1 A REVIEW OF COLUMNAR CELL LESIONS IN FIBROCYSTIC CHANGE OF THE BREAST IN LAGOS UNIVERSITY TEACHING HOSPITAL (LUTH); A 10 YEAR RETROSPECTIVE STUDY (JANUARY 2004 TO DECEMBER 2013) BY DR JIMOH, ABIMBOLA.M (MBBS) A DISSERTATION TO BE SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENT FOR THE AWARD OF FELLOWSHIP OF THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PATHOLOGY 2014.
docx1
A REVIEW OF COLUMNAR CELL LESIONS IN FIBROCYSTIC CHANGE OF THE
BREAST IN LAGOS
UNIVERSITY TEACHING HOSPITAL (LUTH); A 10 YEAR RETROSPECTIVE STUDY
(JANUARY 2004 TO DECEMBER 2013)
BY
DR JIMOH, ABIMBOLA.M (MBBS)
A DISSERTATION TO BE SUBMITTED IN PARTIAL FULFILMENT OF THE
REQUIREMENT FOR THE
AWARD OF FELLOWSHIP OF THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF
NIGERIA IN
PATHOLOGY
2014.
2
CERTIFICATION BY SUPERVISORS
This is to certify that the study in this dissertation, A REVIEW OF
COLUMNAR CELL
LESIONS IN FIBROCYSTIC CHANGES OF THE BREAST IN LAGOS
UNIVERSITY
TEACHING HOSPITAL (LUTH); A 10 YEAR RETROSPECTIVE STUDY
(JANUARY
2004 TO DECEMBER 2013), is the original work of Dr Jimoh Abimbola
of the Department of Anatomic
and Molecular Pathology, Lagos University Teaching Hospital (LUTH),
Idi-Araba, Lagos.
DR. A.O. DARAMOLA, MBBS, FMCPATH
Associate professor and consultant pathologist,
Department of Anatomic and Molecular Pathology LUTH, Idi-Araba,
Lagos, Nigeria
SIGNATURE.................................................................................
Department of Anatomic and Molecular Pathology LUTH, Idi-Araba,
Lagos, Nigeria
SIGNATURE.................................................................................
Professor and Consultant pathologist,
Lagos, Nigeria
CERTIFICATION BY HEAD OF DEPARTMENT
This is to certify that this research project, A REVIEW OF COLUMNAR
CELL LESIONS IN FIBROCYSTIC CHANGES OF THE
BREAST IN THE LAGOS UNIVERSITY TEACHING HOSPITAL (LUTH); A 10 YEAR
RETROSPECTIVE ( JANUARY 2004 TO
DECEMBER 2013), was conducted in the Department of Anatomic and
Molecular Pathology, LUTH, Lagos.
Prof. F. B. Abdulkareem
Lagos University Teaching Hospital Idi-Araba, Lagos
Signature:__________________________________________
4
ACKNOWLEDGEMENT
To the Almighty God, my Father and my Friend I say thank you for
everything.
My husband, Philip Iyayi, for all your support and love. My loving
parents Akogun and Mrs B a b a t u n d e Jimoh,
without you I won’t be here today. I love you both.
To
To Professor Olusegun Ojo, for painstakingly and patiently teaching
me the art of writing. I
appreciate all that you did for me. Thank you.
Acknowledgement
LIST OF TABLES
Table 6.1: Age Distribution of Cases of Fibrocystic Changes of the
Breast
Table 6.2: Relationship between the Histopathologic Subtypes of
Fibrocystic Changes of
the Breast and Age of the Patient
Table 6.3: Relationship between the Subtypes of FCC and Occurrence
of CCLs Table 6.4:
Age Distribution of the Patient with FCC and CCLs
Table 6.5: Relationship Between Age Distribution of the patients
and Pattern of CCLs
Found
8
LIST OF FIGURES
Figure 1: Photomicrographs of Columnar Cell Lesion with no atypia
(a and b)
Figure 2: Photomicrograph of Columnar Cell Hyperplasia
Figure 3: Photomicrograph of Columnar Cell Change with atypia
showing luminal
secretion and apical snouts
Figure 4: Photomicrograph of Columnar Cell Hyperplasia with
atypia
Figure 5: Chart showing pattern and distribution of Columnar Cell
Lesions in the study
UV - Ultraviolet
DAB - Diaminobenzidine
Objectives:
We set out to find out whether CCLs occur among Nigerian women and,
if so, to estimate
their frequency of occurrence of CCLs, using fibrocystic change
(FCC) as a surrogate lesion
so as offer us a peep into its real prevalence in the wider women
population. We also set out
to determine the range of CCLs found using the recognized
histologic criteria
Materials and methods:
11
INTRODUCTION
BACKGROUND
Columnar cell lesions have been generating the interest of
pathologists in recent years as
they are a relatively new entity coming into clinical attention
upon finding them in biopsy
specimen sent for the investigation of microcalcification on
routine screening
mammography.
Screening mammography is not yet a widely practiced procedure in
Nigeria therefore to be
able to study Columnar Cell Lesions we look at the cystic variant
of Fibrocystic Changes
that appears to be the closest in morphologic features. These
benign lesion come into clinical
attention as imaging abnormalities or as palpable lesions found on
physical examination1
Fibrocystic Changes (FCC) of the breast fall into the non
proliferative group having
morphologic patterns such as cysts lined by cuboidal epithelium
often with apocrine
metaplasia, fibrosis and adenosis2. Similarly Columnar Cell Lesions
(CCLs) have cysts
though lined by tall columnar epithelium with apocrine snouts
making it possible for them to
have been previously lumped together however there is a need to
separate them as some
studies have suggested that CCLs may have an increased risk for
breast cancer progression3.
This entity has subsequently been described with a variety of names
and several studies have
been carried out in this regard. Of note is the work done by
Stuart.J.Schnitt who, along with
his team, have been involved in several studies4, 5,6,7,8 aimed at
formulating better
standardized diagnostic criteria and classification for better
projection of clinical
significance.
12
Schnitt and Vincent-Salomon were able to further characterize the
morphologic features of
CCLs and classify them into four categories: Columnar Cell Change,
Columnar Cell
Hyperplasia, Columnar Cell Change with atypia and Columnar Cell
Hyperplasia with
atypia4. In 2003, the WHO introduced the term “Flat Epithelial
Atypia” to describe the later
two categories. Flat epithelial atypia (FEA) is defined by the
presence of a neoplastic
intraductal proliferation characterized by replacement of the
native epithelial cells by a
single layer and up to 3-5 layers of mildly atypical cells.4 The
Schnitt classification was
modified by Simpson PT et al in 2005 into six categories by
addition of architectural atypia.9
Benign epithelial breast lesions have been re-classified and now
include some new groups
such as Columnar Cell Lesions (CCLs), a heterogenous group which,
in developed nations,
has been recognized for many years by pathologists and have been
described under a variety
of names. In our environment however, the lesions in this group
were hardly known among
pathologists until the last decade and have been lumped together
with Fibrocystic Changes
of the breast as the cystically dilated glands seen in these
lesions were often thought to be
microcysts of Fibrocystic Changes of the breast.
The major reason why this lesion is now coming to clinical
significance is the fact that
CCLs are being picked up on routine mammographic screening of the
breast carried out as
one of the cancer prevention strategies in the world over. As a
result many silent but
important breast lesions are being detected. CCLs tend to be
associated with
microcalcifications hence they are being detected more often now on
histologic biopsy
specimen because of the increased use of mammographic screening.
The study of these
13
lesions is done to have a better understanding of their biologic
and prognostic significance,
in the Black women population.
A search of the available literature reveals no previous study of
this nature has been
undertaken in Africa/blacks. The need for this study at this time
is to determine the
frequency of Columnar Cell Lesions in black women, their age
distribution and possible
implications.
Also this study hopes to draw clinical attention to Columnar Cell
Lesions especially CCLs
associated with atypia because of the risk of malignancy associated
with (FEA) which is
thought to represent a very early stage in the evolution of
low-grade DCIS and invasive
carcinoma3
14
CHAPTER TWO
L I T E R A T U R E R E V I E W
2.1 COLUMNAR CELL LESIONS OF THE BREAST
Columnar Cell Lesions (CCLs) are defined as enlarged terminal duct
lobular units (TDLU)
with dilated acini lined by tightly packed columnar epithelial
cells with prominent apical
cytoplasmic snouts and intraluminal secretions10. They have been
described under a variety
of names such as Blunt duct adenosis11, Columnar alteration with
prominent apical snouts
and secretions (CAPSS)12, Clinging carcinoma13, Enlarged lobular
units with columnar
alteration (ELUCA)14 etc. The use of these various names and
terminologies have hindered
the pathologist’s understanding of their biological significance
hence the evolution of the
classification and standard terminology scheme by Schnitt and
Vincent- Salomon in 2003.4
The use of this scheme has facilitated the study of CCLs as a
potential breast cancer risk
factor4.
The term ‘Blunt duct adenosis’ was introduced in 1945 by Foote and
Stewart to describe a
condition affecting the terminal duct lobular unit (TDLU)
characterized by hypertrophy
epithelial and myoepithelial layers with enlargement of lumina.15
‘Columnar metaplasia’
was used by Bonser, Dossett and Jull in 1961to describe the same
process. This term was
never taken into common usage but had the merit of recognizing that
epithelial hypertrophy
was the main feature of the condition.16 Other terms used to
describe this condition include
‘atypical cystic lobules’,17 ‘Columnar alteration of lobules’18,
‘Metaplasia cylindrique’19 and
Hyperplastic terminal grouping.
15
In the 1970s, Azzopardi coined the term ‘Clinging Carcinoma’ to
describe a form of Ductal
Carcinoma in situ (DCIS) characterised neoplastic cells confined to
the periphery of the
affected structures13. Clinging Carcinoma as described by Azzopardi
bears close similarities
to Columnar Alterations with Prominent Apical Snouts and Secretions
(CAPSS) reported by
Frasier et al. In 1998.12 The term CAPSS encompassed a spectrum of
lesions affecting the
TDLU, observed in breast biopsies performed for the evaluation of
microcalcifications.
Kasami et al. used the term ‘Enlarged Lobular Unit with Columnar
Alteration’ (ELUCA) to
describe TDLU with columnar cell alteration.14 In 2003 S.J Schnitt
and V. Salomon
described these lesions as a group as ‘Columnar Cell Lesions’
(CCLs) and further classified
them giving recognition to those with cytological atypia. The term
‘Flat Epithelial Atypia’
was introduced by the WHO to replace Columnar Cell Lesions with
atypia in 2003 and these
are the present nomenclature till date.
Columnar Cell Lesions are usually discovered by a breast cancer
screening mammogram
and in particular by the presence of microcalcifications9. About
75% of breast columnar cell
lesions will show microcalcifications and they usually have a round
or pleomorphic and
heterogeneous appearance on mammography. Columnar Cell Lesions are
typically
associated with calcifications of the calcium phosphate type and
they become deposited
within the variably sized duct lumina of dilated terminal duct
lobular units10.
In fact, in terms of all mammographic findings associated with
breast calcifications,
Columnar Cell Lesions rank fifth, following Fibrocystic Changes of
the breast,
Fibroadenoma, Ductal Carcinoma in situ (DCIS) and Sclerosing
adenosis20. Fine needle
aspiration cytology would usually reveal clusters of epithelial
cells which can be columnar
16
admixed with myoepithelial cells with or without apical snouts and
calcification, 21 if there is
any concern at all, it will tend to be founded upon any 'atypical'
appearance to the columnar
cells. FNA alone is not considered reliable for diagnosing or
categorizing CCLs10.
Columnar cell lesions are commonly seen in premenopausal and
perimenopausal women
usually between the ages of 44 to 513, 10, they occur bilaterally,
are multifocal in most cases
and have not been recorded in men.
In the UK, studies have shown that Columnar Cell Lesions were
reported in 42% of biopsies
specified for microcalcification radiographically.22Although no
study has been done in
Nigeria on Columnar Cell Lesions, several studies have been carried
out on benign breast
diseases with Fibroadenoma and Fibrocystic Changes topping the list
in this category23.
2.2 Fibrocystic Changes of Breast
This applies to a miscellany of changes in the female breast that
include predominantly of
cyst formation, adenosis and fibrosis. In the past, these lesions
were called Fibrocystic
disease however since most of these changes have little clinical
significance beyond the
need to distinguish them from cancer, the term Fibrocystic Changes
is preferred.2
Overall, Fibrocystic Changes of the breast are the most common
breast abnormality seen in
premenopausal women. These changes tend to arise during
reproductive age and most likely
a consequence of cyclic breast changes that occur normally in the
menstrual cycle. Estrogen
therapy and oral contraceptives do not seem to increase the
incidence of these alterations,
oral contraceptives may, in fact, decrease the risk of the
developing FCC.2
17
Fibrocystic changes can be subdivided into non- proliferative and
proliferative patterns. The
non-proliferative changes are the most common types of Fibrocystic
lesions, characterized
by an increased fibrous stroma associated with dilation of ducts
and formation of variably
sized cysts while the proliferative changes comprise of epithelial
hyperplasia and sclerosing
adenosis.
Epithelial hyperplasias are recognized by the presence of more than
two cell layers. The
spectrum of the epithelial hyperplasia ranges from mild and orderly
to atypical hyperplasias
with features that resemble in situ carcinoma.2 Sclerosing adenosis
is significant because its
clinical and morphologic features may mimic those of carcinoma.
They contain marked
intralobular fibrosis and proliferation of small ductules and
acini. Studies have shown that
the non-proliferative pattern of FCC is more prevalent both in
Black-African and other
races23,24
2.3 The relationship of Fibrocystic changes to Breast Cancer.
Although Fibrocystic Changes are benign, some features may confer
an increased risk for
the development of cancer, risks ranging from minimal to
significant increased risk of
development of breast cancer. Fibrosis, cystic changes, aprocrine
metaplasia and mild
hyperplasia have minimal or no risk of development of breast
cancer.2
Mild to florid hyperplasia without atypia, ductal papillomatosis
and sclerosing adenosis have
a slightly increased risk (1.5 – 2 fold) of developing breast
cancer. While on the other hand
are atypical hyperplasias whether ductal or lobular have a
significantly increased risk (5
fold) of developing cancer of the breast.2
18
2.4 Fibrocystic change and Columnar cell lesions
Columnar Cell Lesions are a group of lesions suspected by several
authors to lie within the
constellation of Fibrocystic Changes of the breast.25, 26 They
share some similarities with the
certain patterns of Fibrocystic Changes such as presence of cysts
and epithelial hyperplasia.
Columnar Cell Lesions of the breast share a resemblance with the
cystic type of Fibrocystic
Changes of the breast hence its association with CCLs and this is
what make FCC of the
breast an acceptable surrogate with which CCLs can be reasonably
studied. The previous
terminologies used in describing CCLs such as ‘Blunt Duct
Adenosis’, ‘Enlarged Lobular
Unit with Columnar Alterations’, ‘Columnar Alterations with
Prominent Apical Snouts and
Secretions’ etc create a descriptive confusion between Fibrocystic
Changes and Columnar
Cell Lesions of the breast.
2.5 Classification of Columnar Cell Lesions (CCLs)
CCLs are characterized by dilated TDLUs lined by columnar cells
with prominent apical
snouts that are perpendicular to the basement membrane. The dilated
acini may appear
rounded with a smooth outline giving it a rigid look, may be
angulated or have a branching
configuration.10 There may or may not be an increase in cell layer,
luminal secretions may
be present, calcifications are common and can be granular or
psammomatous.27
The need for the classification of Columnar Cell Lesion arose as a
result of the use of
various terminologies which hindered the Pathologist’s
understanding of their biologic
significance hence the evolution of this classification. The use of
this classification scheme
is to facilitate the study of CCLs as a potential breast cancer
risk factor4
19
Columnar cell change (CCC) with no atypia
Columnar cell hyperplasia (CCH) with no atypia
Columnar cell change with atypia
Columnar cell hyperplasia with atypia.
And was modified by Simpson in 2005 as follows3:
Type 1 (columnar cell change, CCC): 1-2 cell layers, columnar cells
have uniform
ovoid/elongated nuclei perpendicular to the basement membrane;
without/
inconspicuous nucleoli; may have apical snouts but usually not
prominent.
Type 2 (columnar cell hyperplasia, CCH): >2 stratified cell
layers with variable
nuclear crowding and cellular micropapillations, but no complex
architectural
patterns (i.e. no rigid bars, bridges or well-formed micropapillary
structures);
cytology similar to type 1 but may have hobnail cells. Associated
with intraluminal
calcification.
Type 3 (columnar cell hyperplasia with architectural atypia): >2
stratified cell layers
with complex architectural patterns (micropapillary, tufts, fronds,
arcades, rigid
bridges or punched out spaces); type 2 cytology.
Type 4 (columnar cell hyperplasia with cytologic atypia): type 2
architecture; mild
to moderate cytologic atypia, may resemble tubular carcinoma.
Type 5 (columnar cell hyperplasia with cytologic and architectural
atypia): type 3
architecture; type 4 cytology.
Type 6 (columnar cell change with cytologic atypia): 1-2 cell
layers; type 4
cytology.
20
In the current WHO classification, CCLs with cytologic atypia are
referred as Flat Epithelial
Atypia (FEA) in order to describe a presumably neoplastic
intraductal alteration
characterized by replacement of the native epithelial cells by a
single or 3-5 layers of mildly
atypical cells.3
2.6 COLUMNAR CELL CHANGE (CCC): is characterized by TDLUs with
varying
degrees of dilatation and the normal epithelium is replaced by one
or two layers of tall
columnar epithelial cells that have basally placed nuclei and
apical cytoplasmic snouts. The
nuclei are arranged in a regular fashion perpendicular to the
basement membrane, uniform
oval to elongated and have evenly dispersed chromatin without
conspicuous nucleoli.10,27
The myoepithelial layer is retained or even prominent, mitotic
figures are rare. The dilated
acini typically show undulating outline with irregular branching
with or without associated
calcification10
Figure 1: Photomicrograph of Columnar cell change with no atypia
(a) of a TDLU and
(b) showing apical snouts and flocculent secretion28
21
2.7 COLUMNAR CELL HYPERPLASIA (CCH): the acini are lined by more
than
two cell layers. The nuclei are bland in appearance and are mostly
perpendicularly arranged
to the basement membrane. There may be an appearance of
hyperchromasia due to crowding
and overlapping. The architecturally hyperplastic columnar cells
may form small mounds,
tufts or short micropapillations but they do not form bridges or
true micropapillae. Apical
snouts more exaggerated than CCC are present along with luminal
secretions and
calcifications which are sometimes psammomatous may be
present27.
Figure 2: Photomicrograph of Columnar cell hyperplasia with no
atypia showing
prominent apical snout and flocculent secretions.28
2.8 FLAT EPITHELIAL ATYPIA (FEA): a neoplastic proliferation of
TDLUs
characterized by replacement of the normal epithelial cells by one
to several layers of
monomorphic epithelial cells showing low grade cytologic atypia6.
They have smooth
nuclear outlines lacking grooves and notches, chromatin pattern is
fine and evenly dispersed
with one or two nucleoli seen. Mitotic activity is sparse or
absent. Flat in this context is a
22
relative term simply denoting the absence of complex architectural
patterns,7 such as well-
developed micropapillations, rigid cellular bridges, bars and
arcades, or sieve-like
fenestrations, with evidence of cellular polarization within the
micropapillations and bars or
around the fenestrations.
Figure 3: Photomicrograph of Columnar cell change showing atypical
columnar cells
with apical snouts, flocculent secretions and
calcifications.28
23
There is accumulation of cytoplasm at their poles giving rise to
apical snouts. It is of note
that the cells may be cuboidal rather than columnar in shape18.
They have dilated acini
which are often more regular in outline than the undulating pattern
seen in non atypical
lesions i.e. internal borders of the dilated acini typically appear
round and rigid and a
lymphocytic inflammatory infiltrate is commonly seen in the
surrounding stroma10,27.
Figure 4: Photomicrograph of Columnar cell hyperplasia showing
atypia28
24
The absence of architectural complexity and low grade cytologic
atypia are two prerequisite
in making a diagnosis of FEA, by definition the architecture in FEA
is flat, that is, it lacks
micropapillae, arches ,bridges ,cribriform spaces etc this is vital
in separating this lesion
from ADH and low grade DCIS. Their cytological features may be
alike but Atypical Ductal
Hyperplasia (ADH) and low grade DCIS have complex architecture.
High grade cytological
atypia is not a feature of FEA, the presence of high grade
cytological atypia even without
architectural atypia warrants a diagnosis of DCIS. Other names used
to describe lesions
within the category of FEA are Atypical cystic duct29, Atypical
cystic lobules30, Atypical
lobules type A31, Clinging Carcinoma13, Columnar Alteration with
Prominent Apical Snouts
and Secretions with atypia5, Columnar Cell Change with atypia4,
Columnar Cell Hyperplasia
with atypia4, Ductal Intraepithelial Neoplasia of the monomorphic
type32, Hypersecretory
hyperplasia with atypia33 and Small ectactic ducts lined by
atypical ductal cells with
apocrine snouts33.
Due to the fact that an element of subjectivity exists in such
cytological assessments,
difficulties and controversies in assigning a diagnostic category
to some borderline lesion
pose some practical problems but as pathologists gain more
experience with these types of
lesions, hopefully a classification system based on more objective
criteria will be adopted.
2.9 THE IMMUNOHISTOCHEMISTRY OF COLUMNAR CELL LESIONS
CCLs typically show positivity for CK8, 18 and 19 in keeping with
their luminal epithelial
cell nature and show negativity for basal cytokeratin such as CK 5
and 6 therefore they are
not useful in differentiating CCLs with atypia and those without.
CCLs show diffuse and
strong positivity for estrogen (ER) and progesterone (PR) and
androgen receptor (AR). Bcl2
25
and cyclin D1 positivity, low proliferation indices with Ki-67 and
reduced CD117
expression. CCLs are typically negative for HER2 and p5330, 35, 36.
It is worth noting that
patients with ER negative CCLs were at increased risk of malignancy
compared with those
whose lesion were ER positive, but as yet there are no confirmatory
studies14
2.10 THE CLINICAL APPLICATION OF THE IMMUNOHISTOCHEMISTRY
OF CCLs
The Immunohistochemistry of CCLs is useful in differentiating them
from some similar
lesions that share a form of morphological similarity or the other.
ER-PR staining of usual
ductal hyperplasia appears heterogeneous and limited to about
10-15% of cells38 and express
basal markers such as CK5/6.
Studies have shown proliferative labelling index Ki67 of 0.3% in
Columnar Cell Lesions
versus 13.7% in DCIS.
2.11 THE MOLECULAR BIOLOGY OF COLUMNAR CELL LESIONS
Loss of heterozygosity has been demonstrated in the majority of FEA
with loci on 11q, 16q
and 3p being most commonly involved, these genetic alterations are
similar to those
occurring in co-existent with DCIS or invasive carcinoma. Also
there are recurrent losses on
16q, 17p, 17q, 10q, 9q and gains on 15q, 16p and 19p27.
The presence of identical genomic aberrations in CCLs matched with
ADH and Low grade
DCIS provide strong circumstantial evidence to suggest that CCLs
are part of a group of
inter-related lesions, the so called ‘low grade breast neoplasia
family’ and they constitute the
first morphologically identifiable precursor of low grade breast
cancer.32
26
Furthermore, molecular analysis have demonstrated that the majority
of Columnar cell
lesions are clonal and neoplastic rather than hyperplastic.23
Interestingly the degree of
genetic changes found in Columnar cell lesions appears to mirror
the degree of architectural
and cytological atypia found in different types of CCLS.9
Despite the overlapping morphology, phenotype and genetic
aberrations found in Columnar
cell lesions and the fact that CCLs comprise a spectrum of lesions,
from a clinical
standpoint, most authorities argue that the most important
differentiation is between
Columnar cell lesions with atypia (FEA) and those without.
2.12 THE HISTOPATHOLOGICAL EVALUATION OF CCLs
CCLs are characterized by enlarged/dilated TDLUs lined by columnar
cells with prominent
apical snouts that are perpendicular to the basement membrane. The
dilated acini may
appear rounded with a smooth outline giving it a rigid look, may be
angulated or have a
branching configuration.10 There may or may not be an increase in
cell layer, luminal
secretions and calcifications are common.
A number of benign lesions are differentials of CCLs such as
microcyst of Fibrocystic
Changes (FCC), Apocrine Cysts, Pseudolactational Change, Cystic
Hypersecretory
Hyperplasia, Usual Epithelial Hyperplasia and differentiating FEA
from Atypical Ductal
Hyperplasia and low grade DCIS10.
In the cystic variant of Fibrocystic Changes the cells lining the
glands are flat or low
cuboidal cells in contrast to columnar cells10. In Apocrine cysts
of the breast, though the
glands are lined by columnar cells, the cytoplasm is more granular
also the nuclei are round
27
and open with a single prominent nucleolus unlike CCLs whose nuclei
are ovoid. Also
hobnail cells, exaggerated apical snouts and flocculent
intraluminal secretions are seen in
CCLs these features are absent in apocrine lesions. Unlike CCLs,
apocrine cells
characteristically lack the expression of Bcl2 and ER. As for
Pseudolactational change the
epithelial cells are cuboidal not columnar and the foamy appearance
of the cytoplasm
producing lipid should point the pathologist in the right
direction. With Cystic
hypersecretory hyperplasia the dilated ducts are lined by flat
epithelium with a characteristic
abundance of luminal homogenous colloid-like material, there are no
apical snouts and
apocrine metaplasia. In Usual hyperplasia (non atypical) the cells
are ovoid with small
grooves or notches and slightly granular chromatin and small
nucleoli. The cells of Usual
hyperplasia may show overlapping and a more disorderly arrangement
compared to the
orderly arrangement of CCLs. To avoid over-diagnosis, some staining
with cytokeratin 5
and 6 are helpful as they stain positively in usual
hyperplasia.
CCLs with atypia (FEA) do not form complex architectural structure,
if architectural atypia
is present as well as cytological atypia then a diagnosis of ADH or
low grade DCIS is
appropriate.
It has been noted that CCLs sometimes coexist with other well
defined lesions such as
lobular carcinoma, ADH, low grade DCIS and invasive carcinoma
especially lobular
hyperplasia and lobular carcinoma in-situ but it is uncommon for
various types of columnar
cell lesions to coexist in the same area. The “Rosen’s triad has
been proposed for lesions
consisting of CCLs, Lobular carcinoma in situ and Tubular
carcinoma.38,39
28
2.13 THE PROGNOSIS AND CLINICAL SIGNIFICANCE OF CCLs
CCLs of the breast encompass morphological spectrum which may
coexist within a wide
range of lesions that may include in situ and invasive carcinoma.39
However the overall
biological significance of these lesions are not known.40
Eusebi et al discovered 25 cases (0.26%) of what was called low
grade clinging carcinoma
of the flat type, but which appears morphologically equivalent to
FEA, during an average
follow-up interval of 19 years, none of the 25 women with low grade
clinging carcinoma of
the flat type developed invasive carcinoma and only one had a
recurrence, which was
described as consisting of low grade clinging carcinoma of the flat
type41, there are other
studies that also suggest that the risk of developing subsequent
breast carcinoma in patients
with FEA is considerably low.8,42,43 At a more fundamental level,
there is evidence that, in
general, there is progressive allelic damage in FEA through to
DCIS.9,40 However because
of the scarcity of clinical follow up studies addressing the
relationship of CCLs and
malignancy, long term follow-up studies are essential before
definitive conclusions are
reached.
Finally the management for patients with CCLs is controversial. In
a breast biopsy CCLs
with no atypia requires no further investigation or excisional
biopsy however when FEA is
present a follow-up excisional biopsy is recommended because
studies have shown that up
to 30% of formal excisional biopsies will demonstrate more
significant pathology i.e. ADH,
DCIS, or invasive carcinoma and a thorough search must been carried
out on the specimen.
The patient should be managed according to the most advanced lesion
present. If FEA is the
most advanced lesion then it is probable that no further treatment
is required but close
29
clinical monitoring is the current prevailing management10. It is
worth mentioning at this
point that a constellation of Fine needle aspiration cytology
(FNAC), core needle biopsy and
excisional biopsy are the standard approach in the investigation of
CCLs43. However more
studies to better define the long term clinical and biologic
significance of FEA are required.
There are specific groups of breast lesions that are difficult to
diagnose using FNAC alone.
These include the non-palpable borderline lesions such as the
florid epithelial hyperplasia,
columnar cell lesions including flat epithelial hyperplasia and ADH
and low grade DCIS.
Although in general they have distinct cytological features, in
actual daily practice, a
confident classification and differentiation of these entities is
still unachievable. One needs
to put into proper clinical perspective that most of these lesions
are non palpable and it is
difficult to ensure direct sampling at FNAC. Even with imaging
guidance it may not be
possible to sample these lesions adequately by cytological
means.44
Columnar Cell Lesions in breast core biopsies are typically sampled
for histological
assessment of mammographic microcalcifications. These specimens
should be examined at
multiple levels (at least three), if CCC or CCH only is found
without atypia, the lesion
should be regarded as within the constellation of fibrocystic
change and categorised as B2,
benign.45
Columnar Cell Lesions with atypia should be regarded as FEA and
classified as B3, of
uncertain malignant potential.45 As for all such screen-detected
lesions, multidisciplinary
discussion should be undertaken to correlate radiological, clinical
and histopathological
findings.
30
The average age of occurrence of Columnar Cell Lesions is 45+ 2,
most of these lesions
occurred in middle age though these findings are based on studies
carried out on Caucasian
women. Since no study of this nature has been carried out on the
black women race, no age
range is associated with these lesions. The predilection for any
race or geographic
distribution has not been documented so far, this study hopes to
shed light on issues as these.
31
RATIONALE FOR THE STUDY
Columnar Cell Lesions though have come to knowledge since the
1940s, is still evolving.
Several pathologists have carried out studies to determine the
nature and clinical
significance of these lesions. However there is still a lot of grey
areas and controversy in
the evaluation of its clinical significance.
Most of these studies have been carried out on the Caucasian female
breast and,
geographically, in the western world. From an extensive review of
literature done, no study
of this nature has been carried out on the African or
African-American women population
or even in Africa.
Obviously, the study of Columnar cell lesions is in its early days
and, in my own opinion, a
better understanding of this entity cannot be made until more
studies are carried out among
all races and in more locales as to the nature and long term
clinical significance of
Columnar cell lesions.
This study was carried out to establish whether Columnar Cell
Lesions occur at all in
women of African descent, and if so, to determine their patterns of
occurrence and
frequency. This study will hopefully ignite the desire in other
researchers to evaluate the
lesion in terms of their long term clinical significance in black
women and explore the
differences in the behaviour of the lesion in black and white
women, if any.
32
At the present time, very little is known about the occurrence of
CCLs in much of Africa
and Nigeria. In Nigeria, Screening mammography is not in widespread
and consistent use.
This fact constitutes a serious impediment to the study of CCLs in
this country.
However Columnar cell lesions of the breast share a resemblance
with the cystic type of
Fibrocystic changes of the breast hence its association with CCLs
and this makes FCC of
the breast an acceptable surrogate with which CCLs can be
reasonably studied.
33
The aim and objectives of the study are as follows:
4.1 AIM
To investigate the occurrence and nature of CCLs in FCC in LUTH
patients.
4.2 OBJECTIVES
1. To estimate the frequency of occurrence of CCLs in FCC to
probably offer us a peep
into its real prevalence in the wider women population
2. To determine the range of CCLs found in those positive cases
using the conventional
histologic criteria
3. To tabulate the relative proportions of these entities
identified in 2 above
4. To evaluate these data in light of the current thinking on CCLs
worldwide
5. Explore the implication of the findings in 2 and 3 above for the
incidence of breast
cancer in Nigeria, if any.
34
5.1 THE STUDY DESIGN /INCLUSION CRITERIA
The study involved the analysis of tissue blocks and slides of the
breast which received a
final histological diagnosis of Fibrocystic Changes of the breast
at the Department of
Anatomic and Molecular Pathology of the Lagos University Teaching
Hospital, between
January 2004 and December 2013.
The studies of Columnar Cell Lesions have been traditionally
carried out among patients
who had undergone screening mammography. However, since this
procedure is not in
widespread use in Nigeria, a surrogate lesion, FCC was used.
The decision to select only FCC of the breast stemmed from the fact
that Columnar Cell
Lesions have features that can be seen in the cystic variant of
Fibrocystic Changes of the
breast hence the justification for them to have been previously
lumped together.
5.2 THE STUDY POPULATION
Selection Criteria: All consecutive cases of FCC of the breast
within January 2004 and
December 2014 were selected.
The materials that were used for this study were duplicate copies
of histopathological
reports that were issued within this period, tissue blocks and
corresponding archival slides.
40 cases were excluded from this study because their tissue blocks
and corresponding slides
were missing.
5.3 THE METHODOLOGY
Bio data and hospital information such as patient’s age, hospital
numbers laboratory
numbers and clinical details were extracted from the departmental
register. Blocks and
corresponding archival routine haematoxylin and eosin (H&E)
stained slides of all the cases
diagnosed within the ten year study period as fibrocystic changes
of the breast within the
period in question were retrieved. The archival slides were
reviewed and re-classified based
on the current WHO classification5 as: Columnar cell change,
Columnar cell hyperplasia
and Flat epithelial atypia. Only those that met the criteria for
CCLs were so re-classified.
The diagnostic criteria are as follows:
1. Presence of 1-2 layers columnar epithelial cells lining the
glands with no atypia were
called columnar cell change28.
2. The presence of greater than 2 layers of columnar epithelial
cells lining the glands
with no atypia were called columnar cell hyperplasia28.
3. The presence of even a layer of columnar epithelial cell with
atypia lining the glands
but no architectural atypia was called flat epithelial
cells28.
5.4 IMMUNOHISTOCHEMICAL ANALYSIS
Immunohistochemical studies for ER antibodies were carried out on
fresh sections that were
prepared from tissue blocks of the cases of CCLs. The decision to
stain the cases with ER
immunostain arose from previously documented studies35,45 which
showed that Columnar
cell lesions demonstrated diffuse and strong positivity for the
Estrogen Receptor.
36
5.5 DATA ANALYSIS
The data generated included the range and types of Columnar Cell
Lesions, age distribution
and the range of Fibrocystic Changes. These non-parametric data
were analysed manually
using tables and simple arithmetical analysis such as percentages
and proportions.
5.6 ETHICAL CONSIDERATION
Approval for the study was obtained from the Research & Ethical
committee of Lagos
University Teaching Hospital (LUTH). The permission of the Head of
the Department of
Anatomic and Molecular Pathology was also sought for the use of the
laboratory and other
archival materials where required.
RESULTS
6.1 A total of 559 consecutive cases of Fibrocystic Changes of the
breast were obtained
during the study period and analysed for the purpose of this
study.
The frequency of Fibrocystic Changes of the breast, the components
of FCC and pattern of
CCLs were correlated.
Table 6.1: Showing the Age Distribution of the Cases of Fibrocystic
Changes of the
Breast
11-19 Years 55 10%
20-29 Years 179 32%
30-39 Years 156 28%
40-49 Years 121 21.5%
50-59 Years 30 5.3%
60-69 Years 18 3.2%
Total 559 100%
Mean Age=36±12, Min Age=16, Max Age=63, Std Dev=12.104
Table 6.1 shows the age range of cases analysed was 16 years to 63
years, mean age was
36years (SD = 12.1). One hundred and seventy nine cases of
Fibrocystic Changes of the
breast occurred in the 3rd decade making up 32% of all the cases.
One hundred and fifty six
cases (28%) occurred in the 4th decade while 121 cases (21.5%)
occurred in the 5th decade
while 55 (10%) cases occurred in the 2nd decade. There were 30
cases (5.3%) in the 6th
decade and 18 cases (3.2%) seen in the 7th decade.
38
Table 6.2: Showing the Relationship Between the Histopathologic
subtypes of
Fibrocystic Change and Age of the patients.
AGE
CYST
FORMATION
STROMAL
FIBROSIS
ADENOSIS
EPIPHELIAL
PROLIFERATION
11-19 44 7.8% 42 7.5% 13 2.3% 5 0.9%
20-29 163 29.2% 160 28.6% 53 9.5% 18 3.2%
30-39 149 26.6% 149 26.6% 87 15.5% 10 1.8%
40-49 120 21.5% 121 21.6% 63 11.3% 7 1.3%
50-59 25 4.5% 30 5.4% 5 0.9% 4 0.72%
60-69 18 3.2% 18 3.2% 10 1.8% 2 0.36%
TOTAL 519 92.8% 520 93% 231 41.3% 46 8.2%
Table 6.2 show the different components of Fibrocystic Changes of
the breast comprising of
Cyst formation, fibrosis, Adenosis and Epithelial proliferation.
Stromal fibrosis and cyst
formation occurred in 520 and 519 cases respectively of all 559
cases while adenosis and
epithelial proliferation occurred in 231 and 46 cases respectively.
The largest number of
cases occurred in the 3rd decade for each component and the least
occurred in the 7th decade.
39
Table 6.3: Showing the Relationship between the Subtypes of FCC and
Occurrence of
CCLs
11-19 44 3 42 0 13 1 5 0
20-29 163 4 160 0 53 1 18 1
30-39 149 4 149 0 87 1 10 2
40-49 120 6 121 1 63 0 7 1
50-59 25 3 30 1 5 0 4 1
60-69 18 0 18 0 10 0 2 0
TOTAL 519 20 520 2 231 3 46 5
Table 6.3 depicts the relationship between the variants of FCC and
the occurrence of CCLs
in the various age groups. The largest numbers of the variants of
FCC occurred in the 3rd
decade however this does not correlate with the largest number of
CCLs which occurred in
the 5th decade. Most of the CCLs occurred in the cystic subtypes of
FCC with a total of 20
cases through all the age groups, epithelial proliferation variant
had 5 cases in total, 2 cases
in the fibrotic variant and 3 cases in the adenotic variant.
40
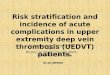
Figure 5: Chart showing the patterns of Columnar Cell Lesions in
the study
Figure 5 show the histopathological pattern in the 30 cases
obtained. The most common
histopathological pattern is pure Columnar Cell change with no
atypia CCC (66.7%) in 20 of
the 30, Columnar Cell Hyperplasia CCH in 5 cases (16.7%) and CCC
and CCH coexisting
in 5 cases (16.7%). No case of Flat Epithelial Atypia (FEA) was
found.
41
Table 6.4: Age distribution of the Patients with FCC and CCLs
Age Range FCC CCLs
11-19 55 9.8% 4 13.3%
20-29 179 32% 6 20%
30-39 156 28% 7 23.3%
40-49 121 21.6% 8 26.7%
50-59 30 5.4% 5 16.7%
60-69 18 3.2% 0 0%
TOTAL 559 100% 30 100%
Table 6.4 shows the occurrence of Columnar Cell lesions in
Fibrocystic Changes of the
breast in each age group. Eight cases of CCLs occurred in 121 cases
of FCC in the 5th
decade, 7 cases of CCLs in 156 cases of FCC in the 4th decade and 6
cases of CCLs in 179
cases of FCC in the 3rd decade. There were 5 cases of CCLs in 30
cases of FCC in the 6th
decade, 4 cases of CCLs in 55 cases of FCC in the 2nd decade and no
cases of CCLs in 18
cases of FCC in the 7th decade.
42
Table 6.5: Relationship between Age Distribution of the Patients
and Pattern of CCLs
found
PATTERN
20-29 Years 5 1 0
30-39 Years 6 0 1
40-49 Years 6 1 1
50-59 Years 1 3 1
60-69 Years 0 0 0
Total 20 5 5
66.7% 16.7% 16.7%
Table 6.5 show the range of patterns of Columnar Cell Lesion that
occurring in different age
groups. Six cases of Columnar Cell Change occurred in the 4th and
5th decade while 5 cases
occurred in the 3rd decade. Two cases of CCC were seen in the 2nd
decade while only one
case was seen in the 6th decade.
The table shows cases of mixed CCC and CCH pattern, 3 cases of such
occurred in the 6th
decade while 1 cases occurred both in the 3rd and 5th decade. The
2nd, 4th and 7th decade had
no cases of CCLs.
Columnar Cell Hyperplasia was seen in 2 cases within the 2nd decade
while 1 case was seen
in the 4th, 5th and 6th decade. No cases of CCH were seen in the
3rd and 7th decade.
43
Table 6.6: Showing the Frequency of Each Types of CCLs found
Age Frequency CCC CCC & CCH CCH
11-19 4 2 0 2
20-29 6 5 1 0
30-39 7 6 0 1
40-49 8 6 1 1
50-59 5 1 3 1
60-69 0 0 0 0
TOTAL 30 20 5 5
Table 6.6 shows the frequency of the range of CCLs within the
different age groups. Of the
8 cases of CCLs seen in the 5th decade 6 were CCC, 1 mixed CCC and
CCH and 1 CCH,
there were 7 cases in the 4th decade of which 6 were CCC, 0 cases
for the mixed pattern and
1 case of CCH.
Six cases of CCLs occurred in the 3rd decade, of these, 5 were CCC,
1 mixed pattern and
none was seen for the CCH pattern. In the 6th decade there were 5
cases, 1 case of CCC, 3
mixed pattern and 1 case of CCH and in the 2nd decade there were a
total of 4 cases of CCLs
seen, 2 cases were CCC and CCH each. There was no case of CCLs in
the 7th decade.
44
Figure 6: Photomicrograph of Columnar Cell Change with no atypia
(H&E x 100)
45
Figure 7: Photomicrograph of Columnar Cell Change with no atypia
(H&E x 100)
46
Figure 8: Photomicrograph of Columnar Cell Change with
micro-calcifications (H&E
x100)
47
Figure 9: Photomicrograph of Columnar Cell Change and Columnar Cell
Hyperplasia
with no atypia containing flocculent secretions (H&E
x100)
48
Figure 10: Photomicrograph of Columnar Cell Hyperplasia with no
atypia (double
arrow) and apocrine metaplasia (single arrow) (H&E x 100)
49
Figure 11: Photomicrograph of Columnar Cell Change with
microcalcifications and
flocculent secretions (H&E x100)
50
Figure 12: Photomicrograph of ER positive immunostain Columnar Cell
Change with
no atypia (x 100)
DISCUSSION
In this study, we looked into the occurrence of Columnar Cell
Lesions and determined the
most predominant pattern among Nigerian women as most of the
studies carried out so far
have been among Caucasians. The study was carried out using
Fibrocystic Changes of the
breast as a surrogate lesion because mammography is not yet widely
done in Nigeria and
CCLs bears some similarities with certain subtypes of FCC.
7.1 FIBROCYSTIC CHANGES OF THE BREAST
Fibrocystic Changes (FCC) of the breast, comprising of a
constellation of changes of cyst
formation, fibrosis adenosis and epithelial proliferation, are a
rather common benign
disorder that affect women within their reproductive years the
world over. Some variants of
FCC, principally the epithelial proliferation variants, have been
associated with an increased
risk of subsequent malignant change.2,10 However, it is emerging in
recent literature that
Columnar Cell Lesions (CCLs), while not clearly belonging to this
previously identified
FCC categories, may bear some risk of malignant change
also.3,4,5,7,8,9 CCLs have not been
studied among black women before now because their existence has
not been reported
among them. In this study we sought to identify CCLs among FCC
cases as a starting point
for the study of CCLs among black subjects.
52
7.1.1 Occurrence
The total number of cases of FCC found by us within the 10-year
study period was 559
cases, when compared with a study conducted in Ile-Ife on benign
breast diseases23 which
includes Fibrocystic Changes of the breast was found to be
significantly higher than that of
Ile-Ife which had 60 cases of Fibrocystic Changes for the same
period of time.
There is a significant difference in the number of cases seen
between the two studies, this
can be explained by the fact that this study was conducted in an
urban area and it would be
expected that there will be more patients with a wider variety of
lesions which FCC was one
of them.
In our series, the highest number of cases was in the 3rd decade
where 179 (32%) cases
occurred. This finding shows similarity with other studies46, 47,
23 carried out in Ibadan, Kano
and Ile-Ife that FCC had a peak occurrence in the third decade and
showed a relatively high
prevalence till the 5th decade before it declined.48
Most studies in the literature on FCC and other breast lesions both
benign and malignant
were done among Caucasian subjects. The documented age range of the
patients with
fibrocystic changes of the breast among Caucasians is between 20-50
years10 which is the
same as that of this study and similar studies conducted in Nigeria
as well as this one.
7.1.2 The Effects of Age on FCC
Fibrocystic Changes of the breast as mentioned earlier had the
highest incidence in the 3rd
decade of life followed by the 4th decade till the 5th decade.
These periods in a woman’s life
marks the peak of the reproductive period. Many studies have
suggested that FCC occurs in
53
the reproductive periods of a woman’s life23, 46, 47, 48 because of
the presence of circulating
hormones. Therefore, expectedly, there is a decline of FCC in post
menopausal women
which usually occurs at the end of the 5th decade to the 6th
decade. The age range of the
patients with FCC in this study is 16-63 which is also in
consonance with the study done in
Ile-Ife whose recorded age range for Fibrocystic Changes of the
breast was 16-60.23
7.1.3 Clinical importance of FCC
Fibrocystic changes of the breast are generally regarded as
harmless however certain
variants are associated with an increased risk of breast cancer
progression hence the need for
follow-up when these changes are found.
In this study, the majority of the cases presented with cysts and
fibrosis with fewer cases of
adenosis and epithelial proliferation, although there were overlaps
of the variants in many
instances. This finding is in agreement with the study on benign
breast diseases conducted in
Ile-Ife23 that found more variants of cyst formation and stromal
fibrosis over sclerosing
adenosis and epithelial proliferation.
In current literature, cystic and fibrotic variants of FCC have
been classified under the non-
proliferative pattern and have mininimal or no clinical
implication. The Proliferative group
of FCC comprising of sclerosing adenosis and epithelial
proliferation have a 1.5-2 fold
increased chances of progression to breast cancer.2
A study done in Yonsei, South Korea24 had majority of the women
92.5% with non-
proliferative pattern of FCC this is in consonance with the
findings in this study as well as
similar studies done elsewhere in Nigeria.23,46,47,48 The clinical
import of this for our
54
patients, in my opinion, is that there is no or minimal risk of
progression of FCC to breast
cancer as the majority of cases were in the non-proliferative
group.
7.2 Columnar Cell Lesions
7.2.1 Relationship between Columnar Cell Lesions and Fibrocystic
Change of the
Breast
Thirty cases of Columnar Cell Lesions were found in 559 cases of
Fibrocystic Changes of
the Breast in this study. Extensive literature search reveal no
previous study of this nature
that has been carried out. This study is unique because the study
population was pre-defined
by the occurrence of FCC in the subjects in the first place.
Traditionally, CCLs, as an entity,
arose out of studies of biopsies that are done after screening
mammography reveal calcific
anomalies in the subjects. Since screening mammography is novel in
Nigeria, we were
unable to do the traditional-type study. Our findings can therefore
only be seen as arising
from an initial, pioneering foray into this field locally in
Nigeria.
The putative relationship between Columnar Cell Lesions and
Fibrocystic Changes of the
breast provide the legitimizing plank for this study. The microcyst
variants of FCC and
CCLs in my own opinion share a similarity that makes it possible
for CCLs to have been
hidden in the category of the cystic variant of FCC in the past.
However it is obvious at this
point that they are not the same but are different entities that
carry different degrees of
association to breast cancer as CCLs only share a similarity with
the cystic variant which is
only a subset of FCC. This relationship is depicted in table 6.3
where 30 cases of CCLs were
found in 559 cases of FCC, the majority of CCLs were found within
the cystic variant this
further buttresses the opinion that the cystic variant of FCC and
CCLs share some
similarities.
55
Fibrocystic changes of the breast contain cysts, stromal fibrosis,
adenosis and epithelial
proliferation. The latter two variants confer a 1.5-2 fold chance
of progression to the breast.
On the other hand, CCLs are cystically dilated TDLU lined by
columnar cells with or
without epithelial hyperplasia and lack of architectural
complexity. The presence of
cytological atypia in CCLs makes it FEA5,28 which is a precursor of
breast cancer.
7.2.2 The Age Occurrence of Columnar Cell Lesions of the
Breast
In this study, we have been able to show that Columnar Cell Lesions
exists among Nigerian
women. It is perhaps most common during the 5th decade, this agrees
with studies conducted
on Caucasian women that the highest prevalence of CCLs is between
ages of 44-51.3, 4, 8, 10
On reviewing the existing body of literature on the subject, it
appears that the jury is still out
on why Columnar Cell Lesions occur majorly in middle age or its
association with this age
group.
7.2.3 The Histopathological types of CCLs
In this study, we found that 67% of Columnar Cell Lesions were
Columnar Cell Change
with no atypia which came to 20 cases of the 30 cases of CCLs.
Literature so far has not
documented a predominant type of Columnar Cell Lesion. This is
probably because it is
believed that only the atypical types are important. There were 5
cases of Columnar Cell
Hyperplasia and an overlap between CCC and CCH for the remaining 5
cases.
In this study, we found no case of Flat Epithelial Atypia (FEA).
This could be due to the
restriction on the number of cases identifiable by us that is
imposed by our using FCC as the
surrogate defining lesion of our study population. It is possible
that in the future, larger
56
studies on CCLs would identify some cases of FEA. We are therefore
unable to make any
comment here on its clinical significance as being a putative
precursor of low grade DCIS
among Nigerians.
7.2.4 Clinical and Biological importance of CCLs
Columnar Cell Lesions are believed to be possible precursors of
breast cancer because they
share immunohistochemal and molecular properties with atypical
Ductal hyperplasia (ADH)
and DCIS.9, 23, 26, 31 however the overall biological significance
is unknown.40 there are some
school of thought that says it is a marker of coexistence of breast
cancer as opposed to being
a precursor to it.37, 38 Due to the fact that no FEA was identified
in this study no deductive
comments can be made on its clinical significance in Nigerian
women.
7.2.5 Screening tools for CCLs
Columnar Cell Lesions have been generating interest among
pathologists in the recent years
as they come into clinical attention because of their frequent
observation in biopsy specimen
taken as a follow-up of screening mammography. As one of the breast
cancer screening tools,
screening mammography has brought CCLs into the spotlight in many
countries where this
is routinely done.
There is obviously a need for routine mammographic screening to be
instituted in Nigeria as
a tool in early detection of breast cancer and probably of its
putative precursor lesions such
as FEA, ADH etc. This is because early detection would bring about
significant reduction in
breast cancer morbidity and mortality generally.
57
7.3 Conclusions
At the end of this study, we come to the conclusion that Columnar
Cell Lesions occur in
Nigeria and, by extension, the black women population. We have also
shown that Columnar
Cell lesions are related to Fibrocystic Changes of the breast. The
prevalence of CCLs in
FCC is (30/559) 5.37%. Perhaps there could be more Columnar Cell
Lesions hidden within
other categories of benign breast diseases, borderline breast
lesions and malignant breast
lesions but these other lesions were not explored for the purpose
of this study because of the
limitation imposed by the nature of the sample.
A major negative finding in this study is that no case of FEA was
found, this could be also
due to the defining criteria of the study population that has put a
restriction on the variety
and extent of the sample. Obviously, larger studies need to be done
in order to extend the
applicability of our conclusions.
We recommend that Pathologists should become more aware of Columnar
Cell Lesions,
because certain variants, particularly FEA, have been identified as
precursor lesions to low
grade DCIS.
CHAPTER EIGHT
FURTHER WORK
This study was conducted to gain insight into the occurrence and
possible biologic and
clinical significance of Columnar Cell Lesions in the Black women
population. CCLs have
been identified and studied within the context of screening
mammography, a procedure that
is still novel in Nigeria.
Thus, in this study, we have had to improvise by studying CCLs
among a cohort of cases of
Fibrocystic Changes of the breast. Understandably, this has imposed
some limitation on
inferences that could be made from our findings.
In future studies, preferably at a time when screening mammography
in Nigeria becomes the
norm, research work should be conducted on a larger population of
women. It is
recommended that such studies should include a follow-up plan in
order to be able to
determine the its clinical significance of CCLs in the patients
thus studied.
59
LIMITATIONS OF THE STUDY
The interest in CCLs has been ignited by the finding of a strong
association between them
and microcalcifications detected on screening mammography for
breast cancer where this is
a routine procedure and core needle biopsies were taken for
evaluation of non palpable
lesions with microcalcification for presence of atypia
This has led to the desire to study CCLs in our environment however
this study was not
based on mammographic studies. Rather Fibrocystic Changes of the
breast (FCC) was
employed as a surrogate lesion and the basic selection criteria for
the sample population
because of the similarities it shares with the cystic variant of
FCC making it an acceptable
surrogate in which this study can be reasonably carried out. Thus
the Fibrocystic Changes of
the breast bias obviously was a major confounding variable limiting
the number of cases and
skewing its distribution among women in Nigeria.
The findings can therefore not be representative and the deductions
not universally
applicable. However, this study should be seen as a pioneer one, in
this field, beckoning for
larger ones when mammography becomes a routine screening proceedure
in Nigeria.
60
REFERENCES
1. Guray M, Sahin AA. Benign breast diseases: Classification,
diagnosis and
management. J Oncologist.2006;5:435-439
2. Vinay K, Abul KA, Nelson F. The Breast by Lester SC in: Robbins
and Cotran
Pathological Basis of Diseases 8th Ed. Elsevier Saunders,
Philadelphia 2010, pg
1126-1129
3. Agnantis NJ, Goussia AC. Epithelial Columnar Breast lesions,
Histopathology and
Molecular markers. 29th Annual International Conference (Greece)
June 2012.
http://www.cancerconferences.org.Presentation.pdf.(Accessed24/12/2012)
4. Schnitt SJ, Vincent-Saloman A .Columnar cell lesions of breast.
Adv Anat Pathol.
2003;10:113-124
5. Schnitt SJ. Columnar alteration with prominent apical snouts and
secretions: A
spectrum of changes frequently present in breast biopsies performed
for
microcalcifications. Am J Surg Pathol. 1998;22:1521-1527
6. Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, Van de Vijver MJ.
Intraductal Proliferative
lesions in: WHO classification of tumors of the breast 4th Ed. IARC
Press, Lyon
2012; pg 67-73
7. Stuart.J Schnitt; The diagnosis and management of preinvasive
breast disease, flat
epithelial atypia classification, pathologic features and clinical
significance. Breast
Cancer Res. 2003;5: 263-268.
8. Aroner SA, Collins LC, Schnitt SJ, Connolly JL, Colditz GA,
Tamimi R. Columnar
cell lesions and subsequent breast cancer risk: a nested case
control study. Breast
Cancer Research. 2010 12:R61.
9. Simpson PT, Gale T, Reis-Filho JS, Jones C, Parry S, Sloase JP
et al. Columnar cell
lesions of the breast – the missing link in breast cancer
progression: A morphological
and molecular analysis. Am J Surg Pathol 2005; 29:734-746.
10. Youngson B, O’Malley FP, Pinder SE, Mulligan AM. Fibrocystic
change and
columnar cell lesions of the breast in: The breast pathology 2nd
Ed. Elsevier Saunders
Philadelphia 2011; pg167-180.
11. Lanyi M, Citoler P. The differential diagnosis of
microcalcification. Microcyst (blunt
duct) Adenosis. Rofo. 1981; 134:225-231.
12. Frasier JL, Raza S, Chorny K, Connolly JL, Schnitt SJ. Columnar
alteration with
prominent apical snouts and secretions; a spectrum of changes
frequently present in
breast biopsies performed for microcalcifications. Am. J. Surg.
Pathol. 1998: 22;
1521-1527.
13. Azzopardi JG. Problems in breast pathology. In Bennington JL,
consulting Ed. WB
Saunders, Philadelphia 1979: pg 89-90.
14. McLaren BK, Gobbi H, Schugler PA, Olsen SJ, Parl FF, Dupont W
et al.
Immunohistochemical expression of estrogen receptor in enlarged
lobular units with
columnar alteration in benign breast biopsies: a nested case
control study. Am J Surg
Pathol. 2005;29(1):105-108.
62
15. Foote FW, Stewart FW. Comparative studies of cancerous versus
non-cancerous
breasts. Ann. Surg. 1945; 121: 6-53.
16. Bonser GM, Dossett JA, Jull W. human and experimental breast
cancer. London;
Pitman Medical, 1966: 336-347.
17. Wellings SR, Jensen HM, Marcum RG. An atlas of subgross
pathology of the human
breast with special reference to possible precancerous lesions. J.
Natl cancer Inst.
1975; 55: 231-273.
18. Page DL, Anderson TJ, Columnar alteration of lobules.
Diagnostic histopathology of
the breast. Edinburgh; Churchill Livingstone, 1987: 86-88.
19. Trojani M. Atlas en couleurs d’histopathologie mammaire. Paris;
Malone, 1988: 38-
43.
20. Picca DA, Shaw de Paredes E. Calcifications in the breast: A
radiological perspective.
Applied Radiology journal. 2003; 32:1-2.
21. Saqi A, Mazziotta R, Hamele-Bena D. Columnar cell lesions: Fine
needle aspiration
biopsy features. Diagn Cytopathol. 2004;31:370-375
22. Pinder SE, Reis-Filho JS. Non operative breast pathology:
Columnar cell lesions. J
Clin pathol. 2007; 60:1307-1312.
23. Adeniji K.A, Adelusola K.A, Odesanmi W.O. Benign disease of the
breast in Ile-Ife:
a 10 year experience and literature review. Central African Journal
of Medicine. 1997;
43: 140-143.
63
24. Hee JA, Nam HC, Woo IY, In JC. Benign proliferative disorders
of the breast. Yonsei
med J. 1990; 31(2): 168-173.
25. Tremblay G, Deschenes J, Alpert L, et al. Overexpression of
estrogen receptors in
Columnar Cell Change and in unfolding breast lobules. Breast J
2005; 11: 326-332.
26. Vincent-Salomon A. [Columnar lesions: a frequent diagnosis in
breast pathology!].
Ann Pathol. 2003; 23:593-596.
27. Feeley L, Quinn CM. Review of Columnar cell lesions of the
breast. Histopathol.
2008; 52:11-19.
28. Troxell ML, Brunner AL, Neff T, Warrick A, Beadling C,
Montgomery K et al.
Phosphatidyl-Inositol 3-kinase pathway mutations are common in
breast columnar
cell lesions. Modern Pathology 2012; 25:930-937.
29. Tsuchiya S. Atypical ductal hyperplasia, atypical lobular
hyperplasia and
interpretation of a new borderline lesion; Jpn. J Cancer Clin.
Oncol. 1998; 44: 548-
555.
30. Oyama T, Iijima K, Takei H, Horiguchi J, Iino Y, Nakajima T et
al. Atypical cystic
lobule of the breast: an early stage of low grade ductal Carcinoma
In Situ. Breast
Cancer. 2000; 7:326-331.
31. Wellings SR, Jensen HM, Marcus RG, Ratschek M, Tavassoli FA. An
atlas of
subgross pathology of the human breast with special reference to
possible
precancerous lesions. J. Nat. Cancer Inst. 1975; 55:231-273.
64
32. Moinfar F, Man YG, Bratthauer GL, Ratschek M, Tavassoli FA.
Genetic
abnormalities in mammary ductal intraepithelial neoplasia flat type
(Clinging
Carcinoma in Situ); a simulator of normal mammary epithelial.
Breast cancer. 2000;
88:2072-2081.
33. Page DL, Kasami M, Jensen Ra. hypersecretory hyperplasia with
atypia in breast
biopsies, what is the proper level of clinical concern?. Pathology
case Rev.1996;
1:36-40.
34. Goldstein NS, O’Malley BA. Cancerization of small ecstatic
ducts of the breast by
ductal carcinoma in situ cells with apocrine snouts: a lesion
associated with tubular
caranoma. Am. J. Clin. Pathol. 1997; 107:561-566.
35. Dessauragie BF, Zhao W, Heel Muller KA, Harvey J, Bentel JM.
Characterization of
columnar cell lesions of the breast: immunophenotypic analysis of
columnar
alteration of the lobules with prominent apical snouts and
secretions. Hum. Pathol.
2007; 38:284-292.
36. Lee S, Moshin SK, Mao S, Hilsenbeck SG, Medina D, Allred DC.
Hormones,
receptors and growth in hyperplastic enlarged lobular units, early
potential
precursors of breast cancer. Breast Cancer Res.2006;8: R6.
37. The mammary gland: Development, Regulation and Function. New
York, NY;
Plenum Press 1987.
65
38. Brandt SM, Young GQ, Hoda SA. The “Rosen Triad”: Tubular
Carcinoma, Lobular
Carcinoma In-situ and Columnar cell lesions of the breast. Adv.
Anat. Pathol. 2008;
15:140-146
39. Rosen PP. Columnar cell hyperplasia is associated with Lobular
Carcinoma in-situ
and Tubular carcinoma. Am. J. Surg. Pathol. 1999; 23(12):
1561.
40. Dabbs DJ, Carter G, Fudge M, et al. Molecular alterations in
Columnar Cell Lesions
of the breast. Mod Pathol 2006; 19: 344-349.
41. Eusebi V, Feudale E, Foschini MD, Micheli A, Conti A, Riva C et
al; Long term
follow up of in-situ carcinoma of the breast. Semin. Diagn. Pathol.
1994;11: 223-235
42. Boulos FI, Dupont WD, Simpson JF, Schuyler PA, Sanders ME,
Freudenthal ME et
al. Histologic associations & longterm cancer risk in cells of
the breast: a
restrospective cohort and a nested case control study. Breast
cancer. 2008;113:2415-
2421
43. Guerra-Wallace M.M, Christensen W.N, White R.Jr. A
Retrospective study of
columnar alteration with prominent apical snouts and secretions and
the association
with cancer. Am. J. Surg. Pathol. 2004; 188: 395-398.
44. Gary Tse, Puay Hoon Tan, Fernando Schmitt. Fine needle
Aspiration Cytology of the
breast: Atlas of Cytohistopathology Correlates. Springer-Verlag
Berlin Heidelberg
2013. Pg 186.
66
45. Rosemary AW, Andy H, Sarah EP, Jeremy T, Ian OE. Current Issues
in Diagnostic
Breast Pathology. J Clin Pathol. 2012; 65(9): 771-785.
46. Ochicha O, Edino ST, Mohammed AZ, Amin SN. Benign breast
lesions in Kano. Nig
J Surg Res. 2002; 4: 1-5
47. Irabor DO, Okolo CA. An audit of 149 consecutive breast
biopsies in Ibadan Nigeria.
Pak J Med Sci. 2008; 24: 257-62.
48. Olu-Eddo AN, Ugiagbe EE. Benign breast lesions in an African
population: A 25
year histopathological review of 1864 cases. Niger Med J. 2011;52:
211-216.
67
Take sections to distilled water
Antigen retrieval should be done using HIER in citrate buffer and
allow to cool for
20minutes.
Rinse in 2 changes of distilled water
Rinse with the wash buffer (Posphate buffer)
Block using hyprogen peroxide block for 10minutes depending on
manufacturer’s
instruction.
Rinse in two changes of wash buffer
Add a UV block for 5minutes (some manufacturers skip this
step)
Flip off the UV block (do not rinse)
Add the primary antibody (ER, PR, and CK 8, 18 or 19) for about 30
min or 1 hour
depending on manufacturer
Rinse in 2 changes of wash buffer
Add an antibody enhancer (varies depending on the kit being
used)
Rinse in 2 changes of wash buffer
Add the secondary antibody
Add Dab substrate and chromogen mixture for 10 minutes
Rinse in distilled water
Counter-stain in Mayer’s haemalum for 1or 2 minutes