negative
Lidocaine gel Negative Lidocaine patch Insufficient data
Lamotrigine Pain improved/-ve Gabapentin Pain improved/-ve Pregabalin Negative
Capsaicin patch (high conc.) Pain improved Cannabis (smoked) Pain improved
Duloxetine/Methadone +ve and -ve

Agents Outcome
Peptide T No effect Prosaptide No effect
Nerve growth factor Pain improved; No regeneration
L-Acetyl carnitine No effect Erythropoetin Failed accrual


NNH 0 5 10 15 20
Antidepressants, SSRI
Valproate Mexiletine
Carbamazepine/lamotrigine/ phenytoin
Gabapentin/pregabalin Opioids
Antidepressants, SNRI Tricyclic antidepressants
NMDA antagonists Capsaicin Tramadol
Topiramate
ns
Finnerup et al. Pain 118 (2005) 289–305
Lidocaine plaster

N=196 Duration
16 17
24
43
0
5
10
15
20
25
30
35
40
45
50
3 to 6 7 to 12 13 to 35 36+ Months
% P
atie
nts
moderate
severe mild
unclear
27%
46%
27%
>70
Neuropathic Pain – Unmet Needs
Pain intensity despite medication


¨ Perform rationale combination therapy
¨ Take into account psychological comorbidities
¨ Develop new compounds with lower side effect profile or acting on new targets
¨ Identify responder profiles to drug treatments based on a detailed phenotypic assessment

· G/PG upregulates spinal cord κ and m receptors1
· Oxycodone acts at κ receptors that increases anti-nociception via m receptors2
· Anecdotal evidence suggests oxycodone and G/PG may have an additive effect
· G/PG and oxycodone are already used in combination in clinical practice
· Benefit with less side effects
1.Shimoyama M et al. Pain 1997; 72: 375–82 2.Khotib J et al. Neuropharmacology 2004; 46: 531–40

Combination therapy • Gabapentin + morphine > gabapentin or morphine monotherapy
in diabetic NP and PHN (level A) – Gilron et al. NEJM 2005
• Gabapentin + nortriptyline > gabapentin or nortriptyline monotherapy in diabetic NP and PHN (level A)
– Gilron et al. Lancet 2009
• Gabapentin + venlafaxine > gabapentin monotherapy in diabetic NP (level B)
– Simpson et al. J Clin Neuromusc disease 2001
• Negative trial in radiculopathy with morphine + nortriptyline combination (level B)
– Khoromi et al. Pain 2007

0
1
2
3
4
5
6
7
Bas
elin
e
Plac
ebo
GB
T
Mor
phin
e
GB
T/m
orph
ine
Pain
inte
nsity
sco
re
Gilron I et al. NEJM 2005; 352: 1324–34

Psychological comorbidities
•Psychological comorbidities frequent in chronic NP (Turk et al Mayo Clin Proc 2010; 85: S42-50)
•Importance of pain coping strategies and catastrophizing in pain chronicity
(Haythorthwaite et al Pain 2003; 106: 453-460; Sullivan et al Pain 2009; 143: 123-129)
•Role of catastrophizing in therapeutic outcome in NP ?

PNS CNS Gene regulation Neurotrophins Anti-NGF
Develop new compounds
Excitability Nav channel blocker Ralfinamide Potassium openers Retigabine
Central sensitization AMPA antagonists Terampanel mGlutamate inhibitors Calcium channel blockers Ziconotide (Prialt) (IT) Novel alpha2delta agonists
Inhibition of transmission Cannabinoid receptor agonists Sativex
Segmental inhibition GABA agonists
Modulatory controls New opioid and NE reuptake inhibitors Tapentadol Cannabinoid receptor agonists Sativex Nicotinic agonists
Microglial activation Cytokine inhibitors MAPK inhibitors
Desensitization Neurogenic inflammation Botulinum toxin A TRTPV1 agonists Capsaicin patches

Botulinum toxin inhibits Ach release at the neuromuscular junction
Synaptic junction
Ach vesicle Exocytosis
Muscular fiber
Slide: D. Ranoux

l Analgesic effects in dystonia (Tsui 1986, Brin 1987)
– Early analgesic effect before the antidystonic effect – More important than would be expected from the effect on
hypertonia l Effects on chronic migraine (Picket Biodrugs 2010)
l Several anecdotical reports of effects on neuropathic pain or trigeminal neuralgia
(eg, Yoon et al Pain Med 2010) l Sustained antiallodynic effects on animal models of
neuropathy (Bach-Rojecky et al E J Pharmacol 2010; Luvisetto et al Neuroscience 2007; Favre-
Guimard et al E J Pharmacol 2009 )

Botulinum toxin A and neuropathic pain Rationale
Purkiss et al Biochem Pharmacol 2000 Durham et al Headache 2004
Botulinum toxin A blocks vanilloid receptor activity
Botulinum toxin A reduces Substance P, CGRP release from DRG neurons or nociceptors
Morenilla-Palao J Biol Chem 2004
Botulinum toxin A may reduce capsaicin-evoked pain in human skin
Tugnoli et al Pain 2008 Gazerani et al Pain 2006, 2009 See however Voller et al Neurology 2003 and Schulte-Malter et al J Neurol Sci 2007
BTXA
saline
Effects on neurogenic inflammation

¨ Peptide mediated transdermal delivery (Carmichael et al Pain 2010) • Recombinant chimera of BoNT/A and BoNT/E (Meng et al J Neuroscience 2009) • Re-engineering of Botulinum toxins that target nociceptive
neurons - modified clostridial endopeptidase - Drug delivery using a clostridial neurotoxin-based vehicle (Picket, Biodrugs 2010)

PNS CNS Gene regulation Neurotrophins: GDNF Anti-NGF
Develop new compounds
Desensitization Neurogenic inflammation Botulinum toxin A TRTPV1 agonists Capsaicin patches
Excitability Nav channel blocker Ralfinamide Potassium openers Retigabine
Central sensitization AMPA antagonists Terampanel mGlutamate inhibitors Calcium channel blockers Ziconotide (Prialt) (IT) Novel alpha2delta agonists
Inhibition of transmission Cannabinoid receptor agonists Sativex
Segmental inhibition GABA agonists
Modulatory controls New opioid and NE reuptake inhibitors Tapentadol Cannabinoid receptor agonists Sativex Nicotinic agonists
Microglial activation Cytokine inhibitors MAPK inhibitors

Lidocaine Patch 5%
C
Capsaicin 8%

•Active ingredient in chili peppers
•Known receptor: VR1
•Respond to heat stimuli
•Pain
•Acidic environment
•Available in a topical cream (max conc 0.075% )
•Exptal hi-conc patch
• (8%, Qutenza®)

Kennedy WR, et al. J Pain 2010 Apr 16 [Epub ahead of print]
DN=dermal fibre; DEJ=dermal-epidermal junction; ENF=epidermal nerve fibre
Week 1 Qutenza Week 1 Control

Capsaicin: Application Procedure
Courtesy of R. Baron


Who are the best responders to capsaicin ?
ÿ No specific assessment of NP symptoms (eg, burning, pain paroxysms, deep pain, evoked pain) ÿ Best potential responders would be patients with mechanical/thermal allodynia and weak thermal deficits (ie, clusters 1 and 4 from Baron et al Pain 2009)

Mean (SE) % Change from Baseline Diary Score for Average Pain in Past 24 Hours
Pooled data from the 30-, 60-, and 90-minute application times are shown.
% C
hang
e fr
om B
asel
ine
-30
-20
-10
0
0 1 2 3 4 5 6 7 8 9 10 11 12 Post-Treatment Week
* † ‡ ‡ † † † † † † P=0.006
* P<0.05, †P≤0.01, ‡P≤0.001 Control NGX-4010
Simpson D, et al. Neurology 2008; 2008;70:2305-2313

% Patients with ³30% Pain Decrease from Baseline to Weeks 2-12
Pooled data from the 30-, 60-, and 90-minute application times are shown.
% P
atie
nts
Control NGX-4010
10
20
30
40
50
18% 34%
P=0.009
18% n=82
34% n=225

Finnerup et al. Pain 2005
Capsaicin and neuropathic pain
NNT 50% pain relief 0 2 4 6 8 10 12
Topiramate SSRI
Capsaicin NMDA antagonists
Mexiletine SRNI
Gabapentin / Pregabalin Tramadol
Opioids Carbamazepine / Lamotrigine
Valproate TCAs 397
389
120
420
1057
81
466
150
214
149
109
83
NNT 7


Rog et al (2005) +ve results for Sativex Spray Svendson et al, Dronabinol in MS Improvement in sleep Reduction in pain Well tolerated
Recent +ve trial for spasticity in MS (doubled share price for GW Pharma)

¨ Smoked cannabis (3.96% Δ9-THC) vs placebo cigs; 3x/d x 5d
¨ N = 50; parallel gp ¨ Pain ¯: Can: 34%, plac:
17% (p = .03) ¨ ≥ 30% pain ¯: Can:
52%, plac: 17% (p= .04) ¨ AE with can: anxiety,
sedation, dizziness, confusion
Abrams et al. Neurol 2007;68:515-521

Campbell F et al., Are Cannabinoids an effective and safe Treatment Option in the Management of Pain? A qualitative, systematic Review.
BMJ 2001; 323:13–16
¨ Systematic review of cannabinoid derivatives tested in cancer, chronic non-malignant and post-operative pain
¨ Cannabinoids no more effective than codeine in controlling pain
¨ Adverse effects [eg CNS depression,] limit their use
Concluded: “ Their (cannabinoids) widespread introduction into clinical practice for pain management is therefore undesirable”

¨ Good in theory ¨ Variable in practice (conflicting views) ¨ No evidence of Ketamine benefit in trial work ¨ Memantine, Amantadine, no +ve work yet. ¨ Opioids with NMDA antagonism?
(methadone, dextromethorphan)
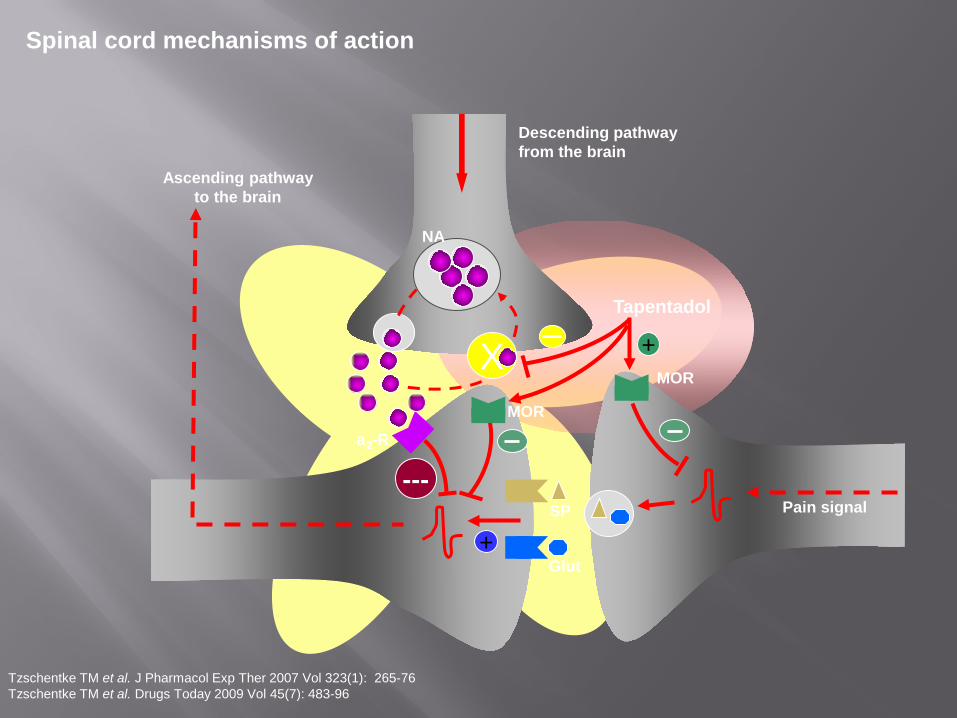
X
a2-R
NA
Descending pathway from the brain
+ SP
Glut
Ascending pathway to the brain
Pain signal ---
+ MOR
Tapentadol
MOR
Spinal cord mechanisms of action
Tzschentke TM et al. J Pharmacol Exp Ther 2007 Vol 323(1): 265-76 Tzschentke TM et al. Drugs Today 2009 Vol 45(7): 483-96

05
10152025303540
Nause
a
Vomitin
g
Const
ipatio
n
Dizzine
ss
Somno
lence
Prurit
us
%
Placebo n=1498
Tapentadol SR n= 3613
Oxycodone CR n= 1472
Data on file
TEAE in ≥ 5% patients Numerical differences only

Algorithm for peripheral neuropathic pain treatment: an evidence based proposal
Lidocaine plaster Capsaicin patch*
TCA (SNRI)
Gabapentin/ Pregabalin
Gabapentin/ Pregabalin
Postherpetic neuralgia and focal neuropathy, allodynia
Peripheral neuropathic pain
yes
TCA (SNRI)
yes
Tramadol, Tapentadol, Oxycodone
TCA contraindication
no yes TCA contra-indication
no
no


¨ Prevention of stroke ¨ better acute management of stroke ¨ SCI , reduction of trauma ¨ SCI, better initial treatment ¨ Acute shingles, reduction, treatment ¨ Diabetic PN, better control of glucose levels ¨ Better Rx of HIV, AIDS

CPSP prevention of strokes lipid reduction, statins blood thinners, aspirin, clopidogrel promotion of active lifestyle reduction of obesity Acute Stroke Management thrombolytics, etc Prophylactic early treatment Brain Derived Neurotrophic Factor TCA’s, Anticonvulsants

In general, promote a fitter, healthier, lifestyle Prevention and treatment of Obesity (CPSP,
Diabetes) Encouragement of Fitness Healthy Habits, ( smoking, veg + fruit) Genetic Manipulation Gene Therapy

¨ More common than previously appreciated ¨ Careful assessment required ¨ Clear treatment algorythyms ¨ Multidisciplinary approach required ¨ Still major deficiencies in success ¨ Need for better treatments with less side effects ¨ Need for better health measures in future


A critical look at new and existing treatments for pain: Back Pain, Neuropathic Pain and Cancer Pain Kenes, WSPC