Embed Size (px)
Citation preview

Dr Mere Kende, MBBS, MMED (Path),MAACB (AUS), MACTM
(AUS),MACRRM (AUS)
Department of Pathology
Faculty of Health Sciences & Medicine
UPNG

Definition?
How is this done? ◦ Sample Collection ◦ Smear Preparation ◦ Preanalytical /laboratory issues
How is it useful clinically? ◦ Red Cells & Hemoglobin Issues ◦ White cell count ◦ Platelet ◦ Hematocrit/PCV ◦ Red Cell indices

Refers to; Hemoglobin measurement
Quantification of red cells, total white cells, platelets, white cell differential count &
Red Cell Indices (MCV, MCHC etc)
May include Blood Film examination depending
on laboratory protocol
Full Blood Examination or Count (FBE/FBC)

Ideally in all patients presenting into hospital
Only selected cases on OPD
Fasting not necessary
Fill request form appropriately with relevant clinical information.
Must have all necessary equipment for blood collection
Explain & reassure patient, be confident!
Ensure adequate sterile technique

Veins
Capillary
Bone Marrow

Protect yourself from blood spill & Needle stick injury
Spend time looking for vein
Avoid prolonged application of tourniquet
Avoid haemolysis/clot (decreased RBC/PLT)
Only gentle mix required

Collect into anti-coagulant tube (EDTA/heparin)
Only 5mls required (do not force blood into tubes)
Analyse within 3hrs
Evenly spread thin film –allow air-dry

Forms:
1- Tri-Potassium EDTA
2- Di-Sodium EDTA
3- Di-Lithium EDTA
EDTA is also known as Versene or Sequestrene. EDTA acts by chelating / removing ionized calcium (calcium is required for blood to clot, so when it is removed blood will not clot).

Excess EDTA
causes shrinkage of RBC’s, causing falsely / erroneously reduced hematocrit (HCT), Subsequently causes:
◦ increase in MCHC
◦ decrease in MCV (MCV and MCHC are RBC indices

PLTs disintegrate, ◦ causing erroneously high PLT count,
EDTA can induce platelet aggregation and clumping, ◦ False thrombocytopenia
◦ False lecocytosis
◦ Correct by repeating PLT count/exam Blood film

Is the anticoagulant of choice
◦ coagulation and platelet function tests,
◦ ESR (erythrocyte sedimentation rate test).

Accid mucopolysaccharide,
It acts by complexing with anti-thrombin to prevent blood clotting (antithrombin is one of the natural/physiological inhibitors of blood coagulation, which is found in vivo, this will be studied later in coagulation and hemostasis modules).
Uses: ◦ LE cells ◦ Biochemistry /Hormones



Manual Cell Count
Automated Cell Count
Blood Film Examination if required










Diagnosis of Anaemia
Screen Bacterial infection
Screen Viral Infection
Screen Blood Cancer (leukaemia)
Screen Poisoning
Monitor Treatment and emergence of complications



Use correct ref Ranges
Affected by age & sex, ethnic group, pregnancy, altitude & Physiological states (exercise)

Red Cells (4000-7000 x109 /L)
Platelets (150-400 x109 /L)
White cells (4-10 x109 /L) ◦ neutrophils, (3-8 x109/L)
◦ Lymphocytes (1.5-4.5 x109 /L)
◦ Monocytes (0.2-0.8 x109 /L)
◦ Eosinophils (0.04-0.5 x109 /L)
◦ Basophils (less than 0.2 x109 /L)



Pancytopenia- All cell Count is low Microcytosis- Smaller size red cells Macrocytosis Larger size red cells Hypochromia Faintly stained red cells
Leucopenia- Low white cell count Leucocytosis – Elevated white cell counts Lymphocytosis – Elevated lymphocytes Eosinophilia- Elevated eosinophils count Neutropenia- Low neutrophil count Neutrophilia- High neutrophil count
Thrombocytosis – Elevated Platelets Count Thrombocytopenia – Low Platelet Count

RBC count- Decreased/Increased
Hemoglobin (120-160g/L)- decreased/ increased
Red Cell Indices
RBC morphology: ◦ Fragmented RBCs, Reticulocytes, erythroblasts cells
◦ abnormal shapes & sizes

Ratio RBC’s volume : WB expressed as %
Affected by RBC count & hydration status
Used to calculate indices
Low –Anaemia
High-polycythaemia/dehydration

Decreased production
Hemoglobin synthesis/Bone Marrow problem
Increased Destruction
Blood Loss/hemolysis

Relative Dehydration Absolute PHYSIOLOGICAL
HIGH ALTITUDE
ATHLETES
BODY BUILDERS
PREGNANCY

PATHOLOGICAL
Lungs Diseases ◦ COAD ◦ Sleep Apnoea
Poisoning ◦ CO intoxication
CVS disorders ◦ CHD/right-left shunt
Neurologic disease Renal disease ◦ CRF ◦ Renal artery stenosis ◦ Focal sclerosing or membranous glomerulonephritis ◦ Renal transplantation

High –polycythaemia , dehydration
Low-Anaemia

Calculated from RBC count, PCV & Hb
Includes
◦ Mean Cell Volume (80-90fl)
◦ Mean Cell Haemoglobin (27-32pg)
◦ Mean Cell Haemoglobin Concentration (310-
350g/L)

male female
Hematocrits [hct] % 47 42
RBC [10x6 / mcl] 5.4 4.8
Hemoglobin Hb [g/dL]
16 14
MCV [fl] = hct x 10 RBC [106 /mcl]
87 87
MCH [pg] = Hb x 10 RBC [106 /mcl]
29 29
MCHC (g/dL) = Hb x 100 hct
34 34

Microcytosis (Low MCV) ◦ Iron deficiency
◦ Thalassemia
◦ Lead poisoning
◦ Sideroblastic Anemia
Megaloblastic ◦ Folate & B12 deficiency (high MCV)

Hypochromic Normochromic Microcytic Normocytic


44

45

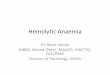
Central color spot in the area of pallor, Resembles a target. Cause: hemolytic anemias, especially sickle cell, HbC disease, and thalassemia.

47

48

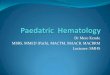
Almost spherical in shape; No area of central pallor Large spherocytes (macrospherocytes) -hemolytic anemia. Small spherocytes (microspherocytes) -severe burns. Other causes: hereditary.

50

51

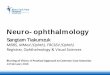
There are numerous fragmented RBC's seen here. Some of the irregular shapes appear as "helmet" cells. Indicates: microangiopathic hemolytic anemia (MAHA) or other cause for intravascular hemolysis.
DIC



◦ Involved in inflammatory response ‘killing zone’
Chemotaxis: attract Neutrophils to inflammatory site
Opsonization: -coding of bacteria with IgG, complement to activate Neutrophils
Phagocytosis/degranulation- ingestion and realase of chemical stored to ‘killing’ bacteria
Respiratory burst/free radical generation-activated N

Myeloperoxidase – convert Cl-, Br- and SCN- to potent acids (hypochloride)
Elastase/collagenase -digest collagen, wall off infection
Thromoxane/platelet aggregating factors/leukotrienes -vasoconstrict, isolate inflammatory response

Neutrophils – ingest bacteria & digest it (microphages)
Basophils-
◦ contain histamine and heparin. Role?
Eosinophils- ◦ attack parasites too large for attack by macrophages &
◦ produce leukotriene C4 & PAF-involved in allergic
reactions
◦ Abundant in mucosa of GIT, resp tract & lower UT

Neutrophil Eosinophil

Lymphocyte Basophil

Monocytes- ◦ Become Tissue macrophages /RES (kupfer cells),
osteclasts, microglia, multinucleated GC)
◦ Macrophages function as Neutrophils
◦ Activated by lymphokines (T-lymphocytes)
◦ M Secrete 100 different substances (PG, IL, CSF)

Neutrophilia
Eosinophilia
Lymphocytosis

Physiological ◦ Physical stress ◦ Emotional stress ◦ Pregancy
Infections ◦ Bacterial ◦ Fungal
Inflammatory conditions ◦ Connective tissue diseases ◦ Arthritis ◦ Dermatitis

Tissue necrosis eg AMI
Hemolyitic Anemia
Myeloproliferative Disorders
Drug Therapy-corticosteroids/cytokines
Leukaemia (early myeloid cells)

Decreased Production ◦ Drugs
◦ Bone Marrow Failure
Diseases ◦ Acute Leukeamia
◦ Myelodysplasia
Nutritional Deficiencies ◦ Vitamin B12 & folate

Increased destruction ◦ INFECTIONS

(1) Drugs,
(2) parasitic infections,
(3) allergic diseases,
(4) collagen vascular diseases,
(5) malignant neoplasms,
(6) hypereosinophilic syndromes

Viral infections ◦ EBV/infectious mononucleosis ◦ CMV infection ◦ HIV infection ◦ Pertusis ◦ Other viruses ◦ TB ◦ Brucellosis ◦ syphilis
Leukaemias (CLL) usually >10 000/ul
Endocrine Disorders (thyrotoxic, adrenal failure)
Absence of spleen

Bacterial infection
Early vital infection
Carcinoma
Drugs eg steroids/cytotoxics
HIV infection
Hodgkin’s Disease
Malnutrition

Leukaemia/infection/toxicity
Auer rods- leukaemia
Toxic granulation- severe infections
Hypersegmented neutrophils -megaloblasti c anaemia/severe bacterial infections
Atypical lymphocytes: viral/EBV infection
LE cells: SLE


2-4microns
Reference ranges: 150-400,000/mcL
Half-life -4 days; transfused survive 2-3 weeks
Derived from Megakaryocytes:
60-70% in circulation-rest mainly in spleen

Membranes-receptors (vWF, Gp 1b, IIa, IIIb)
Cytoplasmic granules: dense-serotonin &ADP, alpha-Clotting factors, PDGF
Healing Wound/Tissue Damage & Clot Formation

Megakaryoblast ◦ 20-50 microns
◦ Nucleus :cytoplasm (10:1)
Pomegakaryocytes ◦ 20-50microns
Megakaryocytes--- ◦ 40-100microns
Platelets (thrombocytes) ◦ 1-4microns

Hereditary/Primary/Essential (>2million/mcl)
Acquired/Secondary/Reactive ◦ Severe hemorrhage,
◦ iron & B12 deficiency,
◦ Surgery/splenectomy (transient)
◦ Malignancy (Hodgkin’s disease, polycythemia vera),
◦ Chronic inflammatory diseases (e.g., inflammatory bowel disease)
◦ Recovery from acute infection,
◦ Drugs (e.g., vincristine, epinephrine/cytotoxic/alcohol).

Hereditary vs Acquired
Bleeding Time is prolonged
Bleeding is unusual unless count < 20,000/μL;
Platelet count < 10,000/μL------associated with serious hemorrhage

Bone Marrow Failure” ◦ Drugs, irradiation/aplastic anaemia
◦ Marrow invasion (e.g., carcinoma, leukemia, fibrosis);
Sequestration due to splenomegaly;
Accelerated destruction— ◦ Drugs: thiazides, ethanol, estrogens, sulfonamides,
quinidine, quinine, methyldopa.
• Heparin-induced thrombocytopenia is seen in 5% of pts receiving >5 days of therapy

Autoimmune destruction SLE, lymphoma, HIV.
Idiopathic thrombocytopenic purpura (ITP)
DIC—platelet consumption & coagulation factor depletion [prolonged PT & aPTT)

Platelet Count (150-450,000/mcl)
Bleeding Time <6mins

1. LG Gomella. Clinician’s Pocket Reference 11th Edition
2. Harrisons Text Book 17th Edition
3. Despopoulos. Colour Atlas of Physiology 5th Edition

















![[Duke] MMED Menstrual Problems (Amended)](https://img.pdfslide.net/doc/110x75/577d25861a28ab4e1e9f02bc/duke-mmed-menstrual-problems-amended.jpg)








