Embed Size (px)
Citation preview

Dr. Jack Dolbin Session 5 1
Role of the Lumbar Spine: The most important region as it relates
to performance, treatment and prevention of soft tissue injuries.
The relation of the spine to somatoautonomic and
somatosomatic components have recently been “discovered” by the
medical profession

Dr. Jack Dolbin Session 5 2
Key to performance:
As it relates to the shoulderVillanova swimmers 75%As it relates to Lower Extremity injuriesAs it relates to injuries of the upper
extremityAs it relates to performance2nd most common injury in sports

Dr. Jack Dolbin Session 5 3

Running Kinesiology
Dr. Jack Dolbin Session 5 4

Dr. Jack Dolbin Session 5 5
Low Back Injuries:
Sprain! StrainPars FracturesSoft Tissue injuriesDisc injuries

Dr. Jack Dolbin Session 5 6
Golf Swing Sequence

Dr. Jack Dolbin Session 5 7
Lumbar Sprain
Flexion: Tearing capsular ligaments, Supraspinous Ligament, possible disc injury.
Extension: Compression facet Joint. Possible Pars fracture.
Dr. Jack Dolbin Session 5 8

Examination
Observation Inspection: APalpation: TRange of Motion: RProvocative TestsNeurology Imaging
Dr. Jack Dolbin Session 5 9

Diagnostic Tests
KempsAdamsSitting BechterewSLRBraggardsSotoHallGolthwaits
Dr. Jack Dolbin Session 5 10

Diagnostic Tests
Stork TestGaenslensObersThomasYeomansNachlasElys
Dr. Jack Dolbin Session 5 11

Neurology
Lower extremity neurologyDTR’sManual Muscle testsPin WheelVascular: Dorsal pedis/TibialPathological Reflexes
Dr. Jack Dolbin Session 5 12

Treatment
If within 24-48 hours deal with the acute tissue response
A. Ice, lazer,HVG, Kinesiotaping. CyriaxAfter 48 hours: Cyriax Cross Fiber,
Muscle energy, Impulse Adjusting. Modalities to promote circulation,
midrange exercise..Adjustments to fixated joints.
Dr. Jack Dolbin Session 5 13
Pars Injuries
Active Spondylo: Inactive Spondylo:Pending Spondylo:
Chapter 5: Dr Terry Yochum Illustration: Steven Soffer MD. FICS
Dr. Jack Dolbin Session 5 14

Epidemiology
Gymnasts: Female AdolescentLong Jumpers, Triple Jumpers.Weight LiftersFemale volleyball, basketball
Athletes that do repetitive hyperextension activities.
Dr. Jack Dolbin Session 5 15

History of repetitive hyperextension activities or extreme vertical stress.
Positive Stork
Positive Kemps.
Dr. Jack Dolbin Session 5 16

Holding our Breath
Dr. Jack Dolbin Session 5 17

Cruising
Dr. Jack Dolbin Session 5 18

Pars Fracture MRI
Dr. Jack Dolbin Session 5 19

Radiological Evidence of pars Defect
Perform spec bone scan or stir MRI
If positive: Boston overlap brace: min 2 mo.
No: make alternate diagnosis
Treat conservatively as per below
Play no play decision??
Does the athlete perform rep hyperextension activities
Perform spec or stir MRI
If no the make alternative diag:
60% have SI Sub. SP/ST Iliolumbar ligament
30% have facet syndrome
Dr. Jack Dolbin Session 5 20

Spondylolysis
There has never been a baby born with a pars defect.
Stress fracture:
Dr. Jack Dolbin Session 5 21

Pars defect Axial View
Dr. Jack Dolbin Session 5 22
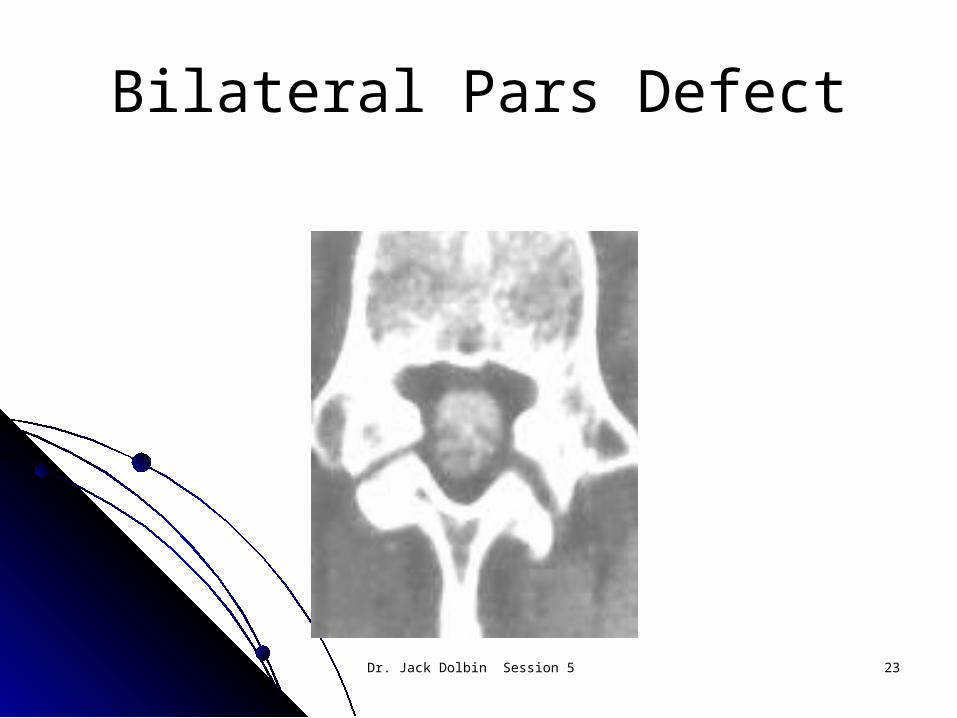
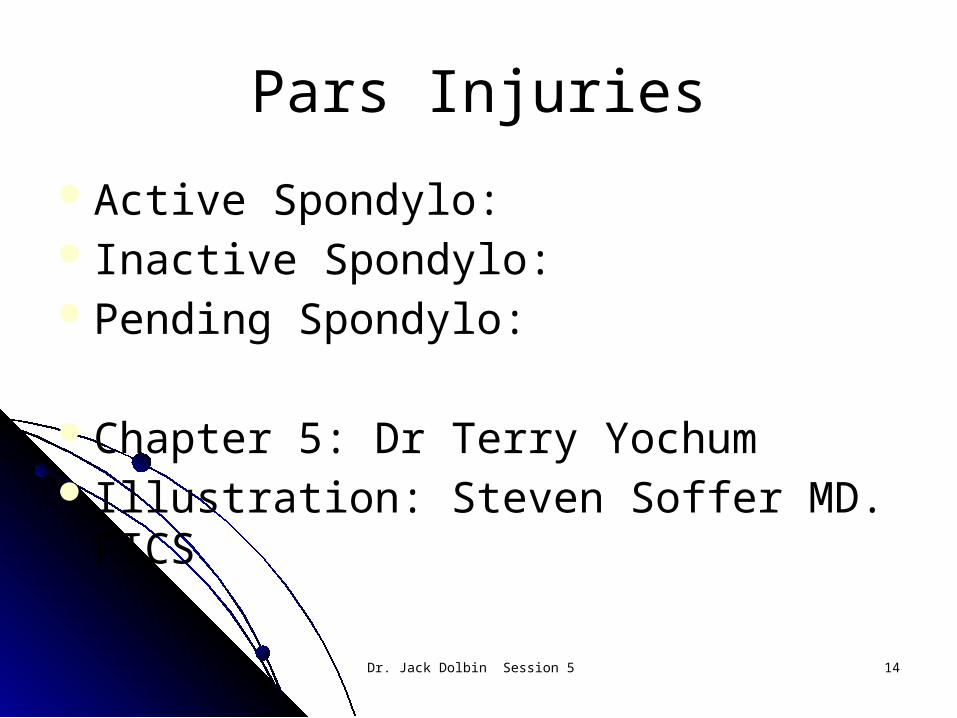
Bilateral Pars Defect
Dr. Jack Dolbin Session 5 23

Scotty Dog
Dr. Jack Dolbin Session 5 24

Active Spondylo
Dr. Jack Dolbin Session 5 25
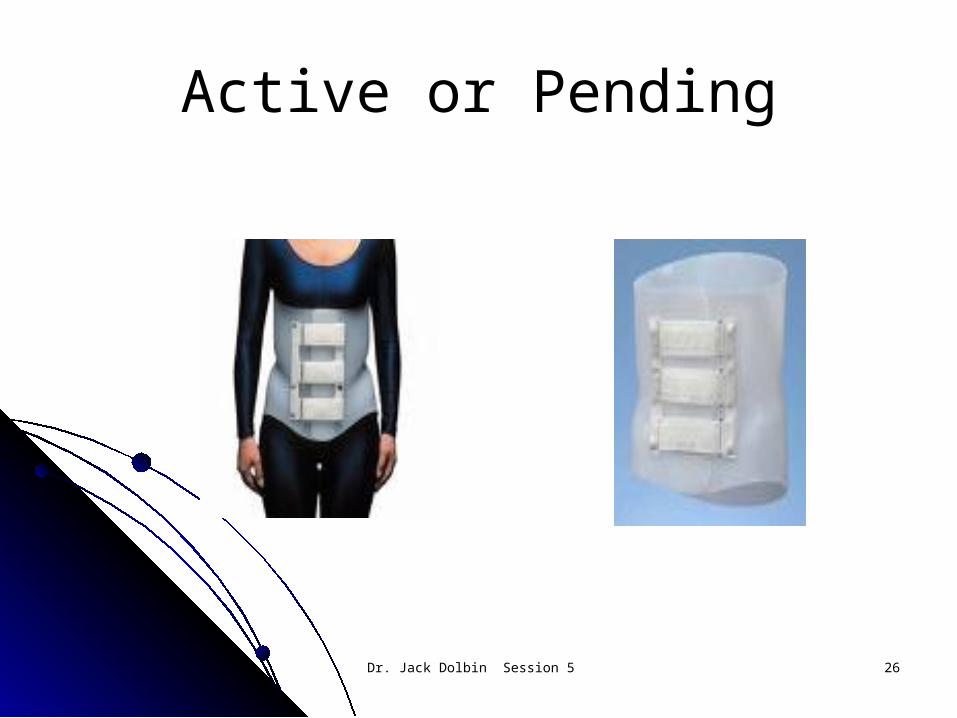
Active or Pending
Dr. Jack Dolbin Session 5 26

Treatment
HF 27 US .02 w/cm2 15 min.Laser/light 360 secondsBoston overlap: Minimum 2 months redo
spec bone scan or MRIOnce FX is healed: CMT, RMT,
progressive resistance exercises as per Wolfes Law.
Dr. Jack Dolbin Session 5 27
Rehab
Dr. Jack Dolbin Session 5 28

Rehab
Dr. Jack Dolbin Session 5 29

Rehab
Dr. Jack Dolbin Session 5 30

Rehab
Dr. Jack Dolbin Session 5 31

Rehab
Dr. Jack Dolbin Session 5 32

Rehab
Dr. Jack Dolbin Session 5 33

Rehab
Dr. Jack Dolbin Session 5 34

Rehab
Dr. Jack Dolbin Session 5 35

Rehab
Dr. Jack Dolbin Session 5 36

Rehab
Dr. Jack Dolbin Session 5 37

Rehab
Dr. Jack Dolbin Session 5 38

Rehab
Dr. Jack Dolbin Session 5 39

Rehab
Dr. Jack Dolbin Session 5 40

Rehab
Dr. Jack Dolbin Session 5 41

Rehab
Dr. Jack Dolbin Session 5 42

The Sacroiliac Joint
Normal function as it relates to performance
Dysfunction as it relates to injuryA. IT BandB. Patellofemoral syndromeC. Medial Shear at kneeD. Hamstring Injuries F. Pronation
Dr. Jack Dolbin Session 5 43
Normal SI Structure/Function
Sits at a 55 degree angle to the sagital plane and 30 degree to the frontal plane
Nutates in both the saggital and frontal plane
Shearing forces ie: long jumping, rebounding can subluxate the sacrum on the ilium spraining the iliolumbar and sacroiliac ligaments.
Dr. Jack Dolbin Session 5 44

Findings
History of shearing force or lifting and twisting
Palpatory exam: Iliolumbar, lumbosacral and sacroiliac ligament
Gaenslens TestYeomansNachlas
Dr. Jack Dolbin Session 5 45

AP SI Joints
Dr. Jack Dolbin Session 5 46

Anterior Inferior Sacrum
Dr. Jack Dolbin Session 5 47

SI ( continued )
Injury involves the quad femoris muscleMagines Syndrome. Marc Heller DCVery prominent in the female athleteUsually involves 5th lumbar facet Iliopsoas Muscle
Dr. Jack Dolbin Session 5 48

Pyriformis
Dr. Jack Dolbin Session 5 49

Pyriformis
Dr. Jack Dolbin Session 5 50

Lumbar Plexus
Dr. Jack Dolbin Session 5 51

Sciatic/Pyriformis relationship
Dr. Jack Dolbin Session 5 52

Iliopsoas
Dr. Jack Dolbin Session 5 53

Iliopsoas-Adductors
Dr. Jack Dolbin Session 5 54

SI Joint Treatment
Modalities as per presentationAdjustment: Long axisA. Does the Innominate rotate or does the
sacrum shear?B. Cyriax on Iliolumbar LigamentC. Check the kinetic chain including the
Head of the fibula, talus, navicularF. M.E on the pyriformis. IT band.
Dr. Jack Dolbin Session 5 55

Dr. Jack Dolbin Session 5 56
Cervical Spine Injuries:
Diagnosis, treatment, rehabilitation, prevention.
On the Field management. A. Range of motion, Spurlings, Jacksons,
Cervical CompressionB. Upper extremity Eval: Strength,
Neurology.

Cervical Spine Treatment
Modalities as per presentationProne Long Axis Adjustment or Impulse
adjustmentMuscle Energy TechniqueRehabilitation exercisesProtection: Collar
Dr. Jack Dolbin Session 5 57

Dr. Jack Dolbin Session 5 58

Head and Neck Injuries
Brain and Spinal CordHeal slowlyCannot regenerateCannot be replaced
Evaluation must be quick and precise

Head and Neck Injuries
Assume any unconscious athlete has a neck fracture
Immobilize head and neck Check airway
Check vitals: Blood pressure, pulse, respiration Assess state of consciousness Check pupils for reactivity, reflexes including
Babinski, reactivity Movement of extremities

Dr. Jack Dolbin Session 5 61

Head and Neck Injuries
Brain InjuriesCompressiveTensileShearing
Coup or contra coupCoup: Head is not accelerated. Injury at the
site of impactContra coup: Head is accelerated. Injury
opposite the site of impact

Dr. Jack Dolbin Session 5 63
Head and Neck Injuries
Skull FracturesLinear: Usually not brain injury.Depressed: Most likely to cause brain injury.

Head and Neck Injuries
Neck Injuries Axial Loading: Most serious. Is caused by flexing the
neck at the point of impact. Can cause a burst injury to the vertebrae. A 20% neck flexion causes the bone to absorb the force.
Flexion Sprain: Injury to the posterior soft tissue, ligaments, capsule, muscles. Most serious.
Extension Sprain: Injury to the anterior soft tissue with compression of the articular facets.

Cervicle Exam InspectionObservationARTCervicle CompressionJacksons Comp.SpurlingsSotoHall
Dr. Jack Dolbin Session 5 65

Upper Extremity Neurology
Inspection: Look for Atrophy/AsymetryARTDTRManual Muscle TestingAdsons, Allens , Wrights
Dr. Jack Dolbin Session 5 66
Treatment
Imflammation/PainRestore normal ROM: Adjustment,
Impulse, ME,Strengthen/Stabilize
Dr. Jack Dolbin Session 5 67

Dr. Jack Dolbin Session 5 68
Concussions:Evaluation Impact StudyReturn to participationRepeat Concussions

Concussions
Def: A complex pathophysiological complex involving the brain induced by traumatic biomechanical forces
Dr. Jack Dolbin Session 5 69

Concussions and Depression
Dr. Jack Dolbin Session 5 70

Common features include
1.Maybe caused by a direct blow to the head, neck or elsewhere in the body which transmits impulsive forces to the head.
2.Typically results in in a rapid onset of short lived impairment of of neurological impairment that resolves spontaneously
3.May result in neuropathological changes but largely functional disturbance rather than structural
Dr. Jack Dolbin Session 5 71

Common features ( cont.)
Result in a graded set of clinical symptoms that may or may not involve loss of consciousness. Resolution of clinical and cognitive typically follow a sequential course. In a small percentage post concussive symptoms may be prolonged
No abnormality on standard structural neuroimaging studies is seen in concussions
Dr. Jack Dolbin Session 5 72

Dr. Jack Dolbin Session 5 73

Symptoms
Somatic( headache) cognitive( feeling in a fog, emotional( lability)
Physical signs: loss of consciousness, amnesia
Behavioral: irritabilityCognitive: Slowed reaction timeSleep disturbance: drowsy
Dr. Jack Dolbin Session 5 74

Evaluation
Exclude Cervical Spine injury firstAddress First Aid IssuesPhysical ExamCognitiveNote: The player should not be left alone.
Monitor for deteriorationNo RTP on the day of the injury
Dr. Jack Dolbin Session 5 75

Concussions:Concussions: 20%/year in High school SportsGrade 1: No loss of consciousness.
Momentary period of post traumatic amnesia.Grade 2: Momentary loss of consciousness
lasting less that 5 minutes. Amnesia longer than 30 minutes but less than 24 hours.
Grade 3: Loss of consciousness greater than 5 minutes. Amnesia longer than 24 hours.

Dr. Jack Dolbin Session 5 77
Concussions: Chronic Brain Injury:
Traumatic encephalitis Repeated head injuries.

Dr. Jack Dolbin Session 5 78
Concussions: Post Concussion Syndrome:
Headache Dizziness Fatigue Irritability Impaired memory and concentration

Head InjuriesIntracranial Hemorrhage: Leading cause of
death from a head injury Epidural
Fracture of the Temporal bone Dramatic deterioration in consciousness in 30-
60 minutes Subdural hematoma
Most common fatal athletic head injury. Unconsciousness at the instant of impact Rapid deterioration

Head Injuries Intracerebral hematoma
Congenital malformation Aneurism Arteriovenous malformation
Subarachnoid Hemorrhage Brain bruise Aneurism a/v malformation

Dr. Jack Dolbin Session 5 81

Head InjuriesMalignant Brain Edema syndrome
Rapid deterioration to ComaDeath in a few hours
Second Impact SyndromeHyperemiaSecond acceleration head injuryRapid progression to coma.

Dr. Jack Dolbin Session 5 83

Concussion Eval
Dr. Jack Dolbin Session 5 84

Concussion Eval
Dr. Jack Dolbin Session 5 85

Return to Play Protocols
1. No Activity: Complete physical and cognitive rest. Until abate of symptoms
2. Light aerobic exercise: Increase HR3. Sport Specific Exer: add movement4. Non contact drills: exercise,
coordination, cognitive load5. Full contact: restore confidience,
assessment of functional skills5. RTP Dr. Jack Dolbin Session 5 86

Dr. Jack Dolbin Session 5 87
Neck and Spinal Cord Injuries
Cervical SprainDamage to musculo/tendinous/
ligamentous unitRemove from competition

Dr. Jack Dolbin Session 5 88

Neck and Spinal Cord Injuries
Spinal Cord ConcussionViolent impact to the vertebral columnTransient loss of motor or sensory
functionSymptoms last less than 24 hoursIf greater than 24 hours may produce
permanent injury

Dr. Jack Dolbin Session 5 90
Neck and Spinal Cord Injuries
Central Cord Syndrome Greater loss in upper extremity Hyperextension Cervical
Sprain Can an adjustment cause a
disc to herniate?

Dr. Jack Dolbin Session 5 91

Neck and Spinal Cord Injuries
Burning Hand Syndrome:
Lateral Pinch( Stinger) Radiate down arm to thumb Several minutes duration Generally if radial in distribution it is the
neck. If ulnar distribution it is the thoracic outlet.

Direct Trauma
Dr. Jack Dolbin Session 5 93

Thoracic Outlet
Dr. Jack Dolbin Session 5 94

Traction
Dr. Jack Dolbin Session 5 95

Compression
Dr. Jack Dolbin Session 5 96

Evaluation
Range of motion cervical spineRange of motion shoulder, elbow, handDeep Tendon ReflexesMuscle testingPathological reflexesMake transport decision
Dr. Jack Dolbin Session 5 97

Evaluation
Adsons
Allens
Wrights
Dr. Jack Dolbin Session 5 98

Treatment
Ice to effected areaLaser Impulse Adjustments to Scalene Muscles Impulse Adjustments to TOSExercises to retract scapulaReturn to competition as symptoms allow.
Dr. Jack Dolbin Session 5 99

Return to competition decision-making
Concussions:Grade 1: 1st concussion: May return if
symptoms clear rapidly at rest and with exertion.
Grade 1: 2nd occurrence: Remove from competition for two weeks. Must then be asymptomatic for 7 days before return.
Grade 1: 3rd occurrence: Season over. No contact for three months.

Return to competition decision-making
MRI or EEG Neuro Psychiatric exam Grade 2: 1st occurrence: Stabilize the neck.
Asymptomatic for 7 days. Grade 2: 2nd occurrence: Asymptomatic for 1
month before return Grade 2: 3rd occurrence: Terminate season Grade 3: Transport, Remove from competition
for 1 month, asymptomatic for 1 week.

Return to competition decision-making
Factors to look at to prevent head and neck injuries
Head gearTechniqueNeck muscle conditioning

Return to competition after a neck injury:
Neurological Exam: Reflexes Hoffman’s sign Motor strength Sensory exam

Return to competition after a neck injury:
Orthopedic Exam: Full ROM in Cervical Spine Negative Spurlings Maneuver. Strength in all planes of motion in
Cervical Spine Normal Neuro exam