Embed Size (px)
Citation preview
THE WORLD BANK
December 2009
DRAFT REPORT ON
RESULTS BASED FINANCING
IN PUBLIC HEALTH SECTOR
IN INDIA
(CONTRACT NO. 7152956)
MSG STRATEGIC CONSULTING
PVT. LTD.

THE WORLD BANK
DRAFT REPORT ON RESULTS BASED FINANCING IN PUBLIC HEALTH SECTOR IN INDIA
CONTENTS
S. NO.
PAGE NO.
1. INTRODUCTION 1
TERMS OF REFERENCE 1
METHODOLOGY 1
PURPOSE AND STRUCTURE OF THE REPORT 2
2 SUMMARY AND RECOMMENDATIONS 3
KEY FINDINGS 3
RECOMMENDATIONS FOR IN-DEPTH ASSESSMENT 6
3 CONCEPTUAL FRAMEWORK 7
OBJECTIVES OF A RBF INITIATIVE 7
KEY COMPONENTS OF A RBF INITIATIVE 7
CLASSIFICATION OF RBF INITIATIVES 8
4 KEY FINDINGS 9
OVERVIEW 9
MATERNAL HEALTH SCHEMES 10
Empanelling private providers for maternity care 11
Performance incentives to increase institutional deliveries
12
Mobilisation of pregnant women 14
Maternal Deaths 15
CHILD HEALTH 15
FAMILY PLANNING 16
IMMUNISATION 17
DIAGNOSTIC & DRUG SERVICES 17
TRANSPORTATION 18
OVERALL HEALTH SERVICES 19
ANNEXES ATTACHED TO THIS REPORT
ANNEX 1 TERMS OF REFERENCE 2 DETAILS OF RESULTS BASED FINANCING INITIATIVES 3 BASIS FOR RECOMMENDATIONS OF RBF INITIATIVES FOR IN-DEPTH STUDY

LIST OF ABBREVIATIONS
ANM : Auxiliary Nurse Midwife
APL : Above Poverty Line
ASHA : Accredited Social Health Activist
AWW : Anganwadi Worker
BPL : Below Poverty Line
CCSP : Comprehensive Child Survival Programme
DLHS : District Level Household Survey
DRCHO : District RCH Officer
GOI : Government of India
IFA : Iron and Folic Acid
JSY : Janani Suraksha Yojana
MNGO : Mother NGO
NGO : Non Governmental Organisation
NRHM : National Rural Health Mission
OPD : Outpatient Department
PHC : Primary Health Centre
PIP : Programme Implementation Plan
PPP : Public Private Partnership
RBF : Results Based Financing
RCH : Reproductive and Child Health
RKS : Rogi Kalyan Samiti
SBA : Skilled Birth Attendant
SC/ ST : Schedule Castes and Scheduled Tribes

Results based financing in Public Health Sector in India – Draft Report
P a g e | 1
1. INTRODUCTION 1.01 Results Based Financing (RBF) is an incentive mechanism which deals with the transfer of money or material goods conditional on: taking a measurable action; achieving a predetermined performance target; or achieving certain desirable behaviour, etc. The transfer can be made at the individual, group, or institutional level. Where there is no result, no payment is made. 1.02 With the launch of the National Rural Health Mission (NRHM) the Government of India (GOI) has steeply increased allocation to the health sector. Increased central transfers to the states are based primarily on population and absorption capacity and are not linked to results. Introduction of RBF would strengthen incentives and accountability mechanisms and sharpen the focus on results. This would lead to improvement in the effectiveness of public health spending and thus contribute to achieving better health outcomes. 1.03 In India, the government has limited experience in RBF. The World Bank, along with local partner institutes is planning to host a national level workshop on RBF in January 2010. The workshop will be aimed at sensitizing and informing the participants about the successful RBF initiatives tried elsewhere and providing practical knowledge to launch RBF initiatives in the country. TERMS OF REFERENCE 1.04 In this context, World Bank retained MSG Strategic Consulting Pvt. Ltd. to carry out a background study to identify, enlist and provide a brief description of various supply side RBF initiatives in the public health sector in India. The assignment also includes developing a template in discussion with the World Bank for documenting the supply side initiatives and based on the documentation to recommend a few RBF initiatives for in-depth study. The terms of reference for this assignment are provided in Annex 1. METHODOLOGY 1.05 The documentation of the supply side initiatives covered 21 major states (including Delhi), which account for over 90% of India’s population. 1.06 The methodology for the assignment consisted of:
Desk review of (1) State Programme Implementation Plans (PIPs) for 2009-10 (and earlier years, where necessary) to obtain details of RBF initiatives (2) Directory of Innovations in the health sector, MoHFW and (3) Information available on the web.
Results based financing in Public Health Sector in India – Draft Report
2 | P a g e
Follow up (telephone/email) with states to fill data gaps, to the extent feasible.
Across the board, data on outcomes and administrative/ monitoring mechanisms has been limited. Standard centrally determined incentives to ASHAs across all states have not been covered as a part of the study. Further, certain initiatives with critical data gaps e.g. on performance indicators have been excluded. 1.07 The details of the references for each initiative are provided in the respective template in Annex 2. PURPOSE AND STRUCTURE OF THE REPORT 1.08 The purpose of this report is to set out key findings and recommendations. The structure of this report is as follows:
Chapter 2 provides a summary of findings and recommendations on RBF initiatives for indepth evaluation.
Chapter 3 provides a conceptual framework for analysis of RBF initiatives.
Chapter 4 sets out the key findings including classification of RBF initiatives by various criteria and a very broad assessment of status of each initiative based on data available.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 3
2. SUMMARY OF KEY FINDINGS AND RECOMMENDATIONS KEY FINDINGS
2.01 A total of 40 RBF initiatives have been identified, across 14 (out of 21) major states covered in the study, with Bihar and Maharashtra implementing as many as 7 initiatives each followed by Assam (4) and Gujarat, Uttar Pradesh and Uttarakhand (3 each). A majority (26) of the initiatives are being implemented throughout the respective state, 12 are under implementation in select districts (based on need) and 2 are being piloted in a few districts. Not surprisingly, the RBF initiatives are financed largely by GoI (RCH II / NRHM), either solely (35) or in conjunction with the State government (3). 2.02 Twenty-four (out of 40) initiatives (refer Exhibit 2.01) address maternal health related services followed by child health including immunisation (12) and overall health services (8). 12 initiatives address more than one area; for example, Outsourcing of Additional PHCs in Bihar covers overall health services expected from a Primary Health Centre; however the performance benchmarks that form the basis for the RBF are based on number of institutional deliveries and sterilisations.
EXHIBIT 2.01: OVERVIEW OF RBF INITIATIVES
S. No.
Service delivery area Name of state / Initiative
Mat
ern
al H
ealt
h
Ch
ild
Hea
lth
Fam
ily
Pla
nn
ing
Imm
un
isat
ion
Dia
gn
ost
ic
serv
ices
& G
ener
ic
dru
gs
Tra
nsp
ort
ati
on
Ove
rall
Hea
lth
S
ervi
ces
Assam
1 Performance incentives for Govt. facilities to improve Institutional deliveries
2 Incentive to ASHA for completion of Full immunisation
3 Chiranjeevi Yojana
4 Mobile Boat Clinics in Riverine Areas
Bihar
5 Muskaan
6 Ultra Modern Diagnostic Centre
7 Generic Drug Store
8 Radiology Services
9 Pathology Services
10 Additional PHCs Outsourcing � � �
11 Urban Health Centre � � �

Results based financing in Public Health Sector in India – Draft Report
4 | P a g e
EXHIBIT 2.01: OVERVIEW OF RBF INITIATIVES (CONTD...)
S. No.
Service delivery area Name of state / Initiative
Mat
ern
al H
ealt
h
Ch
ild
Hea
lth
Fam
ily
Pla
nn
ing
Imm
un
isat
ion
Dia
gn
ost
ic
serv
ices
& G
ener
ic
dru
gs
Tra
nsp
ort
ati
on
Ove
rall
Hea
lth
S
ervi
ces
Chhattisgarh
12 Incentive scheme
Delhi
13 Mamta Friendly Hospital Initiative
Gujarat
14 Chiranjeevi Yojana
15 Bal Sakha Yojana
16 Performance based incentive to Public health facility
Haryana
17 Janani Suvidha yojana
18 Jaccha Baccha Scheme
Kerala
19 Incentive schemes for specialists, MO
20 Call allowance incentive schemes for specialists
MP
21 Janani Express Yojana
22 Performance based incentive for doctors
Maharashtra
23 Incentive grant scheme to enhance institutional deliveries
24 Best Gram Panchayat Scheme
25 Honorarium to the state govt specialists doctors who render their services to adjacent hospitals
26 Screening of female deaths (15 to 49years) for enlisting suspected maternal deaths
27 Maternal Death Audit
28 Dai incentive scheme
29 Compensation to ASHA for promoting IUD 380A
Orissa
30 Incentive for institutional deliveries
31 Janani Express Yojana
Punjab
32 Alternate health care delivery system
33 Performance benchmarks for contractual staff
Uttar Pradesh
34 Soubhagyavati Scheme
35 Performance based incentive to honorary worker (Dais) at sub centres
36 Payment to ASHA under CCSP Program

Results based financing in Public Health Sector in India – Draft Report
P a g e | 5
EXHIBIT 2.01: OVERVIEW OF RBF INITIATIVES (CONTD...)
S. No.
Service delivery area Name of state / Initiative
Mat
ern
al H
ealt
h
Ch
ild
Hea
lth
Fam
ily
Pla
nn
ing
Imm
un
isat
ion
Dia
gn
ost
ic
serv
ices
& G
ener
ic
dru
gs
Tra
nsp
ort
ati
on
Ove
rall
Hea
lth
S
ervi
ces
Uttarakhand
37 Performance based incentives to ASHA
38 Performance based incentives for institutional deliveries
39 Mobile medical units
West Bengal
40 Ayushmati scheme
TOTAL 24 8 5 4 6 2 8
2.03 As many as 19 initiatives seek to primarily increase institutional deliveries. This includes:
PPP schemes wherein private providers / institutions are empanelled, based on a set of criteria, to provide safe delivery and allied services. Chiranjeevi Yojana in Gujarat is the forerunner of a host of similar schemes in five other states. An incentive is provided to the private obstetrician for conducting institutional deliveries. Payment is made per delivery conducted. Chiranjeevi covers only delivery care, whereas the offshoots address antenatal care, diagnostics, medicines, post natal care, and referral transport, to varying degrees. However, a recent addition, the Bal Sakha scheme also covers care for sick newborns. While all the above initiatives have a similar mechanism for budgeting, i.e. estimated cost of 100 deliveries with payment on a per unit basis, there are variations in terms of
Reimbursement to the patient for transportation costs and incentive money for ASHAs (Assam)
Provision of incentive to a grassroots level mobiliser (Janani Suvidha Yojana, Haryana); and
A disincentive by way of termination if the private provider performs less than 50 deliveries in a quarter (Saubhagyavati scheme in UP).
There is some evidence of success in the above schemes. Chiranjeevi Yojana in Gujarat was started as a pilot in 5 districts in 2005 and was upscaled across the state in 2007; similarly Ayushmati in West Bengal has been upscaled throughout the state, while scaling up of Janani Suvidha Yojana is planned.

Results based financing in Public Health Sector in India – Draft Report
6 | P a g e
Nine initiatives which provide performance based incentives to government staff for institutional deliveries/ other services. While in all cases the incentive is applicable after a benchmark (or threshold) there are several variations:
In Uttarakhand and Maharashtra, the benchmark is the number of deliveries in the corresponding month of the previous year; however Maharashtra has an additional minimum cut off of 3 deliveries per PHC per month. Chhattisgarh is the only state which has annual benchmarks.
The highest incentive being paid is in Madhya Pradesh (Rs. 1000 per C-section), and the lowest in Chhattisgarh (Rs. 25 per normal delivery). In Assam, the RKS decides the quantum of the incentive that each level of service provider in the facility will receive..
In Haryana (Jaccha Baccha Scheme), the payment made to the SBA differs for a male (Rs 400) and a female newborn (Rs 600).
Four of the nine initiatives also provide for incentive to the Rogi Kalyan Samiti (RKS), upon achievement of the facility level targets.
None of the RBFs explicitly take into account quality of services delivered, although eligibility criteria for private sector providers are in place. RECOMMENDATIONS FOR IN-DEPTH ASSESSMENT 2.04 Recommendations for in-depth assessment have been made primarily on the basis of the following criteria:
The RBF should have been under implementation for at least 2 years. Only 11 (out of 40) initiatives meet this criteria
There should be some evidence of success i.e. in terms of the initiative having been scaled up / increase in budget.
2.05 Out of the above 11 initiatives, there has been an increase in budget in 7, and 6 have been scaled up. Only 4 RBF initiatives meet all three criteria (refer annex for details). Indepth comparative evaluation of the following groups of initiatives is recommended:
Private sector institutional delivery schemes i.e. Chiranjeevi Yojana (Gujarat), Janani Suvidha Yojana (Haryana) and Ayushmati (West Bengal)
Transportation (referral/other) schemes i.e. Janani Express Yojana in MP and Orissa.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 7
3. CONCEPTUAL FRAMEWORK
OBJECTIVES OF A RBF INITIATIVE 3.01 As indicated in chapter 1, RBF deals with the transfer of money or material goods conditional on: taking a measurable action; achieving a predetermined performance target; or achieving certain desirable behaviour, etc. The transfer can be made at the individual, group, or institutional level. Where there is no result, no payment is made. 3.02 A RBF initiative seeks to:
Increase either demand or supply of a particular good or service by providing incentives linked to performance.
Increase accountability.
Improve the monitoring and evaluation system. KEY COMPONENTS OF A RBF INITIATIVE 3.03 Key components of a RBF initiative are:
A payer / financer – who funds the initiative
A recipient – who receives the funds
Eligibility criteria – for selection of the recipient
Set of services to be delivered (of acceptable quality) – by the recipient of the funds
Target population – to receive the services
A well-defined geographical area for provision of services
Performance indicators – measurable results that form the basis of payment to the recipient
Effective administrative mechanisms, including basis for measuring / validating results, payment formula (e.g. percentage of services delivered vs. rate of payment), payment procedures, dispute settlement and monitoring and evaluation system.
Our documentation/ analysis of RBF initiatives focuses on the above key components.

Results based financing in Public Health Sector in India – Draft Report
8 | P a g e
CLASSIFICATION OF RBF INITIATIVES 3.04 The supply side RBF initiatives currently operational in the public health sector could be classified in several ways:
a. On the basis of the payer and the financer
Government to a health facility (public, private)
Government to an individual (public, private)
Government to an organisation (public, private / NGO)
b. On the basis of the payment formula
Payment per unit of service provided
Payment based on achievement of specific target levels
Payment as a percentage/ratio of the end product
c. On the basis of technical area
Maternal Health – antenatal care, institutional deliveries, post natal care, maternal death audit
Child Health – child death audit, malnutrition, incentive to bring critically ill children to the hospital
Family Planning – IUD services
Immunisation
Referral transport
General services – primary health care, diagnostic services, facility outsourcing
d. On the basis of the target population
BPL
SC/ST
Urban Slums
Entire population
Pregnant women
Infants
Women in the 19 to 49 years age category Analysis of RBF initiatives has been carried out in terms of the above variables, to the extent data was available.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 9
4. KEY FINDINGS OVERVIEW 4.01 A total of 40 schemes have been identified, across 21 major states (detailed documentation in Annex 2). Of these, a majority of the schemes are financed by RCH II / NRHM, either solely (35) or in conjunction with the State government (3):
Sn. Payer Number 1. NRHM / RCH II 35
2. State Government 1
3. Both 3
4. NA 1 Total 40
4.02 In terms of the geographical area of coverage, a majority (26) of the schemes are being implemented throughout the respective state, twelve (12) are under implementation in select districts (based on need), and two (2) are being piloted in a few districts.
Sn. Coverage Number
1. State-wide 26 2. In limited districts / areas 12
3. Pilot in a few districts 2 Total 40
4.03 The recipients of the RBF initiatives on the other hand are more equitably distributed between public and private. The public recipients are mostly individual health care providers, whereas the private schemes mostly target a facility or an organisation.
Sn. Recipient
Public Private Total
1. Individual 13 5 18 2. Facility - 5 5 3. Group of providers 3 - 3 4. Both group / individual &
facility 4 2 6
5. Organisation 1 8 9 Total 21 20 41* * - one of the schemes covers both public and private individuals
Results based financing in Public Health Sector in India – Draft Report
10 | P a g e
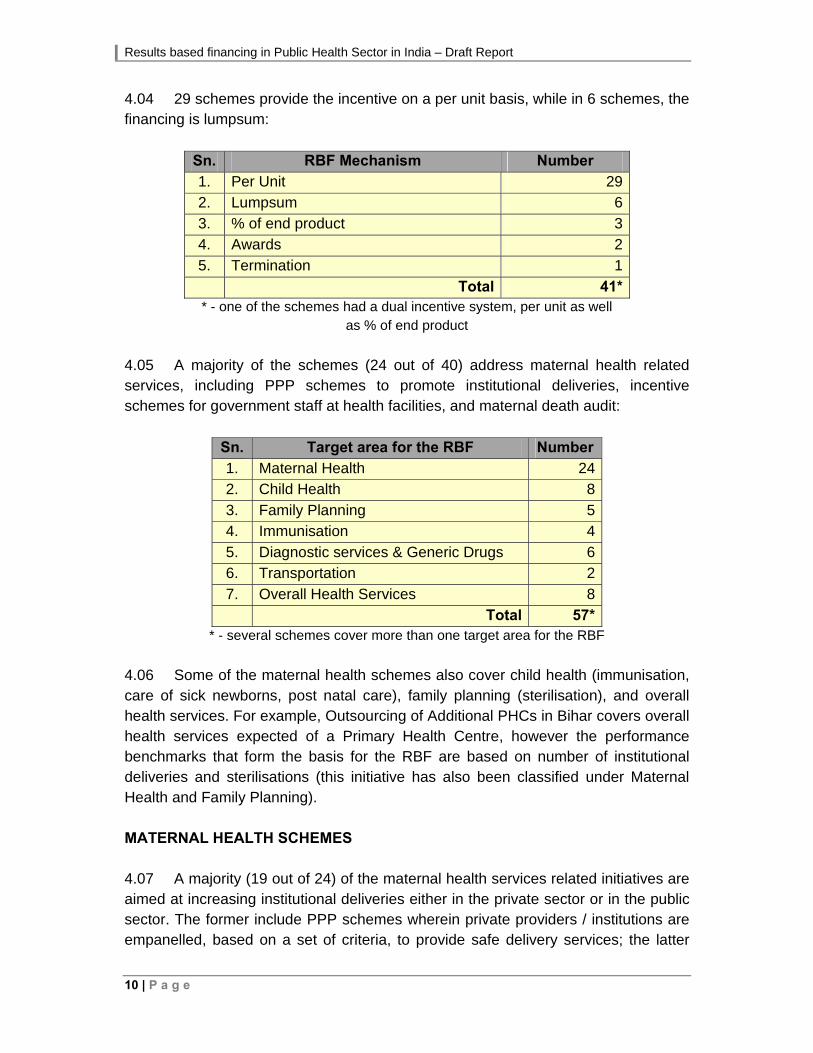
4.04 29 schemes provide the incentive on a per unit basis, while in 6 schemes, the financing is lumpsum:
Sn. RBF Mechanism Number 1. Per Unit 29
2. Lumpsum 6
3. % of end product 3
4. Awards 2
5. Termination 1
Total 41* * - one of the schemes had a dual incentive system, per unit as well
as % of end product
4.05 A majority of the schemes (24 out of 40) address maternal health related services, including PPP schemes to promote institutional deliveries, incentive schemes for government staff at health facilities, and maternal death audit:
Sn. Target area for the RBF Number
1. Maternal Health 24 2. Child Health 8
3. Family Planning 5 4. Immunisation 4
5. Diagnostic services & Generic Drugs 6 6. Transportation 2
7. Overall Health Services 8 Total 57*
* - several schemes cover more than one target area for the RBF
4.06 Some of the maternal health schemes also cover child health (immunisation, care of sick newborns, post natal care), family planning (sterilisation), and overall health services. For example, Outsourcing of Additional PHCs in Bihar covers overall health services expected of a Primary Health Centre, however the performance benchmarks that form the basis for the RBF are based on number of institutional deliveries and sterilisations (this initiative has also been classified under Maternal Health and Family Planning). MATERNAL HEALTH SCHEMES 4.07 A majority (19 out of 24) of the maternal health services related initiatives are aimed at increasing institutional deliveries either in the private sector or in the public sector. The former include PPP schemes wherein private providers / institutions are empanelled, based on a set of criteria, to provide safe delivery services; the latter

Results based financing in Public Health Sector in India – Draft Report
P a g e | 11
largely provide incentives to staff to promote institutional deliveries. Other maternal health related initiatives address maternal death audits and mobilisation of pregnant women. Empanelling private providers for maternity care 4.08 Chiranjeevi Yojana in Gujarat is an NRHM / RCH II and State Govt. initiative which is the forerunner of a host of similar schemes across states. It provides an incentive to the private obstetrician for conducting institutional deliveries. Payment is made per delivery conducted. The range of services is limited to delivery care, whereas other offshoots address antenatal care, diagnostics, medicines, post natal care, and referral transport, to varying degrees:
S. no.
Name of the initiative
State Payer RecipientGeographical area covered
Services PaymentFormula
1 Chiranjeevi Yojana
Assam NRHM Facility Pilot in 6 districts
ANC, institutional delivery, diagnostics, medicines
Per unit
2 Mamta Friendly Hospital Initiative
Delhi NRHM Facility Limited to 6 districts
ANC, referral transport, institutional deliveries, PNC, immunisation
Per unit
3 Chiranjeevi Yojana
Gujarat NRHM & State Govt
Facility Entire state Institutional deliveries
Per unit
4 Janani Suvidha Yojana
Haryana NRHM/ RCH II
Individual, Facility
Urban slums, state-wide
Institutional deliveries, ANC, newborn care, breastfeeding counselling
Per unit
5 Saubhagyavati Scheme
U.P. NRHM/ RCH II
Facility Entire state Institutional deliveries, ANC visits, diagnostics
Per unit
6 Ayushmati scheme
West Bengal
NRHM/ RCH II
Facility Entire state Institutional deliveries, PNC, diagnostics
Per unit
However, a recent addition, the Bal Sakha scheme, provides additional care for sick newborn (details under Child Health). 4.09 Each of the above schemes has a similar mechanism for budgeting, i.e. costing has been done for 100 patients, and payment is on a per unit basis. However, there are variations across the schemes:
a. Chiranjeevi Yojana in Assam also provides reimbursement to the patient for transportation costs, and incentive money for ASHAs.
b. Janani Suvidha Yojana, a voucher scheme, provides incentive to a grassroots level mobiliser / motivator (“Sakhi”), in addition to the private provider.
c. The Saubhagyavati scheme in UP has a disincentive incorporated in the contract. If an agency performs less than 50 deliveries in a quarter then the

Results based financing in Public Health Sector in India – Draft Report
12 | P a g e
agency is debarred from the scheme. This is the only scheme of its kind where there is a minimum target that the private provider has to achieve to avoid termination of the contract. Moreover, the verification of data is done by an independent agency wherein 25% of the beneficiaries are verified. In case of fake reporting/ gaps in service a financial penalty will be imposed as per the state guidelines, and three continuous defaults will result in blacklisting of the service provider.
4.10 There is some evidence of success in these schemes. Chiranjeevi Yojana in Gujarat was started as a pilot in 5 districts in 2005 and was upscaled across the state in 2007; similarly Ayushmati has been upscaled throughout the state, while scaling up of Janani Suvidha Yojana is planned. However, as highlighted in the 3rd NRHM Common Review Mission (Nov 2009), there are some concerns over quality of care in Chiranjeevi Yojana (Gujarat). Performance incentives to increase institutional deliveries 4.11 There are as many as nine initiatives which provide performance based incentives to government staff:
S. no.
Name of the initiative
State Payer Recipient Services Payment Formula
Benchmark1
Frequency Level
1
Performance incentives for Govt. facilities to improve Institutional deliveries
Assam NRHM/ RCH II
Group, facility
Institutional deliveries
Per unit monthly facility
2 Incentive Scheme
Chhattisgarh NRHM/ RCH II
Group Institutional deliveries
Per unit annual facility
3
Performance incentive to Public health facility
Gujarat State Govt.
Group, facility
Institutional deliveries
Per unit monthly facility
4 Jaccha Baccha Scheme
Haryana NRHM/ RCH II
Group Institutional deliveries
Per unit monthly individual
5
Performance based incentive for doctors
Madhya Pradesh
NRHM/ RCH II
Individual
C-sections, MTP, sterilisations, care of sick newborns, care of ARI & diarrhoea cases
Per unit monthly individual
1 Base level performance above which incentive is applicable.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 13
S. no.
Name of the initiative
State Payer Recipient Services Payment Formula
Benchmark1
Frequency Level
6 Incentive for staff
Maharashtra NRHM/ RCH II
Group Institutional deliveries
Per unit monthly facility
7 Incentive for institutional deliveries
Orissa NRHM/ RCH II
Group, facility
Institutional deliveries
Per unit monthly facility
8
Performance benchmarks for contractual staff
Punjab NRHM/ RCH II
Individual
Institutional deliveries, ANC, immunisation, breastfeeding
Termination monthly individual, facility
9
Performance based incentives for institutional deliveries
Uttarakhand NRHM/ RCH II
Group, facility
Institutional deliveries
per unit monthly facility
4.12 The above cover performance incentives for institutional deliveries/ other services. Except for the incentive scheme in Gujarat funded by the State government, all others are funded under NRHM / RCH II. All the above schemes are running state-wide, the only exception being the initiative in Maharashtra, which is limited to 99 talukas which have home deliveries greater than 50%. 4.13 Four of the nine schemes also provide for incentive to the Rogi Kalyan Samiti (RKS), upon achievement of the facility level targets. For the remaining five schemes providing incentives only to individuals / groups of providers (where the RKS does not receive any incentive), the benchmarks could be either at facility or individual levels. Punjab has the only initiative where there is no monetary incentive, but a “disincentive” of termination of the contractual service providers for not achieving the monthly targets (which are a percentage of the facility level targets) for 3 consecutive months. Also, the liability is not clear if the facility itself does not meet its targets. 4.14 The benchmarks themselves vary across states. Chhattisgarh is the only state which has annual benchmarks. The other unique feature of this initiative is that the block administrators (block medical officer, block programme manager, and block staff) also have to attain a benchmark to receive an incentive. In Uttarakhand and Maharashtra, the benchmark is the number of deliveries in the corresponding month of the previous year; however Maharashtra has an additional minimum cut off of 3 deliveries per PHC per month. 4.15 The incentive received by the providers varies across states, with the highest being in Madhya Pradesh (Rs. 1000 per C-section), and the lowest in Chhattisgarh (Rs. 25 per normal delivery). In fact, in Assam, the RKS decides the quantum of the incentive that each level of service provider in the facility will receive, which is a corporate type of practice.
Results based financing in Public Health Sector in India – Draft Report
14 | P a g e
4.16 In Haryana (Jaccha Baccha Scheme), the payment made to the SBA differs for a male and a female newborn. In the case of a male newborn the SBA receives Rs.400 while Rs.600 for a female newborn. Haryana’s sex ratio is amongst the worst in the country, and therefore this difference in payment for a male and female newborn child is seen as a step for reducing their female infanticide and improving their sex ratio. Mobilisation of pregnant women 4.17 The above schemes are all examples where the RBF initiatives’ recipients are those that conduct or assist in an institutional delivery. Promotion of institutional deliveries through interpersonal counselling is the responsibility of village level service providers (Dais, ASHAs, Sakhis etc). Four states provide incentives to field level service providers to promote institutional deliveries. In Uttar Pradesh and Maharashtra, the Dais receive a performance based incentive for bringing the delivery cases to the hospital. In Maharashtra the initiative has not been implemented in the entire state but is restricted to only those districts where ASHAs have not been appointed so as to avoid conflict. In Uttar Pradesh, the NRHM has sponsored incentives for the Dais across the entire state for providing support in deliveries and in clinics. The Dai receives remuneration for each activity that she carries out – Rs. 100 per delivery and Rs. 25 per clinic. The variation between the payment mechanisms of the Dais in the two states is that in U.P. there is an upper limit of 2 deliveries and 4 clinics per month, thus curbing the incentive for the Dai. 4.18 Janani Suvidha Yojana, an initiative implemented in only 8 districts in Haryana initially (and in view of its satisfactory implementation, it is planned to be scaled up state-wide), is now in its fourth year. The initiative provides a performance based incentive to the Sakhis for facilitating the pregnant women for availing ANC checkups, institutional deliveries, post natal checkups, essential newborn care, post delivery IU/ sterilisation if need be, and immunisation of the child. The Sakhi is a link between the client and the private health provider and is a resident woman from the urban slum selected per 1000 people. This initiative targeted towards pregnant women in the urban slums, has a minimum number of cases that need to be achieved for every month, above which payment will be made. In this initiative a bonus on completion of all services is given as appreciation. The number of institutional deliveries has increased steadily and to continue the positive impact and to avoid a fall out, an increase in the incentive to a Sakhi has been planned. 4.19 In Uttarakhand, a performance based incentive for ASHAs was initiated in 2007. However the scope of services to be delivered by ASHA was broadened to be a comprehensive package of incentives for delivering services to pregnant women and newborns in 09-10 after progress was noted in the indicators seen in NFHS-3 and DLHS-3. The services for which the ASHA receives remuneration presently are
Results based financing in Public Health Sector in India – Draft Report
P a g e | 15
ANC registration in the first trimester, three ANC checkups, two TT injections, consumption of 100 IFA tablets, birth registration and early initiation of breastfeeding and exclusive breastfeeding. Payment will be made per service provided per beneficiary. However unlike the payment formula applicable to a Sakhi in Haryana, there is no bonus on completion of all services to be provided, and payment is given for each component of the package that is provided by the ASHA. Therefore there is no motivation to the ASHA to complete all the components of the package. Since the payments are made each month on the components of the package covered, it is not clear how the tracking / monitoring will be done to ensure that each pregnant woman receives the entire package given that the services will be spread over 12-15 months. Under Janani Suraksha Yojana (JSY) all of the services mentioned above (except for birth registration), are intended to be covered by the ASHA, along with motivating pregnant women for institutional delivery and accompanying them to the institution, for which she receives an incentive per case. However, review visits to various states show that the focus seems to be more on the institutional delivery component of JSY. Maternal Deaths 4.20 Identification of the causes of maternal mortality is essential to take corrective steps at the local/ state level, and GoI has recently released guidelines for conduct of facility-based maternal death audit. Maharashtra has two RBF initiatives on-going in this regard. The first entails the screening off all female deaths in the age group of 15 to 49 years, following which analysis at the district level by the DRCHO is carried out to identify maternal deaths and then accordingly carry out investigations. The Extension Officer of Health, Panchayat Samiti gets an incentive of Rs. 200 per month on completion of the screening all the female death cases in the age group mentioned. The second is a Maternal Death Audit carried out by the District RCH Officer, who visits the deceased’s house, does the verbal autopsy and identifies the circumstantial evidence related to the maternal death. The causes identified by the DRCHO are discussed in the district Maternal Death Audit Committee constituted in each district, to take necessary corrective action. The DRCHO, unlike the extension officer of health of the Panchayat Samiti, receives an honorarium of Rs. 200 per maternal death audit conducted, and Rs. 300 for mobility support, report writing etc. CHILD HEALTH 4.21 Bal Sakha Yojana, a child health RBF initiative in Gujarat was launched in January 2009 by NRHM and the state government of Gujarat to improve the provision of outpatient services, referral transport services, in-patient care, initial vaccination etc. The service providers are either private paediatricians in a partnership with Chiranjeevi doctors or independent private paediatricians. The remuneration is done per unit; however, the rates differ for the paediatrician in a

Results based financing in Public Health Sector in India – Draft Report
16 | P a g e
partnership with the Chiranjeevi Yojana doctor and the independent private paediatrician as infrastructure costs are not applicable to both. The private providers are given an advance of Rs. 25,000 and thereafter claims are made via vouchers. 4.22 The second RBF initiative is an incentive to ASHAs under the Comprehensive Child Survival Programme (CCSP) in Uttar Pradesh, to conduct follow up visits and counselling on newborn care, especially for low birth weight babies. This scheme was initiated in 2007-08, however, actual implementation began in 2008-09. At present the initiative covers seventeen old CCSP districts and nineteen new districts. Each ASHA worker receives payment on completion of 6 visits to each low birth weight newborn (Rs. 100) and 3 visits to each normal weight newborns (Rs.50). No details are available regarding the process of verifying the data, the payment procedure or the outcomes of the RBF initiative.
4.23 In addition, child health issues are also addressed by other schemes, i.e. Janani Suvidha Yojana in Haryana, Performance based incentives to ASHAs in Uttarakhand, Ayushmati Scheme in West Bengal, Performance Benchmarks for contractual staff in Punjab, etc. (details in Annex 2). FAMILY PLANNING 4.24 Four out of the 40 schemes address family planning, including for both sterilisations and spacing. Three schemes address sterilisation (including the performance incentive for specialists in MP), while the fourth initiative is for ASHA workers to mobilise the eligible couples for IUD insertion services and counselling. 4.25 In Bihar, APHC outsourcing and the Urban Health centre, both have the same payment formula for performing a certain number of deliveries per month along with a certain number of family planning operations. The target levels are the same – more than 55 deliveries/month and more than 40 family planning operations per month. On achievement of these targets, the facility receives Rs.10,000. Both these schemes were initiated in 2008-09 and outcomes for the same have not been recorded. 4.26 The incentive for ASHA workers in Maharashtra was implemented in 2008-09 and is still in its pilot stage. At present all ASHA workers in Amravati and Parbhani districts are eligible under this initiative. The ASHA worker receives payment for every IUD insertion at the rate of Rs. 75 and on retention of the IUD after three months and follow up ASHA receives Rs.25. An evaluation is proposed to be carried out to study the effectiveness of the initiative in the two districts. The number of achieved insertions can be compared to the expected level of IUD insertions mentioned in the PIP.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 17
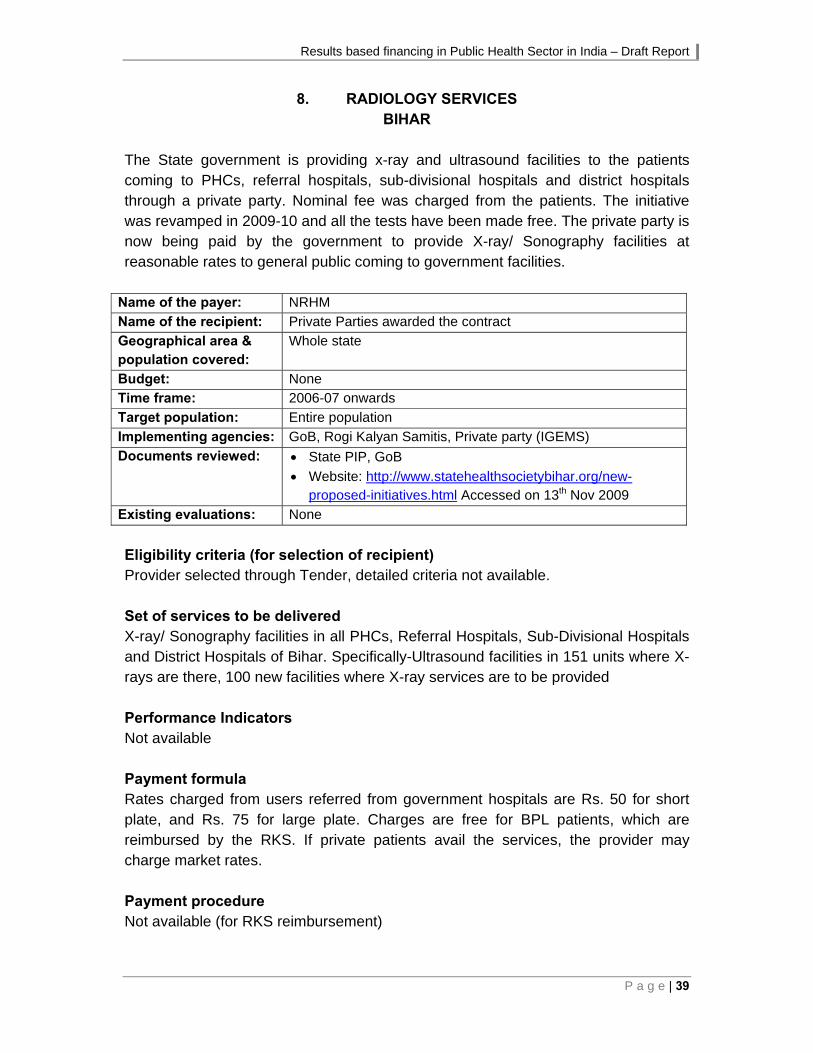
IMMUNISATION 4.27 Three out of the 40 schemes deal with immunisation. Muskaan in Bihar is an NRHM initiative launched in 2007 with the objective to achieve 100% immunisation of infants and pregnant women. ASHAs, AWWs and ANMs receive incentives on the basis of the number of immunisation sessions carried out and the number of beneficiaries in each session. Hence, the motivation is to mobilise more beneficiaries per session and to carry out all the planned sessions. The existing evaluations for the initiative show that there has been a positive impact. 4.28 In Assam, there is an incentive program in place to increase the full immunisation in children, and to reduce the drop-out rate between the BCG vaccination and the Measles vaccine. The ASHA worker receives Rs. 250 per child below one year of age who is fully immunised. Follow up and counselling is a part of the services to be delivered by the ASHA. A record of the number of infants fully immunised is maintained in the ASHA booklet against which payment is made at the monthly ASHA meeting by the Block Programme Manager. 4.29 In Punjab, the performance benchmarks for the contractual staff include a monthly benchmark for the MPHW (F) posted at sub centres, viz. 100% immunisation of the pregnant women and children. Non achievement of the benchmarks for 3 months continuously will be grounds for termination of the contract. A monthly and quarterly review of the benchmarks is to be done, however the monitoring/ verification mechanism hasn’t been clearly spelt out. DIAGNOSTIC & DRUG SERVICES 4.30 All the diagnostic and drug services based RBF initiatives are being implemented in Bihar. The diagnostic centre and generic drugs schemes are on a revenue sharing model, while the pathology services are on a per unit reimbursement model. 4.31 Radiology services in Bihar have been operational since 2006. Space is made available in the hospital for providing the services. A delay in set up, results in liquidation damages of 1% of Bank guarantee for every delay of 30 days. The set of services to be delivered include X Ray/ Sonography facilities in all PHCs, Referral Hospitals, Sub – Divisional Hospitals and the District Hospitals of Bihar. The 151 X-ray units at present are to be equipped with Ultrasound facilities as well and 100 new facilities providing X-Ray services are to be provided as well. A nominal rate is charged from the patients referred by the government hospitals, while market rates may be charged from private patients. Services for BPL patients are free and reimbursed by the RKS.

Results based financing in Public Health Sector in India – Draft Report
18 | P a g e
4.32 Pathology services in 7 districts in Bihar were also operational since 2006-07. Here again the facility is selected through the process of a tender. The set of services to be delivered includes provision of pathology services in rural Bihar – Bio –chemistry, Haematology, Pathology, Micro-Biology, Serology, Clinical pathology. In 2008-09 all the tests were made free. And now the government of Bihar reimburses all the charges to the service provider. 4.33 Ultra Modern diagnostic centres, Bihar is an initiative funded by NRHM since 2008-09. Operational in a few districts in the state, the facility is present in the Regional diagnostic centres of the districts and 6 medical colleges. The services to be provided included Pathology, Bio-Chemistry, Radiology, Digital X ray, USG, CT Scan, MRI, ECG and Mammography. Reimbursement for services provided to BPL families is done through the RKS. Fines are levied for delay in the operationalisation of labs. TRANSPORTATION 4.34 The two Janani Express schemes (Madhya Pradesh and Orissa) are quite similar, the latter an adaptation of the former. Both of them primarily cater to transport of pregnant women for institutional delivery, but also provide services for referral of sick newborns and emergency cases. However, there are some differences:
a. In MP, the rate per case is divided in two slabs – Rs. 150 for < 25 km and Rs. 250 for > 25 km. For beneficiaries under JSY, funds will be provided from the scheme. For other cases, no charges are to be levied from BPL patients (APL patients pay as per above rates). The rate per case is not clear for Orissa. However, both have a fixed monthly rent.
b. The MP model has a fixed monthly benchmark of 1200 km, and any utilisation above this is to be reimbursed at a per km. rate fixed in the contract; not so in Orissa.
c. In MP, if the amount generated per month is higher than the monthly rent, then incentive is given to the provider based on certain slabs: upto 125% - no incentive; 125-150% - incentive of 25% of monthly rental; and 150-200% – incentive of 35% of monthly rental. In Orissa, an incentive of Rs. 10/- for each additional case of attending to a pregnant mother to and fro above 50 institutional deliveries with a minimum mileage of 1500 km per month will be allowed to the driver. This is to ensure that the driver caters to cases of remote villages also. Similarly for every additional case above 100 institutional deliveries with a minimum mileage of 2500 km per month, Rs. 20/- will be given to driver as incentive.
Results based financing in Public Health Sector in India – Draft Report
P a g e | 19
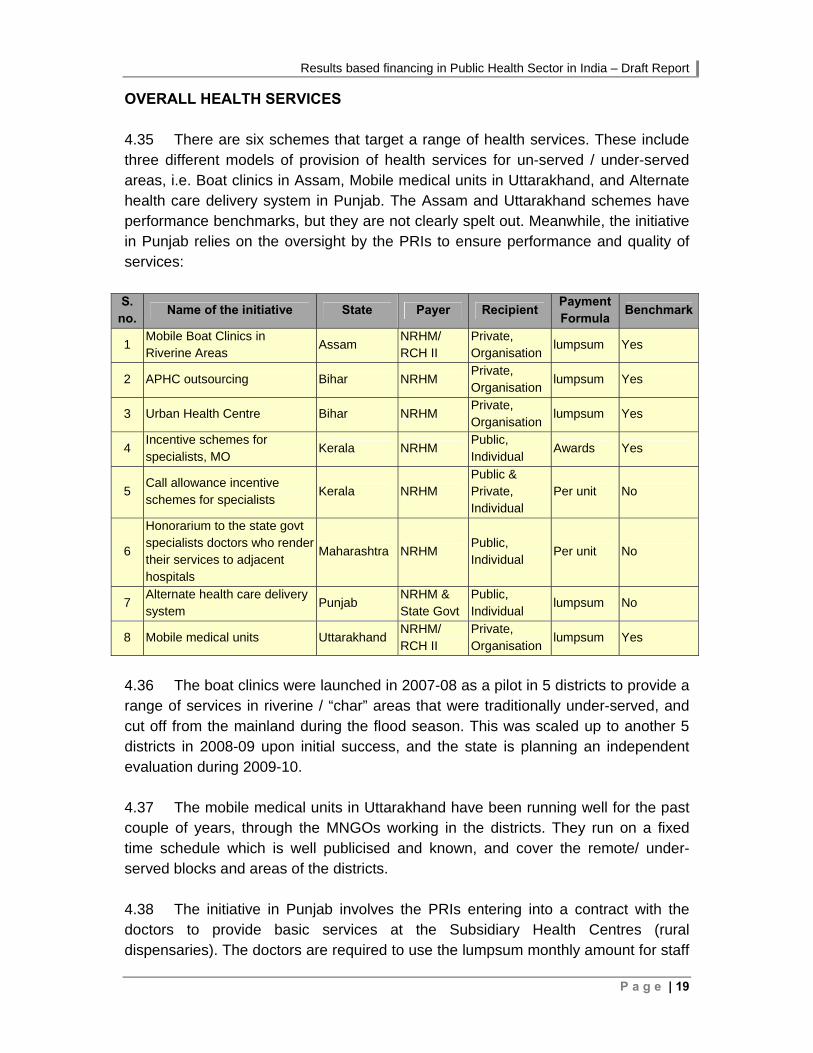
OVERALL HEALTH SERVICES 4.35 There are six schemes that target a range of health services. These include three different models of provision of health services for un-served / under-served areas, i.e. Boat clinics in Assam, Mobile medical units in Uttarakhand, and Alternate health care delivery system in Punjab. The Assam and Uttarakhand schemes have performance benchmarks, but they are not clearly spelt out. Meanwhile, the initiative in Punjab relies on the oversight by the PRIs to ensure performance and quality of services: S.
no. Name of the initiative State Payer Recipient
Payment Formula
Benchmark
1 Mobile Boat Clinics in Riverine Areas
Assam NRHM/ RCH II
Private, Organisation
lumpsum Yes
2 APHC outsourcing Bihar NRHM Private, Organisation
lumpsum Yes
3 Urban Health Centre Bihar NRHM Private, Organisation
lumpsum Yes
4 Incentive schemes for specialists, MO
Kerala NRHM Public, Individual
Awards Yes
5 Call allowance incentive schemes for specialists
Kerala NRHM Public & Private, Individual
Per unit No
6
Honorarium to the state govt specialists doctors who render their services to adjacent hospitals
Maharashtra NRHM Public, Individual
Per unit No
7 Alternate health care delivery system
Punjab NRHM & State Govt
Public, Individual
lumpsum No
8 Mobile medical units Uttarakhand NRHM/ RCH II
Private, Organisation
lumpsum Yes
4.36 The boat clinics were launched in 2007-08 as a pilot in 5 districts to provide a range of services in riverine / “char” areas that were traditionally under-served, and cut off from the mainland during the flood season. This was scaled up to another 5 districts in 2008-09 upon initial success, and the state is planning an independent evaluation during 2009-10. 4.37 The mobile medical units in Uttarakhand have been running well for the past couple of years, through the MNGOs working in the districts. They run on a fixed time schedule which is well publicised and known, and cover the remote/ under-served blocks and areas of the districts. 4.38 The initiative in Punjab involves the PRIs entering into a contract with the doctors to provide basic services at the Subsidiary Health Centres (rural dispensaries). The doctors are required to use the lumpsum monthly amount for staff

Results based financing in Public Health Sector in India – Draft Report
20 | P a g e
salaries (self, pharmacist, cleaner, etc.) and utilities. The government provides the drugs and consumables, and any equipment and repairs needed. The oversight provided by the community / PRIs is the benchmark to ensure that services are provided and quality maintained. 4.39 The schemes in Kerala and Maharashtra provide honorarium/ incentive on a per case basis to doctors and specialists for provision of services. The Maharashtra model aims to ensure that services are made available in health facilities that don’t have specialists (due to HR shortage) through existing resources in the government system, from neighbouring health institutions. There is no ceiling. On the other hand, the Kerala model provides for services delivered beyond working hours, by various specialists on call basis. These could be from the same institution, government institutions in the area, or from the private sector. While there is a ceiling on the number of calls per month for which incentive will be provided, the provider may not use this excuse to not attend a call. If an unsatisfactory reason is provided for not attending a call, the doctor may face disciplinary action (public sector) / removal from the panel (for private sector). 4.40 The two PPPs in Bihar provide overall health services to their target populations (rural for Additional PHCs, and urban poor for the Urban Health Centres) and get a fixed monthly amounts for services provided as per contract. However, however as mentioned earlier, they also get a lumpsum performance incentive upon achievement of certain targets for institutional deliveries and sterilisations.
ANNEX 1
TERMS OF REFERENCE


Results based financing in Public Health Sector in India – Draft Report
P a g e | 21
RESULTS BASED FINANCING IN PUBLIC HEALTH SECTOR IN INDIA: TOR FOR DOCUMENTING RBF INITIATIVES
Background One of the key systemic constraints to achieving better health outcomes in India is low effectiveness of public spending on health, including quality and coverage, due to: (i) general absence of accountability arrangements and incentives for performance, including deficient public management and fiduciary processes; (ii) ineffective targeting and inadequate emphasis on core public health functions; and (iii) very weak information environment, including deficient monitoring and near absence of impact evaluations. With the launch of National Rural Health Mission the GOI has steeply increased allocation to the health sector. Increased central transfers to the states is based on population criteria and supply of infrastructure (e.g., staff per facility) and are not linked to demand or results in any manner. Likewise, increased, and more flexible, funding to health facilities is not linked to results. Introduction of Results Based Financing (RBF)2 would strengthen incentives and accountabilities mechanisms and sharpen the focus on results and thereby would help to improve effectiveness of public health spending which will directly contribute to achieving better health outcomes. Not all kinds of incentives qualify as RBF. RBF deals with transfer of money or material goods conditional on taking a measurable health- related action or achieving a predetermined performance target. The transfer can be made at the individual, group, or institutional level. Financial risk is what drives the change. Where there is no result, no payment is made. Internationally, RBF are being tried in variety of areas. For example, public health facilities such as hospitals are receiving government funding on the basis of performance, over and above the base funding. Likewise, RBF initiatives include staff in health facilities or even community health workers getting incentives on the basis of some performance criteria. Even central government transfers to states as well as transfers from states to districts being made on the basis of achieving certain benchmarks rather than on norm basis. Initiatives that transfer funds to the beneficiaries for seeking care from accredited facilities are demand side RBF. In short, RBF can be viewed as an incentive design mechanism whereby funding is given to individuals, organizations or entities on the basis of certain milestones which
2 RBF is also known by various other names such as Pay for Performance or “P4P”, Output-Based Financing, Performance-Based Financing, Performance-Based Incentives and so forth.

Results based financing in Public Health Sector in India – Draft Report
22 | P a g e
could be outputs, certain level of efficiency or quality or achieving certain desirable behaviour and for forth. Government of India has limited experience in RBF. Through its national flagship program in the health sector, the National Rural Health Mission (NRHM), it is providing financial incentives to pregnant mothers as well as field staff for promotion of institutional deliveries (Janani Suraksha Yojana (JSY) or its variant called JSBY in Bihar and MP). Also, a few Indian states are experimenting with a network of private providers who are being paid a fixed (average) amount per institutional delivery by the poor women at private facilities. These initiatives have performed relatively well, according to available monitoring reports. Nevertheless, the future success of these initiatives may be hampered by low productivity of health providers and poor quality of care delivered at health care facilities frequented by the poor. The World Bank, along with a local partner institutes, is planning to host a national level workshop on RBF sometime in January 2009. The workshop will be aimed at sensitizing and informing the participants, many of whom will be health policy makers at central and state level, about the successful RBF initiatives tried elsewhere, and providing practical, nuts-and-bolts knowledge to launch RBF initiatives. There is a clear knowledge gap which the proposed national level workshop on RBF will help in bridging. The World Bank is interested in commissioning a background study on RBF initiatives in India. This consultancy is for Phase 1 of this study. Objective To identify, enlist and provide a brief description of various supply side RBF initiatives in public health sector in India. Main Activities
To identify and enlist all possible supply side RBF initiatives ongoing in the public health sector in India as well as various supply side RBF initiatives between public and private (not-for-profit as well as for-profit) entities, irrespective of whether they are government funded or donor funded (a few types of supply side initiatives appear later in the document)
To develop a template in discussion with the World Bank for a documenting a brief description of the RBF initiatives (see a draft template later in the document)
To fill out the template for each of the identified initiatives
ANNEX 2
DOCUMENTATION OF RESULTS BASED FINANCING
SCHEMES


Results based financing in Public Health Sector in India – Draft Report
P a g e | 23
S. no.
Name of the initiative
State Payer Recipient
Public/Pvt.Recipient
Geographical area covered
RBF Area RBF Services PaymentFormula
Benchmark
1 Performance incentives for Govt. facilities to improve Institutional deliveries
Assam NRHM/ RCH II
Public Group, facility
Entire state Maternal Health Institutional deliveries Per unit Yes
2 Incentive to ASHA for completion of Full immunisation
Assam NRHM Public Individual Entire State Immunisation Follow up and counselling on immunisation
Per unit No
3 Chiranjeevi Yojana Assam
NRHM/ RCH II
Pvt. Facility Pilot in districtsMaternal Health, Diagnostic Services
ANC, institutional delivery, diagnostics, medicines
Per unit No
4 Mobile Boat Clinics in Riverine Areas
Assam NRHM Pvt. Organisation Limited Overall Health Services
Primary health care lumpsum Yes
5 Muskaan Bihar
NRHM/ RCH II
Public Individual Entire State Immunisation, Maternal Health
Immunisation to children and pregnant women
Per unit Yes
6 Ultra Modern Diagnostic Centre
Bihar NRHM Pvt. Organisation Limited Diagnostic Services
Pathology and Radiology services
% of end product
No
7 Generic Drug Store Bihar NRHM Pvt. Organisation Entire state Generic Drugs Generic drugs
% of end product
No
8 Radiology Services Bihar NRHM Pvt. Organisation Entire state
Diagnostic Services
Radiology Per unit No
9 Pathology Services Bihar NRHM Pvt. Organisation Limited
Diagnostic Services
Pathology Per unit No
10 Additional PHCs Outsourcing
Bihar NRHM Pvt. Organisation Limited Maternal Health, Family Planning
Institutional deliveries, sterilisations
lumpsum Yes
11 Urban Health Centre Bihar NRHM Pvt. Organisation Limited
Maternal Health, Family Planning
Institutional deliveries & sterilisations
lumpsum Yes
12 Incentive Scheme Chhattisgarh
NRHM/ RCH II
Public Group Entire state Maternal Health Institutional Deliveries Per unit Yes

Results based financing in Public Health Sector in India – Draft Report
24 | P a g e
S. no.
Name of the initiative
State Payer Recipient
Public/Pvt.Recipient
Geographical area covered
RBF Area RBF Services PaymentFormula
Benchmark
13 Mamta Friendly Hospital Initiative
Delhi NRHM Pvt. Facility Limited Maternal Health, Immunisation
institutional deliveries, ANC, PNC, immunisation
Per unit No
14 Chiranjeevi Yojana Gujarat
NRHM & State Govt.
Pvt. Facility Entire state Maternal Health Institutional deliveries Per unit No
15 Bal Sakha Yojana Gujarat
NRHM & State Govt.
Pvt. Individual, facility
Entire state Child Health, Immunisation
Outpatient and inpatient care, referral transport, initial vaccination
Per unit No
16 Performance based incentive to Public health facility
Gujarat State Govt.
Public Group, facility
Entire state Maternal Health Institutional deliveries Per unit Yes
17 Janani Suvidha yojana
Haryana NRHM/ RCH II
Pvt. Individual, Facility
Limited Maternal Health, Child Health
Institutional deliveries, ANC, newborn care, breastfeeding counselling
Per unit Yes
18 Jaccha Baccha Scheme
Haryana NRHM/ RCH II
Public Group Entire state Maternal Health Institutional deliveries Per unit Yes
19 Incentive schemes for specialists, MO
Kerala NRHM Public Individual Entire state Overall Health Services
overall performance Awards Yes
20 Call allowance incentive schemes for specialists
Kerala NRHM Public & Pvt.
Individual Entire state Overall Health Services
overall services Per unit No
21 Janani Express Yojana
Madhya Pradesh
NRHM/ RCH II
Pvt. Individual Limited Transportation Referral for institutional deliveries, sick children, and general emergencies
Per unit, % of end product
Yes
22
Performance based incentive for doctors
Madhya Pradesh
NRHM/ RCH II
Public Individual Entire state Maternal Health, Child Health, Family Planning
C-sections, MTP, sterilisations, care of sick newborns, care of ARI & Diarrhoea cases, care of other sick children
Per unit Yes
23 Incentive grant scheme to enhance
Maharashtra NRHM/ RCH II
Public Group Limited Maternal Health Institutional deliveries Per unit Yes
Results based financing in Public Health Sector in India – Draft Report
P a g e | 25
S. no.
Name of the initiative
State Payer Recipient
Public/Pvt.Recipient
Geographical area covered
RBF Area RBF Services PaymentFormula
Benchmark
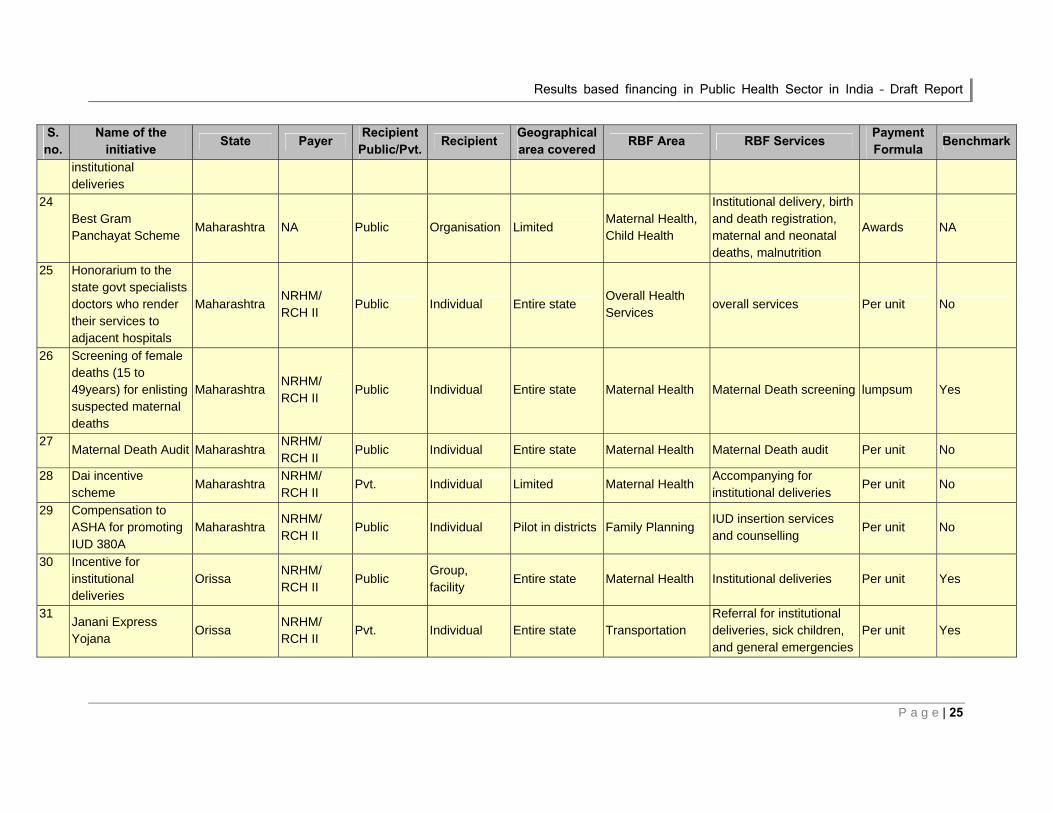
institutional deliveries
24 Best Gram Panchayat Scheme
Maharashtra NA Public Organisation Limited Maternal Health, Child Health
Institutional delivery, birth and death registration, maternal and neonatal deaths, malnutrition
Awards NA
25 Honorarium to the state govt specialists doctors who render their services to adjacent hospitals
Maharashtra NRHM/ RCH II
Public Individual Entire state Overall Health Services
overall services Per unit No
26 Screening of female deaths (15 to 49years) for enlisting suspected maternal deaths
Maharashtra NRHM/ RCH II
Public Individual Entire state Maternal Health Maternal Death screening lumpsum Yes
27 Maternal Death Audit Maharashtra
NRHM/ RCH II
Public Individual Entire state Maternal Health Maternal Death audit Per unit No
28 Dai incentive scheme
Maharashtra NRHM/ RCH II
Pvt. Individual Limited Maternal Health Accompanying for institutional deliveries
Per unit No
29 Compensation to ASHA for promoting IUD 380A
Maharashtra NRHM/ RCH II
Public Individual Pilot in districts Family Planning IUD insertion services and counselling
Per unit No
30 Incentive for institutional deliveries
Orissa NRHM/ RCH II
Public Group, facility
Entire state Maternal Health Institutional deliveries Per unit Yes
31 Janani Express Yojana
Orissa NRHM/ RCH II
Pvt. Individual Entire state Transportation Referral for institutional deliveries, sick children, and general emergencies
Per unit Yes

Results based financing in Public Health Sector in India – Draft Report
26 | P a g e
S. no.
Name of the initiative
State Payer Recipient
Public/Pvt.Recipient
Geographical area covered
RBF Area RBF Services PaymentFormula
Benchmark
32 Alternate health care delivery system
Punjab NRHM & State Govt.
Public Individual Entire state Overall Health Services
Primary Health Care lumpsum No
33 Performance benchmarks for contractual staff
Punjab NRHM/ RCH II
Public Individual Entire state Maternal Health, Child Health, Immunisation
Institutional deliveries, ANC, immunisation, breastfeeding
Termination Yes
34 Soubhagyavati Scheme
Uttar Pradesh
NRHM/ RCH II
Pvt. Facility Entire state Maternal Health Institutional deliveries Per unit No
35 Performance based incentive to honorary worker (Dais) at sub centres
Uttar Pradesh
NRHM/ RCH II
Pvt. Individual Entire state Maternal Health Accompanying for institutional deliveries & support in clinics
Per unit No
36 Payment to ASHA under CCSP Program
Uttar Pradesh
NRHM/ RCH II
Public Individual Limited Child Health Follow up and counselling for newborn care
Per unit Yes
37 Performance based incentives to ASHA
Uttarakhand NRHM/ RCH II
Public Individual Entire state Maternal Health & Child Health
ANC, birth and death registration, breastfeeding counselling
per unit No
38 Performance based incentives for institutional deliveries
Uttarakhand NRHM/ RCH II
Public Group, facility
Entire state Maternal Health Institutional deliveries per unit Yes
39 Mobile medical units Uttarakhand
NRHM/ RCH II
Pvt. Organisation Entire state Overall Health Services
Primary Health Care lumpsum Yes
40
Ayushmati scheme West Bengal NRHM/ RCH II
Pvt. Facility Entire state
Maternal Health, Child Health, Diagnostic Services
Institutional deliveries, diagnostics, newborn care
Per unit No
Results based financing in Public Health Sector in India – Draft Report
P a g e | 27
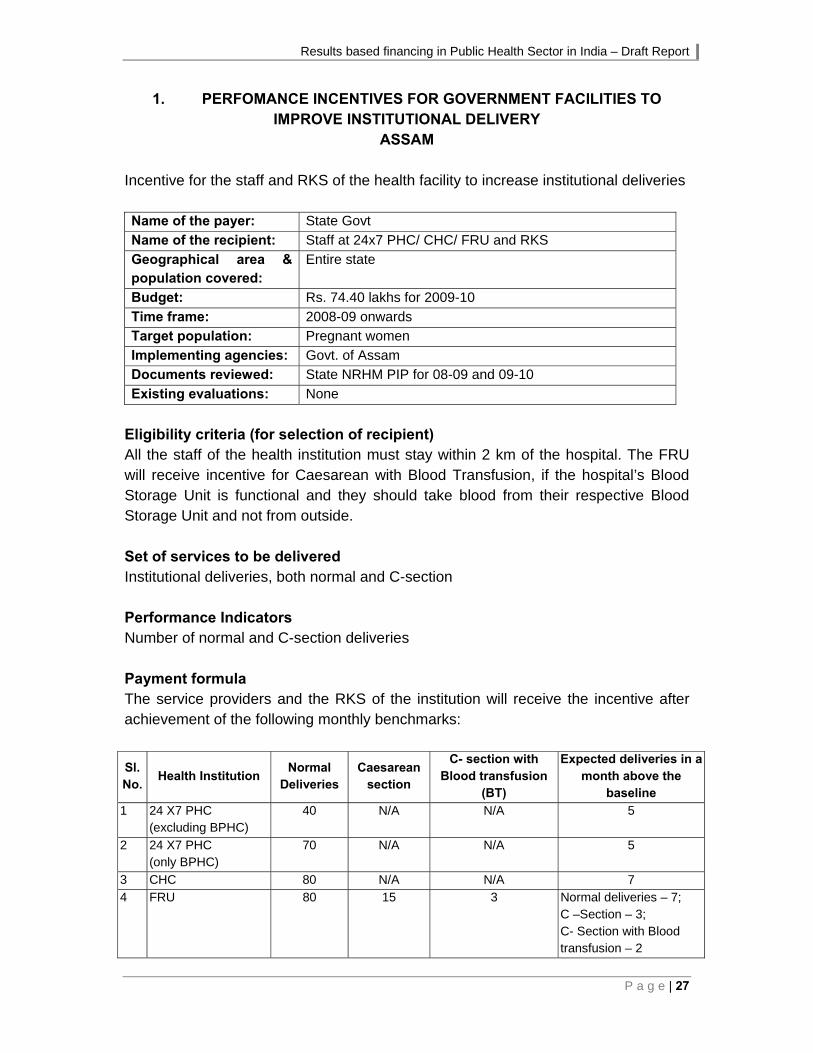
1. PERFOMANCE INCENTIVES FOR GOVERNMENT FACILITIES TO IMPROVE INSTITUTIONAL DELIVERY
ASSAM Incentive for the staff and RKS of the health facility to increase institutional deliveries Name of the payer: State Govt
Name of the recipient: Staff at 24x7 PHC/ CHC/ FRU and RKS
Geographical area & population covered:
Entire state
Budget: Rs. 74.40 lakhs for 2009-10
Time frame: 2008-09 onwards
Target population: Pregnant women
Implementing agencies: Govt. of Assam
Documents reviewed: State NRHM PIP for 08-09 and 09-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All the staff of the health institution must stay within 2 km of the hospital. The FRU will receive incentive for Caesarean with Blood Transfusion, if the hospital’s Blood Storage Unit is functional and they should take blood from their respective Blood Storage Unit and not from outside. Set of services to be delivered Institutional deliveries, both normal and C-section Performance Indicators Number of normal and C-section deliveries Payment formula The service providers and the RKS of the institution will receive the incentive after achievement of the following monthly benchmarks:
Sl. No.
Health Institution Normal
Deliveries Caesarean
section
C- section with Blood transfusion
(BT)
Expected deliveries in a month above the
baseline
1 24 X7 PHC (excluding BPHC)
40 N/A N/A 5
2 24 X7 PHC (only BPHC)
70 N/A N/A 5
3 CHC 80 N/A N/A 7
4 FRU 80 15 3 Normal deliveries – 7; C –Section – 3; C- Section with Blood transfusion – 2
Results based financing in Public Health Sector in India – Draft Report
28 | P a g e
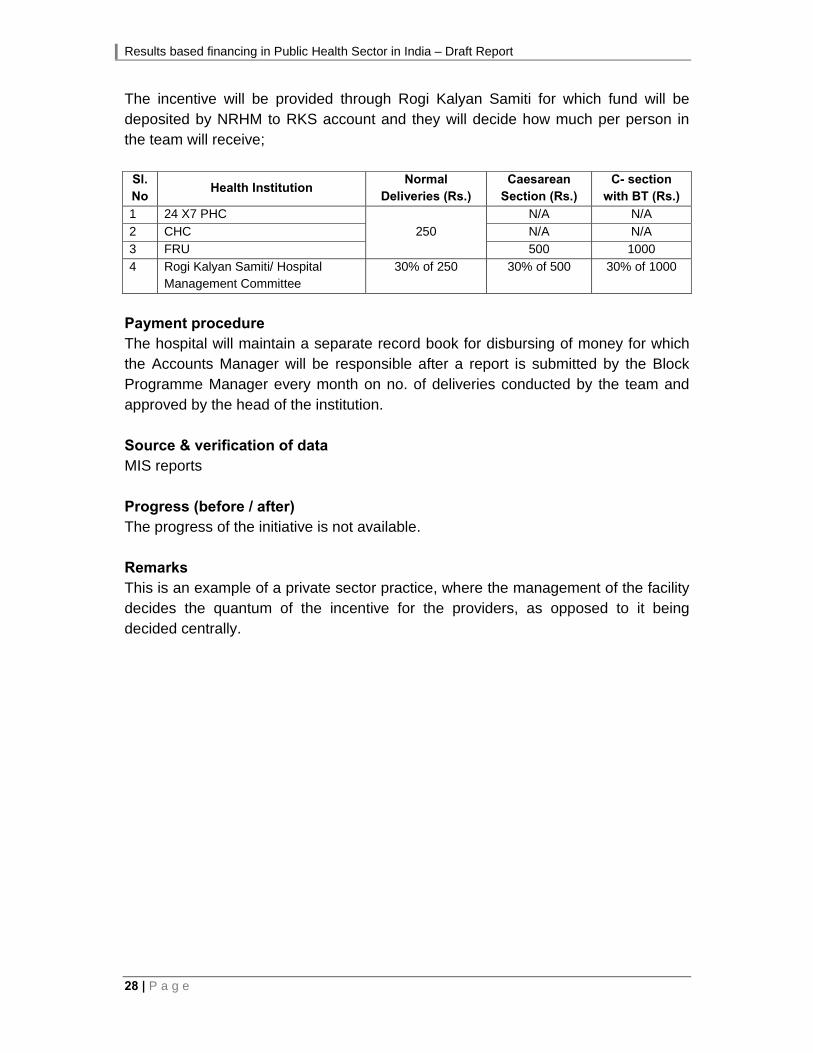
The incentive will be provided through Rogi Kalyan Samiti for which fund will be deposited by NRHM to RKS account and they will decide how much per person in the team will receive;
Sl. No
Health Institution Normal
Deliveries (Rs.) Caesarean
Section (Rs.) C- section
with BT (Rs.)
1 24 X7 PHC
250
N/A N/A
2 CHC N/A N/A
3 FRU 500 1000
4 Rogi Kalyan Samiti/ Hospital Management Committee
30% of 250 30% of 500 30% of 1000
Payment procedure The hospital will maintain a separate record book for disbursing of money for which the Accounts Manager will be responsible after a report is submitted by the Block Programme Manager every month on no. of deliveries conducted by the team and approved by the head of the institution. Source & verification of data MIS reports Progress (before / after) The progress of the initiative is not available. Remarks This is an example of a private sector practice, where the management of the facility decides the quantum of the incentive for the providers, as opposed to it being decided centrally.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 29
2. INCENTIVE TO ASHA FOR COMPLETION OF FULL IMMUNISATION ASSAM
Increase the coverage of full immunisation by reducing the drop out between BCG and measles. ASHAs after BCG will keep a track of the infants in her village and accompany the mother to the Sub Centre for vaccination.
Name of the payer: NRHM
Name of the recipient: ASHA
Geographical area & population covered:
Entire state
Budget: Rs. 1950.76 lakhs for 2009-10
Time frame: 2008-09 onwards
Target population: All the babies under one year of age
Implementing agencies: Govt. of Assam
Documents reviewed: PIP for 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All the ASHAs Set of services to be delivered Follow up and counselling Performance Indicators Number of children fully immunised Payment formula Rs. 250 is given to ASHA per infant fully immunised. Payment procedure ASHA has a booklet "ASHA Booklet" which would be used to keep a record of number of babies being fully immunised and then payment would be made by Block Programme Manager during the monthly ASHA meeting. Source & verification of data MIS data and ASHA Booklet Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
30 | P a g e
3. CHIRANJEEVI YOJANA ASSAM
A PPP initiative that intends to increase access to emergency obstetric care and institutional delivery for the un-served population
Name of the payer: NRHM/ RCH II Name of the recipient: Pvt. obstetricians conducting deliveries Geographical area & population covered: 6 districts Budget: Rs. 52.82 lakhs Time frame: 2009-10 onwards Target population: Pregnant women in BPL families Implementing agencies: Govt. of Assam Documents reviewed: State NRHM PIP for 2009-10 Existing evaluations: None Eligibility criteria (for selection of recipient) Not available
Set of services to be delivered Obstetric services (normal and C- section), pre-delivery consultation, free medicines to the lady after delivery, and transport reimbursement to the family by the hospital on the spot. Cash reimbursement will also be provided for the patient’s attendant wage loss
Performance Indicators The number of institutional deliveries conducted by the contracted private obstetrician.
Payment formula Rs. 2.20 lakhs/ 100 deliveries is provided lumpsum in advance. This compensation amount has been calculated taking into account the costs involved for various procedures / complications such as eclampsia and septicaemia treatment, episiotomy, forceps delivery, vaccum aspiration, blood transfusion. Additionally, pre-delivery visit, sonography, investigations, ASHA costs, and transportation are also covered.
Payment procedure Not available
Source & verification of data MIS reports
Progress (before / after) The initiative has only recently begun, and hence too early to comment.
Results based financing in Public Health Sector in India – Draft Report
P a g e | 31
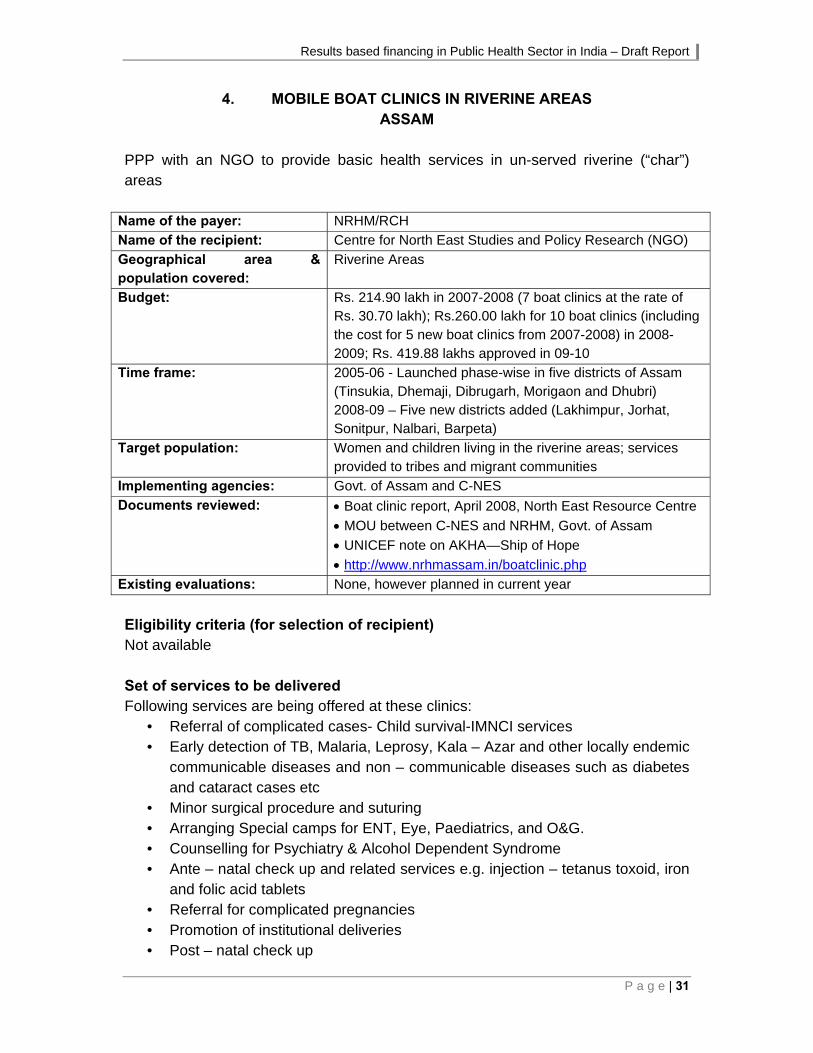
4. MOBILE BOAT CLINICS IN RIVERINE AREAS ASSAM
PPP with an NGO to provide basic health services in un-served riverine (“char”) areas
Name of the payer: NRHM/RCH
Name of the recipient: Centre for North East Studies and Policy Research (NGO)
Geographical area & population covered:
Riverine Areas
Budget: Rs. 214.90 lakh in 2007-2008 (7 boat clinics at the rate of Rs. 30.70 lakh); Rs.260.00 lakh for 10 boat clinics (including the cost for 5 new boat clinics from 2007-2008) in 2008-2009; Rs. 419.88 lakhs approved in 09-10
Time frame: 2005-06 - Launched phase-wise in five districts of Assam (Tinsukia, Dhemaji, Dibrugarh, Morigaon and Dhubri) 2008-09 – Five new districts added (Lakhimpur, Jorhat, Sonitpur, Nalbari, Barpeta)
Target population: Women and children living in the riverine areas; services provided to tribes and migrant communities
Implementing agencies: Govt. of Assam and C-NES
Documents reviewed: Boat clinic report, April 2008, North East Resource Centre
MOU between C-NES and NRHM, Govt. of Assam
UNICEF note on AKHA—Ship of Hope
http://www.nrhmassam.in/boatclinic.php
Existing evaluations: None, however planned in current year
Eligibility criteria (for selection of recipient) Not available Set of services to be delivered Following services are being offered at these clinics:
• Referral of complicated cases- Child survival-IMNCI services • Early detection of TB, Malaria, Leprosy, Kala – Azar and other locally endemic
communicable diseases and non – communicable diseases such as diabetes and cataract cases etc
• Minor surgical procedure and suturing • Arranging Special camps for ENT, Eye, Paediatrics, and O&G. • Counselling for Psychiatry & Alcohol Dependent Syndrome • Ante – natal check up and related services e.g. injection – tetanus toxoid, iron
and folic acid tablets • Referral for complicated pregnancies • Promotion of institutional deliveries • Post – natal check up

Results based financing in Public Health Sector in India – Draft Report
32 | P a g e
• Immunization clinics • Treatment of common childhood illness such as diarrhoea, ARI/ Pneumonia
etc • Treatment of RTI/ STI • Counselling for spacing and permanent method • Distribution of Condoms, Oral Contraceptives, Emergency Contraceptives • IUD Insertion by ANMS, Copper ‘T’ insertion. • Basic Laboratory Services - Haemoglobin, Urine for sugar and albumin and
Malaria – RDK, etc. • Emergency services & care in times of disaster/epidemic/public health
emergency/ accidents etc • IEC material on health including personal hygiene, proper nutrition etc. as well
as screens and projection for health documentary screening and awareness building
Performance Indicators As per the contract document, the performance benchmarks are to be set up between the NGO and district / state authorities, and based on approved workplan. However, not clear, whether payment is made against achievement of benchmarks / or whether expenses are reimbursed at actuals subject to the upper limit in the State PIP. In case of the latter, would not qualify as a RBF. Payment formula Except the construction and insurance of the boats, which is the responsibility of CNES (the NGO), all other expenses including staff, medicine costs etc are born by Govt. of Assam. Payment mechanism is as follows:
• The expenditure for the activities performed for rendering services shall be borne as per State Action Plan.
• Funds shall be released in advance as mentioned in the Action Plan • Release of advance shall be made within two weeks after submission of fund
requirement request from the NGO. • Vaccines, contraceptives and other RCH and Curative drugs and equipment
shall be supplied as per requirement of the boat clinics from the office of the District Health Society and NRHM state and respective district offices. Supply of medicines, vaccines etc. for boat clinics to be made available throughout the year on priority.
Payment procedure Not available
Results based financing in Public Health Sector in India – Draft Report
P a g e | 33
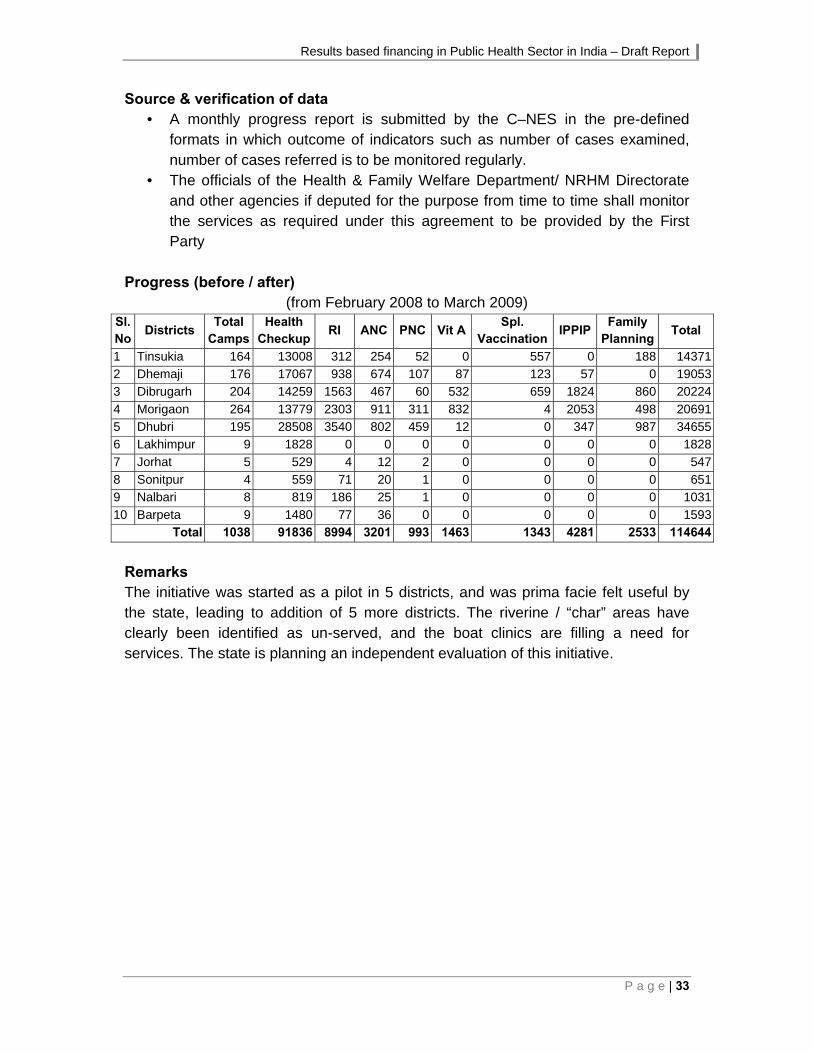
Source & verification of data • A monthly progress report is submitted by the C–NES in the pre-defined
formats in which outcome of indicators such as number of cases examined, number of cases referred is to be monitored regularly.
• The officials of the Health & Family Welfare Department/ NRHM Directorate and other agencies if deputed for the purpose from time to time shall monitor the services as required under this agreement to be provided by the First Party
Progress (before / after)
(from February 2008 to March 2009) Sl. No
Districts Total
Camps Health
Checkup RI ANC PNC Vit A
Spl.Vaccination
IPPIP Family
PlanningTotal
1 Tinsukia 164 13008 312 254 52 0 557 0 188 14371
2 Dhemaji 176 17067 938 674 107 87 123 57 0 19053
3 Dibrugarh 204 14259 1563 467 60 532 659 1824 860 20224
4 Morigaon 264 13779 2303 911 311 832 4 2053 498 20691
5 Dhubri 195 28508 3540 802 459 12 0 347 987 34655
6 Lakhimpur 9 1828 0 0 0 0 0 0 0 1828
7 Jorhat 5 529 4 12 2 0 0 0 0 547
8 Sonitpur 4 559 71 20 1 0 0 0 0 651
9 Nalbari 8 819 186 25 1 0 0 0 0 1031
10 Barpeta 9 1480 77 36 0 0 0 0 0 1593Total 1038 91836 8994 3201 993 1463 1343 4281 2533 114644
Remarks The initiative was started as a pilot in 5 districts, and was prima facie felt useful by the state, leading to addition of 5 more districts. The riverine / “char” areas have clearly been identified as un-served, and the boat clinics are filling a need for services. The state is planning an independent evaluation of this initiative.
Results based financing in Public Health Sector in India – Draft Report
34 | P a g e
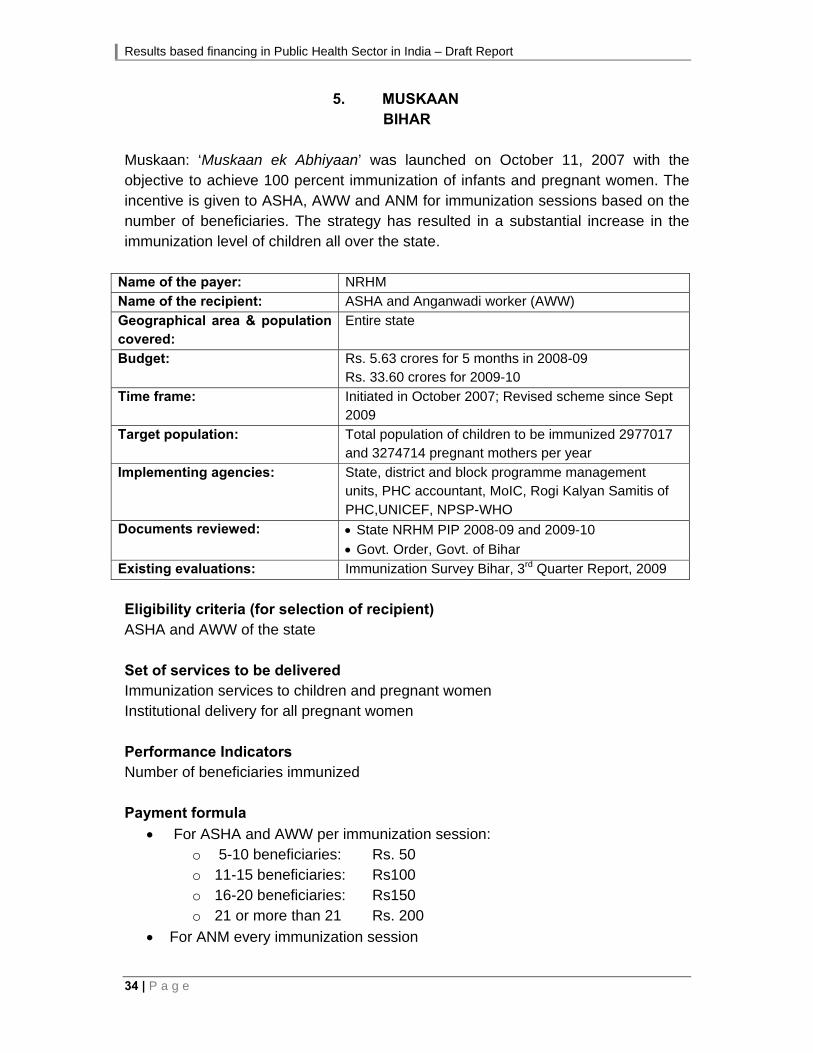
5. MUSKAAN BIHAR
Muskaan: ‘Muskaan ek Abhiyaan’ was launched on October 11, 2007 with the objective to achieve 100 percent immunization of infants and pregnant women. The incentive is given to ASHA, AWW and ANM for immunization sessions based on the number of beneficiaries. The strategy has resulted in a substantial increase in the immunization level of children all over the state.
Name of the payer: NRHM
Name of the recipient: ASHA and Anganwadi worker (AWW)
Geographical area & population covered:
Entire state
Budget: Rs. 5.63 crores for 5 months in 2008-09 Rs. 33.60 crores for 2009-10
Time frame: Initiated in October 2007; Revised scheme since Sept 2009
Target population: Total population of children to be immunized 2977017 and 3274714 pregnant mothers per year
Implementing agencies: State, district and block programme management units, PHC accountant, MoIC, Rogi Kalyan Samitis of PHC,UNICEF, NPSP-WHO
Documents reviewed: State NRHM PIP 2008-09 and 2009-10
Govt. Order, Govt. of Bihar
Existing evaluations: Immunization Survey Bihar, 3rd Quarter Report, 2009
Eligibility criteria (for selection of recipient) ASHA and AWW of the state Set of services to be delivered Immunization services to children and pregnant women Institutional delivery for all pregnant women Performance Indicators Number of beneficiaries immunized Payment formula
For ASHA and AWW per immunization session: o 5-10 beneficiaries: Rs. 50 o 11-15 beneficiaries: Rs100 o 16-20 beneficiaries: Rs150 o 21 or more than 21 Rs. 200
For ANM every immunization session

Results based financing in Public Health Sector in India – Draft Report
P a g e | 35
o 1-15 beneficiaries: Rs 50 o 16 and above: Rs.100
Payment procedure A monthly claim in a specified format is prepared by the ANM and cross-checked by the PHC accountant, under the overall supervision of the MO i/c of the PHC. Source & verification of data: Micro plans, Dues-list register, Muskaan tracking register, MCH register, Tally sheets, list of beneficiaries. The Block Programme Manager will verify the claims of at least 4 ANMs each month. Monthly meetings (on last Tuesday of the month) are to be held by the RKS and the ICDS representative to assess the progress of the initiative. Progress (before / after) Latest coverage evaluation survey findings show an increase in immunisation coverage.

Results based financing in Public Health Sector in India – Draft Report
36 | P a g e
6. ULTRA-MODERN DIAGNOSTIC CENTERS BIHAR
In order to provide Modern diagnostic services to the patients coming to medical colleges and regional diagnostic centres, the state government has entered into an agreement with a private party on revenue sharing basis.
Name of the payer: NRHM
Name of the recipient: Private Parties awarded the contract
Geographical area & population covered:
Regional Diagnostic Centres in Ara, Gaya, Bhagalpur, Munger, Muzaffarpur, Motihari, Purnea, Saharsa and chapra. Government Medical College Hospitals – PMCH, NMCH, SKMCH, DMCH, ANMMCH, JLMNCH
Budget: Rs. 5.40 crores for reimbursement to for services to BPL patients
Time frame: 2008-09 onwards
Target population: Patients needing advanced diagnostic tests
Implementing agencies: Dept. Health & Family welfare, Govt. of Bihar, Regional Deputy Directors
Documents reviewed: State PIP, 2009-10
Website: http://www.statehealthsocietybihar.org/new-proposed-initiatives.html, Accessed on 13th Nov 2009
MOU document
Existing evaluations: None
Eligibility criteria (for selection of recipient) Provider selected through Tender, detailed criteria not available. Set of services to be delivered Pathology- Bio-Chemistry, Radiology – Digital X-ray, USG, CT Scan, MRI, ECG, Mammography (as per list provided by GoB) Performance Indicators Not applicable, since revenue sharing model Payment formula Revenue sharing (5% of gross-revenue) and reimbursement for services provided to BPL patients, nominal rent of Rs.500 per month per unit to be paid to govt. Fines levied for delay in operationalization of labs Payment procedure Reimbursement for services to BPL patients provided through RKS.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 37
Source & verification of data: Reports from the Data Centre and the districts Progress (before / after) Contract awarded to 2 agencies to operate, maintain and report 24-hours centres

Results based financing in Public Health Sector in India – Draft Report
38 | P a g e
7. GENERIC DRUG STORE BIHAR
Generic drug shops at all districts hospitals and medical colleges to provide cheaper (at 50% of MRP) drugs to the patients through private parties on revenue sharing basis.
Name of the payer: NRHM
Name of the recipient: Private Parties awarded the contract
Geographical area & population covered:
In all the medical colleges and district hospitals
Budget: NA
Time frame: 2008-09 onwards
Target population: Entire population
Implementing agencies: Dept. Health & Family welfare, Govt. of Bihar
Documents reviewed: Draft agreement
State PIP, GoB
Website: http://www.statehealthsocietybihar.org/new-proposed-initiatives.html
Existing evaluations: None
Eligibility criteria (for selection of recipient) GMP companies having turnover of Rs. 25 crores or above Set of services to be delivered 188 generic drugs at 50% of the MRP printed, services to be available 24x7 Performance Indicators Not applicable, since revenue sharing model Payment formula Revenue sharing as quoted and decided through tender Payment procedure Not available Source & verification of data: Not available Progress (before / after) Three Generic Drug Shops are being set up in each of the six Medical College Hospitals; two in each of the 38 District Hospitals and two in other Hospitals. Fund has been sent to 23 DHSs for construction of Drug Stores. Out of these five drug stores has been constructed.
Results based financing in Public Health Sector in India – Draft Report
P a g e | 39
8. RADIOLOGY SERVICES BIHAR
The State government is providing x-ray and ultrasound facilities to the patients coming to PHCs, referral hospitals, sub-divisional hospitals and district hospitals through a private party. Nominal fee was charged from the patients. The initiative was revamped in 2009-10 and all the tests have been made free. The private party is now being paid by the government to provide X-ray/ Sonography facilities at reasonable rates to general public coming to government facilities.
Name of the payer: NRHM
Name of the recipient: Private Parties awarded the contract
Geographical area & population covered:
Whole state
Budget: None Time frame: 2006-07 onwards
Target population: Entire population
Implementing agencies: GoB, Rogi Kalyan Samitis, Private party (IGEMS)
Documents reviewed: State PIP, GoB
Website: http://www.statehealthsocietybihar.org/new-proposed-initiatives.html Accessed on 13th Nov 2009
Existing evaluations: None
Eligibility criteria (for selection of recipient) Provider selected through Tender, detailed criteria not available. Set of services to be delivered X-ray/ Sonography facilities in all PHCs, Referral Hospitals, Sub-Divisional Hospitals and District Hospitals of Bihar. Specifically-Ultrasound facilities in 151 units where X-rays are there, 100 new facilities where X-ray services are to be provided Performance Indicators Not available Payment formula Rates charged from users referred from government hospitals are Rs. 50 for short plate, and Rs. 75 for large plate. Charges are free for BPL patients, which are reimbursed by the RKS. If private patients avail the services, the provider may charge market rates. Payment procedure Not available (for RKS reimbursement)

Results based financing in Public Health Sector in India – Draft Report
40 | P a g e
Source & verification of data Not available Progress (before / after) 151 X-ray units set up. The Centers have provided X-ray services to 3.53 lakhs patients in the last two years. Ultrasound Facilities in the District Hospitals and Sub-divisional Hospital are also being provided.
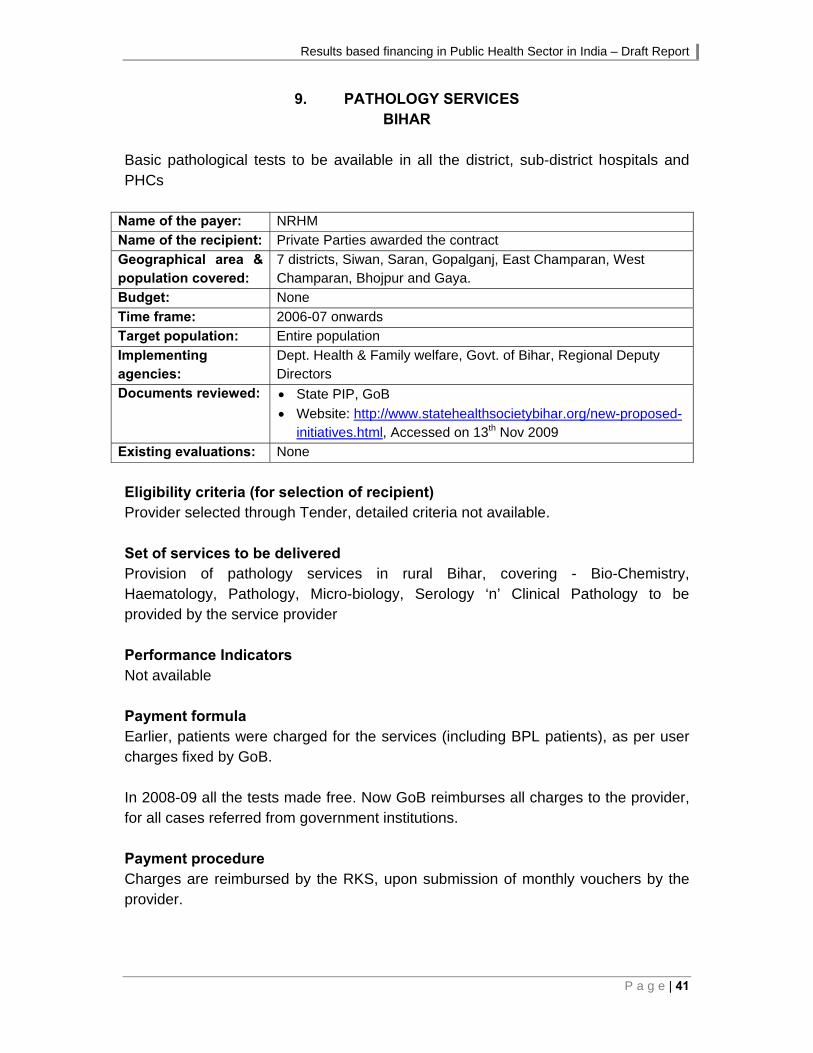
Results based financing in Public Health Sector in India – Draft Report
P a g e | 41
9. PATHOLOGY SERVICES BIHAR
Basic pathological tests to be available in all the district, sub-district hospitals and PHCs
Name of the payer: NRHM
Name of the recipient: Private Parties awarded the contract
Geographical area & population covered:
7 districts, Siwan, Saran, Gopalganj, East Champaran, West Champaran, Bhojpur and Gaya.
Budget: None
Time frame: 2006-07 onwards
Target population: Entire population
Implementing agencies:
Dept. Health & Family welfare, Govt. of Bihar, Regional Deputy Directors
Documents reviewed: State PIP, GoB
Website: http://www.statehealthsocietybihar.org/new-proposed-initiatives.html, Accessed on 13th Nov 2009
Existing evaluations: None
Eligibility criteria (for selection of recipient) Provider selected through Tender, detailed criteria not available. Set of services to be delivered Provision of pathology services in rural Bihar, covering - Bio-Chemistry, Haematology, Pathology, Micro-biology, Serology ‘n’ Clinical Pathology to be provided by the service provider Performance Indicators Not available Payment formula Earlier, patients were charged for the services (including BPL patients), as per user charges fixed by GoB. In 2008-09 all the tests made free. Now GoB reimburses all charges to the provider, for all cases referred from government institutions. Payment procedure Charges are reimbursed by the RKS, upon submission of monthly vouchers by the provider.

Results based financing in Public Health Sector in India – Draft Report
42 | P a g e
Source & verification of data State Data Centre reports Progress (before / after) Two agencies have been selected through tender process. The agencies have set up labs at the District hospitals and sample collection centres at the health facilities below district levels. In the State 407 Centres are operational. More than 4 lakhs tests have been conducted in the last two years.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 43
10. ADDITIONAL PHC OUTSOURCING BIHAR
Running of Additional PHCs in Bihar outsourced to private organisations to provide services.
Name of the payer: NRHM
Name of the recipient: Private Parties awarded the contract
Geographical area & population covered:
Catchment area of 44 Additional PHCs
Budget: Not available
Time frame: 2008-09 onwards
Target population: Catchment area of the Additional PHCs
Implementing agencies: Dept. Health & Family welfare, Govt. of Bihar
Documents reviewed: State PIP, GoB
Website: http://www.statehealthsocietybihar.org/new-proposed-initiatives.html, Accessed on 13th Nov 2009
Existing evaluations: None
Eligibility criteria (for selection of recipient) Provider selected through Tender, detailed criteria not available. Set of services to be delivered Primary Health Care services, including RCH services, OPD, and Diagnostics (Pathology- Bio-Chemistry, Radiology – Digital X-ray, USG, CT Scan, MRI, ECG, Mammography) Performance Indicators Number of deliveries per month and the number of FP operations per month Payment formula The following amount shall be payable to the agency each month
a. Salaries 57,500 b. Drugs 15,000 c. Emergency referral transport 2,000 d. Miscellaneous (Stationary etc.) 1,000
75,500 The Agency shall be paid Rs.8000 (Surgeon & Anaesthetist to be hired @ Rs. 1,000/- per day) for 4 Family Planning days one each week to be paid only where weekly Family Planning days shall be observed and the agency conducts 40 FP operations in a month.
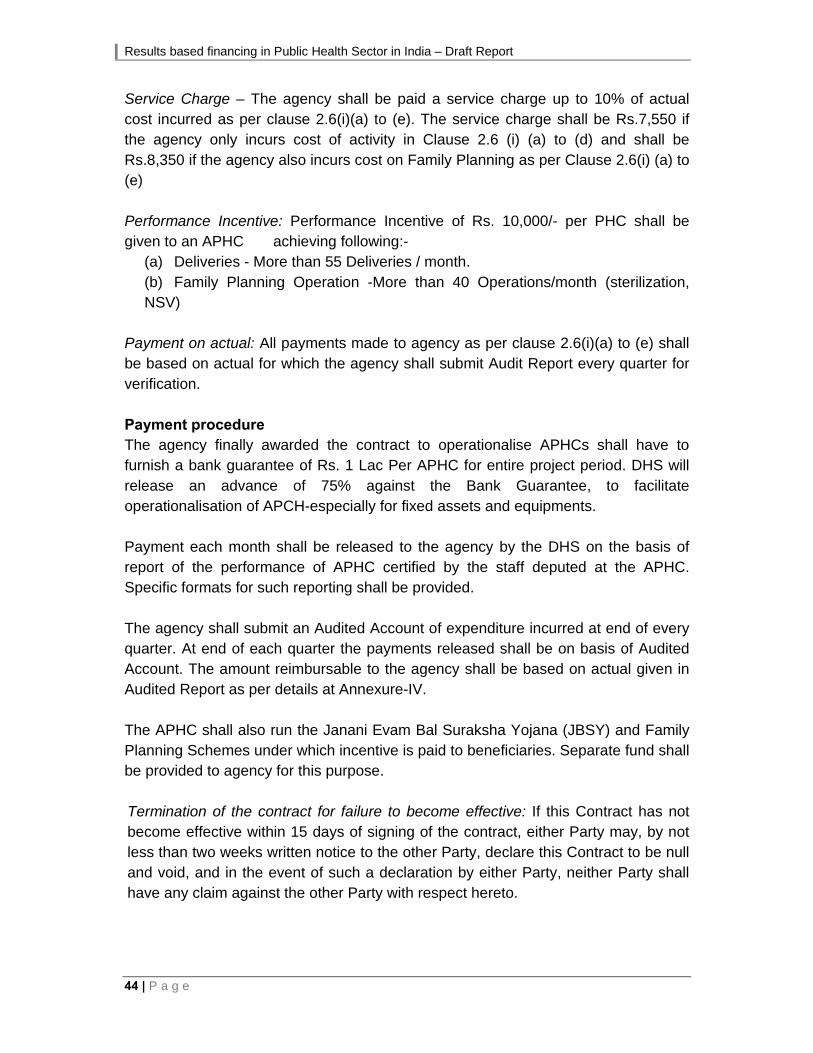
Results based financing in Public Health Sector in India – Draft Report
44 | P a g e
Service Charge – The agency shall be paid a service charge up to 10% of actual cost incurred as per clause 2.6(i)(a) to (e). The service charge shall be Rs.7,550 if the agency only incurs cost of activity in Clause 2.6 (i) (a) to (d) and shall be Rs.8,350 if the agency also incurs cost on Family Planning as per Clause 2.6(i) (a) to (e) Performance Incentive: Performance Incentive of Rs. 10,000/- per PHC shall be given to an APHC achieving following:-
(a) Deliveries - More than 55 Deliveries / month. (b) Family Planning Operation -More than 40 Operations/month (sterilization, NSV)
Payment on actual: All payments made to agency as per clause 2.6(i)(a) to (e) shall be based on actual for which the agency shall submit Audit Report every quarter for verification. Payment procedure The agency finally awarded the contract to operationalise APHCs shall have to furnish a bank guarantee of Rs. 1 Lac Per APHC for entire project period. DHS will release an advance of 75% against the Bank Guarantee, to facilitate operationalisation of APCH-especially for fixed assets and equipments. Payment each month shall be released to the agency by the DHS on the basis of report of the performance of APHC certified by the staff deputed at the APHC. Specific formats for such reporting shall be provided. The agency shall submit an Audited Account of expenditure incurred at end of every quarter. At end of each quarter the payments released shall be on basis of Audited Account. The amount reimbursable to the agency shall be based on actual given in Audited Report as per details at Annexure-IV. The APHC shall also run the Janani Evam Bal Suraksha Yojana (JBSY) and Family Planning Schemes under which incentive is paid to beneficiaries. Separate fund shall be provided to agency for this purpose. Termination of the contract for failure to become effective: If this Contract has not become effective within 15 days of signing of the contract, either Party may, by not less than two weeks written notice to the other Party, declare this Contract to be null and void, and in the event of such a declaration by either Party, neither Party shall have any claim against the other Party with respect hereto.
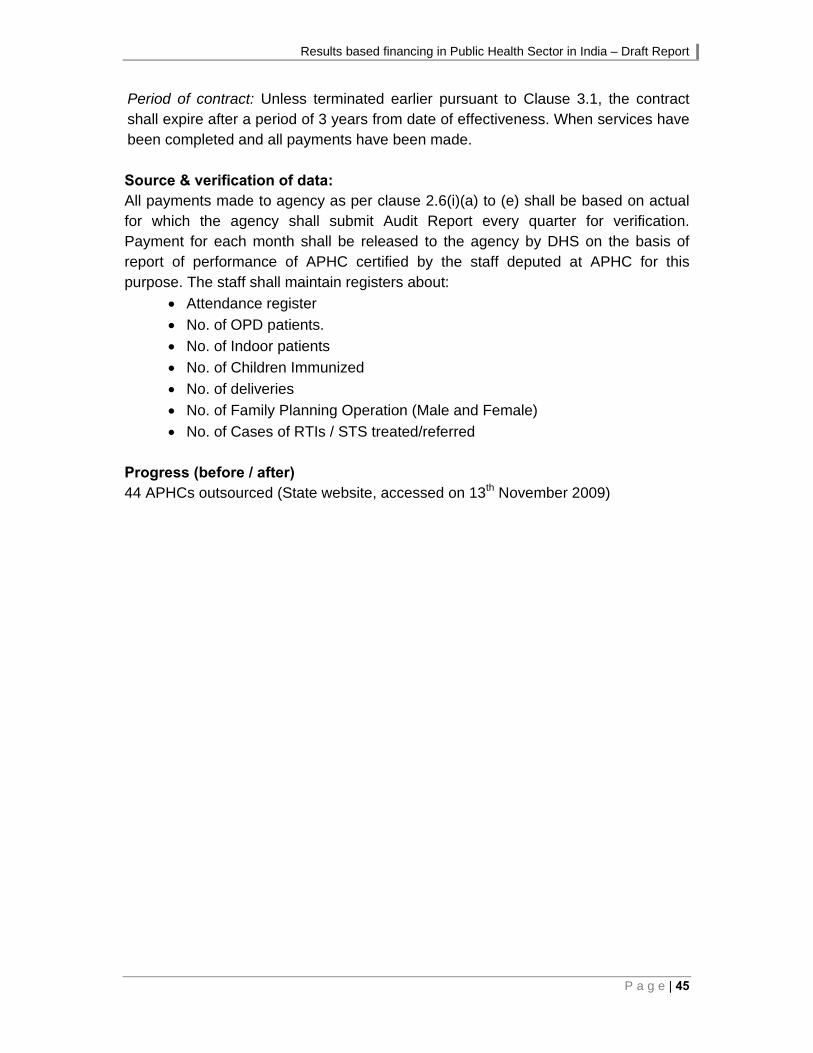
Results based financing in Public Health Sector in India – Draft Report
P a g e | 45
Period of contract: Unless terminated earlier pursuant to Clause 3.1, the contract shall expire after a period of 3 years from date of effectiveness. When services have been completed and all payments have been made. Source & verification of data: All payments made to agency as per clause 2.6(i)(a) to (e) shall be based on actual for which the agency shall submit Audit Report every quarter for verification. Payment for each month shall be released to the agency by DHS on the basis of report of performance of APHC certified by the staff deputed at APHC for this purpose. The staff shall maintain registers about:
Attendance register
No. of OPD patients.
No. of Indoor patients
No. of Children Immunized
No. of deliveries
No. of Family Planning Operation (Male and Female)
No. of Cases of RTIs / STS treated/referred Progress (before / after) 44 APHCs outsourced (State website, accessed on 13th November 2009)

Results based financing in Public Health Sector in India – Draft Report
46 | P a g e
11. URBAN HEALTH CENTRE BIHAR
PPP for basic RCH services to slum dwellers through outsourcing of urban health centres
Name of the payer: NRHM Name of the recipient: Private Parties awarded the contract Geographical area & population covered:
Slums of major cities in Bihar
Budget: Time frame: 2008-09 onwards Target population: Slum population of major cities Implementing agencies: Dept. of Health & Family welfare, Govt. of Bihar Documents reviewed: State PIP 2009-10
Website: http://www.statehealthsocietybihar.org/new-proposed-initiatives.html Accessed on 13th Nov 2009
Existing evaluations: None Eligibility criteria (for selection of recipient) Provider selected through Tender, detailed criteria not available. Set of services to be delivered a. Each UHC shall be assigned an area in such a way that all the slum dwellers of
that area are covered. The size/magnitude of slum population would be around 20,000-30,000, including listed and unlisted slums and other vulnerable community habitations. Irrespective of the area assigned to the agency for specific services the UHC shall provide free OPD facilities to all patients coming to the Clinic.
b. Free OPD, Immunization, Antenatal care (early registration, TT immunization, IFA supplements, nutrition counseling, Physical examination of ante-natal mothers including weighing, blood pressure, abdominal examination for position of the baby, identification of danger signs, referral services), Child Health services, including breastfeeding, immunization, management of diarrhoea and Treatment of minor ailments.
c. The agency has to provide Delivery services and Family Planning services. d. Other services can be included by the agency in the package on the basis of the
need and morbidity profile of the service area. Performance Indicators Institutional deliveries and sterilisations
Results based financing in Public Health Sector in India – Draft Report
P a g e | 47
Payment formula Financial Pattern & Payment mode for UHC- The following amount shall be payable to the agency each month- (a) Salaries for manpower - Rs. 38,000 (b) Service Charge - Rs. 7,000
Rs. 45,000 Payment for Additional Optional Services a) The Agency shall be paid Rs.8000 (Surgeon & Anaesthetist to be hired @ Rs. 1,000/- per day) for 4 Family Planning days, one in each week, to be paid only where weekly Family Planning days shall be observed. b) The UHC shall also run the Janani Evam Bal Suraksha Yojana (JBSY) and Family Planning Schemes under which incentive is paid to beneficiaries. Separate fund shall be provided to agency for this purpose. Performance Incentive: Performance Incentive of Rs. 10,000/- per UHC for achieving:- (a) Deliveries- More than 55 Deliveries per month. (b) Family Planning Operation More than 40 Operations per month. Payment procedure Payments to UHCs shall be made by the respective District Health Society on the basis of report of performance of UHC certified by the staff deputed at UHC for this purpose. Monthly reimbursement will be done for all payments subject to submission of bills by 5th of each month by the Agency to the DHS Member Secretary/Civil Surgeon. DHS will release an advance of 75% against the Bank Guarantee, to facilitate establishment of UHC-especially for fixed assets and equipments. All payments made to agency for regular services and additional services shall be based on actuals for which the agency shall submit Audit Report every quarter for verification. The agency shall submit an Audited Account of expenditure incurred at end of every quarter. At end of each quarter the payments released shall be on the basis of Audited Account. The amount reimbursable to the agency shall be based on actual given in Audited Report. Source & verification of data The UHCs shall send monthly reports to District Health Society in the prescribed format. The DHS/SHSB shall also conduct supervisory visits. A Government Staff shall be deputed for regular monitoring. Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
48 | P a g e
12. INCENTIVE SCHEME CHHATTISGARH
Incentive to the government health providers, to increase the number of deliveries at government health institutions Name of the payer: NRHM/RCH
Name of the recipient: Service providers at sub-centres, PHCs, and CHCs, block administration
Geographical area & population covered:
Entire state
Budget: Rs. 173.66 lakhs
Time frame: 2009-10 onwards
Target population: Pregnant women
Implementing agencies: Gov. of Chhattisgarh
Documents reviewed: PIP for 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All the govt SCs/PHCs/CHCs/BMO/CMHO are entitled to get the incentive Set of services to be delivered Institutional deliveries Performance Indicators Number of deliveries Payment formula The payment is made to the various staff on a per case basis after achievement of the target for the year, as follows: Sn. Type of facility Benchmark (above which
incentive kicks in) Recipient Amount
(per case)
1 Sub-centre (Rural) 40 deliveries/ yr ANM Rs. 50
2 Sub-centre (tribal) 25 deliveries/ yr ANM Rs. 50
3 PHC (rural) 250 deliveries/ yr
MO Rs. 25
SN Rs. 25
Class IV staff Rs. 50
4 PHC (tribal) 180 deliveries/ yr
MO Rs. 25
SN Rs. 25
Class IV staff Rs. 50
5 CHC (rural) 350 deliveries/ yr
MO Rs. 30
SN Rs. 30
Class IV staff Rs. 40

Results based financing in Public Health Sector in India – Draft Report
P a g e | 49
Sn. Type of facility Benchmark (above which incentive kicks in)
Recipient Amount (per case)
6 CHC (tribal) 250 deliveries/ yr
MO Rs. 30
SN Rs. 30
Class IV staff Rs. 40
6 Block Administration (Rural block)
2000 deliveries/ yr
BMO Rs. 5000
BPM Rs. 5000
Other staff Rs. 5000
6 Block Administration (Tribal block)
1500 deliveries/ yr
BMO Rs. 5000
BPM Rs. 5000
Other staff Rs. 5000
Payment procedure Not available Source & verification of data MIS reports Progress (before / after) Not available Remarks This is the only incentive scheme seen for government staff, where the block administration also has benchmarks.
Results based financing in Public Health Sector in India – Draft Report
50 | P a g e
13. MAMTA FRIENDLY HOSPITAL INITIATIVE DELHI
PPP to increase access to safe delivery services for BPL women.
Name of the payer: NRHM / RCH
Name of the recipient: Private hospitals/ Nursing homes under the initiative
Geographical area & population covered:
6 out of the 9 districts in Delhi
Budget: 2007-08: Rs. 3 crores; 2008-09: Rs. 3 crores; 2009-10: Rs. 1.25 crores (Rs. 40 lakh is proposed for IEC/BCC publicity)
Time frame: 2007-08 onwards
Target population: Pregnant women, belonging to the BPL/ SC/ ST category, resident of Delhi, above 19 years of age, and having only one living child.
Implementing agencies: Private hospitals and nursing homes identified in the schemes, ASHA/Link workers, Health & Family welfare, Govt. Of Delhi.
Documents reviewed: http://health.delhigovt.nic.in/nrhm/mamta.PDF
http://nrhm-mis.nic.in/UI/MEActivities/goa_web/PDFs/02-05-08_pdf/Mamta%20(Delhi).pdf
Existing evaluations: None
Eligibility criteria (for selection of recipient)
The Nursing home should be registered under the Delhi Nursing Home Registration Act.
Appropriate staff including gynaecologist and obstetrician, paediatrician, anaesthetist, radiologist, resident medical officer, staff nurse. O.T. Technician, Lab technician.
Availability of diagnostic facilities as under: 1. Haemoglobin estimation. 2. Urine - routine and microscopic examination. 3. VDRL Test. 4. Hepatitis ‘B’ antigen testing. 5. Blood Sugar random. 6. Blood grouping and typing of both husband and wife. 7. Ultrasonography
Availability of equipment, O.T, labour room, nursery - As per conditions laid down under Delhi Govt. Nursing Home Registration Act.
The hospital/ centre/ nursing home should preferably be situated within 5 km of the residence of the patient.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 51
Set of services to be delivered The private hospital/ private nursing home should provide ANC, provision of TT injection and iron folic acid tablets, provision of institutional delivery facilities, administration of birth doses of vaccines to newborns & post natal checkups. The state govt. provides the following facilities for the beneficiaries under the MAMTA initiative: the transportation of sick new born to referral hospital by CATS Ambulance free of cost; Provision of drugs by DHS to pregnant women with medical illness attending MAMTA Initiative Hospital; and Linkages of MAMTA Initiative Hospital to nearby ICTC for HIV testing. Performance indicators
At least three antenatal checkups with all necessary investigations including ultrasound of pregnant woman registered under the initiative.
Provision of Injection TT and Iron Folic Acid Tablets to all pregnant women as per RCH Schedule, provision of institutional delivery facilities, including emergency obstetric care to all registered pregnant women and essential new born care to the new born including administration of birth doses of vaccines to newborns.
One postnatal check-up within first week of delivery but not later than 14 days Payment formula
The hospitals that become partners under this initiative shall be paid @ Rs. 4000/- for normal deliveries and Rs. 5,500 for caesarean deliveries for a maximum of 15% of all deliveries.
The hospital will be eligible for payment only after an institutional delivery is carried out with essential new born care and immunization of the baby with birth doses before discharge and one Post Partum check-up.
In cases where due to some unavoidable reason the beneficiary fails to deliver in the hospital, the hospital shall be eligible for only half package (Rs 2000/-) after the CDMO has verified that a complete antenatal check-up and investigations were done.
If an unregistered pregnant woman presents in an emergency or in labour and is provided with an institutional delivery with essential newborn care, immunization and post natal check-up, the hospital will be eligible for Rs.3000/- for a normal delivery and Rs. 4,500 for a caesarean delivery.
Deliveries for which blood transfusion took place, Rs. 500 will be provided. (For both normal as well as caesarean delivery)
ASHA /Link Worker will be eligible for Rs 100 /- per delivery as motivation incentive.
Payment procedure
Periodic payment to Private Nursing Home in stages on completion of certain activities like ANC visits, investigation, delivery etc.

Results based financing in Public Health Sector in India – Draft Report
52 | P a g e
Source & verification of data
MFH shall submit monthly report on a predesigned format
Designated MAMTA Nodal Officers in the districts to randomly check at least 7% of the beneficiaries through records at the private hospital as well as the at the residence for actual verification
2% random check at state Level
Evaluation at the end of the year by comparing the institutional birth data of a specific ward from the office of the Registrar for births/ Deaths
Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
P a g e | 53
14. CHIRANJEEVI YOJANA GUJARAT
PPP to increase access to safe delivery services for BPL women.
Name of the payer: NRHM & Gujarat State Govt.
Name of the recipient: Pvt. obstetrician conducting deliveries.
Geographical area & population covered:
Entire Gujarat State 11.75 crores (23.5 lakh families, avg. of 5 per family)
Budget: Rs. 11 crores in the 1st year in 5 districts, Rs.50.6 crores for the entire state/year
Time frame: Dec 2005 to Jan 2007: Pilot in 5 districts; scaled up to all districts of the state since Jan 2007
Target population: Pregnant women in BPL families
Implementing agencies:
Commissionerate of health, medical services, Medical education& Research, Health & Family welfare, Govt. Of Gujarat
Documents reviewed: Rapid assessment of Chiranjeevi Yojana, UNFPA, 2006
Maternal Health Financing – Issues and Options, A Study of Chiranjeevi Yojana, IIM-A, Working Paper Series, March 2007
Govt. Of Gujarat – Dept. Of Health website, Nov. 2009
Existing evaluations: Independent Rapid qualitative assessment of Chiranjeevi Yojana by UNFPA – 2006, after six months of operation.
Eligibility criteria (for selection of recipient)
Post graduate qualification in Ob/Gyn
Hospital with min. of 15 beds
labour room and operating room
access to blood in emergency situation
able to arrange for anaesthetists and trained staff to carry out emergency surgery
Facility should be preferably accredited for sterilization procedures by the government.
Norm would be to select 2-3 private Ob/Gyn’s per sub-district. Set of services to be delivered Obstetric services (normal and C- section) Performance Indicators The number of institutional deliveries conducted by the contracted private obstetrician. Payment formula The payment formula is Rs. 1.78 lakhs / 100 deliveries, out of which Rs.50 is paid to the beneficiary for transportation costs. Rs. 0.31 lakhs is given at the time of signing.
Results based financing in Public Health Sector in India – Draft Report
54 | P a g e
This compensation amount has been calculated taking into account the costs involved for various procedures which occur during pregnancies such as Septicaemia, blood transfusion, NICU support, sonography etc. Payment procedure Every month the contracted providers present their filled in vouchers and claim their reimbursement. The entire document for the reimbursement is submitted to the DPMU RCH, which initiates the process of payment. Payment is made after the approval of the Chief District Health Officer and the District Development Officer. Source & verification of data Initiative specific reporting formats are in place for collecting facility-wise data, which is then compiled at the block, district and state level. A nodal person has been designated at the state level for independent monitoring of a sample of beneficiaries. At the district level, the District Programme Management Unit is tasked with monitoring of the initiative. Progress (before / after)
852 obstetricians enrolled in the initiative (nearly 42.5% of total no. of obstetricians in the state), (2007)
Total 3.85 lakhs deliveries conducted till Sep 2009, including 0.23 lakh C-sections
A household survey of the initiative in one of the pilot districts suggests that most of the Chiranjeevi users have annual income levels less than Rs. 12,000 p.a. indicating the initiative was able to target the poor families.
Remarks
The initiative doesn’t take care of the qualitative aspect of the services provided, a concern highlighted in the Common Review Mission visit in November 2009.
The range of services to be delivered by the provider is very narrow. They don’t include ANC’s, neo-natal care, 48 hour stay after delivery, post – Partum sterilisation etc.
Results based financing in Public Health Sector in India – Draft Report
P a g e | 55
15. BAL SAKHA YOJANA GUJARAT
PPP initiative to increase the access to paediatric care to newborn of BPL women Name of the payer: State Govt/NRHM
Name of the recipient: Pvt. Paediatrician
Geographical area & population covered:
Entire state
Budget: Rs. 10.68 crores approved for 2009-10 under NRHM
Time frame: Initiative was launched on 22/01/09
Target population: Newborn children of BPL and SC/ST women
Implementing agencies:
Commissionerate of health, medical services, Medical education & Research, Health & Family welfare, Govt. Of Gujarat
Documents reviewed: PIP for 2009-10
Govt of Gujarat - Dept of Health website, Nov 2009
Existing evaluations: None
Eligibility criteria (for selection of recipient)
• Chiranjeevi Yojana (CY) doctors/institutions can have a partnership with private paediatricians and a MoU can be signed between the 3 parties (Govt., CY doctor, and Paediatrician)
• Govt. would do the tie-up with individual paediatricians for BPL deliveries (other than Chiranjeevi Yojana) in 18 IMNCI districts
Set of services to be delivered Out-patient care, referral transport, in-patient care, initial vaccination etc. Performance Indicators The number of new born babies attended by private paediatricians. Payment formula For two different packages payment formula is as follows:
• tie up with CY doctors/ institutions - Rs. 1.67 lakhs/ 100 new born • individual paediatricians - Rs. 1.75 lakhs/ 100 new born
Payment procedure An advance of Rs. 25,000 would be given in the beginning; after that vouchers have to be submitted every month to DPMU-DHS to get more funds Source & verification of data MIS reports and reporting formats developed for the initiative

Results based financing in Public Health Sector in India – Draft Report
56 | P a g e
Progress (before / after) Number of doctors enrolled – 284; Number of newborns under the initiative – 31151; Number of newborns admitted in NICUs – 7351; Number of newborn deaths – 413 (till Sep 2009)

Results based financing in Public Health Sector in India – Draft Report
P a g e | 57
16. PERFORMANCE BASED INCENTIVE TO PUBLIC HEALTH FACILITIES GUJARAT
To increase the number of institutional deliveries in govt hospitals, and in turn improve the utilisation of services offered at govt facilities
Name of the payer: State Govt
Name of the recipient: Health providers and RKS of PHC/CHC/FRU
Geographical area & population covered:
Entire state
Budget: NA
Time frame: 2008
Target population: Pregnant women
Implementing agencies: Govt. Of Gujarat
Documents reviewed: PIP for 2008-09 and 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All the govt PHCs/CHCs/FRUs where skilled birth can be conducted Set of services to be delivered Institutional deliveries Performance Indicators Number of deliveries conducted by each facility per month Payment formula The following amount will be paid per case, after achievement of minimum monthly benchmarks of 10 deliveries at PHCs and 25 at CHCs/FRUs
Recipient Normal Delivery Assisted Delivery C-section (with BT)
MO Rs. 100 Rs. 200 Rs. 275
MO-Anaesthesia - - Rs. 275
SN Rs. 50 Rs. 100 Rs. 150
CHV Rs. 25 Rs. 50 Rs. 75
RKS Rs. 75 Rs. 150 Rs. 225 Total Rs. 250 Rs. 500 Rs. 1000
Payment procedure Not available Source & verification of data MIS reports Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
58 | P a g e
17. JANANI SUVIDHA YOJANA HARYANA
To provide better health facilities to urban slum population especially the slum dweller pregnant women: • Provide quality MCH services to the neediest and vulnerable population at their
doorsteps • Provide quality and low cost diagnostic services to the pregnant urban slum
dweller women • Provision of good quality contraceptives, vaccinations and others supplies to the
urban vulnerable population • Optimally utilize the existing resources in the state and to increase institutional
deliveries.
Name of the payer: NRHM
Name of the recipient: Empanelled private health providers, and “Sakhi” – a grassroots mobiliser working for the FNGO
Geographical area & population covered:
08 districts, i.e. Panchkula, Yamunanagar, Kurukshetra, Rewari, Narnaul, Gurgaon, Sonepat and Bhiwani
Budget: 2009-10: Rs. 50 Lakhs, 08-09: Rs. 2 crores, 07-08: Rs. 2 crores
Time frame: 2006-07 onwards
Target population: Pregnant women in urban slums
Implementing agencies:
Govt. of Haryana
Documents reviewed: Haryana PIP 2009-10
Haryana safe motherhood report
Existing evaluations: None
Eligibility criteria (for selection of recipient) Not available Set of services to be delivered Sakhi: A resident woman from the urban slum will be selected per 1000 population. She will act as a link between Clients & Private Health Providers. She will be selected by FNGOs/SHGs. She will be responsible for facilitating the clients for availing:
• Antenatal registration • 3 Antenatal Checkups, 2 TT injections, IFA tablets • Institutional delivery • 2 Post natal check ups • Essential Newborn care

Results based financing in Public Health Sector in India – Draft Report
P a g e | 59
• Post delivery IUD insertion/sterilization (if the client wishes so) • Any pregnancy related complication within 42 days of delivery • Immunization of child
The private provider will provide normal delivery services. All high risk cases for C-section delivery to be referred to government hospitals. For emergency and high-risk cases, ambulance Services will be provided to the Sakhi on telephonic request and in case of non-availability of ambulance, she will have sufficient imprest money in advance for referral transportation. Performance Indicators Number of Antenatal registrations, ANC, IFA tablets, TT injections; facilitating mothers for institutional deliveries; essential newborn care, counselling on exclusive breast feeding; birth and death registration. Payment formula The private provider gets Rs. 1500 per normal delivery. The rate for referral transport will be @ Rs. 5 per km or a maximum of Rs. 200, whichever is less. The Sakhis will get honorarium as follows:
• Antenatal registration, 3 Antenatal Checkups,100 IFA tablets and 2 TT injections: 3 case load/month, Rs. 20/ case
• Facilitate mothers for institutional delivery: 3 case load/month, Rs. 75/ case • Provide essential newborn care, counselling on exclusive breast feeding: 3
case load/month, Rs.30/ case • Ensure Birth and Death registration: 5 case load/ month, Rs. 10/case • Appreciation for completion of all activities: Rs. 75
Payment procedure Sakhi will give undertaking to District NGO and will get performance based honorarium after completion of a set of activities. The Sakhis will be provided imprest money of Rs.200 as the revolving fund for referral transport of pregnant mothers for delivery purposes, referral of high risk pregnancies and sick newborns. Source & verification of data Reports from Field NGOs and vouchers submitted by providers on a monthly basis Progress (before / after)
Year Total Deliveries
2006-07 769
2007-08 8371
2008-09 (till Dec. 2008) 9910 (Source: State PIP 2009-10)

Results based financing in Public Health Sector in India – Draft Report
60 | P a g e
Keeping in view the satisfactory implementation of the initiative in 8 districts, the state has now proposed to implement the initiative in all the remaining districts with minor alterations in the initiative.
It has been decided that the incentive to the Sakhi needs to be increased, as she is the only backbone of the initiative, who is from the community itself and mobilizing the community for availing the RCH Services.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 61
18. JACCHA BACCHA SCHEME HARYANA
To provide incentives to the Multi Purpose Health Worker (F), Staff Nurses & Medical Officers who are skilled birth attendants thereby improving the quality, availability and the attitude of these service providers and give a boost to the institutional delivery programme in the health sector.
Name of the payer: NRHM
Name of the recipient: Doctors, ANMs, LTs, Class IV staff
Geographical area & population covered:
Entire State
Budget: 2009-10: Rs. 1.05 crores
Time frame: 2008-09 onwards
Target population: All mothers undergoing deliveries at govt. institutions
Implementing agencies: Department of Health & Family Welfare, Govt. of Haryana
Documents reviewed: State PIP 09-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All Sub-centres, PHCs, CHCs where normal and assisted/ C-section deliveries are conducted Set of services to be delivered Institutional deliveries, both normal and C- section Performance Indicators Number of Deliveries conducted by the service providers Payment formula According to this initiative every skilled provider (SBA) conducting an institutional delivery at Sub Centre PHC or CHC along with other required parameters receives a cash incentive based on the following:
1. The incentive to the ANMs at the Sub Centres is applicable after conducting minimum 3 deliveries pre ANM per month.
2. The incentive to the Staff Nurses at PHCs & CHCs is applicable after they have conducted a minimum of 5 deliveries per Staff Nurse per month.
3. The incentive for the Doctors at PHCs & CHCs is applicable after they have conducted a minimum of 5 deliveries per Doctor per month. The mode of the delivery can be either vaginal or operative.

Results based financing in Public Health Sector in India – Draft Report
62 | P a g e
The incentive to the skilled provider conducting the delivery is Rs.400/- in case of male new born and Rs.600/- in case of female new born. In case of obstructed labour SBA ensures referrals and accompanies mother to the nearest FRU and is entitled to benefit of Rs.100/- in such case. In addition, Staff Nurse/ANM assisting the delivery is paid Rs.100/-, LTs paid Rs.50/- and Class-IV paid Rs.50/- per delivery. Payment procedure Not available Source & verification of data MIS reports Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
P a g e | 63
19. INCENTIVE SCHEMES FOR SPECIALISTS, MEDICAL OFFICERS KERALA
Award scheme for doctors, program managers and health facilities
Name of the payer: NRHM Flexible Pool Mission
Name of the recipient: Specialists, Medical officers etc.
Geographical area & population covered:
Entire State
Budget: 2009-10: Rs.1 lakh
Time frame: 2009-10 onwards
Target population: Entire state
Implementing agencies:
Govt of Kerala
Documents reviewed: Kerala PIP 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All district medical officers, district program managers, CHC’s 24 X 7 PHC’s, PHC’s. Set of services to be delivered Each category is required to carry out the specific set of activities it is required to according to the NRHM guidelines. Performance Indicators Not available Payment formula The various categories for incentive awards for 2009-10 are given below: 1. Best District Medical Officer 2. Best District Program Manager 3. Best CHC 4. Best 24 X 7 PHC 5. Best PHC Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
64 | P a g e
20. CALL ALLOWANCE INCENTIVE SCHEMES FOR SPECIALISTS KERALA
Apart from the rural/ difficult Area allowance, casualty allowance, stay allowance etc., doctors receive a call allowance where payment is made on a per call basis, for services provided beyond normal work hours.
Name of the payer: NRHM Flexible Pool Mission
Name of the recipient: Specialists at health facilities
Geographical area & population covered:
Entire state
Budget: NA
Time frame: 2008-09 onwards
Target population: Entire state
Implementing agencies:
MO/Superintendent of the institution, CEO of the DH&FW Society, DPM, staff nurse in-charge of ward and casualty.
Documents reviewed: Kerala PIP 2009-10, 08-09
Existing evaluations: None
Eligibility criteria (for selection of recipient)
1. Eligible for all Govt. Doctors between 8 pm to 8 am. Where there is only a single Specialist in a particular category, he / she may be given allowance from 3 pm to 8 pm also in exceptional cases where there is dire necessity.
2. If there is no Govt. Doctor in a particular category, other Doctors (NRHM / CRS / Private) may be called in for Emergency cases. For this the Medical Officer / Superintendent shall prepare a panel of experts in each Specialty for the Institution and send the same to the Chief Executive Officer of the DH&FW Society for approval. Doctors in the approved panel only shall be eligible for Call allowance. While preparing the panel, first preference shall be for Govt. Doctors.
3. At the beginning of each month the Superintendent / MO In charge shall publish a Call duty roster for each Specialty. Doctors shall attend Call as per the duty roster.
4. A call shall be sent only in those cases in which the Duty MO needs expert help. A list of emergency surgical cases depending on the situation in the District shall be approved by the CEO and communicated to the Institutions. Allowance for surgeries shall be limited to these cases.
5. Anaesthetists / Gynaecologists can be called for emergency delivery cases as per RCH guidelines apart from the above.
Set of services to be delivered The set of services to be delivered by the gynaecologists are normal deliveries, assisted deliveries, C- section, hysterectomy, emergency hysterectomy. Apart from

Results based financing in Public Health Sector in India – Draft Report
P a g e | 65
this surgery, ophthalmology, ENT, Ortho and anaesthetic services are also provided by the specialists. The details of payment and eligibility have been listed below. Performance Indicators The performance indicators for the incentive are the number of calls a doctor receives and when on call, the number of deliveries conducted, the number of surgeries carried out, and the number or procedures requiring general or block anaesthesia. Payment formula Rates for Call allowance is as noted below For each call Rs.100 For Gynaecologist Rs.200 – Normal delivery Rs.500 – Assisted delivery
Rs.1000 – Caesarean section / Emergency Hysterectomy/Hysterectomy
For Surgeon / Ophthalmic / ENT / Ortho Rs.200 – minor surgeries Rs.500 – Major surgeries
For Anaesthetist Rs.1000 per case for general & spinal anaesthesia and long procedures Rs.500 for minor procedures under block anaesthesia
The ceiling for call allowance, including the allowance for Surgery / delivery is Rs. 10,000/- per doctor per month. It shall be the duty of the Medical Officer / Superintendent to ensure that no Doctor refuses to attend a Call / Surgery because the monthly ceiling has been reached. Any Doctor in the panel who refuses to attend any call, either due to the ceiling being achieved or due to any other reason, shall be removed from the panel immediately. He / She shall not be paid any allowance under NRHM once he is removed from the panel. Maximum number of calls eligible for payment shall be 5 per Doctor per day. However the Doctor on call is liable to attend any call in excess of this number, but payment shall be limited to a maximum of Rs. 500/- per Doctor per day. For Surgeries the maximum limit shall be Rs. 1500/- per Doctor per day. Both are subject to the monthly ceiling limits as per clauses above. In case there is only a single doctor in any particular specialty in a hospital & no govt. / Private Doctor is available from outside to attend the call, the daily & monthly ceilings shall not be applicable.

Results based financing in Public Health Sector in India – Draft Report
66 | P a g e
Payment procedure Only the Doctor who is on call as per the duty roster and those doctors in the approved panel shall be eligible for Call allowance on a particular day. At the end of each month, the MO/ Superintendent shall send a certified copy of the duty roster along with the claim for Call allowance at the end of each month in a prescribed format to the DPM who shall scrutinize the list in consultation with the CEO and release necessary funds to the Medical Officer / Superintendent for payment to the Doctors. Time for deciding eligibility shall be the time at which call is sent from the Institution & not the time at which the call is received / attended. In case of Surgery / Delivery, eligibility shall be decided based on the time at which Surgery was done / delivery was conducted. In this case, the doctor will not be eligible for separate call allowance. A list of emergency surgical cases depending on the situation in the District shall be approved by the CEO and communicated to the Institutions. Allowance for surgeries shall be limited to these cases. Source & verification of data The call shall be written in the book & signed by the Staff Nurse in charge of the Ward / Casualty & countersigned by the Duty M.O. Before sending a Call, the duty MO should have examined the case and a call shall be sent only in those cases in which the Duty MO needs expert help. Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
P a g e | 67
21. JANANI EXPRESS YOJANA MADHYA PRADESH
Provision of 24 hours transport availability at field level in order to bring the pregnant women to government health institutions
Name of the payer: NRHM, Government of Madhya Pradesh
Name of the recipient: Vehicle owner
Geographical area & population covered:
First Phase: Piloted in August 2006 in two blocks each in 10 districts; Phase 2: June 2007 onwards – covers 204 of the total 313 blocks in the entire state
Budget: Funds made available from Janani Suraksha Yojana and Rogi Kalyan Samiti
Time frame: August 2006-ongoing
Target population: All pregnant women – for antenatal check up in 2nd trimester of pregnancy onwards, MTP, institutional delivery, or for any obstetric emergency (antenatal or post natal)
All persons eligible under Deen Dayal Antyodaya Upchar Yojana
Referral for all sick newborns and children
For any medical emergency
Implementing agencies:
Government of Madhya Pradesh, UNFPA
Documents reviewed: MP PIP 2009-10 and 2008-09
Initiative guidelines and MOU/ agreement
Existing evaluations: Evaluation commissioned by UNFPA, June 2007.
Eligibility criteria (for selection of recipient) The transport vehicle will be hired locally on contractual basis for a period of one year on the basis of criteria specified below. A contract / MoU will be signed with a private agency/ NGO. The agency will ensure the 24 hour driver services and vehicle under the programme. The important features of the vehicle are as below.
1. Vehicle less than 24 months old. 2. Long seat in the back of the vehicle, for ease of transport of pregnant women. 3. Folding ladder for climbing to vehicle. 4. Water and light facilities in the vehicle. 5. One folding stretcher 6. Curtains in the windows of the vehicle. 7. Disposable Dai Kits in the vehicle for emergency deliveries 8. Cotton, Bandage, Dettol, Soap and First Aid Kit. (to be provided & replenished
to concerned RKS) The technical aspects of the vehicle are:
1. The vehicle is not older than two years on the day of the signing of the contract.

Results based financing in Public Health Sector in India – Draft Report
68 | P a g e
2. Comprehensive Insurance valid policy is available with the vehicle. 3. The vehicle has all legal papers like registration, fitness certificate, Road Tax
payment paper etc. 4. Valid driving license with the drivers 5. Security deposit of Rs.10,000/- in favour of the RKS of respective health
institution. 6. The agency interested to establish partnership with RKS under the
programme will quote the financial offer keeping in account the road tax, insurance premium, VAT, parking fee, toll tax etc for which State Government or Rogi Kalyan Samiti(RKS) will not pay.
7. The servicing and maintenance of vehicle from time to time is the responsibility of the private agency.
Set of services to be delivered Transport will be made available in the concerned area of Government hospital, CHC, PHC, or to some other appropriate place as decided by the HQ. The vehicle will be attached to the Health Institutions at the disposal of MO I/C. The vehicle owner will be asked to provide the vehicle with drivers on 24X7 basis. The contact telephone number of the driver and the hospital will be displayed on the body of the vehicle for public knowledge. On the front and back of the vehicle “Janani Express” will be painted in English in Hindi, including information about the initiative (mechanism for calling the vehicle, etc.), and other schemes such as JSY. The driver will also be provided a short course on first aid, and kit will be made available in the vehicle (to be replenished by the attached hospital). The provider has to ensure proper maintenance of the vehicle, repair any problem within 48 hours, and provide a replacement vehicle in the interim. The ANM, ASHA, AWW of the area is to provide the EDD to the driver, so that the woman may be brought to the facility one day prior, to help avoid any emergencies. Performance Indicators The number of kilometres covered as well as revenue generated above the monthly rent. The specific details have been given below. Payment formula
1. The monthly rental is to be fixed with the provider. The contract will ensure a minimum of 40 km per day or 1200 km per month.
2. A rent of Rs. 150 upto 25 km and Rs. 250 above 25 km, per case will be charged. For beneficiaries under JSY, funds will be provided from the scheme. For other cases, no charges are to be levied from BPL patients (APL patients pay as per above rates). The daily collection is to be deposited at the facility.
3. For distances above 1200 km in a month, additional charges will be paid to the provider at a pre-fixed per kilometre charge.
Results based financing in Public Health Sector in India – Draft Report
P a g e | 69
4. If in a month, the provider generates revenue greater than the monthly rental, the provider will get an additional incentive as follows:
a. Upto 125% - no incentive b. 125-150% - incentive of 25% of monthly rental c. 150-200% - incentive of 35% of monthly rental
5. Additionally, the RKS will pay the driver Rs. 200 per month towards reimbursement for mobile communication.
Payment procedure RKS is responsible for overall administration and supervision of the scheme vehicles. The additional revenue is deposited in the RKS fund. The monthly report in a prescribed format (along with the log book) is submitted by the provider to the RKS by the subsequent month. Payment is to be made to the provider within 7 days. The remuneration for the additional mileage and the performance incentive is provided on a quarterly basis, while the calculation for the same is done on a monthly basis. If the provider is unable to deliver the services as specified, then he/ she is liable for a fine of Rs. 500 per day of services not provided. Contract termination: To be done upon a notice of 30 days. However, if the driver is found to be under the influence of alcohol at any time, or if the provider is not able to deliver the services for 10 days in a month, the services may be summarily terminated and the deposit of Rs. 10,000 forfeited. Source & verification of data The driver will maintain a log book of vehicle movement. The log book / movement will be verified and checked by the Medical Officer In-charge or any other authorized officer of the District hospital / CHC/PHC. A monthly performance report in the prescribed format is submitted to CDMO/DPMU which will be compiled and consolidated in a prescribed reporting format at the District level by DPMU for submission of the same to NRHM, Madhya Pradesh. Progress (before / after) The evaluation report states that the 54, 202 women have used the scheme. A significant proportion of Scheduled Tribes (36.4%), Scheduled Castes (18.6%), and Backward Castes (32.9%) availed of the scheme. Roughly half of all clients using the scheme were for delivery. Over 50% of the clients belonged to the BPL category. The initiative has enabled multiparas to access institutional delivery for the first time. 61% of women, delivering their second baby accessed institutional delivery for the first time and 72% of women, delivering their third baby accessed institutional delivery for the first time. Overall the initiative seems to enjoy high political and popular support.
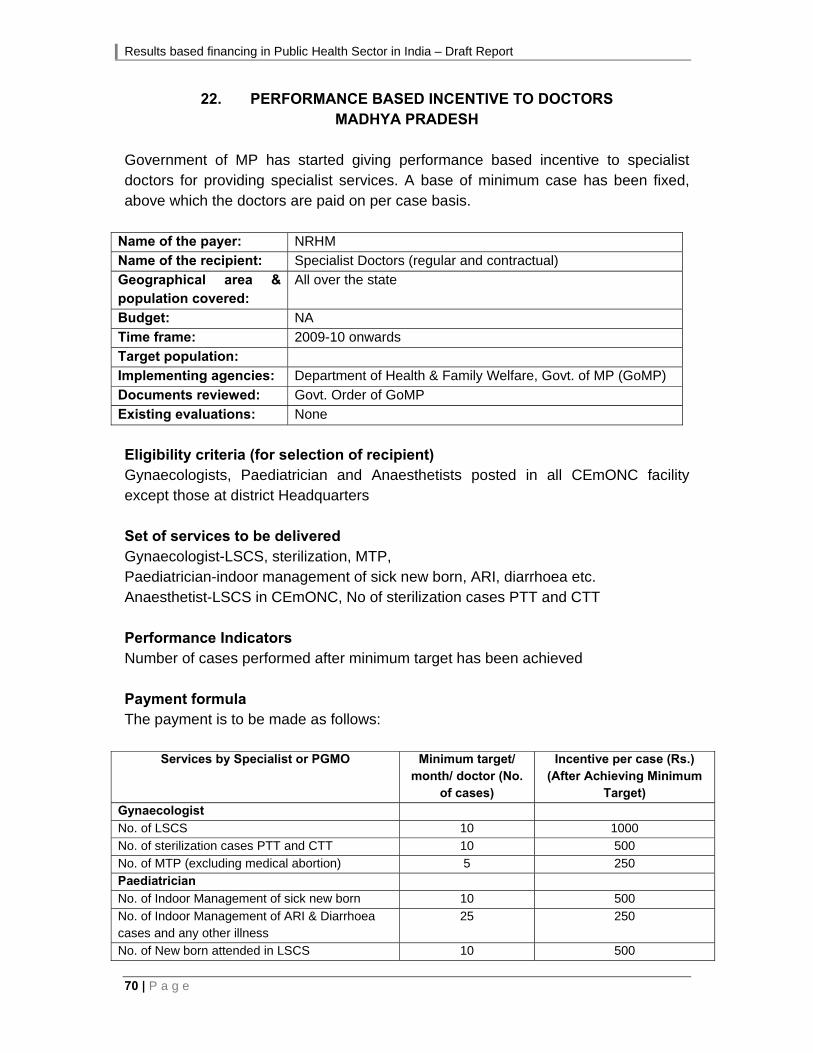
Results based financing in Public Health Sector in India – Draft Report
70 | P a g e
22. PERFORMANCE BASED INCENTIVE TO DOCTORS MADHYA PRADESH
Government of MP has started giving performance based incentive to specialist doctors for providing specialist services. A base of minimum case has been fixed, above which the doctors are paid on per case basis.
Name of the payer: NRHM
Name of the recipient: Specialist Doctors (regular and contractual)
Geographical area & population covered:
All over the state
Budget: NA
Time frame: 2009-10 onwards
Target population:
Implementing agencies: Department of Health & Family Welfare, Govt. of MP (GoMP)
Documents reviewed: Govt. Order of GoMP
Existing evaluations: None
Eligibility criteria (for selection of recipient) Gynaecologists, Paediatrician and Anaesthetists posted in all CEmONC facility except those at district Headquarters Set of services to be delivered Gynaecologist-LSCS, sterilization, MTP, Paediatrician-indoor management of sick new born, ARI, diarrhoea etc. Anaesthetist-LSCS in CEmONC, No of sterilization cases PTT and CTT Performance Indicators Number of cases performed after minimum target has been achieved Payment formula The payment is to be made as follows:
Services by Specialist or PGMO Minimum target/ month/ doctor (No.
of cases)
Incentive per case (Rs.)(After Achieving Minimum
Target)
Gynaecologist
No. of LSCS 10 1000
No. of sterilization cases PTT and CTT 10 500
No. of MTP (excluding medical abortion) 5 250 Paediatrician
No. of Indoor Management of sick new born 10 500
No. of Indoor Management of ARI & Diarrhoea cases and any other illness
25 250
No. of New born attended in LSCS 10 500

Results based financing in Public Health Sector in India – Draft Report
P a g e | 71
Services by Specialist or PGMO Minimum target/ month/ doctor (No.
of cases)
Incentive per case (Rs.)(After Achieving Minimum
Target)
Anaesthetist
No. of LSCS in the CEmONC 10 1000
No. of Sterilization cases PTT and CTT 10 500
A maximum of Rs. 8,000 per month per specialist will be given. Gynaecologists and Anaesthetists will have to achieve at least 50% target for C-sections before they can get incentives for other services. Payment procedure Not available Source & verification of data: State MIS Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
72 | P a g e
23. INCENTIVE GRANT SCHEME TO ENHANCE THE INSTITUTIONAL DELIVERIES
MAHARASHTRA
Incentive scheme for health providers at government institutions in select talukas
Name of the payer: NRHM Name of the recipient: Staff at the PHC Geographical area & population covered:
99 talukas in 21 districts
Budget: Rs. 38.09 lakhs Time frame: 2008-09 onwards Target population: Women undergoing institutional delivery at the PHCs in
these talukas Implementing agencies: Govt. of Maharashtra Documents reviewed: Information provided by the state Existing evaluations: None Eligibility criteria (for selection of recipient) This initiative is applicable to the PHCs in 99 talukas of 21 districts, where home deliveries are greater than 50%. Set of services to be delivered Institutional deliveries to be performed at the PHCs. After delivery that mother should stay at PHC for at least for 48 hours Performance Indicators The incentive to be given after surpassing the number of deliveries for the same month in the previous year, subject to a minimum norm or benchmark of 3 deliveries per PHC per month. Payment formula For each delivery over the benchmark, incentive of Rs. 150/- will be given, out of which Rs. 100/- will be given to the Nurse or Medical officer & Rs.50/- will be given to the cleaning personnel. Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
P a g e | 73
24. BEST GRAM PANCHAYAT SCHEME MAHARASHTRA
Award scheme to panchayats for improvement in health outcomes
Name of the payer: NA
Name of the recipient: Gram Panchayat
Geographical area & population covered:
Amravati District of Maharashtra
Budget: NA
Time frame: NA
Target population: Population of Amravati district
Implementing agencies: Govt. of Maharashtra
Documents reviewed: Information provided by the state
Existing evaluations: None
Eligibility criteria (for selection of recipient) Gram panchayats in Amravati District Set of services to be delivered Under this initiative, gram panchayat will be awarded prizes if they succeed in achieving no infant or maternal death, 100% registration of births and deaths, all deliveries are institutional deliveries, and special efforts to improve the status of grade 3 and 4 children. Performance Indicators Gram panchayat will be awarded prizes during 2 October to 14 November, if – 1) No infant / maternal death takes place 2) 100% registration of births and deaths 3) Every delivery takes place in institution 4) Special efforts to improve status of grade 3 and 4 children Payment formula Prizes will be given as follows:
Population up to Prize Money (Rs.)
1500 10,000/- 1501 – 3000 15,000/- 3001+ 20,000/-
Payment procedure Not available

Results based financing in Public Health Sector in India – Draft Report
74 | P a g e
Source & verification of data Not available Progress (before / after) Not available
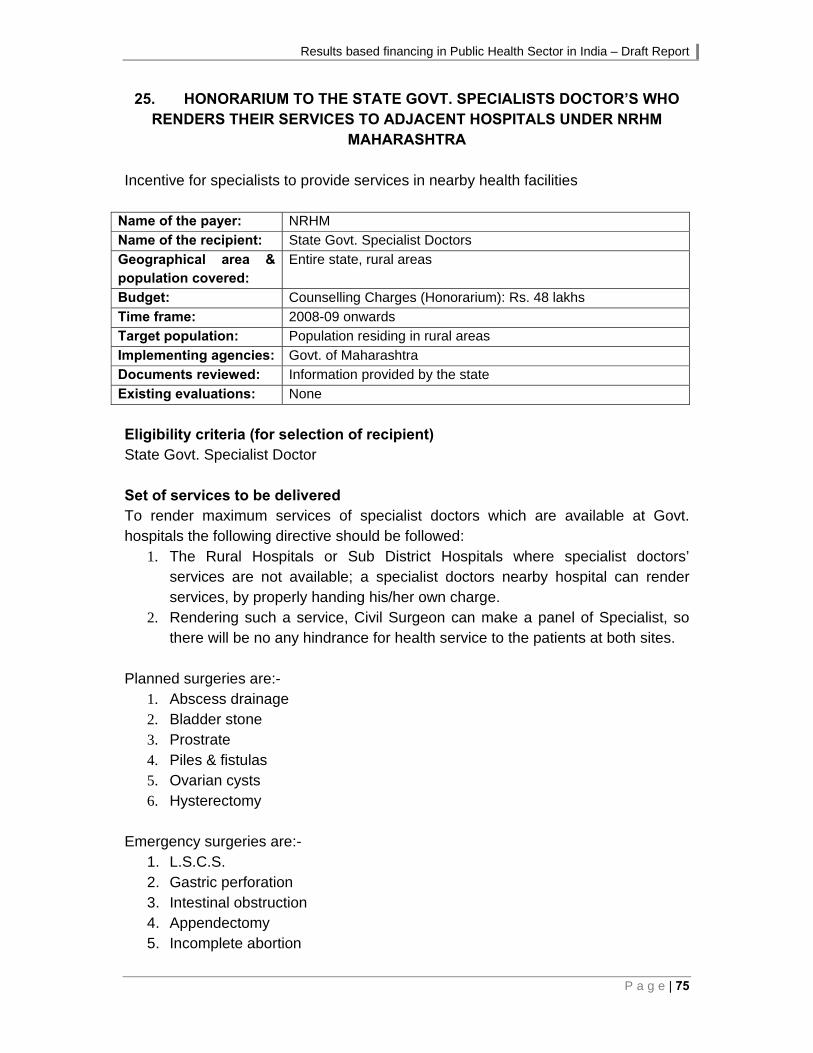
Results based financing in Public Health Sector in India – Draft Report
P a g e | 75
25. HONORARIUM TO THE STATE GOVT. SPECIALISTS DOCTOR’S WHO RENDERS THEIR SERVICES TO ADJACENT HOSPITALS UNDER NRHM
MAHARASHTRA Incentive for specialists to provide services in nearby health facilities
Name of the payer: NRHM
Name of the recipient: State Govt. Specialist Doctors
Geographical area & population covered:
Entire state, rural areas
Budget: Counselling Charges (Honorarium): Rs. 48 lakhs
Time frame: 2008-09 onwards
Target population: Population residing in rural areas
Implementing agencies: Govt. of Maharashtra
Documents reviewed: Information provided by the state
Existing evaluations: None
Eligibility criteria (for selection of recipient) State Govt. Specialist Doctor Set of services to be delivered To render maximum services of specialist doctors which are available at Govt. hospitals the following directive should be followed:
1. The Rural Hospitals or Sub District Hospitals where specialist doctors’ services are not available; a specialist doctors nearby hospital can render services, by properly handing his/her own charge.
2. Rendering such a service, Civil Surgeon can make a panel of Specialist, so there will be no any hindrance for health service to the patients at both sites.
Planned surgeries are:-
1. Abscess drainage 2. Bladder stone 3. Prostrate 4. Piles & fistulas 5. Ovarian cysts 6. Hysterectomy
Emergency surgeries are:-
1. L.S.C.S. 2. Gastric perforation 3. Intestinal obstruction 4. Appendectomy 5. Incomplete abortion

Results based financing in Public Health Sector in India – Draft Report
76 | P a g e
6. Ectopic Pregnancy 7. Close reduction fracture 8. Compound Fracture
Performance Indicators Number of surgeries conducted. Payment formula An incentive will be given to Specialist doctors who render their services to adjoining hospitals.
For planned surgery by Govt. Specialist, doctor will get incentive of Rs. 1000/- and anaesthetist will get incentive of Rs. 500/- for three surgeries, as honorarium.
For emergency surgery a Govt. specialist doctor will get incentive of Rs. 700 & anaesthetist will get incentive of Rs. 300/- per care as honorarium.
For planned specialist services where paediatrician, physician & gynaecologist are not available, adjacent Govt. Specialist will get incentive of Rs. 600/- per day as honorarium.
Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available
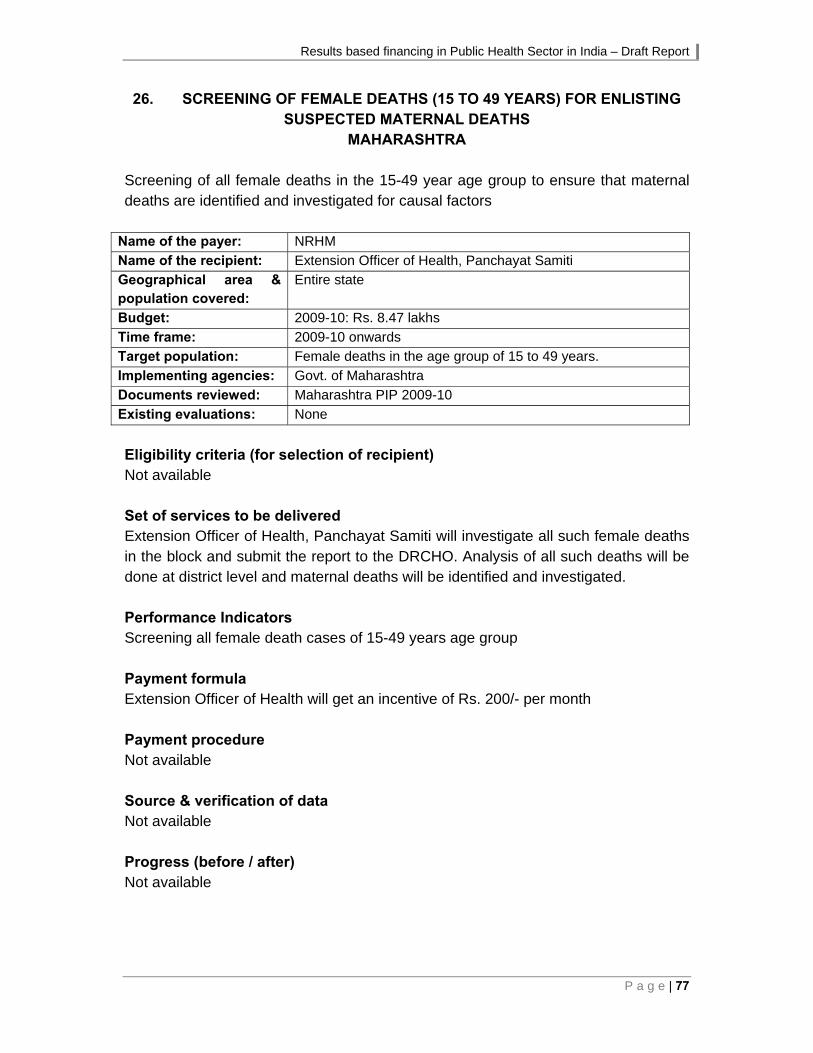
Results based financing in Public Health Sector in India – Draft Report
P a g e | 77
26. SCREENING OF FEMALE DEATHS (15 TO 49 YEARS) FOR ENLISTING SUSPECTED MATERNAL DEATHS
MAHARASHTRA Screening of all female deaths in the 15-49 year age group to ensure that maternal deaths are identified and investigated for causal factors
Name of the payer: NRHM
Name of the recipient: Extension Officer of Health, Panchayat Samiti
Geographical area & population covered:
Entire state
Budget: 2009-10: Rs. 8.47 lakhs
Time frame: 2009-10 onwards
Target population: Female deaths in the age group of 15 to 49 years.
Implementing agencies: Govt. of Maharashtra
Documents reviewed: Maharashtra PIP 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) Not available Set of services to be delivered Extension Officer of Health, Panchayat Samiti will investigate all such female deaths in the block and submit the report to the DRCHO. Analysis of all such deaths will be done at district level and maternal deaths will be identified and investigated. Performance Indicators Screening all female death cases of 15-49 years age group Payment formula Extension Officer of Health will get an incentive of Rs. 200/- per month Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
78 | P a g e
27. MATERNAL DEATH AUDIT MAHARASHTRA
Conducting an audit for all maternal deaths to identify and address the causes
Name of the payer: NRHM
Name of the recipient: District RCH Officer (DRCHO)
Geographical area & population covered:
Entire state
Budget: 2009-10: Rs. 19.17 lakhs approved
Time frame: 2009-10 onwards
Target population: Pregnant women
Implementing agencies: Govt. of Maharashtra
Documents reviewed: Maharashtra PIP 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) Not available Set of services to be delivered Under this activity, the DRCHO will visit the deceased house, do the verbal autopsy, and identify the circumstantial evidences related to the maternal death. The causes identified will be discussed in the District Maternal Death Audit Committee constituted in each district. On the basis of investigation reports, corrective actions to prevent further maternal deaths will be taken. Performance Indicators Number of maternal death audits conducted Payment formula Rs. 500/- per case out of which Rs. 200/- per case will be paid to DRCHO and Rs. 300/- will be incurred for mobility support. Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
P a g e | 79
28. DAI INCENTIVE SCHEME MAHARASHTRA
To promote institutional deliveries and incorporate the Dai's into the system.
Name of the payer: NRHM
Name of the recipient: Dais
Geographical area & population covered:
Districts where ASHAs have not been appointed
Budget: 2009-10: Rs. 28.90 lakhs
Time frame: 2009-10 onwards
Target population: Pregnant women
Implementing agencies:
Govt of Maharashtra
Documents reviewed: Maharashtra PIP 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) Dais in the districts where ASHAs have not been appointed till today (hence no conflict between ASHA and Dais for bringing the delivery cases) Set of services to be delivered To bring the delivery cases to the hospital. Performance Indicators Number of delivery cases brought to the district hospital Payment formula State has decided to give incentive of Rs. 200/- per case to Dais for bringing the delivery cases to the hospital. Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
80 | P a g e
29. COMPENSATION TO ASHA FOR PROMOTING IUD 380 A MAHARASHTRA
Name of the payer: NRHM
Name of the recipient: ASHA
Geographical area & population covered:
Implemented in Amravati & Parbhani districts on a pilot basis
Budget: Rs. 25.00 lakhs for 2009-10
Time frame: 2008-09 onwards
Target population: Eligible couples
Implementing agencies: Govt. of Maharashtra
Documents reviewed: Maharashtra PIP 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All ASHAs Set of services to be delivered IUD insertion services and counselling Performance Indicators Number of IUDs inserted and retained for at least 3 months Payment formula Rs. 200/- per case will be given as an incentive. Out of this, Rs. 100/- to beneficiary, Rs. 75/- to ASHA and Rs. 25/- to inserter will be paid after ensuring three months retention and follow-up. Payment procedure Not available Source & verification of data Not available Progress (before / after) The initiative will be continued with some modifications in these 2 districts during 2009-10, while an evaluation/ survey will be done to check its effectiveness.
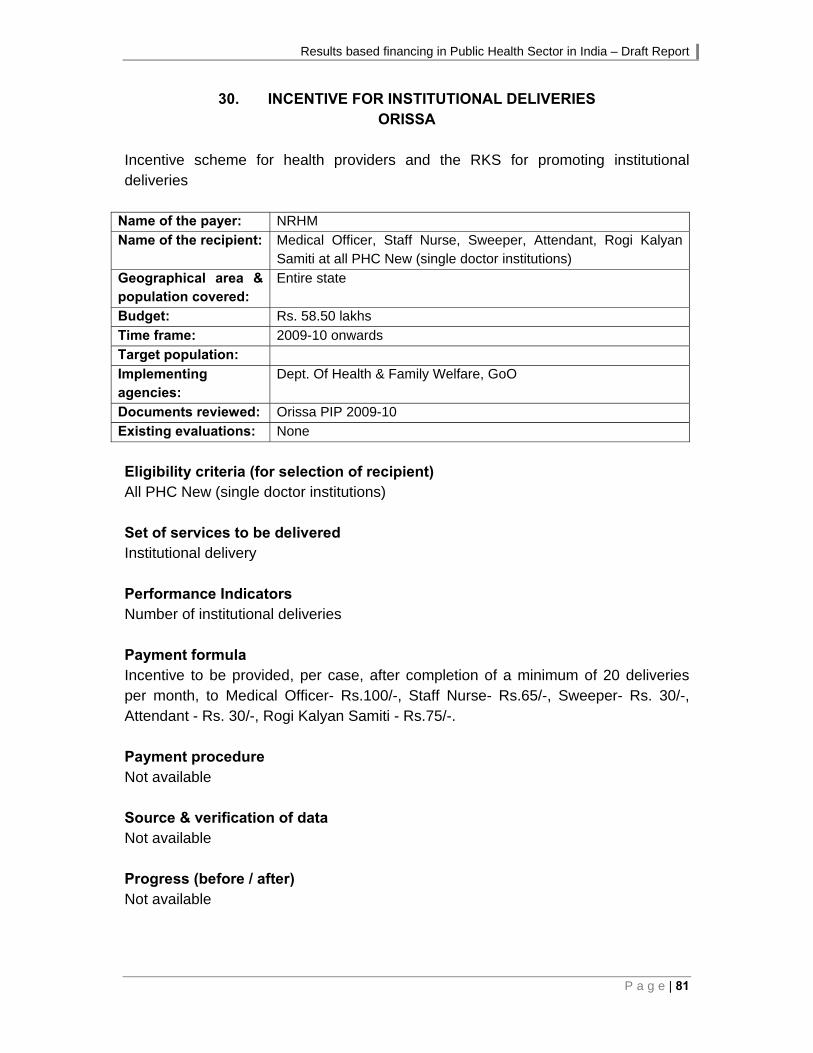
Results based financing in Public Health Sector in India – Draft Report
P a g e | 81
30. INCENTIVE FOR INSTITUTIONAL DELIVERIES ORISSA
Incentive scheme for health providers and the RKS for promoting institutional deliveries
Name of the payer: NRHM
Name of the recipient: Medical Officer, Staff Nurse, Sweeper, Attendant, Rogi Kalyan Samiti at all PHC New (single doctor institutions)
Geographical area & population covered:
Entire state
Budget: Rs. 58.50 lakhs
Time frame: 2009-10 onwards
Target population:
Implementing agencies:
Dept. Of Health & Family Welfare, GoO
Documents reviewed: Orissa PIP 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All PHC New (single doctor institutions) Set of services to be delivered Institutional delivery Performance Indicators Number of institutional deliveries Payment formula Incentive to be provided, per case, after completion of a minimum of 20 deliveries per month, to Medical Officer- Rs.100/-, Staff Nurse- Rs.65/-, Sweeper- Rs. 30/-, Attendant - Rs. 30/-, Rogi Kalyan Samiti - Rs.75/-. Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
82 | P a g e
31. JANANI EXPRESS YOJANA ORISSA
Provision of 24 hours transport availability at field level in order to bring the pregnant women to government health institutions
Name of the payer: NRHM, Government of Orissa
Name of the recipient: Vehicle owner
Geographical area & population covered:
State-wide
Budget: 2009-10: Rs.263.06 lakhs, 2008-09: Rs. 263.06
Time frame: 2008-09 onwards
Target population: • All pregnant women irrespective of caste, religion, age for to and fro travel for institutional deliveries. • Emergency Referral Services for women before and after deliveries. • Sick neonates, Infants and children below 1 year for emergency care and support.
Implementing agencies:
Govt. of Orissa
Documents reviewed: Orissa PIP 2009 – 10 and 2008-09
Initiative guidelines
Existing evaluations: None
Eligibility criteria (for selection of recipient) The transport vehicle will be hired locally on contractual basis for a period of one year on the basis of outsourcing criteria. A contract / MoU will be signed with a private agency/ NGO. The agency will ensure the 24 hour driver services and vehicle under the programme. The important features of the vehicle are as below.
Transport / vehicle which will be hired must possess all the pre-decided technical criteria such as the vehicle should not be of more than 24 months old, must have all the relevant papers including comprehensive insurance.
Preference will be given to vehicles like TATA Sumo, Mahendra Max, Maruti Van, having long seats for transport of pregnant women and sick neonates.
Folding ladder for climbing to vehicle.
Water and light facilities in the vehicle.
One folding stretcher
Curtains in the windows of the vehicle.
Disposable TBA / Dai Kits in the vehicle for emergency deliveries. (to be provided by concern RKS)
Cotton, Bandage, Dettol, Soap and First Aid Kit. (to be provided & replenished to concerned RKS)

Results based financing in Public Health Sector in India – Draft Report
P a g e | 83
The technical aspects of the vehicle are:
The vehicle is not older than two years.
Comprehensive Insurance valid policy is available with the vehicle.
The vehicle has all legal papers like registration, fitness certificate, Road Tax payment paper etc.
Valid driving license with the drivers
Security deposit of Rs.10,000/- in favour of “Rogi Kalyan Samiti” of respective CHC / PHC. In case RKS is not in position in the area the security deposit can be deposited in favour of “Zilla Swasthya Samiti (ZSS)”.
The agency interested to establish partnership with RKS under the programme will quote the financial offer keeping in account the road tax, insurance premium, VAT, parking fee, toll tax etc for which State Government or RKS will not pay.
The servicing and maintenance of vehicle from time to time is the responsibility of the private agency.
In case, the vehicle has to be sent for repair etc, the agency has to arrange an alternative vehicle for the period. In case of accident, the vehicle should be repaired within 48 hours.
Set of services to be delivered Transport will be made available in the concerned area of Government hospital, CHC, PHC, or to some other appropriate place as decided by the district/RKS. The vehicle will be attached to the Health Institutions at the disposal of MO I/C. The vehicle owner will be asked to provide the vehicle with drivers on 24X7 basis. The contact telephone number of the hospital, the driver and the doctor will be displayed on the body of the vehicle for public knowledge. On both sides of the vehicle “Janani Express” or “Janani Surakhya Bahini” will be painted in English in Oriya. The ANMs, AWWs and ASHAs have the information about all the pregnancies and expected date of deliveries. The driver and the agency operating the Janani Express will contact the ANM, AWWs, and ASHAs in the block for expected date of deliveries, place of deliveries and details of pregnant women to provide timely referral services for institutional delivery. The beneficiaries will also directly contact the driver, the doctor, and other service providers to send the vehicle as and when required. The drivers of Janani Express will stay in and around the Campus of concerned health institutions along with the vehicle on 24X7 hours basis. Performance Indicators The number of cases attended to as well as the number of kilometres covered. Payment formula
The agency will be paid the monthly hiring rent upto Rs.12,000/-pm.
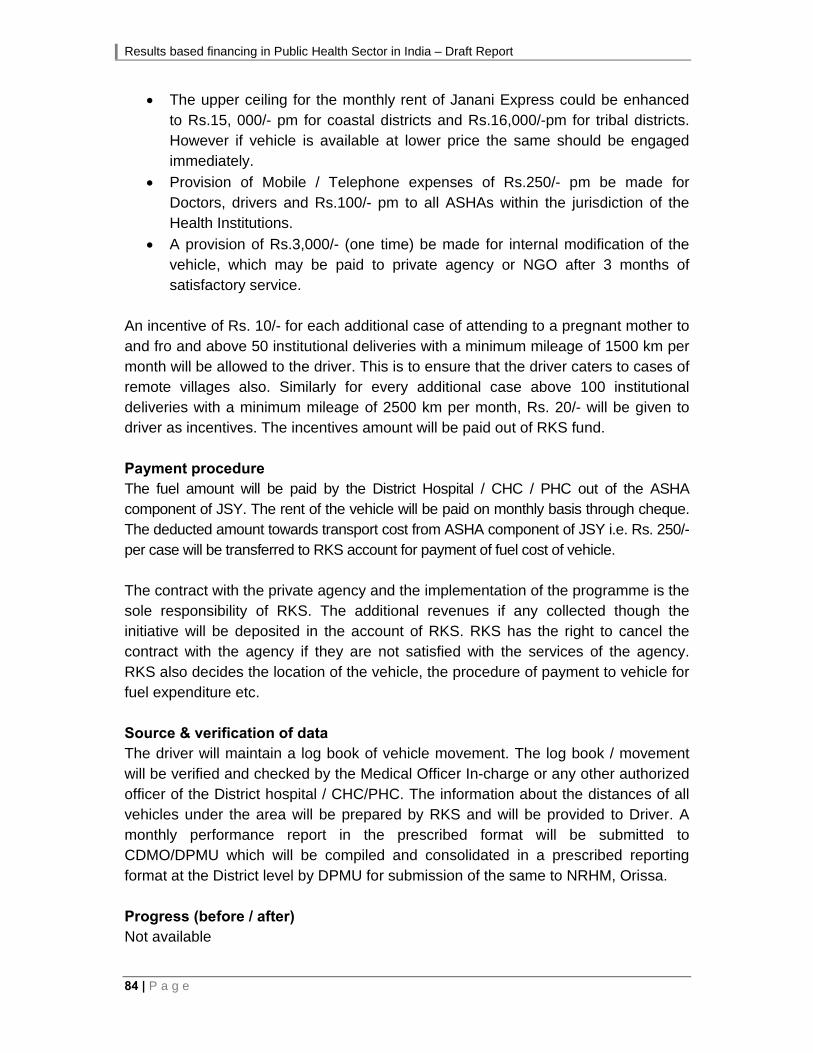
Results based financing in Public Health Sector in India – Draft Report
84 | P a g e
The upper ceiling for the monthly rent of Janani Express could be enhanced to Rs.15, 000/- pm for coastal districts and Rs.16,000/-pm for tribal districts. However if vehicle is available at lower price the same should be engaged immediately.
Provision of Mobile / Telephone expenses of Rs.250/- pm be made for Doctors, drivers and Rs.100/- pm to all ASHAs within the jurisdiction of the Health Institutions.
A provision of Rs.3,000/- (one time) be made for internal modification of the vehicle, which may be paid to private agency or NGO after 3 months of satisfactory service.
An incentive of Rs. 10/- for each additional case of attending to a pregnant mother to and fro and above 50 institutional deliveries with a minimum mileage of 1500 km per month will be allowed to the driver. This is to ensure that the driver caters to cases of remote villages also. Similarly for every additional case above 100 institutional deliveries with a minimum mileage of 2500 km per month, Rs. 20/- will be given to driver as incentives. The incentives amount will be paid out of RKS fund. Payment procedure The fuel amount will be paid by the District Hospital / CHC / PHC out of the ASHA component of JSY. The rent of the vehicle will be paid on monthly basis through cheque. The deducted amount towards transport cost from ASHA component of JSY i.e. Rs. 250/- per case will be transferred to RKS account for payment of fuel cost of vehicle. The contract with the private agency and the implementation of the programme is the sole responsibility of RKS. The additional revenues if any collected though the initiative will be deposited in the account of RKS. RKS has the right to cancel the contract with the agency if they are not satisfied with the services of the agency. RKS also decides the location of the vehicle, the procedure of payment to vehicle for fuel expenditure etc. Source & verification of data The driver will maintain a log book of vehicle movement. The log book / movement will be verified and checked by the Medical Officer In-charge or any other authorized officer of the District hospital / CHC/PHC. The information about the distances of all vehicles under the area will be prepared by RKS and will be provided to Driver. A monthly performance report in the prescribed format will be submitted to CDMO/DPMU which will be compiled and consolidated in a prescribed reporting format at the District level by DPMU for submission of the same to NRHM, Orissa. Progress (before / after) Not available

Results based financing in Public Health Sector in India – Draft Report
P a g e | 85
32. ALTERNATE HEALTH CARE DELIVERY SYSTEM PUNJAB
The alternate health delivery system in Punjab envisages provision of health care services through the Zilla Panchayats. The initiative aims to improve delivery of health services in rural areas (through transfer of management control to PRIs).
Name of the payer: Government of Punjab
Name of the recipient:
Geographical area & population covered:
Entire State
Budget: Year One: Rs. 112.09 crore, Year Two onwards: Rs. 58.95 crore/per year
Time frame: Launched in 2005, planned till 2009
Target population: Entire Rural Population covered by the Rural Dispensaries / Sub-Health Centres
Implementing agencies: Department of Health and Family Welfare, and Department of Panchayati Raj, Government of Punjab
Documents reviewed: State NRHM PIPs
Website of the Department of Health and Family Welfare, Government of Punjab
Existing evaluations: None, report based on routine monitoring data provided by Government of Punjab
Eligibility criteria (for selection of recipient) Punjab has a network of 1,310 rural dispensaries (SHCs), in addition to PHCs, CHCs and district hospitals, of which 1187 SHCs are managed by PRIs. The Zilla Parishads engage a team of doctors and paramedics, to provide outpatient services and elements of national programmes in rural dispensaries, building maintenance, provision of basic infrastructure and drugs worth Rs. 7,500/month (to be provided by the Zilla Parishad). Set of services to be delivered Service Providers (Doctors) not only provide health care but also help in implementation of various National and State Health Programmes aimed to control of specific diseases as well as other priority areas such as Family Welfare and AIDS etc. The maintenance of buildings of Subsidiary Health Centres will be carried out by the Zila Parishads and the requisite necessary basic equipments and furniture will also be provided by the Zila Parishads. The requisite medicines at the Subsidiary Health Centres will be supplied in kind @ Rs. 7,500/- per month which will be provided by Zila Parishads through Government funding.

Results based financing in Public Health Sector in India – Draft Report
86 | P a g e
Performance Indicators The State PIPs mention the following performance indicators, though more information would be available in the contract documents:
Immunization coverage by SHCs
Institutional/ SBA deliveries by SHCs Doctors will be engaged under a service contract, renewable after a three-year period, based on performance against established benchmarks. Doctors engaged under this initiative will be non-transferable. Payment formula Doctors will be paid a lump sum of Rs. 360,000/annum. Out of this they are expected to meet the salary of the paramedics and recurring expenses, such as utilities and day-to-day maintenance. Payment procedure The amount of remuneration package for all the Subsidiary Health Centres in the State will be provided as grant -in-aid to the Zila Parishads. Source & verification of data Not available Progress (before / after) Routine monitoring of the initiative shows that out-patient attendance in the dispensaries increased substantially from the baseline in 2005. Performance in selected programmes such as TB, blindness control and school health programmes also show improvement. Remarks The model has created an alternative to the mainstream health system and an in-depth understanding of the consequences of the initiative on existing public health facilities would enable evaluation of benefits. The innovation here is the Panchayat-managed service provision. Decentralised service delivery and management by institutions of local governance are attractive propositions, when the management and capacity building strategies are clearly thought out. The model demonstrates that the presence of a provider closer to communities and the uninterrupted availability of drugs increase service use. The initiative has demonstrated improved OPD service utilisation. Although data is insufficient to draw on more concrete lessons, it is evident that Panchayat-managed service provision has the potential to improve service utilisation.
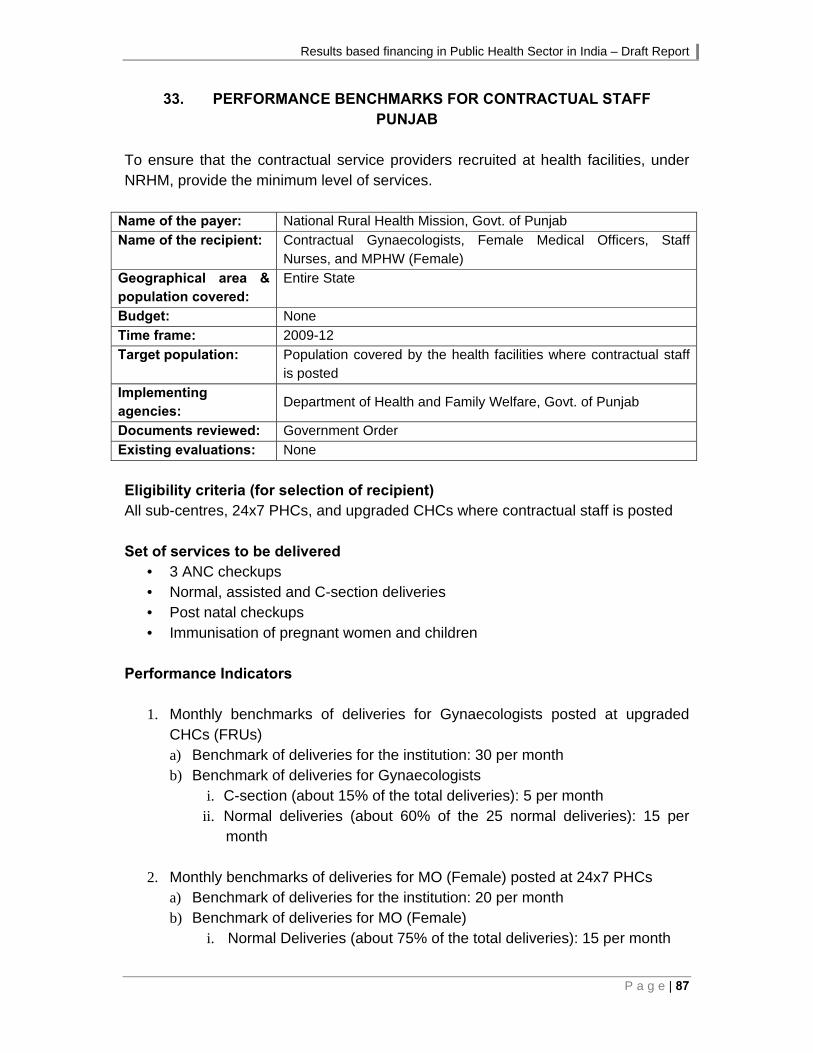
Results based financing in Public Health Sector in India – Draft Report
P a g e | 87
33. PERFORMANCE BENCHMARKS FOR CONTRACTUAL STAFF PUNJAB
To ensure that the contractual service providers recruited at health facilities, under NRHM, provide the minimum level of services.
Name of the payer: National Rural Health Mission, Govt. of Punjab
Name of the recipient: Contractual Gynaecologists, Female Medical Officers, Staff Nurses, and MPHW (Female)
Geographical area & population covered:
Entire State
Budget: None
Time frame: 2009-12
Target population: Population covered by the health facilities where contractual staff is posted
Implementing agencies:
Department of Health and Family Welfare, Govt. of Punjab
Documents reviewed: Government Order
Existing evaluations: None
Eligibility criteria (for selection of recipient) All sub-centres, 24x7 PHCs, and upgraded CHCs where contractual staff is posted Set of services to be delivered
• 3 ANC checkups • Normal, assisted and C-section deliveries • Post natal checkups • Immunisation of pregnant women and children
Performance Indicators
1. Monthly benchmarks of deliveries for Gynaecologists posted at upgraded CHCs (FRUs) a) Benchmark of deliveries for the institution: 30 per month b) Benchmark of deliveries for Gynaecologists
i. C-section (about 15% of the total deliveries): 5 per month ii. Normal deliveries (about 60% of the 25 normal deliveries): 15 per
month
2. Monthly benchmarks of deliveries for MO (Female) posted at 24x7 PHCs a) Benchmark of deliveries for the institution: 20 per month b) Benchmark of deliveries for MO (Female)
i. Normal Deliveries (about 75% of the total deliveries): 15 per month
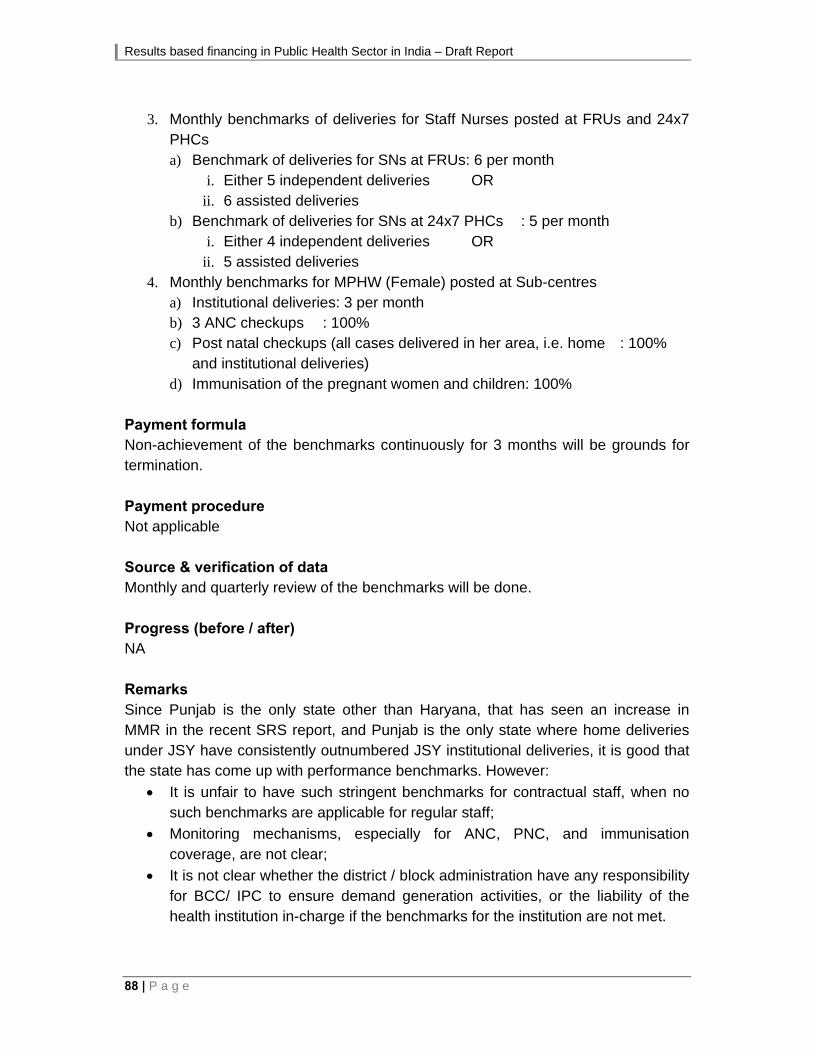
Results based financing in Public Health Sector in India – Draft Report
88 | P a g e
3. Monthly benchmarks of deliveries for Staff Nurses posted at FRUs and 24x7
PHCs a) Benchmark of deliveries for SNs at FRUs: 6 per month
i. Either 5 independent deliveries OR ii. 6 assisted deliveries
b) Benchmark of deliveries for SNs at 24x7 PHCs : 5 per month i. Either 4 independent deliveries OR ii. 5 assisted deliveries
4. Monthly benchmarks for MPHW (Female) posted at Sub-centres a) Institutional deliveries: 3 per month b) 3 ANC checkups : 100% c) Post natal checkups (all cases delivered in her area, i.e. home : 100%
and institutional deliveries) d) Immunisation of the pregnant women and children: 100%
Payment formula Non-achievement of the benchmarks continuously for 3 months will be grounds for termination. Payment procedure Not applicable Source & verification of data Monthly and quarterly review of the benchmarks will be done. Progress (before / after) NA Remarks Since Punjab is the only state other than Haryana, that has seen an increase in MMR in the recent SRS report, and Punjab is the only state where home deliveries under JSY have consistently outnumbered JSY institutional deliveries, it is good that the state has come up with performance benchmarks. However:
It is unfair to have such stringent benchmarks for contractual staff, when no such benchmarks are applicable for regular staff;
Monitoring mechanisms, especially for ANC, PNC, and immunisation coverage, are not clear;
It is not clear whether the district / block administration have any responsibility for BCC/ IPC to ensure demand generation activities, or the liability of the health institution in-charge if the benchmarks for the institution are not met.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 89
34. SOUBHAGYAVATI SCHEME UTTAR PRADESH
Improving institutional deliveries, with the involvement of the private providers
Name of the payer: NRHM/RCH
Name of the recipient: Pvt. obstetrician conducting deliveries.
Geographical area & population covered:
Entire state
Budget: Rs. 377.10 lakhs for 2009-10
Time frame: August 2008 onwards
Target population: Pregnant women of BPL families from rural and urban areas.
Implementing agencies: Govt. of Uttar Pradesh
Documents reviewed: PIP for 2008-09 and 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) Each private agency/provider will be required to select a geographical area of one or more blocks on the basis of first come first served principle. Not more than two agencies will be empanelled for a single block. Agency performing less than 50 deliveries a quarter would be debarred from the scheme. Set of services to be delivered Delivery services (normal / assisted and C- section), ANC visits, diagnostics Performance Indicators Number of institutional deliveries Payment formula An advance payment of Rs.25,000/- would be made to the empanelled provider to start providing services and would be replenished regularly. Payment procedure Not available Source & verification of data 25% of beneficiaries will be verified by an independent agency as per direction of DRHM. In case of fake reporting/ gap in service will draw a financial penalty as per State guidelines. Three continuous defaults would result in automatic blacklisting of the agency/provider. Progress (before / after) Till December 2008, almost 140 providers had been empanelled and around 9000 deliveries, including about 1000 caesarean cases were reported

Results based financing in Public Health Sector in India – Draft Report
90 | P a g e
35. PERFORMANCE BASED INCENTIVE TO HONORARY WORKER (DAIS) AT SUB CENTRES UTTAR PRADESH
Make Traditional Birth Attendants part of the regular system and help Sub Centre ANM in conducting deliveries and clinics
Name of the payer: NRHM/ RCH
Name of the recipient: Dais
Geographical area & population covered:
Entire state
Budget: Not available
Time frame: Not available
Target population: Pregnant women
Implementing agencies: Govt. of Uttar Pradesh
Documents reviewed: PIP for 2009-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All trained Dais Set of services to be delivered Support in deliveries and clinics Performance Indicators Number of deliveries and number of clinics Payment formula Rs. 100 per delivery and Rs. 25 per clinic to be paid to Dais. Payment procedure Not available Source & verification of data Not available Progress (before / after) Not available Remarks This is not a full-fledged RBF initiative since there is an upper limit of 2 deliveries and 4 clinics per month.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 91
36. PAYMENT TO ASHAS UNDER CCSP PROGRAMME UTTAR PRADESH
Incentive scheme for ASHA under the Comprehensive Child Survival Program (CCSP) to carry out home visits for new born care
Name of the payer: NRHM/ RCH Name of the recipient: ASHA Geographical area & population covered:
17 old CCSP Districts + 19 new
Budget: Rs. 6.00 lakhs Time frame: Initiated in 2007-08; however, actual implementation in 2008-09Target population: New born Implementing agencies:
Govt. of Uttar Pradesh
Documents reviewed: PIP for 2009-10 Existing evaluations: None Eligibility criteria (for selection of recipient) ASHAs in CCSP districts Set of services to be delivered Follow up and counselling Performance Indicators Number of newborn visited Payment formula Each ASHA would be paid Rs. 100/- for conducting 6 visits to each Low Birth Weight (LBW) newborn and Rs. 50/- for 3 visits to each normal weight newborns Payment procedure Detailed reporting formats, highlighting the findings at each visit and actions taken, have been developed. These have to be submitted monthly to the medical officer in-charge of the covering facility, after getting verification from the ANM. The payments are made to the ASHA through account payee cheques. This procedure (including the formats) has been standardized for all ASHA incentives under the various schemes (except JSY). Source & verification of data As above Progress (before / after) Not available
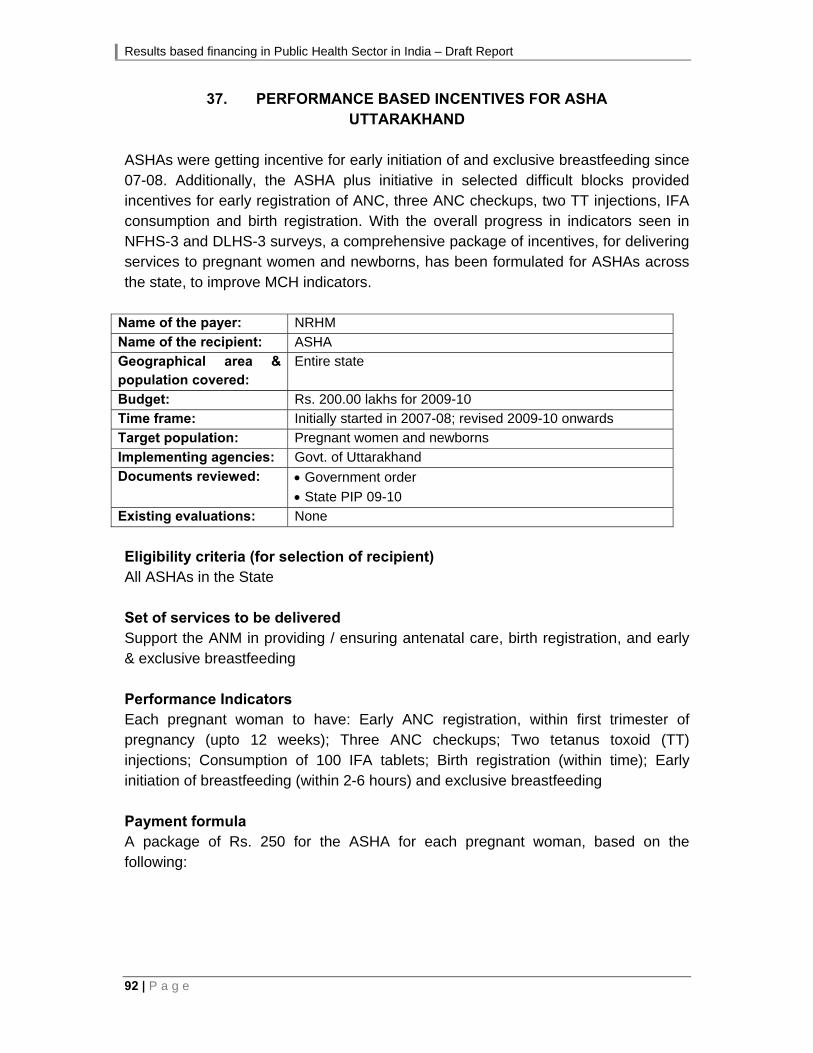
Results based financing in Public Health Sector in India – Draft Report
92 | P a g e
37. PERFORMANCE BASED INCENTIVES FOR ASHA UTTARAKHAND
ASHAs were getting incentive for early initiation of and exclusive breastfeeding since 07-08. Additionally, the ASHA plus initiative in selected difficult blocks provided incentives for early registration of ANC, three ANC checkups, two TT injections, IFA consumption and birth registration. With the overall progress in indicators seen in NFHS-3 and DLHS-3 surveys, a comprehensive package of incentives, for delivering services to pregnant women and newborns, has been formulated for ASHAs across the state, to improve MCH indicators.
Name of the payer: NRHM
Name of the recipient: ASHA
Geographical area & population covered:
Entire state
Budget: Rs. 200.00 lakhs for 2009-10
Time frame: Initially started in 2007-08; revised 2009-10 onwards
Target population: Pregnant women and newborns
Implementing agencies: Govt. of Uttarakhand
Documents reviewed: Government order
State PIP 09-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) All ASHAs in the State Set of services to be delivered Support the ANM in providing / ensuring antenatal care, birth registration, and early & exclusive breastfeeding Performance Indicators Each pregnant woman to have: Early ANC registration, within first trimester of pregnancy (upto 12 weeks); Three ANC checkups; Two tetanus toxoid (TT) injections; Consumption of 100 IFA tablets; Birth registration (within time); Early initiation of breastfeeding (within 2-6 hours) and exclusive breastfeeding Payment formula A package of Rs. 250 for the ASHA for each pregnant woman, based on the following:

Results based financing in Public Health Sector in India – Draft Report
P a g e | 93
Sn. Activity Amount
(Rs.)
1. Early ANC registration, within first trimester of pregnancy (upto 12 weeks) 20.00
2. Three ANC checkups 60.00
3. Two tetanus toxoid (TT) injections 40.00
4. Consumption of 100 IFA tablets 60.00
5. Birth registration (within time) 20.00
6. Early initiation of breastfeeding (within 2-6 hours) and exclusive breastfeeding 50.00
Total 250.00
The ASHA will not be paid for any component / service not provided. Payment procedure ANM will make the payment to ASHAs following verification of the services by the Village Health and Sanitation Committee (VHSC). Source & verification of data Reporting formats have been developed that each ASHA has to duly fill each month, and submit to the ANM after certification from the Secretary of the Village Health & Sanitation Committee. The ANM also has to certify the form submitted by each ASHA, and compile the same for onward submission to the Block Medical Officer (BMO), Chief District Medical Officer (CMO), and state authorities. The same is to be reviewed during district review meetings. A health supervisor in each block is to be made the nodal officer for this initiative. Outputs NA Progress (before / after) NA Remarks It is a good initiative to ensure overall antenatal care. However, since the payments are made each month on the components of the package covered, it is not clear how the tracking / monitoring will be done to ensure that each pregnant woman receives the entire package given that the services will be spread over 12-15 months. Under Janani Suraksha Yojana (JSY) all of the services mentioned above (except for birth registration), are intended to be covered in the role of the ASHA, along with motivating pregnant women for institutional delivery and accompanying them to the institution. For this the ASHA is already receiving Rs. 350 per case under JSY (plus Rs. 250 if she arranges for referral transport). However, visits to various states show that the focus seems to be more on the institutional delivery component of JSY.

Results based financing in Public Health Sector in India – Draft Report
94 | P a g e
38. PERFORMANCE BASED INCENTIVES FOR INSTITUTIONAL DELIVERIES
UTTARAKHAND Performance benchmark for each facility for institutional deliveries is based on the achievement during the same month in the previous year.
Name of the payer: Uttarakhand Health & Family Welfare Society, Department of Health & Family Welfare, Govt. of Uttarakhand
Name of the recipient:
Service providers and RKS
Geographical area & population covered:
Entire state
Budget: Rs. 20.00 lakhs for 2009-10
Time frame: 2009 onwards
Target population: Pregnant women undergoing institutional delivery
Implementing agencies:
Dept. of Health & Family Welfare, Govt. of Uttarakhand
Documents reviewed: Government Order
Existing evaluations: -
Eligibility criteria (for selection of recipient) All health institutions in the State Set of services to be delivered Pregnant women undergoing delivery at an FRU / CHC, PHC or a sub-centre Performance Indicators Benchmark is the number of deliveries at the institution during the same month in the previous year. Payment formula For each delivery above the benchmark, incentive will be given to the service providers and to the facility (RKS or untied fund) based on the following formula:
Beneficiary FRU / CHC 24x7 PHC Sub-centre
Doctor Rs. 200 Rs. 200 ---
Staff Nurse / ANM Rs. 75 Rs. 75 Rs. 200
Support staff (sweeper / ayah) Rs. 50 Rs. 50 Rs. 50
Institution (RKS / untied fund) Rs. 75 Rs. 75 Rs. 50 Total Rs. 400 Rs. 400 Rs. 300

Results based financing in Public Health Sector in India – Draft Report
P a g e | 95
Payment procedure NA (present in an earlier government order) Source & verification of data Facility-wise data to be compiled by each block on a specified reporting format, and submitted to the district. This will be compared the corresponding month of previous year. Progress (before / after) Not available
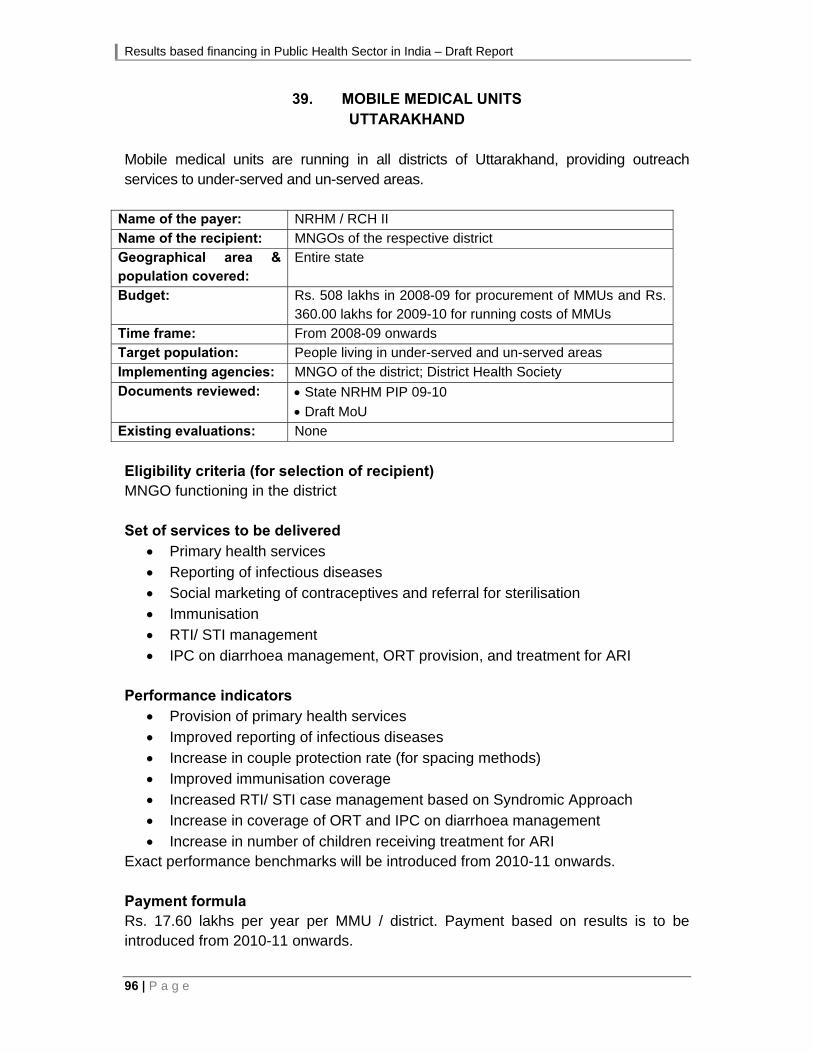
Results based financing in Public Health Sector in India – Draft Report
96 | P a g e
39. MOBILE MEDICAL UNITS UTTARAKHAND
Mobile medical units are running in all districts of Uttarakhand, providing outreach services to under-served and un-served areas.
Name of the payer: NRHM / RCH II
Name of the recipient: MNGOs of the respective district Geographical area & population covered:
Entire state
Budget: Rs. 508 lakhs in 2008-09 for procurement of MMUs and Rs. 360.00 lakhs for 2009-10 for running costs of MMUs
Time frame: From 2008-09 onwards
Target population: People living in under-served and un-served areas
Implementing agencies: MNGO of the district; District Health Society
Documents reviewed: State NRHM PIP 09-10
Draft MoU
Existing evaluations: None
Eligibility criteria (for selection of recipient) MNGO functioning in the district Set of services to be delivered
Primary health services Reporting of infectious diseases Social marketing of contraceptives and referral for sterilisation Immunisation RTI/ STI management IPC on diarrhoea management, ORT provision, and treatment for ARI
Performance indicators
Provision of primary health services Improved reporting of infectious diseases Increase in couple protection rate (for spacing methods) Improved immunisation coverage Increased RTI/ STI case management based on Syndromic Approach Increase in coverage of ORT and IPC on diarrhoea management Increase in number of children receiving treatment for ARI
Exact performance benchmarks will be introduced from 2010-11 onwards. Payment formula Rs. 17.60 lakhs per year per MMU / district. Payment based on results is to be introduced from 2010-11 onwards.

Results based financing in Public Health Sector in India – Draft Report
P a g e | 97
Payment procedure Annual amount given in advance, to be deposited in a separate project account Source & verification of data Monitoring formats developed by the MNGO, and approved by the District Health & Family Welfare Society (DHFWS). Quarterly progress reports highlighting the progress, and the activities that were not completed according to time schedule, along with reasons for the variance. Progress (before / after)
S. No.
Name of the District
Name of the Mother NGO Total No. of OPD
Date of Start Report Upto Expenditu
re
1 Pithoragarh Himalaya Study Circle 5830 May, 09 October, 09 88,351
2 Champawat Himalaya Study Circle 5574 May, 09 October, 09 5,02,680
3 Tehri Garhwal Community Development & Welfare Society
10537 April, 09 October, 09 9,13,475
4 Uttarkashi Shri Bhuvneshwari Mahila Ashram 5640 April 09 October, 09 8,03,275
5 Pauri Himalayan Institute Hospital Trust 2329 July, 09 October, 09 5,68,734
6 Dehradun Himalayan Institute Hospital Trust 3648 April 09 October, 09 8,50,100
7 Haridwar Ambuja Cement Foundation 6428 April 09 October, 09 8,44,581
8 U.S. Nagar IMPART 3512 June 09 October, 09 6,69,984
9 Rudraprayag Gomti Pryag Jan Kalyan Parishad 5620 April 09 October, 09 9,72,000
10 Almora INHERE 4070 May 09 October, 09 7,80,470
11 Bageshwar Gramin Uthan Samiti 5127 April 09 October, 09 8,78,600
12 Nainital Gramin Uthan Samiti 3176 June 09 October, 09 6,10,051
13 Chamoli Shri Bhuvneshwari Mahila Ashram 4077 April, 09 October, 09 8,28,485 Total 65568 93,10,786
S.
No. Distt.
X- Ray
ANC Blood Test UrineTest
PregnancyTest
Contraceptives Immunization
1 Chamoli 73 304 21 31 NR NR
2 Tehri 165 279 1224 304 NR NR 128
3 Bageshwar 209 725 (incl. urine) NR NR NR NR
4 Nainital 128 298 (incl. urine) NR NR NR NR
5 U.S. Nagar 35 164 377 181 NR 1000 Condom 20 OCP packs
NR
6 Rudraprayag 15 48 235 770 37 NR NR
7 Haridwar 10 22 27 NR NR 1000 NR
8 Almora 75 87 110 68 NR NR
9 Dehradun …. 87 56 106 66 NR NR
10 Pauri …. 60 62 100 55 NR NR
11 Uttarkashi 22 574 NR NR NR NR
12 Champawat 1000
13 Pithoragarh 57 110 66 12 1000 126

Results based financing in Public Health Sector in India – Draft Report
98 | P a g e
40. AYUSHMATI SCHEME WEST BENGAL
The objective of the initiative is to increase the number of institutional deliveries by partnering with private sector facilities empanelled against certain pre-determined criteria and also to ensure quality of service delivery in the empanelled private sector facilities by stringent monitoring and supervision.
Name of the payer: NRHM / State Government of West Bengal
Name of the recipient: Empanelled private facilities
Geographical area & population covered:
Initially the initiative was implemented in the following 11districts: Uttar Dinajpur, Malda, Murshidabad, Bankura, Nadia, Purulia, Paschim Medinipur, Coochbehar, Birbhum, Dakshin Dinajpur, Jalpaiguri. At present all the districts are being covered under this initiative.
Budget: 2009-10 Rs. 300 lakhs
Time frame: January 2007 onwards
Target population: Pregnant women from BPL and all SC/ST families
Implementing agencies: Dept. of Health & Family Welfare, GoWB, District Health & Family Welfare Samity, GoWB; Private Hospitals / Nursing Home / facilities run by NGO / CBO
Documents reviewed: http://www.wbhealth.gov.in/nrhm/GUIDELINES%20FOR%20AYUSHMATI%20SCHEME%5B1%5D.pdf
http://www.wbhealth.gov.in/download/ayush_sch.pdf
Draft MoU
West Bengal PIP 09-10
Existing evaluations: None
Eligibility criteria (for selection of recipient) Empanelment of private health facilities, subject to fulfilment of the following:
• No. of beds • Providers: obstetrician, anaesthetist, paediatrician, RMO, staff nurse,
paramedical staff • Necessary medicines • Blood transfusion • Infrastructure • Compliance with the statutory norms • Technical component • Roles, responsibilities, obligations of the private partner.
Empanelment would be carried out by District Team comprising of
• Dy. CMOH III – Chairman • One senior gynaecologist • One senior anaesthetist

Results based financing in Public Health Sector in India – Draft Report
P a g e | 99
• One senior paediatrician • One superintendent of SDH/ SGH of the respective district.
Set of services to be delivered By the private partner:
• Normal delivery • Caesarean Sections • One OPD visit of the mother and new born child post delivery within six weeks
of discharge from the facility • BCG and Polio – O to the new born • Blood for TC, DC, ESR, Hb% • Urine for routine examination • Blood for PPBs • VDRL Test • Blood for grouping and typing • Pregnancy profile – USG screening
The services do not include post partum care, except one post – natal checkup. Also the private partner:
• Shall provide proper infrastructure including manpower, space and equipment for delivery.
• Shall not refuse any pregnant woman registered under the scheme as long as there are unoccupied beds. Shall make available atleast 10%/2 of the beds(whichever is higher) in their facility for the puposes of the beneficiaries under the Ayushmati Scheme having valid documentary evidence of their status as a beneficiary of the scheme.
• Shall keep proper records of the refusal cases • In the event of a pregnant woman registered under the scheme is being
referred, such a referral facility must be a public hospital under the State Health Department.
• Shall adhere to the SOP (ensure quality of service, employing personnel with proper qualifications, ensure cleanliness, etc)
• Shall cooperate with the monitoring team • Shall comply with the reporting requirements • Shall not discriminate the pregnant woman registered under the scheme from
other patients of the nursing home/hospitals • Shall arrange for hands on skill based training of RMOs and nurses in
collaboration with the district level officials.

Results based financing in Public Health Sector in India – Draft Report
100 | P a g e
The ANM: • Shall maintain a list of all pregnant women of BPL and all SC/ ST categories
in her work area and update it on a regular basis. • Shall ensure that all pregnant women have taken two TT injections and gone
for at least three ante- natal check – ups. • Shall make all pregnant women and her family members aware about the
‘Ayushmati Scheme’ and motivate them for institutional delivery. • Motivate the pregnant women to come for post natal check-ups and child
immunisations after the delivery • Shall give JSY vouchers and explain the ‘Ayushmati scheme’ and inform
about the nearby empanelled facility to the pregnant women • Shall fill in the patient satisfaction for of those availing the scheme.
Performance Indicators Number of institutional deliveries, both normal and C- section conducted by the provider. Payment formula For a group of 100 deliveries, cost of the package is Rs. 1.79 lakhs. Of this amount Rs 1515 is meant for the delivery and Rs 275 is for conducting routine investigations relating to delivery. Also the private partner will be entitled to a claim of Rs.75 per case for all cases where referrals are made and a person trained in First Aid is accompanying the patient to the referral point. From 2009-10, after discussion with District Health Officials and private providers the amount has been revised to Rs.3200/- w.e.f 01/02/2009 taking into account the recent price escalation and the continuity of the initiative in future as follows:
• For delivery (Normal/ C-section/ Assisted) Rs.2200/- • Investigations Rs 275/- • Essential newborn care up to 28 days of delivery Rs. 725/-
Grounds for termination of the service contract: In case, all accounts are not found to be transparent and necessary audit and inspections are not carried out, the service quality is not adhered to, the ethical guidelines for clinical examination, treatment initiation and continuation etc is not followed strictly, a review or audit of the facilities find that the manner of implementation are not in accordance with the objectives of the proposal then all subsequent instalments can be withheld and even empanelment may be withdrawn. Moreover in case the private partner becomes insolvent, or there is a criminal indictment against any of the partners or the proprietor, then the contract will be terminated. Dispute Resolution: If a dispute arises, efforts to resolve the dispute through negotiations failing, attempts to resolve the dispute will be strengthened with the

Results based financing in Public Health Sector in India – Draft Report
P a g e | 101
intervention if the Addtl. Chief Secretary - Health, Dept. of Health and Family Welfare, GoWB. If the parties fail to arrive at an amicable resolution, it will be resolved within the provisions of the Indian Arbitration and Reconciliation Act as applicable within WB at that point in time. Payment procedure Women to be registered with the ANMs and having received at least three antenatal check-ups at any of the Sub-centre / nearby public facilities. It will be a cash-less service, that is, the Beneficiaries of the scheme will not have to make payment for the institutional delivery services availed at the Empanelled Private facilities. The BPL Cards / Gram Panchayat certificates / JSY Card / MCH card /SC or ST certificate / SC or ST certification by the Gram Panchayat will be used for the purpose of availing benefit under the scheme. Procedure for claim submission:
a) In case more than 100 deliveries take place in a year, the private partner shall be reimbursed for the additional number of deliveries on pro rata basis.
b) The private partner shall submit utilisation certificate at every month in the prescribed format. For the sake of convenience, the period will be considered from the first day of the first calendar month to the last day of the same calendar month.
c) Utilisation certificate should be submitted within seven calendar days from the last day of the month concerned.
d) The Utilisation Certificate shall be accompanied with the copies of monthly report for the corresponding period.
e) The private partner shall refund the unadjusted amount by A/c payee cheque to DHFWS on expiry/ termination of the contract within seven days from the date of expiry/ termination of the contract.
f) Non-submission of the utilisation certificate within due date shall be considered as a ground for termination of contract.
g) All transactions will be guided by stipulated Grievance Redressal Mechanism, Protocols for claim submission and for claim reimbursement.
Source & verification of data Records are to be maintained as per the MIS template at the facility level which will be communicated to the Block / District level as the case may be. There will be a quality check health team, which will be responsible for periodic quality checks as well as routine checks for accreditation of private facilities and empanelment of obstetric teams. Annual external evaluation shall be carried out by an assigned agency. The monitoring team shall visit the private partner facility atleast once in a quarter without informing the private partner and shall identify the training needs of the RMOs and nurses employed in private sector facilities.

Results based financing in Public Health Sector in India – Draft Report
102 | P a g e
Progress (before / after) 66 facilities are participating in this initiative (Aug 2009). Total number of beneficiaries:
2007-08 2008-09 2009-10(Apr-Aug)
TOTAL
Normal deliveries 742 4512 2357 7611
C-sections 483 2036 953 3472
Total 1225 6548 3310 11083

ANNEX 3
BASIS FOR RECOMMENDATIONS OF RBF INITIATIVES FOR IN-DEPTH STUDY


Results based financing in Public Health Sector in India – Draft Report
P a g e | 103
BASIS FOR RECOMMENDATIONS OF RBF INITIATIVES FOR IN-DEPTH STUDY 1. Eleven out of the 40 RBF initiatives have been under implementation for at least
two years:
No. of Years Number
>3 6
>2 5
<2 17
<1 10
NA 2
Total 40
2. Ten of the 40 RBF initiatives have been scaled up, since implementation began:
Scaled up Number
Yes 10
No 7
Not applicable 21
Not available 2
Total 40
3. Seven of the RBF initiatives have seen an increase in their budget since
implementation began:
Increase in Budget Number
Yes 7
No 8
Not applicable 13
Not available 12
Total 40
4. The following table shows the application of the above criteria across the
schemes: S.
no. Name of the initiative State
No. of Years
Scaled up Increase in
Budget
1 Performance incentives for Govt. facilities to improve Institutional deliveries
Assam <2 Not
applicable Not available
2 Incentive to ASHA for completion of Full immunisation
Assam <2 Not
applicable Not available
3 Chiranjeevi Yojana Assam <1 Not
applicable Not
applicable
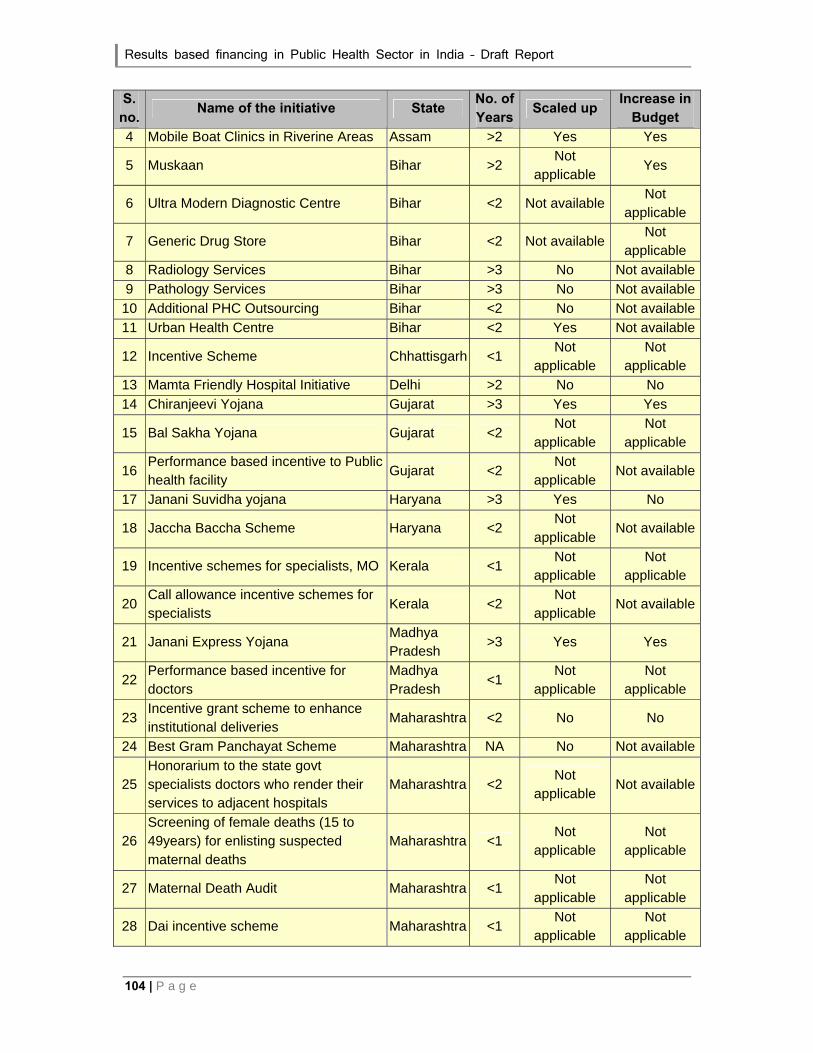
Results based financing in Public Health Sector in India – Draft Report
104 | P a g e
S. no.
Name of the initiative State No. of Years
Scaled up Increase in
Budget
4 Mobile Boat Clinics in Riverine Areas Assam >2 Yes Yes
5 Muskaan Bihar >2 Not
applicable Yes
6 Ultra Modern Diagnostic Centre Bihar <2 Not available Not
applicable
7 Generic Drug Store Bihar <2 Not available Not
applicable
8 Radiology Services Bihar >3 No Not available
9 Pathology Services Bihar >3 No Not available
10 Additional PHC Outsourcing Bihar <2 No Not available
11 Urban Health Centre Bihar <2 Yes Not available
12 Incentive Scheme Chhattisgarh <1 Not
applicable Not
applicable
13 Mamta Friendly Hospital Initiative Delhi >2 No No
14 Chiranjeevi Yojana Gujarat >3 Yes Yes
15 Bal Sakha Yojana Gujarat <2 Not
applicable Not
applicable
16 Performance based incentive to Public health facility
Gujarat <2 Not
applicable Not available
17 Janani Suvidha yojana Haryana >3 Yes No
18 Jaccha Baccha Scheme Haryana <2 Not
applicable Not available
19 Incentive schemes for specialists, MO Kerala <1 Not
applicable Not
applicable
20 Call allowance incentive schemes for specialists
Kerala <2 Not
applicable Not available
21 Janani Express Yojana Madhya Pradesh
>3 Yes Yes
22 Performance based incentive for doctors
Madhya Pradesh
<1 Not
applicable Not
applicable
23 Incentive grant scheme to enhance institutional deliveries
Maharashtra <2 No No
24 Best Gram Panchayat Scheme Maharashtra NA No Not available
25 Honorarium to the state govt specialists doctors who render their services to adjacent hospitals
Maharashtra <2 Not
applicable Not available
26 Screening of female deaths (15 to 49years) for enlisting suspected maternal deaths
Maharashtra <1 Not
applicable Not
applicable
27 Maternal Death Audit Maharashtra <1 Not
applicable Not
applicable
28 Dai incentive scheme Maharashtra <1 Not
applicable Not
applicable

Results based financing in Public Health Sector in India – Draft Report
P a g e | 105
S. no.
Name of the initiative State No. of Years
Scaled up Increase in
Budget
29 Compensation to ASHA for promoting IUD 380A
Maharashtra <2 No No
30 Incentive for institutional deliveries Orissa <1 Not
applicable Not
applicable
31 Janani Express Yojana Orissa <2 Yes Yes
32 Alternate health care delivery system Punjab >3 Not
applicable No
33 Performance benchmarks for contractual staff
Punjab <1 Not
applicable Not
applicable
34 Soubhagyavati Scheme Uttar Pradesh
<2 Not
applicable No
35 Performance based incentive to honorary worker (Dais) at sub centres
Uttar Pradesh
NA Not
applicable Not available
36 Payment to ASHA under CCSP Program
Uttar Pradesh
<2 Yes No
37 Performance based incentives to ASHA
Uttarakhand >2 Yes Yes
38 Performance based incentives for institutional deliveries
Uttarakhand <1 Not
applicable Not
applicable
39 Mobile medical units Uttarakhand <2 Yes Yes
40 Ayushmati scheme West Bengal >2 Yes No