Embed Size (px)
Citation preview
![Page 1: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/1.jpg)
Pathologie des tumeurs neuroblastiques périphériques
M. PeuchmaurUniv. Diderot Paris7, Sorbonne Paris Cité
Sce de Pathologie, R. Debré, APHP
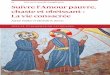
Missions essentielles
• INPC • diagnostic positif• histopronostic • banque tissulaire
congelée
MKI
défavorable
âge
favorable
•Cell. Schwann•Différenciation cell. tumorales
INPC
![Page 2: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/2.jpg)
2 1 3 4
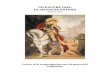
“Cross” sampling
“Book” sampling
SAMPLING OF NEUROBLASTIC
TUMORSFOR PROGNOSTIC
BIOLOGICAL STUDIES
1
3
2
4
1 cm
If possible, minimum 2 samples (A, B) from different sites.Required for therapeutic protocols in pre-treatment specimens!
If possible, minimum 2 samples (A, B) from different sites.Required for therapeutic protocols in pre-treatment specimens!
Type III
Type I
Type IIA
Type IIB
![Page 3: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/3.jpg)
Tumeurs Neuroblastiques Périphériques
• Ganglioneurome• Ganglioneuroblastome mélangé
(intermixed)• Ganglioneuroblastome nodulaire• Neuroblastome
![Page 4: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/4.jpg)
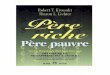
Arbre pour le Diagnostique TNP3 clefs
• Schwann
• Fond fibrillaire
• cellules differenciées < 5%
![Page 5: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/5.jpg)
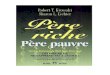
Arbre pour le Diagnostique TNP3 clefs
• Schwann
• Oui = stroma riche: GN, GNBi et nod < 5%
• Oui: NB Peu Différencié–Non: NB différenciant
![Page 6: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/6.jpg)
Contingent schawnnien: PrésentDominant / Riche
GanglioNeurome, stroma dominant
GanglioNeuroblastome,stroma riche,« intermixed » ou« mélangé »
![Page 7: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/7.jpg)
Contingent schawnnien: PrésentMixte, riche et pauvre
Nodule
• GanglioNeuroblastome, stroma mixte riche et pauvre,
• nodulaire
![Page 8: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/8.jpg)
Arbre pour le Diagnostique TNP3 clefs
• Schwann• Oui = stroma riche: GN, GNB
– Non = stroma pauvre
![Page 9: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/9.jpg)
Contingent schawnnien: Absent0% à <50%
• Neuroblastome, stroma pauvre
![Page 10: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/10.jpg)
Arbre pour le Diagnostique TNP3 clefs
• Schwann: Non = stroma pauvre
• Fond fibrillaire Absent :
=NB indifférencié 5%• Oui: NB Peu Différencié
–Non: NB différenciant
![Page 11: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/11.jpg)
Neuroblastome, stroma pauvre, indifférencié
• Fond fibrillaire ou neuropile: absent • IHC: TH & autres
![Page 12: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/12.jpg)
Arbre pour le Diagnostique TNP3 clefs
• Schwann: Non = stroma pauvre
• Fond fibrillaire Présent :
• cellules differenciées < 5%• Oui: NB Peu Différencié
–Non: NB différenciant
![Page 13: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/13.jpg)
Neuroblastome, stroma pauvre, peu différencié
• Fond fibrillaire ou neuropile: Présent
• Cellules tumorales différenciées: <5%
![Page 14: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/14.jpg)
Arbre pour le Diagnostique TNP3 clefs
• Schwann: Non = stroma pauvre
• Fond fibrillaire Présent :
• cellules differenciées < 5% i:–Non: NB différenciant
![Page 15: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/15.jpg)
Neuroblastome, stroma pauvre, différenciant
• Fond fibrillaire ou neuropile: Présent
• Cellules tumorales différenciées: >5%
![Page 16: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/16.jpg)
INPC: international neuroblastoma pathology classification
catégories stroma sous-type critères additionnels
neuroblastome stroma pauvre indifférencié MKI
peu différencié mitoses
différenciant calcifications
ganglioneuroblastome mixte, stroma riche nodulaire MK I
et stroma pauvre mélangé mitoses
calcifications
ganglioneurome stroma dominant maturant
mature
TNP NOS
Neuroblastome NOS
![Page 17: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/17.jpg)
histopronostic
bas <2% haut >4%
âge dépendant: <1.5 an, [1.5-5], >5 ans
différentiation:
in- peu- diff.
MKI: bas (<2%), intermédiaire [2%-4%], haut >4%
![Page 18: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/18.jpg)
Prognostic categorization of neuroblastomas and nodular ganglioneuroblastomas (classic and variants, prognosis determined by the nodule) U and red: unfavorable. F and green: favorableAge <1.5 yrs
Undifferentiated Poorlydifferentiated
Differentiating
Low MKI U F F
Intermediate MKI
U F F
High MKI U U U
Undifferentiated Poorlydifferentiated
Differentiating
Low MKI U U F
Intermediate MKI
U U U
High MKI U U U
Undifferentiated Poorlydifferentiated
Differentiating
Low MKI U U U
Intermediate MKI
U U U
High MKI U U U
F
Age 1.5-5 yrs
Age > 5 yrs
Prognostic categorization of ganglioneuroblastomas, intermixed and ganglioneuromas.Any age
![Page 19: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/19.jpg)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Years Since Enrollment
EF
S R
ate
(%)
Favorable (N = 894)
Unfavorable (N = 665)
P < 0.0001
EFS by Shimada Histology (N = 1559)
![Page 20: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/20.jpg)
Eur J Cancer. 2006;42:1113-9J Clin Oncol. 2012;30:1842-8
Outcome after surgery alone or withrestricted use of chemotherapy for patientswith low-risk neuroblastoma: results ofChildren's Oncology Group study P9641.Douglas R. Strother, et al. J Clin Oncol.2012;30:1842-8
• Excellent survival rates can be achieved in asymptomatic low-risk patients with stages 2a and 2b NBL after surgery alone. Patients with stage 2b disease who have unfavorable histology tumors fare less well.
• Stage 2b, Favorable vs Unfavorable – EFS, p=0.0023
• 90 + 3 (% + SE) vs 72 + 7– OS, p<0.001
• 99 + 1 vs 86 + 5
Favorable Histology (n=427)
P<0.0001
0 2 4 6 8 10 12
PR
OB
AB
ILIT
Y
0.25
0.5
0.75
1.0
YEARS
International Neuroblastoma Pathology Classification adds independent prognostic information beyond the prognostic contribution of ageHideki Sano et al. Eur J Cancer. 2006;42:1113-9
Unfavorable Histology (n=319)
![Page 21: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/21.jpg)
The International Neuroblastoma Risk Group consensu s pre-treatment classification schema
H Intermediate*GNB nodular, poorly differentiated or undifferentiated
NB, poorly differentiated or undifferentiated
H Intermediate*
E LowGNB nodular, differentiatingNB, differentiating
>18m
G Intermediate
D LowAny, except GN maturing or GNB intermixed
<18mL2
A Very LowGN maturingGNB intermixed
L1/L2
Pre-treatment Risk Group
Histological Category/Grade of Tumor Differentiatio nAgemonths
INRG Stage
![Page 22: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/22.jpg)
EFS Rate by Tumor GradeNB & GNB, nod > 18 mo (n=1,270)
![Page 23: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/23.jpg)
TNP: la preuve par 3
• 3 missions– Diagnostic– Pronostic– Banque
• 3 clefs Dg– Schwann– Fond fibrillaire– Cellules différenciées
%
• 3 critères Pc– Différenciation– MKI– Âge
• 3 “nouveautés”– PHOX2B– VBP– Nouvelles entités:
nucléoles, Composite Neuroblastoma
![Page 24: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/24.jpg)
PHOX2B Immunolabeling: A Novel Tool for the Diagnos is of Undifferentiated Neuroblastomas Among Childhood Sma ll-, Round-, Blue-cell Tumors. F. Bielle et al. Am J Surg Pathol 2012, 36:1141-9
Anti-PHOX2B +
Anti-TH neg
Anti-PHOX2B +
![Page 25: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/25.jpg)
Question INRG/LINES, L2: taille des prélèvements
Biopsie représentative ?
![Page 26: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/26.jpg)
On behalf of the Europeran group of PathologistsVirtual Biopsy Project : Proof of concept
1.svs ImageScopeInstaller.exe
![Page 27: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/27.jpg)
A
C
B
D
neuroblastoma poorly differentiated subtype with prominent nucleoli
Negative staining for N-myc proteinNuclear staining for N-myc protein
neuroblastoma poorly differentiated subtype with “salt and pepper” nuclei
“Bull’s eye” tumor
“Conventional” tumor
![Page 28: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/28.jpg)
Composite Neuroblastomas
• to clarify the definition and to attempt to describe groups which could be tested for reproducibility and clinical impact.
n°29
n°1
![Page 29: DUIOP Peuchmaur mars 2015 [Mode de compatibilité] 7... · Mixte, riche et pauvre Nodule • GanglioNeuroblastome, stroma mixte riche et pauvre, • nodulaire. Arbre pour le Diagnostique](https://reader030.pdfslide.net/reader030/viewer/2022031019/5b9cd11709d3f2f6368d49b8/html5/page/29.jpg)
References1/ Pathologie, INPC
• Shimada H, Ambros IM, Dehner LP, et al. The International Neu roblastoma Pathology Classification (the Shimada system) . Cancer.1999;86:364-372.
• Shimada H, Ambros IM, Dehner LP, Hata J, Joshi VV, Roald B.Ter minology and morphologic criteria of neuroblastic tumors:recommendations by the International Neuroblastoma Patho logy Committee. Cancer. 1999;86 :349-363.
• Peuchmaur M, D'Amore ES, Joshi VV, et al. Revision of the inte rnational neuroblastoma pathology classification. Cance r. 2003;98:2274-81.
• Navarro S, Amann G, Beiske K, Cullinane C, D ’Amore E, Gambini C, Mosseri V, de Bernadi B, Michon J, Peuchma ur M. Prognostic value ofInternational Neuroblastoma Pathology Classification in Localized Resectable Peripheral Neurobkastic Tumors. A hi stopathologic study ofLNESG 94.01 Trial and Protocol. J Clin Oncol 2006,24:695-69 9.
• Monclair T, Brodeur GM, Ambros PF, et al; INRG Task Force. The International Neuroblastoma Risk Group (INRG) staging sys tem: an INRGTask Force report. J Clin Oncol. 2009;27:298-303
• Cohn SL, Pearson AD, London WB, et al; INRG Task Force. The Int ernational Neuroblastoma Risk Group (INRG) classificatio n system: anINRG Task Force report. J Clin Oncol. 2009;27:289-97
• F. Bielle et al. PHOX2B Immunolabeling: A Novel Tool for the D iagnosis of Undifferentiated Neuroblastomas Among Childh ood Small-,Round-, Blue-cell Tumors. Am J Surg Pathol 2012, 36:1141-9
2/ Générales
• Lastowska M, Cullinane C, Variend S, et al; United Kingdom Ch ildren Cancer Study Group and the United Kingdom Cancer Cyto geneticsGroup. Comprehensive genetic and histopathologic study re veals three types of neuroblastoma tumors. J Clin Oncol. 200 1;19 :3080-90.
• Brodeur GM. Neuroblastoma: biological insights into a clin ical enigma. Nat Rev Cancer. 2003;3:203-16.
• Attiyeh EF. Chromosome 1p and 11q deletion and outcome in neu roblastomas. NEJM 2005;353:2243-2253
• Janoueix-Lerosey I, Lequin D, Brugière L et al. Somatic and g ermline activating mutation of the ALK kinase receptor in ne uroblastoma.Nature 2008; 455:967-70.
• Janoueix-Lerosey I, Schleiermacher G, Michels E et al. Over all genomic pattern is a predictor of outcome in neuroblasto ma. J Clin Oncol.2009;27:1026-33
• Janoueix-Lerosey I, Schleiermacher G, Delattre O. Molecul ar pathogenesis of peripheral neuroblastic tumors. Oncoge ne. 2010; 29:1566-79.