Embed Size (px)
Citation preview
1
SurgeryNotesDr.YasserAlDuraziNotes+GSnotes
Thyroid:..................................................................................................................................2
Acuteabdomen:.....................................................................................................................9
HepatobiliarySystem:...........................................................................................................11
Pancreatitis:..........................................................................................................................17
ColonCancerandPolyps:......................................................................................................21
Anus:.....................................................................................................................................25
Upper&LowerGIBleeding:..................................................................................................26
Hernia:1...............................................................................................................................29
BreastCancer:.......................................................................................................................34
Carcinoidtumor:...................................................................................................................37
DiabeticFootandUlcers:.......................................................................................................38
Appendicitis:.........................................................................................................................39
Cellulitis:...............................................................................................................................40
SalivaryGlands:.....................................................................................................................41
Sutures:.................................................................................................................................42

2
Thyroid:Thyroidhistory/midlineneckswelling.
• Whendidyoufirstnoticethemass?• Progressionofthemass?• Anyotherswellings?• Anyassociatedsymptoms(askaboutcompressionsymptomsdyspnea,dysphagia,etc)
andpain?• Askabouthypothyroidandhyperthyroidsymptoms• Familyhistoryofthyroiddiseases(thyroidcancer,Hashimoto’sandGraves’disease)• Radiationexposure• Anymedications?• Askaboutfever,nightsweatsandweightlosstoexcludeotherddx
Thyroidexamination:NeckInspection:
• Askthepatienttoswallowandprotrudethetongue,askthepatienttheraisehandsovertheheadandmaintainit2-3minutes(withretrosternalmasstherewillobstructiontotheSVC)“Pemberton’ssign”
Palpation:• Palpatethetracheaforanydeviation• Palpatethemass(describeit)• Palpatethelymphnodes
AuscultationforbruitswiththeBELL!PercussionforretrosternalthyroidEyes:
• Lidlag• Exophthalmos• Extraocularmovement
Hands:• Inspectforacropachy/palmarerythema• Palpatethepulse,feelforwarmthandsweating• Askthepatienttoclosehiseyesandextendhisarmsandputapapertolookfor
tremors• Lookforproximalmuscleweakness“Graves”
Lowerlimbs:• Lookforpretibialmyxedema• Reflexes
3
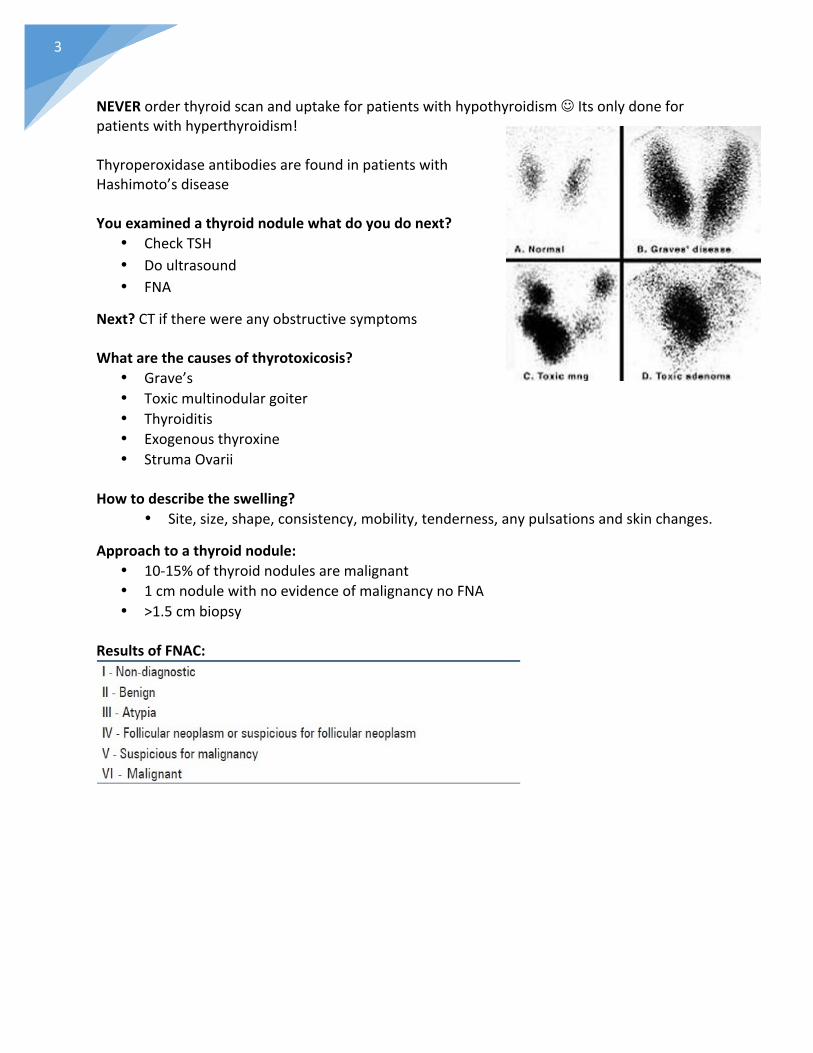
NEVERorderthyroidscananduptakeforpatientswithhypothyroidismJItsonlydoneforpatientswithhyperthyroidism!ThyroperoxidaseantibodiesarefoundinpatientswithHashimoto’sdiseaseYouexaminedathyroidnodulewhatdoyoudonext?
• CheckTSH• Doultrasound• FNA
Next?CTiftherewereanyobstructivesymptomsWhatarethecausesofthyrotoxicosis?
• Grave’s• Toxicmultinodulargoiter• Thyroiditis• Exogenousthyroxine• StrumaOvarii
Howtodescribetheswelling?
• Site,size,shape,consistency,mobility,tenderness,anypulsationsandskinchanges.
Approachtoathyroidnodule:• 10-15%ofthyroidnodulesaremalignant• 1cmnodulewithnoevidenceofmalignancynoFNA• >1.5cmbiopsy
ResultsofFNAC:
4
Thyroidhormonesynthesis:
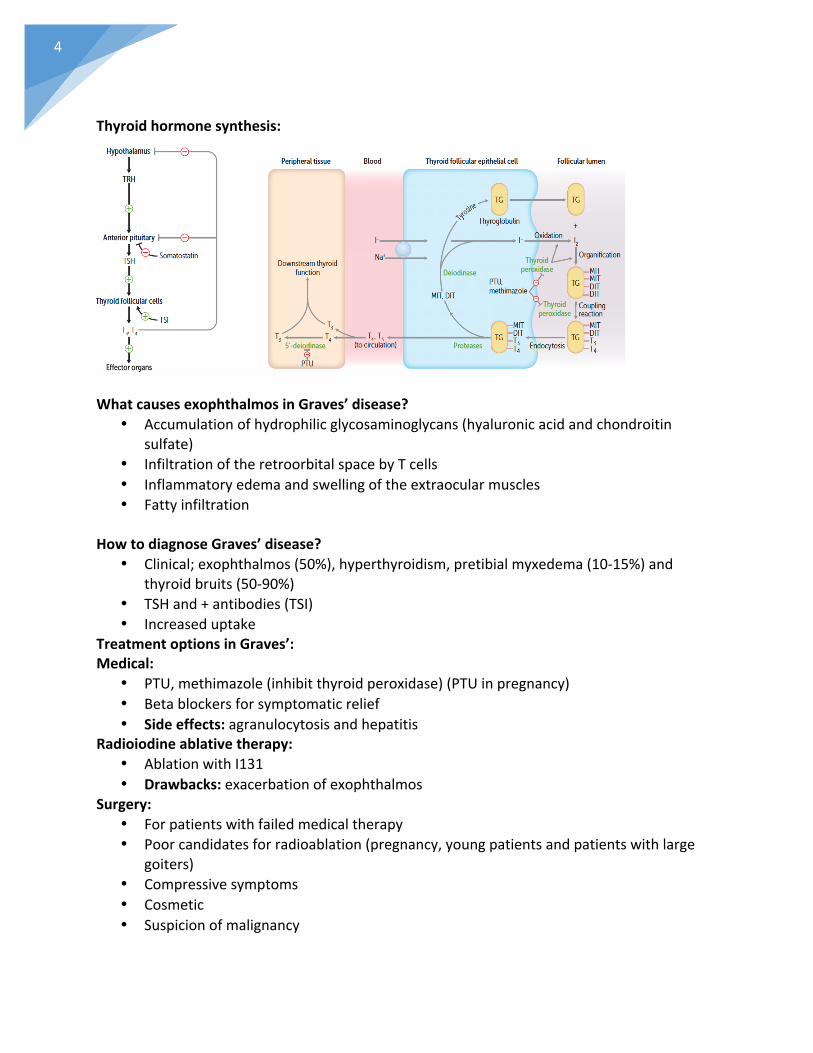
WhatcausesexophthalmosinGraves’disease?
• Accumulationofhydrophilicglycosaminoglycans(hyaluronicacidandchondroitinsulfate)
• InfiltrationoftheretroorbitalspacebyTcells• Inflammatoryedemaandswellingoftheextraocularmuscles• Fattyinfiltration
HowtodiagnoseGraves’disease?
• Clinical;exophthalmos(50%),hyperthyroidism,pretibialmyxedema(10-15%)andthyroidbruits(50-90%)
• TSHand+antibodies(TSI)• Increaseduptake
TreatmentoptionsinGraves’:Medical:
• PTU,methimazole(inhibitthyroidperoxidase)(PTUinpregnancy)• Betablockersforsymptomaticrelief• Sideeffects:agranulocytosisandhepatitis
Radioiodineablativetherapy:• AblationwithI131• Drawbacks:exacerbationofexophthalmos
Surgery:• Forpatientswithfailedmedicaltherapy• Poorcandidatesforradioablation(pregnancy,youngpatientsandpatientswithlarge
goiters)• Compressivesymptoms• Cosmetic• Suspicionofmalignancy
5
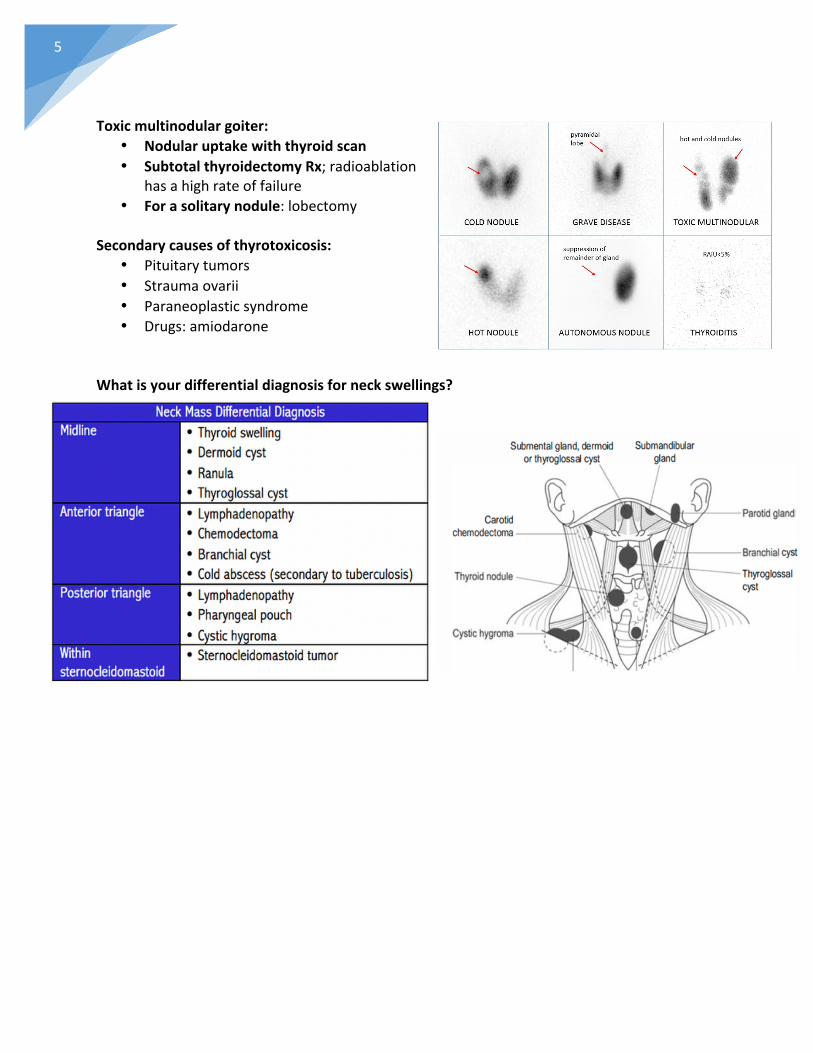
Toxicmultinodulargoiter:
• Nodularuptakewiththyroidscan• SubtotalthyroidectomyRx;radioablation
hasahighrateoffailure• Forasolitarynodule:lobectomy
Secondarycausesofthyrotoxicosis:
• Pituitarytumors• Straumaovarii• Paraneoplasticsyndrome• Drugs:amiodarone
Whatisyourdifferentialdiagnosisforneckswellings?
6
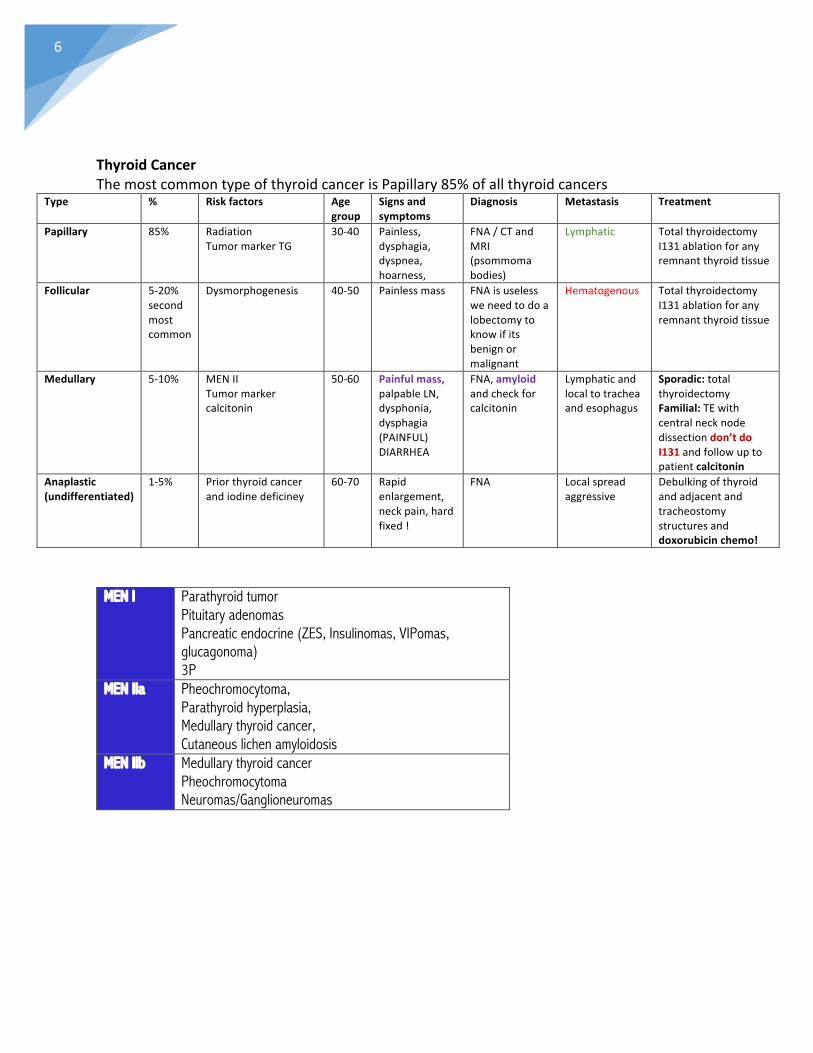
ThyroidCancerThemostcommontypeofthyroidcancerisPapillary85%ofallthyroidcancers
Type % Riskfactors Agegroup
Signsandsymptoms
Diagnosis Metastasis Treatment
Papillary 85% RadiationTumormarkerTG
30-40 Painless,dysphagia,dyspnea,hoarness,
FNA/CTandMRI(psommomabodies)
Lymphatic TotalthyroidectomyI131ablationforanyremnantthyroidtissue
Follicular 5-20%secondmostcommon
Dysmorphogenesis 40-50 Painlessmass FNAisuselessweneedtodoalobectomytoknowifitsbenignormalignant
Hematogenous TotalthyroidectomyI131ablationforanyremnantthyroidtissue
Medullary 5-10% MENIITumormarkercalcitonin
50-60 Painfulmass,palpableLN,dysphonia,dysphagia(PAINFUL)DIARRHEA
FNA,amyloidandcheckforcalcitonin
Lymphaticandlocaltotracheaandesophagus
Sporadic:totalthyroidectomyFamilial:TEwithcentralnecknodedissectiondon’tdoI131andfollowuptopatientcalcitonin
Anaplastic(undifferentiated)
1-5% Priorthyroidcancerandiodinedeficiney
60-70 Rapidenlargement,neckpain,hardfixed!
FNA Localspreadaggressive
Debulkingofthyroidandadjacentandtracheostomystructuresanddoxorubicinchemo!
MEN I Parathyroid tumor Pituitary adenomas Pancreatic endocrine (ZES, Insulinomas, VIPomas, glucagonoma) 3P
MEN IIa Pheochromocytoma, Parathyroid hyperplasia, Medullary thyroid cancer, Cutaneous lichen amyloidosis
MEN IIb Medullary thyroid cancer Pheochromocytoma Neuromas/Ganglioneuromas
7
Whatarethecomplicationsofthyroidsurgery?Thyroidectomy:
• Recurrentlaryngealnerveinjuryresultinginhoarsenessandiftheinjurywasbilateralitwillresultinairwayobstruction
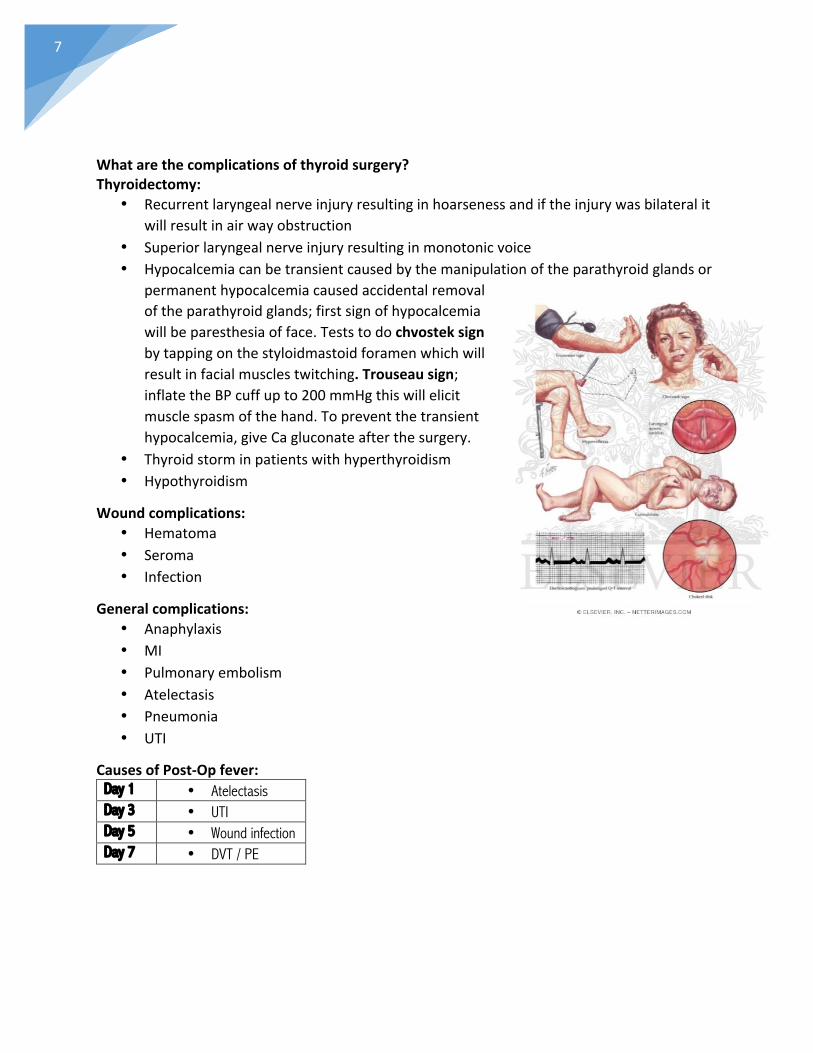
• Superiorlaryngealnerveinjuryresultinginmonotonicvoice• Hypocalcemiacanbetransientcausedbythemanipulationoftheparathyroidglandsor
permanenthypocalcemiacausedaccidentalremovaloftheparathyroidglands;firstsignofhypocalcemiawillbeparesthesiaofface.Teststodochvosteksignbytappingonthestyloidmastoidforamenwhichwillresultinfacialmusclestwitching.Trouseausign;inflatetheBPcuffupto200mmHgthiswillelicitmusclespasmofthehand.Topreventthetransienthypocalcemia,giveCagluconateafterthesurgery.
• Thyroidstorminpatientswithhyperthyroidism• Hypothyroidism
Woundcomplications:• Hematoma• Seroma• Infection
Generalcomplications:• Anaphylaxis• MI• Pulmonaryembolism• Atelectasis• Pneumonia• UTI
CausesofPost-Opfever:Day 1 • Atelectasis Day 3 • UTI Day 5 • Wound infection Day 7 • DVT / PE
8
Youoperatedonapatientwithgravesdiseaseforthyroidectomyseveralhoursafterthesurgerythepatientdevelopeddifficultybreathing,stridorandprogressiveswellingundertheincision.Thisisawoundhematomathiswouldrequirewoundexplorationandairwaycontrol.Ifairwaycontrolisunabletobeobtainedpriortooperatingroom,thewoundshouldbeopenedatthebedside.Topreventsuchcomplicationadrainshouldbeplaced.Whatisatelectasis?Itthecollapseofthealveoli,itisthemostcommoncauseofpost-opfeverinthefirst24hours.Whatkeepsouralveoliopen?
• Positiveendexpiratorypressure(thiswillbelowresultinginthecollapse)• Surfactant
Howtotreatatelectasis?• Chestphysiotherapy• Incentivespirometry• Antibioticsbroadspectrum
Youinducedanesthesia“succinylcholine”inapatienthethendevelopedfever,musclerigidity,tachycardia,hypotension.Whatisyourdiagnosisandwhatdoyoudonext?Malignanthyperthermiawhichisanautosomaldominantdiseasecausedbyryanodinereceptordefectresultinginanimpairedreuptakeofcalciumbythesarcoplasmicreticuluminmuscles.Rx:antidotedantrolene(calciumchannelblocker),hydrateandstopanesthesia.Complications:rhabdomyolysis,death.Whatishungrybonesyndrome?Occursafterthecorrectionofhyperparathyroidism(parathyroidectomy).Increasedboneremodelingunitswillmineralizeandbalancewillbetowardssynthesisofbonesresultinginseverepostoperativehypocalcemiathatmayleadtosymptomsoftetany.
9
Acuteabdomen:RLQpain:
• Appendicitis• Cecaldiverticulitis(notcommon)• Meckelsdiverticulum• Perforatedduodenalulcer(Valentino’ssign)• Gastroenteritis• Mesentericadenitis(usuallyafterupperrespiratoryinfectionmoreinkids)• Renalcolic• UTI• Crohn’sdisease(terminalileitis)• Ovariancystrupture,ovariantorsion,PIDandectopicpregnancyinfemales
LLQpain:• RenalcolicandUTI• Sigmoidvolvulus• Diverticulitis(leukocytosis,feverandLLQinoldage)• Colitis• Ovariancystrupture,ovariantorsion,PIDandectopicpregnancyinfemales
RUQpain:• Inferiorlobepneumonia• Hepatictumors,abscessandhepatitis• Biliarycolic,cholangitis,cholecystitis• Retrocaecalappendicitis
LUQpain:• Pneumonia• Splenicinfarction,abscessorrupture
Epigastricpain• Pancreatitis• Duodenal/gastriculcer• Gastritis
Diffuseabdominalpain:• Bowelobstruction(vomitingandobstipation/constipation)• Aorticaneurysm• Enteritis• Mesentericischemia
Medicalcauses:• MI• Sicklecellcrisis• Leadpoisoning• Mittelschmerz• Shingles• DKAoraddisoniancrisis

10
• Porphyria
WhatinvestigationsyouwillorderinapatientwithRUQpain?• CBC• LFT• Amylaseandlipase• Urinalysis• U/S
Whichtumorsthatcanresultinjaundice?
• Hepatocellularcarcinoma• Cholangiocarcinoma• Ampullarycarcinoma• Pancreaticcancer
Whatisyourdifferentialdiagnosisforananteriorabdominalmass?• Mesenchymalcyst• Gastriccancer• Leiomyosarcoma• Gastrointestinalstromaltumor

11
HepatobiliarySystem:Whatisthefunctionofgallbladder?StorageandconcentrationofbileWhatarethecomponentsofbile?Bileacids,lethicin,bilirubin,cholesteroland90%iswaterConsequencesofgallstones:
• Asymptomatic• Obstructivejaundice• Ascendingcholangitis• Pancreatitis• Biliarycolic• Cholecystitis• Gallstoneileus“pneumobilia”• Gallbladdermucocele>empyema• Mirizzisyndrome(compressiononthecommonhepaticduct)
Indicationsofcholecystectomy:• Immunocompromisedpatients(post-
transplant)• Pediatrics• Porceliangallbladder“increasedriskof
cholangiocarcinoma”• SCD/Thalassemia• Bariatricsurgery• Single2cmstone

12
Disease Cholecystitis Choledocholithiasis Cholangitis Obstruction of the cystic duct by gallstone
Common bile duct obstruction by gallstone
Ascending bacterial infection of the biliary system associated with CBD obstruction
Signs and Symptoms
RUQ pain, fever, nausea, vomiting and positive Murphy’s sign
Epigastric pain, jaundice, recurrent attacks of acute pancreatitis
Charcot’s triad: fever, jaundice and RUQ pain. Reynold’s pentand: charcot’s + CNS symptoms and septic shock
Diagnosis -Labs: increased WBC -U/S: gallbladder wall >4 mm, pericholecystic fluid and stone in the gallbladder. -HIDA scan: non-filling of the gallbladder (if U/S not diagnostic)
-Labs: increased bilirubin, alk phos direct bilirubin -ERCP
-Lab: increased bilirubin, alk phos direct bilirubin -U/S: dilatation of common and intrahepatic bile ducts -ERCP -Blood culture
Treatment Cholecystectomy ERCP ERCP/PTC/T-tube Imaging
ClinicalVingnette:A30yearsoldfemalepresentedtotheA&Ewithahistoryofpainradiatingtothetipofshoulder,nauseaandvomiting,RUQtenderwithpositivemurphysign.AcutecholecystitisNextstep:
• CBCwithdifferentialdiagnosis15kWBC• Amylaseandlipase(-)• LFTandbilirubinnormal• Electrolytes
Radiology:U/Swillshowthickwalls>5mm,edema,stone,pericholecysticfluid.Rx:IVfluids,NPO,analgesia(TramadolorPethidinewithbuscopan),Antibiotics(ceftriaxoneandFlagyl)Whendoweadmitthepatientforcholecystectomy?Waituntil6weeks,askthepatienttoavoidfattyfoodetcthendoit.

13
A40-year-oldmalepresentedtotheA&Ewithahistoryofnausea,vomitingandepigastricpainradiatingtotheback.WBCwerehigh,lipaseandamylasewerehigh.U/Sshowedastoneinthegallbladderanddilatedcommonbileduct.AcutepancreatitisRx:IVhydration,NPO,analgesia“antibioticsarenotindicatedinpancreatitis”NextforthestoneintheCBDdoERCPtoremovethestonethendocholecystectomy.A60yearoldfemalepresentedtotheA&EwithahistoryofRUQpain,fever,jaundice,andherbloodpressurewas80/40.WBClevelswerehigh,increasedbilirubin,alkalinephosphataseandLFT.Ascendingcholangitiswithreynold’spentad(charcotstriad+shock+alteredmetalstatus)Rx:U/Sistheinitialstudy;dilationofthecommonandintrahepaticductsalongwithgallstones,thickedematousgallbladderwall.Definitiverx:ERCP+antibioticsPatientpresentedtoyouwithahistoryofincreasedpain,feverandpalpabletendermassbelowtheliver.Gallbladderempyema,doU/Sguideddrainagewithantibiotics.Geriatricpatientpresentedtoyouwithahistoryofvomiting,abdominaldistentionandpainwithconstipation.Patienthashistoryofpreviousgallstones.GallstoneileusInvestigations:CXR,abdominalXraysupineanderect(airinthebiliarytree)ConfirmitwithCTscanRx:laproscopicremovalofthestonewithcholecystectomy.Patientpresentedwitha3dayhistoryofRUQpainwithnausea,vomitingandpositiveMurphy’ssign.WBClevelswereslightlyelevated,U/Sshowednostones.AcalculouscholecystitisDiagnosis:HIDAscanRx:admit,NPO,Antibiotics+cholecystectomyItpresentsin10%ofcasesofcholecysitis.Riskfactors:ICUpatients,trauma,burns,sepsisandTPN.Whatarethecomplicationsoflaparoscopiccholecystectomy?
• Injurytothecommonbileduct(diagnosedwithERCP)• Injurytotheliver• Injurytothebloodvessels• Trocarsitehernia

14
Whatarethecausesofperitonitis?Classification:Localized:appendicitis,diverticulitis,cholecystitis,salpingitisGeneralized:
• Chemical:perforationofstomach,smallbowelorgallbladder
• Bacterial:intra-abdominalabscess,fecalcontaminatedduetobowelperforation,trauma,surgicalspillageoranastomoticleakafterbowelsurgery
OR• Primary: spontaneous bacterial
peritonitisorsecondarytoperitonealdialysis
• Secondary:causedbyaperforatedviscus• Tertiary:complicationafterasurgery(abscess)
Whatarethecausesofairunderdiaphragm?
• Perforation• Postlaproscopic/laparotomy• Typhoid(Causingsmallbowelperforation)• Abscessunderdiaphragm(C.perfringens)• Penetrationofthediaphragm

15
ObstructiveJaundice:Whatisjaundice?Yellowishdiscolorationoftheskinandmucusmembraneswithhyperbilirubinemia>3g/dLCausesofhyperbilirubinemia:
• Pre-hepatic:anycauseofhemolysis(SCD,G6PD,spherocytosis)• Hepatic:hepatitis,cirrhosis,enzymesdeficiency• Post-hepatic:obstructivejaundice
Whatarethecausesofobstructivejaundice?Proximal
• Cholangiocarcinoma• Lymphodynopathy• Cholangiocarcinoma• Sclerosingcholangitis• Gallstones• Parasite• Postsurgicalstricture
Distal• Choledocholithiasis• Pancreaticcancer• Pseudocyst• Pancreatitis
Whatiscourvoisier’ssign?Jaundicewithapalpablenon-tendergallbladderseeninpatientswithpancreaticheadcancerWhatisyourddxofpalpablegallbladder?
• Pancreaticcancer(non-tender)• Gallbladderempyema(tender)
Historytakinginpatientwithjaundice?Makesuretocoverallthepointsbelow
• Theonset,durationandprogression• Changeinstool/urinecolor• RUQpain• Itching?(patientPBChavepruritusfollowedbyjaundice)• Flulikesymptomsandfever(hepatitis)• Historyofanyhemolyticanemia• Weightlossandanorexia(cancer)• Useofanymedication• ParenteralexposuretoIVdrugsortransfusion• Tattoosandsexualhistory• Recenttravel

16
Whatinvestigationyouwillorderinapatientwithjaundice?
• CBC• Liverfunctiontest
Livercellnecrosis:ALT Specific enzyme for liver necrosis
ALT>AST; viral hepatitis AST AST>ALT; indicates alcoholic hepatitis
Cholestasis:
GGT Intrahepatic or extra-heptic obstruction to bile flow
ALP Synthesized by the bile duct epithelium
• Serumalbumin,PT,BUN,ammoniaRandomtests:SerumIgM PatientswithPBCAnti-mitochondrialantibody
PBC
Anti-smoothmuscleantibody
Autoimmunehepatitis
ANA Autoimmunehepatitisa-fetoprotein HepatocellularcarcinomaOthersinvestigations:
• U/S• CTscan• Percutaneoustrans-hepaticcholangiogram(goodfor
proximalbiliarytree)• ERCP(distalpartofbileduct)• EndoscopicU/Sguidedbiopsy(forpancreaticcancer)
EndoscopicU/S

17
Pancreatitis:Whatisthefunctionofthepancreas?IthasanendocrineandexocrinefunctionEndocrine:
• Insulinproducedbythebetacells• Glucagonbyalfacells• Somatostatinbydeltacells• VIP
Exocrine:• Lipase,amylase,trypsin,phospholipase,protease• Theseenzymesareallsecretedintheinactivezymogenandtheygetactivatedby
enterokinaseintheduodenum.• Iftheygotactivatedbeforethiswillresultintheauto-digestionofthepancreas
Acutepancreatitis:Itistheinflammationofthepancreascausedbyparenchymalauto-digestionbyproteolyticenzymes.Extra-abdominalsymptomsofacutepancreatitis
• Shock• ARDS• Uveitis• Pleuraleffusion
Whatarethecausesofacutepancreatitis?
• Alcohol• Gallstones• hypercalcemia,hyperlipidemia• Druginduced(Azathioprine,cimetidine,steroids,metronidazole,methyldopa,valporic
acid,sulfasalazine,TMP-SMX,thiazides)• ERCP(in5%)• Scorpionvenom(Tityustrinitatis)• Infections(CMV,EBV,Coksakivirusandmumps)• Trauma• Congenital(divisum)• Autoimmune• Idiopathic
18
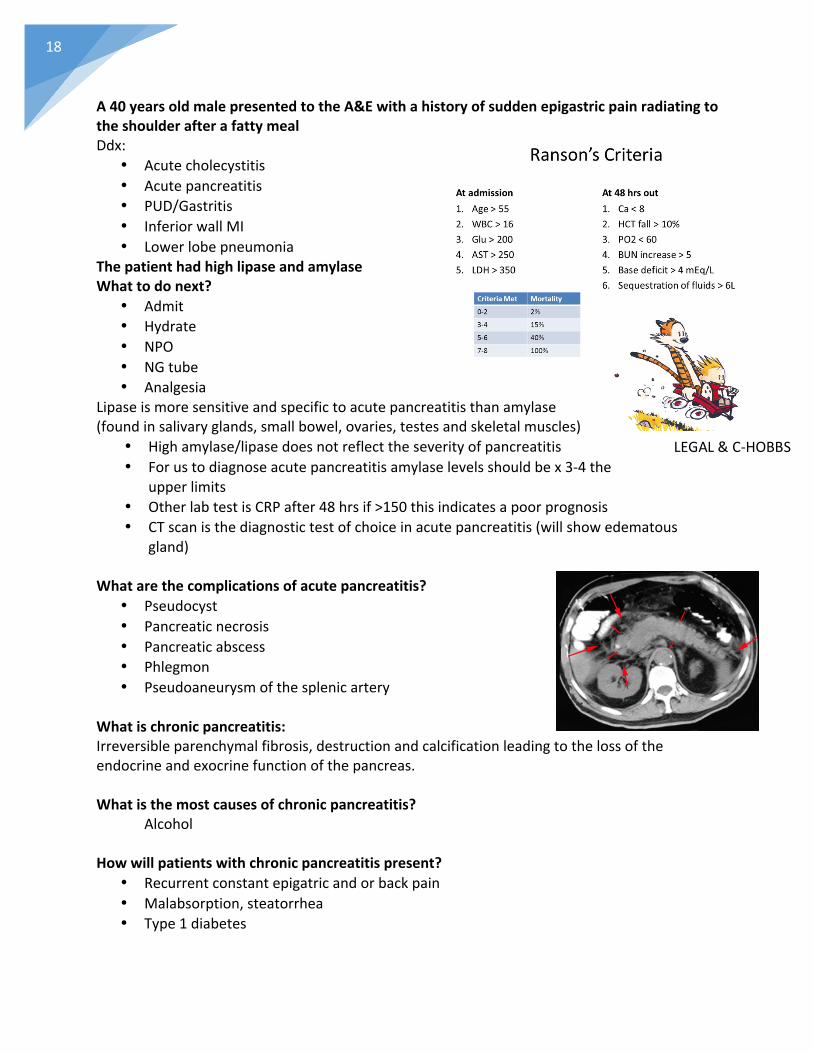
A40yearsoldmalepresentedtotheA&EwithahistoryofsuddenepigastricpainradiatingtotheshoulderafterafattymealDdx:
• Acutecholecystitis• Acutepancreatitis• PUD/Gastritis• InferiorwallMI• Lowerlobepneumonia
ThepatienthadhighlipaseandamylaseWhattodonext?
• Admit• Hydrate• NPO• NGtube• Analgesia
Lipaseismoresensitiveandspecifictoacutepancreatitisthanamylase(foundinsalivaryglands,smallbowel,ovaries,testesandskeletalmuscles)
• Highamylase/lipasedoesnotreflecttheseverityofpancreatitis• Forustodiagnoseacutepancreatitisamylaselevelsshouldbex3-4the
upperlimits• OtherlabtestisCRPafter48hrsif>150thisindicatesapoorprognosis• CTscanisthediagnostictestofchoiceinacutepancreatitis(willshowedematous
gland)Whatarethecomplicationsofacutepancreatitis?
• Pseudocyst• Pancreaticnecrosis• Pancreaticabscess• Phlegmon• Pseudoaneurysmofthesplenicartery
Whatischronicpancreatitis:Irreversibleparenchymalfibrosis,destructionandcalcificationleadingtothelossoftheendocrineandexocrinefunctionofthepancreas.Whatisthemostcausesofchronicpancreatitis?
Alcohol
Howwillpatientswithchronicpancreatitispresent?• Recurrentconstantepigatricandorbackpain• Malabsorption,steatorrhea• Type1diabetes
LEGAL&C-HOBBS

19
Howtodiagnosepatientswithchronicpancreatitis?
• Fecalfatanalysis• PancreaticcalcificationonXray• ERCPorMRCPwillshowchainoflake
pattern–areasofdilatationandstenosis• CT:showsglandsenlargement/atrophy
andcalcificationsHowtotreatpatientswithchronicpancreatitis?
• non-surgical:enzymereplacementtherapy&insulin• surgical:celiacplexusblockforpainrelief/pancreaticojejunostomy
Whatarethecomplicationsofchronicpancreatitis?
• Pancreaticabscess• Pancreaticfistula• Hemorrhagicpancreatitis• Pancreaticcancer
Cases:A40yofemalepresentedwithanepigastricpainof2days’durationradiatingtothebackwithhighlipaseandamylase.Ultrasoundshowedastoneinthecommonbileduct.Thisisacaseofbiliarypancreatitis,treatthepatientjustlikethetreatmentofanypancreatitiswithERCPandlaparoscopiccholecystectomyafter6weeks.A40yofemalepresentedwithasevereepigastricpainradiatingtothebackwithnauseaandvomiting,U/Sshowedbulkyheadofpancreas.Thepatienthadseveralattacksofsuchpainbeforeshealsohasrecurrentkidneystones.CheckthepatientCa+levels,ifthelevelswerehighthencheckforthePTHlevels(hyperparathyroidism).ToconfirmhyperparathyroidismdoU/Sandsestamibiscan.Sheprobablyhadtherecurrentattacksofpancreatitisduetohypercalcemiawhichiscausedbyprimaryhyperparathyroidism.A50yearoldalcoholicmalepresentedwithsevereepigastricradiatingtothebackwithhighlipaseandamylase.NormalU/S,CTshoweddilatedheadofpancreas,Ca+normal.Youstabilizedthepatientandatnightthepatientwasverydisoriented.Deliriumtremensduetoalcoholwithdrawal.TreatthepatientwiththiaminandbenzodiazepinestopreventWernickeencephalopathywhichiscausedbythiamindeficiency.A40yearoldfemalepresentedwithepigastricpainradiatingtoback.BMIis38,U/SandCa+werenormal.Whatdoyouhavetoordernext?LipidprofileDON’TFORGETIT!
Sestamibiscan
20
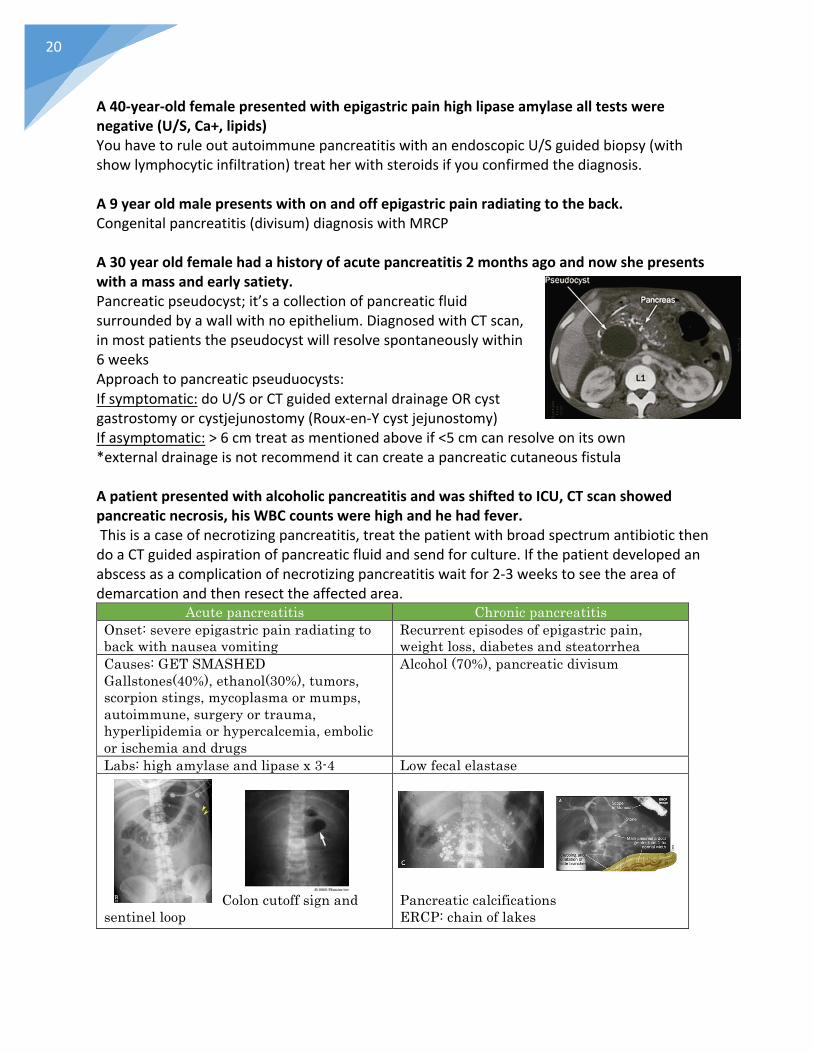
A40-year-oldfemalepresentedwithepigastricpainhighlipaseamylasealltestswerenegative(U/S,Ca+,lipids)YouhavetoruleoutautoimmunepancreatitiswithanendoscopicU/Sguidedbiopsy(withshowlymphocyticinfiltration)treatherwithsteroidsifyouconfirmedthediagnosis.A9yearoldmalepresentswithonandoffepigastricpainradiatingtotheback.Congenitalpancreatitis(divisum)diagnosiswithMRCPA30yearoldfemalehadahistoryofacutepancreatitis2monthsagoandnowshepresentswithamassandearlysatiety.Pancreaticpseudocyst;it’sacollectionofpancreaticfluidsurroundedbyawallwithnoepithelium.DiagnosedwithCTscan,inmostpatientsthepseudocystwillresolvespontaneouslywithin6weeksApproachtopancreaticpseuduocysts:Ifsymptomatic:doU/SorCTguidedexternaldrainageORcystgastrostomyorcystjejunostomy(Roux-en-Ycystjejunostomy)Ifasymptomatic:>6cmtreatasmentionedaboveif<5cmcanresolveonitsown*externaldrainageisnotrecommenditcancreateapancreaticcutaneousfistulaApatientpresentedwithalcoholicpancreatitisandwasshiftedtoICU,CTscanshowedpancreaticnecrosis,hisWBCcountswerehighandhehadfever.Thisisacaseofnecrotizingpancreatitis,treatthepatientwithbroadspectrumantibioticthendoaCTguidedaspirationofpancreaticfluidandsendforculture.Ifthepatientdevelopedanabscessasacomplicationofnecrotizingpancreatitiswaitfor2-3weekstoseetheareaofdemarcationandthenresecttheaffectedarea.
Acute pancreatitis Chronic pancreatitis Onset: severe epigastric pain radiating to back with nausea vomiting
Recurrent episodes of epigastric pain, weight loss, diabetes and steatorrhea
Causes: GET SMASHED Gallstones(40%), ethanol(30%), tumors, scorpion stings, mycoplasma or mumps, autoimmune, surgery or trauma, hyperlipidemia or hypercalcemia, embolic or ischemia and drugs
Alcohol (70%), pancreatic divisum
Labs: high amylase and lipase x 3-4 Low fecal elastase
Colon cutoff sign and sentinel loop
Pancreatic calcifications ERCP: chain of lakes

21
Whatisthemechanismofhypotensioninpancreatitis?Inflammationandcytokinestormcauseendothelialinjuryandincreasedpermeabilityintheperipancreaticvasculature,leadingtofluidleakageintotheretroperitonealspace.Thecytokinestormalsocausesmassivevasodilation.
ColonCancerandPolyps:Whatarethetypesofcolonicpolyps?Benign:inflammatory,lymphoid,hyperplastic,hamartomatousPre-malignant:adenomatous(tubular,tubulovillousandvillous”40%riskofmalignancy”)Howwouldapatientwithcolonicpolypspresent?
• Asymptomatic• Melena/hematochezia• Mucus• Changesinbowelhabits• Largebowelobstruction
DiagnosisismadewithcolonoscopyofcRx:colonoscopicresectionWhataretheriskfactorsofcoloncancer?
• Age• FamilyhistoryofcoloncancerorFAP• Lowfiberdiet,highfatdiet• IBDespUC(riskincreases1-2%everyyearafter2yearsofthedisease)
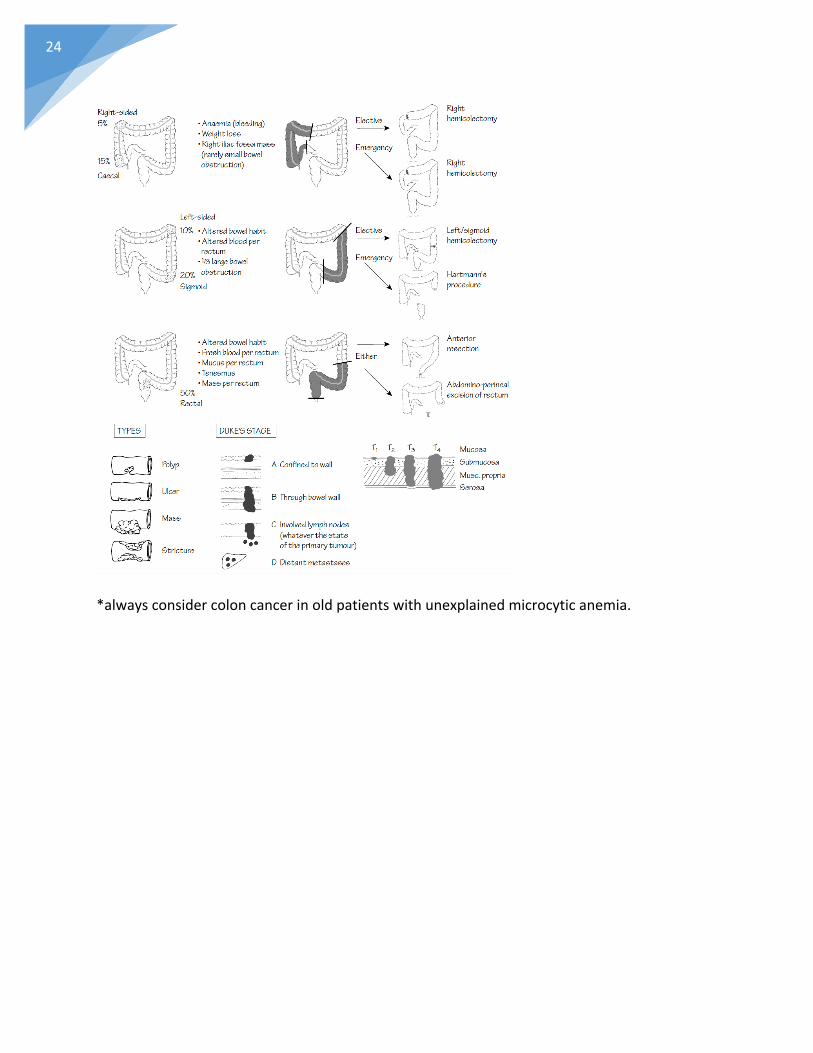
Signsandsymptomsofcoloncancer:
Itwilldependonthelocation• Rightside:occultbleeding,melenaandanemia• Leftside:alteredbowelhabits,rectalbleeding,largebowelobstruction(patientwill
presentearlierthanrightsidedcancer)• Bothwillhaveanorexiaandweightloss
Howtodiagnosecolorectalcancer?
• Colonoscopy• Chest,abdomenandpelvisCT(Staging)• Bonescan(staging)• CEAisatumormarkerusedforfollowupaftertreatmentnotdiagnosis

22
A50-year-oldmanpresentedwithahistoryofPRbleedingof2weeksPMHofhypertension.Whatwillyouask?
• Quantityofblood• Color?Darkorfresh• Timingofbleeding?beggingofstoolorattheend• Alteredbowelhabits• Weightloss,anorexia?• Signsandsymptomsofanemia?• Familyhistoryofcolorectalcancer?(askaboutalltheriskfactors)
Metastasisofcoloncancer:liver,bonesandlungsDukesstagingofcolorectalcancer
A Tumor confined to submucosa 5 years survival 90-95%
B Invasion to the muscle wall 85% C Invasion to serosa
C1: no lymph nodes spread C2: lymph nodes spread
30%
D Distant metastasis (liver, lung and bones)
<1%
Coloncancerstaging:
Stage I T1/T2 Stage II T3/T4 Stage III Any T/N1/N2 Stage Vi Any T any N M1 Screeningforcolorectalcancer:Recommendedscreeninginadultswithaveragerisk,beginningattheageof50untilage75.
• Colonoscopyevery10years• Flexiblesigmoidoscopyevery5years+FOBTevery3years• Fecaloccultbloodtestxannually
Screeninginpatientswithafirstdegreefamilymemberwithcolorectalcancer:Thesepatientsshouldbeginscreeningatageof40or10yearspriortotheonsetofcolorectalcancerinthefirstdegreerelative.Theyshouldcontinuescreeningevery5yearsafter.
23
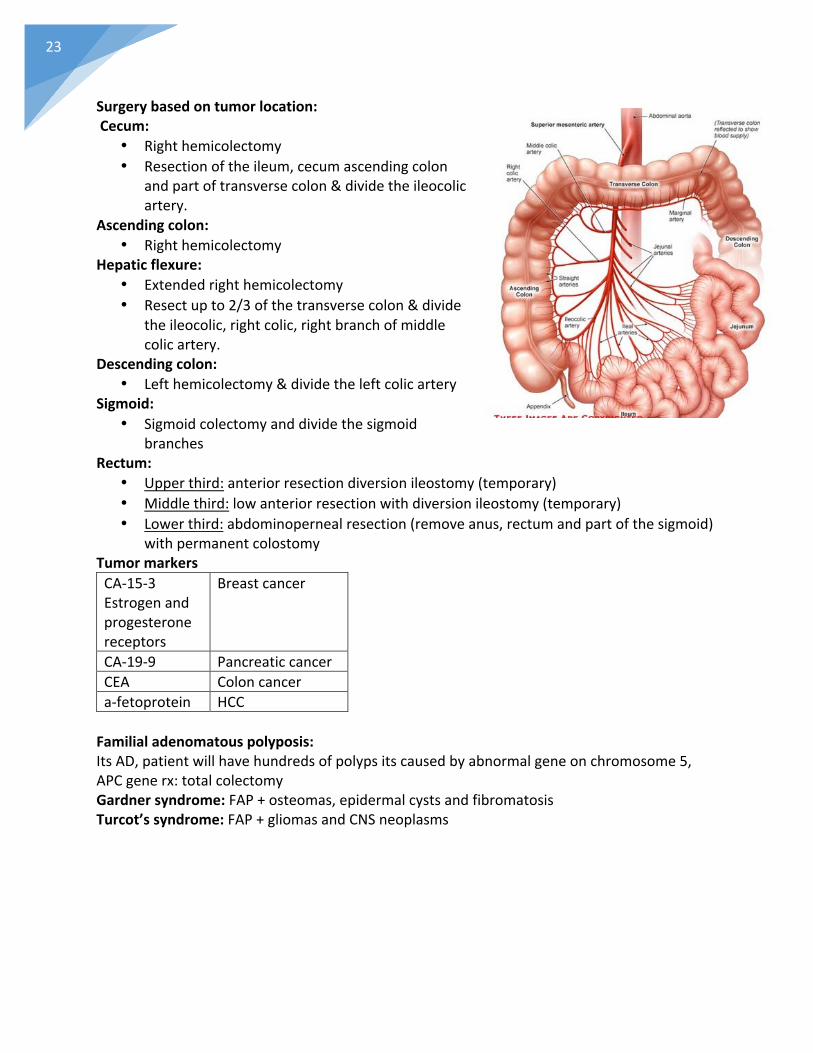
Surgerybasedontumorlocation:Cecum:
• Righthemicolectomy• Resectionoftheileum,cecumascendingcolon
andpartoftransversecolon÷theileocolicartery.
Ascendingcolon:• Righthemicolectomy
Hepaticflexure:• Extendedrighthemicolectomy• Resectupto2/3ofthetransversecolon÷
theileocolic,rightcolic,rightbranchofmiddlecolicartery.
Descendingcolon:• Lefthemicolectomy÷theleftcolicartery
Sigmoid:• Sigmoidcolectomyanddividethesigmoid
branchesRectum:
• Upperthird:anteriorresectiondiversionileostomy(temporary)• Middlethird:lowanteriorresectionwithdiversionileostomy(temporary)• Lowerthird:abdominopernealresection(removeanus,rectumandpartofthesigmoid)
withpermanentcolostomyTumormarkersCA-15-3Estrogenandprogesteronereceptors
Breastcancer
CA-19-9 PancreaticcancerCEA Coloncancera-fetoprotein HCCFamilialadenomatouspolyposis:ItsAD,patientwillhavehundredsofpolypsitscausedbyabnormalgeneonchromosome5,APCgenerx:totalcolectomyGardnersyndrome:FAP+osteomas,epidermalcystsandfibromatosisTurcot’ssyndrome:FAP+gliomasandCNSneoplasms
24
*alwaysconsidercoloncancerinoldpatientswithunexplainedmicrocyticanemia.

25
Anus:Whatisafistula?Abnormalopeningandconnectionbetweentwoepithelizedhollowspaces.Whatarethetypesoffistula?
• Perianal• Enterocutaneousfistula(inIBD)• Enterovesicalfistula• Enteroentericfistula• Enterovaginalfistula• Tracheoesophygealfistula(congenital)• AVfistula
A31yomalewithhistoryofCrohndiseasepresentswithsevererectalpainthathasprogressivelyincreasedlastnight.P/Edemonstratesasmall,erythematous,welldefined,fluctuant,subcutaneousmassneartheanalorficie.Anorectalabscessisthemostlikelydiagnosis.ItisacollectionofpussurroundedbyacavitycausedbyaninfectionarisinginthecryptoglandularepitheliumliningtheanalcanalRx:incisionanddrainagewithantibioticsS.aureuscommonlycausesabscess.A25yofemalewithhistoryofIBSwithconstipationpresentswithseverepainwithpassingstool.Shenotesthatthepainissosevereandisafraidtohaveabowelmovement.Thestoolsarehardandcoveredwithbloodstreaks.ThemostlikelydiagnosisisananalfissureWhatisanalfissure?Painfultearsintheanalmucosabelowthedentatelineinducedbyconstipationorexcessivediarrhea.Patientswillpresentwithpainfuldefecation,brightredPRbleeding,lacerationon6and12o’clockposition.Patientswithchronicanalfissurewillhavehypertrophyofthesurroundingskinandsentinelpileorskintag.Whataretheoptionsfortreatinganalfissures?
• Sitzbath• TopicalnitroglycerinorCCBorinjectionofbotulinumtoxinintotheanalsphincter• Fibersupplements• Bulkingagents• Lateralinternalsphincterotomyordilationforchroniccases

26
Upper&LowerGIBleeding:Rectalbleedinghistory:
• Onset• Color• Amount• Pain?• Withstoolorafter• Meds(aspirin,NSAIDS,warfarin)• Weightlossorlossofappetite• Symptomsofanemia• AskaboutIBD,diverticulosisandotherrisks
HowwillyoumanageapatientwithmassivePRbleeding?
• ABC• 2lVlines;Ringerlactate• NGT• bloodcross-match• Foleycatheter
Whatdoyoudonext?
• Endoscopy+colonoscopyWhatisalowerGIbleeding?AnybleedingdistaltotheligamentofTreitz(betweentheduodenumandjejunum)WhatarethesymptomsoflowerGIbleeding?
• Hematochezia• Melena• Anemia• Shock
WhatarethecausesoflowerGIbleeding?Rectalcauses:
• Fissures• Hemorrhoids• Solitaryrectalulcer• Analtumor• Trauma
Other:• Mostcommon:diverticulosisandvascularectasia(massivelowerGIbleeding)• Coloncancerandpolyps• Ischemiccolitis
27
• IBD• Meckel’sdiverticulum• Infectiouscolitis• Smallboweltumor• Radiationenteritis• Meds:aspirin,warfarinandclopidogrel
WhatarethecausesofupperGIbleeding?
• Duodenalorgastriculcer• Acutegastritis• Esophagealvarices• Mallory-Weisstear• Gastriccancer• Boerhaave’ssyndrome• Aortoentericfistula• Dieulafoy’sulcer(submucosaldilatedlargearterioles)• GIST• AVmalformation
HowwillyoumanageapatientwithanupperGIbleeding?
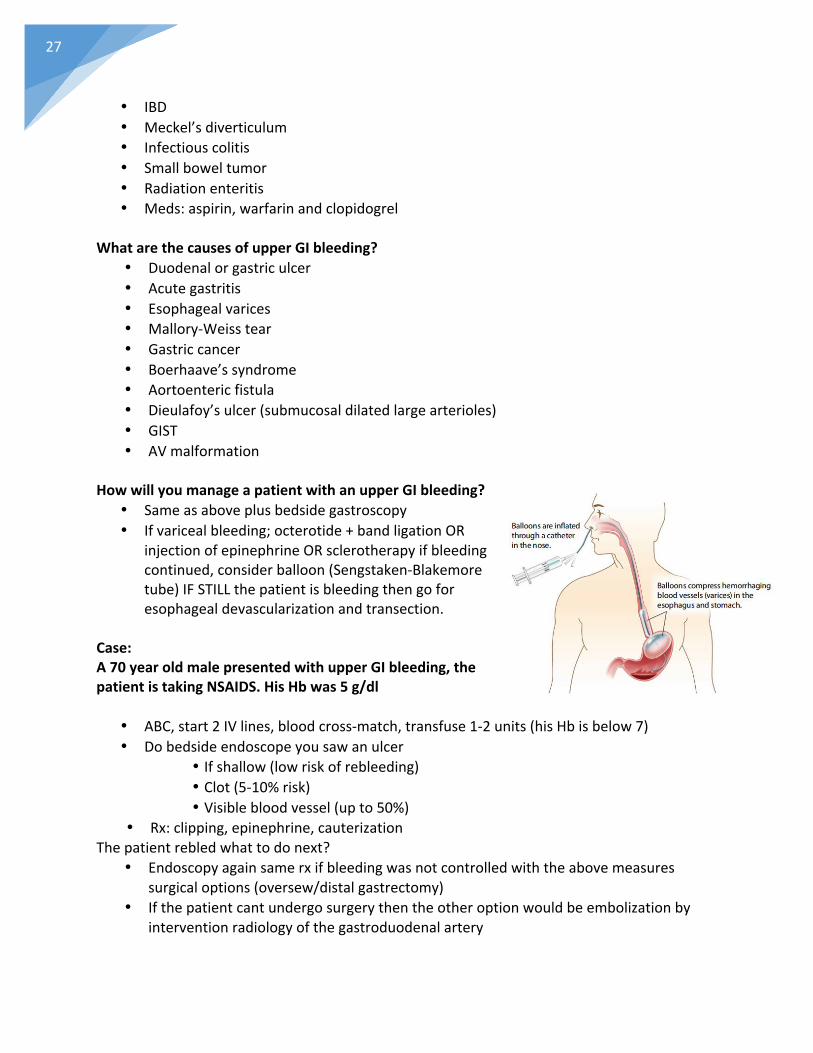
• Sameasaboveplusbedsidegastroscopy• Ifvaricealbleeding;octerotide+bandligationOR
injectionofepinephrineORsclerotherapyifbleedingcontinued,considerballoon(Sengstaken-Blakemoretube)IFSTILLthepatientisbleedingthengoforesophagealdevascularizationandtransection.
Case:A70yearoldmalepresentedwithupperGIbleeding,thepatientistakingNSAIDS.HisHbwas5g/dl
• ABC,start2IVlines,bloodcross-match,transfuse1-2units(hisHbisbelow7)• Dobedsideendoscopeyousawanulcer
• Ifshallow(lowriskofrebleeding)• Clot(5-10%risk)• Visiblebloodvessel(upto50%)
• Rx:clipping,epinephrine,cauterizationThepatientrebledwhattodonext?
• Endoscopyagainsamerxifbleedingwasnotcontrolledwiththeabovemeasuressurgicaloptions(oversew/distalgastrectomy)
• Ifthepatientcantundergosurgerythentheotheroptionwouldbeembolizationbyinterventionradiologyofthegastroduodenalartery
28
A15yearoldmalepresentstotheA&Ewithhistoryofbleedingforfewdays,hisHbwas5g/dLInvestigationstoidentifythebleedingsite?
1. Colonoscopy+PT/PTT(ifnormalthennext)2. TaggedRBCscan>0.5mL/min3. Angiography>1ml/min
Ifnormalthen:4. Capsuleendoscopy(swallowfor24hours)5. Meckl’sscan6. Retrogradeantroscopy7. Lastoption>laproscopicopening
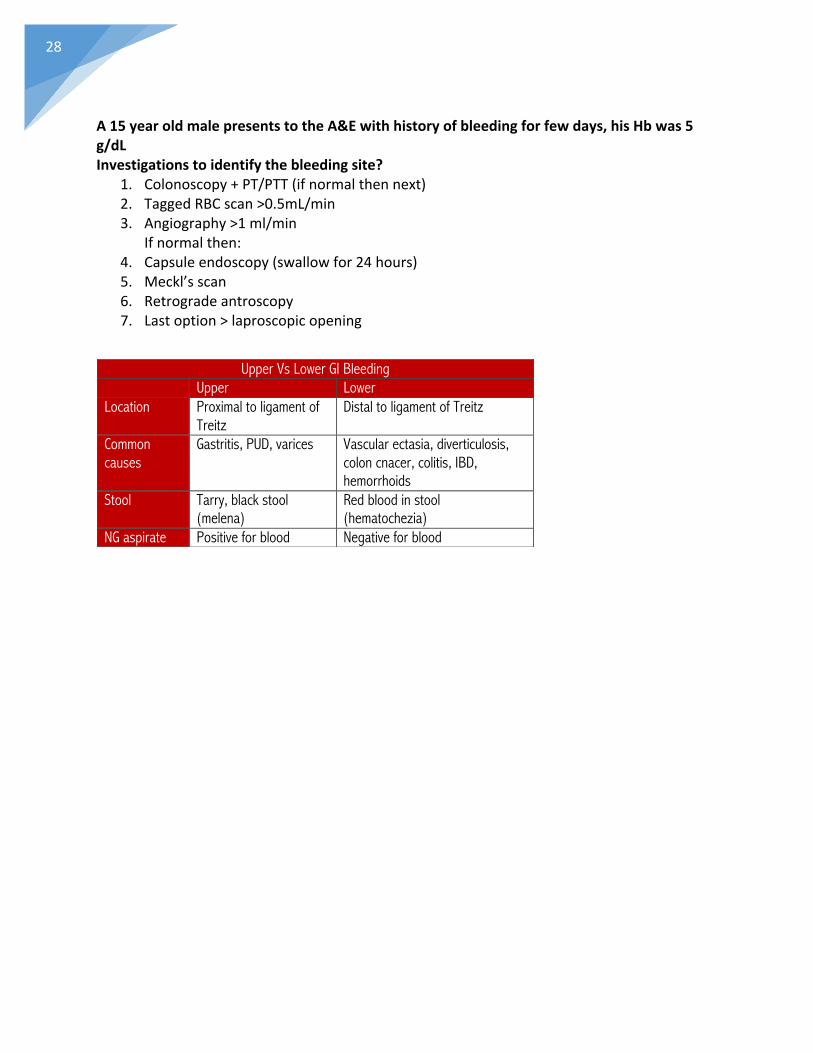
Upper Vs Lower GI Bleeding Upper Lower Location Proximal to ligament of
Treitz Distal to ligament of Treitz
Common causes
Gastritis, PUD, varices Vascular ectasia, diverticulosis, colon cnacer, colitis, IBD, hemorrhoids
Stool Tarry, black stool (melena)
Red blood in stool (hematochezia)
NG aspirate Positive for blood Negative for blood
29
Hernia:1Whatisthedefinitionofhernia?It’saprotrusionofaviscusthroughanabnormalopeninginthewallofacavityinwhichitscontained.Typesofhernia:Internal:
• Diaphragmatichernia• Brainstemherniation• Internalbowelherniation
External:• Inguinalhernia• Femoral• Obturator• Lumbar• Spigelianhernia• Umbilical• Incisional• Richter’shernia• Littershernia• Maydl’shernia• Epigastrichernia
Whatisthecardinalsignofhernia?CoughimpulseCausesofhernia:Congenital:patentprocessvaginalis,collagenvasculardisease“Ehlers-Danlossyndrome”andprematurityAcquired:chronicconstipation,chroniccough,ascites,pregnancy,liftingheavyobjects,BPH,weaknessintheabdominalwall,previoussurgery,trauma.Herniahistory:•Whendidyoufirstnoticethelump?•Askabouttheprogressionofsize?•Anyotherswellings?•Associatedsymptoms?•Askthepatientaboutthecause?Andaskabouteachriskfactorfromabove.Complicationsofhernia:•Incarceration•Strangulation•Obstruction

30
Whatistheinguinalcanal?It’sa4cmfibrouscanalextendingfromthedeepringtothesuperficialringandtheboundariesare:Anterior:aponeurosisofthemedial2/3externalobliqueandlateral1/3internalobliquemusclePosterior:mediallyconjointtendonlaterallytransversalsfasciaRoof:archingfibersoftransversemuscleandinternalobliqueFloor:inguinalligamentandlacunarligamentContentsoftheinguinalcanal:
• Females:roundligamentandilioinguinalnerve• Males:spermaticcordandilioinguinalnerve
Hasselbach’striangle:
• Medially:lateraledgeoftherectusabdominis• Laterally:inferiorepigastricvessels• Inferiorly:inguinalligament
The3ruleofspermaticcord:Whatarethe3nervesinspermaticcord?• Genitalbranchofthegenitofemoral• Cremastericnerve• Sympatheticnervefibers
Whatarethe3arteries?•Testicularartery•Arterytovas•ArterytocremastericWhatarethe3veins?•Pampiniformplexus•Cremastericvein•VeinofvasWhatarethe3structurespassingintheinguinalcanal?•Lymphatics•Vasdeferens•PampniformplexusWhatistheconjointtendon?Formedbythelowerpartofthecommonaponeurosisoftheinternalobliqueandtransversesabdominismuscleanditsinsertedintothepubictubercleandcrest

31
Howtodifferentiatebetweeninguinalherniaandfemoralhernia?Relationtothepubictubercle,femoralherniawillbebelowandlateralwhileinguinalherniaswillbeaboveandmedial.Whatisrichter’shernia?Whenonlypartoftheintestinewallcircumferenceintheherniaitmaystrangulatewithnoobstruction,seeninfemoralandobturatorhernia.WhatisMaydl’shernia?WtypeofintestinalloopherniatesandmystrangulatewiththegangrenouspartbeinginsidetheabdomenwithoutthenoticingofthegangrenouspartWhatarethecomplicationsafterherniasurgery?
• General:hematoma,seroma,woundinfectionanddehiscence• Specific:scrotalhematoma,injurytotesticularartery,injurytoilioinguinalnerve,
chronicpainduetoentrapmentofilioinguinalnerveandrecurrenceWhatisthedifferencebetweenherniorrhaphyandherniotomy?•Herniorrhaphyistherepairofwallwhileherniotomyistheexcisionofthesacwithnorepairofwall,itsusuallydoneinpediatricpatients.Explainhowmeshisusefulinthemanagementofhernia?•Itincreasesthefibroblastactivityandhencewillstrengthenthemuscles.Whataretypesofmesh?
• Mersilenemesh• Prolenemesh
Whataretheprinciplesofmanagementinpatientswithhernia?•Opentissuerepair“tensionrepair”:Bassini,Shouldice,MacVay(femoralhernia)•Tensionfreerepair:usingaprostheticmesh(Lichtenstein’srepair)hasleastrecurrencerate•LaproscopicrepairWhendowerepairthehernialaproscopically?Bilateralorrecurrent
32
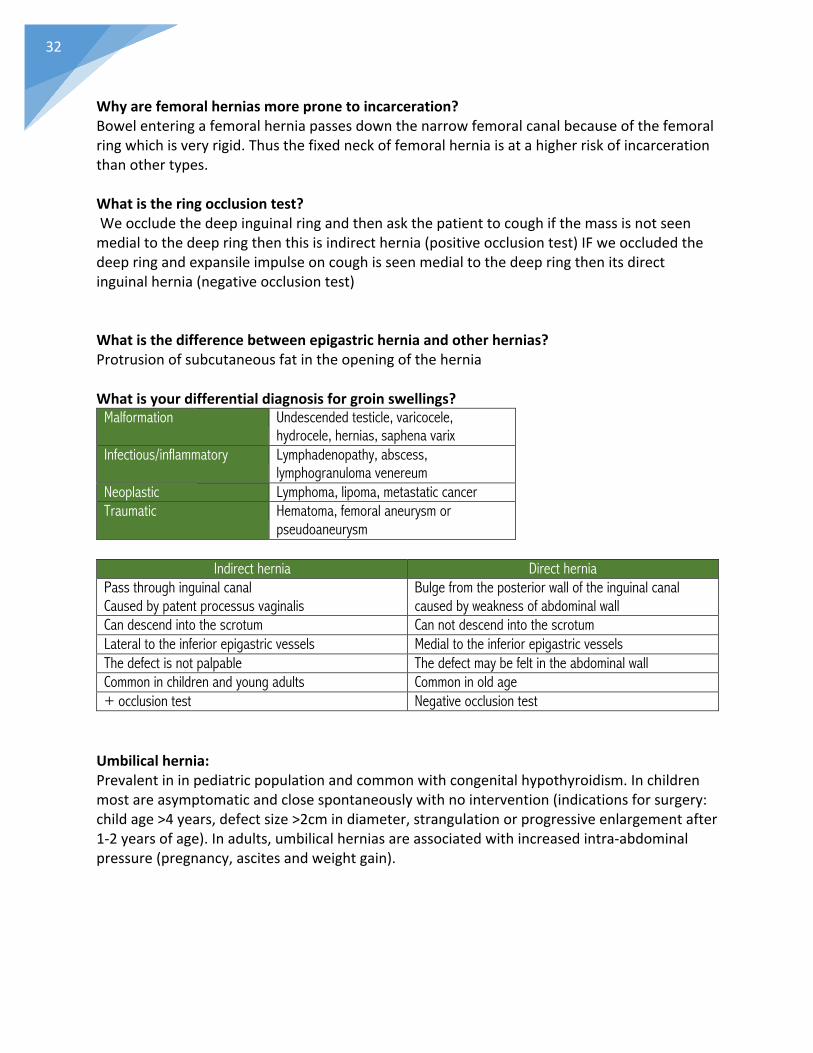
Whyarefemoralherniasmorepronetoincarceration?Bowelenteringafemoralherniapassesdownthenarrowfemoralcanalbecauseofthefemoralringwhichisveryrigid.Thusthefixedneckoffemoralherniaisatahigherriskofincarcerationthanothertypes.Whatistheringocclusiontest?Weoccludethedeepinguinalringandthenaskthepatienttocoughifthemassisnotseenmedialtothedeepringthenthisisindirecthernia(positiveocclusiontest)IFweoccludedthedeepringandexpansileimpulseoncoughisseenmedialtothedeepringthenitsdirectinguinalhernia(negativeocclusiontest)Whatisthedifferencebetweenepigastricherniaandotherhernias?ProtrusionofsubcutaneousfatintheopeningoftheherniaWhatisyourdifferentialdiagnosisforgroinswellings?
Malformation Undescended testicle, varicocele, hydrocele, hernias, saphena varix
Infectious/inflammatory Lymphadenopathy, abscess, lymphogranuloma venereum
Neoplastic Lymphoma, lipoma, metastatic cancer Traumatic Hematoma, femoral aneurysm or
pseudoaneurysm
Indirect hernia Direct hernia Pass through inguinal canal Caused by patent processus vaginalis
Bulge from the posterior wall of the inguinal canal caused by weakness of abdominal wall
Can descend into the scrotum Can not descend into the scrotum Lateral to the inferior epigastric vessels Medial to the inferior epigastric vessels The defect is not palpable The defect may be felt in the abdominal wall Common in children and young adults Common in old age + occlusion test Negative occlusion test Umbilicalhernia:Prevalentininpediatricpopulationandcommonwithcongenitalhypothyroidism.Inchildrenmostareasymptomaticandclosespontaneouslywithnointervention(indicationsforsurgery:childage>4years,defectsize>2cmindiameter,strangulationorprogressiveenlargementafter1-2yearsofage).Inadults,umbilicalherniasareassociatedwithincreasedintra-abdominalpressure(pregnancy,ascitesandweightgain).
33
Epigastrichernia:Thisisusuallyasmallprotrusionthroughthelineaalbaintheupperpartoftheabdomen.Oftentheherniaconsistsofextraperitonealfatonlybutitmaycontaintheomentumorsmallbowel.Thistypeofherniacanbeextremelypainfulbecauseofthetrappingandischemiaoftheextraperitonealfat.Rx:simplesutureofthedefectwithnon-absorbablesutures.Clinicalvignettes.You’vedoneasurgeryona70yearoldmaleinthemorningandatnighthecomplainedofpaininthesuprapubicarea.Whatdoyoususpect.Urinaryretention,canbesecondarytoBPHRx:catheterPatientcametoyourclinicweeksaftersurgicalrepairofherniacomplainingoflossofsensationinthemedialthighandlateralscrotum.InjurytotheilioingunialnervePost-surgicalpatientcamewithchronicpainafterherniarepair.Entrapmentoftheilioingunialnerve“chronicpainsyndrome”Rx:cutthenerveA30-year-oldmalepatientcomplainedofseveretesticularpainafterherniarepairwhatdoyoususpect?Injurytothetesticularartery,doduplexultrasoundtoconfirmyourdiagnosisifnoperfusionwasdetecteddoorchiectomytosavetheothertesticlebecauseantibodiescanbeformedagainstitiftheaffectedtesticlewasnotremoved.

34
BreastCancer:Whataresymptomsofapatientwithbreastcancer?
• Pain• Swelling• Nippledischarge• Skinchanges• Dimpling/nippleretraction• AsymptomaticThemostcommonpresentationofbreastcancerisapainlesslump
Whendowestartscreeningforbreastcancer?• Breastselfexaminationattheageof20shouldbepreformedmonthlydaysfollowing
themenstrualcycle• Clinicalorphysicianbreastexamination• Screeningmammography>attheageof40annually(craniocaudalandmediolateral)
Whataretheabnormalfindingsinamammogram?
• Stellate,massandmicrocalcifications
Whentoscreeninahighriskpatient?5yearsearlierfromthediagnosisofafamilymemberA30yearoldpatientpresentedbreastpain.Whatquestionsyouwillask?
• Relationofpaintomenstrualcycle• Allthecharactersofpain• Anydischarge• Askaboutriskfactorsofbreastcancer
Anypatientpresentingwithabreastmassdothetripleassessment:
• History/physicalexamination• MamoorU/S• FNA
Whatisyourddxofbreastpain?
• Fibrocysticdisease• Inflammatorybreastcancer• Advancedbreastcancer• Mastitis• Breastabscess• Fatnecrosis

35
Whatisyouddxofabreastlump?• Fibroadenoma(mobile,smoothandcircular)• Fibrocysticdisease(tender,bilateralandfluctuatewithmenstrualcycle)• Abscess• Galactocele• Cancer• Chronicgranulomatousmastitis
Ddxofbloodynippledischarge?
• Intraductalpapilloma• Paget’sdisease• Fibrocysticdisease• Intraductalcarcinoma
Yellow/green:• Abscess• Fibrocyticdisease• Ductectasia• Galactocele
White/milky:• Hyperprolactinemia
Whataretheskinchangesseeninbreastcancer?
• Dimpling• Peaud’orange• Rednessofskin• Fungatinglesion(T4)
Whatarethegenesrelatedtobreastcancer?
• BRCA1andBRCA2• K-167• B10andB51
Only5-10%ofallbreastcancersareassociatedwithaninheritedmutationWhataretheriskfactorsofbreastcancer?
• Age• Earlymenarcheandlatemenopause• Nulliparityorfirstpregnancy>30• Obesity• Atypicalhyperplasia• OCPorHRT• Smoking• Gender• Geneticpredisposition
36
FNACresultsinbreastcancer:• C1:inadequate• C2:benign• C3:atypical• C4:suspicious• C5:malignant
Wheredoesbreastcancermetastasize?
• 2B2L• brain,bone,liver,lungsandadrenals.
Staging:
• CTabdomenandchest• Bonescan
Treatment:
StageI,II:simplemastectomy+chemotherapyORlumpectomywithradiation+chemoStageIII:mastectomywithaxillarylymphnodedissectionStageIV:systemicandpalliativetreatment
Complicationsofaxillarylymphnodedissection:• Injurytolongthoracicnerve(wingedscapula)• Lossofsensation• Seroma
TNMclassificationofbreastcancer:T0:Notumor N0:noregionallymphnodesmetastasis M0:nodistantmetastasisTIS:CIS N1:metastasistolevelI,IIaxillaryLN
ipsilateralmovableM1:distantmetastasis
T1:<2cm N2:metastasistoipsilateralLNfixedlevelIandII
T2:2-5cm N3:metastasisipsilateralinfraclavicularLNorsupraclavicularLNT3:>5cm
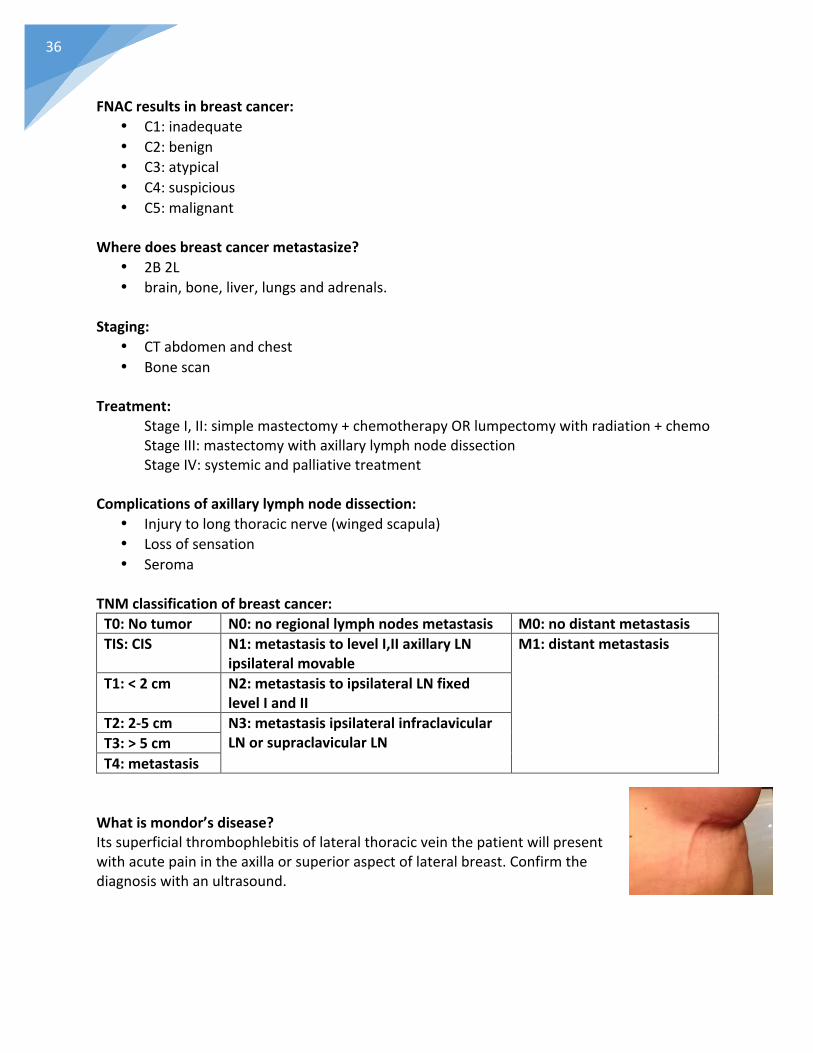
T4:metastasisWhatismondor’sdisease?Itssuperficialthrombophlebitisoflateralthoracicveinthepatientwillpresentwithacutepainintheaxillaorsuperioraspectoflateralbreast.Confirmthediagnosiswithanultrasound.
37
Sentineallymphnodebiopsy:Weinjectaradioactivesubstanceandbluedyetolocatethepositionofthesentinellymphnodes.Weuseadevicethatdetectsradioactivitytofindthesentinealnode,onceitslocatedwemakeasmallincisionandremovethenode.Itsthensendtopathologyifmalignantcellsifsentinealnodeispositiveaxillarydissectioniscompletedifsentinealnodeisnegativeaxillarydissectionisnotperformed.Whatisthetumormarkerofbreastcancer?CA-125andCA-15-3(notspecific)Whatisyourtreatmentforfibrocysticdisease?Initial:NSAIDS,vitaminEandwarmcompressionandavoidcaffeineandtobaccoNext:primroseoil(3-6months)Severe:danazoleandtamoxifenWhatisthetreatmentforfibroadenoma?Observeifasymptomaticsize<2cm.If>2msurgicalexcision.Apatientwithhadnolumpnopaintheyonlyfoundmicrocalcificationsshefoundtohavewhattodonext?Takeastereotacticbreastbiopsyandsendforpathology
Carcinoidtumor:ItsisamalignanttumoroftheenterochromaffincellsthatmostcommonlyoccurintheappendixfollowedbythesmallintestinesandrectumSignsandsymptoms:
Ø SlowgrowingsousuallyasymptomaticatfirstandusuallyfoundincidentallyØ Symptomatic:vagueabdominalpainisthemostcommonsymptomØ Intermittedobstructionin25%ofpatientsØ Rectalbleeding(rectalcarcinods),painandweightloss
Carcinoidsyndromeonlyfoundin10%oftotalpatientswithacarcinoidtumorØ Duetotheproductionofserotonin,bradykininortryptophanbythetumorand
exposureofthebodytotheseproductsØ Cutaneousflushing,sweating,waterydiarrhea,wheezing,dypnea.(niacin
deficiency)Diagnosis:
Ø Mostarefoundincidentallywithradiographicstudies,appendectomyorsurgeryforintestinalobstruction
Ø Ifthepatienthadcarcinoidtumor- 5HIAA(hydroxyindolaceticacid)in24hoururinecollection- plasmachormogranin- pentagastrin(inpatientswithhigh5HAAtherewillbemorecutaneousflushing)

38
Treatment:-Medical:serotoninantagonistsorsomatostaticanalogs(octerotide)forsymptomsofcarcinoidsyndromeSurgery:-appendixcarcinoid<2cmappendectomy-baseofappendixcarcinoidb>2mrighthemicolectomy-smallintestinescarcinoid;resectthetumorwithmesentericlymphnodes
DiabeticFootandUlcers:Ulcerhistorytaking:
• Onset• Progression• Firsttimeornot?• Pain• Dischargeorfoulsmell• Historyofanytraumaorinsectbite• Claudication/restpain• Askabout(diabetes,HT,dyslipidemiaand
smoking)• Occupation
Diabeticfootcanbesecondaryto:
• Neuropathy(presentoverpressurearea,painless)• Ischemia(tipoftoes,painful)• Infection(pusanddischarge,+/-fever)
Examinationofanulcer:• Inspect:site,size,depth,edge,margins,base,discharge,changesin
thesurroundingskin• Inspectionofthefoot:cracksordryness“secondarytoautonomic
neuropathy”,lookbetweenthetoesforfungalinfection,anysignsofcellulitis,Charcotfootdeformity.
• Palpation:sensation,capillaryrefilltime,peripheralpulses,temperature,lookforvascularangle.Monofilamenttest:usedtoassessfordiabeticfootneuropathy.Apositivetestwhenthemonofilamentisbent(10mgforce)indicatesthepresenceofneuropathy.
Investigations:Blood:CBC,glucoselevel,HbA1C,urea,electrolytes,Cr,serumlipidsandbloodcultureifpatientsepticFootinvestigations:woundcultureifitsinfected,footxrayifosteomyelitisorcharcotfootissuspectedIschemiaspecificinvestigations:ABI,arterialduplex,angiogram
39
Appendicitis:Randominfo:
• Weonlygiveoneprophylacticdoseofantibioticsbeforesurgeryinappendicitis• Ifpatienthadperforated,abscessorgangrenousappendicitiswegiveantibioticsfor5
days(ceftriaxone+metronidazole)• PatientsmightcomplainofRLQpainlastingformorethan5dayswithvomitinganda
RLQmassthinkaboutappendicularmass,insuchpatientswedon’toperateRx:IVantibiotics.Iftheylatercomplainedofrecurrentpain,wegoforappendectomyotherwiseitsnotrecommended
• ifapatientcomplainedofhighfever,RLQpainandatendermass(appendicularabscess)diagnosis:CTRx:surgicaldrainage
Examination in appendicitis Sign Finding Peritoneal signs Rebound tenderness: acute increase in pain
after removing the hand from applying pressure Involuntary guarding: tensing of abdominal wall muscles during the palpation of abdomen Rigidity: persistent tension of the abdominal wall muscles
Peritoneal irritation
Psoas sign RLQ pain with extension of right thigh Abscess adjacent to psoas or retrocecal appendix
Obturator sign RLQ pain with internal rotation of right thigh Pelvic appendix or abscess Rovsing’s sign RLW pain with LLQ palpation Acute appendicitis Rectal tenderness Right pelvic pain during rectal examination Pelvic appendix or abscess
40
Cellulitis:AcuteinfectionoftheskininvolvingthedermisandsubcutaneoustissueCauses:S.aureus,b-hemolyticstreptococciRiskfactors:trauma,recentsurgery,PVD,lymphedema,diabetes,crackedskininfeet/toes(tineapedis)Clinicalfeatures:pain,edema,erythemawithindistinctborders+/-regionallymphadenopathy.Fever,chillsandmalaise.Canleadtoascendinglymphangitis(redstreaking)Investigations:CBC,bloodcultureiffebrile,skinswabonlyifopenwoundwithnopusTreatment:
• Antibiotics:cephalexin/ifextensiveerythemaorsystemicsymptomsIVcefazolin• MRSA(anti-MRSA)J• Limbelevationandresttoreduceswelling
Admissioncriteria:• Immunosuppression• Intoleranceoforalantibiotics• Lackofresponseafter72hoursoforaltherapy• Noncompliantwithmedications• ShockorDIC• Signsandsymptomsofsepsis• TotalWBC<1K
ClassI ClassII ClassIII ClassIV-No systemic signs and symptoms -No comorbidities Within a 48-72 hrs will response to therapy Outpatient treatment take a swab of the exudate antibiotics: dicloxacillin oral for 7-10 days OR clindamycin for penicillin allergy if MRSA: clindamycin/TMP-SMX
-Mild-moderate systemic signs and symptoms -Stable comorbidity -Failure of response within 48-72 hrs oral =consider for outpatient IV antibiotics
-Significant symptoms -Unstable comorbidities (poor diabetes/immunosuppression or PAD) -Limb threatening infection = Inpatients with IV or oral antibiotics
• Flucloxacillin or cefazolin • MRSA vanco/linezolid or
tacoplanin
• Severe sepsis • Necrotizing fasciitis
= Inpatients with IV or oral antibiotics • Flucloxacillin or cefazolin • MRSA vanco/linezolid or
tacoplanin
Differential diagnosis of cellulitis • Eczema • Edema • DVT • Chronic venous
insufficiency • Vasculitis
41
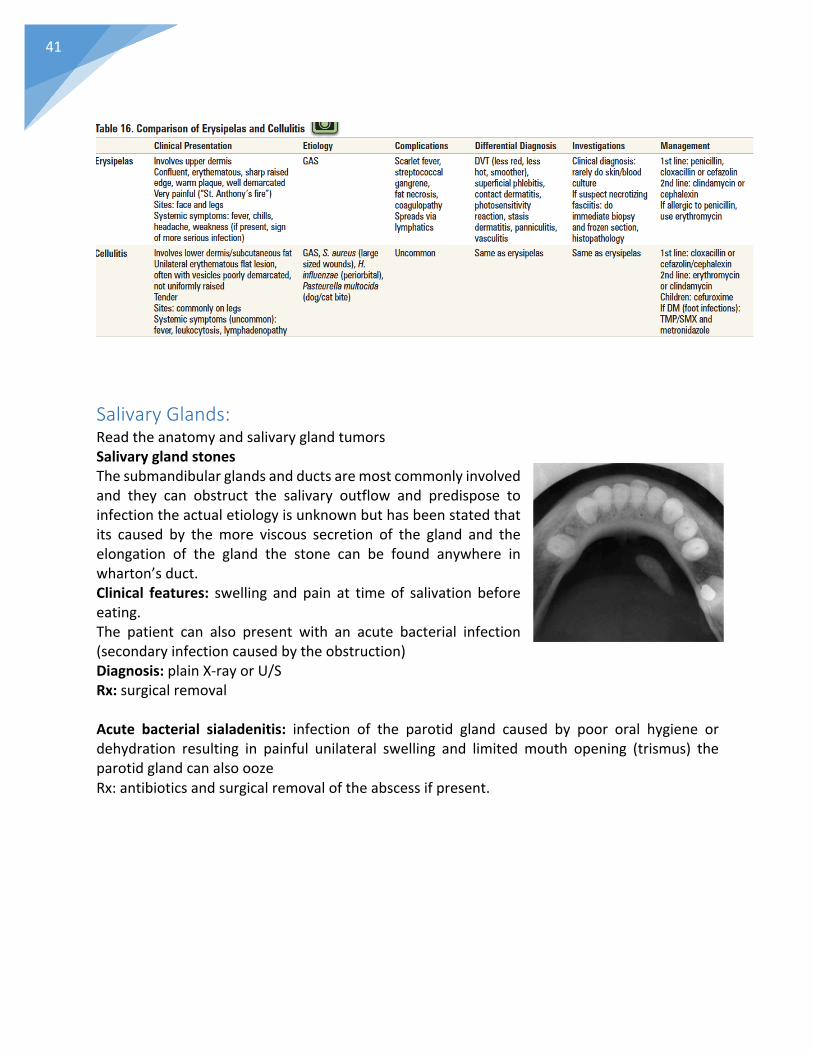
SalivaryGlands:ReadtheanatomyandsalivaryglandtumorsSalivaryglandstonesThesubmandibularglandsandductsaremostcommonlyinvolvedand they can obstruct the salivary outflow and predispose toinfectiontheactualetiologyisunknownbuthasbeenstatedthatits caused by themore viscous secretion of the gland and theelongation of the gland the stone can be found anywhere inwharton’sduct.Clinical features: swelling andpain at timeof salivation beforeeating.The patient can also present with an acute bacterial infection(secondaryinfectioncausedbytheobstruction)Diagnosis:plainX-rayorU/SRx:surgicalremovalAcute bacterial sialadenitis: infection of the parotid gland caused by poor oral hygiene ordehydration resulting in painful unilateral swelling and limitedmouth opening (trismus) theparotidglandcanalsooozeRx:antibioticsandsurgicalremovaloftheabscessifpresent.

42
Sutures:Howlongdowekeepthesutureforthefollowingcases?Midlinelaparotomy:~10days(indiabeticsandimmunocompromisedisupto14days)Cutwoundinfaceorneck:5-7daysLowerlimbs:14days
*KnowthecompositionandtypesofIVfluids






![-RLQ XV IRU OLJKW ELWHV DQG UHIUHVKPHQWV WR VXSSRUW M …ttdems.com/.../07/Matt-Holt-Fundraiser-Invite-2.pdf · m a t t h o l t 5ivstebz "vhvtu ] 1.-rlq xv iru oljkw elwhv dqg uhiuhvkphqwv](https://img.pdfslide.net/doc/110x75/5ecc2f8dbe47280079439692/rlq-xv-iru-oljkw-elwhv-dqg-uhiuhvkphqwv-wr-vxssruw-m-m-a-t-t-h-o-l-t-5ivstebz-vhvtu.jpg)






















