Embed Size (px)
Citation preview

12/11/2015
1
Dwelling on Dwell Time - When
Is it Time to Remove a Peripheral Intravenous Catheter?
12/11/2015 © 2015 Pennsylvania Patient Safety Authority
James Davis, MSN RN CCRN CIC HEM Senior Infection Prevention Analyst
Pennsylvania Patient Safety Authority and
Marcia Ryder, PhD MS RN Research Scientist Ryder Science, Inc.
Objectives
• Identify the gaps in research related to infection prevention and leaving peripheral intravenous catheters in place longer than 72 hours
• Comprehend the risks of peripheral intravenous line infection
• Examine the risks versus benefits of the clinically indicated replacement standard
• Identify a clinical process model for the implementation of clinically indicated PIV replacement
12/11/2015 2 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
2
Centers for Disease Control and Prevention (CDC)
The CDC guidelines for prevention of peripheral vascular catheter–related infection (PVCRI) state the following:
1. There is no need to replace peripheral catheters more frequently than every 72–96 hours. . .Category IB*
2. No recommendation is made regarding replacement of peripheral catheters in adults only when clinically indicated. Unresolved issue†
* “Category IB. Strongly recommended for implementation and supported by some experimental, clinical, or epidemiologic studies and a strong theoretical rationale; or an accepted practice (e.g., aseptic technique) supported by limited evidence.”
† “Unresolved issue. Represents an unresolved issue for which evidence is insufficient or no consensus regarding efficacy exists.”
Centers for Disease Control and Prevention. Guidelines for the prevention of intravascular-related infections, 2011[online]. 2011 [cited 2013 Nov 1] http://www.cdc.gov/hicpac/pdf/guidelines/bsiguidelines-011.pdf
12/11/2015 3 © 2015 Pennsylvania Patient Safety Authority
Caution from the CDC
• “Some studies have suggested that planned removal at 72 hours vs. removing as needed resulted in similar rates of phlebitis and catheter failure.”
• “However, these studies did not address the issue of [PVCRI], and the risk of [PVCRI] with this strategy is not well studied.”
Centers for Disease Control and Prevention. Guidelines for the prevention of intravascular-related infections, 2011[online]. 2011 [cited 2013 Nov 1] http://www.cdc.gov/hicpac/pdf/guidelines/bsiguidelines-011.pdf
12/11/2015 4 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
3
The Infusion Nurses Society (INS)
• In 2006, recommended IV site rotation at least every 72 hours.
• In 2011, recommend that site rotation of the short peripheral catheter be based on clinical indication.
Infusion Nurses Society. Infusion nursing standards of practice. J Infus Nurs 2011;34(1 Suppl):S1-S110.
Infusion Nurses Society. Infusion nursing standards of practice. J Infus Nurs 2006 Jan-Feb;29(1 Suppl):S1-92.
12/11/2015 5 © 2015 Pennsylvania Patient Safety Authority
INS’s Rationale
• INS identified the primary reference for the change in recommendations to be a meta-analysis of five trials that showed changing the catheter every three days did not reduce the risk of infection.
Webster J, Osborne S, Rickard CM, et al. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst Rev 2010 Mar 17;(3):CD007798.
12/11/2015 6 © 2015 Pennsylvania Patient Safety Authority
12/11/2015
4
The Opposition
• Collignon: “in 90% of all PVC sepsis cases, the catheter was in place for three days or more.”
• Trinh et al.: stressed that “PVC-related bacteremia due to S. aureus is an unrecognized complication of PVC use over time.”
• Maki: “abandoning scheduled replacements may not greatly increase the incidence of phlebitis and infiltration, it would probably increase the risk of catheter related bacteremia with Staphylococcus aureus.”
Collignon PJ. Intravascular catheter associated sepsis: a common problem. Med J Aust 1994 Sep 19;161(6):374-8. Trinh TT, Chan PA, Edwards O, et al. Peripheral venous catheter-related Staphylococcus aureus bacteremia. Infect Control Hosp Epidemol 2011 Jun;32(6):579-83. Maki DG. Improving the safety of peripheral intravenous catheters. BMJ 2008 Jul 8;337:a630.
12/11/2015 7 © 2015 Pennsylvania Patient Safety Authority
We Have Some Questions…
• Is it safe to leave a PVC in place until there is a clinical indication for removal?
• Is there a time in hours that a PVC could be re-sited that would likely reduce the risk of PVCRI?
12/11/2015 8 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
5
Looking for a Surrogate Measure
• The National Healthcare Safety Network (NHSN) has no bacteremia criterion for PVCRI.
• Primary bloodstream infection criteria is not specific in terms of source when compared to central line infection criteria.
• S. aureus is the second most common cause of hospital-acquired BSI.
Hidron AI, Edwards JR, Patel J, et al.; National Healthcare Safety Network Team; Participating National Healthcare Safety Network Facilities. NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of the data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006- 2007. Infect Control Hosp Epidemiol 2008 Nov;29(11):996-1011.
12/11/2015 9 © 2015 Pennsylvania Patient Safety Authority
Looking for a Surrogate Measure
• PVCRI related to Staphylococcus aureus (S. aureus) may be as high as 23.5% – 45.2% of PVCRIs related to S. aureus were found in
patients for which the PVC had a dwell time of ≥4 days.
• In the United States, almost 200 million PVCs are used each year.
Stuart RL, Cameron DR, Scott C, et al. Peripheral intravenous catheter-associated Staphylococcus aureus bacteremia: more than 5 years of prospective data from two tertiary health services. Med J Aust 2013 Jun 3;198(10):551-3.
Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc 2006 Sep;81(9):1159-71.
12/11/2015 10 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
6
12/11/2015 11 © 2015 Pennsylvania Patient Safety Authority
Davis, J. Peripheral Vascular Catheter–Related Infection: Dwelling on Dwell Time Pa Patient Saf Advis 2014 Mar;11[1]:30-5.
12/11/2015 12 © 2015 Pennsylvania Patient Safety Authority
Davis, J. Peripheral Vascular Catheter–Related Infection: Dwelling on Dwell Time Pa Patient Saf Advis 2014 Mar;11[1]:30-5.
12/11/2015
7
12/11/2015 13 © 2015 Pennsylvania Patient Safety Authority
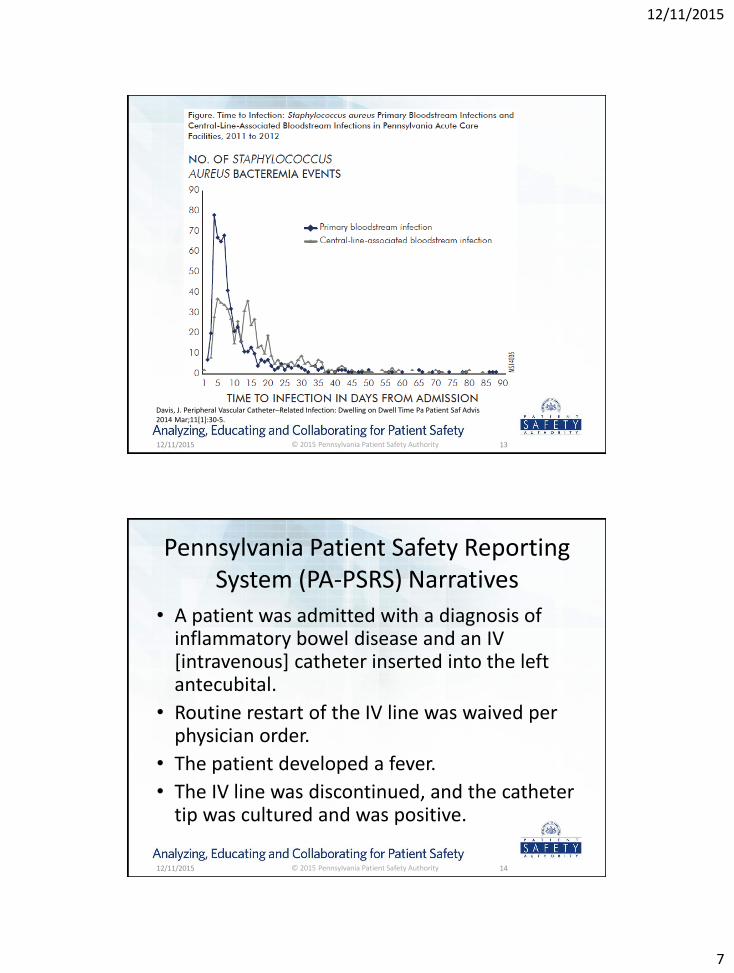
Davis, J. Peripheral Vascular Catheter–Related Infection: Dwelling on Dwell Time Pa Patient Saf Advis 2014 Mar;11[1]:30-5.
Pennsylvania Patient Safety Reporting System (PA-PSRS) Narratives
• A patient was admitted with a diagnosis of inflammatory bowel disease and an IV [intravenous] catheter inserted into the left antecubital.
• Routine restart of the IV line was waived per physician order.
• The patient developed a fever.
• The IV line was discontinued, and the catheter tip was cultured and was positive.
12/11/2015 14 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
8
PA-PSRS Narratives
• Blood cultures were identified with Staphylococcus epidermidis and Staphylococcus aureus.
• Phlebitis was noted on left forearm from old IV catheters.
12/11/2015 15 © 2015 Pennsylvania Patient Safety Authority
PA-PSRS Narratives
• Forearm IV line was in for five days; [when it was] removed, [there were]no signs of infection at that time.
• The next day, the site was red and had a small pocket of pus.
• Site and blood cultures were positive for staph.
12/11/2015 16 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
9
PA-PSRS Narratives
• The patient with chronic ESRD [end-stage renal disease] was on hemodialysis.
• The patient developed respiratory failure prior to cardiac catheterization and was febrile with positive blood cultures.
• [The patient was]diagnosed with peripheral IV catheter bacteremia.
12/11/2015 17 © 2015 Pennsylvania Patient Safety Authority
PA-PSRS Narratives
• A patient was admitted with A-Fib [atrial fibrillation]. • IV catheter #18 inserted at left antecubital space. • Four days later, the site was found to be red and tender. • The IV line was removed. • The patient was started on antibiotics. • The IV catheter tip was sent for culture. • The culture tip and blood were positive for Staphylococcus. • Patient was for pacemaker insertion. • The infectious-disease physician was consulted. • Antibiotics were started, and pacemaker insertion was put
on hold for three days.
12/11/2015 18 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
10
In Reality
• Waiting for a clinical indication of infection to re-site a PVC may place the patient in a position for the development of bacteremia due to prolonged dwell times.
12/11/2015 19 © 2015 Pennsylvania Patient Safety Authority
A Consideration
• Conduct focused surveillance for PVCRI to determine if re-siting peripheral catheters in adult patients every 72 hours is advantageous to re-siting when clinically indicated.
12/11/2015 20 © 2015 Pennsylvania Patient Safety Authority

12/11/2015
11
Moving to Clinically Indicated PIV Replacement vs. Scheduled Replacement
…thinking it through!
Marcia Ryder PhD MS RN
RYDER SCIENCE, Inc …..medical biofilm research
21 12/11/2015
CDC Guidelines (USA 2011)
• There is no need to replace peripheral catheters more frequently than
every 72-96 hours to reduce the risk of infection and phlebitis in adults IB
• No recommendation is made regarding replacement of peripheral
catheters in adults only when clinically indicated unresolved issue
• Replace peripheral catheters In children only when clinically indicated IB
Epic3: National Evidence-Based Guidelines (England 2014)
• IVAD 28: Peripheral vascular catheter insertion sites should be re-sited
when clinically indicated and not routinely, unless device-specific
recommendations from the manufacturer indicate otherwise. Class B
Infusion Nursing Standards of Practice (USA 2011)
• The nurse should consider replacement of the short peripheral catheter
when clinically indicated and when infusion treatment does not include
peripheral parenteral nutrition I
• The nurse should not routinely replace short peripheral catheters in
pediatric patients IV
22 12/11/2015

12/11/2015
12
the goal of this session is to…
• to assist the clinician to critically evaluate the
risks and benefits of the clinically indicated PIV
replacement standard before implementation
• to present a process model for a safe and
effective transition of practice
23 12/11/2015
evidence-based practice
• evidence-based practice is a problem-solving
approach to the delivery of health care that
integrates:
the best evidence from studies and…..
Stillwell SB, et al. AJN. 2010;110:58
24
patient care data with…..
clinician expertise and…..
patient preferences and values.
12/11/2015

12/11/2015
13
what does the evidence tell us?
objective: to assess the effects of removing peripheral IV catheters when clinically indicated (CIR) compared to removing and re-siting the catheter routinely (RR)
method: review randomized controlled trials (7) that compared RR to CIR of PIV catheters in hospitalized or community dwelling patients receiving continuous or intermittent infusions
Webster J, et al. Cochrane Database of Systematic Reviews. 2015;8:1-43
25 12/11/2015
conclusions: • the review found no evidence to support changing catheters every 72-96 hours
• this would provide significant cost savings
• would spare patients the unnecessary pain of routine re-sites in the absence of clinical indications
• consequently, healthcare organizations may consider changing to a policy whereby catheters are changed only if clinically indicated
• to minimize PIV-related complications, the insertion site should be inspected at each shift change and catheter removed if signs of inflammation, infiltration, or blockage are present
26
what does the evidence tell us?
12/11/2015

12/11/2015
14
single center hospital
Webster Webster Rickard
2007 2008 2010
Royal Brisbane
and Women’s Hospital
Queensland
Royal Brisbane
and Women’s Hospital
Queensland
Launceton General Hospital
Tasmania
examine the data
sample • setting
Latrobe Regional Hospital
Homecare Victoria
community
Van Donk
2009
Royal Brisbane
and Women’s Hospital
Queensland
Princess Alexandra Hospital
Queensland
Gold Coast
Hospital Queensland
multicenter
Rickard
2012
27 12/11/2015
methods • insertions, assessments, decisions
Insertions by
• IV Team (100%)
Insertions by
IV Team (75%)
Sites
inspected daily by
• IV Team
Insertions by RNs MDs
and IV Team
• (2 hosp) (40%)
Insertions by RNs MDs
Assessments, decisions by
staff
Insertions by RNs MDs
Assessments, decisions by
homecare RN and PI
single center hospital community multicenter
Webster Webster Rickard Van Donk Rickard
2007 2008 2010 2009 2012
examine the data
28 12/11/2015
12/11/2015
15
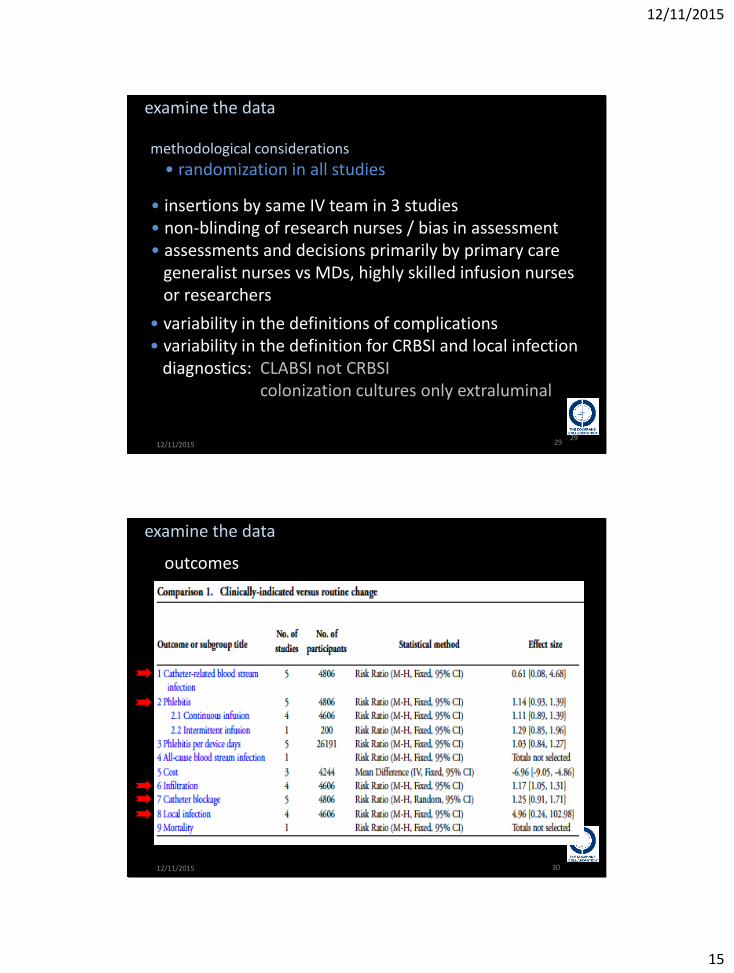
examine the data
methodological considerations
• randomization in all studies • insertions by same IV team in 3 studies • non-blinding of research nurses / bias in assessment • assessments and decisions primarily by primary care generalist nurses vs MDs, highly skilled infusion nurses or researchers
• variability in the definitions of complications • variability in the definition for CRBSI and local infection diagnostics: CLABSI not CRBSI colonization cultures only extraluminal
29 29 12/11/2015
examine the data
outcomes
30 12/11/2015

12/11/2015
16
phlebitis
examine the data
outcomes: phlebitis
p = 0.20
risk ratio statistical likelihood of having the event confidence interval range of value for the population mean
p value probably that the null hypothesis is true Total events
CISC RR 186 166
Forest Plot
31 12/11/2015
total events CISC RR 186 166 518 452
p = 0.004
examine the data
outcomes: infiltration
32 12/11/2015

12/11/2015
17
examine the data
outcomes: catheter blockage total
events CISC RR 186 166 518 452 398 377 1102 990
p = 0.16
33 12/11/2015
examine the data
outcomes: local infections
p = 0.30
confidence interval range of value for the population mean
34 12/11/2015

12/11/2015
18
examine the data
outcomes
• underpowered
• diagnosis
• non-blinding
• generalizability?
0.06%
35 12/11/2015
examine the data
72 hospitals no iv teams
• generalizability
Wischnewski N, et al. Zent.bl. Bakteriol. 1998;287:93-103
36 12/11/2015

12/11/2015
19
examine the data
Wischnewski N, et al. Zent.bl. Bakteriol. 1998;287:93-103
37 12/11/2015
staphylococcus aureus PIV bloodstream infection
• SA is the second most common cause of hospital-acquired bloodstream infection • SA (including MSSA and MRSA) is the primary causative organism for PIV-CRBSI
• pathogenesis is the same as CVC-CRBSI
• diagnosis & treatment is lengthy and very costly • high risk for disseminated infection $$$$ complicated bacteremia endocarditis prosthetic joint infection ascitic fluid infection empyema arthritis • mortality 27%
Gosbell IB. Internal Med J. 2005;35:S45-S62
$$
$$
$$
$$
$$
$$
$$
$$
$$
38 12/11/2015

12/11/2015
20
examine the data
author
Collignon Australia 1998- 7% 38% 6% 90% > 3 days no 2007 2005
country % SA-CRBSI PIV CVC PICC
rate PIV CVC
time to Infection (range)
ER placed
IV team
PIV Δ
dates
Pujol Spain 2001- 65% 0.19 0.18 mean 4.9 days 42% no CISC 2007 2003 per 1000 pt days (1.3-8.9)
Boyd UK 2007- 10% 72h 2011 2008
Heinrich Germany 2012 26% medical 2013 students
Stuart Australia 2007- 24% 8% 10% MRSA mean 3.5 days 39% 2013 2012 23% (0.25-9) median 3 days 45% > 4 days
39 12/11/2015
Trinh USA 2005- 12% 0.07 mean 3 days 67% no 2011 2008 per 1000 (2-6 days) cath days 42% median 4 days complicated (2-7 days) 46% > 3 days
examine the data
author country % SA-CRBSI PIV CVC PICC
rate PIV CVC
time to Infection (range)
ER placed
IV team
dates
Collignon PJ, et al. MJA. 2007;10:551-4
Stuart RL, et al. MJA. June 2013.10:551
Trinh TT, et al. ICHE. 2011;32:579-83.
Boyd S, et al. J Hosp Infect. 2011;72:37-41.
Pujol M, et al. J Hosp Infect. 2007;67:22-9.
Heinrich I, et al. GMS Hygiene Infectt Control. 2013;8:2196-5226
all patients except
catheters inserted in ER
Δ p 24h
multicenter
Rickard
2012
40 12/11/2015

12/11/2015
21
examine the data
Ge
rman
y
Spai
n
UK
USA
Kaasch AJ, et al. J Infect. 2014;68:242-51
2006-2011 3395 patients 20 tertiary care centers
41
USA
UK
Spai
n
Ger
man
y
12/11/2015
examine the data
Davis J. Pa Patient Saf Advis. March 2014;11(1):30-5
conclusion
sample size: • 1,890 events
• “when the epidemiological links of time to infection are combined with the definition of primary BSI, and when the sheer prevalence of the PIV is considered, it is likely that the majority of acute care adult primary BSIs are due to PIV-CRI”
42 12/11/2015

12/11/2015
22
examine the data
Ray-Barruel G, et al. J Eval Clin Practice. 2014;20:191-202.
purpose • identify the measures used in infusion phlebitis assessment and evaluate evidence regarding their reliability, validity, responsiveness and feasibility conclusion • many scales exist, but none has been thoroughly validated for use in clinical practice • a lack of consensus on phlebitis measures has likely contributed to disparities in reported phlebitis incidence, precluding meaningful comparison of phlebitis rates
• definitions
43 12/11/2015
examine the data
• diagnosis
Helm RE, et al. JIN. 2015;38:189-203
Mermel LA. Clin Infect Disease. 2009;49:1-45 44 12/11/2015

12/11/2015
23
examine the data
• clinical diagnosis
phlebitis erythema pain tenderness edema warmth streak formation palpable venous cord purulent drainage
infection erythema edema pain warmth purulent drainage
Sanchez KT. Scand J Infect Disease. 2012;44:551-4
Mermel LA. Clin Infect Disease. 2009;49:1-45 45 12/11/2015
• this would provide significant cost savings
Stuart: PIV-SAB total cost $4.04 million
Helm RE, et al. JIN. 2015;38:189-203
p = 0.00001
Stuart RL, et al. MJA. June 2013.10:551
cost of time & materials cost of complication
conclusion
46 12/11/2015

12/11/2015
24
conclusion
• would spare patients the unnecessary pain of routine re-sites in the absence of clinical indications
neither pain nor satisfaction were measured in any of the reviewed studies
….patient preferences and values • patient dissatisfaction with the venipunture skill level 1996 - 18% 2003 - 58%
• 40% success rate with first canulation attempt
• on average, each peripheral catheter requires 2.1 catheters
• 27% patients suffer 3 or more attempts
Barton A, et al. J Nurs Care Quality. 1998;13:77-85
Kokotis K. JIN. 2005;28:522-32
Wolosin RJ. Press Ganey Satisfaction Report. 2003;VII:2-4
Robinson-Reilly M, et al. Support Care Cancer. 2015;1-7
• quality improvement: vascular access team
47 12/11/2015
Helm RE, et al. JIN. 2015;38:189-203
• consequently, healthcare organizations may consider changing to a policy whereby catheters are changed only if clinically indicated
• up to 90% of catheters fail before completion of therapy
conclusion
48 12/11/2015
12/11/2015
25
conclusion
• to minimize PIV-related complications, the insertion site should be inspected at each shift change and catheter removed if signs of inflammation, infiltration, or blockage are present
• this policy most likely will not reduce the incidence of catheter failure
49 12/11/2015
thinking points:
from the Cochrane review…. • there is considerable imprecision around the measures for local infection, CRBSI and mortality outcomes giving a high level of uncertainty in the measures
• multidisciplinary vascular access teams need professional development
• the incidence and rate of catheter failure is unacceptably high
from the literature…..
• on-going PIV surveillance is needed
• PIV infection diagnostics (intra and extraluminal) need definition and protocol
• sterile technique for PIV insertion must be considered and evaluated
sound theoretical rationale…..
50 12/11/2015

12/11/2015
26
• evidence-based practice is a problem-solving approach
to the delivery of health care that integrates:
the best evidence from studies and…..
patient care data with…..
clinician expertise and…..
patient preferences and values.
Stillwell SB, et al. AJN. 2010;110:58
how can we do this?
reduce peripheral IV catheter failure through a patient focused quality improvement initiative
51
clinically indicated site change or not…….
quality improvement in peripheral vascular access is the challenge!
12/11/2015
Bennett B, Provost L. QP. July 2015;110:36-43 www.qualityprogress.com
52 12/11/2015

12/11/2015
27
quality improvement in vascular access
outcome primary secondary specific change change model for
drivers drivers ideas concepts improvement
provide
patient
focused
quality
care in vascular access
patient
focused
quality
Improvement
program
professional organization,
administration recognition and support
vascular access patient safety
initiative
establish quality
improvement project by
vascular access team
key leverage points
in the system
specific ideas, concepts and bundles that could generate the desired state
Ryder M. AVA 2015
53 12/11/2015
outcome primary secondary specific change change model for
drivers drivers ideas concepts improvement
focused surveillance
Create formal process
Establish focused quality improvement program
1.Standardize surveillance definitions
2.Conduct point prevalence survey
3 Establish surveillance/reporting/feedback
system
4 Revise documentation form
reduce
PIV
failure
professional competency
pathogenesis-based
protocols/procedures
technology assessment
diagnosis/treatment protocols
vascular access team
infection prevention
collaboration
specialist vs. generalist
generalist competency
revision insertion protocols/technol
ogy
revision complication
diagnostic/treatment criteria
revision post- insertion protocols
/technology
5. Establish surveillance/reporting system
6. Establish VAT serving all VAD patients
7. Staff education program
8. Staff competency assessment
9 Early assessment/device selection program
10. Pain management protocols
11. Insertion checklist
12. Surgical site antisepsis
13. Aseptic (sterile) technique
14. Ultrasound-guided insertion
15. Insertion site CHG-containing dressing
16. Liquid adhesive/adhesive remover
17. Post-insertion site care/dressing protocol
18. IV filtration
19. Antimicrobial/anticoagulant lock/flush
20. Antireflux/low bacteria transfer connector
21. Access site disinfection/scrubbing
22. Daily check for necessity
23. Revision diagnostic criteria
24. Phlebitis/infection protocols
Investment in quality,
patient satisfaction,
cost reduction
Focus on outcomes
Ryder M. AVA 2015
54 12/11/2015

12/11/2015
28
Questions?
55
Like the Authority on Facebook
12/11/2015 © 2015 Pennsylvania Patient Safety Authority



























