Embed Size (px)
Citation preview

1
Drugs in HypertensionDrugs in HypertensionDrugs in HypertensionDrugs in Hypertensiong ypg ypg ypg yp
Dr. Yuri Clement Dr. Yuri Clement Pharmacology Unit, FMSPharmacology Unit, FMS
Objectives Objectives Objectives Objectives Revision of physiological control of BP.Revision of physiological control of BP.
What is hypertension? Associated risks of uncontrolled hypertensionWhat is hypertension? Associated risks of uncontrolled hypertension
ANTIHYPERTENSIVE DRUGS: ANTIHYPERTENSIVE DRUGS:
1.1. Sympathetic Nervous System inhibitionSympathetic Nervous System inhibitionββ--blockers, blockers, αα11 blockers, mixed blockers, mixed αα, , ββ blockers, central blockers, central αα agonists, agonists, peripheral adrenergic blockers.peripheral adrenergic blockers.
2.2. Sodium/Renin Angiotensin Aldosterone System balanceSodium/Renin Angiotensin Aldosterone System balance2.2. Sodium/Renin Angiotensin Aldosterone System balanceSodium/Renin Angiotensin Aldosterone System balanceDiuretics, ACE inhibitors, AT11 receptors blockersDiuretics, ACE inhibitors, AT11 receptors blockers
3.3. Vasodilators Vasodilators CaCa2+2+--channel blockers, oral and parenteral vasodilators channel blockers, oral and parenteral vasodilators
Mechanisms of action, other indications, contraindications and adverse effectsMechanisms of action, other indications, contraindications and adverse effects

2
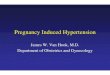
Hemodynamic factors affecting BPHemodynamic factors affecting BPHemodynamic factors affecting BPHemodynamic factors affecting BP
Arterial Blood Arterial Blood Pressure Pressure
Cardiac OutputCardiac Output(CO)(CO)
Total Peripheral Total Peripheral Resistance (TPR)Resistance (TPR)≈ x
Arteriolar volume
Contractility Heart rate
Filling pressureBlood volume
Venous tone
Arteriolar volume
BP Regulation:BP Regulation:SNS and RAAS SNS and RAAS
↑ th ti↑β1 receptor
cardiac activation↑ CO
Baroreceptor reflex system mediatedBaroreceptor reflex system mediated
↑sympathetic activity
cardiac activation
↑α1 receptor smooth muscle activation ↑ TPR
↑ BP
↓ BP
↑
Renal blood volumeRenal blood volume--pressure systempressure system
↓ Renal flow ↑ renin ↑ Angiotensin II
↓GFR ↑Na+, H2O retention ↑ Blood volume
↑Aldosterone

3
What is hypertension? What is hypertension? What is hypertension? What is hypertension? JNC 6 CategoryJNC 6 Category JNC 7 Category JNC 7 Category (2004)(2004)
SBP/DBP (mmHg)SBP/DBP (mmHg)SBP/DBP (mmHg)SBP/DBP (mmHg)
Optimal Optimal <120/80<120/80 NORMAL NORMAL
NormalNormal 120120--129/80129/80--8484PREHYPERTENSIONPREHYPERTENSION
BorderlineBorderline 130130--139/85139/85--8989
HypertensionHypertension >140/90>140/90 HYPERTENSIONHYPERTENSION
A chronic disease of persistent elevated arterial blood pressure.A chronic disease of persistent elevated arterial blood pressure.
Stage 1Stage 1 140140--159/90159/90--9999 STAGE 1STAGE 1
Stage 2 Stage 2 (moderate)(moderate) 160160--179/100179/100--109109STAGE 2STAGE 2
Stage 3 Stage 3 (severe)(severe) ≥180/110≥180/110
ClassificationClassificationClassificationClassification
11oo or essential hypertension (> 95%)or essential hypertension (> 95%)Genetic Genetic Ethnic Ethnic Lifestyle Lifestyle Gender and ageGender and age
22o o hypertension (~5%)hypertension (~5%)Chronic renal disease Chronic renal disease PheochromocytomaPheochromocytomaPheochromocytomaPheochromocytomaCushing’s syndrome and glucocorticoid excess states Cushing’s syndrome and glucocorticoid excess states 11o o aldosteronism and other mineralocorticoid excess statesaldosteronism and other mineralocorticoid excess statesCoarctation of the aorta Coarctation of the aorta DrugDrug--inducedinduced

4
Associated risks Associated risks Associated risks Associated risks Chronic Chronic ↑↑arterial BP arterial BP ↑↑ likelihood of morbidity likelihood of morbidity and mortality.and mortality.
1.1. CADCAD2.2. LVH LVH 3.3. CHF CHF 4.4. MIMI55 ArrhythmiasArrhythmias5.5. ArrhythmiasArrhythmias6.6. AnginaAngina7.7. StrokeStroke8.8. DementiaDementia9.9. Renal disease Renal disease
CVD risk doubles for each increment of 20/10 mmHgCVD risk doubles for each increment of 20/10 mmHg
Why treat? Why treat?
Treating hypertension:Treating hypertension:LVH
–– ↓↓stroke by 40% stroke by 40% -- 45%45%–– ↓↓CHF by 40% CHF by 40% -- 50%50%–– ↓↓CAD by 16% CAD by 16% -- 25%25%
>30% unaware>30% unaware>30% unaware>30% unawareEducational intervention Educational intervention ↓↓ BP. BP. In UK, only ~6% adequately treated.In UK, only ~6% adequately treated.

5
SNS inhibitionMi dMi d ββ t i tt i t CentralCentral αα agonistsagonists
Drug classification Drug classification Drug classification Drug classification
ββ antagonistsantagonists
αα11 antagonistsantagonists
Mixed Mixed αα,,ββ antagonistsantagonists
Peripheral adrenergic Peripheral adrenergic antagonistsantagonists
Central Central αα2 2 agonists agonists
Sodium/RAAS balance
ACE InhibitorsACE InhibitorsDiureticsDiuretics ATII antagonistsATII antagonistsACE InhibitorsACE Inhibitors ATII antagonistsATII antagonists
Vasodilators
CaCa2+2+ channel blockerschannel blockers OthersOthers
ββ antagonistsantagonistsββ antagonistsantagonistsGeneric nameGeneric name Trade name(s)Trade name(s) Doses available Doses available
PropranololPropranolol Inderal®Inderal® Oral: 10, 20, 40, 60, 80, 90mg; 4, 8mg/mL oral Oral: 10, 20, 40, 60, 80, 90mg; 4, 8mg/mL oral soln; Inderal LA: 60, 80, 120, 160mgsoln; Inderal LA: 60, 80, 120, 160mgParenteral: 1mg/mL solnParenteral: 1mg/mL soln
Nadolol Nadolol Corgard®Corgard® Oral: 20, 40, 80, 120, 160mgOral: 20, 40, 80, 120, 160mg
Pindolol Pindolol Visken®Visken® Oral: 5, 10mgOral: 5, 10mg
Acebutolol (*)Acebutolol (*) Sectral®Sectral® Oral: 200, 400mgOral: 200, 400mg
Metoprolol (*)Metoprolol (*) Toprol®, Toprol®, Lopressor®Lopressor®
Oral: 50, 100mg; XL: 25, 50, 100, 200mgOral: 50, 100mg; XL: 25, 50, 100, 200mgParenteral: 1mg/mL solnParenteral: 1mg/mL solnLopressor®Lopressor® gg
Atenolol (*)Atenolol (*) Tenormin® Tenormin® Oral: 25, 50, 100mg; Oral: 25, 50, 100mg; Parenteral: 0.5mg/mL solnParenteral: 0.5mg/mL soln
Betaxolol (*)Betaxolol (*) Kerlone®Kerlone® Oral: 10, 20mgOral: 10, 20mg
Bisoprolol (*)Bisoprolol (*) Zebeta®Zebeta® Oral:5, 10mgOral:5, 10mg
(*) cardioselective(*) cardioselective

6
Mechanism of ActionMechanism of ActionMechanism of ActionMechanism of ActionAcute effect Long term effect
β1 blockade in myocardial cells β1 blockade in juxtaglomerular cells-ve inotropic-ve chronotropic
↓↓ COCO
Shift in whole bodyautoregulation
↓ Renin release
↓ [Angiotensin II]plasma
Change in arterial ↓ arterial
↓ aldosterone
↓ Na+ retention
↓ Blood volumeg
remodellingvasoconstriction
↓↓ TPRTPR
↓↓ BPBP
OtherOther IndicationsIndicationsOtherOther IndicationsIndications
Angina pectorisAngina pectoris
Arrhythmias
Glaucoma (applied topically)
Migraineg
IHD and prevention of 2nd MI.
Useful as monotherapy in Stage 1 HTN Useful as monotherapy in Stage 1 HTN or with vasodilators (and diuretics) in stage 2.or with vasodilators (and diuretics) in stage 2.

7
ContraindicationsContraindicationsContraindicationsContraindications
CHF and nodal conduction diseases. CHF and nodal conduction diseases. But carvedilol (Coreg®) misoprolol and metoprololBut carvedilol (Coreg®) misoprolol and metoprolol–– But, carvedilol (Coreg®), misoprolol and metoprolol But, carvedilol (Coreg®), misoprolol and metoprolol ↓↓ mortality in CHFmortality in CHF
NonNon--selective selective ββ blockersblockers in asthma. Cardioin asthma. Cardio--selective selective drugs lose selectivity at higher doses.drugs lose selectivity at higher doses.
Use with caution in insulinUse with caution in insulin--dependent diabetic patients. dependent diabetic patients. –– Glycogenolysis is adrenergically mediated. Glycogenolysis is adrenergically mediated. ββ
blockersblockers antagonize sympathetic response to antagonize sympathetic response to hypoglycemia and blunt recovery. hypoglycemia and blunt recovery.
Adverse Effects Adverse Effects Adverse Effects Adverse Effects
CNS: Sedation, depression, lethargy, sleep disturbancesCNS: Sedation, depression, lethargy, sleep disturbances
CV: CHF in LV dysfunction, heart block, bradyarrhythmiasCV: CHF in LV dysfunction, heart block, bradyarrhythmias
Bronchospasms (nonBronchospasms (non--selective blockers) in asthma and selective blockers) in asthma and COPD. COPD.
↓↓HDL dHDL d ↑↑ l t i l l ll t i l l l↓↓HDL and HDL and ↑↑plasma triacylglycerolplasma triacylglycerol
Abrupt cessation may induce unstable angina, MI or death in Abrupt cessation may induce unstable angina, MI or death in patients predisposed to ischemic myocardial events. Taper patients predisposed to ischemic myocardial events. Taper over 14 days.over 14 days.

8
α1 antagonistsα1 antagonists
Generic nameGeneric name Trade name(s)Trade name(s) Doses available Doses available
PrazosinPrazosin Minipress®Minipress® Oral: 1, 2, 5mgOral: 1, 2, 5mgTerazosinTerazosin Hytrin®Hytrin® Oral: 1, 2, 5, 10mgOral: 1, 2, 5, 10mg
DoxazosinDoxazosin Cardura®Cardura® Oral: 1, 2, 4, 8mgOral: 1, 2, 4, 8mgCardura®Cardura® Oral: 1, 2, 4, 8mgOral: 1, 2, 4, 8mgTamsulosin Tamsulosin Flomax®Flomax® Oral: 0.4mgOral: 0.4mg
α1 antagonistsα1 antagonistsMechanism of Action:Mechanism of Action:
Arterial and venous relaxation Arterial and venous relaxation -- ↓↓ TPR ; TPR ; ↓↓ BP.BP.Minimal Minimal ↑↑ CO, renal blood flow or GFR. No longCO, renal blood flow or GFR. No long--term tachycardia term tachycardia and and ↑↑ reninrenin release.release.
Indication:Indication:Benign prostatic hypertrophy and hypertension (prostate capsule Benign prostatic hypertrophy and hypertension (prostate capsule relaxation decreases resistance to urinary flow) relaxation decreases resistance to urinary flow)
Adverse Effects:Adverse Effects:1.1. 11stst dose dizziness or syncope dose dizziness or syncope ––give at bedtime (caution in elderly). give at bedtime (caution in elderly). 2.2. Initial reflex tachycardia (Initial reflex tachycardia (propranololpropranolol to counteract) to counteract) 3.3. Postural hypotensionPostural hypotension4.4. Infrequent and mild CNS: vivid dreams, lassitude and depression.Infrequent and mild CNS: vivid dreams, lassitude and depression.

9
Mixed Mixed αα, , ββ antagonistsantagonistsMixed Mixed αα, , ββ antagonistsantagonists
Generic nameGeneric name Trade name(s)Trade name(s) Doses available Doses available LabetalolLabetalol Normodyne® Normodyne® Oral:100, 200, 300mgOral:100, 200, 300mg
Parenteral: 5mg/mL soln Parenteral: 5mg/mL soln CarvedilolCarvedilol Coreg® Coreg® Oral: 3.125, 6.25, 12.5, 25mgOral: 3.125, 6.25, 12.5, 25mg
LabetalolLabetalolLabetalolLabetalol
Equimolar mixture of 4 stereoisomers:Equimolar mixture of 4 stereoisomers:2 i ti 12 i ti 1 bl k thbl k th l til ti ββ bl k dbl k d2 inactive, 1 2 inactive, 1 αα11--blocker, other nonblocker, other non--selective selective ββ--blocker and blocker and ββ22-- partial agonist.partial agonist.Useful in hypertensive emergencies (as Useful in hypertensive emergencies (as iv)iv)Similar efficacy and sideSimilar efficacy and side--effects as effects as ββ-- and and αα11--antagonists antagonists when given orally. when given orally.
Mechanism of action:Mechanism of action:1.1. αα1 1 blockade and blockade and ββ22 stimulation stimulation cause rapid vasodilatation, cause rapid vasodilatation, ↓↓
TPR leading to TPR leading to ↓↓BPBP
Contraindications same as nonContraindications same as non--selective selective ββ blockers blockers

10
Peripheral adrenergic antagonists Peripheral adrenergic antagonists Peripheral adrenergic antagonists Peripheral adrenergic antagonists
Generic nameGeneric name Trade name(s)Trade name(s) Doses available Doses available
ReserpineReserpine -- Oral: 0.1, 0.25mgOral: 0.1, 0.25mg
GuanethidineGuanethidine Ismelin®Ismelin® Oral: 10, 25mgOral: 10, 25mgGuanadrelGuanadrel Hylorel®Hylorel® Oral: 10, 25mgOral: 10, 25mg
Reserpine: Reserpine: Mechanism of actionMechanism of actionReserpine: Reserpine: Mechanism of actionMechanism of action
1.1. Binds avidly to NE and 5Binds avidly to NE and 5--HT storage vesicles in HT storage vesicles in t l d i h lt l d i h l d id icentral and peripheralcentral and peripheral adrenergic neurons adrenergic neurons
inducing catecholamine leakage. inducing catecholamine leakage.
2.2. Overall Effect: Minimal active transmitter Overall Effect: Minimal active transmitter discharged from depolarized nerve endings. discharged from depolarized nerve endings.
3.3. Neurotransmitter depletion in brain and Neurotransmitter depletion in brain and myocardium leads to sedation, depression and myocardium leads to sedation, depression and ↓↓CO.CO.
Rauwolfia serpentinaRauwolfia serpentina root used in Ayuvedic medicine, root used in Ayuvedic medicine, isolated in 1950’s and used in Western medicineisolated in 1950’s and used in Western medicine

11
ReserpineReserpineReserpineReserpine
↓↓CO, CO, ↓↓TPR TPR ↓↓HR (NHR (N ++ d Hd H O t ti )O t ti )↓↓HR, (NaHR, (Na++ and Hand H22O retention)O retention)Low doses + diuretic Low doses + diuretic ≅≅ diuretic + propranolol or methyldopa diuretic + propranolol or methyldopa
Adverse Effects Adverse Effects 1.1. CNS: Sedation, inability to concentrate, nightmares, doseCNS: Sedation, inability to concentrate, nightmares, dose--
related psychotic depression related psychotic depression –– contraindicated in precontraindicated in pre--existing depression. existing depression. e st g dep ess o .e st g dep ess o .
2.2. Unabated parasympathetic activity Unabated parasympathetic activity -- nasal stuffiness, nasal stuffiness, ↑↑gastric acid secretion (contraindicated in peptic ulcer), gastric acid secretion (contraindicated in peptic ulcer), diarrhea and bradycardiadiarrhea and bradycardia
Central α2 agonistsCentral α2 agonists
Generic nameGeneric name Trade Trade name(s)name(s)
Doses available Doses available
ClonidineClonidine Catapress®Catapress® Oral: 0.1, 0.2, 0.3mgOral: 0.1, 0.2, 0.3mgTransdermal patch: 0.1, 0.2, 0.3mg/24hrs Transdermal patch: 0.1, 0.2, 0.3mg/24hrs
MethyldopaMethyldopa -- Oral:250, 500mgOral:250, 500mgGuanabenzGuanabenz Wytensin®Wytensin® Oral: 4, 8mgOral: 4, 8mgGuanfacineGuanfacine Tenex®Tenex® Oral:1, 2mgOral:1, 2mg

12
Mechanism of actionMechanism of actionMechanism of actionMechanism of action
Selective Selective αα22 agonists in the CNS:agonists in the CNS:Selective Selective αα22 agonists in the CNS:agonists in the CNS:↓↓ CNSCNS sympathetic outflow sympathetic outflow –– enhanced enhanced parasympathetic activity parasympathetic activity -- ↑↑vagal tone vagal tone -- ↓↓BPBP
↓↓HR, HR, ↓↓CO, CO, ↓↓ TPR, TPR, ↓↓plasma renin, blunted plasma renin, blunted baroreceptor reflexes.baroreceptor reflexes.
↓↓ NE plasma levels directly NE plasma levels directly ↓↓ TPR with TPR with ↓↓BP.BP.
Clonidine useful in pheochromocytoma diagnosisClonidine useful in pheochromocytoma diagnosis
∝∝--MethyldopaMethyldopa∝∝--MethyldopaMethyldopa
D f h i i thi l f l li it d bD f h i i thi l f l li it d bDrug of choice in this class; usefulness limited by Drug of choice in this class; usefulness limited by adverse effects. adverse effects.
Chronic use results in Chronic use results in NaNa++ and fluid retention (and fluid retention (diureticdiuretic).).
Metabolized to its active form (Metabolized to its active form (αα--methylnorepinephrine) methylnorepinephrine) in the brainin the brain

13
∝∝-- MethyldopaMethyldopa∝∝-- MethyldopaMethyldopa
tt1/21/2: 2hrs; peak effect: ~6: 2hrs; peak effect: ~6--8hrs; Duration of action: 8hrs; Duration of action: 24h24h~24hr~24hr
In elderly: In elderly: ↓↓HR and HR and ↓↓ stroke volume resulting in stroke volume resulting in ↓↓CO, in young uncomplicated patient no such effect.CO, in young uncomplicated patient no such effect.
Adverse effects:Adverse effects:S d ti l it d i ht d iS d ti l it d i ht d iSedation, lassitude, nightmares, depression, Sedation, lassitude, nightmares, depression, vertigo, vertigo, galactorrheagalactorrhea (men & women). (men & women).
ClonidineClonidineClonidineClonidine↓↓ CO and CO and ↓↓ TPRTPR
↓↓ cardiac sympathetic tone leads to cardiac sympathetic tone leads to ↓↓ iontropyiontropy, , ↓↓ chronotropychronotropy
Adverse Effects:Adverse Effects:1.1. CNS CNS –– Sedation; avoid in depressionSedation; avoid in depression2.2. Dry mouthDry mouth2.2. Dry mouthDry mouth
Not 1Not 1stst line therapyline therapy

14
ClonidineClonidine
Caution:Caution:
DoseDose--related withdrawal syndrome within 18related withdrawal syndrome within 18--36 hrs; 36 hrs; ↑↑sympathetic discharge leading to rebound hypertension sympathetic discharge leading to rebound hypertension or overshoot hypertension. or overshoot hypertension.
Symptoms: headache, apprehension, tremors, abdominal Symptoms: headache, apprehension, tremors, abdominal pain, sweating, and tachycardia.pain, sweating, and tachycardia.
ACE InhibitorsACE InhibitorsACE InhibitorsACE Inhibitors
Generic nameGeneric name Trade name(s)Trade name(s) Doses available Doses available
EnalaprilEnalapril Vasotec®Vasotec® Oral: 2.5, 5, 10, 20mgOral: 2.5, 5, 10, 20mg
CaptopilCaptopil Capoten®Capoten® Oral: 12.5, 25, 50, 100mgOral: 12.5, 25, 50, 100mg
LisinoprilLisinopril Zestril®, Prinivil®Zestril®, Prinivil® Oral: 2.5, 5, 10, 20, 40mgOral: 2.5, 5, 10, 20, 40mg
FosinoprilFosinopril Monopril®Monopril® Oral:10, 20, 40mgOral:10, 20, 40mgBenazeprilBenazepril Lotensin®Lotensin® Oral: 5, 10, 20, 40mgOral: 5, 10, 20, 40mgQuinaprilQuinapril Accupril®Accupril® Oral: 5, 10, 20, 40mgOral: 5, 10, 20, 40mg

15
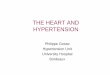
Renin-Angiotensin-Aldosterone SystemRenin-Angiotensin-Aldosterone SystemAngiotensinogen
Angiotensin I
Renin
g
Angiotensin IIAngiotensin Converting Enzyme
Aldosterone↑ Na+, H2O retention
↑ Blood volume Facilitates NE transmission
Vasoconstriction
↑COCO ↑TPRTPR
↑BPBP
X
ACE inhibitors block bradykinin degradation, stimulate PEACE inhibitors block bradykinin degradation, stimulate PE2 2 & prostacyclin& prostacyclin
ACE InhibitorsACE InhibitorsACE InhibitorsACE Inhibitors
As effective as diuretics and β-blockersAs effective as diuretics and β-blockers
Supervise 1st dose
↓TPR without reflex ↑CO, HR or inotrophy
Fetotoxic (absolutely contraindicated in pregnacy)
Initiate with very low dose with slow titration.Initiate with very low dose with slow titration.

16
Other IndicatorsOther Indicators
CHF (↓nonfatal and fatal events).
LVH (may prevent or partial regression).
Type 1 diabetic nephropathyType 1 diabetic nephropathy
Adverse EffectsAdverse EffectsAdverse EffectsAdverse Effects
Acute hypotension Acute hypotension (at onset, esp in severe Na(at onset, esp in severe Na++& volume depletion)& volume depletion)
Ski h ( ti t i t)Ski h ( ti t i t)Skin rash (sometimes transient)Skin rash (sometimes transient)Cough (10% Cough (10% -- 20%)20%)
To a lesser extent (<1%)To a lesser extent (<1%)::Hematologic toxicity: neutropenia, agranulocytosisHematologic toxicity: neutropenia, agranulocytosisA i dA i d i Af ii Af iAngioedema Angioedema –– more in Africansmore in AfricansAcute renal failure Acute renal failure –– esp. in unilateral/bilateral renal artery stenosisesp. in unilateral/bilateral renal artery stenosisGlomerulonephritisGlomerulonephritisProteinuria (captopril)Proteinuria (captopril)Hyperkalemia Hyperkalemia –– esp. in renal disease, DM, on NSAIDs, Kesp. in renal disease, DM, on NSAIDs, K++ supp. or K+supp. or K+--sparing diureticssparing diureticsFeverFever

17
Angiotensin II receptor antagonistsAngiotensin II receptor antagonistsAngiotensin II receptor antagonistsAngiotensin II receptor antagonists
Generic nameGeneric name Trade name(s)Trade name(s) Doses available Doses available
LosartanLosartan Cozaar®Cozaar® Oral: 25, 50, 100mgOral: 25, 50, 100mg
ValsartanValsartan Diovan®Diovan® Oral: 40, 80, 160, 320mgOral: 40, 80, 160, 320mg
CandesartanCandesartan Atacand®Atacand® Oral: 4, 8, 16, 32mgOral: 4, 8, 16, 32mg
OlmesartanOlmesartan Benicar®Benicar® Oral: 5, 10, 20, 40mgOral: 5, 10, 20, 40mgTelmisartanTelmisartan Micardis®Micardis® Oral: 20, 40, 80mgOral: 20, 40, 80mgIrbesartanIrbesartan Avapro®Avapro® Oral: 75, 150, 300mgOral: 75, 150, 300mg
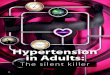
Mechanism of ActionMechanism of ActionBlockade of AgII receptors
↓ vasocontriction ↓Na+ retention
↓↓BPBP
↓ Blood volume
↓↓COCO
↓↓TPRTPRAcute effect
Ag II Stimulation of arterial wall growth
Ag I
growth
↑wall to lumen ratio(remodelling)
↑ vasoconstriction
Long term effect
No effect on bradykinin breakdownNo effect on bradykinin breakdown

18
Angiotensin II receptor subtypes Angiotensin II receptor subtypes ATAT1 1 (site of action of ATII antagonists)(site of action of ATII antagonists)–– VasoconstrictionVasoconstriction–– AldosteroneAldosterone releaserelease–– Sympathetic activationSympathetic activation–– ADH releaseADH release–– Constriction of efferent Constriction of efferent glomerularglomerular arteriolesarterioles
ATAT2 2 (beneficial effect not blocked)(beneficial effect not blocked)–– VasodilationVasodilation
AgII also produced by enzymic reactions of chymasesAgII also produced by enzymic reactions of chymases
Other IndicationsOther IndicationsOther IndicationsOther Indications
“ACE inhibitor without the cough”
Heart failure
Intolerance to other hypertensive drugs
All have similar antihypertensive efficacy with flat doseAll have similar antihypertensive efficacy with flat dose--response curveresponse curve

19
Adverse Effects Adverse Effects Adverse Effects Adverse Effects
Renal insufficiency (Renal insufficiency (↓↓glomerular perfusion pressure)glomerular perfusion pressure)
HyperkalemiaHyperkalemia
Caution: History of ACE inhibitorCaution: History of ACE inhibitor--induced angioedema induced angioedema
DiureticsDiureticsDiureticsDiureticsGeneric nameGeneric name Trade Trade
name(s)name(s)Available dosesAvailable doses
ChlorothiazideChlorothiazide Diuril®Diuril® Oral: 250, 500; 250mg/mL oral suspensionOral: 250, 500; 250mg/mL oral suspension
HydrochlorothiazideHydrochlorothiazide Hydrodiuril®Hydrodiuril® Oral: 25, 50, 100mg tabs; 12.5mg capsulesOral: 25, 50, 100mg tabs; 12.5mg capsulesParenteral: 10mg/mLsolnParenteral: 10mg/mLsolnParenteral: 10mg/mLsolnParenteral: 10mg/mLsoln
ChlorthalidoneChlorthalidone Thalitone®Thalitone® Oral: 250, 500 mg; 250 mg/5mL oral Oral: 250, 500 mg; 250 mg/5mL oral suspensionsuspension
IndapamideIndapamide Lozol®, othersLozol®, others Oral: 1.25, 2.5mgOral: 1.25, 2.5mg
MetolazoneMetolazone Zaroxolyn®Zaroxolyn® Oral: 0.5mgOral: 0.5mg
FurosemideFurosemide Lasix®Lasix® Oral: 20, 40, 80 mg; Parenteral: 10mg/mLOral: 20, 40, 80 mg; Parenteral: 10mg/mL
BumetamideBumetamide Bumex® Bumex® Oral: 0.5, 1, 2 mg; Parenteral: 0.5mg/2mLOral: 0.5, 1, 2 mg; Parenteral: 0.5mg/2mL
TorsemideTorsemide Demadex®Demadex® Oral: 5, 10, 15, 20mg; Parenteral: 10mg/mLOral: 5, 10, 15, 20mg; Parenteral: 10mg/mL
Ethacrynic AcidEthacrynic Acid Edecrin®Edecrin® Oral: 25, 50mg; Parenteral: 50mg/mLOral: 25, 50mg; Parenteral: 50mg/mL
SpironolactoneSpironolactone Aldactone®Aldactone® Oral: 25, 50, 100mgOral: 25, 50, 100mg
EplerenoneEplerenone Inspra®Inspra® Oral: 25, 50mgOral: 25, 50mg
AmilorideAmiloride Midamor ®Midamor ® Oral: 5mgOral: 5mg
TriamtereneTriamterene Dyrenium®Dyrenium® Oral: 50, 100mg Oral: 50, 100mg

20
Diuretics Diuretics –– Thiazides Thiazides (1(1stst line)line)Diuretics Diuretics –– Thiazides Thiazides (1(1stst line)line)
Block renal tubule Na+-Cl- reabsorption
ve effect
Acute effect
↑ urinary loss of Na+ and H2O
↓ extracellular volume
↓CO ↓BP
↑ angiotensin II
↑ renin release
-ve effect
Long term effect•CO returns to normal•CO returns to normal•Slight ↓ in body Na+
•Opening of K+ channels(hyperpolarization)
↓[Ca2+] in vascular smooth muscle cells↓affinity of vascular smooth muscle cells
for vasoconstrictor hormones
↓ Contractility of vascularsmooth muscle cells
↓BP ↓TPR
Diuretics Diuretics –– Furosemide Furosemide (not 1(not 1stst line)line)Diuretics Diuretics –– Furosemide Furosemide (not 1(not 1stst line)line)
Binds to Cl- binding site of Na+-K+-2 Cl- cotransporter in thick ascending loop of Henle
Acute effectthick ascending loop of Henle
↑ loss of Na+ and H2O
↓ Extracellular fluid volume
↓↓ COCO ↓↓BPBP
↑ Angiotensin II
↑ Renin release
L t ff tLong term effect•CO returns to normal•Slight ↓ in body Na+
↓ Contractility of VSMC
↓↓TPRTPR? ? ↓↓BP ?BP ?

21
Loop Diuretic – FurosemideLoop Diuretic – Furosemide
Indications:Indications:Resistant hypertension (not 1st line)
Edema (renal impairment or volume overload)
HypercalcemiaHypercalcemia
Hyperkalemia
CaCa2+2+ channel blockerschannel blockersCaCa2+2+ channel blockerschannel blockersGeneric nameGeneric name Trade Trade
name(s)name(s)Doses available Doses available
BenzothiazepineBenzothiazepineDiltiazemDiltiazem
Cardizem®Cardizem® Oral: 30, 60, 90, 120mg; sustained release: 60, Oral: 30, 60, 90, 120mg; sustained release: 60, 90, 120, 180, 240, 300, 360, 420mg.90, 120, 180, 240, 300, 360, 420mg.Parenteral: 5mg/mL solnParenteral: 5mg/mL solnParenteral: 5mg/mL solnParenteral: 5mg/mL soln
DiphenylalkylamineDiphenylalkylamineVerapamilVerapamil
Calan®, Calan®, Isoptin®Isoptin®
Oral: 40, 80, 120mg; sustained release: 120, Oral: 40, 80, 120mg; sustained release: 120, 180, 240mg180, 240mgParenteral: 2.5mg/mL solnParenteral: 2.5mg/mL soln
DihydropyridineDihydropyridineNifedipineNifedipine
Adalat® CC, Adalat® CC, Procardia®Procardia®XLXL
Oral: 10, 20mg. Extended release: 30, 60, 90mgOral: 10, 20mg. Extended release: 30, 60, 90mg
AmlodipineAmlodipine Norvasc®Norvasc® Oral: 2 5 5 10mgOral: 2 5 5 10mgAmlodipineAmlodipine Norvasc®Norvasc® Oral: 2.5, 5, 10mgOral: 2.5, 5, 10mg
FelodipineFelodipine Plendil®Plendil® Oral extended release: 2.5, 5, 10mgOral extended release: 2.5, 5, 10mg
IsradipineIsradipine DynaCirc®DynaCirc® Oral:2.5, 5mg; controlled release: 5, 10mgOral:2.5, 5mg; controlled release: 5, 10mg
NicardipineNicardipine Cardene®Cardene® Oral:20, 30mg; sustained release: 30, 45, 60mgOral:20, 30mg; sustained release: 30, 45, 60mgParenteral: 2.5mg/mL solnParenteral: 2.5mg/mL soln
NisoldipineNisoldipine Sular®Sular® Oral extended release: 10, 20, 30, 40mgOral extended release: 10, 20, 30, 40mg

22
Mechanism of ActionMechanism of ActionMechanism of ActionMechanism of Action
DihydropyridinesNifedipine Amlodipine
Verapamil, DiltiazemNifedipine, Amlodipine
Block L-type Ca2+ channelsin arterial smooth muscle
Block L-type Ca2+ channelsin SA and AV node
↓↓ TPRTPR ↓ or abolishes reflex tachycardia
↓↓ BPBP
Baroreceptor-mediated reflex tachycardia
Inhibit influx of CaInhibit influx of Ca++++ ions thru’ voltageions thru’ voltage--gated channelsgated channels
Relative efficacyRelative efficacyRelative efficacyRelative efficacy
DrugDrug VasodilationVasodilation --ve inotropyve inotropy AutomaticityAutomaticity AVAVDrugDrug Vasodilation Vasodilation (coronary (coronary
flow)flow)
--ve inotropyve inotropy Automaticity Automaticity (SA node) (SA node)
suppressionsuppression
AV AV conduction conduction suppressionsuppression
DiltiazemDiltiazem 33 22 55 44
NifedipineNifedipine 55 11 11 00
VerapamilVerapamil 44 44 55 55
Relative cardiovascular effect: 0=no effect, 5=maximum effectRelative cardiovascular effect: 0=no effect, 5=maximum effect

23
IndicationsIndicationsIndicationsIndications
Mild to moderate HTN associated with exercise-induced, variant and unstable angina.
MI (ACE inhibitors>protective than dihydropyridines)
Antiarrhythmic (diltiazem and verapamil for (supraventricular tachycardia atrial fibrillation and(supraventricular tachycardia, atrial fibrillation and atrial flutter).
Not clinically superior to diuretics or Not clinically superior to diuretics or ββ--blockers,blockers,uusually 2sually 2ndnd & 3& 3rdrd line therapy.line therapy.
Vasodilatory-related (more with
Adverse Effects Adverse Effects
Vasodilatory-related (more with dihydropyridines): dizziness, flushing, headache, peripheral edema
Gingival hyperplasia
Mood swings & fatigueMood swings & fatigue
Verapamil causes constipation (7%) and contraindicated in CHF

24
Oral and parenteral vasodilatorsOral and parenteral vasodilatorsOral and parenteral vasodilatorsOral and parenteral vasodilators
Generic nameGeneric name Trade name(s)Trade name(s) Doses available Doses available
HydralazineHydralazine Apresoline®Apresoline® Oral: 10, 25, 50, 100mgOral: 10, 25, 50, 100mgParenteral: 20mg/mL solnParenteral: 20mg/mL soln
NitroprussideNitroprusside Nitropress®Nitropress® Parenteral: 50mg/vialParenteral: 50mg/vial
MinoxidilMinoxidil Loniten®Loniten® Oral: 2.5, 10mgOral: 2.5, 10mgTopical (Rogaine®, etc): 2% solnTopical (Rogaine®, etc): 2% soln
DiazoxideDiazoxide Hyperstat® IVHyperstat® IV Oral: 50mg capsuleOral: 50mg capsuleParenteral: 15mg/mLParenteral: 15mg/mL
FenoldopamFenoldopam Corlopam®Corlopam® Parenteral: 10mg/mL soln Parenteral: 10mg/mL soln
HydralazineHydralazineHydralazineHydralazine
Well absorbed orally, short tWell absorbed orally, short t1/21/2 (1 hr), peak effect (1/2 hr to (1 hr), peak effect (1/2 hr to 2 hrs) & duration of action (12hr)2 hrs) & duration of action (12hr)2 hrs) & duration of action (12hr). 2 hrs) & duration of action (12hr).
Bioavailability determined by acetylator status: Bioavailability determined by acetylator status: 16% in ‘fast’ and 35% in ‘slow’ acetylators.16% in ‘fast’ and 35% in ‘slow’ acetylators.
Adverse effects limit use. Reserved for Adverse effects limit use. Reserved for refractory severe refractory severe hypertension used concomitantly with diuretics and hypertension used concomitantly with diuretics and ββ--yp yyp y ββblockers (never as monotherapy).blockers (never as monotherapy).
Used occasionally with isosorbide dinitrate in CHF.Used occasionally with isosorbide dinitrate in CHF.
Contraindicated in CAD and > 40yearsContraindicated in CAD and > 40years

25
HydralazineHydralazineHydralazineHydralazine
Direct relaxation of arteries (not veins), cAMP Direct relaxation of arteries (not veins), cAMP ect e a at o o a te es ( ot ve s), cect e a at o o a te es ( ot ve s), cmediated.mediated.
Vasodilatation causes baroreceptorVasodilatation causes baroreceptor--mediated reflex, mediated reflex, sympathetic stimulation sympathetic stimulation →→ tachycardia tachycardia →→ ↑↑ CO; CO; ↑↑renin release renin release →→ ↑↑ NaNa++ and Hand H22O retention. O retention.
↑↑CO and fluid retentionCO and fluid retention cause tachyphylaxis, unless cause tachyphylaxis, unless used in combination with used in combination with ββ--blockers (blockers (↓↓reflex reflex tachycardia) and diuretics (tachycardia) and diuretics (↓↓fluid retention).fluid retention).
Hydralazine: Adverse EffectsHydralazine: Adverse EffectsHydralazine: Adverse EffectsHydralazine: Adverse Effects
Direct extension of pharmacological activity:Direct extension of pharmacological activity:Direct extension of pharmacological activity:Direct extension of pharmacological activity:headache, nausea, flushing, dizziness, hypotension, headache, nausea, flushing, dizziness, hypotension, palpitation, tachycardia, angina pectoris, MIpalpitation, tachycardia, angina pectoris, MI
Immunological reactions (unknown mechanism):Immunological reactions (unknown mechanism):–– Serum sickness, hemolytic anemia, Serum sickness, hemolytic anemia, vasculitisvasculitis, rapidly , rapidly
progressing progressing glomerulonephritisglomerulonephritis–– 1010--20%incidence of reversible dose20%incidence of reversible dose--related lupus related lupus
erythematosuserythematosus--like syndrome like syndrome –– high dose or after high dose or after >6mth chronic use. (Use <200mg daily) >6mth chronic use. (Use <200mg daily) Effect > in females and ‘slow Effect > in females and ‘slow acetylatorsacetylators’.’.
Limited usefulness in hypertensionLimited usefulness in hypertension

26
MinoxidilMinoxidilMinoxidilMinoxidil
Direct relaxation of arteries (not veins).Direct relaxation of arteries (not veins).
↑↑blood flow to skin, skeletal muscles, GI blood flow to skin, skeletal muscles, GI tract, heart.tract, heart.
Reflex Reflex ↑↑CO, renal vasodilatation and CO, renal vasodilatation and ↑↑renin secretionrenin secretion.
MinoxidilMinoxidilMinoxidilMinoxidil
> potency than > potency than hydralazinehydralazinep yp y yy
Well absorbed orally, short tWell absorbed orally, short t1/21/2:3:3--4 hrs, duration of action: 4 hrs, duration of action: 12hr. 12hr.
NEVER as as monotherapymonotherapy, use with , use with ββ--blockers and blockers and diuretics (loop diuretic). diuretics (loop diuretic). ( p )( p )
Reserved for refractory severe hypertension.Reserved for refractory severe hypertension.

27
Minoxidil Minoxidil –– Adverse EffectsAdverse EffectsMinoxidil Minoxidil –– Adverse EffectsAdverse Effects
↑↑More dramatic More dramatic ↑↑fluid retention than fluid retention than hydralazinehydralazine (n(not ot ↑↑reninrenin and and aldosteronealdosterone secretion related). secretion related). ↓↓ renal renal perfusion pressure and reflex stimulation of renal tubular perfusion pressure and reflex stimulation of renal tubular αα--receptors. receptors.
Headache, sweating Headache, sweating
HypertrichosisHypertrichosis::Used topically to treat of maleUsed topically to treat of male--pattern baldness.pattern baldness.
Sodium nitroprussideSodium nitroprussideSodium nitroprussideSodium nitroprussideGiven by Given by iviv continuous infusion. Onset: 30sec; peak continuous infusion. Onset: 30sec; peak effect: 2 mins.effect: 2 mins.effect: 2 mins. effect: 2 mins.
Metabolized to NO and cyanide. Metabolized to NO and cyanide. 1.1. NO causes vasodilatation.NO causes vasodilatation.2.2. Cyanide is poisonous, and further metabolized to Cyanide is poisonous, and further metabolized to
thiocyanate. thiocyanate.
Very potent vasodilator of both arteries and veins Very potent vasodilator of both arteries and veins
Drug of choice in hypertension emergencies Drug of choice in hypertension emergencies (BP>210/150mmHg).(BP>210/150mmHg).

28
Sodium nitroprussideSodium nitroprussideSodium nitroprussideSodium nitroprusside
M dM d ↑↑HRHR dd ↓↓ di ldi l OO d dd dModest Modest ↑↑HR HR and and ↓↓myocardial myocardial OO22 demanddemand
Other indications: Other indications: –– Acute aortic dissection (propranolol given first Acute aortic dissection (propranolol given first
to prevent reflex sympathetic activation).to prevent reflex sympathetic activation).–– In CHF toIn CHF to ↑↑COCOIn CHF to In CHF to ↑↑COCO–– In acute MIIn acute MI to to ↓↓myocardial myocardial OO22 demanddemand
Sodium Nitroprusside: Sodium Nitroprusside: Adverse EffectsAdverse EffectsSodium Nitroprusside: Sodium Nitroprusside: Adverse EffectsAdverse Effects
Cyanide and thiocyanate poisoning: Cyanide and thiocyanate poisoning: –– Anorexia, nausea, fatigue, disorientation, toxic Anorexia, nausea, fatigue, disorientation, toxic
psychosis.psychosis.Closely monitor BP and plasma thiocyanate (<0.1Closely monitor BP and plasma thiocyanate (<0.1μμg/mL). g/mL). Antidote: Infusion of sodium thiosulphate Antidote: Infusion of sodium thiosulphate →→ thiocyanatethiocyanate↑risk of poisoning in impaired renal function
Worsens arterial hypoxemia in COPDWorsens arterial hypoxemia in COPD
Abrupt cessation after shortAbrupt cessation after short--term use causes rebound HTN.term use causes rebound HTN.

29
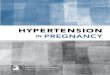
Prescribed Antihypertensive Drugs in Trinidad (n=442)Prescribed Antihypertensive Drugs in Trinidad (n=442)
Drug Class/Generic Drug name All HTN N (%) HTN alone N (%) HTN with DM N (%)
ACE Inhibitors (ACEI)EnalaprilLisinoprilFosinoprilCaptopril
281 (63.6)2473022
113 (58.9)951512
168 (67.2)1521510
β-blockers (BB)AtenololPropranololBisoprolol
129 (29.2)11793
65 (33.9)6141
64 (25.6)5652
DiureticsThiazide (bendrofluazide)Furosemide
114 (25.8)8925
66 (34.4)5016
48 (19.2)399
Calcium channel blockers (CCB)NifedipineAmlodipineVerapamil
53 (12.0)4553
23 (12.0)2201
30 (12.0)2352
α-blockersTerazosinDoxasosin
3 (0.7)12
1 (0.5)10
2 (0.8)02
Angiotensin receptor blockers (ARB)ValsartanPresartan
10 (2.3)91
5 (2.6)50
5 (2.0)41
Other drugsMethydopaReserpine
27 (6.1)234
18 (9.4)162
9 (3.6)72
Antihypertensive drug therapy in Trinidadian patients with complete accessible drug records (n=442)Antihypertensive drug therapy in Trinidadian patients with complete accessible drug records (n=442)
Antihypertensive drug therapy All HTN patients N (%)
HTN alone N (%)
HTN with DM N (%)
No drug therapy 26 (5.9) 8 (4.2) 18 (7.2)
Monotherapy 242 (54.8) 86 (44.8) 156 (62.4)
Dual drug therapy 121 (27.3) 62 (32.3) 59 (23.6)
Triple drug therapy 45 (10.2) 30 (15.6) 15 (6.0)
Quadruple drug therapy 8 (1.8) 6 (3.1) 2 (0.8)
TOTAL 442 192 250

30
↑sympathetic activity
↑β1 receptor cardiac activation
↑ CO
↑ BP
ββ--blockersblockers αα11--blockersblockers
y↑α1 receptor
smooth muscle activation ↑ TPR↑ BP
↓ BP
↓ Renal flow ↑ renin ↑ Angiotensin II
CaCa2+2+--channel channel blockersblockers
ACE inhibitorsACE inhibitorsVasodilators Vasodilators
↓GFR ↑Na+, H2O retention ↑ Blood volume
↑Aldosterone
DiureticsDiuretics
AgII receptor AgII receptor blockersblockers