Embed Size (px)
Citation preview

Baby Cure
Early initiation of anti-retroviral therapy in
in-utero infected newborns; the potential for cure
Dr Jane Millar
1

No conflicts of interest to declare
2

Curing HIV
76.1 million [65.2 million–88.0 million] people have become infected with HIV since the start of the epidemic1
Only 1 person cured - “Berlin Patient”
Where to from here?
1. http://www.unaids.org/en/resources/fact-sheet3
0 10 20 30 40 50101
102
103
104
105
106
107
Age (m)
Viral lo
ad
c/m
l
Mississippi ChildViral load
ART ART
27.6m off ART
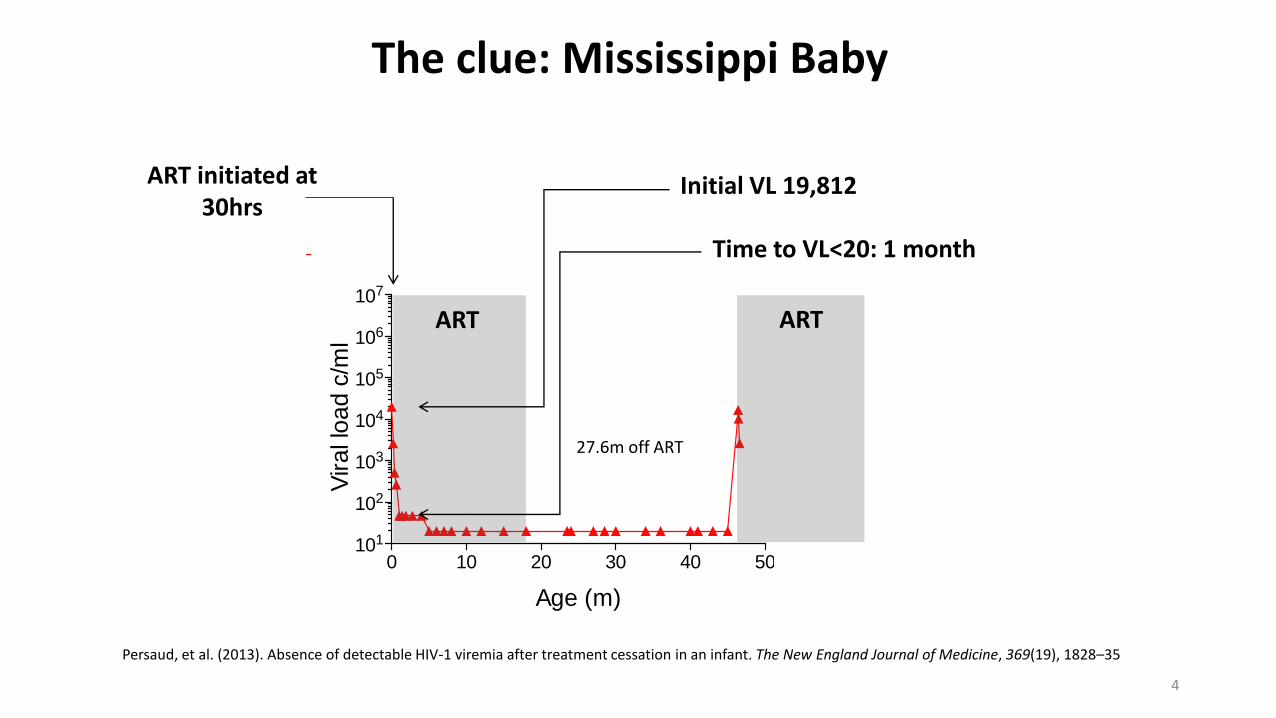
The clue: Mississippi Baby
Initial VL 19,812
Time to VL<20: 1 month
ART initiated at 30hrs
Persaud, et al. (2013). Absence of detectable HIV-1 viremia after treatment cessation in an infant. The New England Journal of Medicine, 369(19), 1828–35
4

What is special about babies?
1. Ability to treat early in infection
2. Immuno-tolerance
∴ Treatment reduces viral reservoir more efficiently
5

1. Ability to treat early in infection
Most in-utero infections occur late in 3rd trimester1
∴ Birth = early in infection
(Except maternal seroconversion in pregnancy)
1.Brossard et al. Frequency of early in utero HIV-1 infection: a blind DNA polymerase chain reaction study on 100 fetal thymuses. AIDS (1999)1. Rouzioux et al. Estimated timing of mother-to-child human immunodeficiency virus type 1 (HIV-1) transmission by use of a Markov model. Am. J. Epidemiol. (1995)
6

2. Different immune response
In-utero
Birth
Infant
Adult
Immuno-tolerance
• Higher levels of T regulatory cells (15 v 5%)
• Higher levels immunoregulatory and anti-inflammatory cytokines
• T helper 17 cell response (instead of damaging Th1)
Immune activation
• Vaccines (BCG)
• Infections (CMV)
• Gut microbial translocation in preterm infants
Immunocompetent
• Strong immune activation from HIV
• (damaging)
7

2. Different immune response
In-utero
Birth
Infant
Adult
Immuno-tolerance
• Higher levels of T regulatory cells (15 v 5%)
• Higher levels immunoregulatory and anti-inflammatory cytokines
• T helper 17 cell response (instead of damaging Th1)
Immune activation
• Vaccines (BCG)
• Infections (CMV)
• Gut microbial translocation in preterm infants
Immunocompetent
• Strong immune activation from HIV
• (damaging)
Early in infection
8

1. van Zyl et al Early antiretroviral therapy in South African children reduces HIV-1-infected cells and cell- associated HIV-1 RNA in blood mononuclear cells. J. J. Infect. Dis. (2015)2. Persaud, D. et al. Dynamics of the resting CD4+T-celllatent HIV reservoir in infants initiating HAART less than 6 months of age. AIDS 26, 1483–1490 (2012) 3. Hocqueloux et al. Long-term antiretroviral therapy initiated during primary HIV-1 infection is key to achieving both low HIV reservoirs and normal T cell counts. J. Antimicrob. Chemother. (2013)
∴ Treatment in neonates reduces viral reservoir more efficiently
Stevenson et al. Nature Medicine (2003)
HIV reservoir declines faster and for longer in babies1
T1/2 latently infected cells - Infants starting treatment at 8weeks = 11months2
- Adults in chronic infection 44m - (Adults faster if treated in acute infection)3
9

Veldsman et al. Rapid decline of total HIV DNA in children starting ART within 8 days of birth CROI (2017)
∴ Treatment in neonates reduces viral reservoir more efficiently
10

Introducing…
Baby Cure StudyPrinciple Investigator Professor Philip Goulder
Oxford UniversityWellcome Trust Funded
Is HIV cure more likely in children?
Does size of viral reservoir decline more rapidly in early-treated infants than early-treated adults/is it
smaller to start with?
Does ART initiation within 48hrs of birth versus within 2 wks of birth significantly affect viral reservoir?
How common is the Mississippi baby?
If ART is initiated within 48hrs of birth, and viral load undetectable by 1m and maintained on ART to 24m,what proportion of children have undetectable viral
reservoirs at 24m?
11

Study sites
Durban
Stanger
Empangeni
EdendaleMGMH
• 30,000 deliveries/year• Maternal HIV seroprevalence 38.4%• 11,500 babies born to HIV positive mothers/year• In-utero HIV transmission rate 0.5%
= In-utero HIV infections 55-60/year
12

High risk for HIV transmission in pregnancy
Immediate ARMDiagnose (GXP) + start
ART <48h of age
Early ARMDiagnose (DST) + start
ART 3-14d of age
Follow up monthly until 6m then 3 monthly– until 2020
Recruitment began August 201564 in-utero HIV infected babies enrolled so far
Study Essence
13

0 2 4 6 8 10 12 14101
102
103
104
105
106
107
0
1000
2000
3000
4000
5000
age (m)
Vira
l lo
ad
c/m
l
207-50-0473-1 Absolute CD4 countViral load
Ab
so
lute
CD
4 c
ou
nt
0 1 2 3 4 5 6 7 8 9101
102
103
104
105
106
107
0
1000
2000
3000
4000
5000
Age (m)
Vira
l lo
ad
c/m
l
207-60-1633-1 Absolute CD4 countViral load
Ab
so
lute
CD
4 c
ou
nt
0 1 2 3 4 5 6 7 8 9101
102
103
104
105
106
107
0
1000
2000
3000
4000
5000
age (m)
Vira
l lo
ad
c/m
l
207-60-1763-1 Absolute CD4 countViral load
Ab
so
lute
CD
4 c
ou
nt
Undetectable VL by 1m, maintained VL<20c/ml
Horizontal grey lines: 10th, 50th and 90th centiles, absolute CD4 counts in HIV-uninfected infantsBlue circles: absolute CD4
Red triangles: viral load
Potential Mississippi-type babies so far?
14

Two babies with initial viral load <20 c/ml
0 1 2 3 4 5101
102
103
104
105
106
107
0
1000
2000
3000
4000
5000
Age (months)
Vira
l lo
ad
(c/m
l)
207-70-0095-1A
bso
lute
CD
4 c
ou
nt/u
l
0 1 2 3 4 5 6101
102
103
104
105
106
107
0
1000
2000
3000
4000
5000
6000
Age (months)
Vira
l lo
ad (
c/m
l)207-50-2054-1
Ab
so
lute
CD
4 c
oun
t/ul
Each baby DNA PCR positive x3
Horizontal grey lines: 10th, 50th and 90th centiles, absolute CD4 counts in HIV-uninfected infantsBlue circles: absolute CD4
Red triangles: viral load15
~18% have died or are lost to follow up by 2 months
However…
16

Of those followed up…
~15% babies never reach VL<20 by 6m
0 1 2 3 4 5 6 7 8 9 10 11 12 13101
102
103
104
105
106
107
0
1000
2000
3000
4000
5000
Age (m)
Vira
l lo
ad
c/m
l
207-60-1251-1 Absolute CD4 countViral load
Ab
so
lute
CD
4 c
ou
nt
Horizontal grey lines: 10th, 50th and 90th centiles, absolute CD4 counts in HIV-uninfected infantsBlue circles: absolute CD4
Red triangles: viral load17

~55% of those who reach VL<20 don’t maintain suppression
0 2 4 6 8 10 12 14 16101
102
103
104
105
106
107
0
1000
2000
3000
4000
5000
Age (months)
Vira
l loa
d c
/ml
207-50-0555-1
Ab
solu
te C
D4
co
un
t
Horizontal grey lines: 10th, 50th and 90th centiles, absolute CD4 counts in HIV-uninfected infantsBlue circles: absolute CD4
Red triangles: viral load18

Where PMTCT fails, ART is not the answer
19

Answer: broadly neutralizing antibodies: bnAbs
• Long acting
• Directly neutralize virus
• Stimulate immune system• Cell mediated control
20

1. Hessell et al Nature Medicine 2016
VRC07-523 and PGT-121given to SHIV-infected macaques at
1, 3, 7 and 10d
By 1d, SHIV already established in the tissues
If bnAbs were given 1d after infection SHIV was cleared
21

2. Nishimura et al Nature 2017
3BNC117 and 10-1074given to SHIV-infected macaques
When bnAbs wore off, the macaques controlled viral
rebound elite controllers
Viral control mediated by CD8+ T-cells
22

In summary
• Mississippi Baby ignited the idea that babies may hold the potential for HIV cure
• ART treatment in babies can rapidly reduce the HIV viral reservoir because of the ability to treat early and their relative immuno-tolerance.
• The BabyCure study has demonstrated some ”Mississippi Baby” potentials
• However, where PMTCT fails, ART is difficult
• Antibody therapy in babies looks hopeful and should be explored further
23

Thank you
• To the audience for your attention
• The BabyCure study participants
• Prof Goulder and Oxford University
• The BabyCure study team
• Prof N’dungu and HPP
• Global Laboratory
• Wellcome Trust Fund
24





























