Embed Size (px)
Citation preview

Drug Pricing, Repricing,
Rebates, and Patient
Access
Jack Hoadley, Ph.D.Health Policy Institute, Georgetown University
Bipartisan Policy Center
April 13, 2016
1

Credits and Notes
Some of my drug policy research has
been done under contract with the Kaiser
Family Foundation
Find links to full reports:
hpi.georgetown.edu/medicarepartd
Thanks to Kaiser Family Foundation and
the Medicare Payment Advisory
Commission for use of their slides2

Outline
Background basics
How are drugs priced?
Who gets what rebate?
How are drugs re-priced over time?
Do payer actions affect patient access
Looking to the future
3

Background
Drug spending trends
Brands, generics, and specialty drugs
Components of the drug supply chain
Flow of dollars for drug purchases
Drug pricing terminology and definitions
4

Drug Spending Growth, 1970s-2024
7%
12%
10%
15%14%
13%
11%
8%
5%
8%
4%
2%
4%
-1%
2%
-1%
2%
11%
10%
4%
5% 5% 5% 6% 6% 6% 6% 6%
19
70
s
19
80
s
19
90
s
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
20
12
20
13
20
14
20
15
20
16
20
17
20
18
20
19
20
20
20
21
20
22
20
23
20
24
Prescription (Actual) Prescription (Projected)
Total Health (Actual) Total Health (Projected)
NOTE: Average annual growth rate of prescription drug spending per capita for 1970’s – 1990’s; annual change in actual prescription drug
spending per capita 2000 – 2014 and projected prescription drug spending per capita 2015 – 2024. 2014 to 2015 percent changes are calculated
using 2014 actual and 2015 projected amounts.
SOURCE: Kaiser Family Foundation analysis of National Health Expenditure (NHE) Historical (1960-2014) and Projected (2014-2024) data from
Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group (Accessed on December 7, 2015)
Average annual growth per capita, actual and projected
5

Drug Spending as Share of Health
Retail drug spending = all spending at outlets
that directly serve patients
1965-2015: as low as 6% of health spending versus
12% today
Non-retail drug spending = spending by medical
providers for drugs they provide to patients
Inpatient hospital, outpatient hospital, physicians’
offices, infusion centers
2009-2015: about 4-5% of health spending
Combined retail and non-retail drug spending:
2015: 17% of spending on personal health services6
SOURCE: DHHS/ASPE, Observations on Trends in Prescription Drug Spending March 2016. Based on data from DHHS National Health
Expenditure Accounts and the Altarum Institute.

76%
23%
75%
20%
72%
16%
71%
14%
72%
12%
Brand Versus Generic Drugs, 2010-2014
SOURCE: IMS Institute for Healthcare Informatics, Medicines Use and Spending Shifts: A Review of the Use of Medicines in the U.S. in 2014
Share of Dispensed Prescriptions: Brand DrugsShare of Spending: Brand Drugs
2010 2011 2012 2013 2014 2010 2011 2012 2013 2014
1998 brand share of
prescriptions = 49%
7

Specialty versus Traditional Drugs
No universal definition
Characteristics tend to include:
Expensive (at least $600/month for Part D)
Manufactured in living systems (biologicals)
Difficult to administer; may be injected or infused
Prescribed by specialist physicians
May require complex patient follow-up, monitoring
Used to treat serious conditions for which few or
no alternative therapies available
Administered through specialty pharmacies
Require special handling (temperature control) 8

24%25%
28%30%
33%
Spending on Specialty Drugs, 2010-2014
SOURCE: IMS Institute for Healthcare Informatics, Medicines Use and Spending Shifts: A Review of the Use of Medicines in the U.S. in 2014
2010 2011 2012 2013 2014
As Share of Total Spending
9

Supply Chain for Drug Delivery
Manufacturers
Wholesalers
Retail Pharmacies
Chain
Pharmacies
and Food
Stores with
Pharmacies
Independent
Pharmacies
Mail-Order
Pharmacies
Consumers
Consumers Who Have Some or All Purchases Paid for by a
Third Party (Including health plans and public-sector programs)
Hospitals, HMOs,
Clinics, Home Health
Care Providers,
Nursing Homes, and
Federal Facilities
Nonretail Providers
Consumers Paying for
Purchases Out of
Source: Congressional Budget Office, Prescription Drug Pricing in the Private Sector, 200710

Supply Chain Functions Manufacturers
Develop, produce, and market drugs
Set list prices as a basis for price negotiations
Negotiate rebates and discounts with plans or PBMs
Wholesalers Link manufacturers with outlets that dispense drugs
Help smaller pharmacies negotiate with generic manufacturers
Pharmacies Stock drugs and fill prescriptions on demand
Negotiate discounts with generic drug manufacturers
Pharmacy Benefit Managers (PBMs) Administer drug benefit for health plan or employer
Build pharmacy networks
Negotiate rebates with manufacturers 11

Supply Chain Market Shares
Mail Order
Food Stores
Chain
Pharmacies
Independent
Pharmacies
ClinicsRetail
Pharmacies
Hospitals
Long Term
Care
Other
Source: IMS Institute for Healthcare Informatics, Medicines Use and Spending Shifts: A Review of the Use of
Medicines in the U.S. in 2014
By non-discounted spending, 2014
12

Drug Spending by Payer, 1960-2024
SOURCE: MedPAC analysis of historical and projected data from CMS’s national health expenditure accounts as of July 2015.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
19
60
19
62
19
64
19
66
19
68
19
70
19
72
19
74
19
76
19
78
19
80
19
82
19
84
19
86
19
88
19
90
19
92
19
94
19
96
19
98
20
00
20
02
20
04
20
06
20
08
20
10
20
12
20
14
20
16
20
18
20
20
20
22
20
24
Out of pocket
Private health insurance
Medicare
Medicaid
Other
Start of
Medicare
Part D
Projected
13

Source: Congressional Budget Office, Prescription Drug Pricing in the Private Sector, 2007
Flow of Funds for a Brand Drug
Negotiated Rebate for
Brand-Name Drugs
Preferred
Placement on
Formulary
Copayment
Drugs
Premium
Drug Coverage
Premium
Share of Rebates
from Manufacturer
Managed
Drug
BenefitsPayment
WAC
DrugsDrug
Manufacturer
Pharmacy Benefit
ManagerPharmacy
Health Plan Beneficiary
Wholesaler
Employer
Flow of Funds
Flow of Prescription Drugs
Services
AMP
Drugs
Note: AMP = average manufacturer price; WAC = wholesale acquisition cost
Negotiated
Payment
14

Source: Congressional Budget Office, Prescription Drug Pricing in the Private Sector, 2007
Pricing for a Brand Drug
$80 (Adjusted AMP)
$83 (Average price paid by
independent pharmacies)
Wholesaler
(Retains $3)
Independent Pharmacy
(Retains $5)
Pharmacy Benefit Manager
(Has a net cost of $82)
$88 Payment $6 Rebated from
Manufacturer
$88 (based on 15% discount
off AWP of $101, plus $2 fee)
Drug Manufacturer
(Receives net payment of $74)
$80 Payment $6 Rebate to PBM
15

How Are Drugs Priced?
What is the “price”?
Pricing rationales
Factors influencing pricing
Price variation by payer
16

What is the Price of a Drug?
List prices AWP = average wholesale price, defined as the published list
price that wholesalers post for retailers and other providers
WAC = wholesale acquisition cost, defined as list prices posted by manufacturers
Price measures calculated by the government AMP = average manufacturer price, defined as the average of
prices actually paid by wholesalers and retailers who buy directly from manufacturers
ASP = average sales price, defined as the average price realized by manufacturers for sales to all purchasers net of rebates, discounts, and price concessions
Discounts Retail discounts = discounts available to large-volume retailers
on purchases from wholesalers or manufacturers
Manufacturer rebate = amounts paid by manufacturer to health plan or PBM to create a discount price
17

Rationales for Launch Prices
Lack of transparency
Cost of research & development
Industry estimate: $2.6 billion for an average drug Source: J. DiMasi et al, Innovation in the pharmaceutical industry: New estimates of
R&D costs, Journal of Health Economics May 2016. Tufts Center for the Study of
Drug Development
Savings accrued for the health care system
as a result of taking the new drug
Presence and pricing of competing therapies
Strategic positioning relative to products on
the market or coming soon18

Drug Discovery, Development and Review
SOURCE: Adapted by MedPAC from Pharmaceutical Research and Manufacturers of America.
Drug discovery and
preclinical studiesFDA
review
Post-marketing
studies and
surveillance
Fo
od
an
d D
rug A
dm
inis
tration a
ppro
va
l
Basic
researchClinical trials
Phase I Phase II
20 –100 healthy volunteers
100 – 500 volunteers with the condition
1,000 – 5,000 volunteers with the condition
5,000 – 10,000 compounds narrowed
down to ~2501 approved
drug
6 – 7 years3 - 6 years
Phase IV
1.5 years
Inve
stiga
tio
na
l N
ew
Dru
g a
pp
lica
tion su
bm
itte
d
New
Dru
g A
pp
lica
tio
n / B
iolo
gic
s L
icen
se
Ap
plic
ation s
ub
mitte
d
5 compounds
Phase III
19

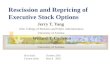
Price of Oncology Drugs per Life-Year Gained
SOURCE: David Howard, Peter Bach, Ernst Berndt, and Rena Conti, “Pricing in the Market for Anticancer Drugs,” Journal of Economic
Perspectives, vol. 29, no. 1 (Winter 2015): 139-162.
20

Supply-Side Factors Influencing Prices
Increasing complexity of biopharmaceuticals
Emphasis on treatments for small disease
populations (e.g., orphan drugs), often with few
competing therapies
Patents and temporary monopolies granted by
the government
Consolidation within biopharmaceutical industry
Changes in the drug supply chain
21

Demand-Side Factors Influencing Prices
Shift from out-pocket purchases by
consumers to a third-party payment system
Shift from private to public insurance
Consolidation in the insurance industry
Discounts and rebates mandated by law
(Medicaid, VA, DOD, 340B program)
Increased demand as the population ages
22

Who Gets What Rebate?
Factors influencing rebates
Trends over time
Public-sector rebates
23

Factors Influencing Rebates
Proprietary
Ability of a payer to grow market share for the
manufacturer’s drug
Ability of a payer to move market share
Encouraging use of one manufacturer’s drug over
competing therapies
24

Tools Payers Use in Negotiating Rebates
Formulary management tools
Exclusion of competing drugs from the formulary
Preferential tier placement on the formulary, with
lower cost sharing for the consumer
Utilization management tools, such as prior
authorization, for competing drugs
Other factors
Evidence of comparative effectiveness or clinical
preferences
Access to needed drugs for plan members
Marketing considerations
25

11%
15%17%
33%
Estimated Rebate Amounts
* Refers to the top 53 therapeutic classes of drugs, which accounted for 70 percent of Part D spending in 2010
SOURCE: Adapted from Congressional Budget Office, Competition and the Cost of Medicare’s Prescription Drug
Program, July 30, 2014
Share of Total Drug Spend (2010)
Share of Brand Drug Spend (2010)
Share of Brand Drug Spend for
Top Classes* (2010)
Illustrative Rebate for Drug with Competition
26
As Percentage of Drug Costs by Category

8.6% 9.6% 10.4% 11.1% 11.3% 11.5% 11.7%12.9%
14.4%16.6% 16.8% 16.8% 16.8% 16.8% 16.8%
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Trends in Medicare Part D Rebates, 2006-20
SOURCE: Medicare Trustees Report, 2015
As Percentage of Total Drug Costs
27
Projected

How Are Drugs Re-Priced?
Interaction of price and utilization
Price trends over time
Factors driving price changes for generics
Impact of generic substitution
Factors driving price changes for brand
drugs, including specialty drugs
28

Growth in Drug Prices and Utilization
SOURCE: Kaiser Family Foundation analysis of Bureau of Economic Analysis data
Annual percent change in price and quantity indexes of pharmaceutical
and other medical products, index numbers 2009=100
0%
2%
4%
6%
8%
10%
12%
14%
Price Index Quantity Index
29

2.0% 1.9%
6.8%3.2%
-2.1%
11.0%
5.2%
-0.1%
17.7%
All Drugs Traditional Drugs Specialty Drugs
Unit Cost
Utilization
SOURCE: Express Scripts 2015 Drug Trend Report
Components of Drug Spending Trend, All Payers,
2015 versus 2014
30

Peterson-Kaiser Health System Tracker
Source: IMS Institute for Healthcare Informatics. Medicines Use and Spending Shifts: A Review of the Use of Medicines in the U.S. in 2014.
Components of Drug Spending Growth, 2010-2014
Contribution to growth in drug spending, by spending growth drivers, in billions, 2010 -2014
$10.4 $7.2 $8.5 $5.7 $9.5
$4.6 $6.4 $5.7 $6.5
$20.2$16.6 $17.9 $15.6 $20.3
$26.3
-$1.4 -$4.2 -$2.9 -$2.1 -$0.7-$14.7 -$14.3
-$29.3-$19.6
-$11.9
-$40
-$30
-$20
-$10
$0
$10
$20
$30
$40
$50
$60
$70
2010 2011 2012 2013 2014
Generics New Brands Protected Brands Price
Protected Brands Volume Patent Expirations
31

Medicare Part D Drug Price Trends, by
Brand-Generic-Biological Status, 2006-2013
15%
32
2.29
2.14
0.30
1.47
0.0
0.5
1.0
1.5
2.0
Generic drugs
All Part D covered drugs
Single source
brand name
Biologics*
Dru
g p
ric
e in
de
x e
qu
alto
1.0
at
the s
tart
of
the P
art
D p
rog
ram
NOTE: Chain-weighted Fisher price indexes.
* The shift in biologics price index in October 2012 is due in part to a change in how prescription quantifies were reported for Avonex.
SOURCE: Adapted from MedPAC, Report to the Congress: Medicare Payment Policy, March 2016, Figure 13-8 (Acumen LLC analysis for MedPAC)

Part D Drug Price Trends, with Effects of
Generic Substitution, 2006-2013
15%
33NOTE: Chain-weighted Fisher price indexes.
SOURCE: Adapted from MedPAC, Report to the Congress: Medicare Payment Policy, March 2016, Figure 13-7 (Acumen LLC analysis for MedPAC)
1.47
1.02
0.70
0.80
0.90
1.00
1.10
1.20
1.30
1.40
1.50
All drugs and biologics
All drugs and biologics accounting
for generic substitution
Dru
g p
ric
e in
de
x e
qu
al to
1.0
at
the s
tart
of
the P
art
D p
rog
ram

Factor Driving Generic Price Changes
Number of generic manufacturers in market
Timing of generic approvals
Special circumstances
Markets with limited entry of generics
Mergers and acquisitions, resulting in market
concentration
Shortages resulting from permanent or temporary
market exit
Special cases of new patents or market exclusivity
(e.g., asthma drugs)
34

94%
52%
44%39%
33%26% 23%
6%
1 2 3 4 5 6 7 . 19
Number of generic manufacturers
Prices Relative to Number of Generic Entries
SOURCE: MedPAC, based on FDA analysis of retail sales data from IMS Health, IMS National Sales Perspective, 1999-2004, extracted
February 2005
Average relative price per dose
35

Brand Share After Patent Expiration
SOURCE: IMS Health, National Prescription Audit, February 2011, used from “The Use of
Medicines in the United States: Review of 2010,” IMS Institute for Healthcare Informatics.36

Factors Driving Generic Substitution
Traditional Drugs
Automatic substitution by pharmacists with patient
consent, based on state laws
Biosimilars
Estimates of lower prices: 20% to 40% (CBO,
European experience)
FDA policies on interchangeability
State laws on substitution of biosimilars
Consumer and prescriber acceptance
Public and private insurance rules
37

Factors Driving Brand Price Changes
Introduction of competing therapies
Other changes in competitive environment
Negotiations with PBMs on behalf of plans
and employers
Stage in patent protection cycle
38

Source: Alliance of Community Health Plans, from Medi-Span® Price Rx®.
Note: Figures reflect wholesale acquisition cost. Price modifications will alter the values reflected above.
Price Increases, Diabetes Drugs, 2010-2015
39

Components of Diabetes Spending Growth,
2013-2014
In billions of dollars
40

Changes in MS Drug Spending, 2010-2014
In billions of dollars
41

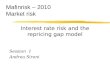
MS Drug Prices from FDA Approval Date
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
Betaseron Avonex Copaxone
Rebif Tysabri Extavia
Gilenya Aubagio Tecfidera
42
SOURCE: D Hartung et al., The cost of multiple sclerosis drugs in the US and the pharmaceutical industry, Neurology 84, May 26, 2015, 2185-2192.

Do Payer Actions Affect Patient Access?
Utilization management
Decisions by payers to raise or lower access
barriers (e.g., PA criteria) in concordance with
price negotiations (e.g., new hepatitis C drugs)
Impact of price changes on the cost to
consumers
Varying use of coinsurance versus copay
Impact of closed and open formularies on
consumers
Effectiveness of appeals and exceptions43

12.9%
5.6%
3.3%
Express Scripts Plan Management Strategies
SOURCE: Express Scripts 2015 Drug Trend Report.
Unmanaged Plans Managed Plans Tightly Managed Plans
44
Average annual increase in per-member per-year spending, 2014-2015,
compared to overall U.S. trend of 5.2%

20
20
2
16
8
6
20
12
7
20
20
20
18
4
12
14
8
13
Harvoni
Sovaldi
Viekira Pak
Copaxone
Tecfidera
Avonex
Humira
Enbrel
Orencia
Gleevec
Revlimid
Zytiga
Plans listing drug on formulary in 2016 Plans not listing drug on formulary in 2016
NOTE: Analysis includes 20 national and near-national stand-alone prescription drug plans in Baltimore, MD (zip code 21201).SOURCE: Georgetown/Kaiser Family Foundation analysis of 2016 Medicare Plan Finder data.
Formulary Coverage of Specialty Drugs Varies
Across Medicare Part D Plans, 2016
He
pat
itis
CM
ult
iple
Sc
lero
sis
Rh
eu
mat
oid
A
rth
riti
sC
ance
r
45

$1,271
$392
$430
$382
$472
$173
$172
$154
$86
$56
$181
$142
$60
$47
$47
$47
$33
$40
$29
$31
$29
$29
$0 $200 $400 $600 $800 $1,000 $1,200 $1,400
Spiriva (COPD/emphysema)
Namenda (Alzheimer's disease)
Lantus Solostar (diabetes)
Advair Diskus (asthma)
Januvia (diabetes)
Crestor (high cholesterol)
Lowest cost when onformulary
Median cost when onformulary
Highest cost when onformulary
Highest cost when noton formulary
NOTE: Analysis includes 20 national and near-national stand-alone prescription drug plans in Baltimore, MD (zip code 21201) and reflects pricing at a Rite Aid pharmacy in this zip code. SOURCE: Georgetown/Kaiser Family Foundation analysis of 2016 Medicare Plan Finder data.
Difference Between the Lowest and Highest Out-of-Pocket
Monthly Cost, Brand Drugs, Medicare Part D, 2016
Part D enrollees’ out-of-pocket costs in 2016:
46

0.4%
17.4%
0.7%
16.8%
1.3%
17.2%
SOURCE: Express Scripts 2015 Drug Trend Report
Future Projected Trend, All Payers, 2016-2018
Trend Forecast: Specialty DrugsTrend Forecast: Traditional Drugs
2016 2017 2018 2016 2017 2018
47

What Does the Future Hold?
Factors to watch that will influence trends
Approvals of new drugs (brands, generics,
biologics, biosimilars)
Trends in drug benefit management by public
and private payers
Price sensitivity by consumers and prescribers
Price transparency
Evidence on comparative effectiveness
Innovations in value-based purchasing
48