Embed Size (px)
Citation preview

Dr Mohammed Al-UzriConsultant Psychiatrist &Honorary Senior Lecturer
A University Teaching Trust

ContentsBackground
IMHS
IASC Guidlines
Support from UK
Conclusion


BackgroundPopulation: estimated 30 millionnearly half of the population of Iraq are
under the age of 18. Breaking of social fabricDeterioration of education systemDeterioration of health system

Iraq Mental Health Survey“It is against the background of ongoing
insecurity situation in Iraq and the recognised need for the organisation of mental health services , the Iraq Mental Health survey was undertaken in order to insure policies and strategies are based on an evidence to support the development of services for persons with mental and psychosocial needs“
World Psychiatry8:2- June 2009
http://www.wpanet.org/news/2009/March/iraq-mental-health-survey.pdf

Iraq Mental Health SurveyThe methodology of the Iraq Mental Health Survey is
the same as the WHO World Mental Health Survey (WMH)
In all South/Centre governorates except Anbar governorate, fieldwork began on the 1st of August 2006, and completed on the 8th of September 2006. The fieldwork in Anbar governorate was delayed until the 1st of October 2006, due to the security problems, and was completed on the 17th of November 2006. In Kurdistan region, the survey began on the 1st of February 2007 and completed on the 11th of March 2007.
The data collection tool was Composite International Diagnostic Interview (CIDI).
Sample size: 4332

Composite International Diagnostic Interview (CIDI) CIDI is a fully structured lay administered
interview that generates both the ICD-10 and DSM-IV diagnoses. The disorders included:
anxiety disorder( panic disorder, agoraphobia without panic disorder, specific phobia, social phobia, generalised anxiety disorder (GAD),
post-traumatic stress disorder (PTSD), mood disorders ( major depressive disorder (MDD),
moderate depressive disorder, minor depressive disorder, dysthymic disorder, bipolar disorder I and II )
substance use disorders (alcohol and drug abuse with or without dependence).

Objectives of the Iraq Mental Health Survey to identify the prevalence (life time, 12 month and
30 day) of mental disorders among 18 years and older;
to find out the relationship between prevalence of mental disorders with trauma exposure and socio-demographic characteristics (age , gender, education… etc);
to identify the impact of mental disorders in the adult population 18 years and older ;
to assess the treatment utilisation by the persons with mental disorders;
to provide policy-and decision-makers and researchers with reliable, accurate and relevant data for the development of mental health care policies.

SUMMARY FINDINGSOverall 12 month prevalence rate is 13.6%Prevalence rate in females is more than in
malesAnxiety disorders is the most common mental
disorder group followed by mood disordersNo sex difference in the prevalence rate of
PTSDHigher prevalence rates in those 65 years
and aboveSome mental disorders have higher
prevalence rates in urban areasAny disorders is higher in the Kurdistan region
(14.13%) than in the south/centre (10.51%)

SUMMARY FINDINGSHigh rates of exposure to trauma in the
population (56%) Males (65%) are more exposed to
trauma than females (46%).Higher rates of exposure to trauma
among mentally ill personsHigher the exposure to trauma, greater
the chance of having mental disorder

SUMMARY FINDINGS2 out of 5 persons with mental disorders
express suicidal ideasPrevalence of suicidal ideas are higher in
females(53.80%) as compared to males(29.16%)
10.8% of respondents with one or more 12-month DSM-IV/CIDI disorders reported receiving treatment for emotional problems at any time in the 12 months before their interview

Rates of mental disorders-Comparison with other surveys in developing countries 12 month 12 month prevalence prevalence
IraqIraq LebanLebanonon
ChinaChina NigeriaNigeria
Affective Affective DisorderDisorder
4.14.1 6.66.6 2.22.2 1.31.3
Any Anxiety Any Anxiety disorderdisorder
PTSDPTSD
10.410.4
1.11.1
11.211.2
2.02.0
2.72.7
0.20.2
4.14.1
0.00.0
Any Any Substance Substance DisorderDisorder
0.20.2 1.31.3 1.61.6 0.80.8
Any DisorderAny Disorder 13.613.6 17.017.0 7.07.0 5.85.8

However,Stress and trauma are related concepts and
experiences at basic biological and psychosocial levels
Stress responses are normal reactions to abnormal situations and are not necessarily pathological.
Not everyone who experiences a stressful situation/ trauma develops PTSD or any other mental disorder.
There are numerous factors of resilience, most notably supportive families and communities and, by extension, international communities, which enable people to cope and even prevail in the face of adversity.

Posttraumatic Stress Disorder(PTSD)
Complex PTSD (Herman)
Ongoing Traumatic Stress Disorder(OTSD)
A: Stressor (experiencedor witnessed)Reaction of fear,helplessness,or horrorB: AnxietyC: DissociationD: HyperarousalE: NightmaresF: Flashbacks
Multiple traumas and stressors in childhoodSevere relationship impairmentsDisturbances of mood regulation(e.g., outbursts of anger)
Stress endures in timePerson experiences psychologicalsymptoms plus• physiological correlates• changes in vital signs:Temperature,Blood pressure,Heart rate,Respiratory rate, pain• endocrine/metabolicchanges• difficulty maintaininginternal milieu
From Dyer & Bhadra 2012

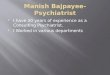
IASC Guidelines for mental health and psychosocial support in emergencies
IASC = Inter-Agency Standing Committee, established (1992) by UN General Assembly Forum to coordinate humanitarian responses to emergencies
Focus on community-based psychosocial support rather than a primary focus on treating individuals
community-level workers (CLW) trained in basic psychosocial aspects of care, with ongoing support of social workers, and medical professionals trained in disaster mental health to support those with more significant mental health needs.
http://www.humanitarianinfo.org/iasc/content/products
IASC Bodies Individual NGOs
ICVA IFRC InterAction IOM OCHA UNFPA UNHCR UNICEF WFP WHO
ACF MdM-EAmerican Red Cross Mercy CorpsAction Aid Int. MSF-HCARE Austria Oxfam GBCCF RETHealthNet TPO SC-UKIMC SC-USICMC ACT Int.INEEIRC

16
Specialisedservices
Focused,non-specialised supports
Basic services and security
Community and family supports

Layer 1 Basic services and security
The well-being of all people should be protected through the provision of basic needs in a way that is participatory, safe and socially appropriate No specific psychosocial or mental health activities, but of those basic activities that are necessary for any psychosocial wellbeing such as
- Basic information
– Legal position
– Primary health care services
– Work,
– Nutrition
– Shelter– Advocacy to decision makers to protect displaced population
– Coordination with other sectors

Layer 2 Community and family supports
Smaller number of people who are able to maintain their mental health and psychosocial well being if they receive help in accessing key community and family supports.
– Support and mobilize the community in re-establishing daily life and community activities. Train and support community members in psychosocial support, including effective coping mechanisms and discouraging harmful practices.
– Provide information to the population on the situation, assistance and effective coping mechanisms
– Train and supervise community workers
– Concentrate the above mentioned activities in multifunctional social centers or safe spaces, and ensure that the activities are run by both Iraqis, and by members of the host community

Layer 3: Focused, non-specialised supports
Support structures for people who require more individual, family or group interventions by trained and supervised workers who are not specialists in the domain of mental health and psychosocial support.
–Basic mental health and first aid psychosocial interventions in primary health care centres
–Psychosocial care for humanitarian workers
–Organize a system of caseworkers who are able to give psychosocial support to families and individuals. (training and supervision!)
–Referral

Layer 4: Specialised services.
Required for a small percentage of the population with complaints and symptoms are intolerable and causes severe dysfunction.
–Organising multidisciplinary mental health services in general health care where the population have easy access
–Organisation of psychological support for people with severe psychological reaction to current or past situations traumatic reactions that disrupt social functioning of family and or individual.
–Avoid programming that focuses solely on one single diagnosis (e.g. PTSD) or one single category beneficiaries.
–Integrate or attach such support to existing health, social or educational services

Role of UK’s DiasporaRelocate to Iraq
Formation of IMHF
Establishing Iraq Sub Committee, RCPsych (http://www.rcpsych.ac.uk/college/internationalaffairsunit/iraqsubcom.aspx)

Input of DiasporaBuilding Capacity (CPD/CME, ToT, supervision)Training Curriculum developmentIntegrating mental health into primary care
servicesIntroduction and development of Psychological
InterventionsService Development Al-Uzri, Abed & Abbas , International Psychiatry 2012http://www.rcpsych.ac.uk/college/internationalaffairsunit/
iraqsubcom.aspx

IMHS conclusion “the findings of the Iraq Mental Health
Survey showing significant prevalence of mental disorders, their association with trauma, their impact on the health status of the population and the currently very low level of medical treatment received by the ill individuals, calls for a concerted effort to develop community based mental health services in Iraq on a priority basis. “

ConclusionsStrong association between stress/ trauma
and mental health problemsExpect an increase in mental health problems
with reduction in violenceExpect different type of mental health
problemsTailor intervention to hierarchy of needsNeed to collaborate with relevant
organisations

Personal lessonsProtect yourself!Manage your expectationWork in teamsWork with local partnerCollaborate with othersProfessional neutrality