Embed Size (px)
Citation preview

Dr Jonathan KuttnerMusculoskeletal & Pain Specialist
Auckland
14:00 - 16:00 WS #18: Musculoskeletal Medicine 3
Dr Keith LaubscherPain Specialist
Auckland
Dr Ian WallbridgeMusculoskeletal Physician
Rotorua
Practical Pain Management- Interventional for Lumbar and Cervical Spinal Pain
Keith LaubscherAuckland 2018
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Outline
1 Why treat pain? - Pain as a disease
2 Principles: General consideration for IPM
Pain management -general
3 Interventions
- Cervical somatic
- Lumbar somatic
- Lumbar radicular pain
- Cervical radicular
- CRPS
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Why treat pain
Chronic pain prevalence: -New Zealand 16.9% (lasted or expected to last 6 months or more) (Bligh F et al. NZMJ 2011: 124; 1337; 63-76)
Pain related suffering, disability and economic cost to society may be more important than the underlying aetiology
Fine PG. Pain Medicine 2011; 12: 996–1004
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Pain as a disease: Consequences
• Distress – anxiety, depression
• Disability
• Destitute
• Drugged:
• Dementia – cognitive impairment
• Death
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
“Thus, it is important to effectively manage pain in its early stages before it progresses to further affect patients’ function.”
Fine, Perry G. "Long‐Term Consequences of Chronic Pain: Mounting Evidence for Pain as a Neurological Disease and Parallels with Other Chronic Disease States." Pain medicine 12, no. 7 (2011): 996-1004
“it is axiomatic that pain can be safely treated as a symptom only when the underlying cause is known and when all treatment directed towards this has been completed”
The Pain Clinic: A clinic for the management of intractable pain: McEwen B, de Wilde F, Dwyer B: MJA : 8thMay 1965: 1: 676-682
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

General considerations in interventional pain management
1 Clinical diagnosis (and red flags)
2 Pain duration: acute vs chronic
3 Type of pain: “mechanistic pain classification”(Central sensitisation vs Chronic pain)
4 Treatment options: Individualized management(Psycho-physical; Pharmacological; Interventional; Surgery)
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
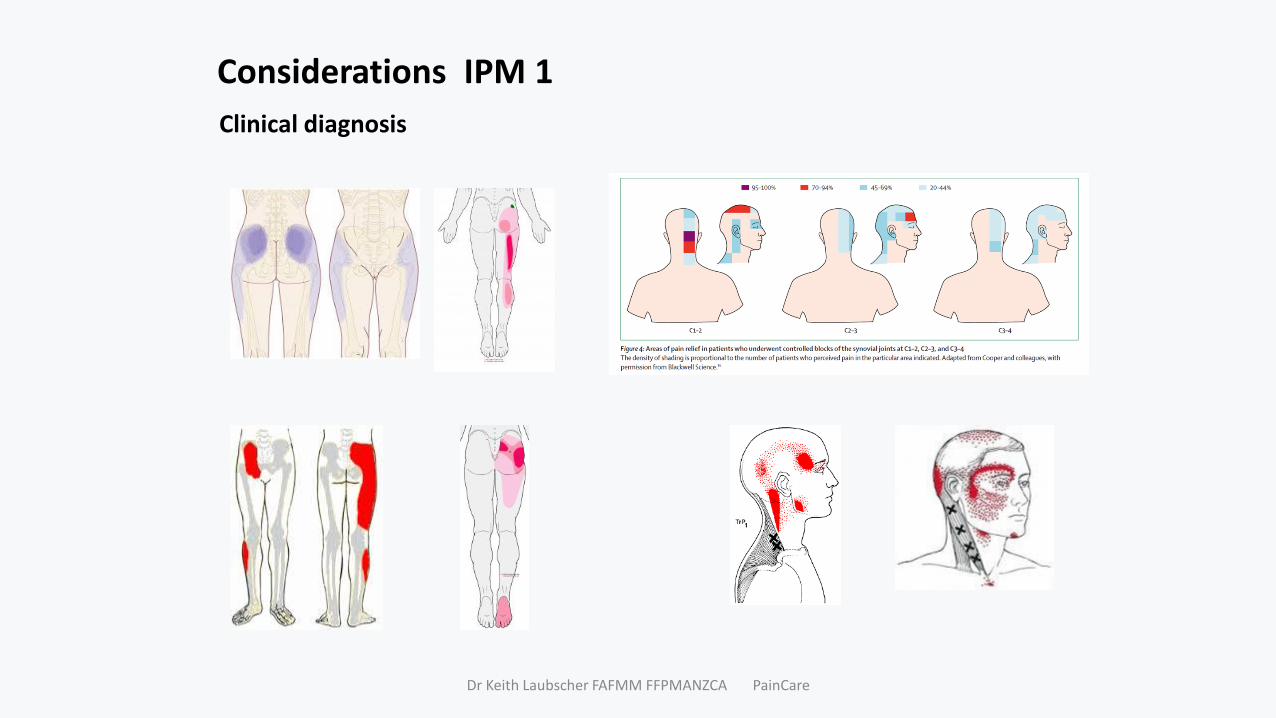
Considerations IPM 1
Clinical diagnosis
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
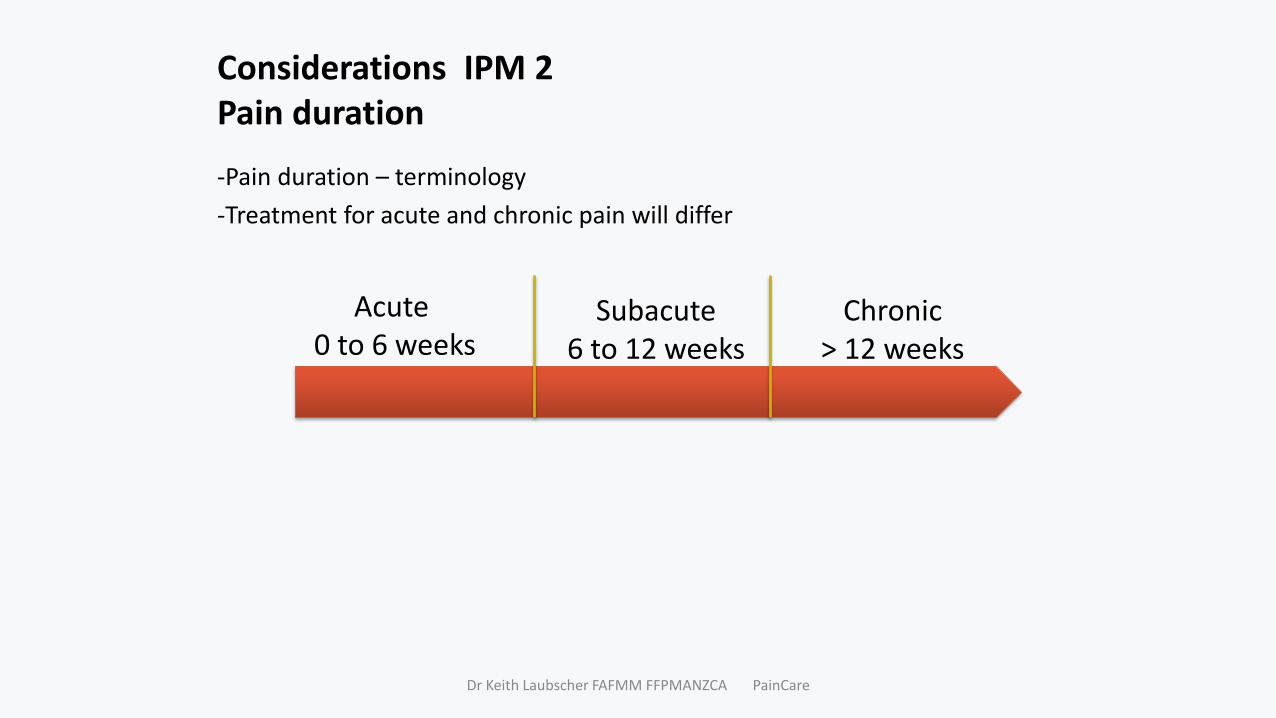
Considerations IPM 2Pain duration
-Pain duration – terminology
-Treatment for acute and chronic pain will differ
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Acute 0 to 6 weeks
Subacute6 to 12 weeks
Chronic> 12 weeks
Considerations IPM 3Mechanistic classification of pain
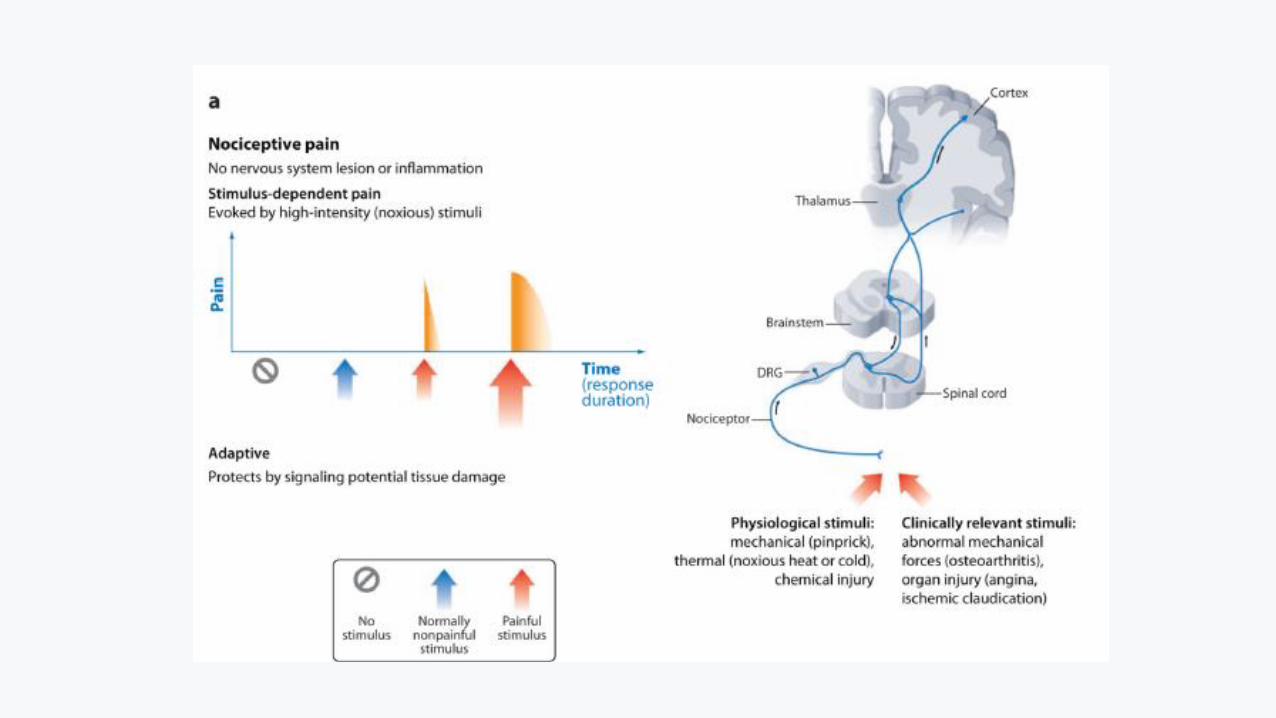
• Nociceptive – somatic, somatic referred, visceral
• Neuropathic (nerve damage)
– Peripheral eg radicular
– Central eg cauda equina, myelopathy
• Neuroplastic pain/Dysfunctional pain
(“Central sensitisation”/“Pain syndrome”/“Pain disorder” (????)
• Mixed
So what about?
• Myofascial pain = pain, tender/trigger points, referral, ROM, weakness
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
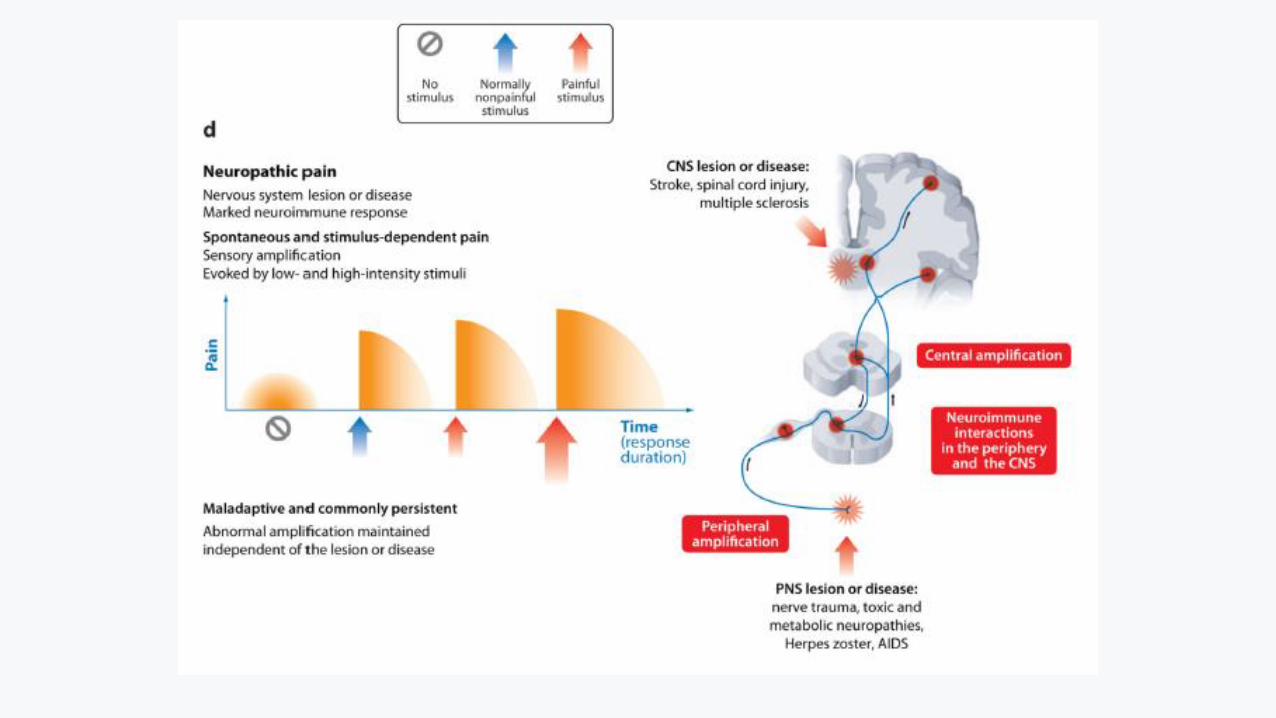
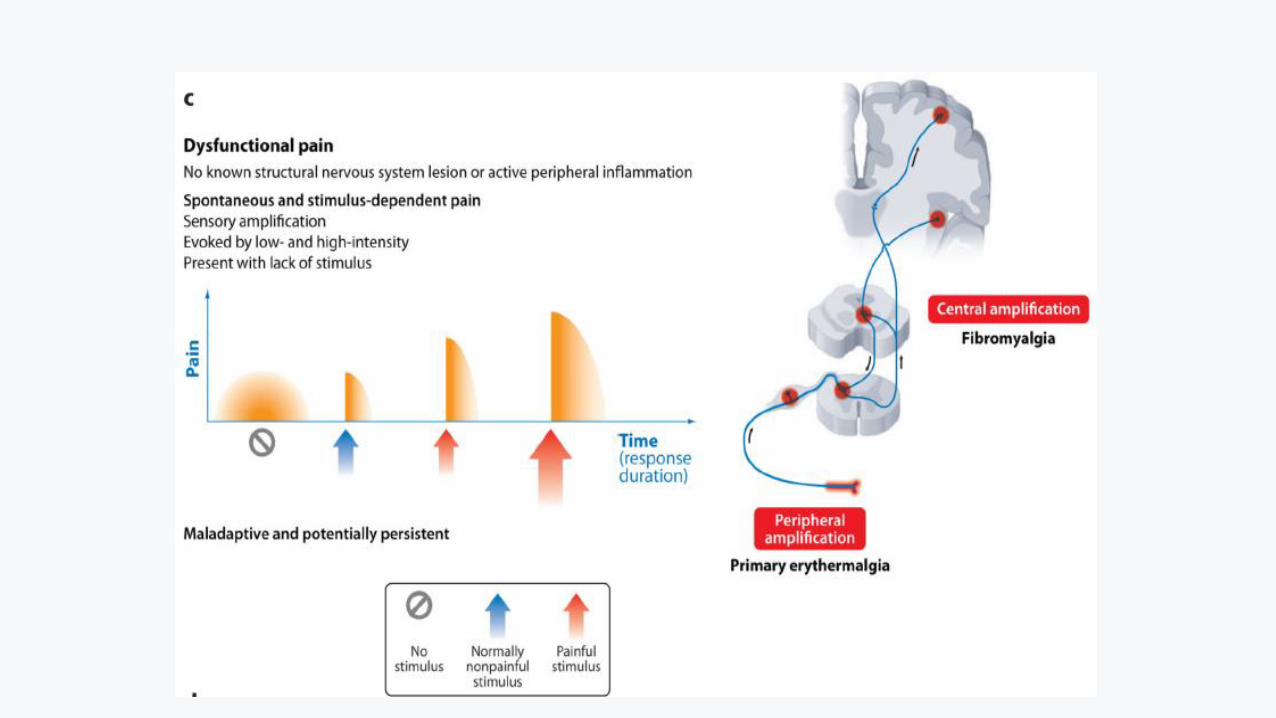
Considerations IPM 3aNeuroplastic pain, pain syndromes, sensitisation and chronic pain
Mismatch conundrum
Pain vs pathology and “pain syndromes”
• IBS, FMS, OA, “CLBP”, “WAD”
Central sensitisation: A physiological phenomenon and not a diagnosis(Any sensory experience greater in amplitude, duration and spatial extent than that would be expected from a defined peripheral input under normal circumstances qualifies as potentially reflecting a central amplification due to increased excitation or reduced inhibition. These changes could include a reduction in threshold, exaggerated response to a noxious stimulus, pain after the end of a stimulus, and a spread of sensitivity to normal tissue)C Woolf.Pain 152 (2011) S2-S15
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Sensitization*Increased responsiveness of nociceptive neurons to their normal input, and/or recruitment of a response to normally subthreshold inputs.• …..neurophysiological term ; may only be inferred indirectly from
phenomena such as hyperalgesia or allodynia.
Central sensitization*Increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input.• include increased responsiveness due to dysfunction of endogenous
pain control systems.
Peripheral sensitization*Increased responsiveness and reduced threshold of nociceptive neurons in the periphery to the stimulation of their receptive fields.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Central Sensitisation- bedside recognition
• No agreed diagnostic criteria
Clinical features:• History -neurological descriptors
Examination - ↓ threshold, ↑ response, ↑extent ↑duration • Sensory: dynamic allodynia ; secondary punctate hyperalgesia or pressure
hyperalgesia; cold allodynia• Regional and remote hyperalgesia • Temporal summation and after sensations• (Non-dermatomal sensory deficits)
CS as a component of wider syndrome:• Multisystem sensitivities • Nonspecific symptoms: fatigue, sleep, cognitive difficulties
Experimental laboratory: not today
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Differential diagnosis of widespread pain.
• Connective tissue: SLE, Sjogren’s syndrome
• Inflammatory:
• Malignancy: myeloma, leukaemia, paraneoplastic
• Neurological: multiple sclerosis, neuropathy
• Muscle: myelopathy,
• Endocrine/Metabolic : Hypo and hyperthyroid, Diabetes, Hyperparathyroid, Acromegaly
• Infection: Hepatitis B/ C, Lyme disease
• Drugs: statins, (opioids)
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Treating the cause and central sensitisationRFN for Cervical zygapophysial joint pain
• 53 patients WAD grade 2
• Standardise measures pre and post RFN
• Improvements in pain, disability, local and widespread hyperalgesia , NFR threshold, and brachial plexus provocation test responses, and ROM (all P < 0.0001).
• Changes were early within 1 month, and sustained at 3 months
Smith, Ashley Dean, et al. "Cervical radiofrequency neurotomy reduces central hyperexcitability and improves neck movement in individuals with chronic whiplash." Pain Medicine 15.1 (2014): 128-141.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Sensitisation managementEffective treatment – when possible
• Kosek E, Ordeberg G. Abnormalities of somatosensory perception in patients with painful osteoarthritis normalize following successful treatment. Eur J Pain 2000;4(3):229–38
• Graven-Nielsen T, Wodehouse T, Langford RM, Arendt-Nielsen L, Kidd BL. Normalization of widespread hyperesthesia and facilitated spatial summation of deep-tissue pain in knee osteoarthritis patients after knee replacement. Arthritis Rheum 2012; 64(9):2907–16
• Aranda‐Villalobos, Pilar, et al. "Normalization of widespread pressure pain hypersensitivity after total hip replacement in patients with hip osteoarthritis is associated with clinical and functional improvements." Arthritis & Rheumatism65.5 (2013): 1262-1270.
• Seminowicz DA, Wideman TH, Naso L, et al. Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function. J Neurosci 2011;31(20):7540–50.
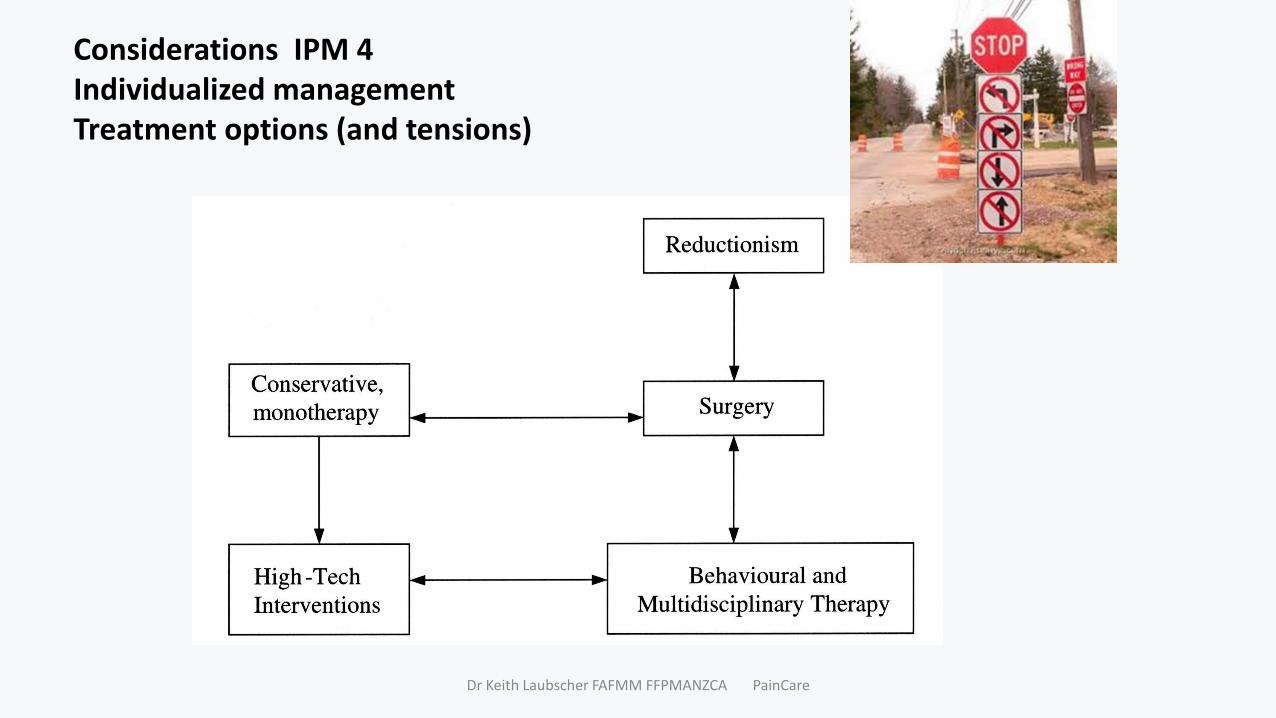
Considerations IPM 4Individualized managementTreatment options (and tensions)
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
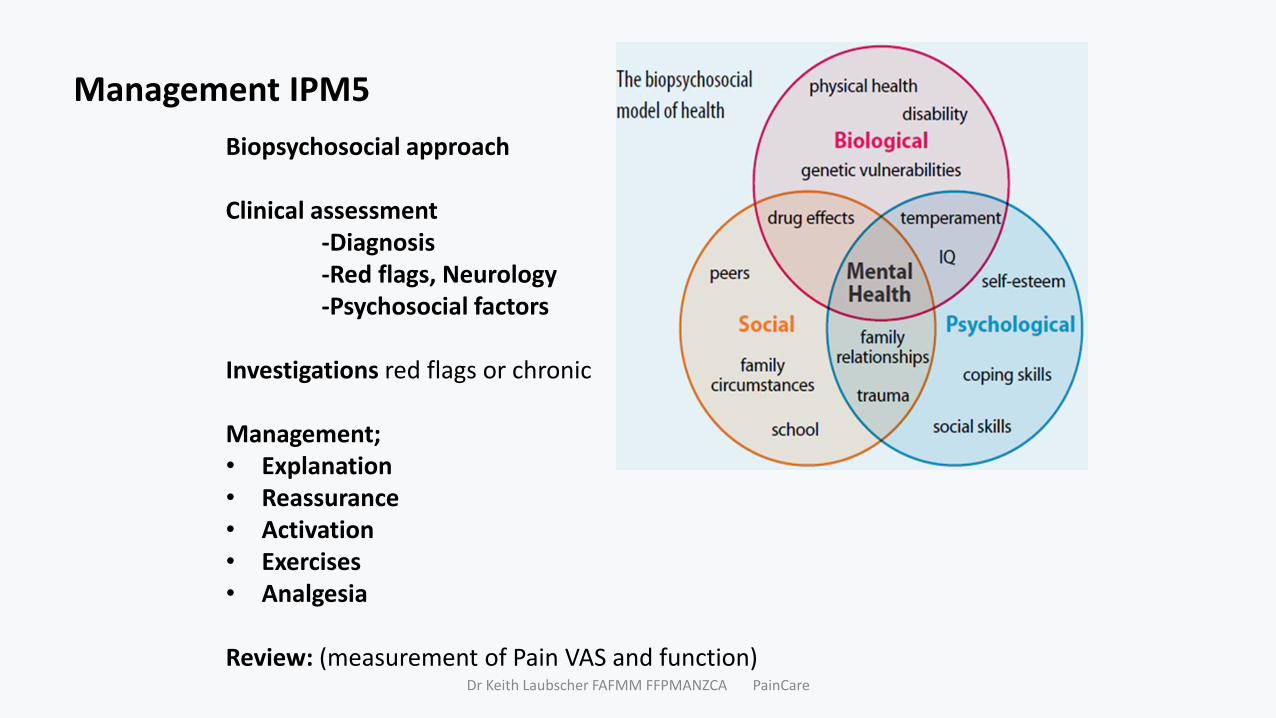
Management IPM5
Biopsychosocial approach
Clinical assessment-Diagnosis-Red flags, Neurology-Psychosocial factors
Investigations red flags or chronic
Management;• Explanation• Reassurance• Activation• Exercises• Analgesia
Review: (measurement of Pain VAS and function)Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Pain management 1The Indahl Approach (Indahl, Spine, 1995)
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
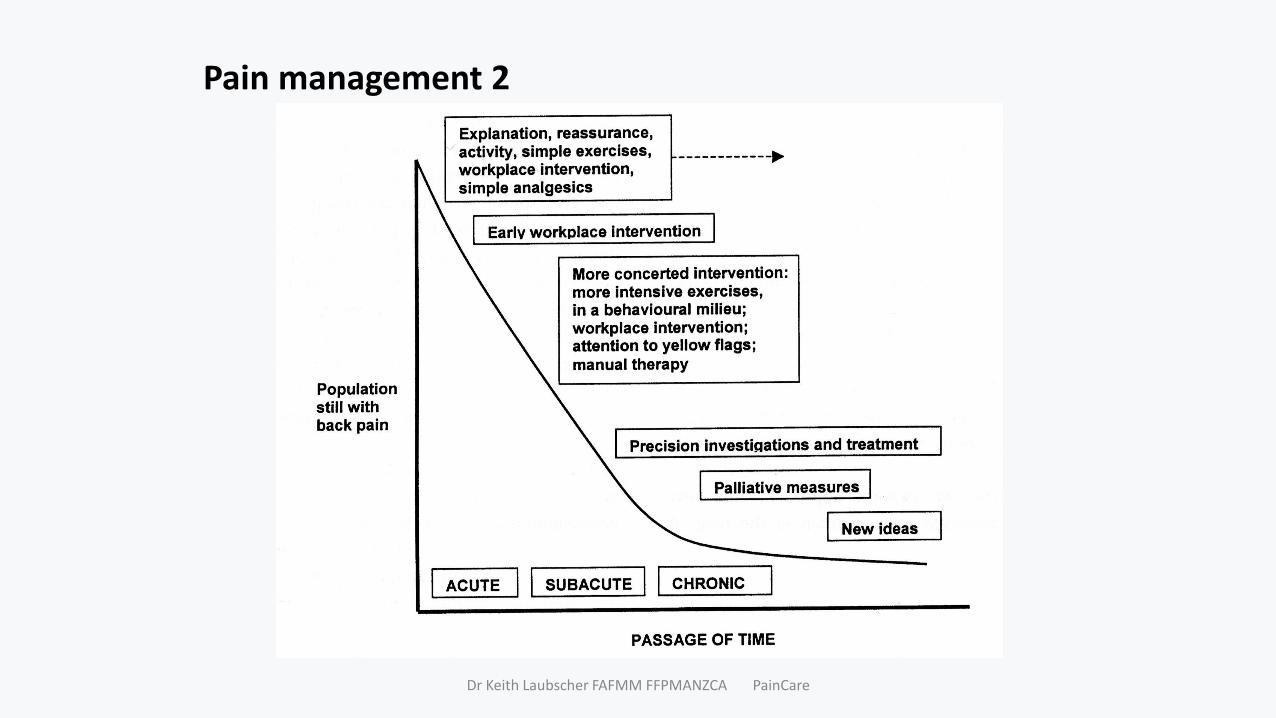
Pain management 2
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Pain management 3Medication
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
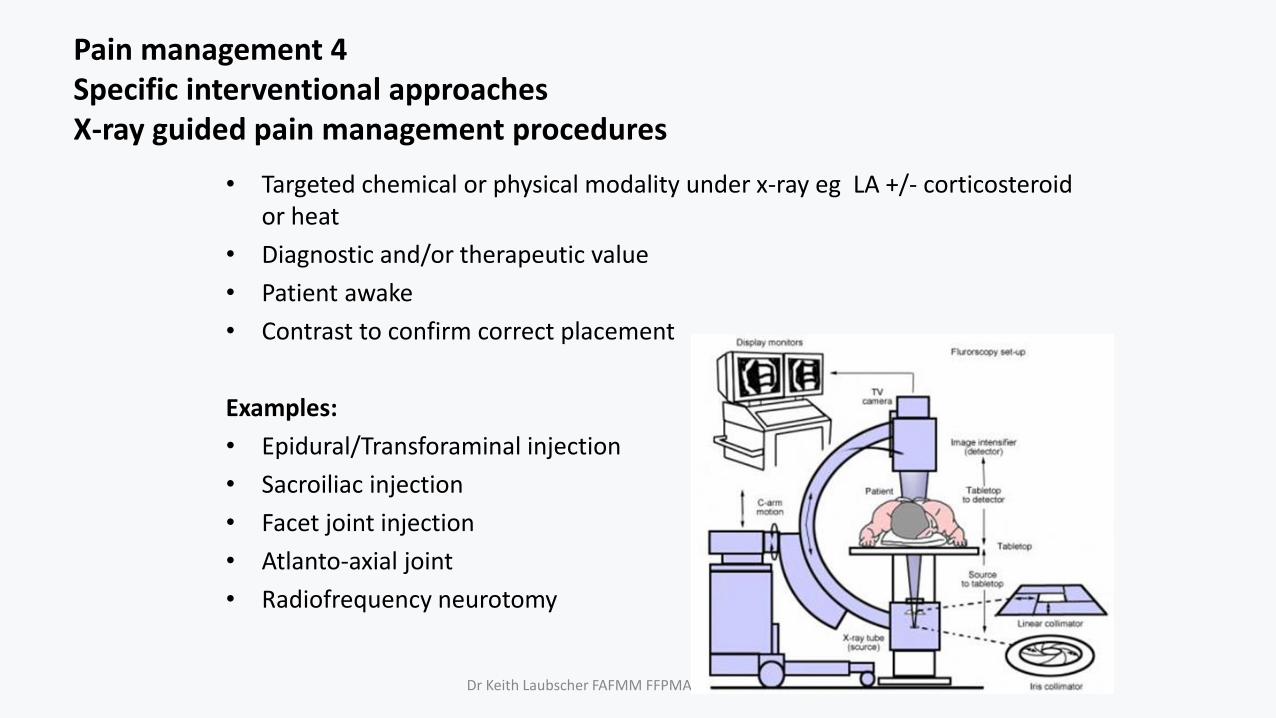
Pain management 4 Specific interventional approachesX-ray guided pain management procedures
• Targeted chemical or physical modality under x-ray eg LA +/- corticosteroid or heat
• Diagnostic and/or therapeutic value
• Patient awake
• Contrast to confirm correct placement
Examples:
• Epidural/Transforaminal injection
• Sacroiliac injection
• Facet joint injection
• Atlanto-axial joint
• Radiofrequency neurotomy
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Pain management 4 Surgery
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare
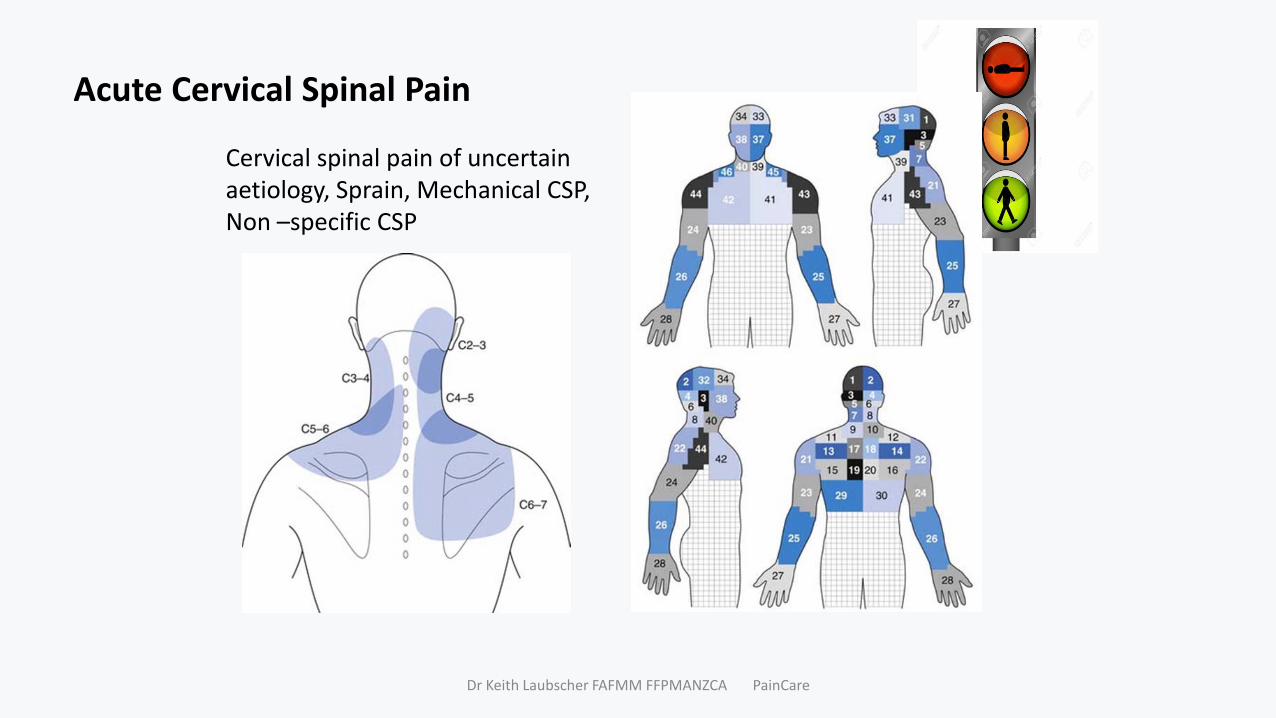
Acute Cervical Spinal Pain
Cervical spinal pain of uncertain aetiology, Sprain, Mechanical CSP, Non –specific CSP
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Acute Cervical Spinal Pain
Cervical spinal pain of uncertain aetiology, Sprain, Mechanical CSP, Non –specific CSP
Assessment: • Red flags• Yellow flags
Management:
Conservative• BSP - “Indahl”• Physical therapy• Symptom relief; Adequate analgesia
incl opiate +-co-analgesics eg TCA, spasm
• Reassess
Refer - red flags
Refer specialist• If no improvement 6 weeks or
unrelieved pain– x-ray, “screening” bloods– MRI (?)
• Intervention= ESI (various routes)• Surgery
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Vilfredo Pareto5 July 1848 – 19 August 1923)
Chronic Cervical Spinal PainEpidemiology: Incidence 15- 40%Clinical: Neck +/- shoulder 2/3, headache 1/3Common• Whiplash associated neck pain
(80% better at 12 months)• Cervical spinal pain of uncertain aetiology,
Sprain, Mechanical CSP, Non –specific CSP
Uncommon• Fracture, Tumour, Infection• Arthropathies - Spondylosis (80% age 50)• Aneurysms• Neurological • Referred visceral: anterior neck (oesophagus,
pharynx), angina; shoulder, headache disorder, systemic (eg FM)
• Neurological deficit myelopathy, radiculopathyDr Keith Laubscher FAFMM FFPMANZCA PainCare
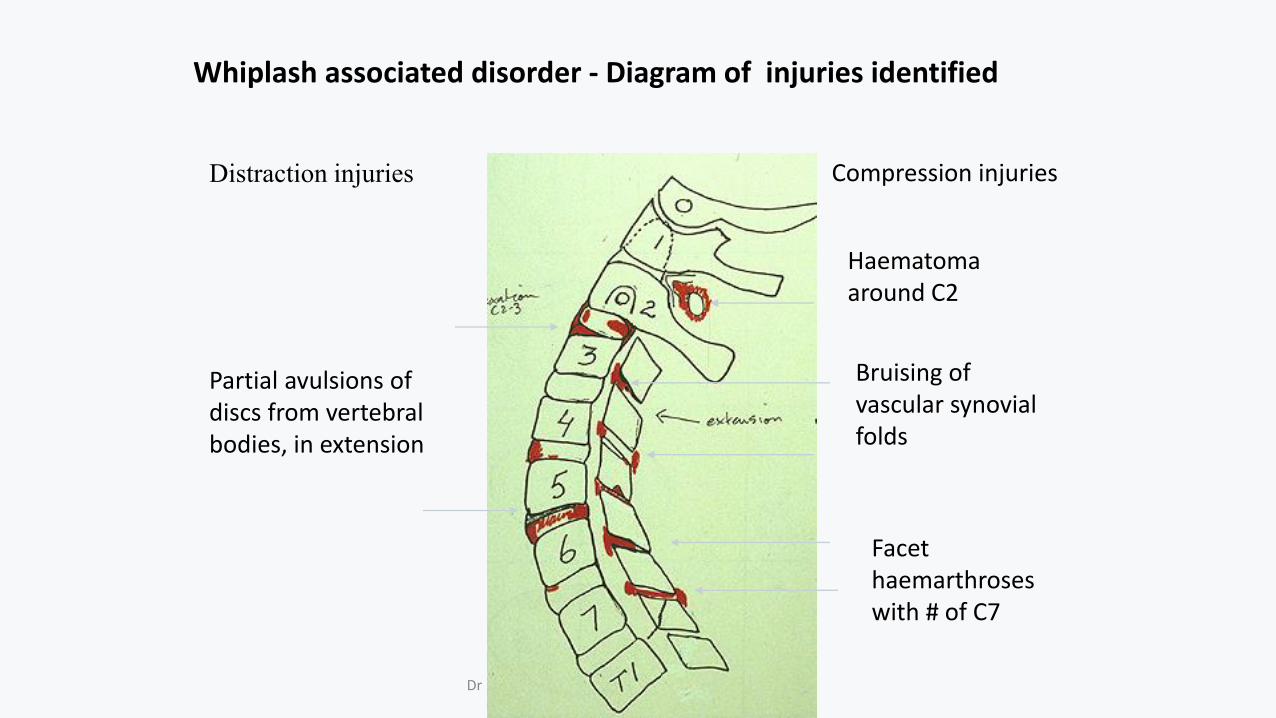
Whiplash associated disorder - Diagram of injuries identified
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Partial avulsions of discs from vertebral bodies, in extension
Facet haemarthroseswith # of C7
Bruising of vascular synovial folds
Haematoma around C2
Distraction injuries Compression injuries
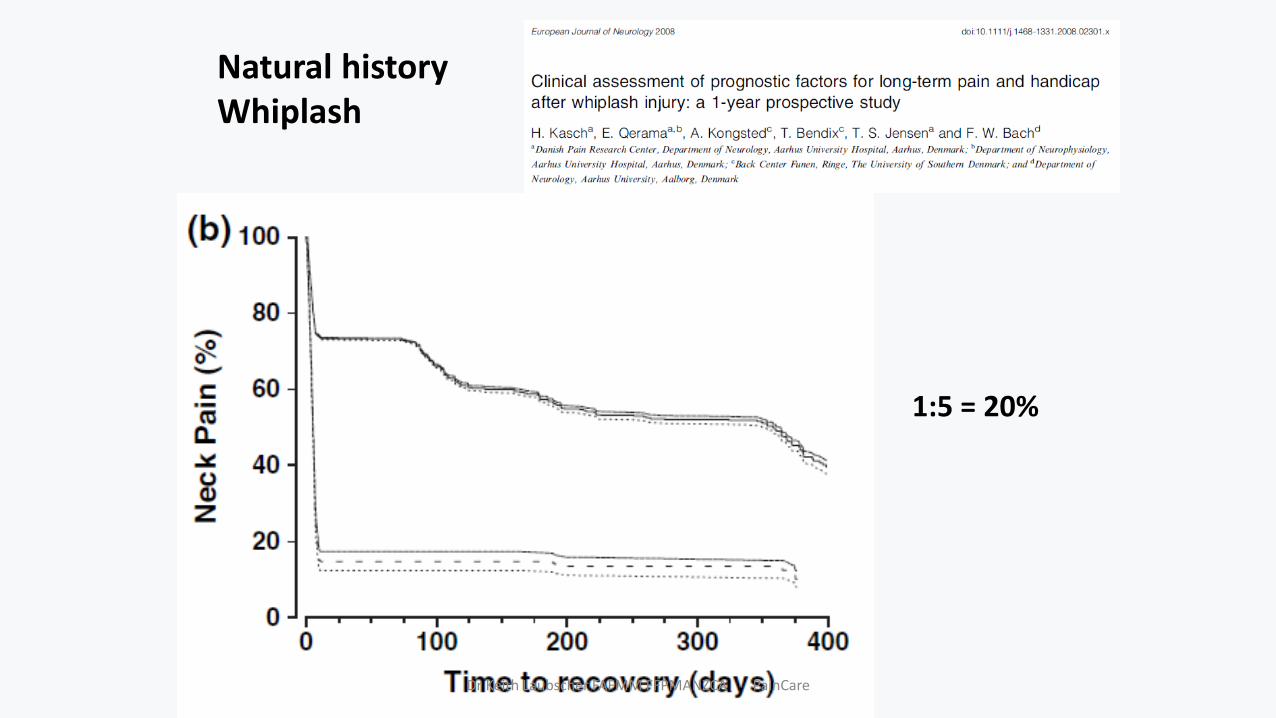
Natural historyWhiplash
1:5 = 20%
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
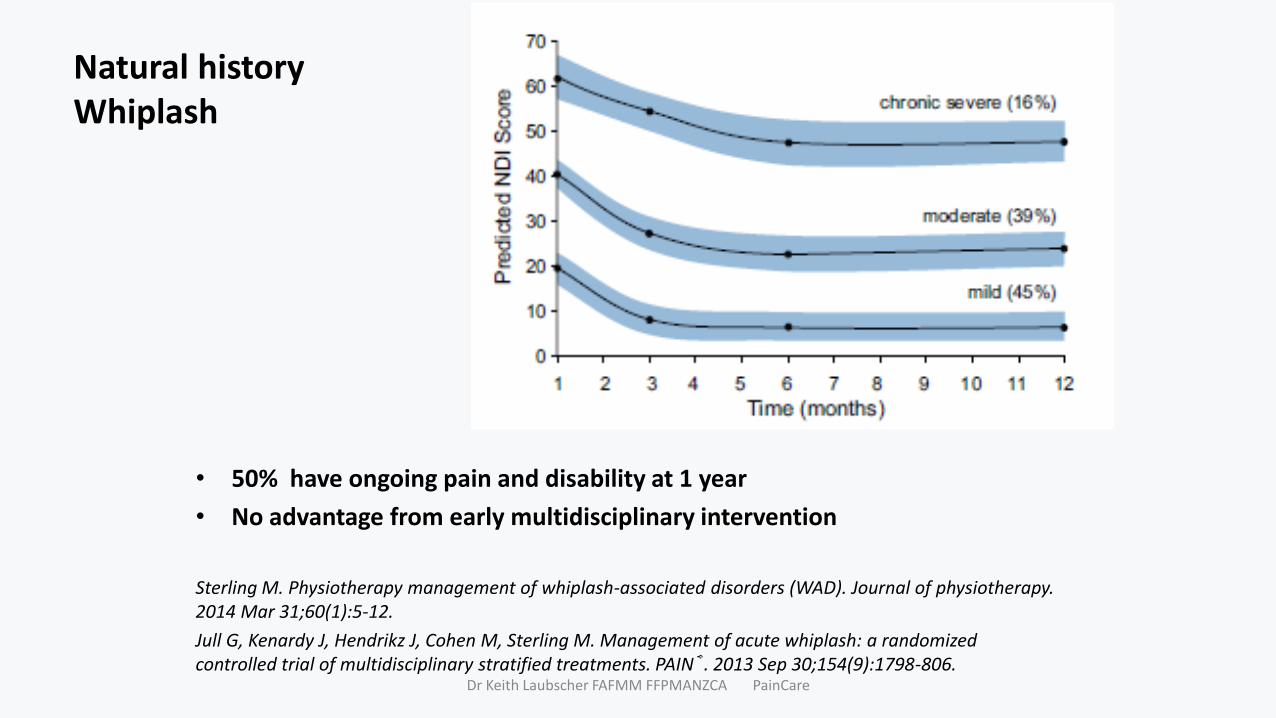
Natural historyWhiplash
• 50% have ongoing pain and disability at 1 year
• No advantage from early multidisciplinary intervention
Sterling M. Physiotherapy management of whiplash-associated disorders (WAD). Journal of physiotherapy. 2014 Mar 31;60(1):5-12.
Jull G, Kenardy J, Hendrikz J, Cohen M, Sterling M. Management of acute whiplash: a randomized controlled trial of multidisciplinary stratified treatments. PAIN®. 2013 Sep 30;154(9):1798-806.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
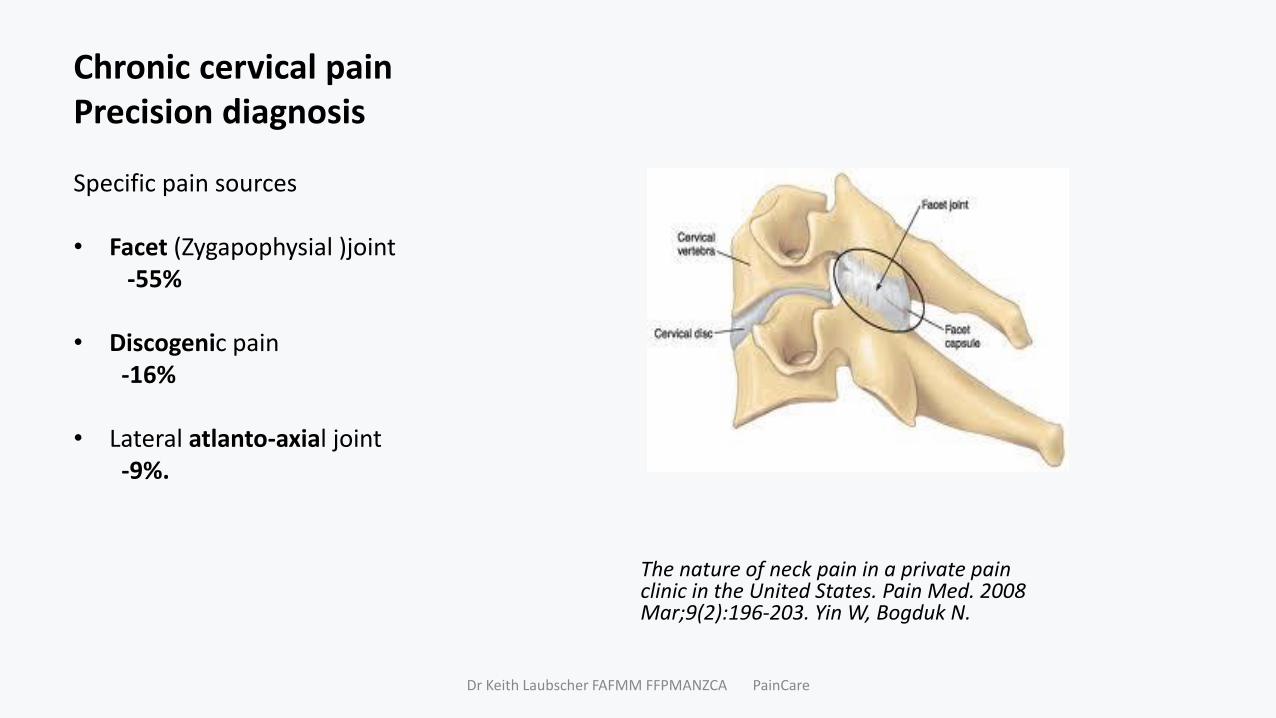
Chronic cervical painPrecision diagnosis
Specific pain sources
• Facet (Zygapophysial )joint -55%
• Discogenic pain -16%
• Lateral atlanto-axial joint -9%.
The nature of neck pain in a private pain clinic in the United States. Pain Med. 2008 Mar;9(2):196-203. Yin W, Bogduk N.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
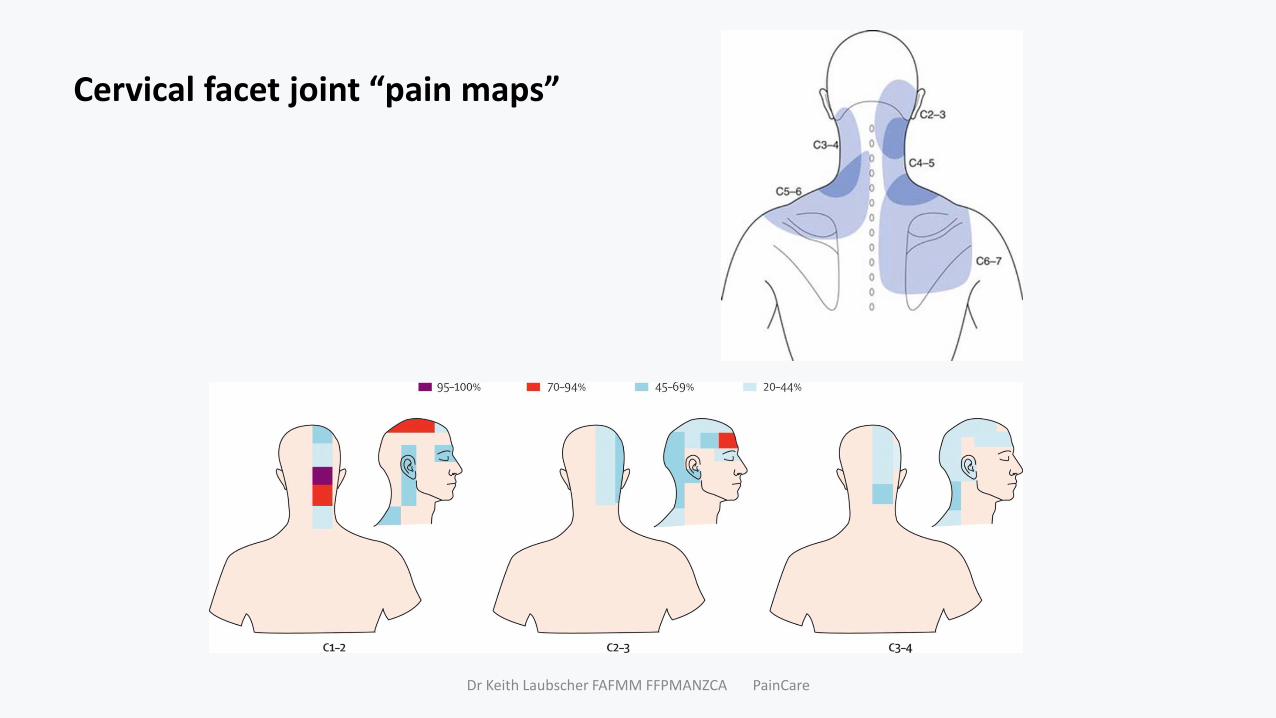
Cervical facet joint “pain maps”
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
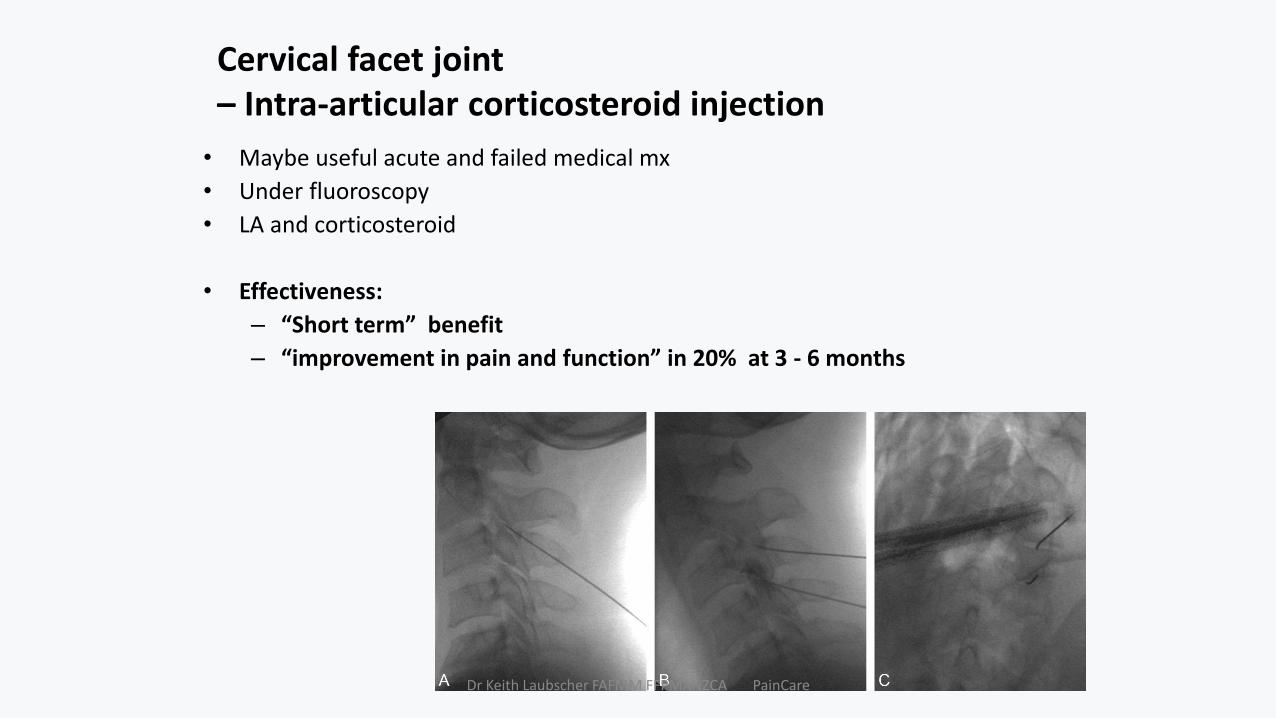
Cervical facet joint – Intra-articular corticosteroid injection
• Maybe useful acute and failed medical mx
• Under fluoroscopy
• LA and corticosteroid
• Effectiveness:
– “Short term” benefit
– “improvement in pain and function” in 20% at 3 - 6 months
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
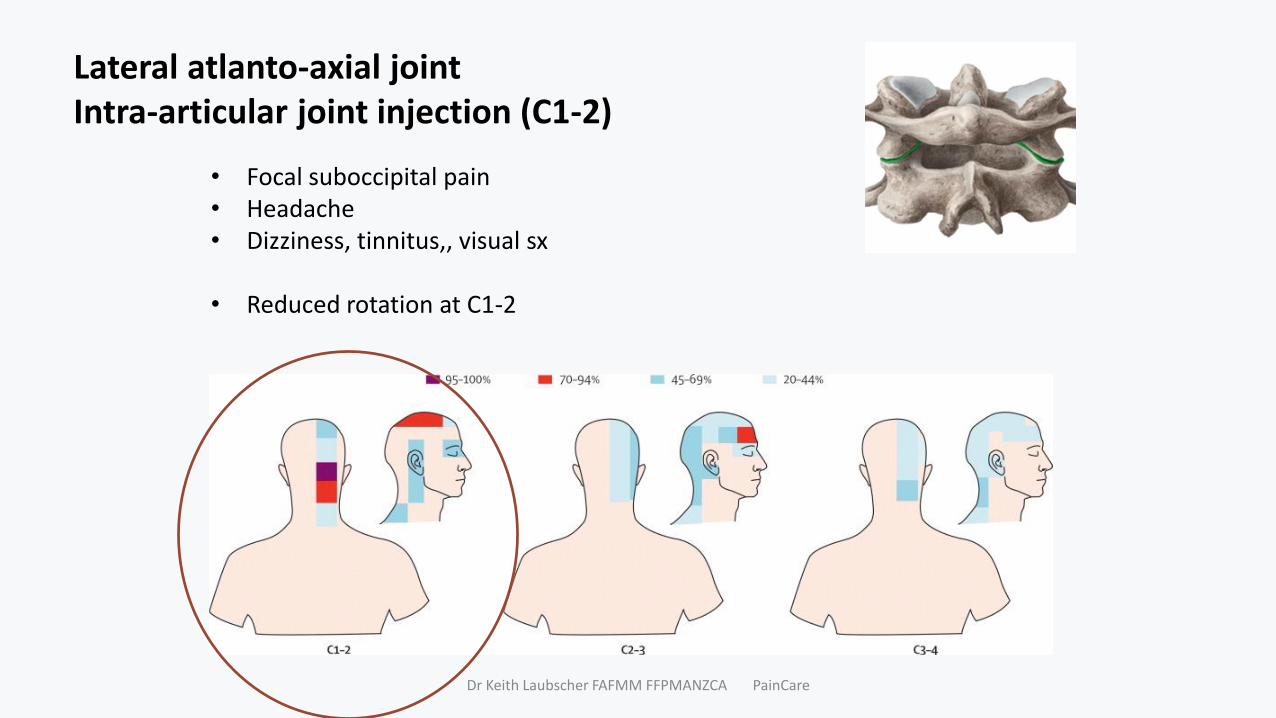
Lateral atlanto-axial jointIntra-articular joint injection (C1-2)
• Focal suboccipital pain • Headache• Dizziness, tinnitus,, visual sx
• Reduced rotation at C1-2
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
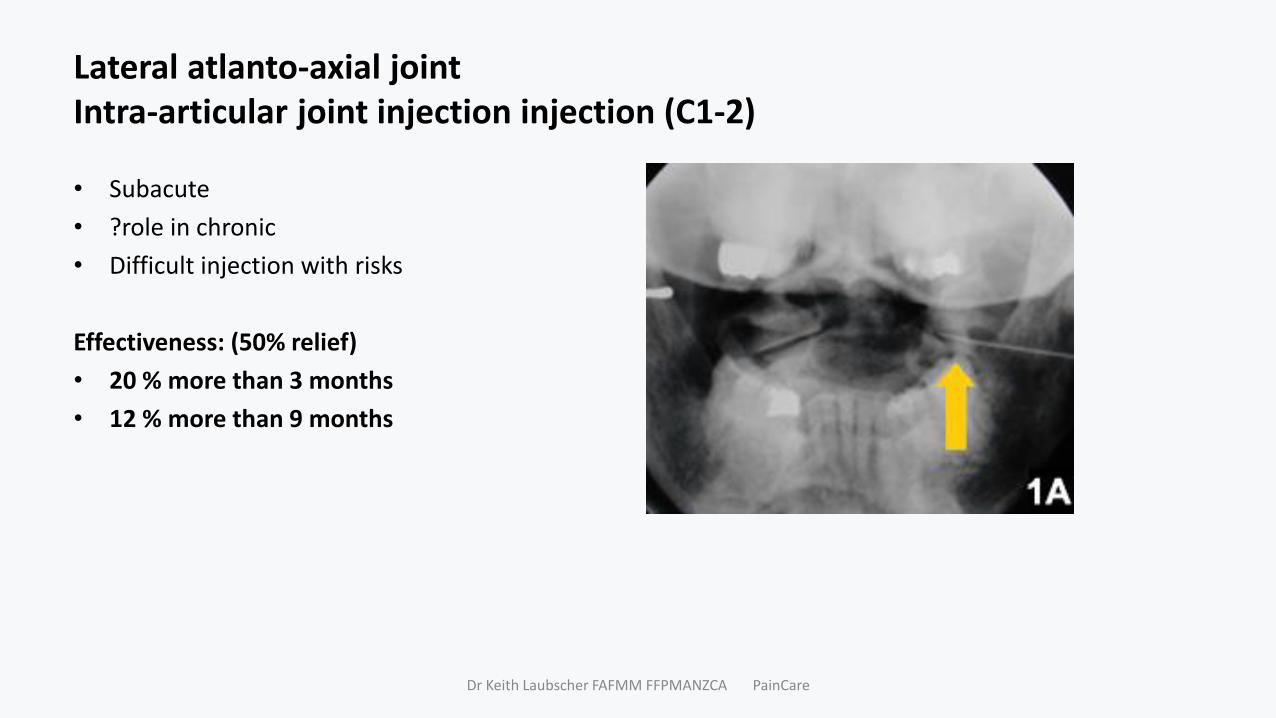
Lateral atlanto-axial jointIntra-articular joint injection injection (C1-2)
• Subacute
• ?role in chronic
• Difficult injection with risks
Effectiveness: (50% relief)
• 20 % more than 3 months
• 12 % more than 9 months
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
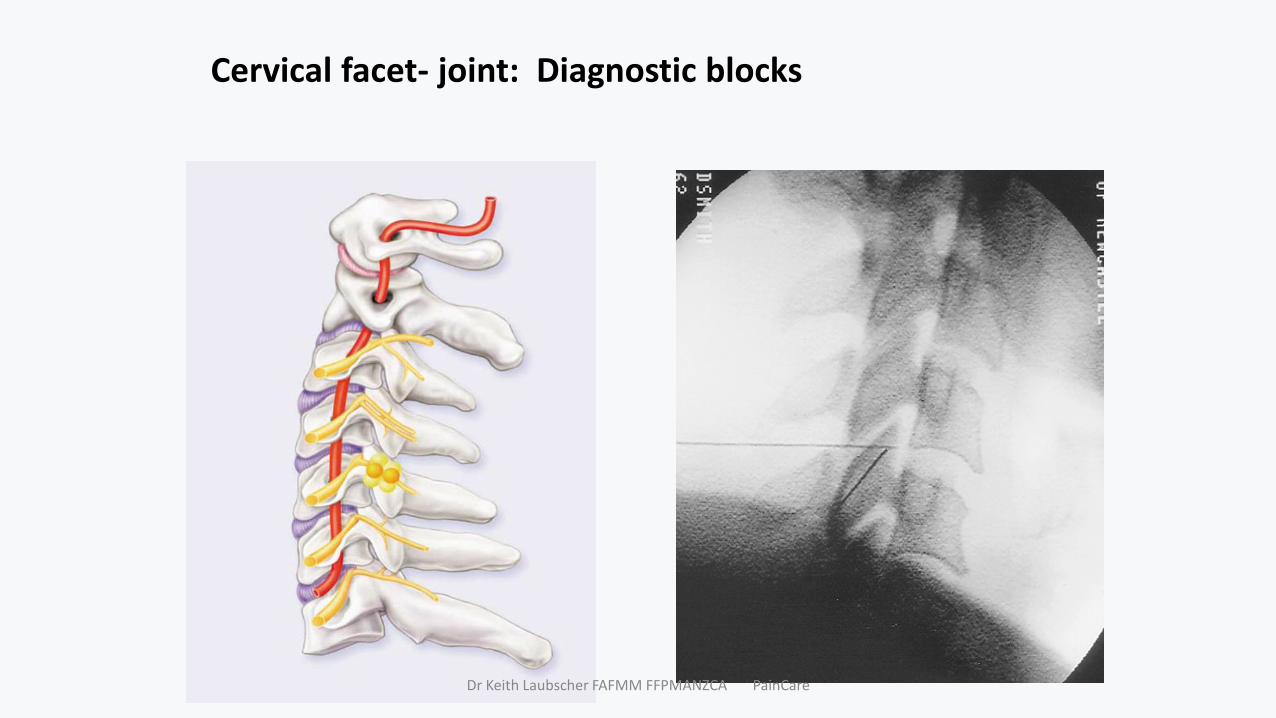
Cervical facet- joint: Diagnostic blocks
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Cervical facet joint
• Facet joint single most common focus – axial pain
• Somatic /referred pain pattern
• No specific clinical or radiological feature
• Easily tested - controlled double blind local anaesthetic nerve block (MBB)
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Facet joint Nerve blocks and radiofrequency neurotomy
PRECISION DIAGNOSIS
Diagnostic Nerve Block
Target specific under x-ray
Volume 0.3 ml – 0.5 ml
Spread limited
Controlled: double blind comparative local anaesthetic or placebo controlled
Sensitivity 54; Specificity 88
Reliable 85% (ie 15 % positive also respond to placebo
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
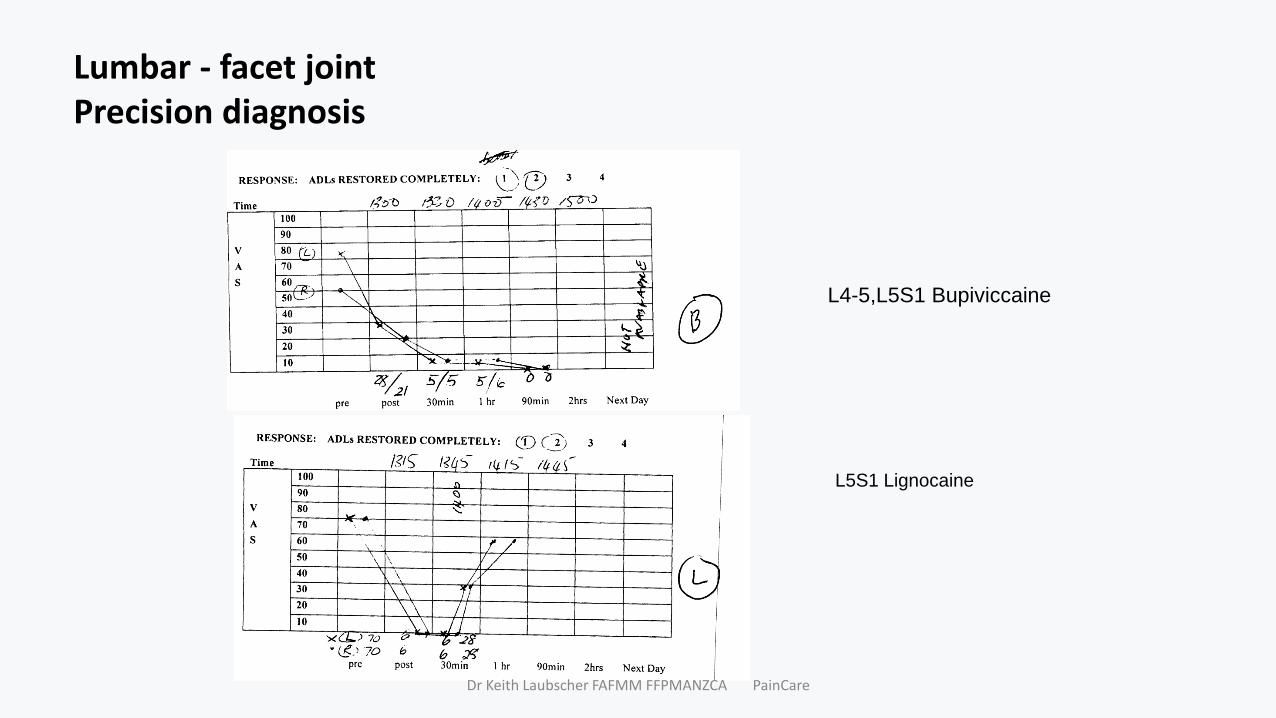
Lumbar - facet jointPrecision diagnosis
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
L5S1 Lignocaine
L4-5,L5S1 Bupiviccaine

Cervical radiofrequency neurotomy
Technical
• Heating course of nerve to joint
• Under fluoroscopy
• Local anaesthetic
• Specific electrode
• 80 -850 C 2 – 6 lesions 90 sec each
• 1-2 hours
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Cervical RFNEffectiveness
104 patients, 5 -300 monthsPositive MBB
Result 68% patients achieved a successful outcome.Relief median 20-26 months, 60% still relief at follow-up.
Successful: Complete relief > 6 months, Complete restoration of ADLNo need further health careReturn to work. Failed to meet any of these criteria = failed treatment.
MacVicar, J., Borowczyk, J. M., MacVicar, A. M., Loughnan, B. M., & Bogduk, N. (2012). Cervical medial branch radiofrequency neurotomy in New Zealand. Pain medicine, 13(5), 647-654.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Acute lumbar spinal pain
Acute lumbar spinal pain of uncertain aetiology, Sprain, Mechanical CSP, Non –specific CSP
• Common; mostly somatic • Variable course and recovery• Precise diagnosis often not
possible, nor needed• Serious causes are rare; excluded
with careful history & examination
Assessment: • Red flags• Yellow flags
Management: Conservative• BSP - Indahl• Physical therapy• Symptom relief; Adequate analgesia
+-co-analgesics eg TCA, spasm• Reassess
Refer - red flags
Refer specialist assessment:• If no improvement 4-6 weeks or
unrelieved pain– x-ray, “screening” bloods– MRI (?)
• Intervention= ESI (various routes)• Surgery
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Chronic lumbosacral spinal pain “Chronic /persistent low back pain”
Was acute at one stage
At 12 months: 1/3 not fully recoveredHenschke BMJ 2008
At 12 months -75% not fully recovered-90% stopped consultingCroft BMJ 1998
Some 14% are highly disabled.Von Korff, 1993
2 month status predicts the 12 month statusKlennerman, 1995
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Vilfredo Pareto5 July 1848 – 19 August 1923)
Chronic lumbosacral spinal pain “Chronic low back pain”
Epidemiology: Incidence 36 -72%Disabling in 10%
Common• Lumbar spinal pain of uncertain aetiology,
Mechanical LBP, Non –specific LBP
Uncommon• Fracture, Tumour, Infection• Arthropathy - Spondylosis (80% age 50)• Vascular• Neurological
• Referred visceral: Urogenital, AAA, GIT, Pancreas, systemic (eg FM)
• Neurological deficit cauda equina, radiculopathy
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Chronic lumbosacral spinal pain ”Reductionist approach to management
Validated sources of CLBP:
intervertebral disc –• prevalence 40%
zygapophysial (facet) joint)10 -15% younger injured workers; 40% older non-injured population
Sacroiliac joints15 -20%
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
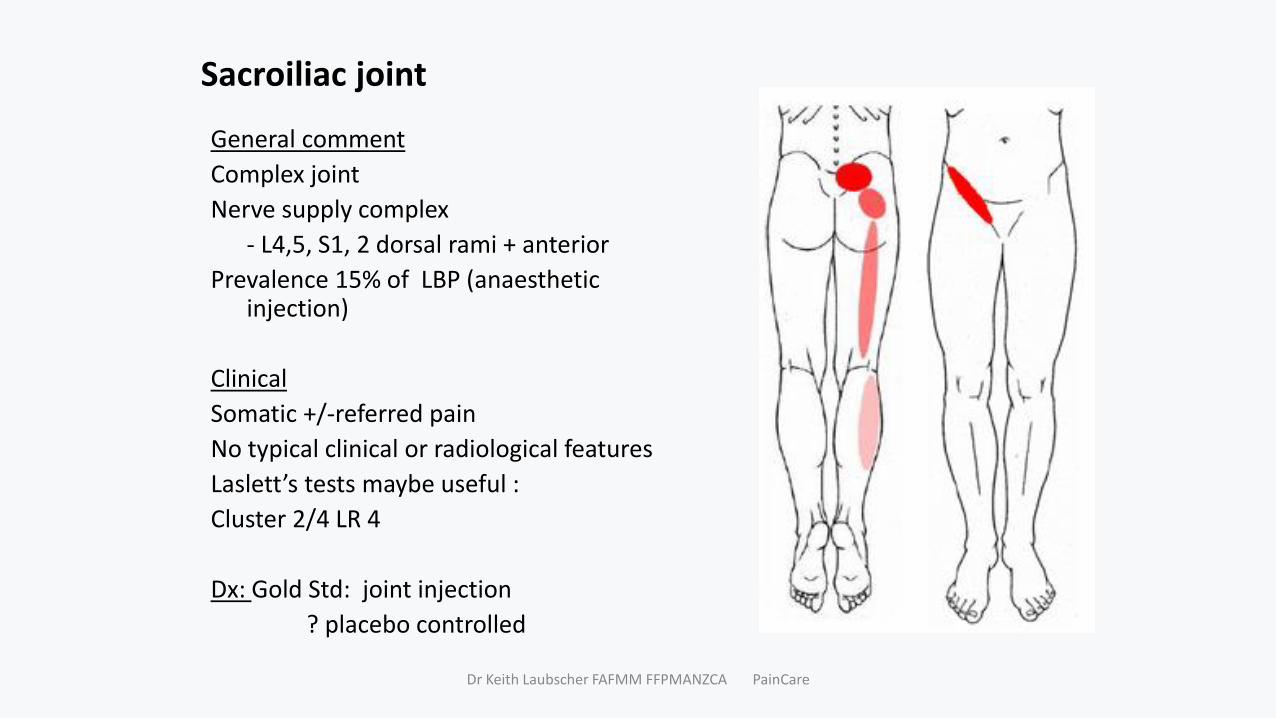
Sacroiliac joint
General comment
Complex joint
Nerve supply complex
- L4,5, S1, 2 dorsal rami + anterior
Prevalence 15% of LBP (anaestheticinjection)
Clinical
Somatic +/-referred pain
No typical clinical or radiological features
Laslett’s tests maybe useful :
Cluster 2/4 LR 4
Dx: Gold Std: joint injection
? placebo controlled
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Sacroiliac joint injection - utility
Therapeutic efficacy50% relief in 60 % , 4 –6 weeks
Indication: Persistent sacroiliac region pain
Diagnostic:Medico-legalSurgical planning (positive + negative result useful)
New treatmentsPercutaneous radiofrequency neurotomy ?? More studies needed…….
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Facet (Zygapophysial) Joint Pain
Incidence 15-40%
Clinical • Somatic +/- referred pain
• Considerable overlapping patterns
• No single specific feature on clinical examination,
• Revells tests -conflicting
• No specific features MRI, CT scan, Bone scan(?)
• Gold Std: nerve block
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Lehman, American Journal of Neuroradiology 35.3 (2014)

Dr Keith Laubscher FAFMM FFPMANZCA PainCare
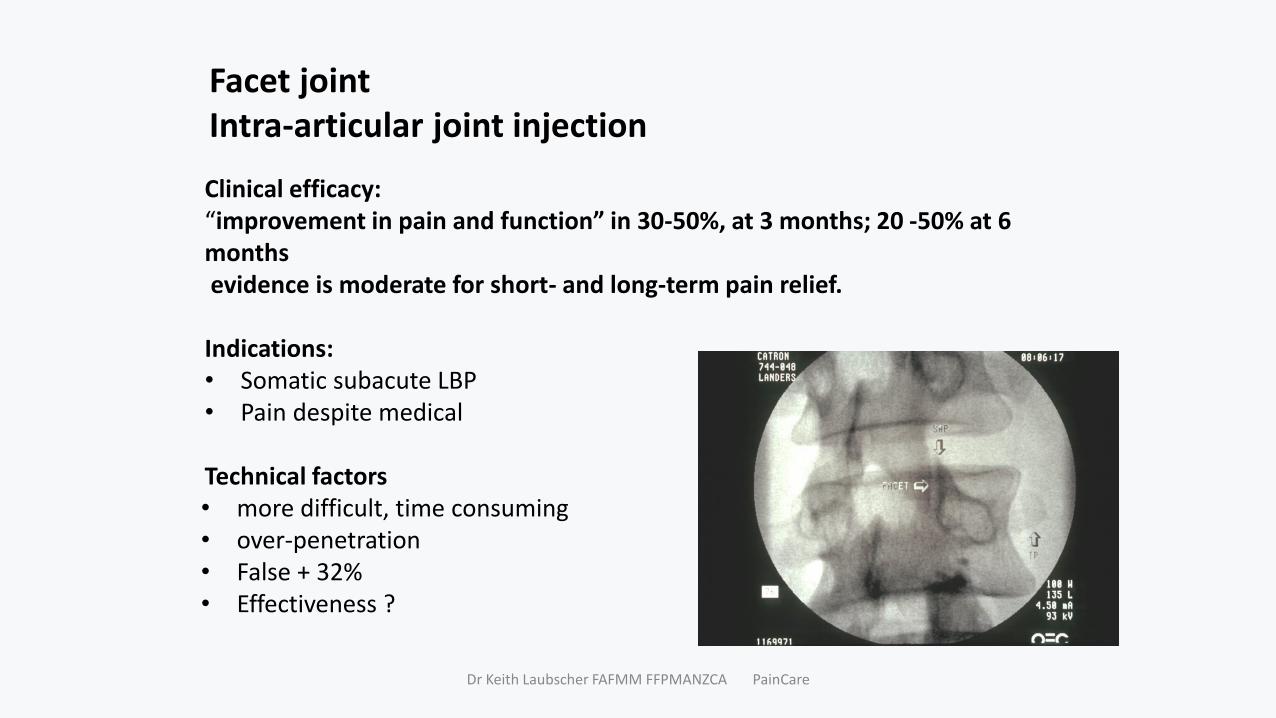
Facet joint Intra-articular joint injection
Clinical efficacy:“improvement in pain and function” in 30-50%, at 3 months; 20 -50% at 6 monthsevidence is moderate for short- and long-term pain relief.
Indications: • Somatic subacute LBP • Pain despite medical
Technical factors • more difficult, time consuming• over-penetration• False + 32%• Effectiveness ?
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
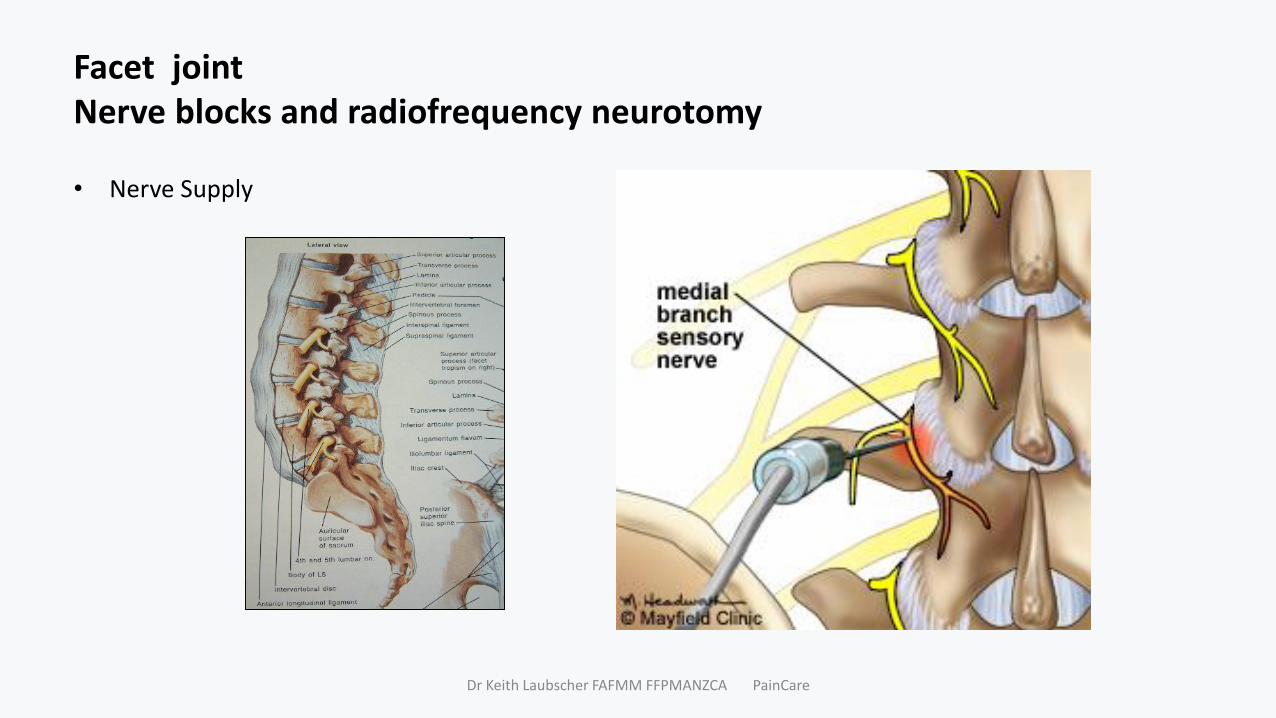
Facet joint Nerve blocks and radiofrequency neurotomy
• Nerve Supply
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
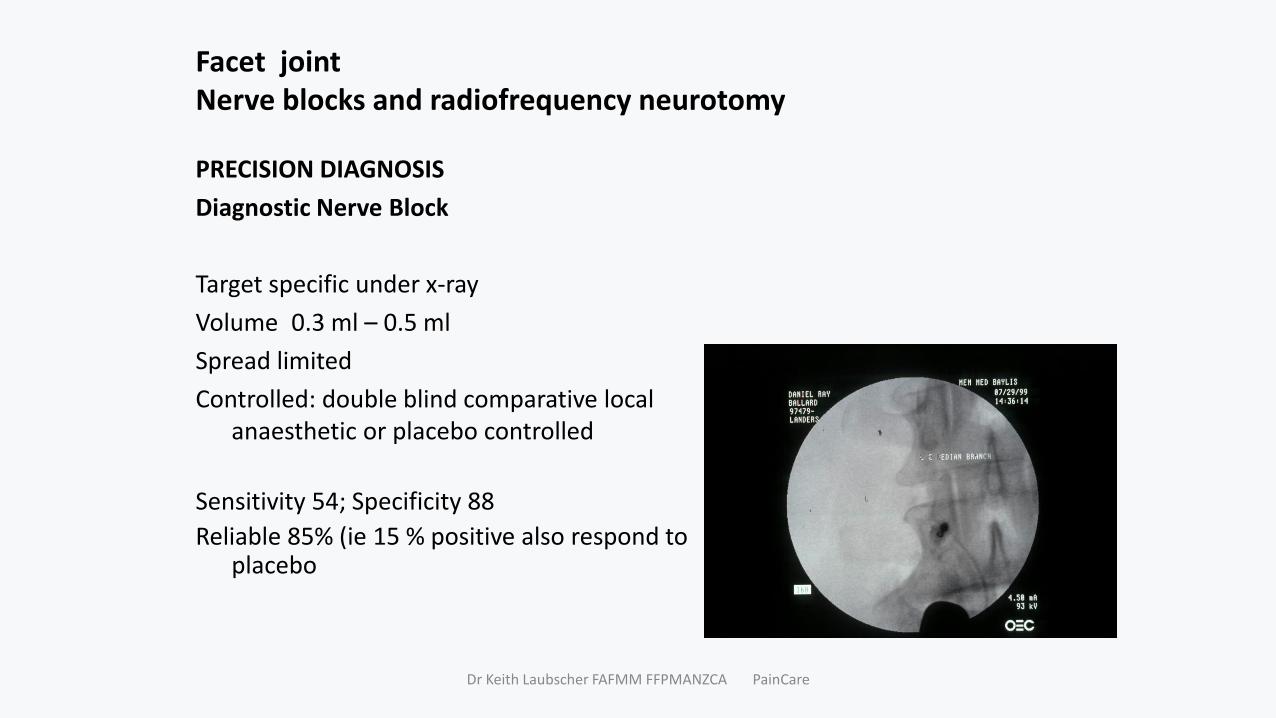
Facet joint Nerve blocks and radiofrequency neurotomy
PRECISION DIAGNOSIS
Diagnostic Nerve Block
Target specific under x-ray
Volume 0.3 ml – 0.5 ml
Spread limited
Controlled: double blind comparative local anaesthetic or placebo controlled
Sensitivity 54; Specificity 88
Reliable 85% (ie 15 % positive also respond to placebo
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Lumbar – facet joint Precision diagnosis
Indication:
• Persistent somatic lumbosacral pain (VAS > 4/10)
• Pain despite medical management
• Activity restriction
Utility
• Diagnostic
• Medicolegal
• (Surgical planning)
• Therapeutic RFN
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
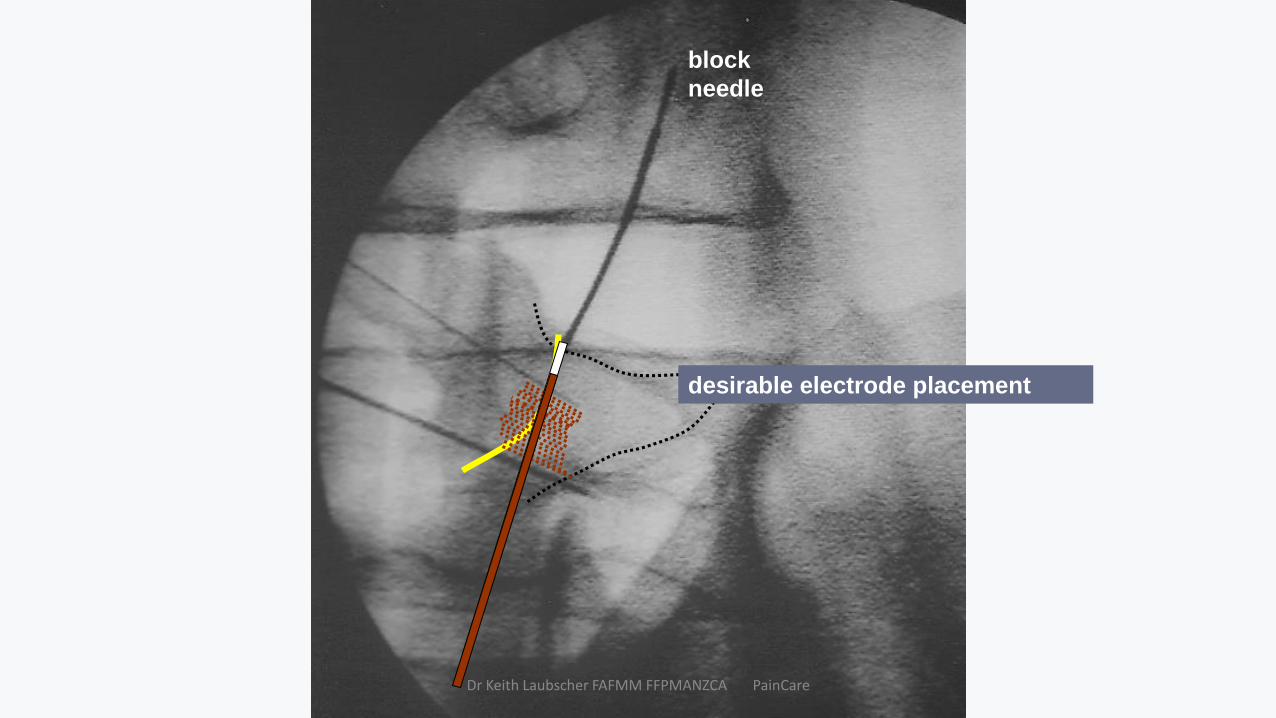
block
needle
desirable electrode placement
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
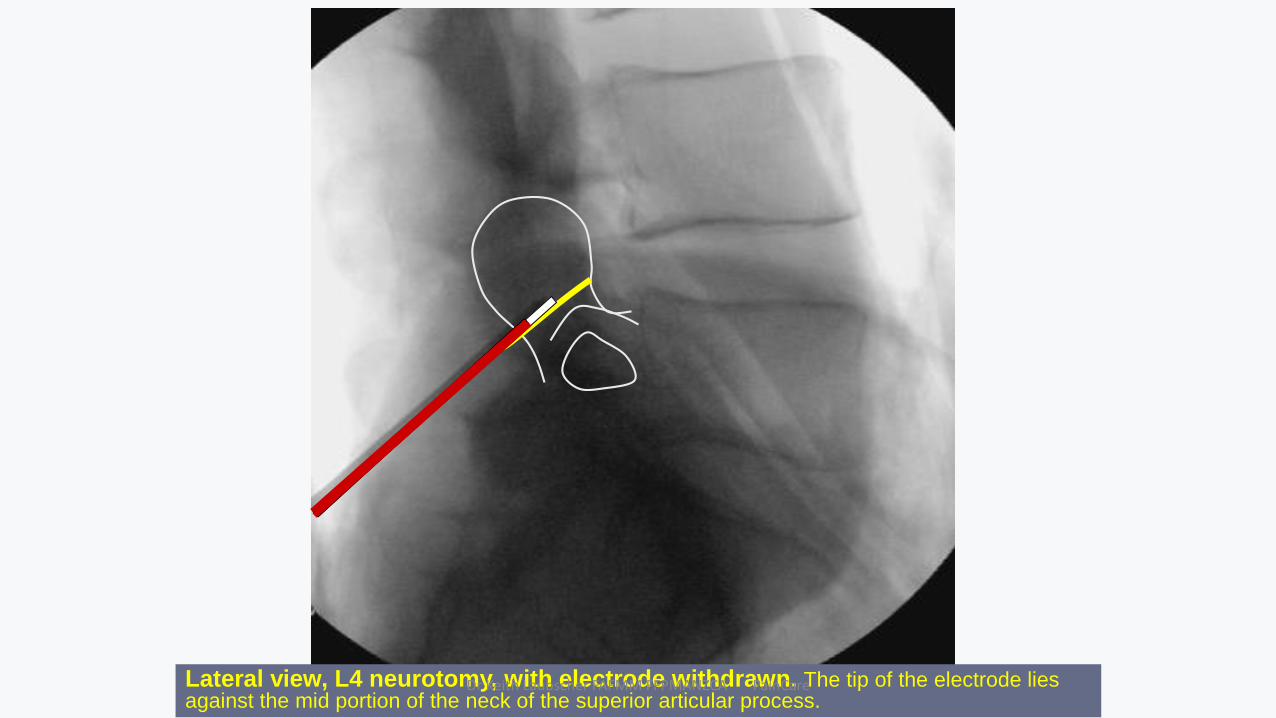
Lateral view, L4 neurotomy, with electrode withdrawn. The tip of the electrode lies against the mid portion of the neck of the superior articular process.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Lumbar RFNEfficacy
109 patients, 5 -418 monthsPositive MBB
Result 56% patients achieved a successful outcome.Relief median 17–33 months, 70% still relief at follow-up.
Successful: Complete relief > 6 months, Complete restoration of ADLNo need further health careReturn to work. Failed to meet any of these criteria = failed treatment
MacVicar, J., Borowczyk, J. M., MacVicar, A. M., Loughnan, B. M., & Bogduk, N. (2013). Lumbar medial branch radiofrequency neurotomy in New Zealand. Pain Medicine, 14(5), 639-645.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare
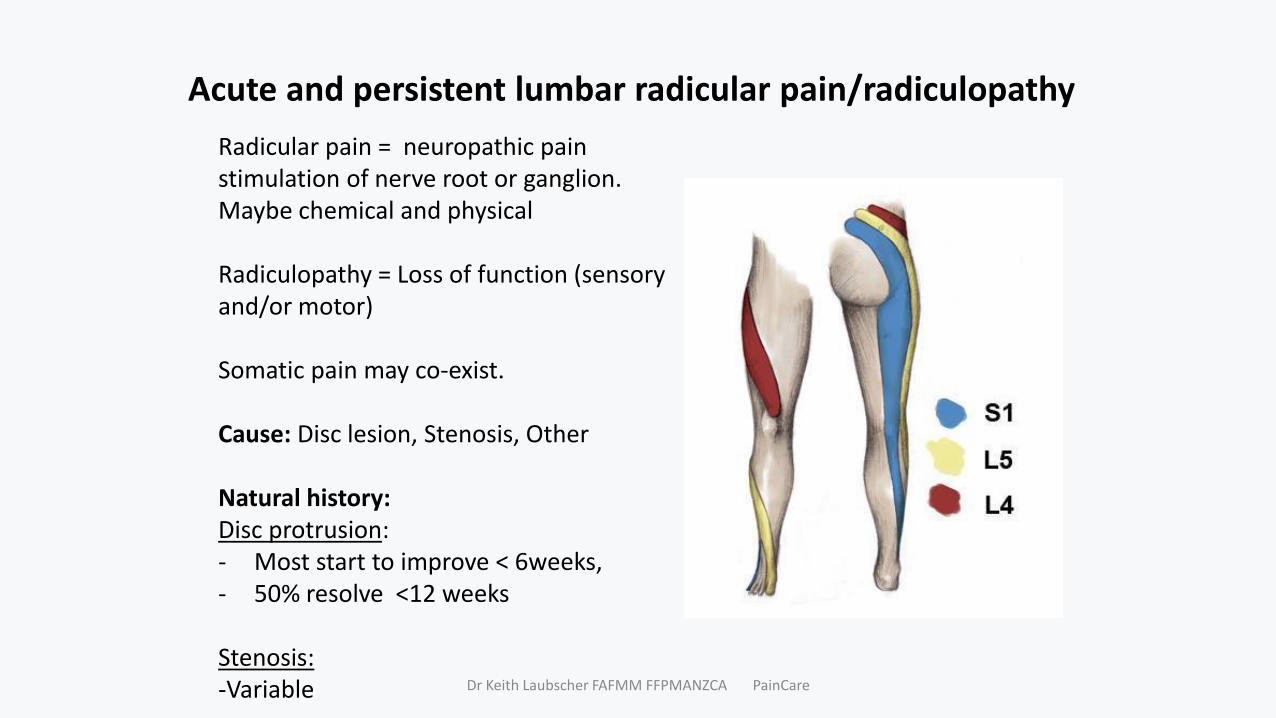
Acute and persistent lumbar radicular pain/radiculopathy
Radicular pain = neuropathic pain stimulation of nerve root or ganglion.Maybe chemical and physical
Radiculopathy = Loss of function (sensory and/or motor)
Somatic pain may co-exist.
Cause: Disc lesion, Stenosis, Other
Natural history:Disc protrusion: - Most start to improve < 6weeks, - 50% resolve <12 weeks
Stenosis:-Variable Dr Keith Laubscher FAFMM FFPMANZCA PainCare
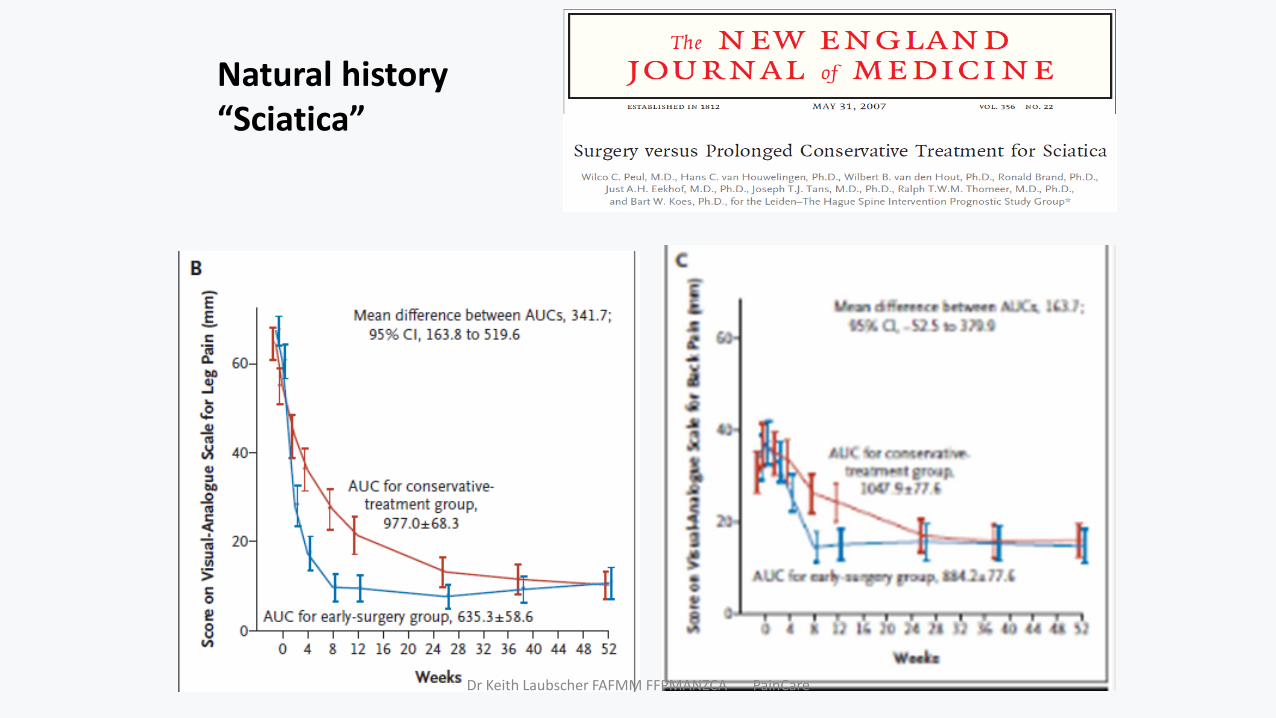
Natural history“Sciatica”
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
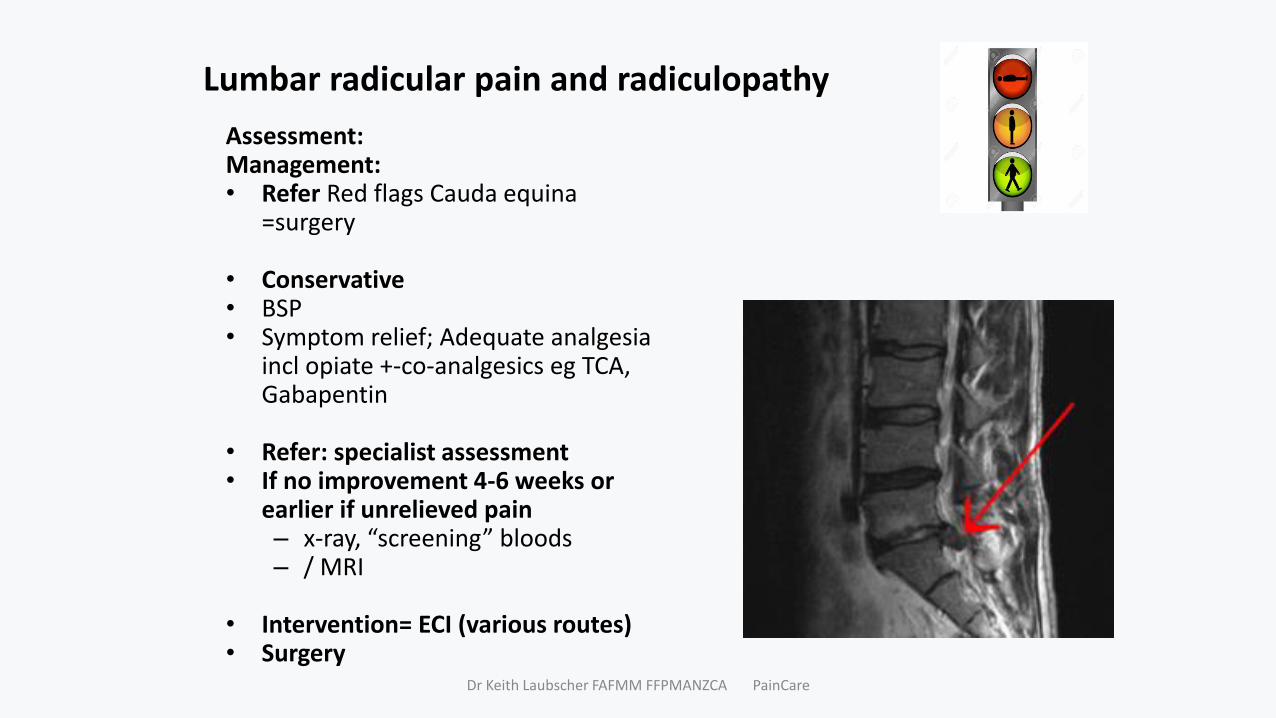
Lumbar radicular pain and radiculopathy
Assessment:Management: • Refer Red flags Cauda equina
=surgery
• Conservative• BSP • Symptom relief; Adequate analgesia
incl opiate +-co-analgesics eg TCA, Gabapentin
• Refer: specialist assessment• If no improvement 4-6 weeks or
earlier if unrelieved pain– x-ray, “screening” bloods– / MRI
• Intervention= ECI (various routes)• Surgery
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
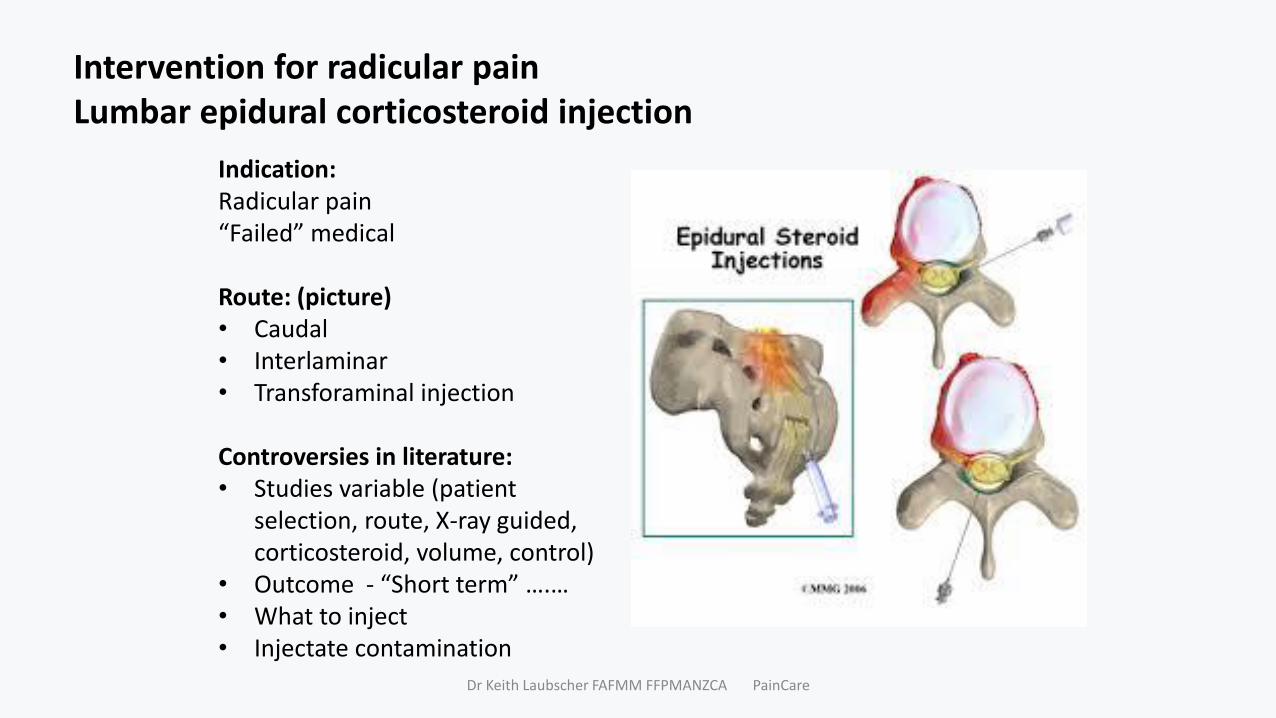
Intervention for radicular painLumbar epidural corticosteroid injection
Indication:Radicular pain“Failed” medical
Route: (picture)• Caudal• Interlaminar• Transforaminal injection
Controversies in literature:• Studies variable (patient
selection, route, X-ray guided, corticosteroid, volume, control)
• Outcome - “Short term” ….…• What to inject• Injectate contamination
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Lumbar epidural corticosteroid injection
Effectiveness:• TFIS > ILECI > Caudal
PIVD: • 60% patients - 50% relief 2 months, 40%
sustained 12 months• NNT 3• Restores function, reduces need for other
healthcare, reduces need for surgery• Cost effective
Spinal stenosis: • Limited data (acute –on-chronic)• 50% patients - 50% relief 6 months (or more)
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Lumbar epidural corticosteroid injection
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
2 4 6 8 2 4 6 8 10 12 16 18 20 22 24
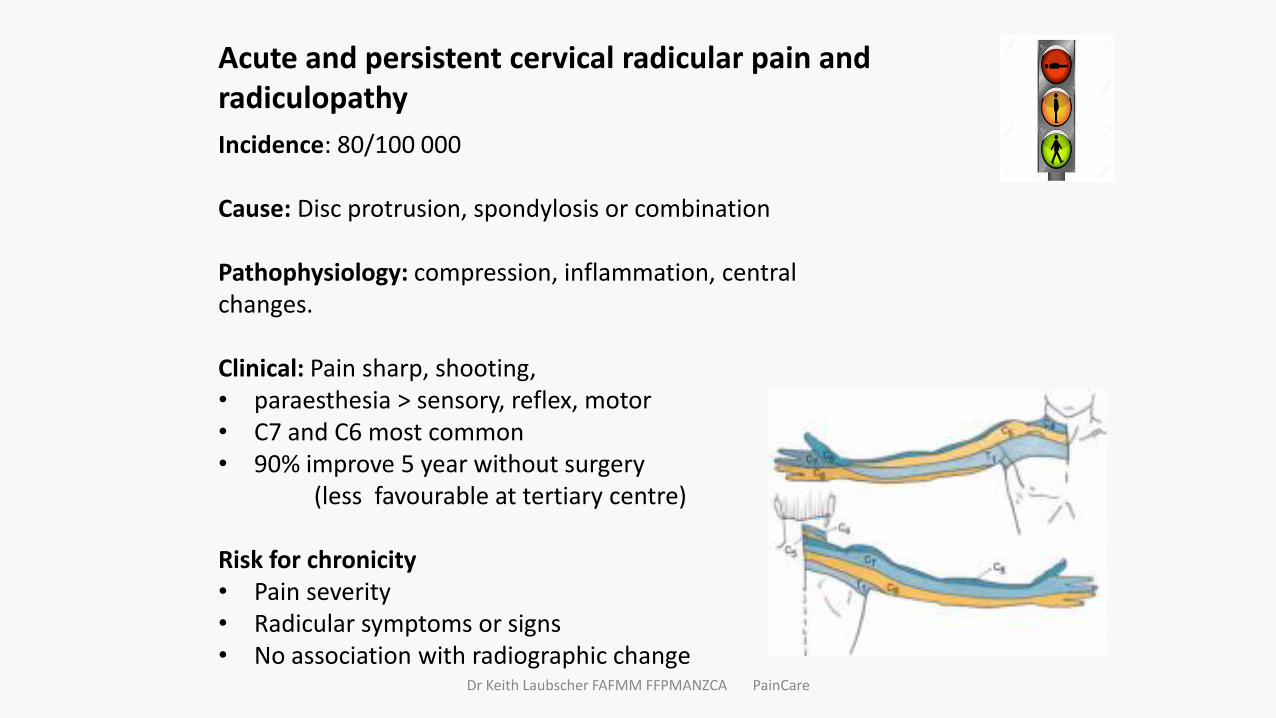
Acute and persistent cervical radicular pain and radiculopathy
Incidence: 80/100 000
Cause: Disc protrusion, spondylosis or combination
Pathophysiology: compression, inflammation, central changes.
Clinical: Pain sharp, shooting, • paraesthesia > sensory, reflex, motor • C7 and C6 most common• 90% improve 5 year without surgery
(less favourable at tertiary centre)
Risk for chronicity• Pain severity• Radicular symptoms or signs• No association with radiographic change
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
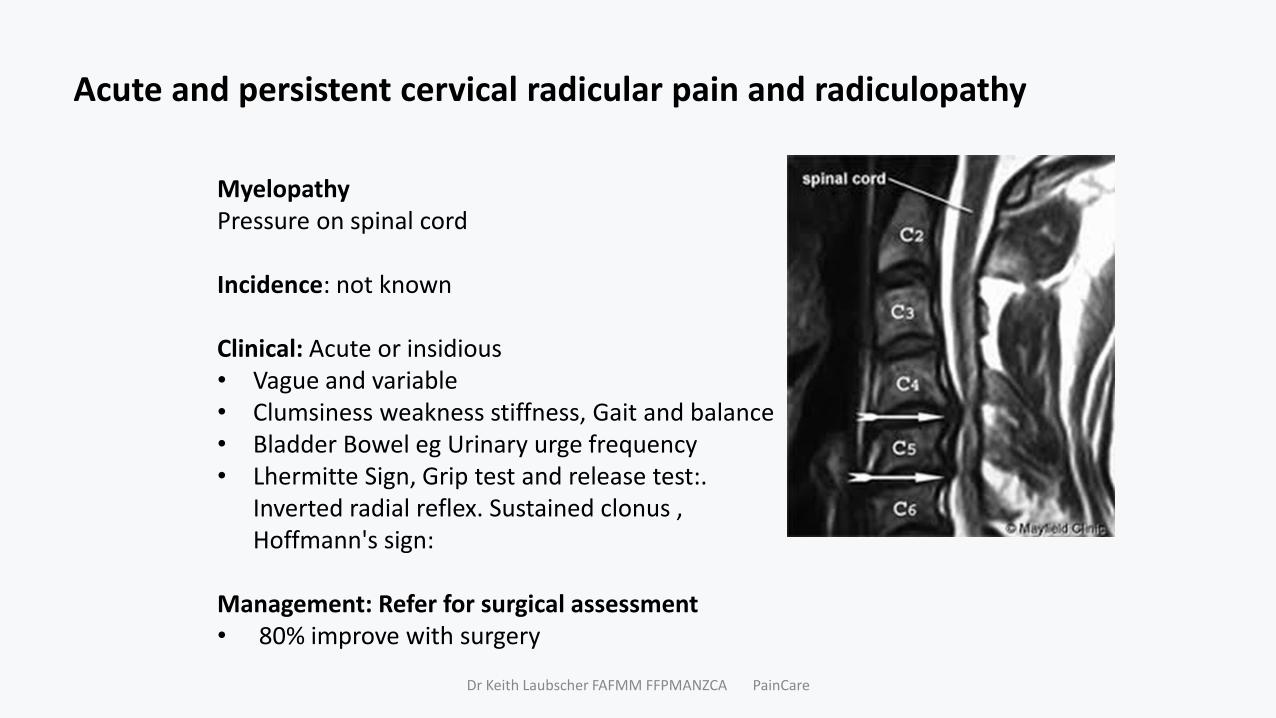
Acute and persistent cervical radicular pain and radiculopathy
MyelopathyPressure on spinal cord
Incidence: not known
Clinical: Acute or insidious• Vague and variable• Clumsiness weakness stiffness, Gait and balance• Bladder Bowel eg Urinary urge frequency• Lhermitte Sign, Grip test and release test:.
Inverted radial reflex. Sustained clonus , Hoffmann's sign:
Management: Refer for surgical assessment• 80% improve with surgery
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
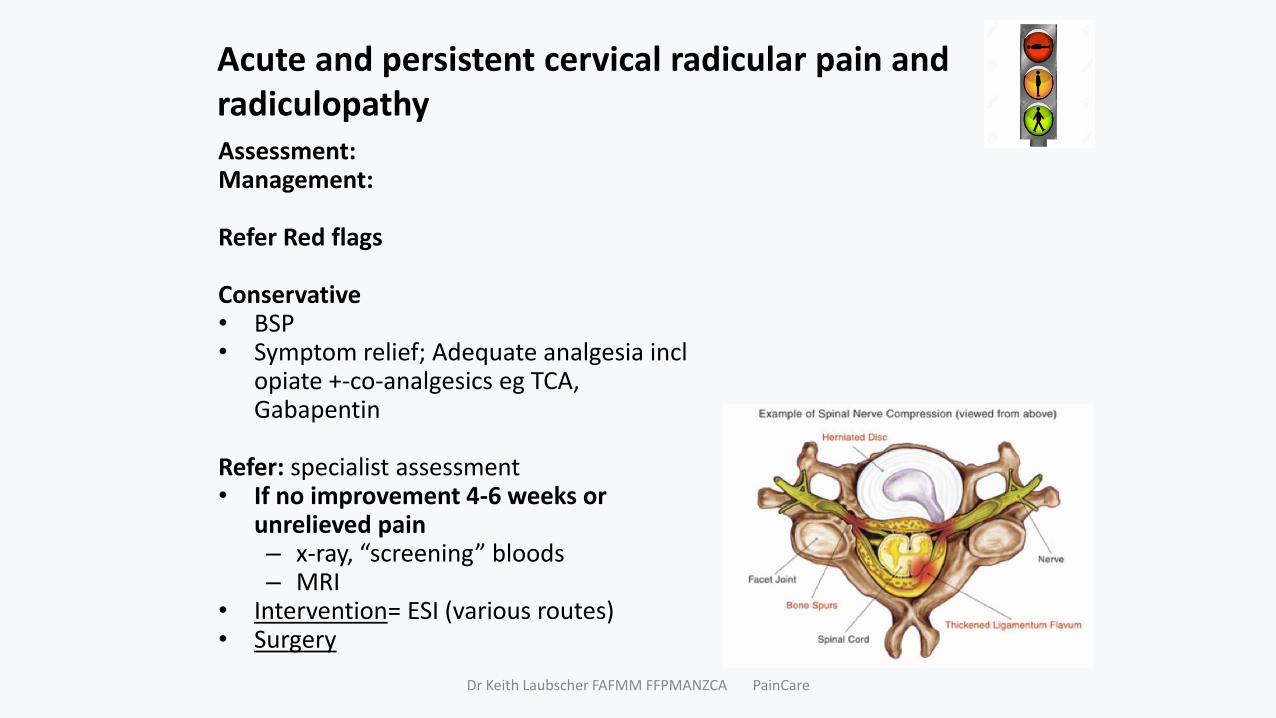
Acute and persistent cervical radicular pain and radiculopathy Assessment:Management:
Refer Red flags
Conservative• BSP • Symptom relief; Adequate analgesia incl
opiate +-co-analgesics eg TCA, Gabapentin
Refer: specialist assessment• If no improvement 4-6 weeks or
unrelieved pain– x-ray, “screening” bloods– MRI
• Intervention= ESI (various routes)• Surgery
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
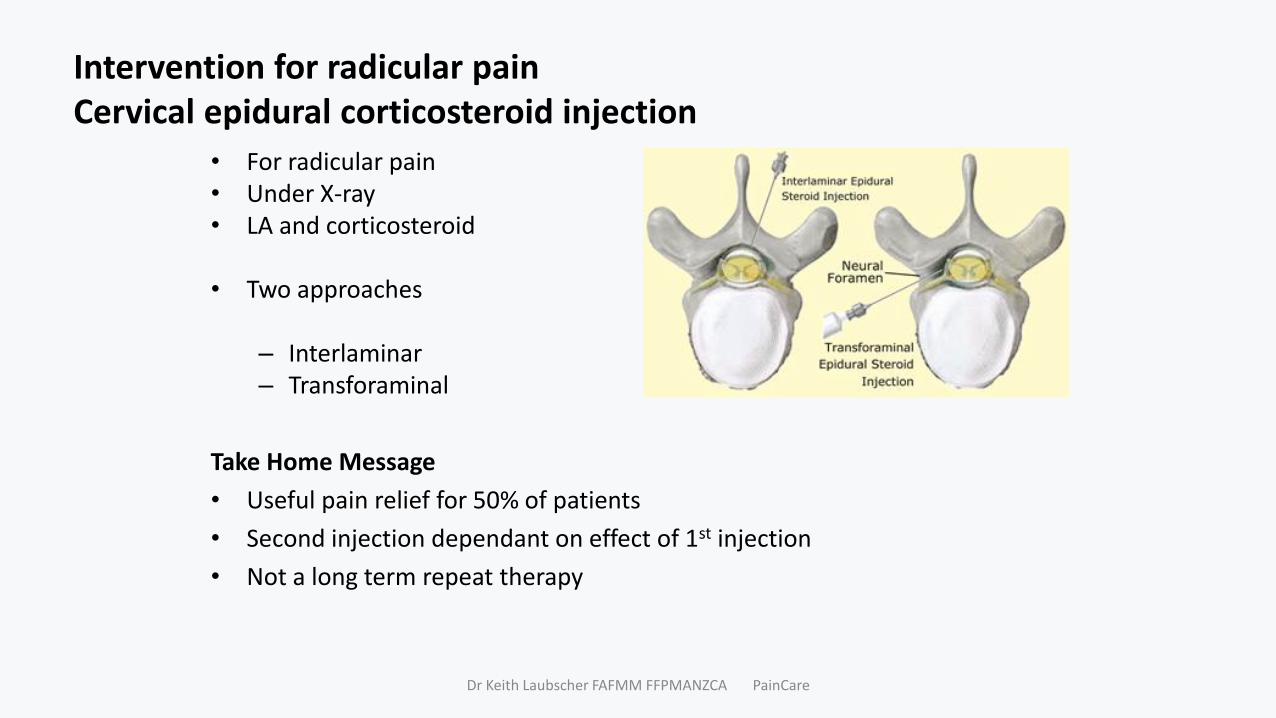
Intervention for radicular pain Cervical epidural corticosteroid injection
• For radicular pain• Under X-ray• LA and corticosteroid
• Two approaches
– Interlaminar– Transforaminal
Take Home Message
• Useful pain relief for 50% of patients
• Second injection dependant on effect of 1st injection
• Not a long term repeat therapy
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Cervical epidural corticosteroid injectionInterlaminar
Effectiveness
defined as 50% relief or more +/- 50% improvement in function)
Disc Herniation
70% good or very good relief – for 1 year
-1-3 injection
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
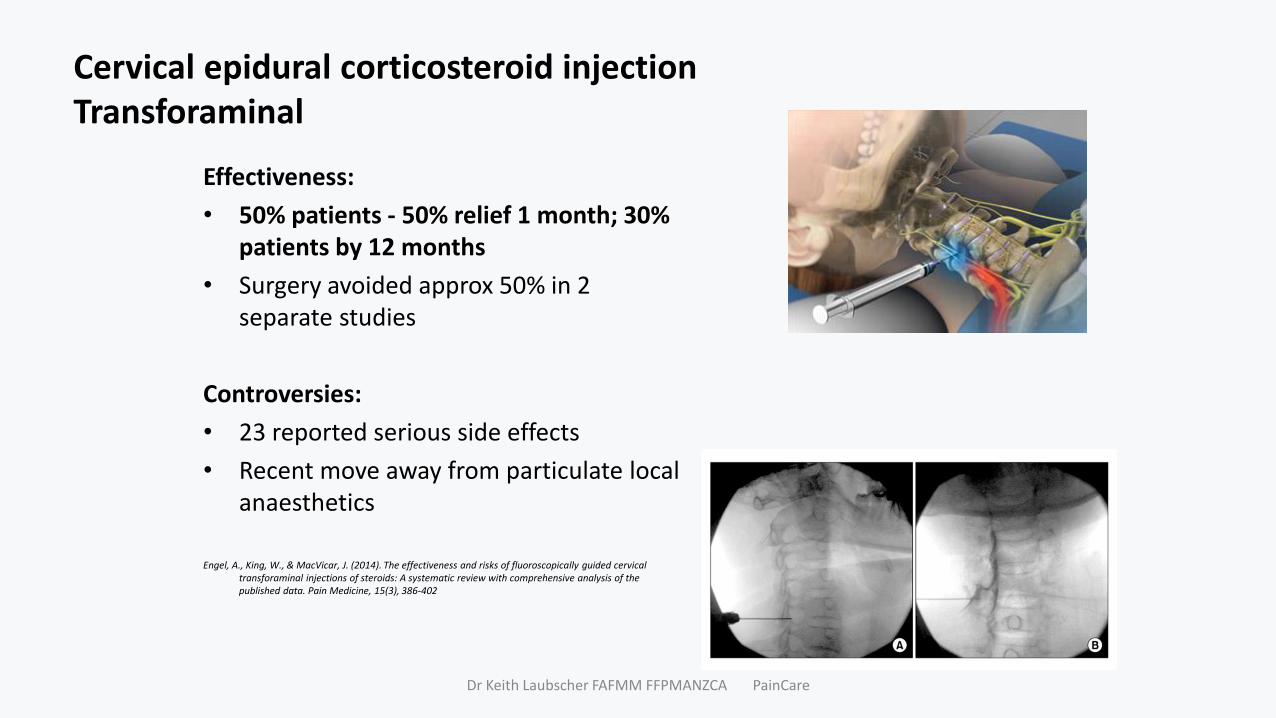
Cervical epidural corticosteroid injectionTransforaminal
Effectiveness:
• 50% patients - 50% relief 1 month; 30% patients by 12 months
• Surgery avoided approx 50% in 2 separate studies
Controversies:
• 23 reported serious side effects
• Recent move away from particulate local anaesthetics
Engel, A., King, W., & MacVicar, J. (2014). The effectiveness and risks of fluoroscopically guided cervical transforaminal injections of steroids: A systematic review with comprehensive analysis of the published data. Pain Medicine, 15(3), 386-402
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Summary lumbar intervention efficacy
Acute low back pain: NA
Lumbar radicular pain: Epidural Corticosteroid Injection• PIVD: 60% patients - 50% relief 2 months, 40%
sustained 12 months• Restores function, reduces need for other healthcare,
reduces need for surgery• Spinal stenosis: ~ 50% patients - 50% relief 6 months
Persistent /Chronic low back pain:• SIJ corticosteroid injection: 50% relief in 60 % , 2 months• Facet joint cotricosteroid injection: “improvement in pain/
function” in 50% at 3 months; 30% at 6 months• Facet joint FFN: 60% near complete relief 17- 33 months
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Summary cervical intervention efficacy
Acute cervical: NA
Cervical radicular pain: Epidural Corticosteroid Injection 50% relief in 50% patients 1 month; 30% patients 12 months; Surgery avoided in approx 50%
Persistent /Chronic cervical pain • Atlantoaxial joint Corticosteroid Injection : short term benefit; 50% relief in 20
% > 3 months; 12 % > 9 months• Cervical facet Corticosteroid Injection : short term benefit; “improvement in
pain/function” in 20% at 3 months• Cervical facet RFN: 68% near complete relief for 20 months; repeatable.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
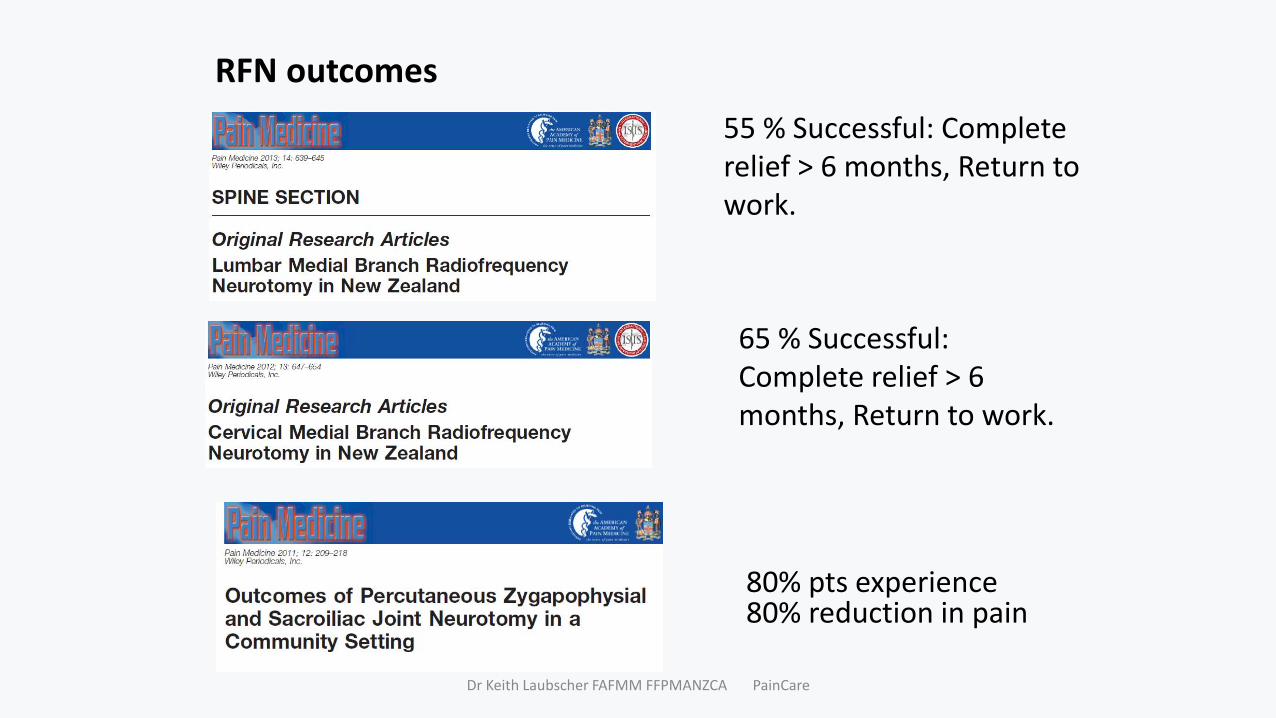
RFN outcomes
65 % Successful: Complete relief > 6 months, Return to work.
80% pts experience 80% reduction in pain
55 % Successful: Complete relief > 6 months, Return to work.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Specific mechanisms and specific management
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Specific interventional approaches
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Pain Cases 101
Dr Keith Laubscher
PainCare
Auckland 2018
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Purpose of assessment
• CAUSE:
– Diagnosis (RED FLAGS: Serious or sinister pathology); History Exam Inv
• MECHANISM:
– Nociceptive /Neurogenic/ “Central sensitisation”
• DURATION:
– Acute /Chronic
• CONTEXT:
– Psychosocial- biological (YELLOW FLAG)
• MANAGEMENT:
– Personalised: Surgery vs Interventional vs Pharmacological vs “Pain
Management”
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Clinical Assessment
• Pain: SOCRATES
• Fxn: ADL, Work, Social
• Psychosocial: mood, expectations
• Rx: Meds, Physical
• PMH and Meds:
• Exam:
• PDx
• Mx Inv.
• DIAGNOSIS
• MANAGEMENT:
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Rame S NHI: HQH6352
40-year-old Syrian tailor NZ 20 year
dived into a pool, struck his head 2 years ago; dazed, helped out
fractures superior endplates lower cervical and upper thoracic and C5/6 disc bulge
Pain left lower cervical trapezius, medial scapula border. Less so right. sharp, hot, or numbness. worse head forward, ors arms out in front. intermittent frontal headache tightness. VAS 3 -6/10, with activity modification.
Fxn: Wakes in night. At work
Psych: flashbacks, irritable. worried; Married 1st baby on the way
Rx: Physiotherapy extensive. Paracetamol 1g bd, Tramadol 50mg prn nausea and cognitive impairment. Nortriptyline no benefit.
PMH: N
Exm: Reduced ROM, tight paravertebral; no neurology
PDx: Persistent post-traumatic cervical spinal pain -past fractures
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Inv: BPI disability index: 3.3/10.
HAD scores: Anxiety 6, depression 3.
MRI (26.5.16) and SPECT scan cervical spine (17.10.16): C5/6 disc bulge, anterior deformities wedging upper thoracic spine T1, T2, T3 with Modic type II signal change at some levels, possibly T4; increased radiotracer uptake at C5/6 endplate, right C6/7 facet, less so left C6/7 facet, anterior osteophytes C6/7 and T2 end-plate.
Diagnosis
Mx: Surgery; Pain intervention; Medication: PPP
FInv:
DIAGNOSIS:
MANAGEMENT:
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Desmond N NHI: LQX103049 chef own take-away Ex-Macua, NZ 30 years, married 2 children, Moderate ETOH non smokerP: 8 weeks; shifting furniture; lumbosacral aching; fleeting paraesthesia in shins; BBC –ve ; VAS 7-9/10Fxn: Struggling physical work Psych: limited English; worried; not keen medicationRx: Chiropractor, Acupuncture no benefit; CelebrexPMH: NCExm: Reduced LROM, tight paravertebral; no neurologyInv: X-ray NHAD anxiety 12; depression 5 PDx: Persistent somatic lumbar spinal pain; Anxiety symptomsInv: MRI L2/3 small right disc protrusion; minor changes L3/4L 4/5
DASS21: Depression 26 / 42; Anxiety 26 / 42; Stress 26 / 42; PCS 25 / 52
DIAGNOSIS:
MANAGEMENT: Surgery; Pain intervention; Medication: PPP
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
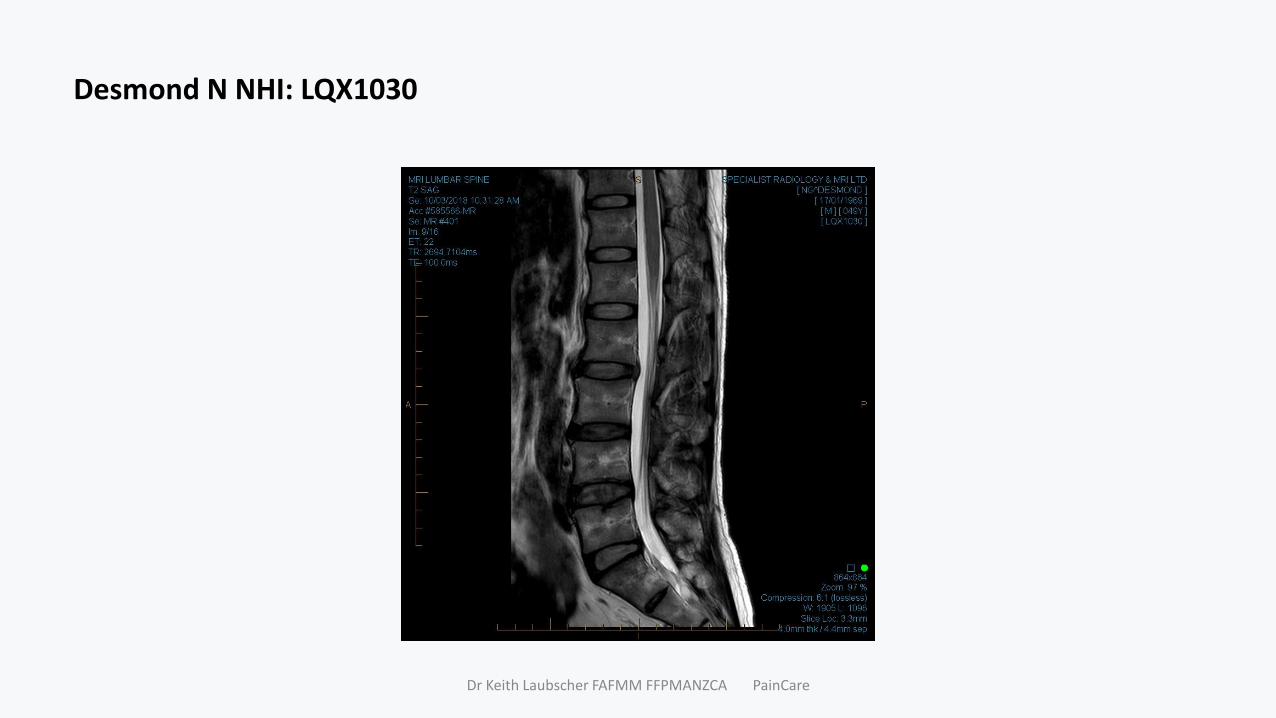
Desmond N NHI: LQX1030
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Susan B NHI: LNF7805 50 Business Consultant; Married 2 children; Etoh occ, Non-smoke- veSlip/fall onto buttock wet kitchen floor 10 days; Left lumbosacral thigh calf aching stabbing paraesthesia; BBC -veFxn: Off - ADL’s; Chores, work, ↓↓sleepPsy: Distress, anxiousRx: Diclofenac SR 75mg bd (dyspepsia), Codeine 60mg QID, Paracetamol2QID. Tramadol - 0 help. (amitriptyline not taken –fear of constipation)PMH: Asthma; pneumonia; acne rosacea; vitreous detachment; Migraine; IBS(with tendency to constipation); Hypertension; Rosacea; uterine fibromyoma; gynaecological pain (endometriosis); Anxiety disorder; laparoscopy; caesarean section.Med: Laxsol, Isotretinoin, Rosex gel, Bricanyl, Symbicort, Clonazepam, Propranolol prn.Ex: Distress; crutches; lying in waiting room, movement nil; AJ ↓; Sensation ↓ dorsum lat foot; WMP –veInv: X-ray - age related change, minimal marginal spurring.BPI disability index: 9.1/10.HAD scores: anxiety 15, depression 11.PDx: Acute post-traumatic lumbar spinal pain with left S1 radicular pain; Medical co-morbidities; Anxiety
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Inv: MRI : L5S1 disc herniation left S1 nerve root compressionDIAGNOSIS:MANAGEMENT: Surgery; Pain intervention; Medication: PPPAdd Amitriptyline; TFI
Progress: at 1month)Residual pain – VAS 3 -7/10 (back)RTWWalking dailyRx: Naproxen 750mg daily, Amitriptyline 25mg at night and she uses Paracetamol/Codeine x2 prn.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
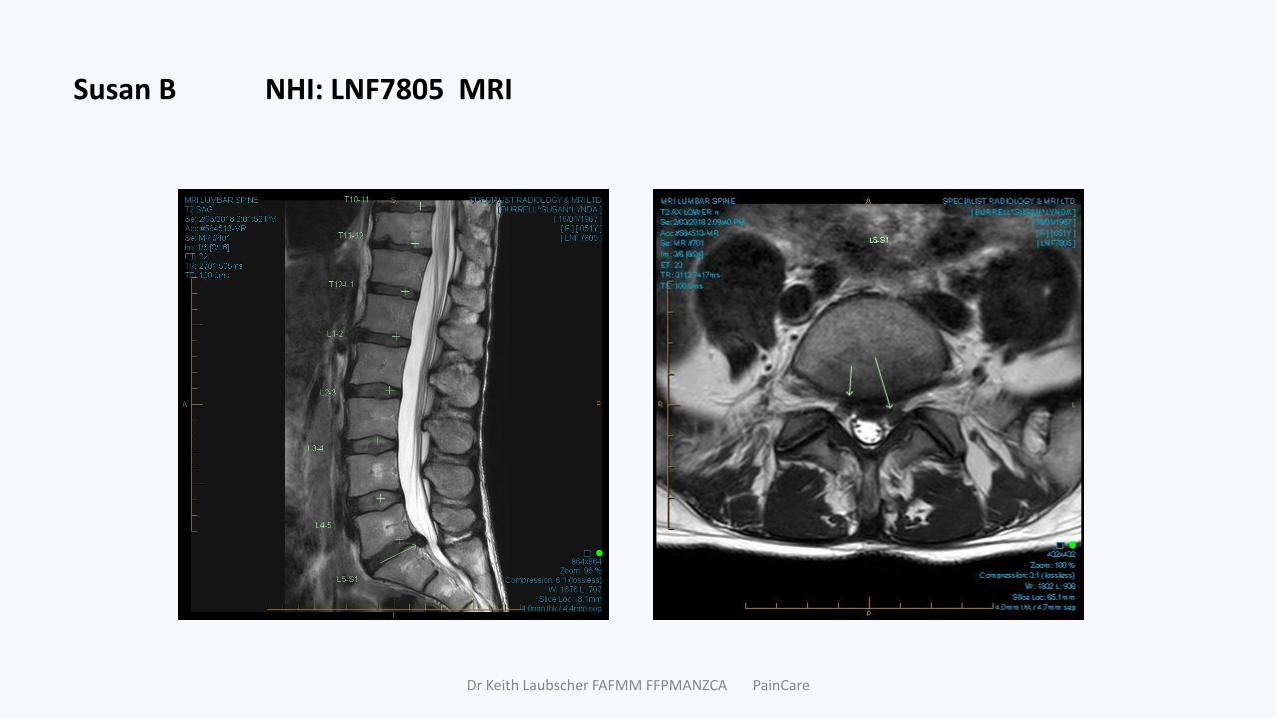
Susan B NHI: LNF7805 MRI
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
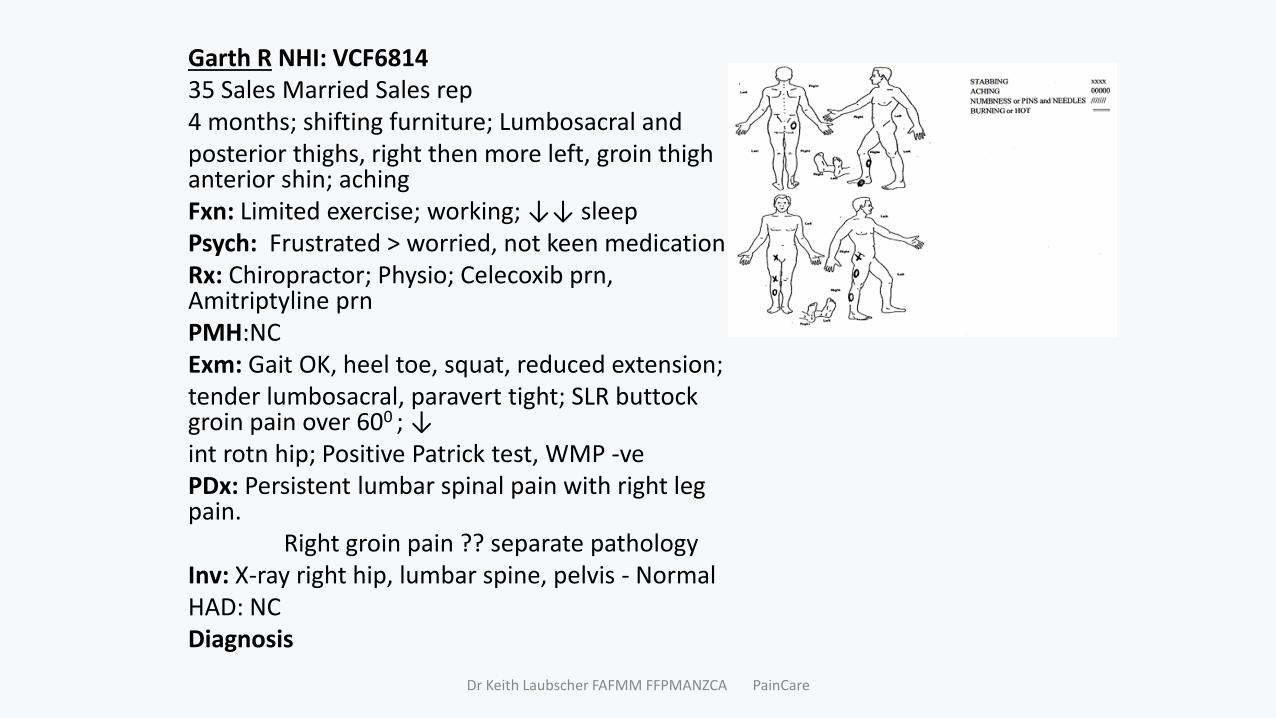
Garth R NHI: VCF681435 Sales Married Sales rep4 months; shifting furniture; Lumbosacral and posterior thighs, right then more left, groin thigh anterior shin; aching Fxn: Limited exercise; working; ↓↓ sleep Psych: Frustrated > worried, not keen medicationRx: Chiropractor; Physio; Celecoxib prn, Amitriptyline prnPMH:NCExm: Gait OK, heel toe, squat, reduced extension; tender lumbosacral, paravert tight; SLR buttock groin pain over 600 ; ↓int rotn hip; Positive Patrick test, WMP -vePDx: Persistent lumbar spinal pain with right leg pain.
Right groin pain ?? separate pathology Inv: X-ray right hip, lumbar spine, pelvis - NormalHAD: NCDiagnosis
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Management:
• Medication: Regular Celebrex, Amtriptyline (no help)
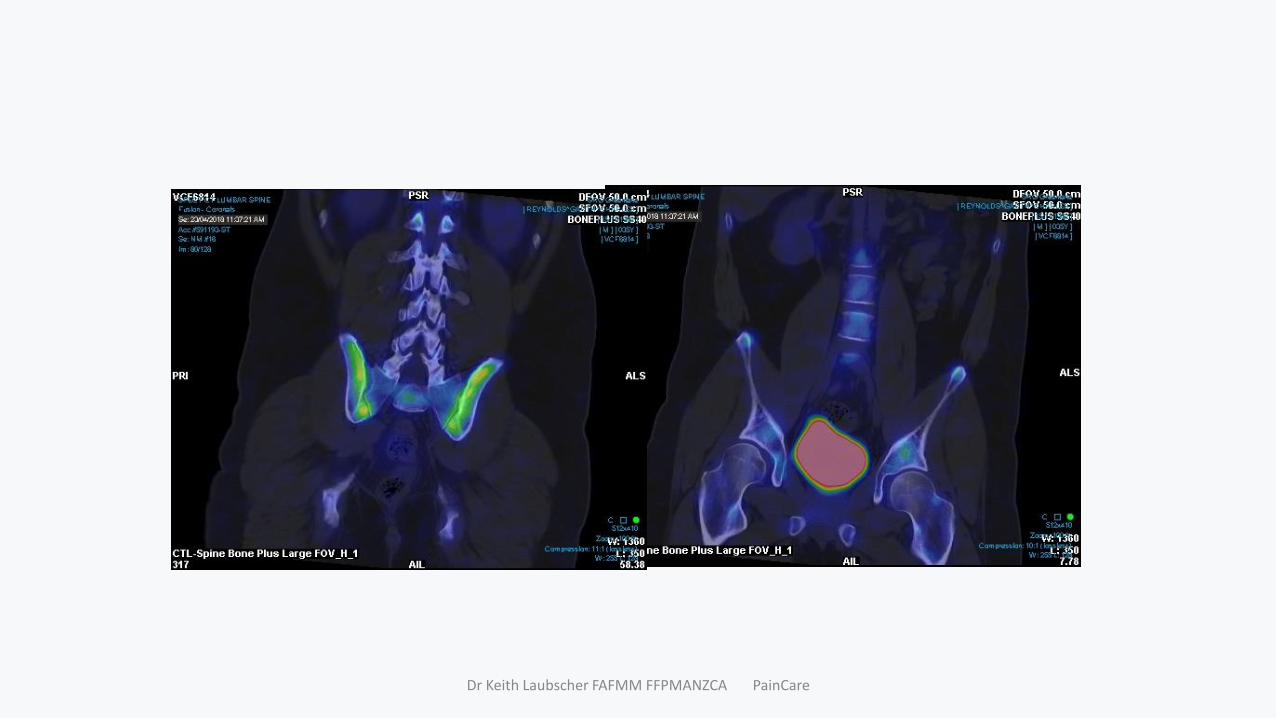
• AdInv: Imaging:
SPECT CT LUMBAR SPINE (23.4.18) No abnormal uptake is seen in the lumbosacral spine and pelvis and hip joints.
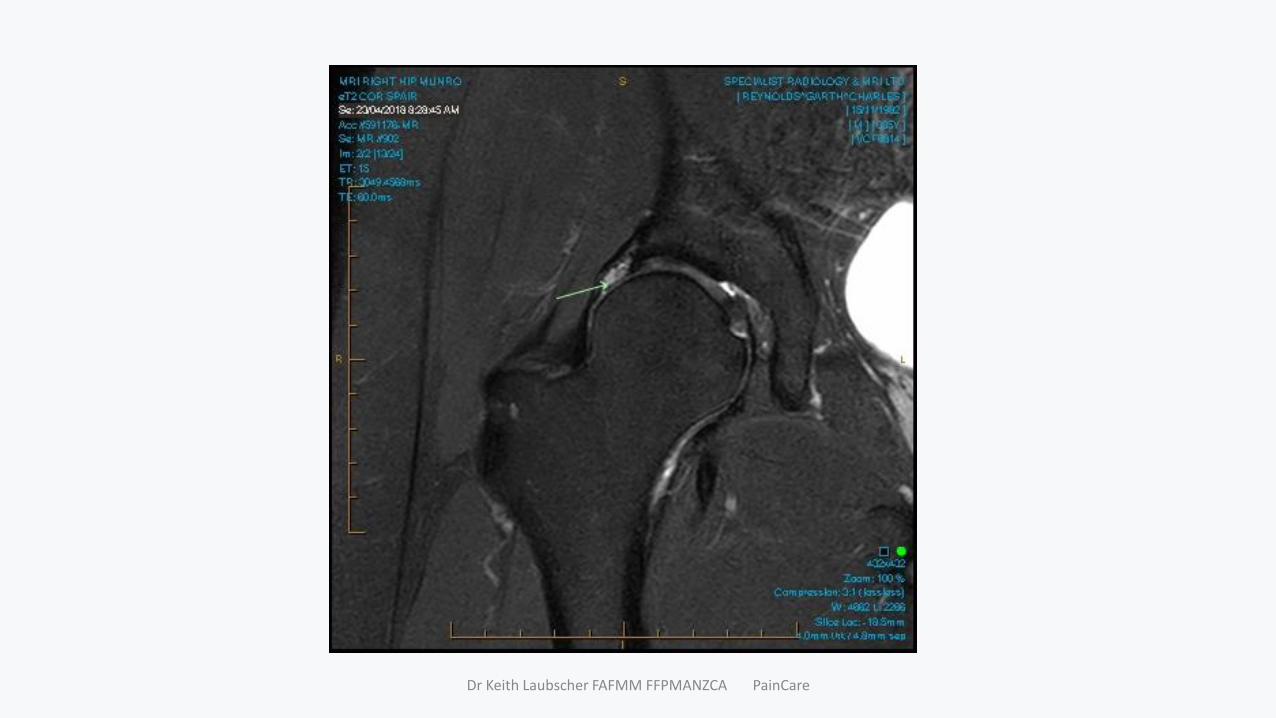
MRI RIGHT HIP (23.4.18) Right acetabular labral tear with extensive intralabral cyst formation.Cystic change at the right femoral head / neck junction. Preserved right hip joint articular cartilage.
Dx: Persistent lumbar spinal pain with right leg pain.
-L4/5 disc bulge, L5S1 central left paracentral herniation
• Acetabular labral injury, dysplasia
MANAGEMENT: Surgery; Pain intervention; Medication: PPP
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Garth R NHI: VCF6814 MRI
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
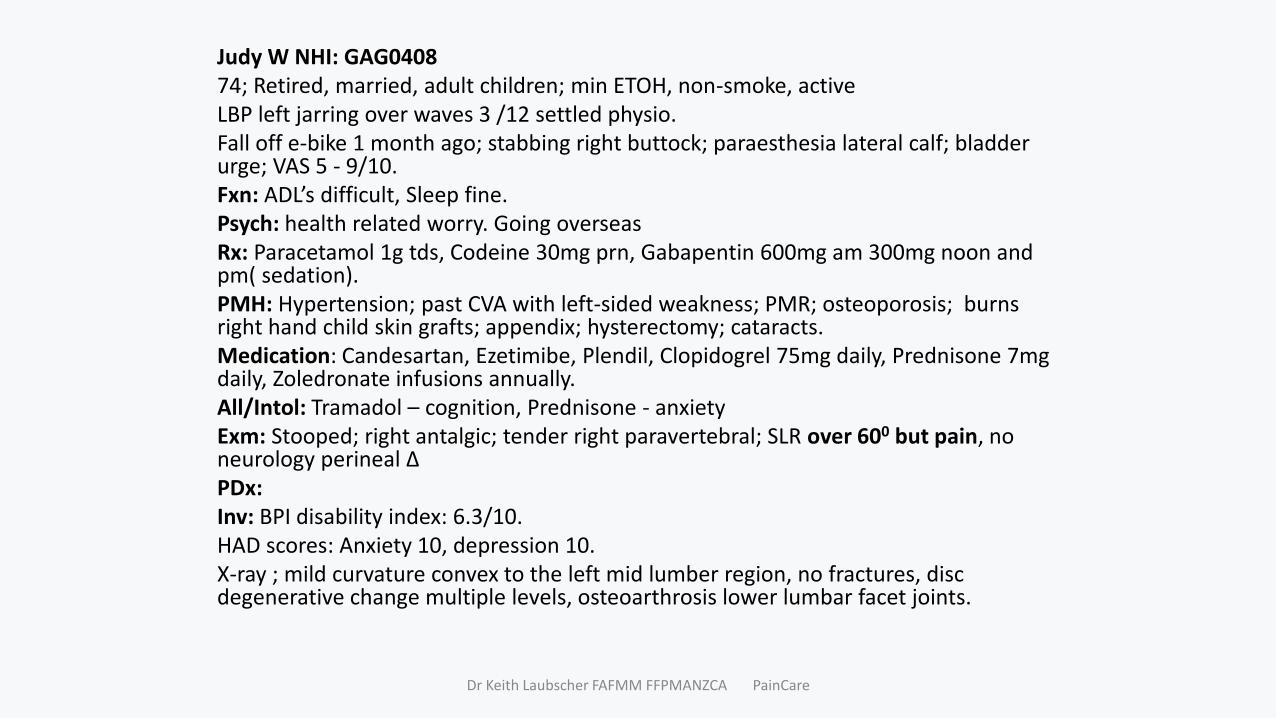
Judy W NHI: GAG040874; Retired, married, adult children; min ETOH, non-smoke, activeLBP left jarring over waves 3 /12 settled physio.Fall off e-bike 1 month ago; stabbing right buttock; paraesthesia lateral calf; bladder urge; VAS 5 - 9/10. Fxn: ADL’s difficult, Sleep fine. Psych: health related worry. Going overseasRx: Paracetamol 1g tds, Codeine 30mg prn, Gabapentin 600mg am 300mg noon and pm( sedation).PMH: Hypertension; past CVA with left-sided weakness; PMR; osteoporosis; burns right hand child skin grafts; appendix; hysterectomy; cataracts.Medication: Candesartan, Ezetimibe, Plendil, Clopidogrel 75mg daily, Prednisone 7mg daily, Zoledronate infusions annually. All/Intol: Tramadol – cognition, Prednisone - anxietyExm: Stooped; right antalgic; tender right paravertebral; SLR over 600 but pain, no neurology perineal ∆PDx:Inv: BPI disability index: 6.3/10.HAD scores: Anxiety 10, depression 10. X-ray ; mild curvature convex to the left mid lumber region, no fractures, disc degenerative change multiple levels, osteoarthrosis lower lumbar facet joints.
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
DiagnosisManagement:• Medication:• AdInv: Imaging:• MRI lumbar spine (21.5.18) shows
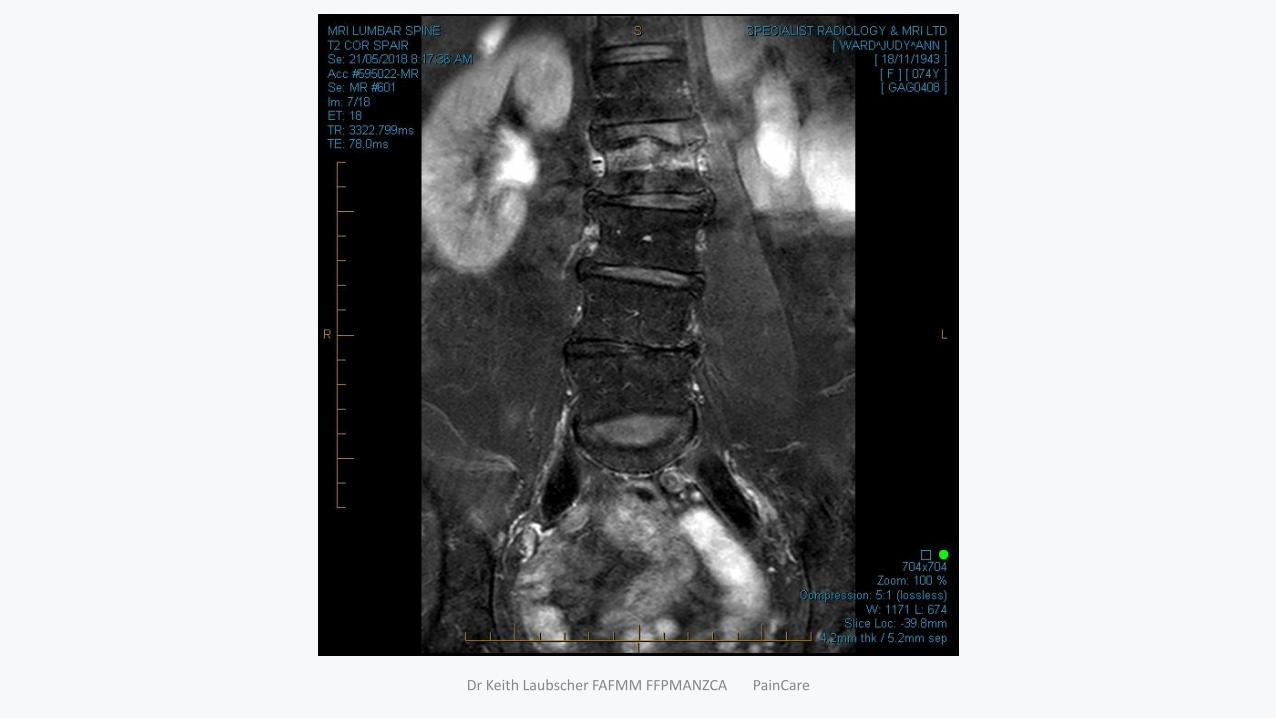
insufficiency fracture of L2, multilevel spondylosis most marked at L4/5, zygapophysial joint arthrosis, a L5/S1 right synovial cyst with associated spinal stenosis. There appears to be a left L4 pars defect – not active (not reported).
DIAGNOSIS:• RX MANAGEMENT: Surgery; Pain
intervention; Medication: PPP
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
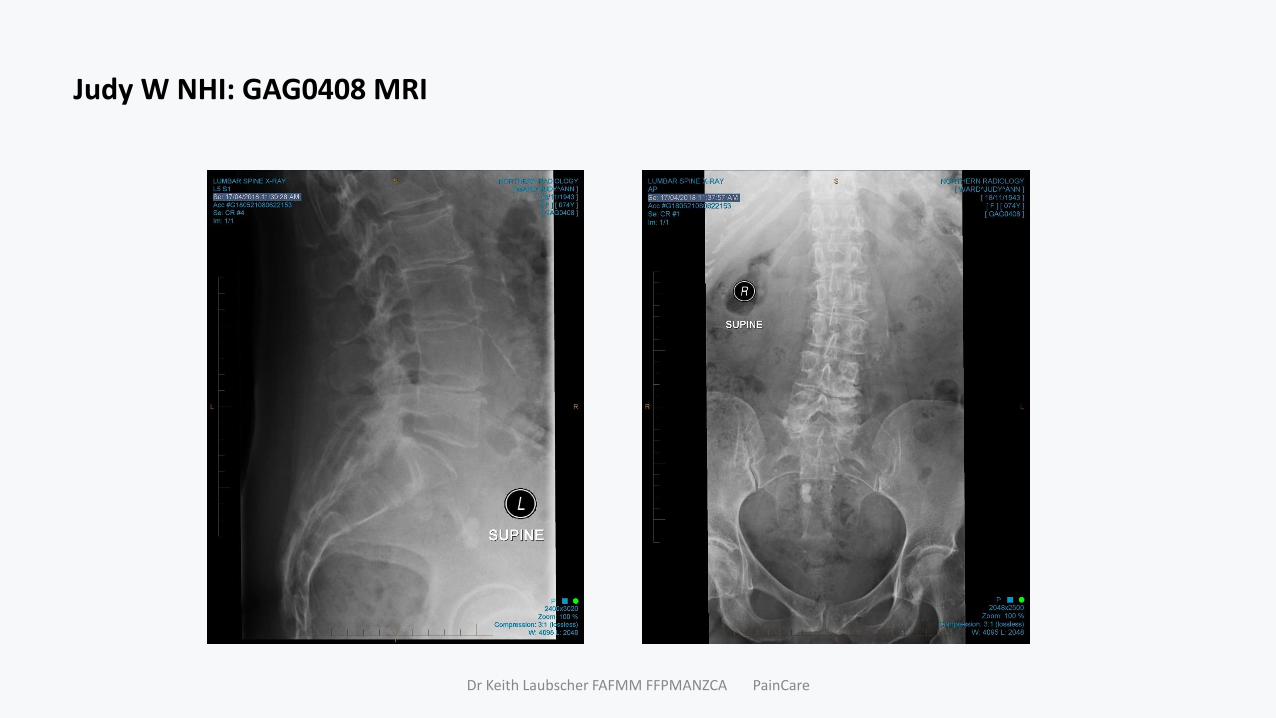
Judy W NHI: GAG0408 MRI
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Peter C PCD7352
73-year-old, USA NZ 30 years, Married adult children
LBP on and off teens - fall on coccyx. Exacerbation 3 years ago bending doing shoelaces.
Variable right +/- left lumbosacral region., aching. VAS 2- 6/10, variable, activity dependent, once flared days to settle.
Fxn: cant drive long, cant sail restore boat,
Rx: physio +++, home programme; Paracetamol 1g most days, Codeine prn, Diclofenac for exercise
Psych: earnest, frustrated, wants fix, wants to do more, avoid medication. ACC now declined
PMH:: Hypercholesterolaemia; musculoskeletal chest pain, mild coronary artery disease (angiogram 2015); bladder neck excision, sinus surgery, cataracts, dental implants.
Meds: Simvastatin. Zopiclone prn
Ex: Taller, slim build. Flexion distal tibia, Extension and rotation aggravate; nil Neurological. No WMP.
Inv: BPI disability index: 2.6/10. HAD scores: NC
X-ray multilevel spondylosis, ZJ OA, L5S1 spondylolisthesis
PDx: Persistent right more than left lumbosacral pain.
-Lumbar spondylosis, L5S1 spondylolisthesis, zygapophysial osteoarthrosis
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
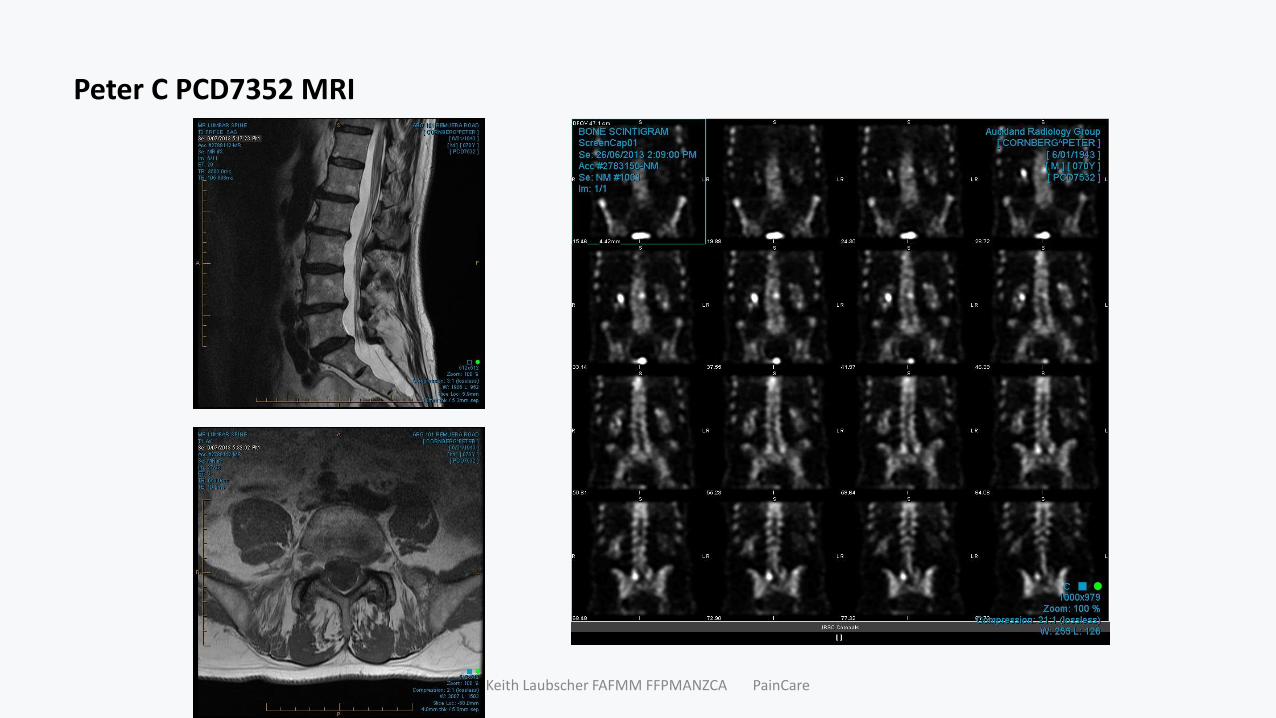
Inv: MRI lumbar spine (9.7.13) notes multilevel disc disease, severe bilateral L5/S1 facet arthrosis, mild dextroconvex scoliosis centred on L2. Bone scintigram (26.6.13) notes increased uptake in the posterior elements L5/S1 on the right, less marked on the left.CT bilateral L5/S1 facet joint injection pain records that his pain reduced to zero.
DIAGNOSIS:RX MANAGEMENT: Surgery; Pain intervention; Medication: PPPMBB RFN
Outcome
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Peter C PCD7352 MRI
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
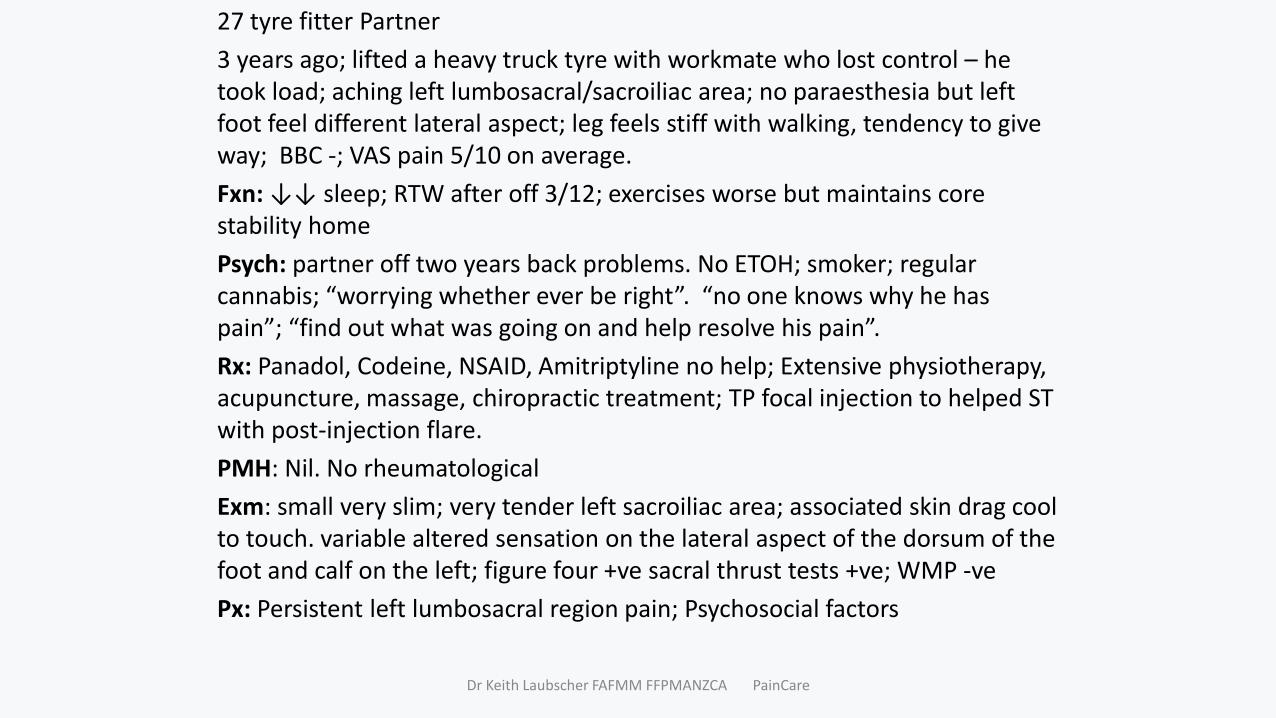
27 tyre fitter Partner
3 years ago; lifted a heavy truck tyre with workmate who lost control – he took load; aching left lumbosacral/sacroiliac area; no paraesthesia but left foot feel different lateral aspect; leg feels stiff with walking, tendency to give way; BBC -; VAS pain 5/10 on average.
Fxn: ↓↓ sleep; RTW after off 3/12; exercises worse but maintains core stability home
Psych: partner off two years back problems. No ETOH; smoker; regular cannabis; “worrying whether ever be right”. “no one knows why he has pain”; “find out what was going on and help resolve his pain”.
Rx: Panadol, Codeine, NSAID, Amitriptyline no help; Extensive physiotherapy, acupuncture, massage, chiropractic treatment; TP focal injection to helped ST with post-injection flare.
PMH: Nil. No rheumatological
Exm: small very slim; very tender left sacroiliac area; associated skin drag cool to touch. variable altered sensation on the lateral aspect of the dorsum of the foot and calf on the left; figure four +ve sacral thrust tests +ve; WMP -ve
Px: Persistent left lumbosacral region pain; Psychosocial factors
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Inv:
BPI disability index average: 7/10.
HAD scores; anxiety 9, depression 9.
Xray: normal
DIAGNOSIS
FInv:
CT scan (8.10.12) notes subcortical cyst within the left ilium likely relates to small overlying area of cartilage damage but is unlikely to be of significance.
MRI lumbar spine (11.9.14) 3mm area of low T1 signal surrounded by bone marrow oedema in the ilium adjacent to the left lower sacroiliac joint. The sacroiliac joint is otherwise normal.
Managment:
Inv:
DIAGNOSIS:
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
• RX MANAGEMENT: Surgery; Pain intervention; Medication: PPP• SIJ Injection/block•
• Outcome: TO DO•
• Recurring episodes • MRI changes persist MRI LUMBAR SPINE 07/10/2015 •
• RX MANAGEMENT: Surgery; Pain intervention; Medication: PPP
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Dr Keith Laubscher FAFMM FFPMANZCA PainCare
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Boris C DNH0997 MRI
Dr Keith Laubscher FAFMM FFPMANZCA PainCare

Dr Keith Laubscher FAFMM FFPMANZCA PainCare





























