Embed Size (px)
Citation preview
DENGUE EPIDEMIOLOGY DENGUE EPIDEMIOLOGY AND CONTROL STRATEGYAND CONTROL STRATEGYAND CONTROL STRATEGYAND CONTROL STRATEGY
Dr Noor Rizawati MahpotPrincipal Assistant Director
Vector Borne Diseases Control and Prevention UnitPerak State Health Department
1

OUTLINES OF PRESENTATION
� Epidemiology of Dengue � Dengue Mortality � Dengue Mortality � Control Activities Strategies� Conclusion

NATIONAL DENGUE STATUS FOR 2012 Until 3rd March 2012 ( EW 9 )
• Cases: 4,680 cases with 16 deaths (4,093 cases with 8 deaths in 2010)� Increase of cases – 14%� increase of death – 100%
• Case Fatality Rate: 0.34% (0.18% last year)
• KPI (NDSP)� 10% reduction of cases annually� target CFR ≤ 0.2%
3

COMPARISON OF CASES 2011 AND 2012 (EW 08, 1st JAN UNTIL
25 FEB 2012)
MALAYSIAWEEKLY DENGUE CASES 2012
800
1000
1200
JUM
LA
H
KE
S
0
200
400
600
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
JUM
LA
H
KE
S
MINGGU EPID
Median 2007-2011 2011 2012
4
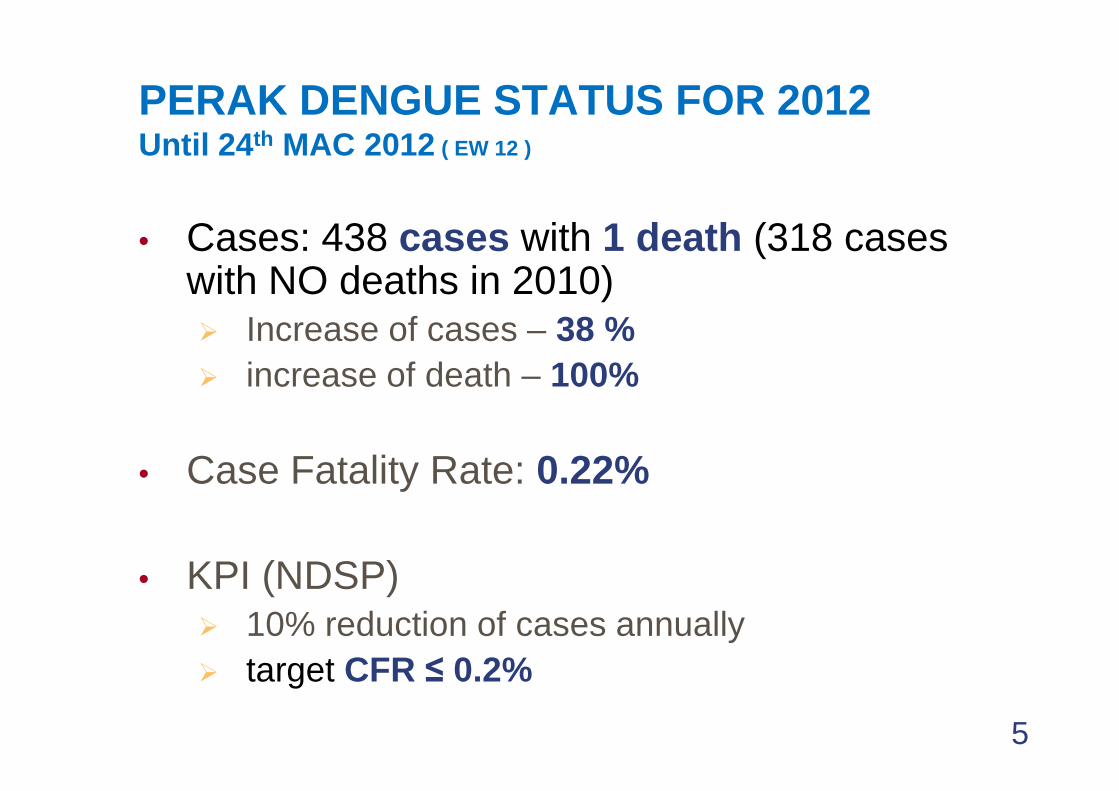
PERAK DENGUE STATUS FOR 2012 Until 24th MAC 2012 ( EW 12 )
• Cases: 438 cases with 1 death (318 cases with NO deaths in 2010)� Increase of cases – 38 %� increase of death – 100%
• Case Fatality Rate: 0.22%
• KPI (NDSP)� 10% reduction of cases annually� target CFR ≤ 0.2%
5

COMPARISON OF CASES 2011 AND 2012 (EW 12, 1st JAN UNTIL
24 MAC 2012)
PERAK WEEKLY DENGUE CASES 2012
70
80
90
100
6
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53
Ke
s
Minggu Epid2011 2012 median

DENGUE TREND IN PERAK, 2008-2011
10
20
30
40
50
60
70
80
90
100
Kes
2011
2010
median
0
10
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53
Minggu Epid
2008 2009 2010 2011 Percentage
CASES 4,256 2,732 2,288 1,411 -38.3%
DEATHS 8 3 6 2 -66.7%
OUTBREAKEPISODS
350 193 163 88 -46.0%
UNCONTROLLEDOUTBREAKS
22 4 7 1 -85.7%

DENGUE BY DISTRICTS, 2010-2011
K M K MKINTA 941 2 108 0 -66.2PERAK TENGAH 78 0 43 0 -44.9BATANG PADANG 195 1 129 0 -33.8HILIR PERAK 138 0 98 0 -29.0
2010 2011 % Penurunan Kes
DAERAH
HILIR PERAK 138 0 98 0 -29.0HULU PERAK 170 0 125 0 -26.5MANJUNG 264 0 207 0 -21.6LMS 166 0 132 0 -20.5KERIAN 67 0 60 0 -10.4KUALA KANGSAR 269 1 250 2 -7.1KAMPAR 0 0 49 0 0.0JUMLAH 2288 6 1411 2 -38.3

DENGUE IR PER 100,000 POP BY DISTRICTS, 2011
Hulu PerakHulu PerakHulu PerakHulu PerakIRIRIRIR : 111.0: 111.0: 111.0: 111.0CaseCaseCaseCase : 125: 125: 125: 125DeathDeathDeathDeath : 0: 0: 0: 0
K KangsarK KangsarK KangsarK KangsarIRIRIRIR : 145.0: 145.0: 145.0: 145.0CaseCaseCaseCase : 250: 250: 250: 250DeathDeathDeathDeath : 2: 2: 2: 2
LMSIR : 40.6 Case : 132 Death : 0
KerianIR : 31.9Case : 60Death : 0
ManjungManjungManjungManjung
KintaKintaKintaKintaIRIRIRIR : 42.5: 42.5: 42.5: 42.5CaseCaseCaseCase : 367: 367: 367: 367DeathDeathDeathDeath : 0: 0: 0: 0
Batang PadangIR : 69.3Case : 129Death : 0
ManjungManjungManjungManjungIRIRIRIR : 81.3: 81.3: 81.3: 81.3CaseCaseCaseCase : 207 : 207 : 207 : 207 DeathDeathDeathDeath : 0: 0: 0: 0
Perak TengahIR : 37.3Case : 43Death : 0
Hilir PerakIR : 43.9Case : 98Death : 0
National National National National IR = 69.6IR = 69.6IR = 69.6IR = 69.6
IR < 50/100,000IR < 50/100,000IR < 50/100,000IR < 50/100,000IR 50 IR 50 IR 50 IR 50 –––– 100/ 100,000100/ 100,000100/ 100,000100/ 100,000IR >100/100,000IR >100/100,000IR >100/100,000IR >100/100,000

DENGUE KPI INDICATOR 2010
2011TARGET
1. Percentage of cases which fulfills dengue case defination 93 93.9 100%
2.Percentage of registered cases confirmed by IgM serology test 75 52.7 <70%
3.Percentage of registered cases notified by Primary Health Care facilities 40 64.4 >85%
4.Percentage of cases registered within 3 days of case onset 43 58.1 >85%
5.Percentage of cases registered which has fogging activity done within 5 days of case onset 69 58.1 >85%
6. Percentage of outbreaks controlled by 2 weeks of onset 95 98.9 >85%
7. Percentage of annual registered cases reduction 16 38.3 >10%
8. Percentage of annual outbreak locality reduction 16 46.0 >25%
9. Case Fatality Rate (CFR)0.26
0.14 <0.2%
10. Percentage of preventable deaths reduction 0.0 0.0 >50%

CHARACTERISTICS OF DENGUE CASES IN PERAK , 2011
182
151 149160
180
200
AGE DISTRIBUTION
11
15
42
72
128
151 149
105 10790
98 100
6146
65
0
20
40
60
80
100
120
140
160
<1 1-5 6-10 11-15 16-20 21-25 26-30 31-35 36-40 41-45 46-50 51-55 56-60 61-65 > 65
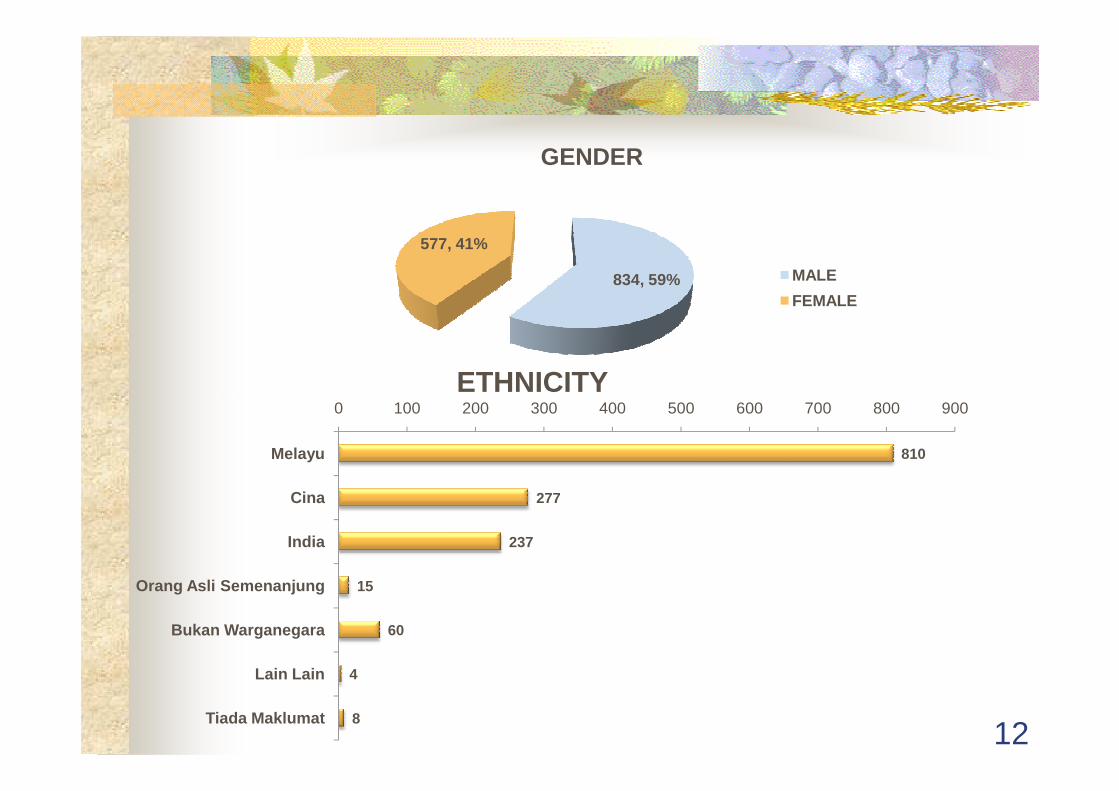
834, 59%
577, 41%
GENDER
MALE
FEMALE
ETHNICITY
12
810
277
237
15
60
4
8
0 100 200 300 400 500 600 700 800 900
Melayu
Cina
India
Orang Asli Semenanjung
Bukan Warganegara
Lain Lain
Tiada Maklumat
ETHNICITY

DENGUE DEATHS ANALYSIS FOR 2012ANALYSIS FOR 2012
13

PRIMARY CARE
ISSUESCases (n=10)
%
Failure to diagnose Dengue for cases presented with fever + 2 symptoms
5 50%
Mismanagement of cases• improper follow up e.g. case dx as URTI but daily f/u
for FBC review • improper referral e.g.
- patient was ask to go to hospital without referral 6 60%
- patient was ask to go to hospital without referral letter
- Referred to hospital with Dx URTI• Cases with wrong diagnosis – no f/u done
6 60%
Failure to notify-2 government clinics & 1 Private clinic
3 30%
Case of Dengue with warning signs –1 case - not reviewed by MO or Specialist in A&E @ 9.29pm
- admitted to the ward @ 10.30 pm, review by HO and only @ 2.30 am reviewed by specialist
1 10%
14

HOSPITALISSUES
Cases (n=10)
%
A&E Department
Case of Dengue with warning signs –1 case - not reviewed by MO or Specialist in A&E @ 9.29pm
- admitted to the ward @ 10.30 pm, review by HO and only @ 2.30 am reviewed by specialist
1 10%
WardWard
Dengue with warning signs, admitted to normal ward
4 40%
Delayed review by specialist (cases with warning signs) - (4 hrs, 5 hrs, 11 hrs and 15 hours)
4 40%
Not reviewed by specialist 1 10%
Delay in seeking ICU caree.g. Dx with warning signs - referred after 24 hrs and after 48 hrs
2 20%15

FACTORS CONTRIBUTING TO DEATH (FROM STATES MORTALITY REVIEW MEETING)
PRE ADMISSION FACTORS Cases
Presented with severe dengue (on admission) 7
Delayed in referral 1
Delayed in diagnosis 1
SEVERITY OF ILLNESS ON ADMISSION (Initial Diagnosis at A&E / OPD)
Cases
Dengue without warning signs 3
Dengue with warning signs (5 cases) or severe dengue (2 cases)
7
Delayed in diagnosis
16

FACTORS CONTRIBUTING TO DEATH (FROM STATES MORTALITY REVIEW MEETING)
IN PATIENTDelay in Diagnosis of Dengue with Warning Signs / Severe Dengue
Cases%
Delay in review by doctor 1 10%Delay in review by doctor 1 10%
Results delayed or not traced / not reviewed 0 0
Low index of suspicion 0 0
Inadequate monitoring of FBC and other blood investigations
2 20%
Inadequate monitoring of vital signs 1 10%
17

FACTORS CONTRIBUTING TO DEATH (FROM STATES MORTALITY REVIEW MEETING)
IN PATIENTPitfalls in management
Cases (n=10 cases)
%
Inadequate monitoring of FBC and other blood investigations
2 20%
Inadequate monitoring of vital signs 1 10%
Inadequate fluid resuscitation 2 20%
Delayed referral 1 10%
Bleeding not suspected / recognized 1 10%
Insufficient blood products given 1 10%
Delay in seeking ICU care 1 10%
Overloading / pulmonary edema 2 20%
18
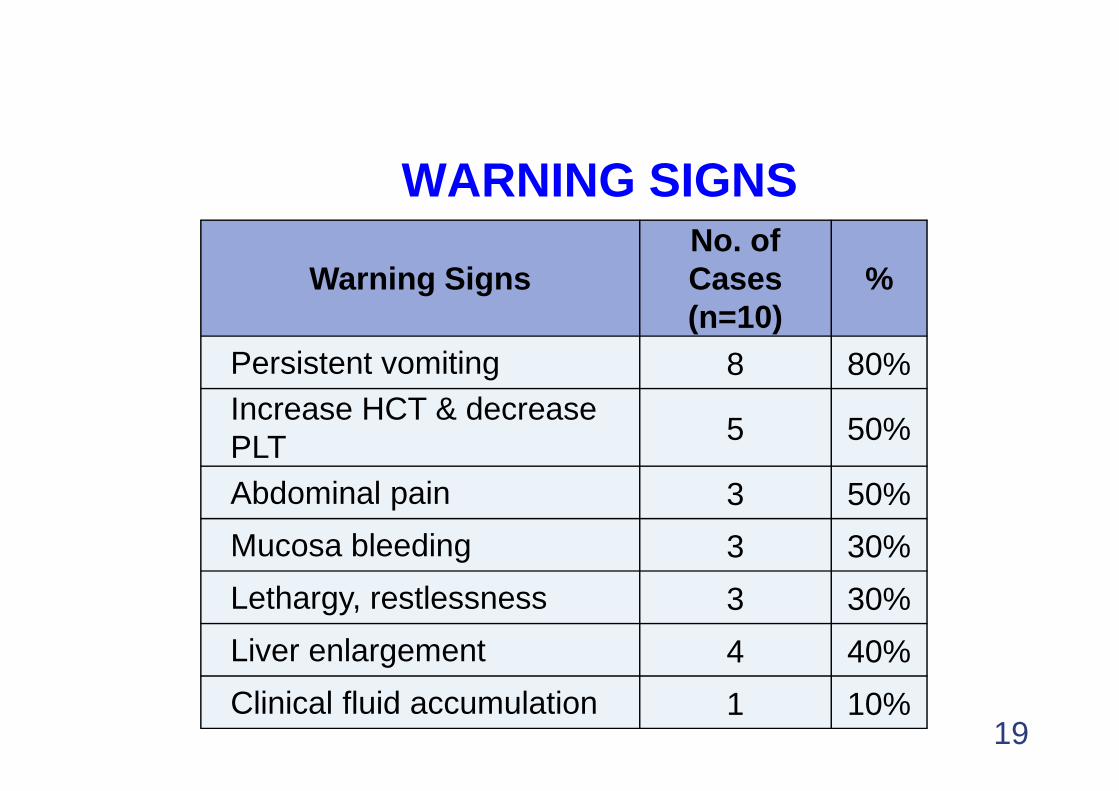
WARNING SIGNS
Warning Signs No. of Cases(n=10)
%
Persistent vomiting 8 80%Increase HCT & decrease Increase HCT & decrease PLT 5 50%
Abdominal pain 3 50%
Mucosa bleeding 3 30%
Lethargy, restlessness 3 30%
Liver enlargement 4 40%
Clinical fluid accumulation 1 10%19
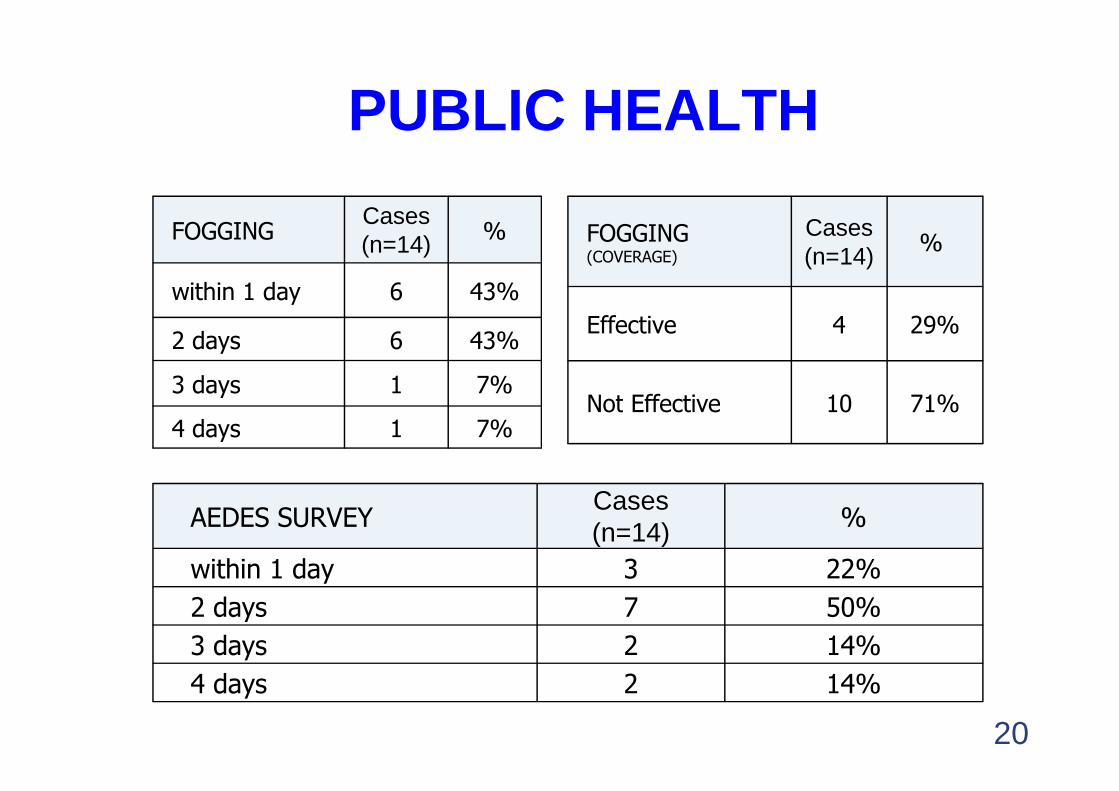
PUBLIC HEALTH
FOGGINGCases(n=14) %
within 1 day 6 43%
2 days 6 43%
3 days 1 7%
FOGGING(COVERAGE)
Cases(n=14) %
Effective 4 29%
Not Effective 10 71%3 days 1 7%
4 days 1 7%Not Effective 10 71%
AEDES SURVEYCases(n=14) %
within 1 day 3 22%
2 days 7 50%
3 days 2 14%
4 days 2 14%
20

PUBLIC HEALTH
AEDES SURVEY AT CASES RESIDENTIAL AREA
Cases (n=14)
%
AI ≤ 1% 6 43%
AI > 1% (2.9 - 18 %) 8 57%
Area with high Aedes IndexCases (n=8)
%
Gotong-royong carried out 5 62%
Gotong-royong Not carried out 3 38%
21

IS DEATH PREVENTABLE?(n=10)
YES 60% (6)
NO 20% (2)
NOT SURE 20% (2)
22

DISTRIBUTION BY GENDER(n=14)
23

DISTRIBUTION BY AGE GROUP
(n=14)(n=14)(n=14)(n=14)
42% (6) 42% (6) 42% (6) 42% (6) –––– aged aged aged aged between 5 to 19 between 5 to 19 between 5 to 19 between 5 to 19 years oldyears oldyears oldyears oldyears oldyears oldyears oldyears old
42% (6) 42% (6) 42% (6) 42% (6) –––– aged aged aged aged between 35 to 49 between 35 to 49 between 35 to 49 between 35 to 49 years oldyears oldyears oldyears old
14% (2) 14% (2) 14% (2) 14% (2) ---- ≥ 50 years ≥ 50 years ≥ 50 years ≥ 50 years oldoldoldold
24

DURATION BETWEEN ONSET AND 1ST
TREATMENT
(n=14)
85% of patients sought early treatment:early treatment:
� within 1 days from onset - 64% (9)
� 85% within 3 days from onset
25

TYPES OF HEALTH FACILITIES :PATIENT WENT FOR THE 1ST TREATMENT
(n=14)(n=14)(n=14)(n=14)
71% (10) 71% (10) 71% (10) 71% (10) –––– sought sought sought sought 1st treatment at the 1st treatment at the 1st treatment at the 1st treatment at the 1st treatment at the 1st treatment at the 1st treatment at the 1st treatment at the primer clinic primer clinic primer clinic primer clinic (private or (private or (private or (private or government).government).government).government).
50% (7) – Private Clinic
26
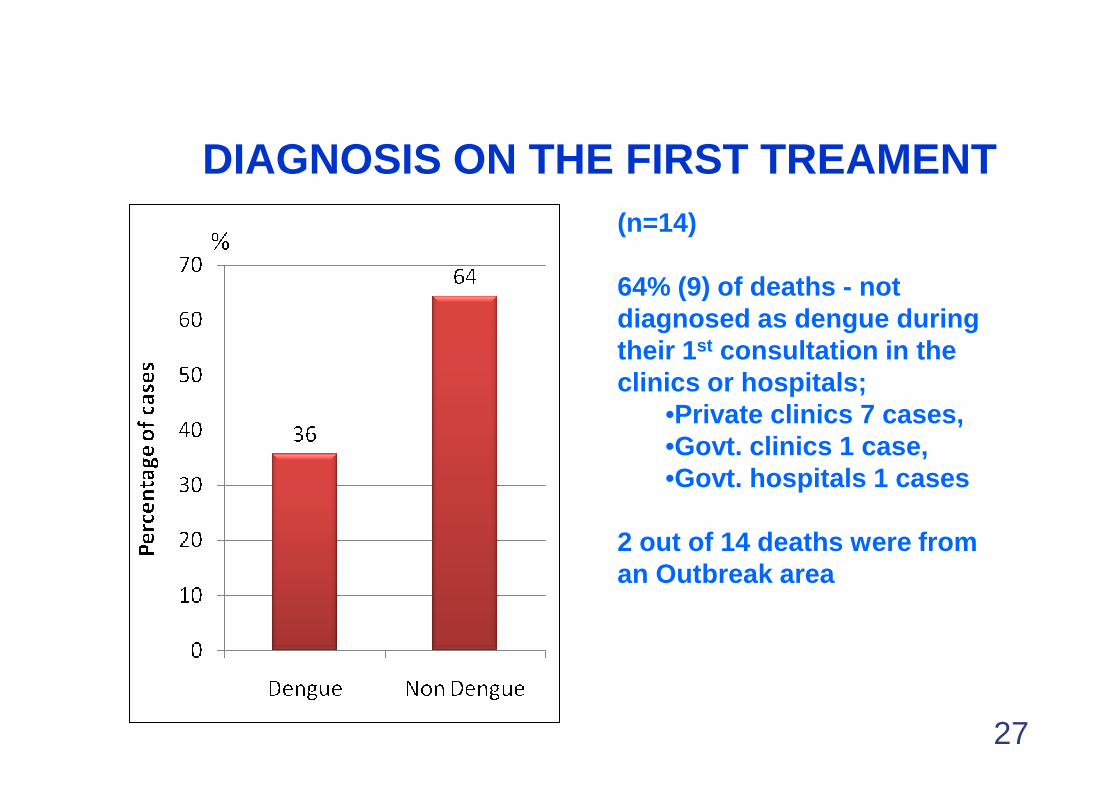
DIAGNOSIS ON THE FIRST TREAMENT(n=14)
64% (9) of deaths - not diagnosed as dengue during their 1st consultation in the clinics or hospitals;clinics or hospitals;
•Private clinics 7 cases, •Govt. clinics 1 case, •Govt. hospitals 1 cases
2 out of 14 deaths were from an Outbreak area
27

NUMBER OF CONSULTATION BEFORE ADMISSION
(n=14)
36% (5 patients) -
more than twice
consultation consultation
before admission
28

DURATION BETWEEN ADMISSION AND ONSET OF DISEASE
(n=14)(n=14)(n=14)(n=14)
93% (13) of the 93% (13) of the 93% (13) of the 93% (13) of the patients admitted patients admitted patients admitted patients admitted ----patients admitted patients admitted patients admitted patients admitted ----within 5 days from within 5 days from within 5 days from within 5 days from onset onset onset onset
29
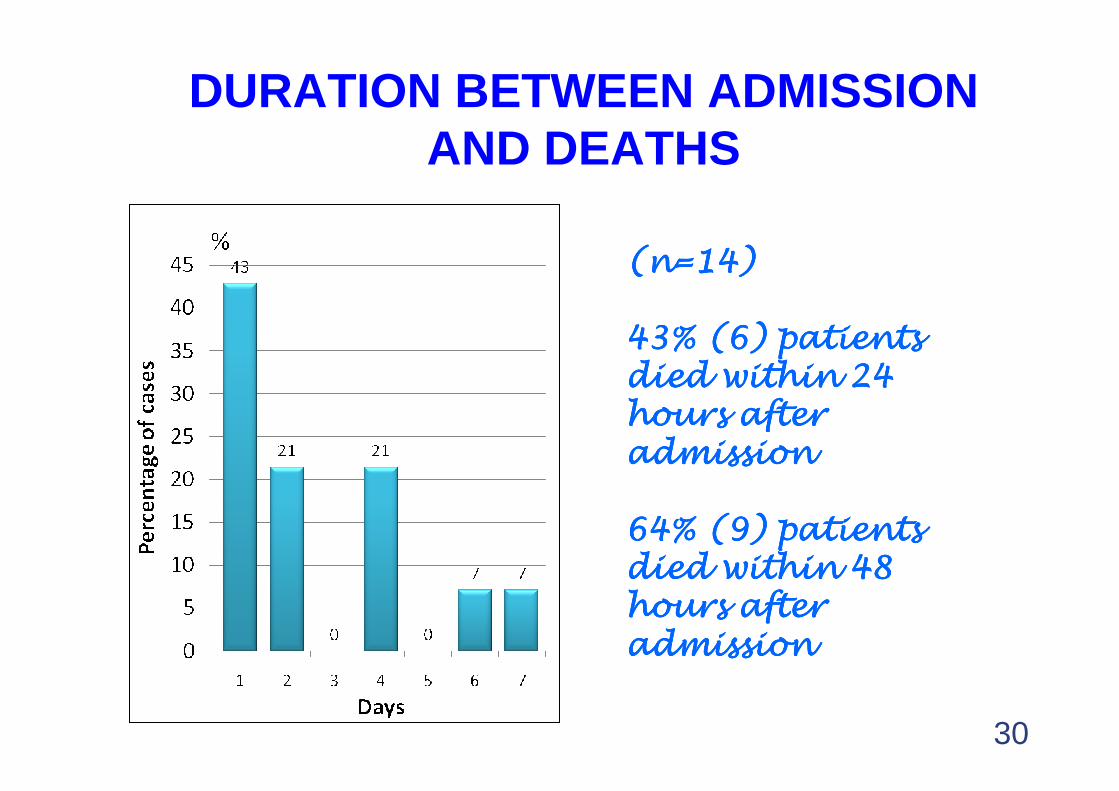
DURATION BETWEEN ADMISSION AND DEATHS
(n=14)(n=14)(n=14)(n=14)
43% (6) patients 43% (6) patients 43% (6) patients 43% (6) patients died within 24 died within 24 died within 24 died within 24 hours after hours after hours after hours after died within 24 died within 24 died within 24 died within 24 hours after hours after hours after hours after admissionadmissionadmissionadmission
64% (9) patients 64% (9) patients 64% (9) patients 64% (9) patients died within 48 died within 48 died within 48 died within 48 hours after hours after hours after hours after admissionadmissionadmissionadmission
30

CIRCULATING DENGUE VIRUS SEROTYPE:
31

ROLES OFPRIMARY CARE DOCTORS
1. To be updated with Dengue status in their localities e.g. number of cases and out-break localities.
2. Able to recognize warning sign and to
32
2. Able to recognize warning sign and to diagnose Dengue.
3. To provide the optimum treatment based on Clinical Practice Guidelines.
4. Dengue cases with warning signs must be referred to hospital (Pekeliling KPK Bil23/2010, 13 Oct 2010)
ROLES OFPRIMARY CARE DOCTORS
5. Dengue cases treated as an out patient, must be provided with “Rekod Pemantauan PesakitDenggi dan Panduan Penjagaan di Rumah”.
6. All confirmed or suspected Dengue cases compulsory to be notified to the nearest District Health Office within 24 hours after been Health Office within 24 hours after been diagnosed.
7. To give advice and provide health education on Dengue prevention, to patient and local community
8. To give full cooperation to the Health Department in matters related to Dengue

ROLES OF PHYSICIANS
1. To provide an optimum treatment for the Dengue cases based on Clinical Practice Guidelines.
2. To ensure the HO, MO and their subordinates able to recognized warning signs and complications of Dengue.
3. To review all dengue cases that treated and admitted 3. To review all dengue cases that treated and admitted to the ward.
4. To ensure that all the Dengue cases be closely monitored.
5. The attending or the physician in charge of death case, to inform the Director General of Health, Deputy Director General of Health (PH) and the Director of Disease Control within 24 hours via SMS, on the deaths case (Pekeliling KPK Bil 15/2010, 24 May 2010)

ROLES OF PHYSICIAN6. To notify all the confirmed or suspected Dengue
cases to the nearest District Health Office.7. To set up a Dengue Management Team in all
hospitals.8. To set up a Dengue ward or cubical and high 8. To set up a Dengue ward or cubical and high
dependency ward or area in all hospitals.9. To ensure all dengue cases will be monitored
closely and managed properly using the DENGUE CARE CHART and the CLERKING SHEET FOR SUSPECTED DENGUE CASES

ROLES OF PHYSICIANS10. To conduct trainings on Dengue Cases
Management to all health personnel 11. To conduct a Mortality Review for all
Dengue death and submit the report within 1 Dengue death and submit the report within 1 week (Dengue DIX./11/2006 Rev2).
12. To give advice and provide health education to the patient and local community on Dengue preventions.

Super-efficient vector
�Breeds near humanBreeds near humanBreeds near humanBreeds near human�TransTransTransTrans----ovarialovarialovarialovarial transmissiontransmissiontransmissiontransmission�Transmission occurs up to 5Transmission occurs up to 5Transmission occurs up to 5Transmission occurs up to 5thththth
generation generation generation generation

Key Components of Dengue Control Strategy� Early diagnosis and treatment
� Training of frontliners� Health education to public on importance of early diagnosis
and treatment� Active case detection in outbreak localities
� Prompt notification� Within 24 hours � Within 24 hours � By phone� Nearest District Health Office� Case Investigation within 24 hours
� Prompt vector control response� Within 24 hours of notification� Fogging within 200 m radius� 400 m if outbreak locality� Quality Assurance Program -Dengue Outbreak Control
Index (DOCI): 100% outbreak controlled within 14 days

Key Components of Dengue Control Strategy
� Proper Case Management� CPG- The Management Of Dengue Infection In
Adult/Children (2nd Edition revised 2010)� All dengue death are audited immediately.� Appropriate remedial actions are taken by the relevant
parties and report to be sent to the Disease Control parties and report to be sent to the Disease Control Division within 2 weeks
� Health Education And Community Mobilization� Production of health materials/ mass media� Guidelines on health education and community
mobilization activities in outbreak localities� Guidelines on COMBI For Dengue Prevention and
Control

CHALLENGES IN THE DENGUE PREVENTION ACTIVITIES
� Health seeking behavior of the dengue patient:�Only 4% of cases were from the clinic and majority
from hospital�50% of the dengue mortality cases were admitted on
day 4 or 5 after onset - delay in seeking treatment �47% of dengue mortality cases came in already ill
40
� Difficult to break the dengue virus transmission:� Only 35% of patient diagnosed within 3 days from the
onset of illness� Only 19% of dengue cases’ residence were fogged
within 5 days of onset of illnessThus other patients infected with the dengue virus may still transmit the disease

CHALLENGES IN THE DENGUE PREVENTION ACTIVITIES
� Low index of suspicion of dengue cases by the attending doctors:
�Delayed notification�Delay in giving appropriate treatment
41
Delay in giving appropriate treatment
� Lack in community cooperation and participation in the dengue prevention and control activities

CONCLUSION-1
� To strengthen the implementation of dengue prevention and control measure (to be alert and responsive)
Ensure effective and efficient � Ensure effective and efficient performance of the control activities through:
�Monitoring & supervision�Analysis of data at district, state, and
MOH level
CONCLUSION-2
� Strengthen the prevention and control activities at district and state level
� Facilitate training for healthcare workers to increase knowledge and skills on the to increase knowledge and skills on the dengue management and vector control
� Continuous monitoring of dengue status and mortality at all levels, as to address uncontrolled situation of the disease

THANK YOU FOR YOUR ATTENTIONATTENTION
44