Embed Size (px)
Citation preview

MATERNAL MORTALITYIssues, Challenges & The Way
Forward
By
DR. PARAMJOTHI. P (FRCOG)Senior Consultant Obstetrician &
GynaecologistHospital Selayang
1


STATES 2009 2010 2011 (Jan. – June)
Perlis 1 3 0
Kedah 20 20 4
P. Pinang 11 13 3
Perak 18 14 8
Selangor 52 40 19
F. T KL 10 9 2
F. T Putrajaya 0 0 1
N. Sembilan 4 10 5
Melaka 3 4 7
Johor 37 25 16
Pahang 12 18 9
Terengganu 12 14 3
Kelantan 20 18 9
Sabah 67 56 32
Labuan 0 1 0
Sarawak 27 28 12
MALAYSIA 294 273 142
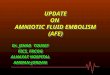
NUMBER OF MATERNAL DEATHS NOTIFIED TO MOH, 2009-2011 (J-J)

Maternal Deaths by Ethnic Specific
MMR in Others, Other Bumiputera, Malay & Indian are double the rate among Chinese

Source: CEMD, MoH


7
MATERNAL MORTALITY CHALLENGE
MDG 5 : IMPROVE MATERNAL HEALTH
Target 5A :
Reduce by three-quarters between 1990 and 2015, the maternal mortality ratio
Indicators :-Maternal mortality ratio-Proportion of birth attended by skilled health

8
MATERNAL MORTALITY CHALLENGE
MDG 5 : IMPROVE MATERNAL HEALTH
Target 5B :
Universal access to reproductive health by 2015
Indicators :-Contraceptive prevalence rate-Adolescent birth rate-Antenatal care coverage (1st visit & 4th visit)-Unmet need for family planning


MATERNAL MORTALITY ISSUES
HIGH RISK GROUPS
Remote communities
Orang Asli
Illegal immigrants
High Risk Pregnancies
Previous Near Misses
10
Special AttentionClose monitoring

11
MATERNAL MORTALITY ISSUES
HOME DELIVERIES
Low Risk..??
Screening – M.O
Tragedies Maternal Deaths
Trained / Untrained birth attendants

12
MATERNAL MORTALITY CHALLENGE
ALL DELIVERIES AT:
Hospitals
Low Risk Centres
Birth Centres

MATERNAL MORTALITY MALAYSIA
Per 100,000 live births
•1950 - 530
•1970 - 148
•1990 - 20
*Confidential enquiries started 1991
•1991 - 44.0
•1992 - 47.9
•1993 - 45.8
•1994 - 39.0
•2008 - 25.013

MATERNAL MORTALITY MALAYSIA
1992 – 1993
Place of Delivery
Home - 53.4 per 100,000
Government Hospitals - 36.1 per 100,000
Private Institutions - 20.7 per 100,000
*Home deliveries ~ 5 x more risk.
14

15

POSTPARTUM HAEMORRHAGE - Mx
Obstetric haemorrhage is one of leading causes of
deaths in pregnancy.
Prevention of mortality from haemorrhage mainly
depends on
PROMPT TREATMENT
of its cause to prevent further bleeding and
REPLACEMENT of BLOOD LOSS
to maintain the
CIRCULATION
16

POSTPARTUM HAEMORRHAGE - Mx
CAESAREAN SECTION
17

POSTPARTUM HAEMORRHAGE – Mx
4 Components undertaken SIMULTANEOUSLY
1. Communication
2. Resuscitation
3. Monitoring and Investigation
4. Arresting the bleeding
18

POSTPARTUM HAEMORRHAGE – Mx
Treat the Cause:
Atonic uterus - 80%
Injuries - Genital Tract
Retained placenta
Placenta Accreta / percreta
Inversion of uterus
Rupture uterus
Disseminated Intravascular Coagulation (DIVC)
19

POSTPARTUM HAEMORRHAGE – Mx
Atony - Hysterectomy20

POSTPARTUM HAEMORRHAGE – Mx
Uterus - Repaired
21

SM08.222

23
ILLEGAL IMMIGRANTS
Major contributor-MM
No antenatal visits
Refuse Hospital Mx
Brought in TOO LATE
Arrested
Charged first class fees
MATERNAL MORTALITY ISSUES
Laws – charged

24
MATERNAL MORTALITY ISSUES
HEART DISEASE
One of leading causes
Mortality high Severe cases
Cyanotic Heart disease
Pre-pregnancy Counselling
BTL / Vasectomy
Adoption Fast track

25
POSTNATAL HOME VISITS
Fulfilled Quantity
Quality poor
Hospitals = Public Health
Well trained staff
Early pickup Hospitals
Family aware
MATERNAL MORTALITY ISSUES

26
HOSPITALS WITHOUT SPECIALISTS -1
Emergencies poorly Mx
Delays, indecisions
No specialist involment
No facilities eg: O.T
MATERNAL MORTALITY ISSUES

27
HOSPITALS WITHOUT SPECIALISTS -2
Upgrade
Post Obstetricians – enough being trained
Direct contact with Tertiary Centre
O.T facilities / Trained staff
Resusciate Transfer
Specialist Hospital
MATERNAL MORTALITY CHALLENGE

28
POSTMORTEMS - 1
Confidential Enquries – U.K - Success
Diagnosis / Cause of death - unknown
Home deaths / Dead on arrival
Medico - Legal
Clinicians / Forensic Pathologist
Police
Consent
MATERNAL MORTALITY ISSUES

29
POSTMORTEMS - 2
Compulsory
Coroner’s case
Immediately done
MATERNAL MORTALITY CHALLENGE

30
MATERNAL MORTALITY ISSUES
PATIENT FACTORS
Unbooked cases
Non – compliance to advice
Non – compliance to admission
Non – compliance to therapy
Ignorant; not educated
Migration

31
MATERNAL MORTALITY CHALLENGE
PATIENT FACTORS
Improve Patient Education
Patient Education to Effective care
Empower patients
Improve awareness
Tab on migrations
Compulsory Antenatal Care

32
MATERNAL MORTALITY ISSUES
REMEDIABLE CLINICAL FACTORS
Failure to inform seniors
Failure of combined care (Team)
Failure of communication
Failure to diagnose
Failure to appreciate severity
Inadequate, inappropriate or delayed therapy

33
OBSTETRICIANS
Resident
NHS Consultant in Labour SuiteShifts
Preform Difficult LSCS
Consultant involvement early / called-in
Obstetric Hysterectomies
MATERNAL MORTALITY RECOMMENDATIONS

34
MORBIDITY REDUCTION
No statistics
Numerous near misses
Need investigations
To reduce MMR
MATERNAL MORTALITY CHALLENGE
SeriousMorbidity
Mortality

35
RED ALERT SYSTEM
High power team - Obstetrician- Anaesthetist- Paediatrician- Blood bank- Haematologist
Alerted immediately
Every Hospital - Compulsory
PA system / Operators
MATERNAL MORTALITY CHALLENGE

36
OBSTETRIC FLYING SQUAD
High Quality Team (with Doctor)
Immediate response
Resusciate
Transport to Hospital
Helicopters – remote areas
MATERNAL MORTALITY CHALLENGE

37
MATERNAL MORTALITY PROGRESS
MDG 5 : IMPROVING MATERNAL HEALTH
MMR decline from 44 deaths per 100,000 LB (1991) to 27.3 (2008) and plateau
Contraceptive prevalence rate 52% (1984) decline to 51.9% (2004)
Proportion of births attended by skilled health personnel increased from 74.2% (1990) to 98.6% (2009)
Adolescent birth rate 28 births per 1,000 adolescents age 15-19 years (1991) to 13 (2007)
Antenatal care coverage at first visits 78% (1990) to 93.7% (2008)


PPH as a cause of maternal death (projected), 1991 - 2015
39
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
Postpartum Haemorrhage 61 52 58 58 60 44 31 35 28 31 27 21 16 25 17 24 24 27 20 16 11 8 5 1 0
0
10
20
30
40
50
60
70
To
tal
Year

1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Hypertensive Disorders in Pregnancy
46 29 39 37 31 30 24 32 24 13 18 18 18 12 20 22 25 14 10 8 7 5 3 1 0
0
5
10
15
20
25
30
35
40
45
50
To
tal
Year
HDP as a cause of maternal death (projected), 1991 - 2015
40

41
MATERNAL MORTALITY CHALLENGE
QUALITY MATERNAL CARE
To formulate a structured credentialing and privileging process
- for nurses and doctors who manage pregnant women in health centres & district Hospital without specialist
Advanced Diploma in Midwifery
To improve the manpower norms for MO’s and Specialist in O&G in all Hospitals

42
MATERNAL MORTALITY CHALLENGE
PRE-PREGNANCY CLINICS
To start a pre-pregnancy clinic for high risk mothers in hospitals and health centres
Establishing and running of pre-pregnancy clinics in every specialist hospital and major health centres

43
MATERNAL MORTALITY CHALLENGE
OBSTETRIC MEDICINE PHYSICIAN
To train more physicians in Obstetric Medicine and get more obstetrician in maternal medicine
Starting a sub-specialty in Obstetric Medicine and giving emphasis in maternal medicine among maternal fetal medicine specialists

44
MATERNAL MORTALITY CHALLENGE
CONTRACEPTION
Make available contraceptive methods in hospitals, beside health clinics.
Budget to allocate for contraceptive methods in hospitals
Enforce/increase promotion of FP in daily practice – out & in patient setting
Provision of health educator to promote FP-hospital & health clinic
Increase patient awareness and empowerment
Utilize patient information leaflets / checklist to enhance health education / patient empowerment
Increase HO awareness in FP
Include MEC as one of the ‘must read’ materials for O&G Houseofficerinclude this topic in O&G HO assessment

45
CONFIDENTIAL INQUIRIES - UK
1. Pre-Pregnancy Counselling
2. Professional interpretation services
3. Communications and referrals
4. Women with potentially serious Medical Condition require immediate and appropriate multidisciplinary specialists care
5. Clinical skills and training
MATERNAL MORTALITY RECOMMENDATIONS

46
CONFIDENTIAL INQUIRIES - UK
6. Specialist clinical care: identifying and managing very sick women.
7. Systolic hypertension requires treatment.
8. Genital tract infections / sepsis
9. Serious Incident Reporting and Maternal Deaths
10. Pathology
MATERNAL MORTALITY RECOMMENDATIONS

47
MATERNAL MORTALITY DIRECTIVES
DG’s EXPECTATIONS...WE MUST
There should not be more than 45 maternal deaths nationwide.....By 2015
All midwifery trained staff will be placed in O&G facilities both in the hospital and health side.....By end of 2011
Contraception is to be made available to all women of reproductive age without unnecessary hassle or questions.....By end of 2011

48
MATERNAL MORTALITY DIRECTIVES
DG’s EXPECTATIONS...WE MUST
Be competent in knowledge and skills
Be community motivators and leaders
Promote practices that are beneficial to mothers and their newborns
Be able to supervise and monitor

49
MATERNAL MORTALITY DIRECTIVES
DG’s EXPECTATIONS...WE MUST
Reaching the MDG 5 targets will require a clear commitment from “US”
We have the power to make profound impact
Women, families and the nation is counting on us to DELIVER on time

ACTIVITIES AND TARGET
NO. ACTIVITY INDICATOR TARGET 2011
1. Antenatal care i. % coverage new antenatal mothers
ii. % coverage antenatal mothers at 36 POG
>90.0%
2. ANC at 1st visit % of antenatal mothers seen<12 wks POG
>70.0%
3. Screening for HIV & Syphilis % antenatal mothers screened 100% (MOH)
4. ATT immunisation (MOH) % coverage ATT >80.0%
5. Anemia in pregnancy % pregnant mothers with Hb <11 gm% at 36 wks POG
<19.5%
6. SRH status of PLKN trainee % of trainee detected pregnant and referred to health clinic
100.0%
7. Surveillance of pregnant adolescents
% pregnant adolescents among new antenatal cases
Monthly report
50

CONT….NO. ACTIVITY INDICATOR TARGET 2011
8. Safe deliveries % deliveries conducted by trained personnels
> 99.0%
9. Safe deliveries among pregnant adolescents
% registered pregnant adolescents delivered by trained personnel
100.0%
10. Home visits/nursing of postnatal mothers by health staff (hospital/home)
% postnatal mothers visited on the 2nd or 3rd day after delivery
100.0%
11. Maternal mortality (KPI) Maternal mortality ratio < 25/100,000
12. Maternal mortality surveillance Notify within 48 hrs 100.0%
13. Review and follow-up maternal deaths (PPH, HDP , Hrt Dis)
Report In one month
14. Death among pregnant single mother
No. of death No death
51

STRATEGIES TO ACHIEVE MDG 5
No. Strategy
1.
2.
3.
4.
5.
6.
Strengthen referral, feedback and retrieval systems
Skills training of health care providers
Advocacy on health to women in reproductive age
groups
Family planning for high risk mothers
Implementing pre-pregnancy care
Strengthening access to sexual and reproductive
health information and services for the under
privileged groups
52

53
THANK YOU