Embed Size (px)
Citation preview
ORIGINAL CONTRIBUTION diagnosis-related groups
DRGs and the "Negative" Trauma Workup
We conducted a study to assess the financial impact of the diagnostic workup and care of 136 trauma patients admitted to our institution dur- ing a six-month period who were subsequently found to have only minor injuries (Injury Severity Score <~ 9, Abbreviated Injury Score < 3). The New Jersey DRG reimbursement system, an all-payer system, failed to pro- vide adequate financial compensation overall, as the average loss per pa- tient (operating cost minus reimbursement) was $508. Lost potential reve- nue (hospital charges minus reimbursement) was even greater, averaging $1,834 per patient. We conclude that the New Jersey DRG reimbursement system, in its current form, provides inadequate reimbursement for the proper workup and treatment of trauma patients with minor injuries. Be- cause these patients are those most likely to help "subsidize" the care of sicker patients, changes in the system are necessary to allow hospitals to continue to provide state-of-the-art trauma care and to continue to mini- mize the number of preventable deaths due to trauma. [Flancbaum L, Dougherty C, Brotman DN, Avedian J, Trooskin SZ: DRGs and the "nega- tive" trauma workup. Ann Emerg Med July 1990;19:741-745.]
INTRODUCTION Earlier diagnosis and treatment of life-threatening injuries through the
use of regionalized trauma care systems have reduced the number of pre- ventable deaths due to trauma.~,z Concurrently, escalating health-care ex- penditures have led to the implementation of programs designed to curtail costs. Since 1980, all hospital care in New Jersey has been reimbursed through a prospective payment system (diagnosis-related groups [DRGs]) in which the "case mix" of patients is supposed to "average out" (ie, "profits" gained from the care of less-ill patients offset "losses" incurred in caring for sicker patients). 3 Since the introduction of DRG methodology for hos- pital reimbursement, several studies have documented net financial losses resulting from the care of seriously injured patients. 4 ~2 The purpose of this study was to evaluate the financial impact of DRG reimbursement on our hospital resulting from the care of minimally injured patients and de- termine whether these less-ill patients do indeed help subsidize the care of sicker trauma patients.
MATERIALS A N D METHODS We reviewed the charts of all patients admitted to Robert Wood Johnson
University Hospital with a diagnosis of multiple trauma between July l, 1987, and December 31, 1987, who subsequently were found to have only minor injuries. Robert Wood Johnson University Hospital is a 420-bed uni- versity hospital that serves as the primary teaching facility for the Univer- sity of Medicine and Dentistry of New Jersey - Robert Wood Johnson Med- ical School and is a tertiary-care referral center for the more than 2 million citizens of central New Jersey. The hospital has had an active trauma pro- gram (admitting more than 600 injured patients yearly) since 1985 and has served de facto as an undesignated Level I trauma center for central New Jersey pending final plans for the further designation of trauma centers by the New Jersey Department of Health.
All patients were triaged in the emergency department by an attending emergency physician to the trauma service, and then evaluated and resus-
Louis Flancbaum, MD Catherine Dougherty, RN David N Brotman, MD John Avedian, RRN Stanley Z Trooskin, MD New Brunswick, New Jersey
From the Department of Surgery, Section of Trauma Surgery, UMDNJ -- Robert Wood Johnson Medical School, New Brunswick, New Jersey.
Received for publication Juty 7, 1989. Revision received December 11, 1989. Accepted for publication February 1, 1990.
Presented at the Society for Academic Emergency Medicine Annual Meeting in San Diego, May 1989.
Address for reprints: Louis Flancbaum, MD, Department of Surgery, Ohio State University Medical Center, 410 West 10th Avenue, Columbus, Ohio 43210.
19:7 July 1990 Annals of Emergency Medicine 741/39
TRAUMA WORKUP Flancbaum et al
citated according to institutional pro- tocols based on the advanced trauma life support (ATLS) course under the supervision of a full-time attending trauma surgeon, a3
The Injury Severity Score (ISS), as described in the Hospital Trauma In- dex of the American College of Sur- geons, 14 was calculated as the sum of the squares of the three highest Ab- brevia ted Injury Scores (AISs) for each patient. Patients having an ISS of 9 or less with every AIS less than 3 were considered to have sustained only minor injuries. Data regarding age, sex, diagnosis, DRG coding, op- erative therapy, length of stag inten- sive care management (monitoring), laboratory tests, radiographs, and in- t e r v e n t i o n a l p rocedures were ex- tracted and collated. Hospital finan- cial reports documenting final DRG categorizat ion, actual th i rd-par ty (DRG) reimbursement, cost of total hospitalization (defined as the sum of the individual depar tment charges multiplied by their respective cost- to-charge ratio), and actual "billed" hospital charges (had there not been DRG reimbursement) were generated for these patients and subsequently analyzed.
Standard fiscal analyses including determination of financial loss (de- fined as cost minus re imbursement ["contribution margin"]) and poten- tial revenue lost (defined as charges minus re imbursement) were calcu- lated for each patient, each individ- ual DRG group, and the study group as a whole.
RESULTS There were 136 patients, of whom
91 (67%) were male. The average age was 30.1 years (range, 17 days to 87 years), with nearly 70% between the ages of 11 and 40 years. The average ISS was 4.7, with a mode of 5. The most common mechanism of injury was m o t o r v e h i c l e a cc i den t (91, 67%), followed by fall (11, 8%), mo- torcycle accident (nine, 7%), and gunshot wound (seven, 5%).
Average length of stay for all pa- tients was 3.8 days. Twenty-one pa- tients required intensive care obser- vation for an average of 1.7 days. Of these, six observations were to rule out myocardia l contusion, 14 were for monitoring of closed-head injury, and one was to rule out aortic rup- ture. In these 21 patients, the overall length of stay was 4.2 days. Fifteen
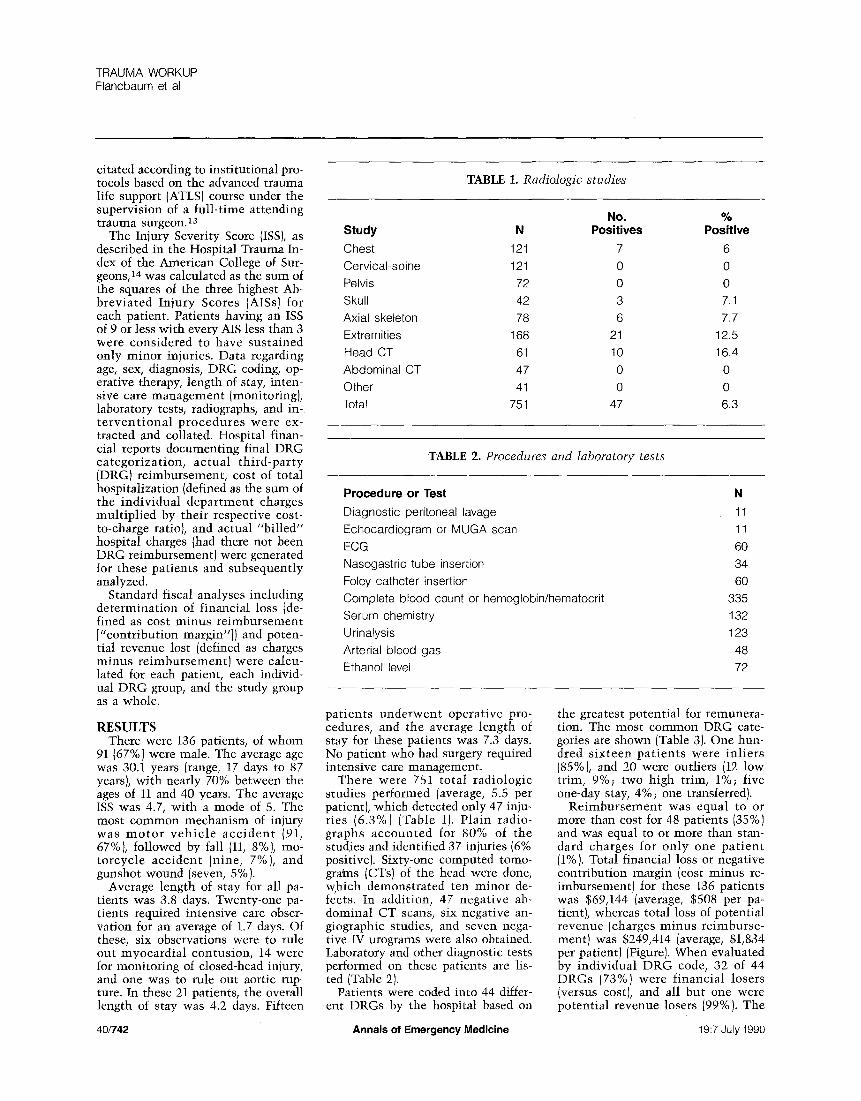
TABLE 1. Radiologic studies
No. % Study N Positives Positive
Chest 121 7 6 Cervical-spine 121 0 0
Pelvis 72 0 0
Skull 42 3 7.1
Axial skeleton 78 6 7.7
Extremities 168 21 12.5
Head CT 61 10 16.4
Abdominal CT 47 0 0
Other 41 0 0
Total 751 47 6.3
TABLE 2. Proceduzes and laboratory tests
Procedure or Test
Diagnostic peritoneal lavage
Echocardiogram or MUGA scan
ECG Nasogastric tube insertion
Foley catheter insertion
Complete blood count or hemoglobin/hematocrit
Serum chemistry
Urinalysis
Arterial blood gas Ethanol level
N
11
11
60 34
60
335 132
123
48
72
pat ients underwent operative pro- cedures, and the average length of stay for these patients was 7.3 days. No patient who had surgery required intensive care management.
There were 751 total radiologic studies performed (average, 5.5 per patient), which detected only 47 inju- ries (6.3%) (Table 1). Plain radio- graphs accounted for 80% of the studies and identified 37 injuries (6% positive). Sixty-one computed tomo- grains (CTs) of the head were done, which demonstrated ten minor de- fects. In addition, 47 negative ab- dominal CT scans, six negative an- giographic studies, and seven nega- tive IV urograms were also obtained. Laboratory and other diagnostic tests performed on these patients are lis- ted (Table 2).
Patients were coded into 44 differ- ent DRGs by the hospital based on
the greatest potential for remunera- tion. The most common DRG cate- gories are shown (Table 3). One hun- dred s ixteen pa t ien ts were inl iers (85%), and 20 were outliers (12 low trim, 9%; two high trim, 1%; five one-day stay, 4%; one transferred).
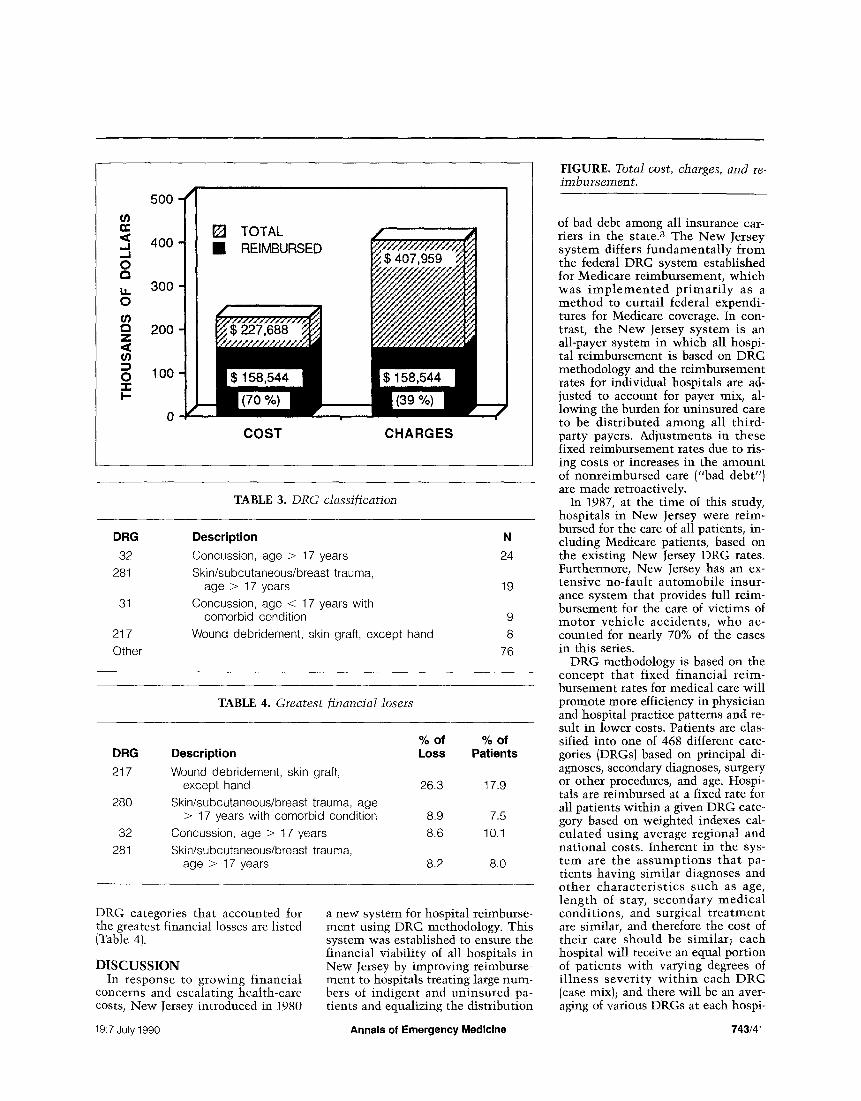
Re imbursement was equal to or more than cost for 48 patients (35%) and was equal to or more than stan- dard charges for only one pa t i en t (1%). Total financial loss or negative contribution margin (cost minus re- imbursement) for these 136 patients was $69,144 (average, $508 per pa- tient), whereas total loss of potential revenue (charges minus reimburse- ment) was $249,414 (average, $1,834 per patient) (Figure). When evaluated by individual DRG code, 32 of 44 DRGs (73%) were financial losers (versus cost), and all but one were potential revenue losers (99%). The
40/742 Annals of Emergency Medicine 19:7 July 1990
,.,I .,,,J 0
14. 0 U) Z
0 "I- I--
500 -
400 -
300
200
1 O0
i
[] TOTAL REIMBURSED
COST CHARGES
TABLE 3. DRG classification
DRG
32
281
31
217
Other
Description
Concussion, age > 17 years
Skin/subcutaneous/breast trauma, age > 17 years
Concussion, age < 17 years with comorbid condition
Wound debridement, skin graft, except hand
N
24
19
9
8
76
TABLE 4. Greatest financial losers
DRG
217
280
32
281
% o f Description Loss
Wound debridement, skin graft, except hand 26.3
Skin/subcutaneous/breast trauma, age > 17 years with comorbid condition 8.9
Concussion, age > 17 years 8.6
Skin/subcutaneous/breast trauma, age > 17 years 8.2
% o f Patients
17.9
7.5
10.1
8.0
DRG categories that accounted for the greatest financial losses are listed (Table 4).
DISCUSSION In response to growing financial
concerns and escalating health-care costs, New Jersey introduced in 1980
a new system for hospital reimburse- ment using DRG methodology. This system was established to ensure the financial viability of all hospitals in New Jersey by improving reimburse- ment to hospitals treating large num- bers of indigent and uninsured pa- tients and equalizing the distribution
FIGURE. Total cost, charges, and re- im bursement.
of bad debt among all insurance car- riers in the state. 3 The New Jersey system differs fundamentally from the federal DRG system established for Medicare reimbursement, which was imp lemen ted pr imar i ly as a method to curtail federal expendi- tures for Medicare coverage. In con- trast, the New Jersey system is an all-payer system in which all hospi- tal reimbursement is based on DRG methodology and the reimbursement rates for individual hospitals are ad- justed to account for payer mix, al- lowing the burden for uninsured care to be distributed among all third- party payers. Adjustments in these fixed reimbursement rates due to ris- ing costs or increases in the amount of nonreimbursed care ("bad debt") are made retroactively.
In 1987, at the time of this study, hospitals in New Jersey were reim- bursed for the care of all patients, in- cluding Medicare patients, based on the existing New Jersey DRG rates. Furthermore, New Jersey has an ex- tensive no-fault automobile insur- ance system that provides full reim- bursement for the care of victims of motor vehicle accidents, who ac- counted for nearly 70% of the cases in this series.
DRG methodology is based on the concept that fixed financial reim- bursement rates for medical care will promote more efficiency in physician and hospital practice patterns and re- sult in lower costs. Patients are clas- sified into one of 468 different cate- gories (DRGs) based on principal di- agnoses, secondary diagnoses, surgery or other procedures, and age. Hospi- tals are reimbursed at a fixed rate for all patients within a given DRG cate- gory based on weighted indexes cal- culated using average regional and national costs. Inherent in the sys- tem are the assumptions that pa- tients having similar diagnoses and other characterist ics such as age, length of stay, secondary medical conditions, and surgical t reatment are similar, and therefore the cost of their care should be similar; each hospital will receive an equal portion of patients with varying degrees of illness severity wi th in each DRG (case mix); and there will be an aver- aging of various DRGs at each hospi-
19:7 July 1990 Annals of Emergency Medicine 743/41

TRAUMA WORKUP Flancbaum et al
tal ("referral patterns").~, ~5 N u m e r o u s methodologic flaws in
the DRG system have been identi- fied. 16-19 For e x a m p l e , h o s p i t a l s treating large numbers of uncompli- cated pat ients wi th in a given DRG might enjoy a substantial profit mar- gin as compared with hospitals treat- ing more complicated cases, which consume greater resources. The case mix of pat ients t reated in various hospitals might be further altered if tertiary-care hospitals were forced to accept large numbers of complicated cases t h a t were t r ans fe r r ed f r o m smaller hospitals to avoid financial losses (altering referral patterns). In addition, others have criticized DRG methodology for significant clinical overlap among various DRG catego- ries and for a lack of staging for acu- ity and severity of illness.
The New Jersey DRG system ad- dressed the issue of case mix by cate- gorizing all hospitals as either major teaching facilities with a full comple- ment of residency training programs, m i n o r t e a c h i n g h o s p i t a l s w i t h a smaller n u m b e r of res idency posi- tions, or nonteaching hospitals with no res idency programs. The major teaching hospitals are reimbursed at a higher rate to compensate for the higher overhead expenses associated with maintaining their training pro- grams and because they are expected to treat the greatest percentage of complex cases within each DRG cat- egory. To date, the issues of clinical overlap and indexing for severity of illness wi~thin the DRG system have not been addressed nor is any special consideration given to Level I trauma centers in the New Jersey system.
Recent ly , considerable a t t en t ion has been focused on the potential ad- verse effects of DRG reimbursement for t rauma care. It is now well docu- mented that the implementa t ion of reg iona l i zed t r a u m a care sy s t e m s that concentrate critically ill and in- jured patients in a few highly quali- f ied i n s t i t u t i o n s (Level I and II t rauma centers) is associated with a reduction in the number of prevent- able deaths.i, 2 Several authors have demonstrated that widespread adop- tion of an all-payer fixed-reimburse- ment system similar to DRGs would not adequately reimburse for t rauma care in Level I centers and have em- phasized the fact that the greatest fi- nancial losers were the most severely injured patients. 3-12
Schwab et al reported that reim- bursement for the care of t rauma pa- t i e n t s a d m i t t e d to t h e i r Level I t r auma center ICU averaged more than $3,500 less than the cost of car- ing for those patients. 9 All ISS groups in their study were financial losers, a l though losses increased wi th in- creasing injury severity. DeMaria et al concluded that projected DRG re- imbursement for the t reatment of el- derly t rauma patients (more than 65 years of age) failed to meet hospital costs and showed that there was no correlation between hospital cost and p r o j e c t e d D R G r e i m b u r s e m e n t . 7 These studies suggested that mod- ifications in the DRG system, such as indexing for severity or the intro- duct ion of other "identifiers," were necessary to prevent a s i tuat ion in which the financial disincentives re- su l t ing f rom the care of these pa- tients might jeopardize the future of regionalized t rauma systems.
In contrast to previous studies that focused on severely injured patients, this study analyzed the financial im- pact on our hospital of DRG reim- b u r s e m e n t for the care of pat ients who were s u b s e q u e n t l y shown to have only minor injuries. This group of pat ients was specifically selected because the DRG me thodo logy as- sumes that the case mix of patients within each DRG category will aver- age out so that the opportunity exists for the hospital to realize a profit.
For t r a u m a pat ients , one wou ld logical ly assume that it would be those patients with minimal injuries, w h o r e q u i r e less t r e a t m e n t and shor ter hospi ta l stays, who should generate that profit. All of the pa- tients in this study had an ISS of 9 or less, with no single component hav- ing an AIS of more than 2. All pa- tients were evaluated and treated in accordance with established institu- tional protocols based on guidelines out l ined in the ATLS course of the American College of Surgeons' Com- m i t t e e on T r a u m a . 13 D i a g n o s t i c workups were comprehens ive , yet appropriate, to exclude serious occult injuries and, by definition, identified only minor injuries in these patients.
One migh t argue that too m a n y tests were per formed in these pa- tients, that more reliance on clinical findings and better clinical judgment cou ld have avo ided a s i gn i f i c an t number of negative studies, and that this, in fact, is one major goal of the
DRG re imbursement system. How- ever, numerous reports document ing the inaccuracy of clinical signs in evaluat ing vic t ims of blunt t rauma n o w exist, va l ida t ing the c o n c e p t that a thorough diagnostic workup is necessary to avoid miss ing poten- t ia l ly lethal occu l t injuries and to l i m i t the n u m b e r of p r e v e n t a b l e deaths. 1,2,2o,21
Most of the patients in this study were inliers (85%) or low-t r im out- liers (9%). Only two pat ients were high-trim outliers, indicating that in- efficiency within the system was not a major confounding variable. Nev- ertheless, r e i m b u r s e m e n t failed to meet costs in the majori ty of DRG categories (73%)and patients (65%). When reimbursement was compared with hospital charges, 98% of DRGs and 99% of patients were losers. The aggregate financial loss was $69,144 ($508 per patient), and the total loss of po ten t ia l revenue was $249,414 ($1,834 per patient).
While the sample size in this study was relatively small, the data suggest tha t the al l-payer DRG sys t em in New Jersey inadequately reimburses hospitals for the care of those trauma pat ients who are u l t ima te ly deter- mined to have only minor injuries. This is par t icu lar ly impor t an t be- cause the patients reported here (ISS
9, AIS < 3) are not those for w h o m t rea tment in a Level I or II t rauma center is necessary or recommended but rather are those who should be able to be properly cared for in any hospital. L3
C O N C L U S I O N The cost of appropriate diagnostic
evaluat ion and t rea tment of t rauma patients who are subsequently deter- mined to have only minor injuries exceeds the current DRG reimburse- men t in the majori ty of cases. The New Jersey DRG reimbursement sys- tem in its present form discourages, from a financial perspective, the per- formance of a thorough negative di- agnostic workup in t rauma patients.
Modificat ions i n DRG reimburse- ment methodology are clearly neces- sary to enable all hospitals to provide appropriate care to injured patients wi thout financial penalty. Failure to do so could ul t imately deny patients the benefits of recent advances in the diagnosis and t r e a t m e n t of poten- tially lethal injuries and adversely af- fect the future of t rauma care in the
42/744 Annals of Emergency Medicine 19:7 July 1990

United States.
REFERENCES 1. Cales RH, Trunkey DD: Preventable trauma deaths, lAMA 1985;254:1059-1063.
2. Krcis DJ Jr, Plasencia G, Augenstein D, et ah preventable trauma deaths: Dade County, Flor- ida. J Trauma 1986;26:649-654.
3. Sapolsky HM: An evaluation of the New Jer- sey DRG hospital payment system. N] Med 1988i85:32-37.
4. Jacobs LM, Schwartz RJ: The impact of pro~ spective re imbursement on trauma centers. Arch Surg 1986;121:479-483.
5. Kreis DJ Jr, Augenstein D, Civctta JM, et ah Diagnosis-related groups and the salvagable trauma patient in the intensive care unit. Surg Gyneco] Obstet 1986;163:539-542.
6. Kreis DI Jr, Augenstem D, Civetta JM, etal : Diagnosis related groups and the critically in- jured. Surg Gynecol Obstet 1987;165:317-322.
7. DeMaria EJ, Merriam MA, Casanova LA, et ah Do DRG payments adequately reimburse the costs of t rauma care in geriatric patients? /
Trauma 1988;28:1244-1249.
8. Pories SE, Gamelli RL, Vacek P, et ah Pre- dicting hospital charges for trauma care. Arch Surg 1988;123:579-582.
9. Schwab CW, Young G, Civil I, et ah DRG re- imbursement for tramna: The demise of the trauma center {the use of ISS grouping as an early predictor of total hospital cost). ] Trauma 1988;28:939-946.
10. Thomas F, Clemmer TP, Larsen KG, et al: The economic impact of DRG payment policies on air-evacuated trauma patients. J Trauma 1988;28:446-451.
11. Bondurant FJ, Cotler HB, Buckle R, e t a l : The medical and economic impact of severely injured lower extremities. J Trauma 1988;28: 1270d273.
12. Cone JB, Eisner JA: Econonrics of trauma in a small academic medical center. South Med ] 1989;82:23-25.
13. American College of Surgeons, Committee on Trauma: Advanced Trauma Life Suppor~ Fro- gram. Chicago, ACS, 1989.
14. American College of Surgeons: Hospital
Trauma Index. Bull Am Coil Surg 1980;65: 32-33.
15. Munoz E, Regan DM, Margolis IB, et ah Surginomics: Prospective payment systems and the surgeon. Curt Surg 1986;43:4-20.
16. Iezzoni LI, Moskowitz MA: Clinical overlap among medical diagnosis related groups. JAMA 1986;255:927-929.
17. Gonnella JS: Case mix classification: The need to reduce inappropriate homogeneity (edi- torial). ]AMA 1986;255:941-942.
18. Gonnella JS, Hornbrook MC, Louis DZ: Staging of disease: A case mix measurement. lAMA 1984;251:637-644.
19. Zook CJ, Moore FD: High cost users of med- ical care. N Engl J Med 1980;302:996-1002.
20. Rodriguez A, DuPriest RW, Shatney CH: Recognition of intra-abdominal injury in blunt trauma victims: A prospective study comparing physical examination with peritoneal lavage. Am Surg 1982;48:456-459.
21. Trooskin SZ, Boyarsky AH, Grcco RS: Pori toneal lavage in patients with normal menta- tion and hematuria after blunt trauma. Surg Gy- necoI Obstet 1985;160:145-147.
19:7 July 1990 Annals of Emergency Medicine 745/43