Embed Size (px)
Citation preview

Dr Mary FoleyDirector-General
June 2012

• Supporting devolution and local
decision making about patient care
• Establishing a Statewide system
framework
• Providing a clear funding and
performance framework
• Developing new service models to
meet changing demand and growth
pressures
Our journey to a better health system: Where are we up to?


• 2012/13 Budget
• Service Agreements
• Activity Based Funding
• Transparent, meaningful
performance reporting (BHI, CI,
CEC)
2. Providing a clear funding and performance framework

Budget supports growth and is aligned to our priority areas – all within a tight fiscal environment
• $17.3b recurrent funding
• $1.16b capital
• $810M in state funding for growth
• 1.2m acute separations in 2012/13
• 2.6m ED attendances in 2012/13
NSW Budget 2012/13

Are the key to real devolution:
3. Service Agreements – delivering transparency
• A transparent funding and purchasing model
• Provide information to inform decision making
• Relate funding to clinical practice and individual patient care
• Sets the performance framework

How does ABF work?
• State and Commonwealth funds paid to LHDs on basis of number of patients treated– Acute inpatient– ED– Outpatients– Mental Health and Subacute from 1 July 2013
• Block funding– teaching and research– community and population health– small country hospitals < 3500 separations– State only block grants

How ABF doesn’t work• It is not uncapped
– fixed Commonwealth funding till 2014, then 45 % contribution to growth above 2013 baseline
• State remains dominant funder of health services.
• The State purchases volumes and service streams from Districts under a capped budget allocation.

The State Funding Model under ABFYear 1
• Determines LHD total funding through a service agreement
• 70% ABF, 30 % block funded
• State Price = total cost of LHD services divided by total volume ($4471)
• Transparent allocation to types of service
• Admitted and ED services purchased using patient volumes
• Full cost of growth volumes funded at lower of State/LHD Price
• NWAU based
• Visible transition grants where average cost exceeds state price
• Turnaround plans, efficiency savings

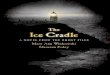
Funding Structure of Service Agreement
LHD's Budget
State $'s by NWAU Vol. =
State $'s by NWAU Vol. =
Block Grant - = Outpatient Activity
Teaching & ResearchBlock Values determined by
Cost data collections
Other State Programs
eg Pop.HlthCommunity HthAboriginal Hlth
EtcTransition
Grants
Inpatient Activity
ED Activity
Cwth / State ABF Pool
Sub-AcuteMental Health
Cwth/State Block
Converted into a Price and NWAU Vol
Other Block Funded Hospitals

LHD Relativity to State Price

4. Future Development of ABF• Our key priority during the next
two transition years is to keep the system safe and operating while introducing new funding drivers
• The new purchasing approach will focus on how we develop the right models of care (evidence based), develop effective alternatives to hospitalisation, and better link hospital and primary care, based on local decision making and clinical involvement.
• The Pillars – ACI, CEC and HETI will have key roles in supporting LHDs to use the new funding framework to support the development of services to meet the needs of their communities