Embed Size (px)
Citation preview

Driving Knowledge Generation
What Does It Take?
James E. Tcheng, MD Professor of Medicine, Professor of
Community and Family Medicine (Informatics) IOM Digital Learning Collaborative
April 16th, 2013
2
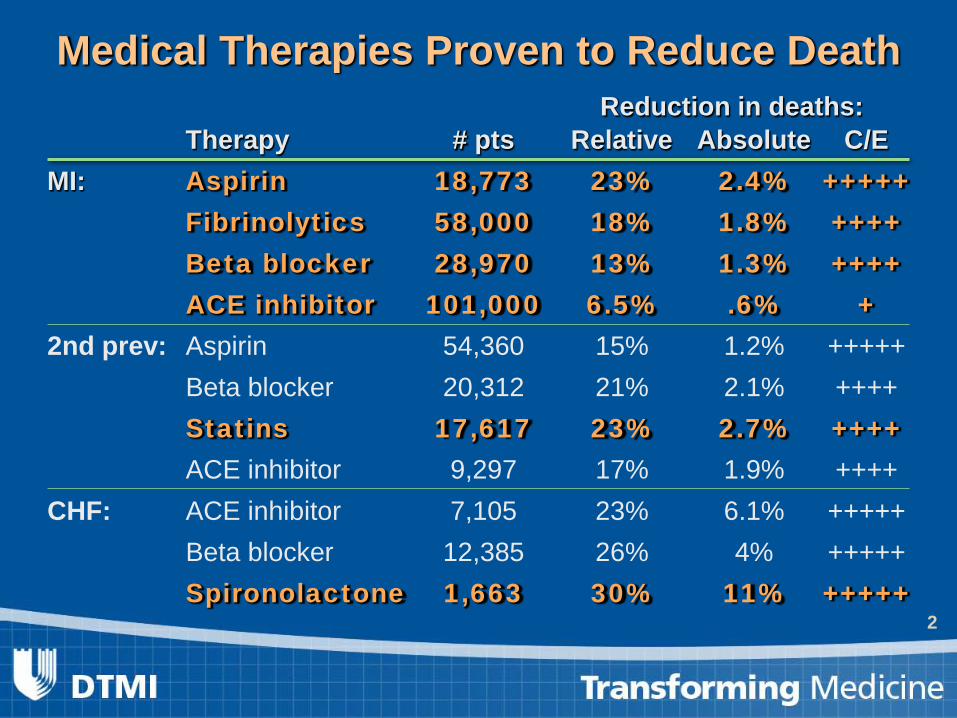
Medical Therapies Proven to Reduce Death Reduction in deaths: Therapy # pts Relative Absolute C/E MI: Aspirin 18,773 23% 2.4% +++++ Fibrinolytics 58,000 18% 1.8% ++++ Beta blocker 28,970 13% 1.3% ++++ ACE inhibitor 101,000 6.5% .6% + 2nd prev: Aspirin 54,360 15% 1.2% +++++ Beta blocker 20,312 21% 2.1% ++++ Statins 17,617 23% 2.7% ++++ ACE inhibitor 9,297 17% 1.9% ++++ CHF: ACE inhibitor 7,105 23% 6.1% +++++ Beta blocker 12,385 26% 4% +++++ Spironolactone 1,663 30% 11% +++++

3
The Cycle of Quality: Generating Evidence to Inform Policy
Califf RM et al, Health Affairs, 2007
Measurement and
Education
Early Translational
Steps
Clinical Trials
Clinical Practice
Guidelines Performance
Measures
Outcomes
Discovery Science
Data Standards Network
Information
Empirical Ethics
Priorities and Processes
Inclusiveness
Use for Feedback
on Priorities
Conflict-of-interest Management
Evaluation of Speed and Fluency
Pay for Performance
Transparency to Consumers
FDA Critical Path
NIH Roadmap 1 2 3
4
5
6
7
8
9 10
11
12
4
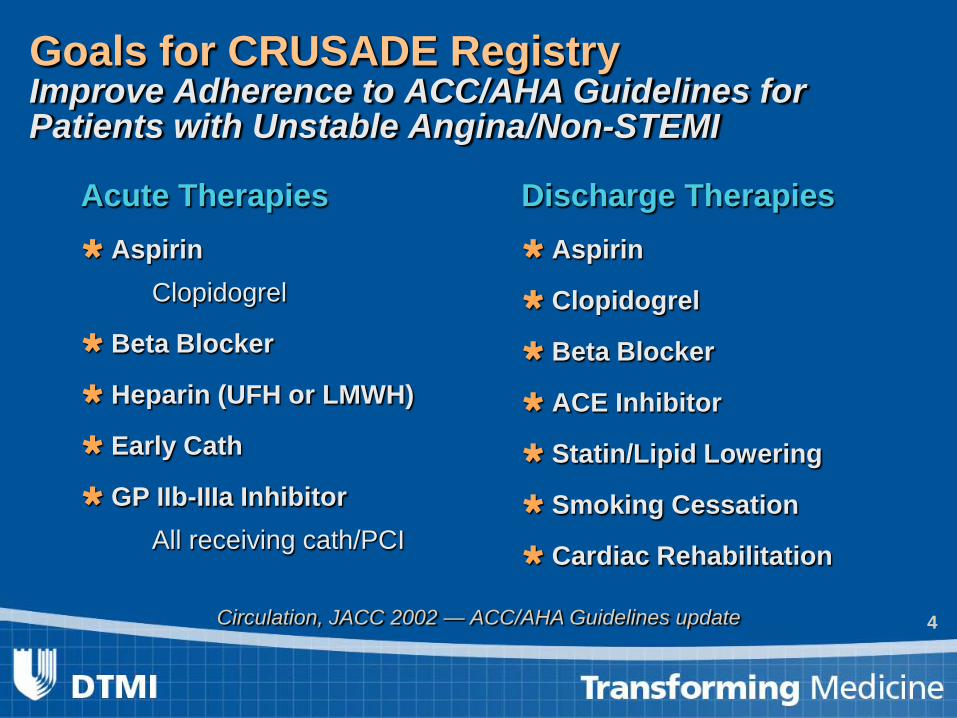
Goals for CRUSADE Registry Improve Adherence to ACC/AHA Guidelines for Patients with Unstable Angina/Non-STEMI
Acute Therapies Aspirin
Clopidogrel
Beta Blocker
Heparin (UFH or LMWH)
Early Cath
GP IIb-IIIa Inhibitor All receiving cath/PCI
Discharge Therapies Aspirin
Clopidogrel
Beta Blocker
ACE Inhibitor
Statin/Lipid Lowering
Smoking Cessation
Cardiac Rehabilitation
Circulation, JACC 2002 — ACC/AHA Guidelines update
5
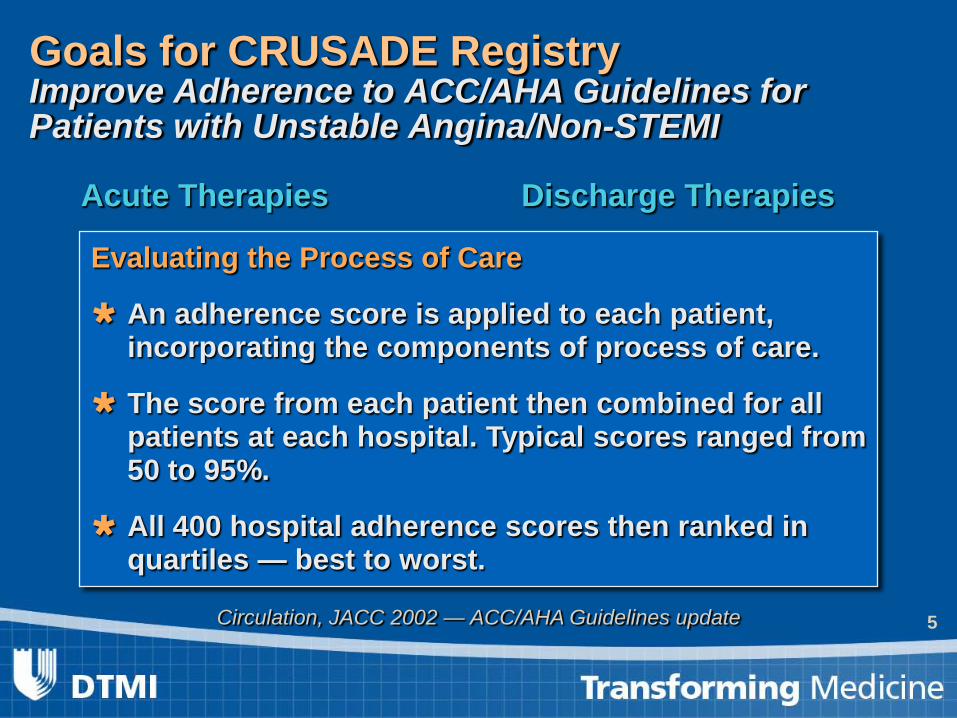
Goals for CRUSADE Registry Improve Adherence to ACC/AHA Guidelines for Patients with Unstable Angina/Non-STEMI
Acute Therapies Aspirin
Clopidogrel
Beta Blocker
Heparin (UFH or LMWH)
Early Cath
GP IIb-IIIa Inhibitor All receiving cath/PCI
Discharge Therapies Aspirin
Clopidogrel
Beta Blocker
ACE Inhibitor
Statin/Lipid Lowering
Smoking Cessation
Cardiac Rehabilitation
Circulation, JACC 2002 — ACC/AHA Guidelines update
Evaluating the Process of Care
An adherence score is applied to each patient, incorporating the components of process of care.
The score from each patient then combined for all patients at each hospital. Typical scores ranged from 50 to 95%.
All 400 hospital adherence scores then ranked in quartiles — best to worst.

6 Peterson et al, ACC 2004
Link Between Overall ACC/AHA Guidelines Adherence and Mortality
Every 10% ↑ in guidelines adherence → 11% ↓ in mortality
Electronic Health Records are the Obvious Transforming Factor
• Record every health transaction and use the information to improve quality, service and decision making
• Every major business in the US already does this using sophisticated decision support, and increasingly RCTs
• Seems simple

Duke’s Vision of the Data Mart

A partnership between Duke Medicine and the Durham community that seeks to improve the health status of Durham County residents.
In 2009, DHI funded 10 planning teams to
find ways to reduce death or disability from specific diseases or disorders prevalent in the community.

Sample Health Application: Preventing Lead Exposure

DM patients, no HbA1C (3434, 24%) DM patients, w/ HbA1C (10,811, 76%)
HbA1C < 7 (5817, 54%) 7 < HbA1C < 9 (3279, 30%)
HbA1C > 9 (1715, 16%)

Missing data
monthly data extract + risk algorithms
Lower intensity Higher intensity Intervention Spectrum
Medical-Social Risk Phenotypes
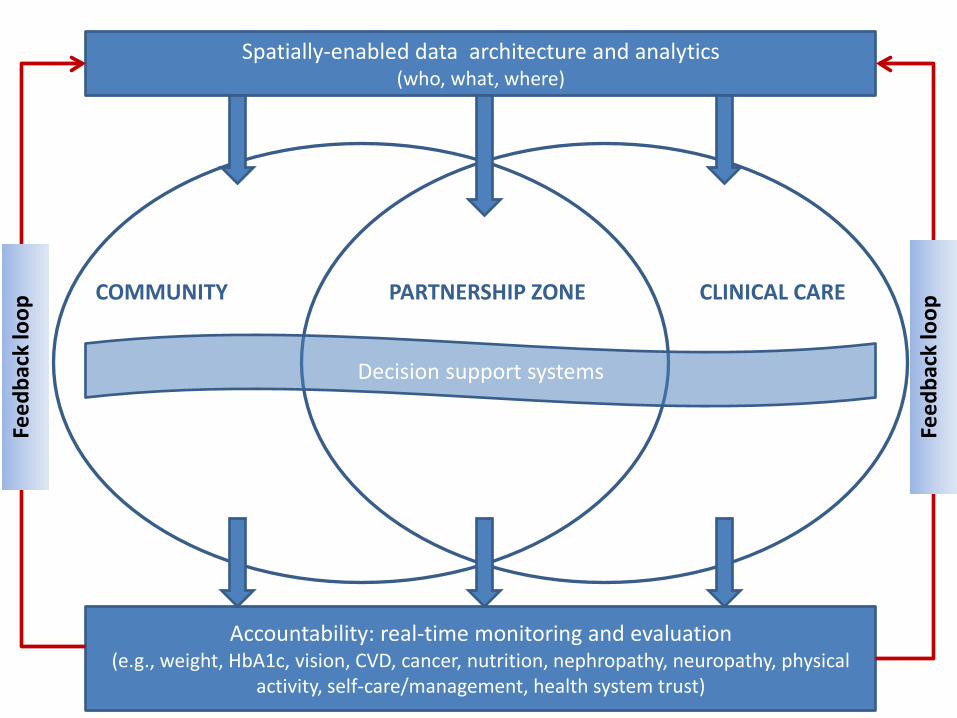
Spatially-enabled data architecture and analytics (who, what, where)
COMMUNITY PARTNERSHIP ZONE CLINICAL CARE
Accountability: real-time monitoring and evaluation (e.g., weight, HbA1c, vision, CVD, cancer, nutrition, nephropathy, neuropathy, physical
activity, self-care/management, health system trust)
Decision support systems
Feed
back
loop
Feed
back
loop
14
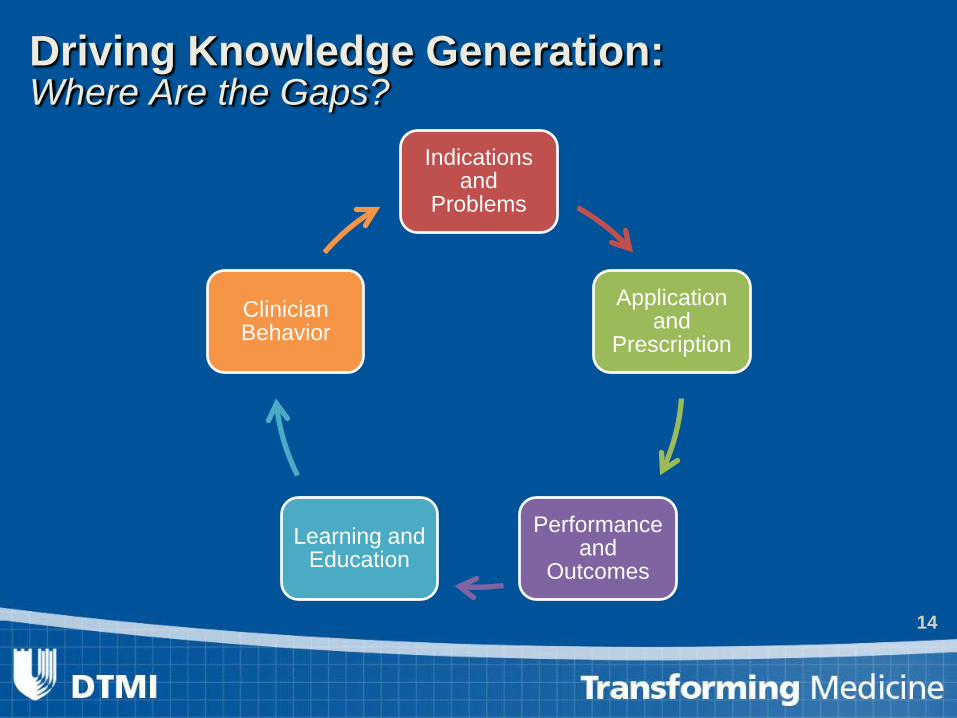
Driving Knowledge Generation: Where Are the Gaps?
Indications and
Problems
Application and
Prescription
Performance and
Outcomes Learning and
Education
Clinician Behavior

Integrated at “enterprise level”
Disease Registries—Granular, Detailed Primary
Care Cancer Mental Health
Cardio vascular Etc…
Health System A
Health System B
Etc…
ElectronicHealth Records
Adaptable to all!
Fundamental Informatics Infrastructure-Matrix Organizational Structure

What Is a Registry?
Data elements and definitions
Quality Assessment
Clinical Research
Quality Improvement
Clinical Data Observational
Database
Bufalino VJ et al. Circulation. 2011;123:2167-2179

That was then...
Launched 1998 1 Registry Focused on quality measurement / support local QI
This is now... 7 National Programs More than 2,500 hospitals and 1000 practices
Health plans, state and government adoptions >12 societal partners
>150 publications
FDA uses NCDR data for post market surveillance
This is our future…
Integrated programs
Point of care tool(s) to support needs of clinicians/hospitals (e.g. quality reporting)
EHR Integration / Structured reporting/ Meaningful use
Support MOC / MOL / LLL
International collaborations
Platform for clinical trials and CER; and FDA / CMS : post market, coverage with evidence

Maintenance of
Certification
Performance Improvement -
CME Value Based Purchasing
Physician Quality
Reporting System
Benchmarking • Appropriate Use
Criteria • Guideline
Adherence • Hospital and
Physician Level Performance Measures
What if…?
19
THE ESSENTIAL ISSUE The “Tower of Babel” of data from databases,
literature, and clinical trials: without controlled vocabulary and data standards we are lost!

Technical • EHR consistency
– Interfaces, standardized data, data access • Controlled terminologies
– >350 biomedical ontologies (NCBO) – Still lacking depth, specificity
• Workflow integration, usability – Lack of best practice
• Health Information Technology – Does not improve (physician) efficiency
The Impediments …

Policy / Culture • High value targets only?
– Data requires resources – What about needles in the haystack?
• Linking patient data – Registry contracts, HIPAA
• Clinician culture – Speed over data (pen, dictation) – Richness of language – E&M coding / remuneration / incentives
• Patient engagement?
The Impediments …





























