Embed Size (px)
Citation preview

Dupuytren’s Disease
Murali KrishnanHand Term - April 2007

Overview
• Who is Dupuytren?• Definition of Dupuytren disease• Anatomy of the bands and cords• Aetiology and pathopysiology• Recurrence• Clinical assessment • Treatment options

Introduction
BARON GUILLAUME DUPUYTREN
(1777-1835)
“First among surgeons, Last among men"

Definition
Dupuytren’s disease is an abnormal thickening of the fascial tissue resulting in digital flexion contractures.
Cell Responsible - Myofibroblast

Anatomy
Bands – Normal tissue
Cords – Abnormal tissue

Fascias
Fascias- Thenar aponeurosis- Ulnar aponeurosis- Palmar aponeurosis- Palmodigital fascia (entraps digital nerve)- Digital fascia

Palmar fascia
Palmar fascia - Longitudinal- Transverse - Vertical

Palmar fascia

Palmodigital fascia and bands

Spiral band and cord

Spiral cord and Nerve

Digital band and cord
Digital cord - Central- Lateral

Anatomy

Anatomy

Anatomy
Pretendinous cord causes MCPJ contractures

Anatomy
Central and Spiral cords causes PIPJ contracture

Anatomy
• Superficial transverse ligament is not involved in the disease process
• Natatory ligament causes web space contractures. • In the index finger, Natatory ligament becomes the
distal Commisural ligament and causes contracture between the index finger & thumb.

Anatomy
• Cleland's ligament is not involved in Dupuytren's.• Grayson's ligament contributes to the spiral cord.• The spiral cord pushes the NVB toward the skin &
midline of the finger.
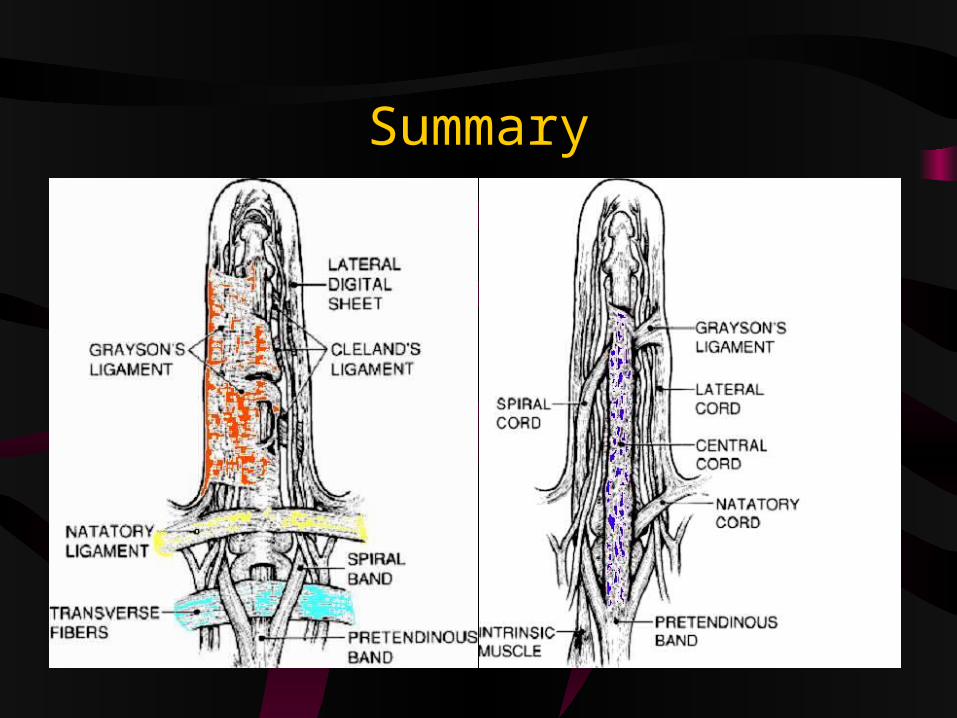
Summary


Pathogenesis

Myofibroblast
• Responsible for contracture • Metaplasia of fibroblast into myofibroblast• Features of smooth muscle cell and fibroblast• Contains actin microfilaments

Similar fibromatosis
• Garrods pads• Ledderhose disease -5%• Peyronies disease -3%

Associated conditions
1. Epilepsy (42%) 2. Alcohol-induced liver disease 3. Diabetes mellitus 4. COAD5. Hypertension6. IHD

Influencing factors
• Genetics • Trauma• Ischaemia• Alcohol• Phenobarbitone• MMPs and TIMPs• Reduced apoptosis• Free radicals• Interleukin 1

Genetics
• Common among Caucasian (Scottish)– Curse of Mac Crimmons
• Rare in Africans and Middle Eastern descent• Male predominance

Trauma
• Micro ruptures in palmar fascia triggers IL-1• Vasomotor disturbance following swelling in hand
causing secondary Ischaemia

IschaemiaIschaemia
Adenosine Triphosphate Xanthine dehydrogenase(ATP)
Hypoxanthine Xanthine Oxidase
Xanthine &
Uric Acid
OxidationFree Radicals

Ischaemia
• Increase in free radicals• Decrease in antioxidant enzyme activity• Microangiopathy with narrow vessels are found in
dupuytren tissue
Alcohol
• Conversion of Xanthine dehydrogenase to Xanthine oxidase
Increases in free radicals
• Increase in Lysophospatidic acid (LPA)Increases intracellular calcium aiding contracture

Phenobarbitone
• Increase in Lysophospatidic acid (LPA)Increases intracellular calcium aiding contracture

MMPs and TIMPs
• Normal levels of MMPs• Increased levels of TIMPs-1 • Abnormally low MMP : TIMPs ratio
– External fixator to improve contraction prior to surgery is said to increase the level of MMPs

Reduced Apoptosis
• IL 1 and TGF beta reduces the apoptosis of damaged and inflamed cells

Free radicals
• Fibroblast proliferation6 fold increase in cords40 fold increase in nodule
• Increased production of IL-1• Indirect increase in collagen III

Collagen
• Normal palmar fasciaPredominantly type I collagenLesser extent type III collagen
• Dupuytren fasciaIncreased ratio of type III to type I collagen

IL-1
• Fibroblast proliferation• Stimulates platelets and macrophages to produce
various growth factors (TGF beta)• Reduces apoptosis• Stimulates langerhans cells of the epidermis
Extrinsic pathway: Migration to dermo-epidermal junction – initiates events – contractures

Pathogenesis
Mechanisms
Intrinsic ExtrinsicTGF beta induces Langerhans
cells the differentiation pathwayof fibroblasts into
myofibroblasts

Mechanism
Intrinsic Extrinsic

Final contraction
Myosin triggered by LPA
Contraction of Intracellular actin microfilaments
Dupuytren contracture
Stages
Proliferativelarge myofibroblastsvery vascular
InvolutionDense network of myofibroblastsIncreased ratio of type III to type I collagen
ResidualMyofibroblasts disappearPredominantly fibrocytes

Recurrence/Aggressive
1. Young 2. Male 3. Family history 4. Bilateral 5. Fibromatosis elsewhere 6. Garrod's knuckle pads

Future
1. BMP2. Gene therapy3. Nitric oxide

Summary
• Associated conditions• Various pathways• Role of Free radicals, Interleukin etc• Collagen I replaced by collagen III• Intrinsic and extrinsic theories • Contracture formation• Stages

Thank you





























