Embed Size (px)
Citation preview

REDUCING HEALTHCARE COSTS AND IMPROVING PATIENT HEALTH: LEVERAGING THE AFFORDABLE CARE ACT TO
ADDRESS THE GROWING DIABETES EPIDEMIC
by
Meredith Dyer
A thesis submitted to Johns Hopkins University in conformity with the requirements for
the degree of Master of Arts in Government
Baltimore, Maryland
August 2015
© 2015 Meredith Dyer All Rights Reserved
Abstract
The enactment of Patient Protection and Affordable Care Act (ACA) of 2010
marks the largest shift in U.S. healthcare delivery since the enactment of Medicare and
Medicaid. High costs of care, poor access to health insurance, and a lack of efficiency in
healthcare delivery required comprehensive reform in order to address these problems.
While the passage of the ACA was an intensely divisive and partisan process, its
implementation has the potential to achieve these goals by restraining discriminatory
insurance practices, making coverage more affordable, and implementing new care
models that improve quality, reduce costs, and use integrated approaches to healthcare
delivery.1
As chronic disease is a key driver of healthcare costs and poor patient outcomes,
this thesis will discuss the extent to which key provisions in the ACA can address the
growing diabetes epidemic in America. The first chapter of this thesis lays the
groundwork for the necessitation of healthcare reform and how rising healthcare costs
and rates of the uninsured have further contributed to an already broken system. This
analysis will discuss how the implementation of the ACA will attempt to address these
problems. The second and third chapters will discuss specific provisions in the ACA that
address diabetes prevention and treatment which, if fully scaled, have the potential to
significantly reduce healthcare expenditures. This thesis will conclude that the
implementation of the ACA has reduced the rates of the uninsured and has improved
access to low-cost, preventive services that can improve the overall population health.
1 Frederic E. Shaw, et al. “The Patient Protection and Affordable Care Act: Opportunities for Prevention and Public Health,” The Lancet 384, no. 14 (2014): 75.
ii

This thesis will further conclude that additional research and refinement will be needed
to understand if new healthcare delivery models can improve care for patients with
diabetes while also reducing costs.
Thesis Readers: Dorothea Wolfson Thomas Stanton
iii

Table of Contents Abstract………………………………………………………………………………………………………..……ii
Table of Contents…………………………………………………………………………………………......iv
Introduction…………………………………………………………………………………………………...…1
Addressing America’s Broken Healthcare System……………………………………………..12
Leveraging Prevention and Public Health Programs to Improve Diabetes Care…38
Reducing Costs and Improving Care for Patients with Diabetes…………………..……65
Conclusion ……………………………………………………………………………………………………….92
Bibliography…………………………………………………………………………………………..……….104
Curriculum Vitae…………………………………………………………………………………………....115
iv
Introduction
The passage of the Affordable Care Act (ACA) in 2010 marked the largest shift in
health policy since the implementation of Medicare and Medicaid. While the passage of
this landmark legislation was an intensely divisive and partisan process, its
implementation has ushered in the following reforms thus far: enhancing access to
health insurance for millions of Americans, restraining discriminatory insurance
practices, improving affordability of insurance coverage, and implementing new care
models that improve quality and reduce costs.2 Through these efforts, by 2017 it is
anticipated that more than 25 million Americans will be afforded coverage who could
not previously obtain insurance.3 Despite these reforms to the health care system,
fundamental issues surrounding chronic diseases, like diabetes, still need to be
addressed in order to truly make the ACA a success. The ACA provides a critical
opportunity to slow the progression of the diabetes epidemic while also bolstering
reform efforts. Evaluating provisions included in the ACA that address chronic disease
prevention and new care models to treat these patients can provide insight into how
the implementation of the ACA can be leveraged to reduce the incidence of diabetes
and its resulting costs to the United States healthcare system.
Currently, there are more than 26 million Americans who have been diagnosed
with diabetes and an additional 86 million who are projected to have prediabetes.4 This
disease alone accounts for $245 billion in direct and indirect medical costs to the U.S.
2 Frederic E. Shaw, et al. “The Patient Protection and Affordable Care Act: Opportunities for Prevention and Public Health,” The Lancet 384, no. 14 (2014): 75. 3 David Blumenthal and Sara Collins. “Health Care Coverage under the Affordable Care Act—A Progress Report,” The New England Journal of Medicine 371(2014):275. 4 National Diabetes Statistics Report 2014. (Atlanta, GA: Centers for Disease Control and Prevention, 2014).
1
healthcare system each year.5 Several key provisions included in the ACA have the
potential to reduce the economic burden of diabetes by preventing and effectively
treating this disease. These programs, however, must be coordinated and fully scaled in
order to achieve the necessary change. The aim of this research is to comprehensively
evaluate the diabetes healthcare crisis and the extent to which the ACA can provide
solutions to this growing problem.
Before the passage of the Affordable Care Act, nearly 2 million patients with
diagnosed diabetes lacked health insurance.6 These individuals were less likely to obtain
prescriptions, make an office visit to a physician, or have a source for care.7 High costs
of care and medications to prevent disease progression further exacerbated failures to
seek treatment for this disease, resulting in unnecessary hospitalizations and
complications.8 While the disease can be prevented, it is essential for diabetes to be
detected and treated early. However, due to the aforementioned problems with access
and cost, it is not surprising that the highest rate of undiagnosed diabetes is found
among those who are uninsured.9
The ACA includes a number of provisions to expand access to care and to
improve the health of individuals with diabetes. Since the implementation of these
provisions, the number of newly diagnosed individuals has increased significantly.10
Because of these diagnoses, effective treatment can delay the progression of the
5 Ibid. 6 Derek Brown and Timoth McBride. “Impact of the Affordable Care Act on Access to Care for U.S. Adults with Diabetes, 2011–2012,” Preventing Chronic Disease 12 (2015): 140431. 7 Ibid. 8Ibid. 9 Ibid. 10 Ibid.
2
disease—and in some cases even reverse it—which can prevent or reduce long-term
complications and hospitalizations11. For example, the expansion in coverage among the
Medicaid population has resulted in a 23% increase in individuals with newly identified
diabetes.12 By comparison, in those states that failed to expand the Medicaid program,
there was only a 0.4% increase in diabetes diagnoses.13 These figures clearly
demonstrate the critical relationship between increased insurance access and the
detection and treatment of diseases like diabetes.
While there are many aspects of why the ACA was needed to address the broken
healthcare system, this thesis will focus on aspects which impact patients with diabetes.
The first chapter will establish an understanding of why healthcare reform was needed
and how provisions included in the ACA can help improve access to the healthcare
system. Subsequent chapters will use diabetes as a case study to evaluate ways in which
the ACA can directly improve outcomes and reduce costs. This will be achieved by
discussing key sections of the ACA that have broad implications for diabetes care,
including national prevention provisions like the National Diabetes Prevention Program
and the development of new patient care models. These programs have demonstrated
the potential to reduce costs and improve care through team-based approaches,
increasing access to care and patient education. This analysis will detail how the
implementation of these programs will improve care and reduce long-term costs by
11 Brown, 140431. 12 Harvey W. Kaufman, et al. “Surge in Newly Identified Diabetes Among Medicaid Patients in 2014 Within Medicaid Expansion States,” Diabetes Care 38 (2015) 835. 13 Ibid.
3
both preventing and delaying the onset of diabetes and by reducing acute complications
that stem from this disease.
This thesis will conclude that through a coordinated strategy, provisions of the
ACA have the ability to reduce the incidence of diabetes in America by fully scaling
prevention efforts through coordinated care teams that can improve patient outcomes.
These efforts, if implemented properly, can also reduce healthcare expenditures
resulting from the diabetes epidemic which will help further reform our nation’s
healthcare system.
The Impact of Diabetes on the U.S. Healthcare System
The impact of diabetes on the U.S. healthcare system must be critically
evaluated in order for true reform efforts to take hold. According to the Centers for
Disease Control and Prevention (CDC), more than 26 million Americans have diabetes
and an additional 86 million have prediabetes.14 By 2020, it is anticipated that nearly
half of Americans will have diabetes or prediabetes.15 This disease is the 7th leading
cause of death in the United States which carries a 50 percent higher risk of death for
adults with the disease than for adults without it. 16 Medical costs for people with
diabetes are twice as high as for people without the disease.17 These individuals are also
14 National Diabetes Statistics Report 2014. (Atlanta, GA: Centers for Disease Control and Prevention, 2014). 15 The United States of Diabetes: Challenges and Opportunities in the Decade Ahead. (Washington, D.C., UnitedHealth Center for Health Reform & Modernization, 2010) 4. 16 Ibid. 17 Ibid.
4

at a higher risk for serious complications such as blindness, kidney failure, heart disease,
stroke, and amputation.18
While the scope of this epidemic is massive, Americans continue to be ill-
informed about diabetes and the need to be screened when potential risk factors, like
being overweight, arise. In fact, one in four Americans do not know that they have the
disease and 9 out of 10 do not know that they have prediabetes.19 Poor access to
primary care physicians due to workforce shortages, a lack of insurance, as well as the
stigma attached to being overweight are only a few reasons for this failure. However,
with direct medical costs estimated to be $176 billion annually with an additional $69
billion in indirect costs like disability, work loss, and premature death, education and
prevention efforts to elevate the importance of this disease are critical to address this
issue.20 These costs marked a 41 percent increase over a 5-year period, costs that are
expected to continue to rise in the future.21
The role of diabetes cannot be underestimated when evaluating insolvency of
healthcare and its impact on the American economy. One in ten healthcare dollars can
be directly attributed to diabetes.22 More than 40 percent of these expenditures come
from increased hospital admission rates and longer-than-average lengths of stay which
is the greatest contributor to medical costs of diabetes.23 In fact, of the $475 billion in
national expenditures for hospitalizations, 26 percent can be attributed to diabetes.24 Of
18 Ibid. 19 Ibid. 20 The United States of Diabetes: Challenges and Opportunities in the Decade Ahead, 4. 21 Ibid. 22 Wenya Yang, et al. “Economic Costs of Diabetes in the U.S. in 2012,” Diabetes Care, 35 (2013): 1033. 23 Ibid. 24 Ibid.
5

the $286 billion in national costs for medications, 27 percent ($77 billion) is incurred by
patients with diabetes.25 Among the Medicare population, these figures are even more
dramatic because costs and complications continue to increase as the patient ages and
their disease worsens. Total spending for Medicare beneficiaries amounted to 60
percent of all health systems expenditures—costs that are expected to increase as the
Baby Boomer population continues to age into Medicare.26
While the costs of diabetes to the healthcare system are staggering, many of
these costs can be avoided through efforts to improve patient compliance and
adherence to medical treatments. The implementation of the ACA provides a key
opportunity to utilize federal resources to both improve public awareness of diabetes
and to implement prevention and treatment efforts that can reduce the costs of this
disease. To further analyze these issues, this thesis will evaluate the need for healthcare
reform and how provisions included in the ACA can help improve care and reduce costs
to the overall healthcare system.
Schools of Thought
To contextualize the impact that ACA could have on patients with diabetes, it is
important to understand the diverging perspectives on how to best reform that nation’s
healthcare system. This debate has been a highly contentious issue which has been at
the forefront of American politics for more than a century. This is largely due to the fact
that millions of Americans have been unable to afford insurance coverage and
25 Ibid. 26 The United States of Diabetes: Challenges and Opportunities in the Decade Ahead, 4.
6
healthcare costs have risen to a level that is unsustainable. Because of the poor access
to insurance and the rising healthcare costs, there has been widespread agreement that
some type of reform was needed. However, the costs and mechanisms to achieve these
changes have been very divisive. In examining this conflict in ideology, two main schools
of thought have emerged: those who believed reform could be achieved through
indirect savings and federal intervention (ACA proponents) and those who believed
savings should be achieved directly by reducing government intervention and increasing
market choice (free market capitalists).
To increase access to affordable insurance, ACA proponents argued that federal
oversight was necessary to effectively scale reform efforts. This school of thought
believed that if every American had health insurance, uncompensated costs would
decrease and more individuals would utilize preventive services that would keep them
healthier and lower healthcare expenditures in the long run. To achieve this, ACA
proponents support the development of healthcare exchanges to help form a collective
that would lower the cost of insurance for those who did not have similar access
through their employer. Proponents also believed that federal programs like Medicare
and Medicaid should be expanded and reformed to increase access to these services
and to address the unsustainable rise in costs. These proponents argue that change
could be best achieved through savings mechanisms that address failures of healthcare
delivery that drive up costs. These failures include poor care coordination,
overtreatment, and fraud and abuse that can be addressed through new care models
and federal oversight that can identify wasteful spending. These savings mechanisms
7
also emphasize preventive care by enhancing care coordination and wellness services
that prevent individuals from getting sick rather than defensive medicine. For patients
with diabetes, preventive services and care coordination are critical components to
ensuring that costly complications and hospitalizations do not occur.
Free market capitalists, on the other hand, believe that federal oversight of
healthcare reform would lead to rising costs that would further impede access, add to
the national debt, and employ onerous regulations that would negatively impact small
businesses and job growth. This largely conservative school of thought believes that
greater market choice and market competition would help drive costs down and
therefore increase access to health insurance. The free market capitalist approach
utilizes direct savings to reduce costs and emphasizes ways in which to lower the
national debt by reducing expenditures. These direct savings mechanisms include
lowering payments for services, capping Medicare and Medicaid payments, and shifting
costs away from federal programs to the beneficiary through cost-sharing. Deregulation
of healthcare through the privatization of government sponsored programs like
Medicare and Medicaid would also be supported by this approach. To achieve this,
these programs would transition into premium-support models with defined
contribution financing and would utilize a more targeted, need-based subsidy with
market pricing.27 While this may reduce costs, it is also risky as individuals may not be
able to afford cost-sharing and because providers may withdraw from federal programs
due to lower payments. As a result, if implemented improperly, privatizing these
27 Tom Miller. “Conservative Health-Care Reform: A Reality Check,” National Affairs 17 (2013): 12.
8
programs could further exacerbate an already difficult access to care problem in
America due to the uninsured.
While there continues to be disagreement about the best approach in which to
reform the U.S. healthcare system, these perspectives can help inform tactics to address
chronic diseases, like diabetes. Both the free market capitalists and the ACA-proponents
agree that individuals with chronic disease need access to care to avoid costly, life-
threatening complications. There is also agreement that addressing this issue through
prevention and effective treatment would help reduce costs. However, these schools of
thought continue to diverge on the best approach to achieve this change. ACA
proponents encourage the development of prevention programs and strategies to
thwart the progression of chronic diseases like diabetes. These services require
additional expenditures in the short-term. Free market capitalists, on the other hand,
discourage additional expenditures on these programs as they add to the national debt.
Instead, they would encourage the development of new delivery models that emphasize
value-based approaches to care and involve some level of risk on the part of the
provider to help promote quality and efficiency.
Road Map
This thesis will evaluate the aforementioned perspectives on why the ACA was
needed and how reform efforts can be leveraged to increase access to affordable
healthcare while reducing costs through new delivery models. This portfolio will delve
deeper into these issues by assessing the potential for healthcare reform to impact
9
accessibility and cost reduction for diabetes as this disease is a key driver of growing
healthcare costs. The first chapter will discuss the necessitation of the ACA by reviewing
the history of large-scale reform efforts and how failures to achieve progress resulted in
a fragmented healthcare system. This chapter will also detail the causes behind the
rising rates of the uninsured and increasing healthcare costs to help frame the need for
reform. Providing this context will be critical in establishing problems with the
healthcare system and how the implementation of the ACA may address these issues.
The second chapter will examine how prevention efforts included in the ACA can
help improve access to care, thereby improving population health. This chapter will
utilize the diabetes epidemic as a case study to determine whether these prevention
efforts have the ability to achieve long-term reform and prevent the rise of chronic
disease in America. This case study will discuss why leveraging provisions in the ACA to
address diabetes will have a greater impact on healthcare expenditures than many
other conditions and how increasing access to care can help drive down costs.
Chapter three will evaluate ways in which the ACA can further generate savings
by streamlining approaches to healthcare delivery. The chapter will discuss the
implementation of new models that promote care coordination and patient-centered
approaches to evaluate whether healthcare delivery provisions included in the ACA can
help reduce costs. Reduction of wasteful spending will also be addressed to better
understand how the ACA intends to inhibit unnecessary spending that contributes to
the affordability problem of insurance coverage.
10

This thesis will conclude that the ACA has had an overall positive impact on
population health. The law has decreased the rates of the uninsured and has expanded
access to more comprehensive health plans that provide low- or no-cost preventive
services. Expansion of federal programs, like Medicaid, has increased coverage among
the most vulnerable populations; however, these programs will need to be fully scaled
in order to address coverage gaps that have resulted from some state failures to
implement the expansion. These provisions have improved access for patients with
diabetes and have the potential to reduce the incidence of the disease through
prevention and public awareness efforts. Furthermore, new healthcare delivery models
have demonstrated an ability to improve quality and reduce costs. However, data is
mixed as to whether these models can achieve both goals for patients with diabetes.
Therefore, this thesis will conclude that additional refinement of these models will be
needed to achieve the intended results.
11

Chapter One:
Addressing America’s Broken Healthcare System
The structure of the healthcare system has been a consistent issue of debate in
U.S. public policy throughout the 20th and 21st centuries. During this time, there have
been numerous proposals on how best to address the lack of insurance coverage.
Reform efforts have been incremental due to the economic implications and political
viability of large-scale reforms. As a result, the U.S. healthcare system has become
highly fragmented, consisting of a patchwork of public and private plans. This
incremental approach to reform has also led to large gaps in coverage, which have been
exacerbated by economic recessions, labor market shifts, and rising costs of health
care.28
The implementation of the Patient Protection and Affordable Care Act (ACA) is
the first large-scale effort to reform this broken system since the passage of Medicare
and Medicaid in 1965.29 This landmark legislation seeks to expand access to affordable
health insurance through a comprehensive approach to reducing costs and improving
the quality of healthcare delivery. To evaluate the extent to which the ACA can actually
achieve these goals, one must first understand how the healthcare system became
broken and what factors influenced the growing rates of the uninsured and the high
costs of care. This analysis will provide insight into access problems and growing
28 Beatrix Hoffman. “Health Care Reform and Social Movements in the United States,” American Journal of Public Health 93, no. 1 (2003): 76. 29 Ibid.
12
healthcare expenditures in order to understand whether the ACA provisions contained
in the ACA can effectively address these issues.
The History of Healthcare Reform
Throughout the past century, the structure of the U.S. healthcare system has
been an integral part of American public policy. The Industrial Revolution that emerged
in the late 19th century led to a rapid urbanization which caused a number of public
health problems.30 While America was an agrarian society in the mid-to-late 1800s, by
the turn of the century, nearly half of all citizens lived in urban areas.31 Because of
crowded housing and poor sanitary conditions in the cities, diseases spread rapidly
causing many to miss work and lose wages. During this time, illness was a major driver
of poverty in America. As a result, a number of public policies were proposed to help
protect workers and bolster public health. An employer-sponsored disability policy
emerged in 1911 to replace wages lost due to illness; however, this policy did not cover
medical expenses.32 The next year, Theodore Roosevelt endorsed a compulsory system
to protect workers from wage loss and medical expenses during his presidential run.33
By 1915, progressive reformers, the American Association for Labor Legislation,
demonstrated their support for this approach and put forth a model on which to base
this system.34 This universal system gained popularity in the progressive and socialist
movements (and among suffragists as well). However, businesses, insurance companies,
30 Hoffman, 77. 31 David Rosner. “Public Health in the Early 20th Century,” Public Health Reports 125, no. 3 (2010), 39. 32 Ibid. 33 Ibid 34 Hoffman, 78.
13
and conservative legislators were adamantly opposed to this concept, branding it
“Bolshevism.”35 As a result, calls for universal coverage soon lost momentum.
By the 1920s, medical care had become more effective and expensive,
particularly with the discovery of antibiotics.36 During this time, policies to improve
healthcare shifted away from universal medicine to proposals on group medicine and
voluntary insurance. These proposals were denounced as socialized medicine by the
American Medical Association and gained no popular support, however. By the time
that the Great Depression struck in 1929, there had been little progress in developing a
structure to provide insurance to Americans who became ill.37 As the depression
continued throughout the 1930s, popular social movements largely focused on
unemployment and healthcare issues took a backseat.38 During World War II, organized
labor emerged in support of national health insurance reinvigorating the healthcare
debate.39 While both Franklin Roosevelt and Harry Truman were supportive of this
issue, opposition from business leaders and the medical community again made passage
of such legislation unviable.40
The rise of unions in the 1950s was a turning point for health insurance that led
to one of the many fissures in the American healthcare system.41 Given failures by the
federal government to enact legislation to protect workers from medical expenses,
unions were utilizing collective bargaining agreements with employers to obtain health
35 Hoffman, 78. 36 Hoffman, 79. 37 Ibid. 38 Ibid. 39 Ibid. 40 Hoffman, 80. 41 Ibid.
14
benefits.42 This led to the rise of employer-sponsored, private health plans which
became increasingly prevalent and popular. Organized labor continued to support
universal coverage; however, the emergence of private plans made this issue less
urgent.43 Realizing that large-scale efforts were not politically viable, reformers utilized
a new approach to addressing health policy: incrementalism.
To avoid the barriers of passing a national health plan, reformers began focusing
on efforts to provide coverage to politically sympathetic populations like the elderly and
the poor. This incremental approach to expanding access to health insurance was
supported by John F. Kennedy, Lyndon Johnson, and by civil rights activists of that
time.44 Organized labor continued to support expansion in health care as negotiating
health benefits for union workers became increasing difficult.45 In 1965, the federal
government enacted the Medicare and Medicaid programs to provide health insurance
coverage to the elderly and to low-income, at-risk populations.46 This marked the
largest healthcare expansion of the 20th century which quieted movements calling for
more sweeping reforms. 47
The expansion in coverage created by the passage of Medicare and Medicaid
also increased the cost of healthcare, however. Additional pressure on physicians and
hospitals because of the additional access to insurance led to a massive increase in the
cost of healthcare services in the 1970s.48 These costs were further compounded by a
42 Ibid. 43 Oberlander, 586. 44 Ibid. 45 Ibid. 46 Hoffman, 80. 47 Ibid. 48 Ibid.
15

move by the federal government to provide tax exemptions on premiums for both
employers and employees.49 These exemptions eventually grew to be the government’s
third largest expenditure on healthcare after Medicare and Medicaid.50 By 2016, these
costs are estimated to grow to $260 billion.51 Because of these growing costs, calls for
national coverage expansion were replaced by those urging cost-containment. However,
the women’s health movement, including the passage of Roe vs. Wade, re-sparked calls
for improvements in public health and for universal coverage, noting that the majority
of the underinsured and uninsured were women.52 The emergence of AIDs by the 1980s
further bolstered calls for reform, which moved healthcare reform into the national
spotlight by the early 1990s.53
By the 1990s, the healthcare reform debate became increasingly contentious,
with opinions largely diverging along party lines. Conservatives supported a free market
approach to making insurance more affordable. President George H.W. Bush proposed a
plan to provide the poor with vouchers to purchase private health insurance and tax
credits for families with incomes up to $80,000.54 This proposal also included small
business pools and health insurance networks.55 Liberals, on the other hand, supported
universal coverage and reforms to federal programs to create more efficiency. President
Bill Clinton proposed the Health Security Act which proposed mandating coverage and
49 Johnathan Gruber and James Poterba. “Tax Incentives and the Decision to Purchase Health Insurance: Evidence from the Self-Employed.” The Quarterly Journal of Economics 109, no. 3 (1994): 701. 50 The National Bureau of Economic Research. Tax Breaks for Employer-Sponsored Health Insurance (Cambridge, MA: National Bureau of Economic Research, August 13, 2015). 51 Ibid. 52 Oberlander, 586. 53 Ibid. 54 Congressional Research Service. The President’s Health Care Reform Proposal (Washington, D.C.: CRS, March 5, 1992). 55 Ibid.
16
reforming managed care plans to take into account quality and cost control.56 These
schools of thought continued into the next decade and laid the groundwork for the
political environment and controversy surrounding the debate of the ACA in 2009-2010.
As the 1990s progressed, a number of reforms were implemented to expand
coverage to the uninsured. The Health Insurance Portability and Accountability Act of
1996 was enacted to prohibit the inclusion of pre-existing condition clauses for
individuals who changed their employer plans.57 The Balanced Budget Act of 1997
expanded coverage to children and families with incomes up to 200 percent above the
federal poverty level through the State Children’s Health Insurance Plan (SCHIP).58 As a
result of SCHIP, State Medicaid programs were required to cover children aged 6-18 in
families below the poverty level. While these laws did not comprehensively address
problems with the U.S. healthcare system, they did have a broader scope than those in
decades past. These efforts served as a primer for the possibility of a broader package
and kept healthcare at the forefront of public policy into the next century.
As efforts to reform the nation’s healthcare system moved into the 21st century,
political opinion became even more highly contentious and divisive. There was
widespread agreement that some action needed to be taken to address the more than
49 million Americans without insurance by 2010.59 However, the concept of passing a
large-scale, expensive piece of legislation during the largest economic recession since
the Great Depression was controversial. Democratic proponents of healthcare reform
56 Ibid. 57 Ibid. 58 Congressional Research Service, 1992. 59 The Department of Health and Human Services. Assistant Secretary for Planning and Evaluation Issue Brief. Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey. Washington, DC, 2014, http://aspe.hhs.gov/health/reports/2011/cpshealthins2011/ib.pdf (accessed July 1, 2015).
17

supported a universal option to ensure that all Americans had insurance coverage. As in
the 1920s, when the concept of universal coverage in America first arose, this idea was
met with a great deal of backlash by the conservative right. Republicans argued that
federal oversight of healthcare would result in a system riddled with inefficiency that
would further drive up the national debt. The opinion was largely supported by
business-owners who would be saddled with providing workers with additional
coverage at their own expense. Instead, conservatives argued that market competition
could reduce cost and make insurance more affordable. However, these conservatives
failed to offer a counter-proposal that was politically viable.
In sum, over the past century, there have been numerous, large-scale efforts to
expand coverage for Americans. However, due to economic implications and political
divisiveness, only a few of these proposals were enacted, thus necessitating an
incremental approach. This has resulted in a fragmented healthcare system consisting of
private, employer-sponsored insurance for working-age adults, Medicare for the elderly
and disabled, and Medicaid and SCHIP for economically disadvantaged adults and
children. While these coverage options work for many Americans, coverage gaps and
the lack of affordability have prevented millions of Americans from obtaining health
insurance. To understand these barriers, and therefore the necessitation of healthcare
reform, it is important to ascertain the scope of the uninsured problem and how the
aforementioned, incremental policy changes have impacted this lack of coverage.
18

The Necessitation of Healthcare Reform
The history of healthcare reform is critical in understanding the need for a
comprehensive approach to restructuring the nation’s healthcare system. However, it is
also important to assess how failures to enact large-scale legislation have contributed to
rising rates of the uninsured and to growing healthcare costs. By evaluating the
coverage gaps that developed through the emergence of private and public health
plans, as well as factors contributing to rising healthcare costs, one can better
understand the necessitation of comprehensive legislation to reform the nation’s
healthcare system.
Coverage Gaps
While federal efforts to reform healthcare were fragmented, those policies that
were enacted expanded coverage to a number of vulnerable populations. The passage
of Medicare and Medicaid in 1965 afforded coverage to the low-income and the
elderly.60 Subsequent legislation expanded access to these programs to at-risk
populations like pregnant women, children, and the permanently disabled.61 Collective
bargaining tactics employed by organized labor contributed to the rise of employer-
sponsored insurance that provided coverage to some working adults.62 However, unless
an individual was included in one of the at-risk populations or was employed by a
60 Beatrix Hoffman. “Health Care Reform and Social Movements in the United States,” American Journal of Public Health 93, no. 1 (2003): 76. 61 Ibid. 62 Ibid, 78.
19
company that offered an affordable plan, gaining access to insurance was difficult. As a
result, since the 1970s, the rate of the uninsured has steadily increased and, since that
time, 12-18% of the population has consistently been without insurance coverage.63
These coverage gaps were caused and exacerbated by a number of factors,
including cuts to public programs and restrictive policies employed by private insurers.
For example, private insurance plans, which determine whether to provide coverage
based on actuarial risks, could deny coverage or offer high-cost plans if an individual had
a pre-existing condition.64 Many individuals who were eligible for private insurance
could not afford it or simply could not access it. Coverage by employer-based insurance
plans also declined due to the economic recession and because of job market shifts
from manufacturing jobs that typically provided better coverage because of organized
labor negotiations.65 As a result, more individuals were uninsured or seeking coverage
through federal programs like Medicaid. During this time, cuts to federal programs
were also taking effect.66 In the Medicaid program, because of the economic recession,
programs that offered coverage to optional, at-risk populations landed on the chopping
block. Due to these factors, by 2010, 49 million Americans were uninsured.67
The growth in the number of uninsured Americans is highly problematic to
overall population health. Individuals without insurance are more likely to delay seeking
medical care, to report poor health, and to forgo care for potentially serious
63 Karen Davis. “Universal Coverage in the United States: Lessons from Experience of the 20th Century,” Journal of Urban Health 78, no. 1 (2001): 50. 64 Davis, 51. 65 Ibid. 66 Ibid. 67 Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey, 2014.
20
symptoms.68 As a result, they are more likely to be hospitalized for avoidable conditions
and face an increased risk of death.69 Because of the high cost of care, these individuals
also receive fewer screening and prevention services, which contribute to a greater
likelihood of being diagnosed with a disease at a later, and more costly, stage. In fact,
almost two-thirds of the increase in healthcare spending can be attributed to worsening
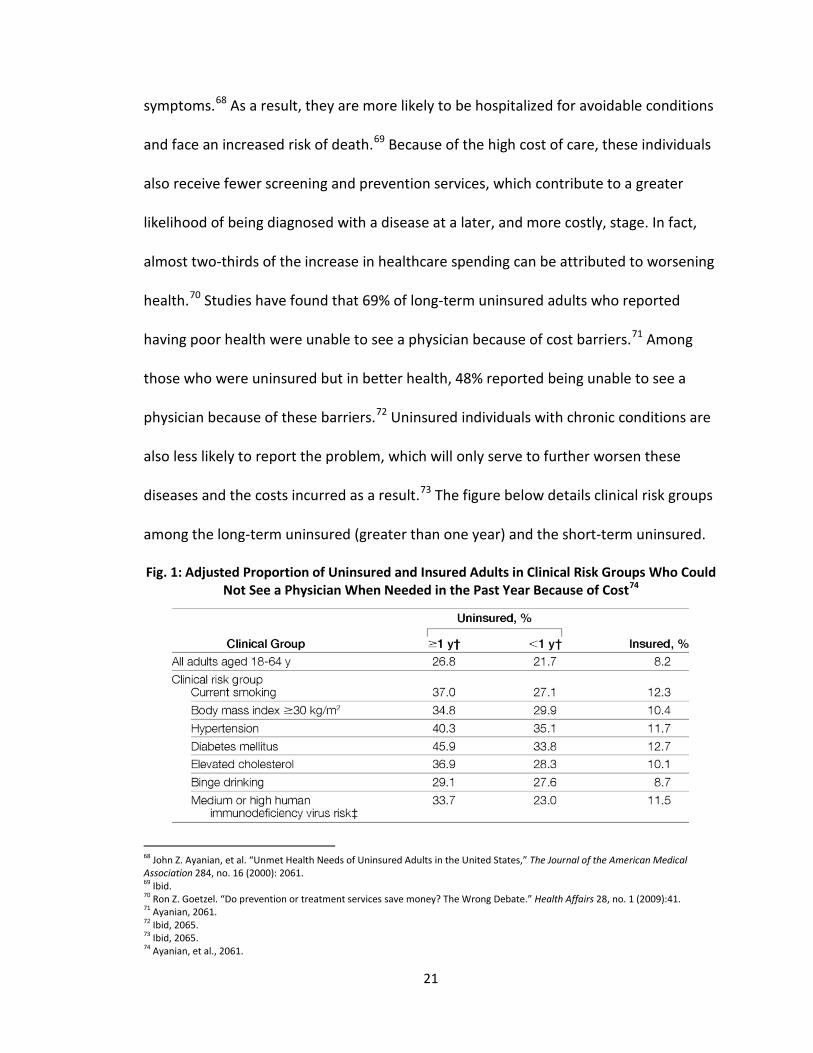
health.70 Studies have found that 69% of long-term uninsured adults who reported
having poor health were unable to see a physician because of cost barriers.71 Among
those who were uninsured but in better health, 48% reported being unable to see a
physician because of these barriers.72 Uninsured individuals with chronic conditions are
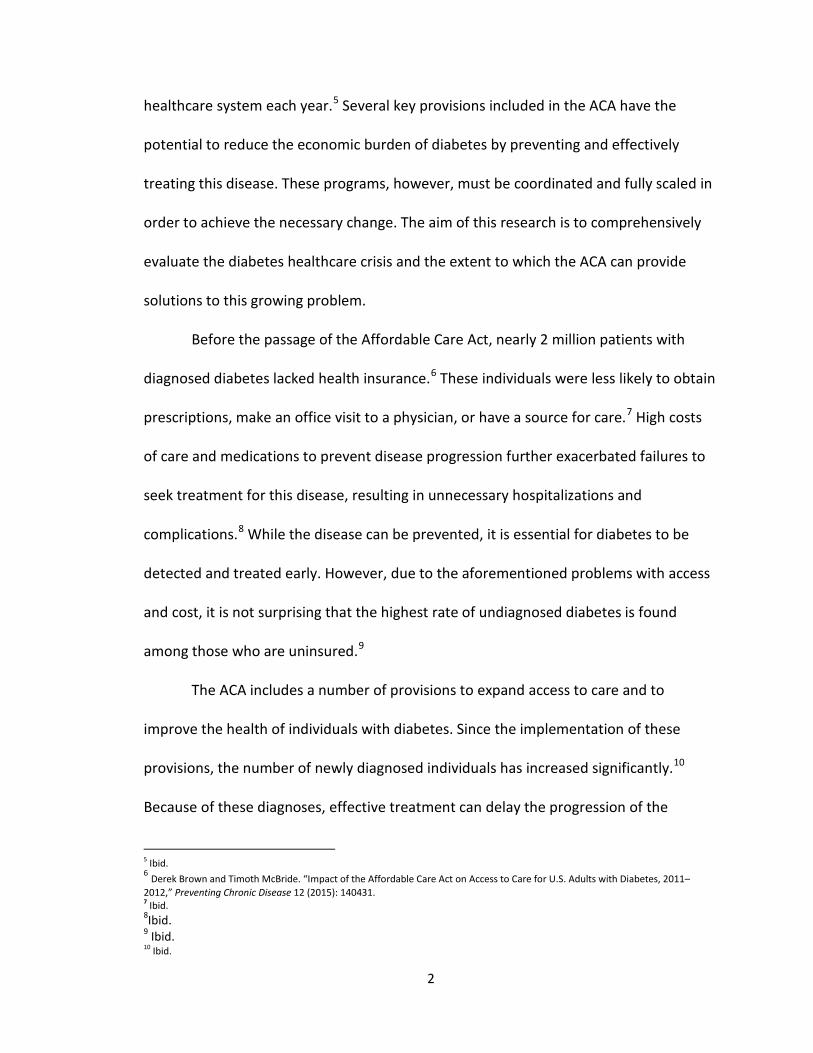
also less likely to report the problem, which will only serve to further worsen these
diseases and the costs incurred as a result.73 The figure below details clinical risk groups
among the long-term uninsured (greater than one year) and the short-term uninsured.
Fig. 1: Adjusted Proportion of Uninsured and Insured Adults in Clinical Risk Groups Who Could Not See a Physician When Needed in the Past Year Because of Cost74
68 John Z. Ayanian, et al. “Unmet Health Needs of Uninsured Adults in the United States,” The Journal of the American Medical Association 284, no. 16 (2000): 2061. 69 Ibid. 70 Ron Z. Goetzel. “Do prevention or treatment services save money? The Wrong Debate.” Health Affairs 28, no. 1 (2009):41. 71 Ayanian, 2061. 72 Ibid, 2065. 73 Ibid, 2065. 74 Ayanian, et al., 2061.
21
Rising Healthcare Costs and Rates of the Uninsured
Coverage gaps caused by the piecemeal approach to health policy have
contributed to rising rates of the uninsured. These rates are exacerbated by increased
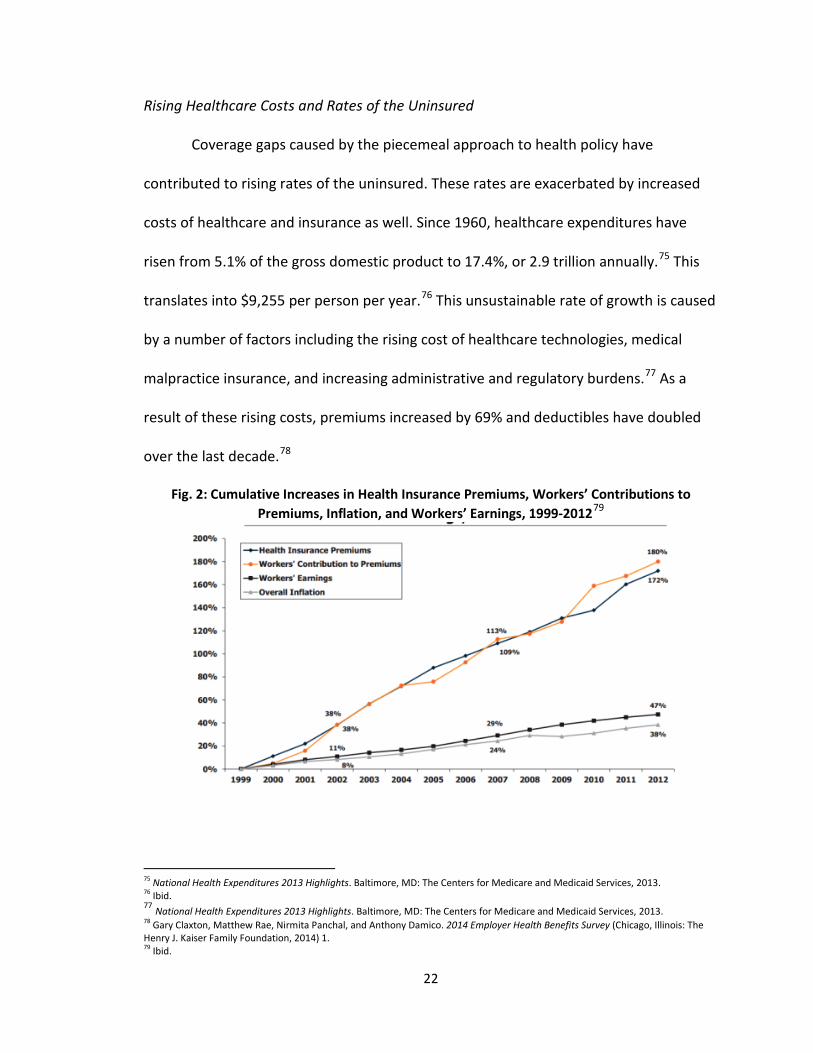
costs of healthcare and insurance as well. Since 1960, healthcare expenditures have
risen from 5.1% of the gross domestic product to 17.4%, or 2.9 trillion annually.75 This
translates into $9,255 per person per year.76 This unsustainable rate of growth is caused
by a number of factors including the rising cost of healthcare technologies, medical
malpractice insurance, and increasing administrative and regulatory burdens.77 As a
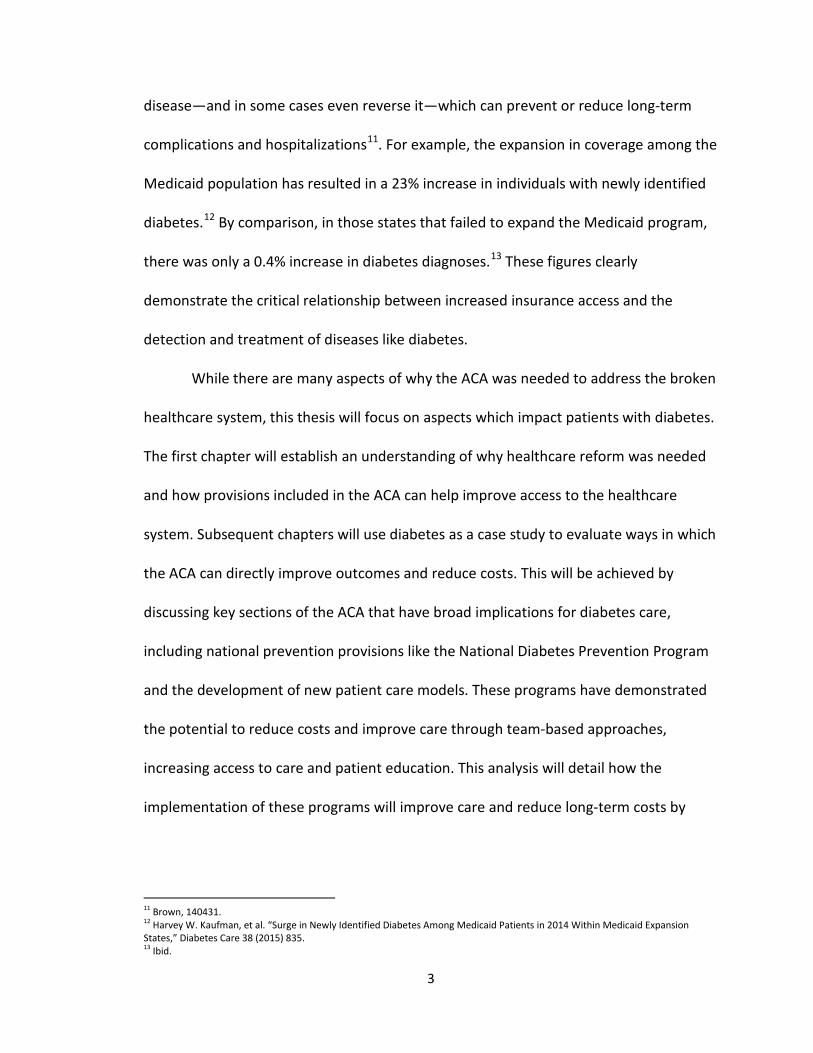
result of these rising costs, premiums increased by 69% and deductibles have doubled
over the last decade.78
Fig. 2: Cumulative Increases in Health Insurance Premiums, Workers’ Contributions to Premiums, Inflation, and Workers’ Earnings, 1999-201279
75 National Health Expenditures 2013 Highlights. Baltimore, MD: The Centers for Medicare and Medicaid Services, 2013. 76 Ibid. 77 National Health Expenditures 2013 Highlights. Baltimore, MD: The Centers for Medicare and Medicaid Services, 2013. 78 Gary Claxton, Matthew Rae, Nirmita Panchal, and Anthony Damico. 2014 Employer Health Benefits Survey (Chicago, Illinois: The Henry J. Kaiser Family Foundation, 2014) 1. 79 Ibid.
22

Employers have been forced to increase cost-sharing, which made insurance less
affordable to employees because of these growing costs. Many small businesses were
unable to provide coverage to their employees at all.80 From 2000 to 2009, only 30% of
the 59 million U.S. workers had employer-sponsored, family coverage.81 Due to these
high costs, by 2012, 31.5 million Americans under the age of 65 were underinsured and
an additional 47 million were uninsured.82 At least 79 million Americans were at risk for
not being able to afford needed care.83 In 2013, studies found that one-third of
uninsured individuals often went without needed medical care because of high costs.84
Among uninsured individuals who did receive care, 40% had outstanding medical bills
and one-fifth stated that these bills caused serious financial hardship.85 Overall, 70% of
uninsured individuals lacked confidence that they could pay for the healthcare that they
need.86
While access to affordable health insurance can be cost-prohibitive, the lack of
coverage often results in higher costs to the individual and to the overall healthcare
system. The passage of the Emergency Medical Treatment and Labor Act in 1986
required hospitals to provide emergency services to any individual in need without
regard for their ability to pay for those services.87 As a result, costs for uncompensated
services increased. In 2013, the total cost of medical care for the uninsured was $121
80 Ibid. 81 Ibid. 82 Ibid. 83 Cathy Schoen, et al. America’s Underinsured: A State-by-State Look at Health Insurance Affordability Prior to the New Coverage Expansions, (Washington, D.C.: The Commonwealth Fund, 2014) 3. 84 Key Facts about the Uninsured Population. (Washington, D.C.: The Kaiser Commission on Medicaid and the Uninsured, 2014) 1. 85 Ibid. 86 Rachel Garfield, Rachel Licata, and Katherine Young. The Uninsured at the Starting Line: Findings from the 2013 Kaiser Survey of Low-income Americans and the ACA (Menlo Park, CA: The Kaiser Family Foundation, 2014) 17. 87 The Centers for Medicare and Medicaid Services. Emergency Medical Treatment & Labor Act. https://www.cms.gov/Regulations-and-Guidance/Legislation/EMTALA/
23
billion and 70% of this cost went uncompensated.88 While much of this cost was
covered by public and private funding sources like Medicare and Medicaid, $21 billion in
services were not covered.89 Cost-shifting caused by providers who were not
compensated, or were undercompensated, resulted. This contributed to private payers
increasing premiums as a result.
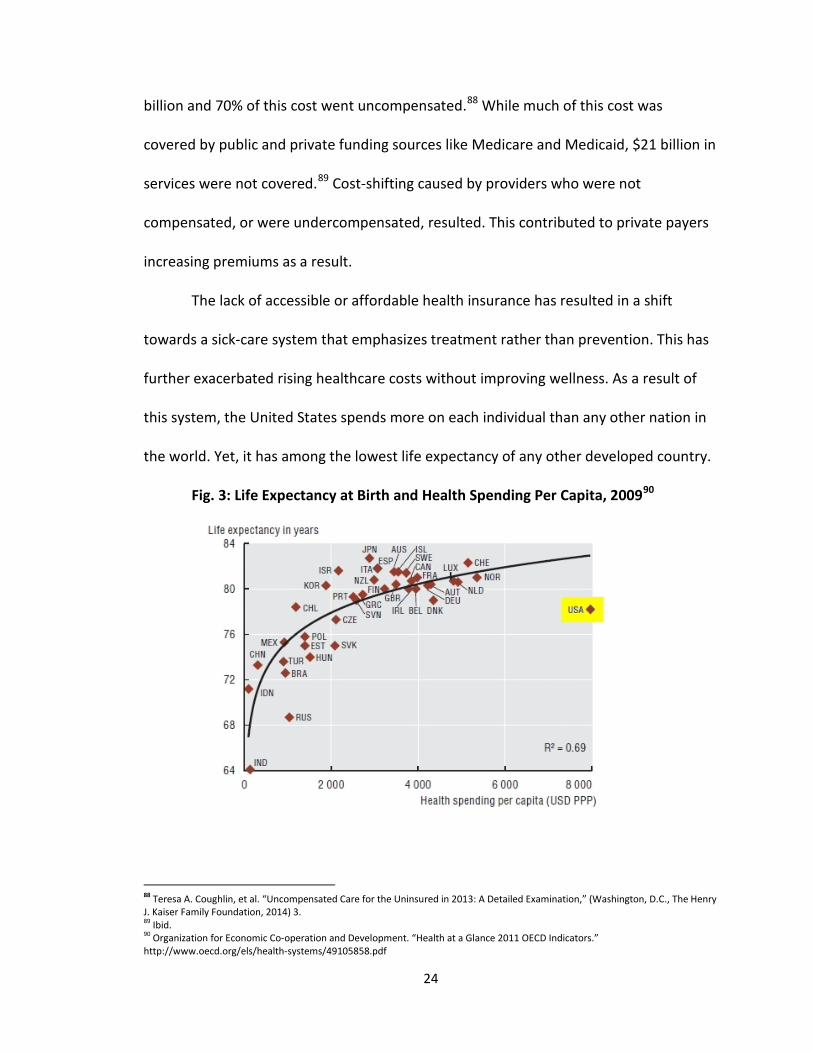
The lack of accessible or affordable health insurance has resulted in a shift
towards a sick-care system that emphasizes treatment rather than prevention. This has
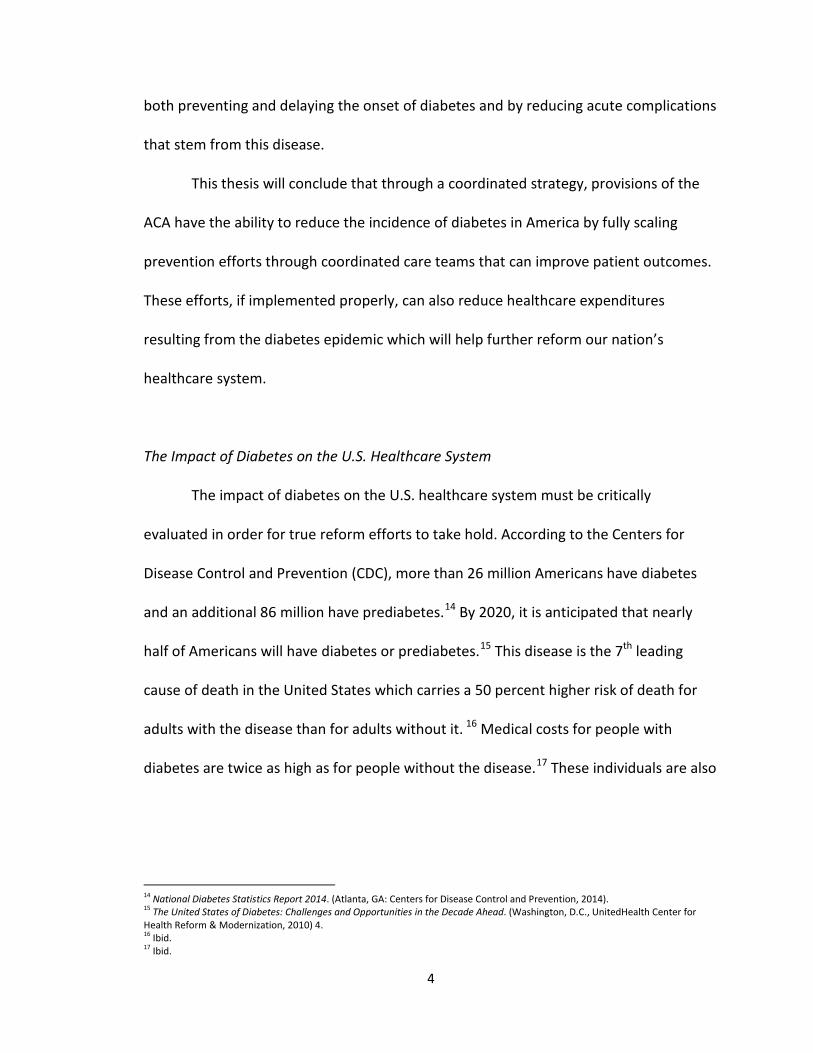
further exacerbated rising healthcare costs without improving wellness. As a result of
this system, the United States spends more on each individual than any other nation in
the world. Yet, it has among the lowest life expectancy of any other developed country.
Fig. 3: Life Expectancy at Birth and Health Spending Per Capita, 200990
88 Teresa A. Coughlin, et al. “Uncompensated Care for the Uninsured in 2013: A Detailed Examination,” (Washington, D.C., The Henry J. Kaiser Family Foundation, 2014) 3. 89 Ibid. 90 Organization for Economic Co-operation and Development. “Health at a Glance 2011 OECD Indicators.” http://www.oecd.org/els/health-systems/49105858.pdf
24

While many conditions can be prevented by receiving care earlier, the high cost
of insurance and the high cost of care have impeded access to these services. Individuals
are forgoing services or are waiting to receive care until symptoms are already present,
a practice that often results in costly complications and hospitalizations. Many of these
costs are due to an increased prevalence of these conditions and complications from
disease advancement or lack of treatment.91
As a result, Americans are getting sicker and are being diagnosed with chronic
diseases at an earlier age. In fact, because of earlier diagnoses of chronic diseases like
obesity and diabetes, children of this generation are expected to live 2-5 years less than
their parents.92 One in three children born in 2000 will develop type 2 diabetes in their
lifetime.93 This is largely caused by the rise in childhood obesity which has been found to
be the greatest risk factor for premature deaths caused by chronic disease.94 While the
rates of diabetes have dramatically increased among the adult population as well, the
parents of these children were not diagnosed until much later in life. Many argue that
this later diagnosis is due to lower rates of obesity in these individuals in their
childhood. Because of increased sugar intake and higher rates of sedentary lifestyles, in
addition to some genetic risk factors, children are being diagnosed with diabetes and
obesity at an earlier age and they are expected to live with the disease for a greater
amount of time than their parents. The increased disease longevity and progression has
91 Rising Health Care Costs. (Washington, D.C. America’s Health Insurance Plans, 2015). 92 Pam Belluck. “Children’s Life Expectancy Being Cut Short by Obesity,” New York Times, March 17, 2005. 93 K.M. Narayan, et al. “Lifetime Risk for Diabetes Mellitus in the United States.” The Journal of the American Medical Association 290, no. 14 (2003): 1884. 94Paul Franks, et al. “Childhood Obesity, Other Cardiovascular Risk Factors, and Premature Death.” The New England Journal of Medicine 362 (2010): 485.
25

the potential to cause more premature deaths and complications, thus translating into a
shorter life expectancy than the previous generation.
Impact of Chronic Conditions on the U.S. Healthcare System
The rising rate of chronic disease is a key contributor to the overall growth in
healthcare spending. By 2023, total expenditures for chronic diseases are estimated to
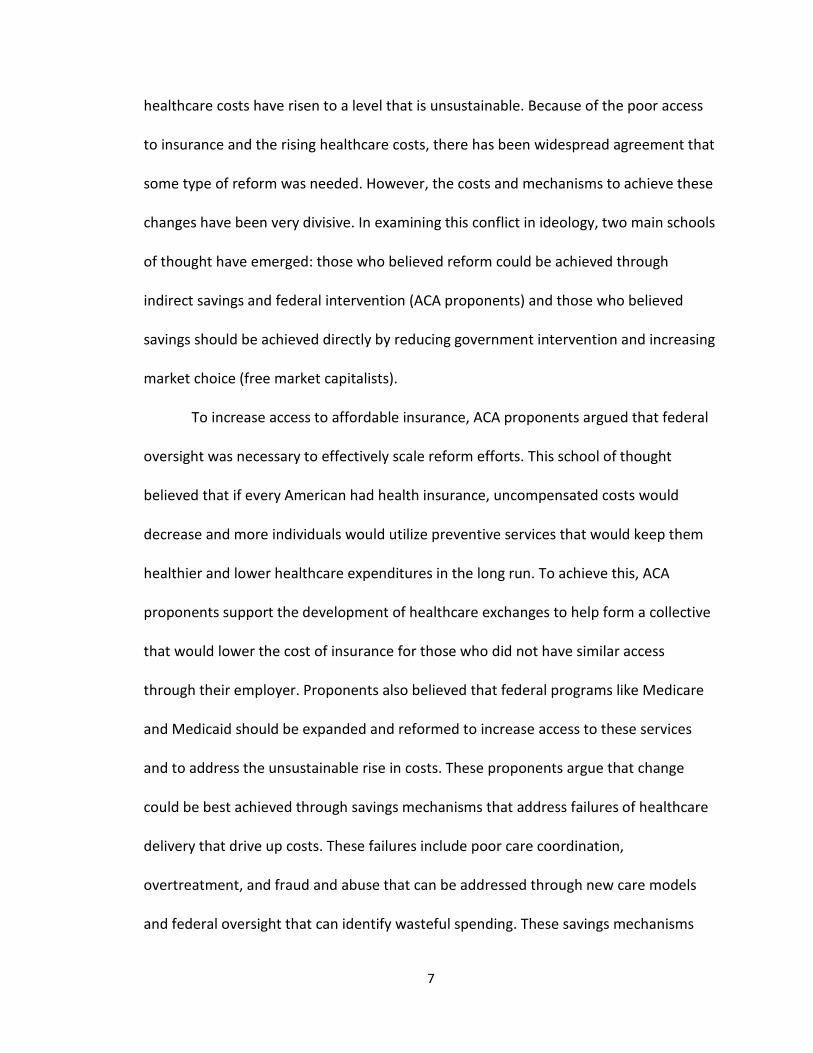
be $4.2 trillion annually.95 From 1987 to 2002, private health insurance spending
increased nearly 60% with chronic conditions accounting for 53% of these
expenditures.96 These diseases accounted for 67% of the growth in this spending.97
Among these chronic diseases, a major driver of this spending growth is attributable to
obesity and co-morbid conditions such as diabetes and cardiovascular disease.
95 Thomas Bodenheimer, Ellen Chen, and Heather D. Bennett. “Confronting the Growing Burden of Chronic Disease: Can the US Health Care Workforce Do the Job?” Health Affairs 28, no. 1 (2009): 66. 96 Kenneth E. Thorpe, et al. “The Rising Prevalence of Treated Disease: Effects on Private Health Insurance Spending,” Health Affairs (2005), doi: 10.1377/hlthaff.w5.317. 97 Ibid.
26
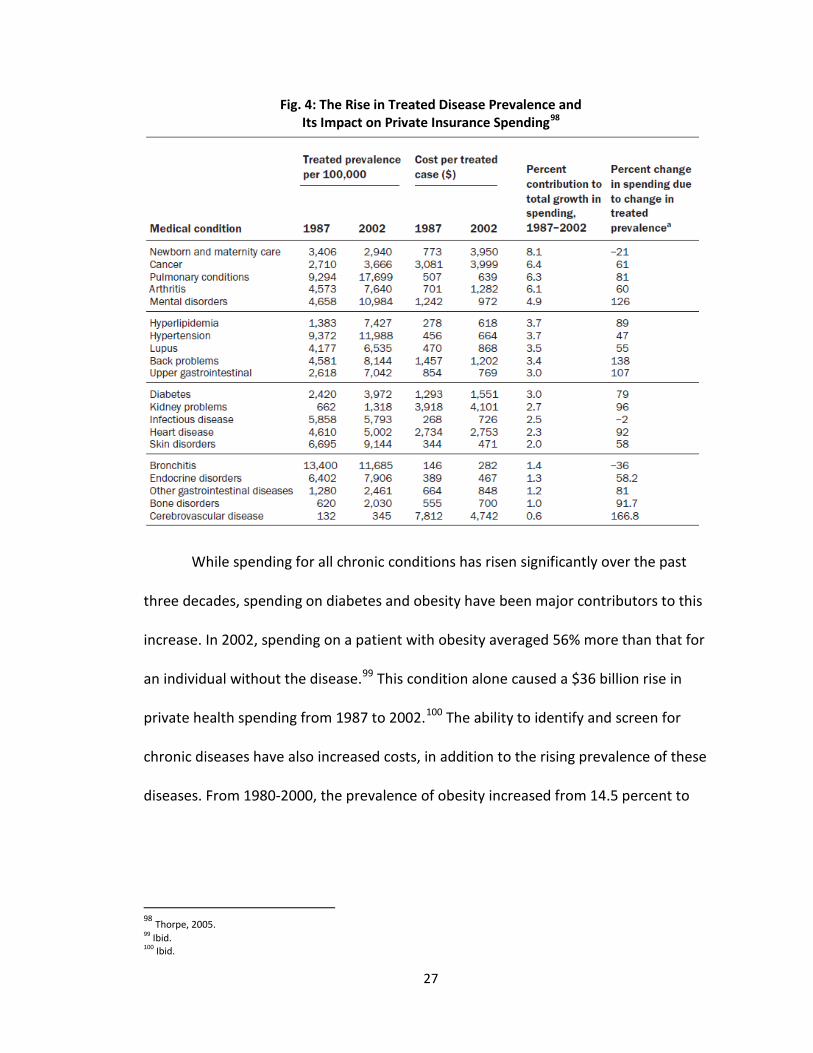
Fig. 4: The Rise in Treated Disease Prevalence and Its Impact on Private Insurance Spending98
While spending for all chronic conditions has risen significantly over the past
three decades, spending on diabetes and obesity have been major contributors to this
increase. In 2002, spending on a patient with obesity averaged 56% more than that for
an individual without the disease.99 This condition alone caused a $36 billion rise in
private health spending from 1987 to 2002.100 The ability to identify and screen for
chronic diseases have also increased costs, in addition to the rising prevalence of these
diseases. From 1980-2000, the prevalence of obesity increased from 14.5 percent to
98 Thorpe, 2005. 99 Ibid. 100 Ibid.
27
30.4 percent.101 Diabetes, a clinically linked condition, increased 53 percent during the
same period; treatment for this disease alone accounts for $245 billion annually.102
The high costs of health insurance and the high cost of care have created a
number of problems in the public health sphere, thereby contributing to the need for
healthcare reform. The rising rates of chronic disease that have resulted from these
problems have further exacerbated the need for such reform as well. By evaluating ways
in which the ACA addresses the affordability of health insurance as well as the rising
costs of care, one can better understand potential solutions for addressing America’s
broken healthcare system.
Leveraging the ACA to Address Access & Affordability
Rising healthcare costs and the rate of the uninsured led to a year-long
contentious debate on the best path forward for reforming the nation’s healthcare
system. In 2010, Congress passed the ACA, largely along party lines, and the legislation
has remained controversial ever since. Conservatives, arguing that the ACA was
unconstitutional because it mandated insurance coverage, have voted and failed to
repeal the law 56 times.103 As the federal government moves forward in implementing
the ACA, it is helpful to understand the provisions included in this legislation to better
identify ways in which they can be leveraged to increase access to affordable care.
The ACA is an expansive piece of legislation with many provisions to help provide
coverage to Americans who are uninsured. The central aspect to achieve this end is the
101 Thorpe, 2005. 102 Ibid. 103 Michael McAuliff. “House Passes 56th Anti-Obamacare Measure,” The Huffington Post, February 3, 2015.
28
individual mandate, a requirement that all individuals must obtain health insurance or
face penalties. Federal subsidies have been put into place to help support those who
need financial help to purchase health insurance. Individuals with incomes up 400%
above the federal poverty level are eligible to receive these subsidies, as are small
businesses with fewer than 25 employees.104 All businesses with more than 50
employees are required to offer insurance or face penalties.105
Aside from the individual mandate, the ACA includes a number of provisions to
ensure that employer-sponsored, or private health insurance, is accessible and
affordable. Adult, dependent children up to the age of 26 can remain on their parents’
insurance plans.106 Insurance companies are barred from denying coverage to
individuals because of pre-existing conditions. Lifetime limits on coverage are
eliminated as are discriminatory practices to drive up costs due to age or gender. The
ACA also establishes Health Insurance Marketplaces (exchanges) that enable individuals
to compare plans and determine their eligibility for Medicaid or tax credits that can help
make insurance more affordable. Individuals with incomes under 400% of the federal
poverty level are eligible to receive federal subsidies to obtain insurance.107
The implementation of the ACA is still in progress. While major provisions went
into effect in January 2014, many of these statutes are just taking effect due to several
issues caused by malfunctioning websites and cancellations by private insurers.
104 Sara Rosenbaum. “The Patient Protection and Affordable Care Act: Implications for Public Health Policy and Practice,” Public Health Reports 126, no. 1 (2011): 131. 105 Laxmaiah Manchikanti, et al. “Patient Protection and Affordable Care Act of 2010: Reforming the Health Care Reform for the New Decade.” Pain Physician 14, no. 1 (2011): E35. 106 Ibid. 107 Brian L. Ung and C. Daniel Mullins. “The Affordable Care Act, Health Care Reform, Prescription Drug Formularies and Utilization Management Tools,” Research in Social & Administrative Pharmacy 11(2015): 459.
29
However, the preliminary analysis indicates that the ACA has had a positive impact on
coverage and access so far. By 2015, more than 11.7 million Americans have enrolled
through the exchanges; the vast majority of these individuals (85%) have been eligible
for premium tax credits.108,109 By 2017, it is anticipated that 25 million Americans will be
insured who were not previously.110
As a result of the comprehensive requirements for insurance coverage that were
included in the ACA, many uninsured and underinsured Americans have access to
needed services. However, affordable insurance is still out of reach for some healthcare
consumers. Because plans under the ACA are more comprehensive than those many
individuals had previously obtained, the cost of insurance is higher. On average, costs
for insurance have increased by 5.4%.111 However, this increase is a record low when
compared to rate increases in years prior.112 Growth in overall healthcare spending has
slowed but is projected to be 6.8% higher in 2016 because of greater utilization of
services, technology, and high cost drugs.113 These costs trickle down to the consumer
which makes accessing care and being able to afford health insurance more difficult.
Employers are increasingly switching to higher deductible plans to reaction to these
costs which require greater cost-sharing by the individual. Since 2009, employers
offering high deductible plans increased by 300%.114 Deductibles for in-network services
108 Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report. (Washington, D.C. The Department of Health and Human Services, 2015). 109 Premium, Affordability, Competition, and Choice in the Health Insurance Marketplace, 2014. (Washington, D.C., The Department of Health and Human Services, 2014). 110 David Blumenthal. “Health Care Coverage under the Affordable Care Act—A Progress Report,” The New England Journal of Medicine 371 (2014) 275. 111 Stephanie Armour. “States Offer a Mixed Picture of Health Insurance Costs,” The Wall Street Journal. June 24, 2015. 112 Medical Cost Trend: Behind the Numbers 2016. (Washington, D.C., PriceWaterhouseCoopers, 2015,) 3. 113 Ibid 114 Ibid
30
grew by $500 and those for out of network care grew by $1,000 during the same
period.115
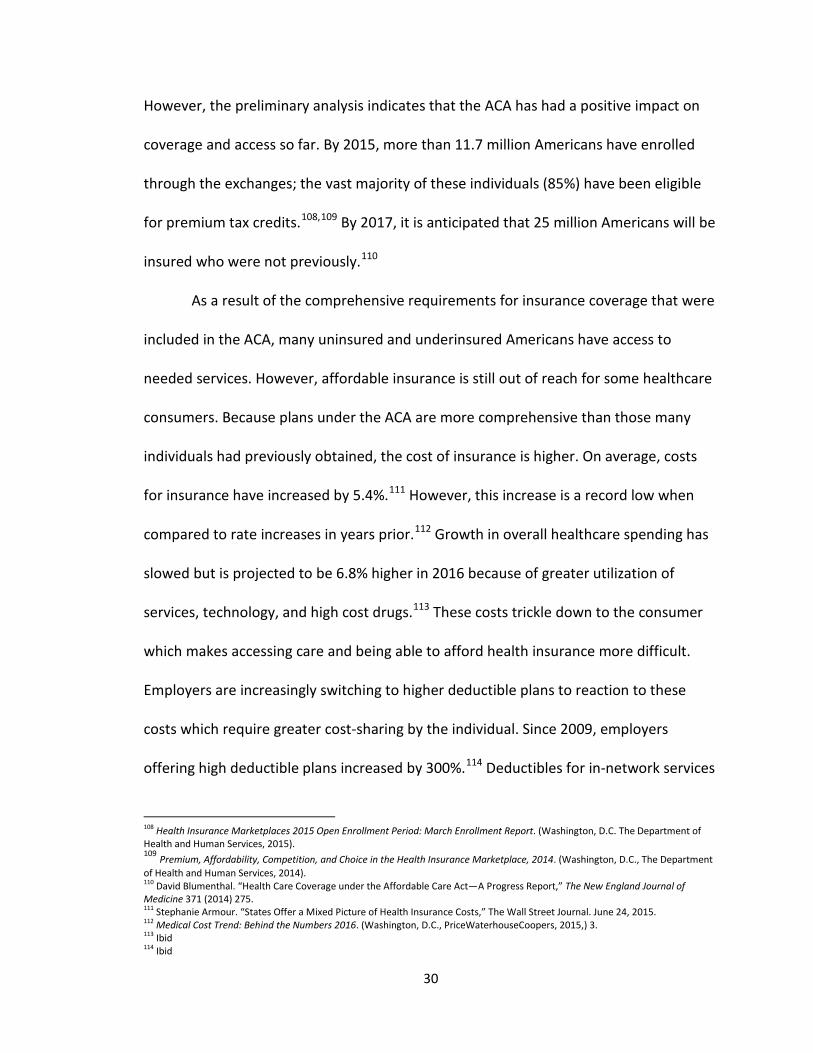
Fig. 5: Effects of the Affordable Care Act on Insurance Coverage (in millions)116
While nearly 85% of individuals who enrolled through the exchanges received
subsidies to help cover these costs, it is critical to evaluate whether these increases will
prevent some individuals from obtaining insurance.117 While there has been no
evidence that insurance uptake is slowing, once the ACA is fully implemented, 31 million
Americans will still be without insurance.118
115 Ibid. 116 Ibid. 117 Medical Cost Trend, 2015. 118 Frederic E. Shaw, Chisara N. Asomugha, Patrick H. Conway, Andrew S. Rein. “The Patient Protection and Affordable Care Act: Opportunities for Prevention and Public Health.” Lancet 384 (2014): 78.
31
In addition to increasing access to care, the ACA was intended to slow the
growth of healthcare spending. The ACA seeks to address healthcare costs by utilizing
new care delivery models that emphasize quality and patient outcomes rather than
compensating physicians for the individual services that they provide. These value-
based models will provide incentives to providers who improve patient outcomes while
reducing costs. Physicians who fail to achieve these goals will be penalized. These
models increase the stake that providers have in patient care in hopes that it will help to
improve population health. While the success of these models has yet to be fully
realized, there have been some preliminary data which suggests the potential to
improve care. The Pioneer Accountable Care Organization, one such care model, found
that costs for participating beneficiaries were less than half of their peers.119 The
Centers for Medicare & Medicaid Innovation has employed several pilot programs to
test these models, which are expected to be scaled nationally by 2019 as Medicare fully
transitions away from fee-for-service.120 Spending reduction mechanisms were also
included, like the Hospital Readmissions Reduction Program and the Community-based
Transitions Program which could generate $12 billion in savings over the next 10
years.121
The Congressional Budget Office has estimated that the ACA would reduce the
deficit by $143 billion over the first decade of its implementation, and by $1.2 trillion in
119 Ibid. 120 Thomas S. Crane, Lauren Moldawer, and Andy Shin. “Beyong SGR—MACRA Provides Additional Payment Provisions and Offsets,” Health Policy & Law Matters, April 21, 2015. http://www.healthlawpolicymatters.com/2015/04/21/beyond-sgr-macra-provides-additional-payment-provisions-and-offsets/ 121 Ibid.
32

the second decade.122 This estimate has been criticized by a number of individuals:
some believe that these figures have been underestimated; others believe that the ACA
will increase the deficit long-term. To evaluate ways in which the ACA can address the
needs of those with chronic illness, it is important to analyze the environment in which
individuals with diabetes faced before the passage of healthcare reform.
Conclusion & Key Findings
The necessitation of healthcare reform stemmed from a century of failures to
enact large-scale public policies that address the uninsured and the high cost of care.
These failures caused a fragmented system to develop with substantial coverage gaps
that were exacerbated by economic recessions, labor market shifts, and rising costs of
healthcare that made obtaining affordable health insurance even more difficult. The
symbiotic relationship between rising healthcare costs and the affordability of health
insurance has made it impossible to address one issue without addressing the other.
The ACA was passed in an effort to address these problems by utilizing federal resources
to make coverage more affordable and to help contain healthcare costs through the use
of more efficient, cost-saving care models that can help contain healthcare costs.
Growing rates of chronic disease in America have also exacerbated the broken
healthcare system. Poor access to care and growing healthcare costs have made early
detection and treatment of these diseases difficult, which has further added to already
rising costs of health spending. Enhancing preventive and wellness services are also
122 Mark R. Burge and David S. Schade. “Diabetes and Affordable Care Act,” Diabetes Technology & Therapeutics 16 (2014) 402. DOI: 10.1089/dia.2014.0171
33

critical to ensure that these diseases are identified and treated early to improve the
overall population’s health and to reduce costs to the healthcare system. In order to
effectively address this problem, large-scale reform was needed to restructure
healthcare delivery into a model that could better care for these patients.
This chapter evaluated the necessitation of healthcare reform and to what
extent the ACA could achieve its goals of making health insurance more affordable while
reducing costs to the healthcare system. A review of the history of healthcare reform
efforts concluded that due to the economic and political unviability of large-scale health
policy efforts, a patchwork system of public and private health plans emerged that left
millions of Americans uninsured. Due to a tipping point in the economic recession, a
new Democratic President, and 49 million Americans without health insurance, there
was a resurgence of the healthcare debate about the best way to address the lack of
affordable health insurance as well as the rising costs of care.123 This led to a multi-year,
highly controversial debate between conservatives who believed that these problems
should be solved by expanding market choice and progressives who argued that such a
national problem could not be unraveled without federal resources and regulatory
requirements.
While the progressive arguments won out in the end, culminating in the passage
of the ACA, public opinion on whether the law will have the intended impact on public
health continues to be widely-varied. Conservatives believe that the ACA will fail to
improve access to affordable insurance and to healthcare services. These critics argue
123 Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey. (Washington, D.C., The Department of Health and Human Services, 2014) 2.
34
that the onerous regulations will negatively impact small businesses and add to the
national debt. They also argue that the more comprehensive requirements will increase
the cost of health insurance. ACA-proponents, on the other hand, have seen the
growing numbers of insured since the passage of the law and argue that this will
increase utilization in prevention and wellness programs that can improve population
health. ACA supporters also argue that these provisions will contribute to long-term
savings that will negate the up-front costs of passing the law.
While much remains to be seen about whether the ACA will improve health and
reduce growing healthcare costs, there is some promising data to date. Since the
implementation of the ACA more than 11.7 million Americans had enrolled in exchanges
that were established to increase access and affordability of health insurance.124
Individuals who are up to 400% of the federal poverty limit are eligible for subsidies to
help make obtaining insurance more affordable.125 Of those newly enrolled in the
healthcare exchange, 85% were eligible for subsidies to help cover these costs.126 Over
the next two years, it is expected that the number of enrollees will increase to 25
million.127 As a result, one can conclude that the ACA has expanded access to affordable
health insurance to many individuals who could not previously afford it. In terms of
reducing costs, much of the return on investment will occur in the years ahead. The
Congressional Budget Office has estimated that the ACA will reduce the deficit by $143
124 Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report. (Washington, D.C. The Department of Health and Human Services, 2015). 125 Rosenbaum, 131. 126 Premium, Affordability, Competition, and Choice in the Health Insurance Marketplace, 2014. (Washington, D.C., The Department of Health and Human Services, 2014). 127 Blumenthal, 275.
35

billion over the first ten years that it is implemented and an additional $1.2 trillion in the
subsequent decade.128 These long-term savings result from a number of programs
included in the ACA that aim to reduce waste and abuse practices, incentivize the
reduction of hospitalizations and readmissions, and utilize wellness services to prevent
individuals from becoming sick.
In conclusion, the implementation of a large-scale, comprehensive reform
package is critical in addressing the growing number of uninsured individuals and the
rising cost of healthcare in America. Attempts at achieving this goal have repeatedly
failed over the past century, resulting in a more broken system that cannot be fixed
through the piecemeal approach used in years past. The passage of the ACA has the
potential to improve access to affordable insurance, to improve care, and to reduce
overall healthcare spending. However, the extent to which the law can achieve these
goals remains to be seen. To gain a better understanding of successes and failures to
date, it is important to assess provisions included in the ACA that address access and
treatment of chronic disease, a key driver of poor outcomes and high costs.
Diabetes, one such chronic disease that disproportionately contributes to these
problems, can serve as a key case study in evaluating these successes and failures. The
following chapters will evaluate how the ACA will reform the way that healthcare is
delivered to patients with chronic disease and how increasing access to prevention and
wellness services can prevent the rates of chronic disease from continuing to grow.
These chapters will specifically look at these provisions through the lens of diabetes to
128 Mark R. Burge and David S. Schade. “Diabetes and Affordable Care Act,” Diabetes Technology & Therapeutics 16 (2014): 402.
36

assess whether these efforts have the potential to reform the healthcare system to
improve care and reduce costs.
37
Chapter Two:
Leveraging Prevention and Public Health Programs to Improve Diabetes Care
The Affordable Care Act (ACA) contains a number of provisions to improve
population health through prevention and wellness programs. Given the 25 million
Americans that are expected to gain access to affordable insurance by 2017, it is a
critical tipping point for evaluating the extent to which these provisions are able to
reduce the incidence of disease in America.129 Addressing chronic diseases like diabetes
are of particular importance as they disproportionately contribute to rising healthcare
costs. This chapter will evaluate prevention and wellness programs included in the ACA
through the lens of diabetes to determine how these provisions can improve population
health through disease prevention and health promotion.
The Current Diabetes Landscape
The economic burden of chronic disease cannot be ignored when reforming the
nation’s healthcare system. By 2020, 157 million Americans are expected to be living
with at least one chronic condition.130 This accounts for nearly 78% of total health
spending.131 Diabetes is a key contributor to these high healthcare costs because of the
number of co-morbid conditions caused by the disease and because of poor self-
management that leads to costly complications and hospitalizations. Currently, there
are more than 26 million Americans with diabetes and an additional 86 million with
129 Updated Estimates of the Insurance Coverage Provisions of the Affordable Care Act. The Budget and Economic Outlook: 2014 to 2024. (Washington, D.C. Congressional Budget Office, 2014). 130 Thomas Bodenheimer, Ellen Chen, and Heather D. Bennett. “Confronting The Growing Burden Of Chronic Disease: Can The U.S. Health Care Workforces Do The Job?,” Health Affairs 28, no. 1 (2009): 64. 131 Ibid.
38
prediabetes (i.e., individuals with elevated blood sugar levels who are at high risk for
developing diabetes).132 One in three Medicare dollars is spent on diabetes and a high
percentage of these costs are caused by the disease being unmanaged or
undermanaged.133 By 2020, half of Americans are expected to have diabetes which will
further add to these already exorbitant costs.134 Because of these factors, the extent to
which the ACA can slow or delay the onset of diabetes is critically important in
improving overall population health and in reducing the costs incurred by treating the
disease and its comorbidities.
One in four Americans do not know that they have diabetes and 9 out of 10 do
not know that they have prediabetes.135 As a result, even though the scope of this
disease is far-reaching, many Americans continue to be ill-informed about diabetes and
their individual risk based on predictive factors such as excess body weight or high blood
glucose. While preventive care and screening have been shown to mitigate the
incidence of diabetes, the inability to access primary care physicians, a lack of health
insurance, and the stigma of being overweight are key contributors to the failure of
Americans to leverage these services. However, with an estimated $176 billion in annual
medical costs and an additional $69 billion in indirect costs like disability, work loss, and
premature death, education and prevention efforts to elevate the importance of this
disease are critical to address this issue.136 Among individuals who have been diagnosed
with the diabetes, high costs of care and the complexity of self-management often
132 National Diabetes Statistics Report 2014. (Atlanta, GA: Centers for Disease Control and Prevention, 2014). 133 Medicare Health Support Overview. (Washington, D.C., The Centers for Medicare and Medicaid Services, 2015). 134 National Diabetes Statistics Report 2014. 135 Ibid. 136 Ibid.
39

contributes to uncontrolled diabetes and therefore costly complications and
hospitalizations. In 2012 alone, there were 43 million inpatient hospital days incurred by
people with diabetes, more than 25% of all inpatient stays for that year.137 An additional
15 million emergency department visits and 174 million physician office visits were
incurred because of diabetes that year as well.138 The figure below details the
percentage of health resources used on patients with diabetes in comparison to those
individuals without diabetes and the U.S. population as a whole.
Fig. 6: Health Resource Use in the U.S. by Diabetes Status and Cost Component139
Diabetes can serve as a case study of whether the ACA can improve population
health through prevention and wellness provisions as the disease is largely preventable.
Lifestyle prevention programs and early detection have been widely successful in
137 Wenya Yang, et al. “Economic Costs of Diabetes in the U.S. in 2012,” Diabetes Care 35 (2013): 1040. 138 Ibid. 139 Ibid.
40
preventing or delaying the onset of the disease. However, because the vast majority of
individuals who are at-risk for the diabetes do not know it, in order for lifestyle
intervention and prevention programs to be effective, one must first enhance public
awareness of the disease and access to screening and early detection programs.
Accessing Preventive Services
While millions of Americans have obtained health insurance as a result of the
ACA, the law’s ability to have a positive impact on population health will be diminished
unless individuals take advantage of the preventive health services afforded to them.
Before the passage of the ACA, nearly half of U.S. adults were not receiving preventive
health services which evaluate an individual’s health when they are symptom-free to
detect and treat diseases earlier so that more serious, and costly, complications do not
arise.140 Such care includes annual wellness exams in physicians’ offices that provide
routine health screenings based on factors such as age, gender, health status, personal
health history, and current health problems.141
Preventive services have the most potential to reduce healthcare costs by
identifying, preventing, and treatment of diseases before they become serious in an
effort to avoid complications and hospitalizations. The increased use of preventive
services by 5% has the potential to save an estimated 100,000 lives annually.142 Studies
indicate that individuals with health insurance access preventive services far more often
140 Nearly Half of U.S. Adults Were Not Receiving Key Preventive Services Before 2010. (Atlanta, GA, The Centers for Disease Control and Prevention, 2012). 141 Ibid. 142 Ashley B. Coffield and Michael Maciosek. Preventive Care: A National Profile on Use, Disparities, and Health Benefits. (Washington, D.C., The Robert Wood Johnson Foundation, 2007,) 1.
41
than their uninsured counterparts. In 2013, only one-third of uninsured adults received
preventive care while 74% of adults with health insurance reported a preventive visit
with their physician.143 As the uninsured population is generally at a higher risk for
preventable hospitalizations and serious health conditions, expanding access to these
services is vital. 144
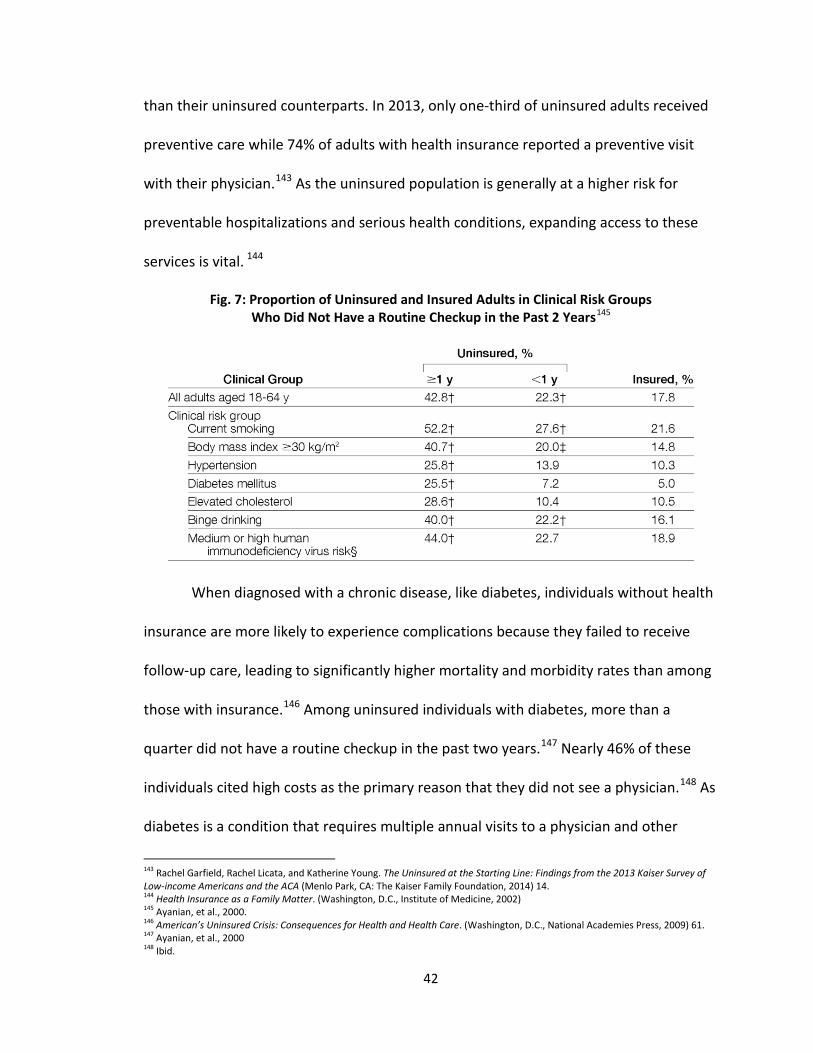
Fig. 7: Proportion of Uninsured and Insured Adults in Clinical Risk Groups Who Did Not Have a Routine Checkup in the Past 2 Years145
When diagnosed with a chronic disease, like diabetes, individuals without health
insurance are more likely to experience complications because they failed to receive
follow-up care, leading to significantly higher mortality and morbidity rates than among
those with insurance.146 Among uninsured individuals with diabetes, more than a
quarter did not have a routine checkup in the past two years.147 Nearly 46% of these
individuals cited high costs as the primary reason that they did not see a physician.148 As
diabetes is a condition that requires multiple annual visits to a physician and other
143 Rachel Garfield, Rachel Licata, and Katherine Young. The Uninsured at the Starting Line: Findings from the 2013 Kaiser Survey of Low-income Americans and the ACA (Menlo Park, CA: The Kaiser Family Foundation, 2014) 14. 144 Health Insurance as a Family Matter. (Washington, D.C., Institute of Medicine, 2002) 145 Ayanian, et al., 2000. 146 American’s Uninsured Crisis: Consequences for Health and Health Care. (Washington, D.C., National Academies Press, 2009) 61. 147 Ayanian, et al., 2000 148 Ibid.
42
health providers to prevent the progression of the disease and to receive necessary
prescription medications, this figure suggests that millions of Americans may
uncontrolled diabetes.
The ACA provides a key opportunity to increase access to preventive care by
increasing insurance coverage and by expanding the benefits afforded under these plans
at low or no cost. Expanded access to preventive services and insurance coverage
healthcare services will help to identify diseases like diabetes at an earlier stage so that
they can be treated before it progresses. However, the increased use of these services
may also increase the number of diseases being treated, and therefore increase overall
costs to the U.S. healthcare system. This is particularly of note for chronic diseases
which often need to be treated over the course of a lifetime. For 2016, it is estimated
that healthcare costs will rise by 6.8% because of increased utilization of services,
technology, specialty drugs, and physician employment. 149 After accounting for benefit
design changes and narrow provide networks, the net growth rate is expected to be
4.5%.150 These costs are likely to trickle down to the consumer through higher
deductibles as a result. More than 85% of employers are considering moving to high
deductible plans.151 Twenty-five percent of employers have already implemented these
plans as the only option for their employees, a 40% increase since 2012.152 Therefore,
while the ACA has expanded access to and use of healthcare services, there are
potential downstream effects that may impede future utilization. Current projected
149 Medical Cost Trend: Behind the Numbers 2016. (Washington, D.C., PriceWaterhouseCoopers, 2015). 150 Ibid. 151 Ibid. 152 Medical Cost Trend: Behind the Numbers 2016. (Washington, D.C., PriceWaterhouseCoopers, 2015).
43

increases are minimal but increased cost-sharing for healthcare services because of high
deductible plans negatively impact the use of some preventive and wellness services.
With these factors in mind, it is essential to evaluate provisions in the ACA that
increase access to low or no cost preventive services that can keep American’s healthier
and to reduce costs through early detection and treatment. By evaluating the
implementation of key prevention provisions, including the Essential Health Benefits
(EHBs), increased access and screening because of the expansion of the Medicaid
program, the closure of the Medicare Part D “donut hole”, and funding for the National
Diabetes Prevention Program, one can understand the extent to which the ACA can be
effective in reducing the burden of diabetes in America. These provisions are further
detailed below.
Essential Health Benefits
A central feature of the ACA is its emphasis on prevention and wellness
programs as an included benefit in all health insurance plans. One key provision to
achieve this end is the inclusion of EHBs in health plans. These benefits serve as a
minimum standard for all plans and include 10 different categories of services like
ambulatory patient services, emergency services, coverage for hospitalizations, mental
health and substance abuse, prescription drug coverage, and chronic disease
management.153 In general, EHBs are provided to enrollees at standard cost-sharing,
meaning that services are not covered until deductibles are met. However, there are at
153 Mark R. Burge and David S. Schade. “Diabetes and Affordable Care Act,” Diabetes Technology & Therapeutics 16 (2014) 403.
44
least 15 free preventive services and one annual wellness visit that are covered under
the EHBs at no cost to the individual. These free services are a key bridge between
increasing insurance coverage and ensuring that enrollees access these benefits for the
purposes of disease prevention and health promotion. The inclusion of EHBs in the ACA
is particularly beneficial for individuals at-risk for or already diagnosed with diabetes as
these services can even prevent the onset and progression of the disease.
While the implementation and usage of EHBs is still in its early stages, data has
indicated that this provision has expanded access to care for millions of Americans. By
2014, 76 million Americans had received care under the EHBs at no cost.154 Cost-sharing
is a key barrier to the uptake of healthcare services. The CDC estimates that removing
cost sharing from mammography increased utilization by up to 9%.155 Low or no cost
preventive services are critical for individuals to actually utilize them. Beyond benefits
afforded to all individuals, those at-risk for diabetes have access to additional services
including screening for the disease, nutritional counseling, blood pressure screening,
and other screening tests for high-risk individuals who may have prediabetes.156
Resources such as diabetes self-management training and medical nutrition therapy are
also offered to support patients with diabetes with making long-term lifestyle changes
that can help to prevent the development of complications or comorbidities.157 In the
Medicare Advantage plans, a Medicare plan offered by private insurance companies,
patients are offered additional benefits including: 1) educational resources on how to
154 The Department of Health and Human Services, “Affordable Care Act Helps 76 Million Americans with Private Coverage Access Free Preventive Services,” press release, June 27, 2014, http://www.hhs.gov/news/press/2014pres/06/20140627b.html. 155 The Centers for Disease Control and Prevention. “Building a Healthier Community,” fact sheet, October 29, 2014, http://www.cdc.gov/nccdphp/dch/programs/communitytransformation/. 156 Burge, 403. 157 Ibid.
45

prevent diabetes, 2) additional self-management training for individuals with diabetes,
and 3) disease management programs that provide additional care coordination and in-
home monitoring to avoid complications and co-morbid conditions in patients with
diabetes.
Fig. 8: Number of Americans Estimated to be Newly Covered for Expanded Preventive Services Under the Affordable Care Act (in Millions)158
Critics have argued that this expansion is problematic as it forces individuals to
purchase plans with services that they will never use. For example, health plans for men
and post-menopausal women include maternity services. Instead, these individuals
argue that health consumer should be able to select plans that are more tailored to
them. However, this approach is problematic in that it reinforces discriminatory practice
by insurance companies that the ACA was intent on eliminating. By ensuring that every
158 The U.S. Department of Health and Human Services. “Increased Coverage of Preventive Services with Zero Cost Sharing Under the Affordable Care Act,” issue brief, June 27, 2014. http://aspe.hhs.gov/health/reports/2014/preventiveservices/ib_preventiveservices.pdf
46
American has access to EHBs, which include mental health and substance abuse
counseling and maternity care, individuals are on more equal footing and the collective
public can receive better access to services.
Non-exclusion of Preexisting Conditions & Lifetime Limits
Mandating the inclusion of EHBs in all health plans was essential in increasing
access to these services. The ACA also includes two provisions that help improve upon
this goal: the non-exclusion of pre-existing conditions and the elimination of lifetime
limits. The ACA precludes plans from imposing lifetime limits on most health benefits,
including the EHBs, and from denying coverage to individuals with pre-existing
conditions. It is estimated that, prior to the ACA, pre-existing condition exclusions
impacted between 50-129 million Americans.159 This practice has disproportionately
impacted the millions of Americans living with diabetes from accessing affordable
insurance coverage because of their condition. Prior to the passage of the ACA, lifetime
limits forced many patients with diabetes to pay out of pocked for services like office
visits, hospital care, and prescription drugs once they met their lifetime limit. Since
diabetes is a chronic disease that can last over the course of one’s lifetime, these out of
pocket expenditures could prevent many individuals from accessing preventive services
and from taking their medications.
159 The U.S. Department of Health and Humans Services. “At Risk: Pre-Existing Conditions Could Affect 1 in 2 Americans: 129 Million People Could Be Denied Affordable Coverage without Health Reform,” November 2011, http://aspe.hhs.gov/health/ reports/2012/pre-existing/index.shtml.
47
Medicare Part D Donut Hole
One of the most promising provisions to effectively manage and prevent the
progression of disease is the closure of the Medicare Part D “donut hole.” The donut
hole is a gap in prescription drug coverage that occurs once all deductibles have been
met and a $2,850 limit on annual payments has been reached.160 Beyond this limit,
individuals are responsible for 100% of the drug costs until a yearly cap of $4,950 in out
of pocket costs have been met.161 This coverage gap primarily affects seniors, Medicare
beneficiaries who are enrolled in Part D and have incomes that preclude them from
receiving low-income subsidies.162 Patients with diabetes are particularly impacted by
the donut hole as they have higher than average costs to treat their disease. In 2006,
studies found that 41% of Medicare Part D beneficiaries who had diabetes met the
donut hole threshold; among patients without diabetes, only 25% achieved this
threshold.163 Paying for medications out of pocket as a result of this gap can be difficult,
especially for those with chronic diseases, like diabetes, that require multiple, monthly
medications. This may result in individuals forgoing some or all medications which can
lead to costly complications or hospitalizations.
The ACA will address the donut hole by reducing copayments on generic and
brand-name Medicare drugs to 25% by 2020.164 This reduction has already saved 6.1
160 Geoffrey F. Joyce GF, Julie Zissimopoulos, and Dana Goldman. “Digesting the Doughnut Hole,” Journal of Health Economics 32, no. 6(2013) 1345. 161 Ibid. 162 Ibid. 163 Ibid. 164 Joyce, 1345.
48
million Americans more than $5.7 billion on drug costs.165 This is an average of $706 per
beneficiary.166 In 2012 alone, these beneficiaries saved $425 million on diabetes
medications, $240 million on lipid-lowering medications, and $138 million on
antihypertensive medications.167 Since each of these medications is often used by
patients with diabetes, this provision alone can have a significant impact in slowing or
preventing the progression of the disease. In fact, studies have suggested that the donut
hole disproportionately impacted patients with diabetes and inhibited use of high-cost
drugs by 18% and low-cost drugs by as much as 5%.168
Medicaid Expansion
To increase access to affordable health insurance, the ACA contained a provision
that expanded the Medicaid program to individuals with incomes greater than or equal
to 138% of the federal poverty level.169 The intent of this provision was to help reduce
the number of uninsured by providing a continuum of coverage options through
Medicaid, Medicare, and the new health insurance exchanges. In addition to increasing
the number of insured individuals under the Medicaid program, the ACA also included
provisions to expand benefits covered under the program. Additional benefits covered
under program include key preventive health services and prescription drug coverage
165 The Centers for Medicare & Medicaid Services. The Affordable Care Act—A Stronger Medicare Program in 2012. (Washington, DC, 2012) http://www.cms.gov/apps/files/Medicarereport2012.pdf 166 Ibid. 167 Burge, 402. 168 Joyce, 1345. 169 John Holahan, et al. “The Cost and Coverage Implications of the ACA Medicaid Expansion: National and State-by-State Analysis,” (Washington, D.C., The Urban Institute, 2012).
49
which were included under the EHBs.170 As a result, all individuals who receive insurance
through Medicaid have access to better healthcare options. Because of this expansion,
more than 7.2 million additional people have been able to obtain insurance and have
access to preventive health services through the Medicaid program.171 By 2023, it is
estimated that there will be 11.9 million newly enrolled adults because of this
expansion.172 In addition to increasing the number of insured individuals under the
Medicaid program, the ACA also included provisions to expand benefits covered under
the program. As a result, all individuals who receive insurance through Medicaid have
access to better healthcare options.
Expanded coverage is ineffective without sufficient healthcare professionals to
provide the necessary care. Given shortages in the physician workforce, the ACA
incentivized physicians to carry out these newly-covered services by raising fees for
Medicaid services to the level of Medicare rates. This was an average increase of73%.173
Lower payments for Medicaid services resulted in fewer physicians accepting Medicaid
patients. By increasing the reimbursement for Medicaid services, more physicians were
willing to provide critical health care services, including preventive care, for patients in
the program. In addition, funding to expand community health centers and the National
Health Service Corps, which supplies physicians to underserved areas, was also included.
170 Ibid. 171 The Centers for Medicare and Medicaid Services. “Medicaid & CHIP: June 2014 Monthly Applications, Eligibility Determinations and Enrollment Report,” press release, August 8, 2014. http://medicaid.gov/medicaid-chip-program-information/program-information/downloads/june-2014-enrollment-report.pdf 172 Dana Mangan. “Higher Costs for Obamacare’s New Medicaid Patients,” CNBC, July 13, 2015. 173 Julia Paradise. “Medicaid Moving Forward,” (Washington, D.C., The Kaiser Commission on Medicaid and the Uninsured, 2015) 8.
50
As a result of this provision, these health centers and new health sites now provide
comprehensive primary care services to 21 million individuals.174
The expansion of Medicaid has also demonstrated a pent up demand for
healthcare services among those who were newly insured. In 2014, the average cost of
new enrollees was 19 percent higher than those who were in the Medicaid program
prior to the expansion because of the need for services these individuals have no had
access to for a number of years.175 After 2014, however, the actuary estimates that this
cost will continue to decline due to normalized use of healthcare services and because
of disease prevention among the newly insured.176 This year, projections indicate that
new enrollees will actually cost less than those who were previously eligible for
Medicaid.177 By 2023, this gap is expected to widen further with newly eligible
individuals costing $5,076 annually and previously enrolled individuals costing $7,299.178
Millions of additional individuals could be enrolled in Medicaid and more
preventive health services could be provided if the expansion was scaled nationally,
however. Due to a 2012 Supreme Court ruling, states are able to opt-out from
expanding their Medicaid programs. To date, 19 states have declined expanding their
Medicaid programs and two additional states are discussing whether to move
forward.179
174 Paradise, 8. 175 Dana Mangan. “Higher Costs for Obamacare’s New Medicaid Patients,” CNBC, July 13, 2015. 176 Ibid. 177 Ibid. 178 Ibid. 179 Status of State Action on the Medical Expansion Decision. (Washington, D.C., The Henry J. Kaiser Family Foundation, 2015).
51
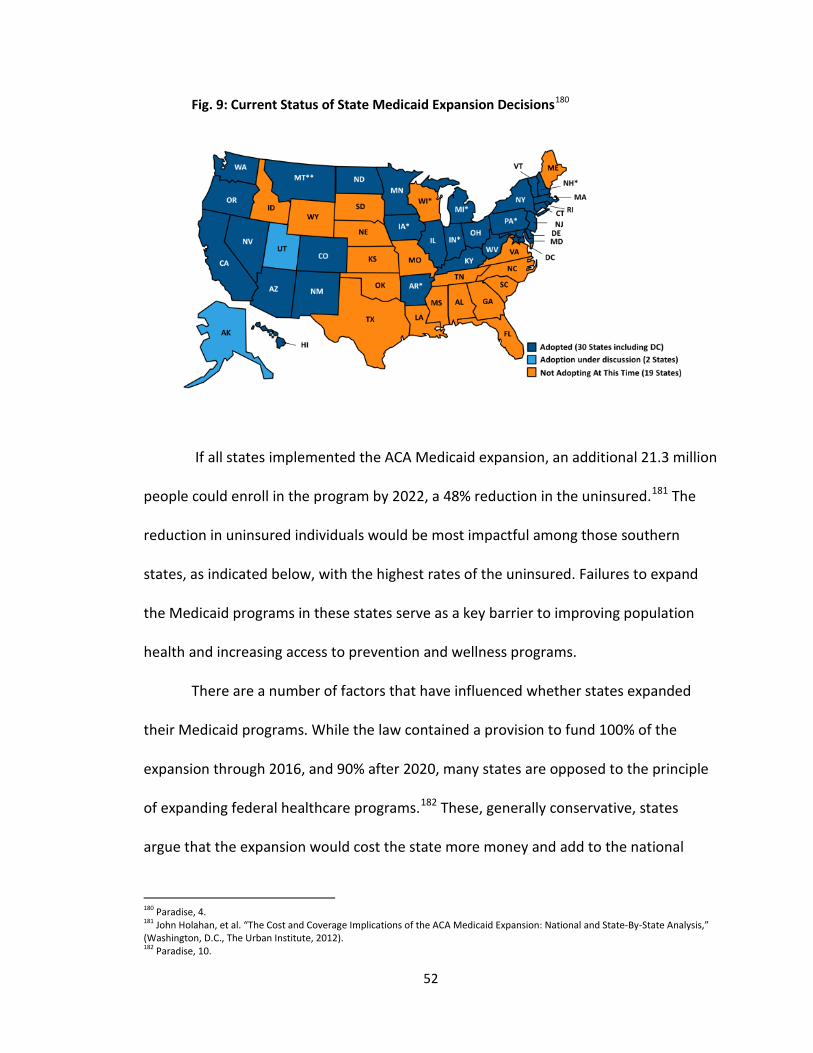
Fig. 9: Current Status of State Medicaid Expansion Decisions180
If all states implemented the ACA Medicaid expansion, an additional 21.3 million
people could enroll in the program by 2022, a 48% reduction in the uninsured.181 The
reduction in uninsured individuals would be most impactful among those southern
states, as indicated below, with the highest rates of the uninsured. Failures to expand
the Medicaid programs in these states serve as a key barrier to improving population
health and increasing access to prevention and wellness programs.
There are a number of factors that have influenced whether states expanded
their Medicaid programs. While the law contained a provision to fund 100% of the
expansion through 2016, and 90% after 2020, many states are opposed to the principle
of expanding federal healthcare programs.182 These, generally conservative, states
argue that the expansion would cost the state more money and add to the national
180 Paradise, 4. 181 John Holahan, et al. “The Cost and Coverage Implications of the ACA Medicaid Expansion: National and State-By-State Analysis,” (Washington, D.C., The Urban Institute, 2012). 182 Paradise, 10.
52
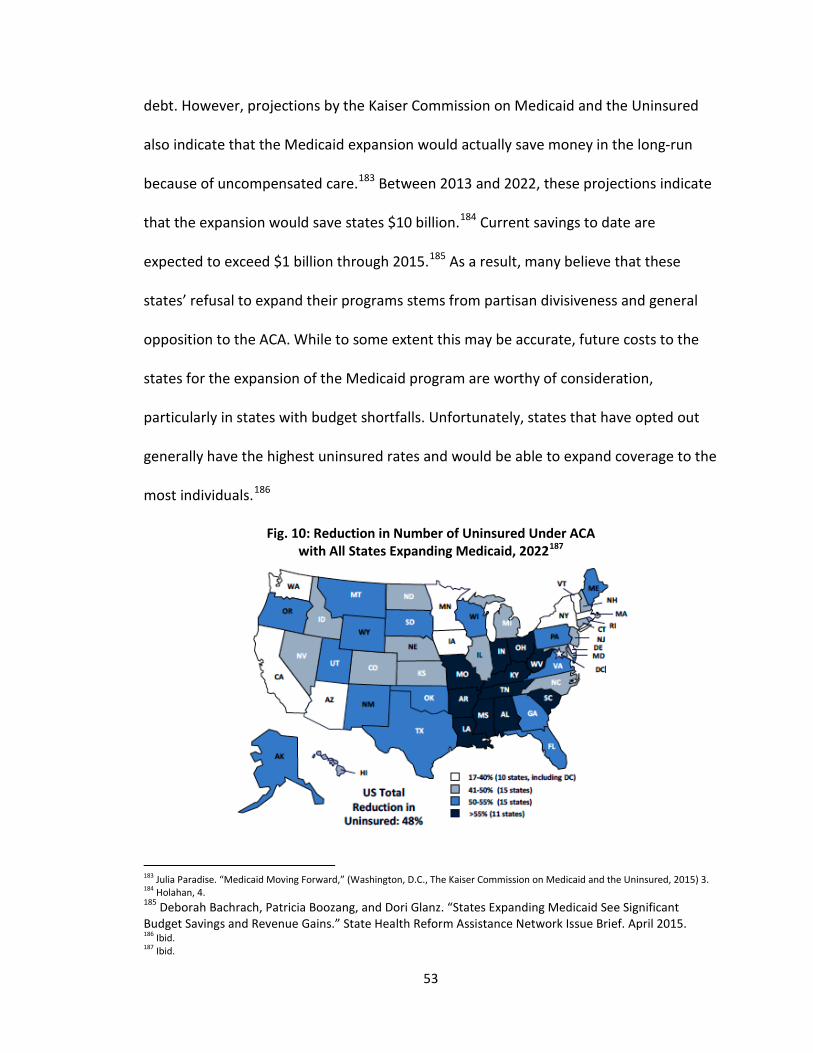
debt. However, projections by the Kaiser Commission on Medicaid and the Uninsured
also indicate that the Medicaid expansion would actually save money in the long-run
because of uncompensated care.183 Between 2013 and 2022, these projections indicate
that the expansion would save states $10 billion.184 Current savings to date are
expected to exceed $1 billion through 2015.185 As a result, many believe that these
states’ refusal to expand their programs stems from partisan divisiveness and general
opposition to the ACA. While to some extent this may be accurate, future costs to the
states for the expansion of the Medicaid program are worthy of consideration,
particularly in states with budget shortfalls. Unfortunately, states that have opted out
generally have the highest uninsured rates and would be able to expand coverage to the
most individuals.186
Fig. 10: Reduction in Number of Uninsured Under ACA with All States Expanding Medicaid, 2022187
183 Julia Paradise. “Medicaid Moving Forward,” (Washington, D.C., The Kaiser Commission on Medicaid and the Uninsured, 2015) 3. 184 Holahan, 4. 185 Deborah Bachrach, Patricia Boozang, and Dori Glanz. “States Expanding Medicaid See Significant Budget Savings and Revenue Gains.” State Health Reform Assistance Network Issue Brief. April 2015. 186 Ibid. 187 Ibid.
53
State failures to expand their Medicaid programs caused a new coverage gap to
emerge. While the Medicaid reform was intended to cover over 20 million Americans,
up to 5.7 million are estimated to go without insurance because of state refusals to
expand the Program. Subsidies provided under the ACA to help low-income individuals
purchase health insurance are only offered to those making between 100% and 400% of
the federal poverty level.188 Under the intent of the law, individuals who make less than
100% of the federal poverty level (FPL) would have been eligible for Medicaid under the
expansion. However, in states that failed to expand their programs, the Medicaid
eligibility threshold can be as little as 50% of the FPL.189 As a result, individuals who
make too little to receive federal subsidies but who make too much to be eligible for
Medicaid are left to pay out of pocket for health insurance. In total, nearly 4 million low-
income, uninsured adults fall into this coverage gap.190
The distribution of adults in the coverage gaps has wide-ranging implications for
individuals with diabetes. A disproportionate number of southern states, which have the
highest incidence of diabetes, opted out of the Medicaid expansion. As a result, more
low-income individuals, a demographic at a higher-risk of having diabetes, do not have
access to preventive health services. As a result of the incongruent state Medicaid
programs, it is possible to delve deeper into how failures to expand these programs can
impact population health. By evaluating how increasing access to preventive health
services in states that have expanded their programs and comparing them to those
188 Rachel Garfield, et al. “The Coverage Gap: Uninsured Poor Adults in States That Do Not Expand Medicaid—An Update,” (Washington, D.C., 2015). 189 Ibid. 190 Ibid.
54

states that did not, one is able to assess the impact that increasing access can have in
identifying and treating diseases like diabetes.
In 2014, Quest Diagnostics conducted a study to ascertain whether states that
had expanded its Medicaid programs increased the number of patients with diabetes
that were being diagnosed and treated earlier. The study found that the Medicaid
expansion resulted in a 23% increase in patients newly identified with diabetes.191
States that did not expand their Medicaid programs only saw an increase of 0.4 percent
in newly diagnosed individuals with diabetes. The figure below details the number of
newly identified patients with diabetes in Medicaid expansion states when compared to
non-expansion states. These data include Medicaid (column 2) and non-Medicaid
patients (column 3), which comprise the total number of newly identified individuals
with diabetes (column 1).
Fig. 11: Patients with Newly Identified Diabetes in All States, Medicaid Expansion States, and Non-Expansion States192
191 Harvey W. Kaufman, et al. “Surge in Newly Identified Diabetes Among Medicaid Patients in 2014 Within Medicaid Expansion States,” Diabetes Care 38 (2015) 835. 192 Ibid.
55

The successes in diagnosing patients with diabetes resulted from the
implementation of preventive services like screening for diabetes which were accessed
because of insurance coverage afforded to low-income individuals who were previously
uninsured. To test for diabetes, an A1C test is used to determine whether blood sugar
levels are higher than normal. Among those who were newly identified to have
diabetes, these levels were lower meaning that the disease was early-stage and could
be effectively treated and perhaps reversed.193 On the whole, these findings indicate
increasing access to preventive health services can be effective for identifying and
treating diseases earlier, thereby improving patient outcomes and lowering costs.
Utilizing Prevention Programs to Improve Health
In addition to increasing access to preventive health services, the ACA also
focuses on developing a coordinated strategy to address disease prevention and health
promotion. The Prevention and Public Health Fund (PPHF) is a $2 billion annual
allocation to fund community-based programs that can help improve population health
by preventing chronic disease.194 The PPPHF was passed by the ACA to focus on chronic
disease prevention to reduce health costs and to improve the quality of care. The PPHF
addresses factors that serve as barriers to good public health like housing,
transportation, education, and the availability of affordable food, in order to develop
193 Kaufman, 835. 194 The U.S. Department of Health and Human Services. “Building Healthier Communities by Investing in Prevention,” fact sheet, February 9, 2011, http://www.hhs.gov/healthcare/facts/factsheets/2011/09/prevention02092011.html.
56
more comprehensive programs based on wellness and prevention.195 The program
focuses specifically on chronic disease with the goal of preventing, detecting, and
treating these conditions early to improve health and reduce costs. As 7 out of 10
deaths result from chronic conditions, the federal government believed that focusing its
efforts in this area has the most potential to make the biggest impact.196 In 2015, the
PPHF invested $750 million on four critical areas to address this growing problem:
community prevention, clinical prevention, public health infrastructure and training, and
research and tracking. Each of these programs has great potential to improve
population health for patients with diabetes.
In the area of community prevention, the PPHF has invested $222 million to
implement the Community Transformation Grant (CTG) program which uses evidence-
based interventions to prevent heart attacks, strokes, obesity, and other chronic
conditions. The CTG program is expected to reach 130 million Americans through
programs implemented by 61 state and local governments, tribes and territories, and
nonprofit organizations in 36 states.197 An additional $16 million was allocated to
improve nutrition and to increase physical activity to prevent obesity and its related
conditions and costs.198 Since diabetes is an obesity-related disease, programs that seek
to address obesity also help to prevent diabetes.
CTG programs are required to address at least one in five of the following health
measures: weight, nutrition, physical activity, tobacco use prevalence, and mental
195 Ibid. 196 Ibid. 197 The Centers for Disease Control and Prevention. “Building a Healthier Community,” fact sheet, October 29, 2014, http://www.cdc.gov/nccdphp/dch/programs/communitytransformation/. 198 Ibid.
57

health.199 Each of these measures is a key contributor to the rising rate of diabetes and
the exacerbation of the disease through poor health. While many of these programs are
still being carried out, there have been a number of successes to date. Since the release
of the first year funds in 2011, these programs have demonstrated a great deal of
success. One such success is the National Diabetes Prevention Program.
The National Diabetes Prevention Program
While the ACA includes a number of programs to address chronic disease
prevention, lifestyle intervention programs, like the National Diabetes Prevention
Program (NDPP), are the most significant due to their scalability and proven successes
to date. By evaluating ways in which programs like the NDPP can be expanded nationally
and coordinated with other provisions included in the ACA, one can better understand
ways in which diabetes prevention can be addressed through federal resources. Lifestyle
intervention programs as well as new care models that utilize team-based approaches
to provide education and treatment for diabetes have great potential to improve care
and reduce the economic burden of diabetes. Following the passage of the ACA,
UnitedHealth Group projected that $250 billion could be saved if current prevention
efforts were fully scaled.200 The ACA reinforces these approaches through a number of
programs, like the NDPP, that implement prevention programs and team-based care to
improve care coordination and patient education.
199 Ibid. 200 The United States of Diabetes: Challenges and Opportunities in the Decade Ahead.(Washington, D.C., UnitedHealth Center for Health Reform & Modernization, 2010,) 5.
58
The NDPP is an evidence-based lifestyle intervention program that enables
individuals with prediabetes that emphasizes weight loss, stress-reduction, and
establishing coping skills through a year-long program. The program is administered by
the Centers for Disease Control and Prevention (CDC) and offered in a variety of
community centers, like the YMCA. During the program, the goal for each participant is
to lose at least five percent of their body weight by reducing calorie intake through
improved choices, increasing moderate physical activity to more than 150 minutes per
week, and by developing behavioral problem-solving and coping skills.201 The program
consists of an initial six-month phase that offers at least 16 sessions over 16-24 weeks
and a second six-month session that requires participation in at least one session per
month.202 These sessions are facilitated by a trained lifestyle coach utilizing CDC-
approved curriculum that highlights the importance of behavior modification, stress
management, and peer support. Patients with prediabetes and who are overweight can
be referred to these programs by their physicians; however many insurance programs,
including Medicare, do not provide coverage for these services.
The NDPP is based on a $200 million clinical study conducted in 2002 by the
National Institutes of Health (NIH) which found that even moderate weight lost (5-7
percent) can prevent or delay the onset of diabetes by 58 percent overall, and by 71
percent in individuals over the age of 60.203 The Diabetes Prevention Program (DPP)
study randomly assigned participants into one of three interventions to address their
201 Preventing Type 2 Diabetes. (Atlanta, GA, The Centers for Disease Control and Prevention, 2014) 3. 202 Ibid. 203 Diabetes Prevention Program Research Group. “The Diabetes Prevention Program Description of Lifestyle Intervention,” Diabetes Care 25, no. 12 (2002): 2165.
59
prediabetes: standard lifestyle recommendations plus metformin (a first-line diabetes
medication), standard lifestyle recommendations with a placebo, or an intensive
program of lifestyle modification. The standard lifestyle recommendation cohort was
given 20-30 minute individual sessions that emphasized the importance of a healthy
lifestyle. The intensive lifestyle medication group was asked to achieve and maintain a 7
percent weight loss through low-calorie, low-fat diet and at least 150 minutes of
moderate exercise each week. This cohort was also given a 16 session curriculum which
discussed diet, exercise, and behavior modification—much like the NDPP, which was
created as a resulted of this study.204
The results of this study were a pivotal step in determining ways in which to
prevent diabetes. Fifty percent of the participants in the lifestyle intervention group
achieved a 7 percent weight loss by the end of the 16 sessions and 38 percent achieved
this goal at the time of their most recent visit.205 The study found that lifestyle
intervention reduced the incidence of diabetes by 58 percent whereas the standard
intervention with metformin only reduced the incidence by 31 percent.206 As such, the
lifestyle intervention was significantly more effective in preventing diabetes. A ten year
follow-up to the DPP found that reductions in diabetes incidence persisted even after a
decade: rates of diabetes among individuals who participated in the lifestyle
intervention program were 34 percent lower than among those in the placebo group.207
204 Diabetes Prevention Program Research Group. “The Diabetes Prevention Program Description of Lifestyle Intervention,” Diabetes Care 25, no. 12 (2002): 2165. 205 Ibid. 206 Diabetes Prevention Program Research Group. “Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin,” The New England Journal of Medicine 346, No. 6 (2002): 1. 207 Kenneth E. Thorpe, “The Affordable Care Act Lays The Groundwork For a National Diabetes Prevention and Treatment Strategy,” Health Affairs 31, no.1 (2012): 62.
60
This finding is critical in assessing the scalability of these programs to determine if
similar results would be achieved if the NDPP is expanded nationally.
While the DPP study found weight loss to be a strong predictor of diabetes
prevention, costs to deliver the DPP intervention in year one amounted to $1,400 per
participant—a cost that precludes scalability on the national level.208 However, in 2007,
in the annual per capita healthcare expenditure for a person with diabetes was $11,700.
Prevention of this disease, even at a rate of $1,400 per person, would drastically reduce
the cost of diabetes. Recent studies found that if the NDPP was scaled to those aged 60-
64 with prediabetes, it would result in net savings to Medicare of over $2 billion in 10
years, and $15 billion over a lifetime.209 If the NDPP were fully scaled, it could amount to
$191 billion in savings over 10 years.210
Conclusion & Key Findings
Expanding access to preventive care services is critical in improving population
health, particularly given the growing rates of chronic disease in America. These
provisions have far-reaching implications for patients with diabetes and must be
leveraged appropriately for the intended impact of the ACA to be fully realized. By 2020,
157 million Americans are expected to living with at least one chronic disease and half
of all Americans are estimated to have diabetes.211 The expansion of preventive services
and access to care under the ACA is crucial in slowing the progression this epidemic.
208 John Anderson, Meghan Riley, and Tekisha Everette. “How Proven Primary Prevention Can Stop Diabetes,” Clinical Diabetes 30, no. 2 (2012): 77. 209 Ibid, 78. 210 Ibid, 77. 211 Thomas Bodenheimer, Ellen Chen, and Heather D. Bennett. “Confronting the Growing Burden of Chronic Disease: Can the US Health Care Workforce Do the Job?” Health Affairs 28, no. 1 (2009): 64.
61
Prior to the passage of this law, 49 million Americans did not have access to health
insurance which led to a higher risk of preventable hospitalizations and serious health
conditions.212 Uninsured individuals who had been diagnosed with a chronic disease,
like diabetes, were more likely to experience complications leading to higher rates of
mortality and morbidity which were largely avoidable. Failures to receive preventive
services because of high costs of care and a lack of access to health insurance were key
contributors to these risk factors.
The individual mandate and subsidies for low-income individuals that make
insurance more affordable are a key step forward in improving access to care.
Individuals with health insurance have been found to receive preventive health services
far more often than the uninsured which can lead to better out comes in the long- and
short-term. Since the implementation of the ACA, 76 million Americans are estimated to
be newly covered for the expanded preventive services afforded under the law at low or
no cost.213 This estimate includes those individuals who were uninsured or underinsured
under less costly plans. As a result of this expansion, health plans are more
comprehensive in nature and offer beneficiaries greater access to a wider range of
services.
Projected increases in healthcare spending because of a higher utilization of
care, technology, and more expensive drugs could impede access to these services,
however. Employers are shifting to higher deductible plans that require individuals pay
212 The Department of Health and Human Services. Assistant Secretary for Planning and Evaluation Issue Brief. Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey. Washington, DC, 2014, http://aspe.hhs.gov/health/reports/2011/cpshealthins2011/ib.pdf (accessed July 1, 2015). 213 The U.S. Department of Health and Human Services. “Increased Coverage of Preventive Services with Zero Cost Sharing Under the Affordable Care Act,” issue brief, June 27, 2014.
62
more out of pocket costs for receiving care. While this may impede access in the future,
the establishment of many preventive services, including a free annual wellness exam in
the EHBs may mitigate this problem.
In addition to the inclusion of EHBs in all health plans, the ACA also prevented
the use of discriminatory practices that precluded access to insurance. The elimination
of lifetime limits and the exclusion of pre-existing conditions as a rationale for denying
coverage were key steps forward in expanding access to care. Given the estimated 129
million Americans that could be impacted by these clauses, the elimination of these
practices has the potential to increase early detection and treatment of diseases before
they become serious.214 For patients with diabetes, this was particularly impactful as
most of these individuals experienced one or both discriminatory practices over the
course of the lifetime of their disease. However, some patients continue to have
difficulties in access insurance and treatment because of their conditions. Insurance
companies have increased cost-sharing for some patients, particularly those with
chronic diseases, which make access to care and medications unaffordable. While these
companies cannot establish lifetime limits they can make enrollees pay more of the
costs themselves. Therefore, while the inclusion of these clauses in the ACA did increase
access to care and to services, high cost of healthcare is an issue that still needs to be
addressed to improve overall patient health.
For low-income individuals who receive insurance through the Medicaid
program, the ACA takes a critical step in increasing access to care through the expansion
214 The U.S. Department of Health and Humans Services. “At Risk: Pre-Existing Conditions Could Affect 1 in 2 Americans: 129 Million People Could Be Denied Affordable Coverage without Health Reform,” November 2011, http://aspe.hhs.gov/health/ reports/2012/pre-existing/index.shtml.
63
of the program and in closing the Part D donut hole. The expansion of the Medicaid
program has enabled 11.9 million Americans to receive health insurance coverage. State
failures to adopt the expansion has prevented almost 6 million additional people from
having such access and has created a coverage gap among those who would have been
eligible under the ACA. This coverage gap will need to be address in the coming years in
order to ensure that low-income individuals are able to access affordable health
insurance. The closure of the Medicare Part D donut hole will enable many seniors to
access affordable medications as a result of the ACA as well. Large out-of-pocket costs
because of this gap prevented many individuals from receiving adequate and
appropriate treatment. This closure is critical in preventing the progression of disease
and in preventing costly hospitalizations and complications that could result from
improper treatment.
Prevention programs, like the NDPP, have also proved promising for individuals
at risk for diabetes. While the ACA funds some NDPP programs throughout the country,
if these were fully scaled the savings in preventing or delaying the onset of diabetes
could amount to $191 billion over 10 years.215 Because of this, the federal government
should consider putting additional funding towards the expansion of the NDPP as it has
great potential to improve overall population health.
215 John Anderson, Meghan Riley, and Tekisha Everette. “How Proven Primary Prevention Can Stop Diabetes,” Clinical Diabetes 30, no. 2 (2012): 77.
64
Chapter Three:
Reducing Costs and Improving Care for Patients with Diabetes
In the decades leading up to the passage of the Affordable Care Act (ACA), U.S.
healthcare became increasingly fragmented because of public policy failures to enact
large-scale reforms. These failures have led to a patchwork structure comprised of
public and private health insurance programs marred by so much inefficiency and
bureaucracy that many characterize the healthcare system as a “non-system.” Rising
rates of the uninsured and increasing costs of healthcare have further exacerbated
already existing fissures in this broken system. As such, the passage of the Affordable
Care Act provides a critical opportunity to comprehensively address how to improve
access to quality care while reducing healthcare spending. By evaluating ways in which
the ACA will restructure care delivery to enhance care coordination, one can better
understand how these new care models can reduce costs while improving care. Because
fragmented treatment approaches to chronic diseases, like diabetes, serve as a key
driver of increasing healthcare costs, it is also critical to assess how these new models
can more effectively care for these patient populations.
The Rise of Fragmented Care
The U.S. healthcare system is comprised of public and private programs that
provide insurance coverage to various patient populations. Medicare and Medicaid are
public programs enacted in 1965 to provide coverage for low-income populations and
65

the elderly. These programs also contain provisions for at-risk populations like pregnant
women, children, and the permanently disabled. Private, employer-based insurance
programs provide coverage for working-aged adults with costs being shared between
employers and employees. These plans offer coverage to the individual and to families
and can also be purchased outside of the employer market, generally at a higher cost to
the individual. While the existing programs provide coverage for the vast majority of the
American population, significant coverage gaps remain. For example, individuals who
are just above the poverty level do not qualify for Medicaid; however, they are also
unable to afford private insurance. Smaller federal programs, like the State Children’s
Health Insurance Program, have been enacted over the past few decades to address
these gaps. However, since the 1970s, the rate of the uninsured has continued to
steadily increase and by 2012, 49 million Americans did not have health insurance.216
Due to high costs, health insurance is difficult to obtain, particularly among low-wage
workers and the unemployed.
One key driver is the high cost of care, costs that are shifted to insurance plans
and then on to the employer and the individual. Therefore, to evaluate reasons behind
the rising costs of health insurance, it is important to first assess the key drivers of
overall healthcare costs. The United States spends $2.7 trillion on healthcare services
annually.217 In 2011, this amounted to 18% of the gross domestic product.218 These
expenditures can be attributed to a number of factors including “higher prices for
216 The Department of Health and Human Services. Assistant Secretary for Planning and Evaluation Issue Brief. Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey. Washington, DC, 2014, http://aspe.hhs.gov/health/reports/2011/cpshealthins2011/ib.pdf (accessed July 1, 2015). 217 Ibid. 218 “Rising Health Costs,” American’s Health Insurance Plans, accessed June 20, 2015. https://www.ahip.org/Issues/Rising-Health-Care-Costs.aspx.
66
medical services, paying for volume over value, defensive medicine, use of new
technologies and treatments without considering cost-effectiveness, and a lack of
transparency of information on prices and quality.”219 A 2010 study has indicated that
the practice of defensive medicine alone costs the U.S. healthcare system $45.6 billion
each year. All of these practices roll up into a system known as fee-for-service (FFS), a
payment model that compensates physicians and hospitals based on the number of
services that they provide.
The FFS model compensates physicians and hospitals based on the quantity of
the services that they provide, rather than the quality. There is no incentive for
improving patient care or reducing costs. In fact, studies have shown that primary care
physicians who are paid by the service that they provide tend to treat patients more
often with costlier procedures.220 As a result, the FFS system raises costs and
discourages integrated care. This practice also contributes to outright fraud and abuse
by billing for services and medical equipment that are unnecessary or unused.221
Insurance companies, in response, review the services billed to determine whether they
are medically necessary and deny claims that they believe to be wasteful. These denials
leave patients responsible for paying out of pocket for healthcare services and hospitals
with uncompensated care.
In response to the rising costs for healthcare services, in part caused by the FFS
system, the federal government and private payers lowered reimbursement rates for
219 “Rising Health Costs,” 2015. 220 Toby Godsen, et al. "Capitation, Salary, Fee-for-service and Mixed systems of Payment: Effects on the Behaviour of Primary Care Physicians," The Cochrane Library 3(2000):9. 221 Ibid.
67
many of the highly utilized services. Additional regulatory demands, like the purchase
and use of electronic health record systems, which average at a cost of $50,000 -70,000
for an initial set-up and an additional $10,000-20,000 per provider for installation, have
further contributed to cuts in physicians’ revenue.222 As a result, physicians, especially
those in primary care practices, have had to increase the number of patients that they
see in order to make up the difference in revenue. In 2008, the average physician saw
23 patients each day.223 By 2012, however, this figure decreased to an average of 20
patients.224 Rather than a decrease in patient work load or a lesser need to make up lost
revenue, the reason for this decline can be attributed to increasing non-clinical work.
Regulatory reporting requirements and quality improvement measure are two key
examples of this clinical paperwork, which physicians spend an average of 11 hours each
week completing.225 The high patient workload and increasing amount of time spent on
non-clinical duties have contributed to lower quality care as a result.
Studies have indicated that primary care physicians would need to spend 21.7
hours each day to provide all of the recommended acute, chronic, and preventive care
for the average annual patient workload of 2,300.226 Patients only receive about 55% of
these recommended services because of time constraints which results in lower quality
of care and an exacerbation of diseases.227 As a result, among the half of Americans
have at least one chronic disease, 50% of those with hypertension have uncontrolled
222 Nir Menachemi and Robert G. Brooks. "Reviewing the Benefits and Costs of Electronic Health Records and Associated Patient Safety Technologies." Journal of Medical Systems: 159. 223 “A Survey of America’s Physicians: Practice Patterns and Perspectives,” (Washington, D.C., The Physician Foundation, 2012) 46. 224 Ibid. 225 Ibid, 45. 226 Ibid. 227 Justin Altschuler, et. al. "Estimating a Reasonable Patient Panel Size for Primary Care Physicians with Team-Based Task Delegation." The Annals of Family Medicine (2012): 396.
68
blood pressure, 80% of those with hyperlipidemia do not have control of their
cholesterol, and 43% of those with diabetes have not achieved glycemic control.228 This
difficult practice environment has dissuaded many medical students from the primary
care field, leading to increasing workforce shortages that cannot meet current or
projected demands.
Healthcare delivery has also become increasingly fragmented under the FFS
system because there is no incentive, and often no time, to effectively coordinate care.
Physicians often work in silos, billing for services that they deliver without working in a
coordinated effort with other members of their patient’s care team to ensure optimal
healthcare delivery. This is largely caused by pressures to see more patients and to
increase revenue by billing more services. In these already demanding settings, lower
rates of reimbursement from public programs have caused many practices not to accept
Medicare or Medicaid patients which have further exacerbated access to care. In 2012,
35% of practices stated that they were closed to these programs, a 47% increase from
2008.229 With millions of additional individuals entering into these programs because of
expansions included in the ACA, this barrier may prevent many patients from having
access to physicians. When combined with workforce shortages of 15-20%, new care
models that extend physician care teams and technology that can help track and
coordinate care are critical to improving the quality of care.230
228 Ibid. 229 “A Survey of America’s Physicians: Practice Patterns and Perspectives,” (Washington, D.C., The Physician Foundation, 2012) 46. 230 Ibid.
69
The Impact of Chronic Disease on an Already Fragmented System
The ACA contains a number of programs to achieve these goals by shifting
healthcare delivery from a volume-based, FFS system to one that emphasizes integrated
delivery and quality improvement. While a number of studies have shown that these
new care models and transformation programs are successful at improving care and
reducing costs, it is critical to assess whether these successes are also applicable for
individuals with chronic disease. Patients with chronic diseases like diabetes are
particularly vulnerable population at-risk of falling through the cracks in care transitions
and poor care delivery. New payment models enacted under the ACA have shown great
potential to address these two problems by implementing coordinated, patient-
centered approaches to team-based care. Patients with chronic disease are also a key
driver of health care costs because of disease complexity and severity as well as the
failings of care delivery under the FFS system. Therefore, it is also important to assess
whether these models can reduce healthcare expenditures while also improving costs.
By 2020, it is expected that 157 million Americans will be living with at least one
chronic disease, more than double the number in 2005.231 The economic burden of
chronic disease accounts for 78 percent of total health expenditures and this figure is
expected to continue to increase dramatically over the coming years.232 There are a
number of reasons for the rising costs and prevalence of chronic disease in America.
These include rising risks for disease-specific factors (like obesity) as well as an overall
231 Thomas Bodenheimer, Ellen Chen, and Heather D. Bennett. “Confronting The Growing Burden Of Chronic Disease: Can The U.S. Health Care Workforces Do The Job?,” Health Affairs 28, no. 1 (2009): 64. 232 Ibid.
70

aging population.233 This prevalence is significantly higher among populations at or
below the federal poverty level.234 As a result, federal programs that focus on providing
care for at-risk populations with chronic disease have the best chance at addressing this
growing issue.
Among chronically-ill patients who rely on care coordination for effective
treatment, this fragmentation is particularly impactful as these individuals receive care
from different physicians for different conditions and are very vulnerable because of this
disjointed approach. For example, when a patient is discharged from a hospital, new
medications that were prescribed may not have been communicated properly back to
the patient’s nursing home. As a result, there is a greater likelihood that the patient will
be readmitted to the hospital, leading to unnecessary healthcare expenditures as well as
poor healthcare delivery. In this one example, failures to coordinate care led to a $9,700
unnecessary hospital stay.235
A failure to coordinate care, or effectively transition a patient from one physician
to another, has contributed to unnecessary spending. In 2011, it was estimated that
poor transitional care management led to $25-45 billion in wasteful spending because of
avoidable complications and unnecessary hospital readmissions.236 These factors have
also led to costly readmission rates. A 2009 study found that 20% of all Medicare
beneficiaries who were discharged from the hospital were readmitted within 30 days,
233 Ibid. 234 Thomas Bodenheimer, Ellen Chen, and Heather D. Bennett. “Confronting The Growing Burden Of Chronic Disease: Can The U.S. Health Care Workforces Do The Job?,” Health Affairs 28, no. 1 (2009): 64. 235 Anne Pfuntner, Lauren M. Wier, and Claudia Steiner. “Costs for Hospital Stays in the United States, 2010,” Agency for Healthcare Research and Quality, last modified January 2013, http://www.hcup-us.ahrq.gov/reports/statbriefs/sb146.pdf. 236 Rachel Burton. “Improving Care Transitions,” Health Affairs Policy Brief, last modified September 13, 2012, http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_76.pdf.
71

and 34% were readmitted within 90 days.237 As a result, healthcare costs have risen
significantly over the past several decades, and many of these costs are due to wasteful
spending.
Wasteful & Unnecessary Spending
Throughout the healthcare reform debate, problems caused by the FFS system
were a key argument for the development of new care models that emphasize quality
rather than volume. Another critical component of reforming the nation’s health system
was to address wasteful spending. While the FFS system included a number of
inefficiencies related to care coordination and poor care delivery, there are a number of
additional issues plaguing the healthcare system that also contribute to wasteful
spending. Failures of care delivery including poor execution and failure to adopt best
care practices contributed to $102-154 billion in wasteful spending in 2011 alone.238
Overtreatment, administrative complexity, and pricing failures contributed to hundreds
of billions in additional costs, along with outright fraud and abuse. In total, it is
estimated that between 558 billion and 1.2 trillion dollars are spent wastefully each
year.239 To address problems with the FFS system, including failures to coordinate care
and wasteful spending, there are a number of provisions included in the ACA to help
streamline care delivery and ensure higher quality care.
237 Stephen F. Jencks, Mark V. Williams, and Eric A. Coleman. “Rehospitalizations among Patients in the Medicare Fee-for-Service Program,” The New England Journal of Medicine 360 (2009) 1421. 238 Rachel Burton. “Improving Care Transitions,” Health Affairs Policy Brief, last modified September 13, 2012, http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_76.pdf. 239 Ibid.
72

Provisions to Improve Care and Reduce Costs
In response to fragmented approach of the FFS system, and the rising healthcare
costs that resulted, the ACA included a number of provisions to begin shifting care
delivery away from a volume-based system into one that incentivizes improvement in
patient outcomes and cost-efficiency. Achieving this goal required developing new care
delivery models that provide performance-based compensation and team-based
approaches to address failures in care coordination and unnecessary spending caused
by inefficiency. These programs included the Medicare Shared Savings Program (MSSP),
the Pioneer Accountable Care Organization (ACO), and Patient-Centered Medical Homes
(PCMHs). Each of these programs seeks to improve care and reduce costs by
streamlining the way that healthcare is delivered. These care models leverage a team-
based approach to improving patient outcomes by incentivizing physicians to provide
quality care at lower costs.
One population that can be most impacted by the establishment of these new
models are individuals living with chronic diseases like diabetes. Diabetes is a disease
closely linked to obesity and one that, like obesity, has been rising to an epidemic
proportion. Currently, it is estimated that nearly 1 in 3 Medicare dollars are spent on
diabetes or its complications—a figure estimated to be $245 billion annually.240 Patients
with diabetes are particularly primed for patient-centered care delivery through models
like the PCMH or ACO. These models’ focus on coordinated care and shared decision
making are particularly useful in improving outcomes. Evaluating how these programs
240 National Diabetes Statistics Report 2014. Atlanta: Centers for Disease Control and Prevention, 2014.
73

can improve care and reduce costs and successes to date in the area of diabetes can
help inform whether the ACA can actually reform the U.S. healthcare system.
The Medicare Shared Savings Program
The MSSP was established to as a new approach to healthcare delivery which
utilizes new care models called accountable care organizations (ACOs) to deliver
coordinated, high-quality care while reducing healthcare costs. ACOs incentivize
physicians and hospitals to work together to improve outcomes while reducing costs for
the patients that they treat. These organizations can take many forms. Integrated
delivery systems, involving common ownership by multiple hospitals and physician
practices are the largest such models.241 These entities often have shared financial
incentives, electronic health records, and care teams across the care continuum.242
Multispecialty group practices are either owned by the hospital, or have a strong tie to
one, and have robust mechanisms for providing coordinated clinical care.243 Physician-
hospital organizations (which are a subset of a hospital’s staff), independent practice
associations comprised of individual physician practices, and virtual physician
organizations of independent practices that are generally in rural areas are also
examples of structures that can make up an ACO. 244
In order to become an ACO, providers must be able to care for at least 5,000
Medicare beneficiaries, have the ability to report cost and quality data, and agree to
241 Stephen M. Shortell, Lawrence P. Cassalino, and Elliott S. Fisher. “How The Center for Medicare and Medicaid Innovation Should Test Accountable Care Organizations,” Health Affairs 29, no. 7 (2010): 1294. 242 Ibid. 243 Ibid. 244 Ibid.
74
participate for at least 3 years. Participating ACOs receive payments for shared savings
when they can provide care to beneficiaries at a lower cost than Medicare benchmarks
while also achieving quality standards. This helps to incentivize higher quality care at
lower costs. Whether an ACO meets these goals is based on data reported to Medicare
that details the quality of patient and caregiver experiences, caring for at-risk
populations, effective care coordination and patient safety, and preventive care.245
These practices must also accepted shared financial risk for any losses that occur. While
establishing an ACO can be cost-prohibitive, the federal government has put aside
resources to help smaller practices join alternative payment models, like ACOs. This
shared-risk, shared-reward model intends to increase the stake that physicians and
practices have in improving outcomes for their patients. Overall, the goals of these ACOs
are to improve the health of the population, to reduce per capita costs, and to improve
care for the individual. These ACOs would receive a share of the savings as an incentive
for achieving these goals.
ACOs have the potential to address a number of issues that plagued the pre-ACA
healthcare system. Financial incentives provided by shared savings can help promote
team-based care and the use of performance measures to improve patient care. These
models can also enable primary care practices to care for more patients by leveraging
this approach. This is particularly important given workforce shortages currently
experienced by primary care and the expected increase in the number of insured
245 The Centers for Medicare and Medicaid Services. Division of Accountable Care Organization Populations Seamless Care Models Group. Accountable Care Organization 2014 Program Analysis Quality Performance Standards Narrative Measure Specifications. (Baltimore, Maryland, 2014), http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Downloads/ACO-NarrativeMeasures-Specs.pdf (accessed July 2, 2015).
75
patients due to the ACA. In 2014, 4 million Medicare beneficiaries, or 14% of the
Medicare population, were being cared for by an ACO.246 When combined with the
private sector, 428 provider groups were participating in an ACO.247
Since the implementation of the MSSP, the ability for ACOs to improve patient
outcomes and to reduce costs have been mixed.248 Of the 204 ACOs that participated in
the program in 2012 and 2013, 53 of the organizations demonstrated costs savings
which totaled more than $300 million.249 In analyzing the savings that were achieved,
the Centers for Medicare and Medicaid Services found that preventing initial hospital
visits was a key aspect of these cost reductions. This analysis also found lower costs for
primary care services because of lower-cost settings and chronic disease prevention and
management.250
Successes for patients with diabetes were also mixed. In a Wisconsin ACO
comprised of two health systems, Bellin Health and ThedaCare, patients with diabetes
had significantly lower blood sugar levels than the target established by Medicare.251
Eighty-four percent of patients were able to meet that target, which exceeds the
average ACO rate of 65%.252 In the Accountable Care Coalition of Maryland, however,
246 Jenny Gold. “FAQ on ACOs: Accountable Care Organizations, Explained,” Kaiser Health News, last modified April 16, 2014, http://kaiserhealthnews.org/news/aco-accountable-care-organization-faq/. 247 Ibid. 248 Farzad Mostashari and Ross White. “The ACO Hypothesis: What We Are Learning,” The Healthcare Blog, March 12, 2014, http://thehealthcareblog.com/blog/2014/03/12/the-aco-hypothesis-what-were-learning/. 249 Andrew J. Shin, Stephen M. Weiner, and Stephanie D. Willis. “CMS Releases MSSP and Pioneer ACO Data on Shared Savings and Loses—Where Do We Go From Here?,” Health Law and Policy Matters, last modified September 23, 2014, http://www.healthlawpolicymatters.com/2014/09/23/cms-releases-mssp-and-pioneer-aco-data-on-shared-savings-losses-where-do-we-go-from-here/ 250 Ibid. 251 Jordan Rau. “Medicare Data Show Wide Differences in ACOs’ Patient Care. Kaiser Health News, last updated February 27, 2014, http://khn.org/news/medicare-data-shows-wide-differences-in-acos-patient-care/. 252 Ibid.
76
only 24% of patients with diabetes were able to keep their blood sugar under control.253
These diverging outcomes can be attributed to a number of factors. Because of the wide
variance in the types of ACOs (physician practices vs. integrated health systems),
comparing this data is difficult. However, those ACOs that have been successful have
been smaller, more flexible practices that provide a higher number of primary care
services which can improve care and reduce costs.
The shared-risk, shared-reward nature of ACOs could be problematic for patients
with diabetes as it may cause participating practices to only provide care for low-risk
patients that have the most potential to improve their health. Given the complex nature
of diabetes, this practice could be particularly detrimental as physicians have poor
control over the outcomes that occur. The self-management and adjustment of various
therapies can lead to poor progress even when the patient is educated on how to dose
themselves. The correlation between poor diet and disease progression is a
compounding factor, particularly among lower-income individuals who cannot afford to
improve their eating habits to positively impact their health. Adverse selection practices
should be monitored among ACOs to ensure that even the most complex patients have
access to optimal care.
Pioneer ACO
A similar healthcare delivery model to the MSSP is the Pioneer ACO. The Pioneer
ACO was also included in the ACA for practices that are already experienced in high-
253 Jordan Rau. “Medicare Data Show Wide Differences in ACOs’ Patient Care. Kaiser Health News, last updated February 27, 2014, http://khn.org/news/medicare-data-shows-wide-differences-in-acos-patient-care/.
77

quality care coordination for patients across care settings. The Pioneer ACO will enable
these practices to transition from a shared savings payment model to a population-
based, per patient per month payment model. These ACOs are similar to those used in
the MSSP but they are tracked separately and have a higher risk and reward model that
can serve as a basis for future iterations of ACOs.254 This enables Medicare to test
alternative program designs and payment arrangements that can best improve care and
generate savings to the program.255 These efforts can then inform future requirements
and models for participating in the MSSP. This program also works with private payers
to align incentives offered from the federal programs to improve the quality and health
outcomes for patients in the Pioneer ACO and to achieve cost savings.256
As a result of the implementation of this provision of the ACA, the Pioneer ACO
saved Medicare $384 million in two years.257 Participants in the program spent an
average of $300 per patient per year while continuing to deliver high-quality patient
care. Currently the Pioneer ACO is serving more than 600,000 Medicare patients who
reported that they receive more timely and better communication with their provides,
use inpatient hospital services less, have fewer tests and procedures and see their
physicians more often following a hospital discharge than their counterparts in the FFS
system.258 In addition, the Pioneer ACOs prevented an estimated 70,000 hospital
readmissions collectively by keeping patients healthier and ensuring that they
254 “Pioneer ACO Model Frequently Asked Questions,” (Washington, D.C., The Centers for Medicare and Medicaid Services, 2015). 255 Ibid. 256 “Pioneer ACO Model Frequently Asked Questions,” (Washington, D.C., The Centers for Medicare and Medicaid Services, 2015). 257 The U.S. Department of Health and Human Services. “Affordable Care Act Payment Model Saves More than $384 Million in Two Years, Meets Criteria for First-ever Expansion,” press release, May 4, 2015, http://www.hhs.gov/news/press/2015pres/05/20150504a.html. 258 Ibid.
78
understand their treatment plans.259 For example, one of the participating ACOs, Banner
Health Network, sends nurse to patients’ homes to help with prescription drug
management, diabetes care education, and arranging for needed services on a patient-
by-patient basis.260 Compared to FFS practices, each ACO performed better overall in
providing quality care.261
The Pioneer ACO also demonstrated some improvements for the care of patients
with diabetes. Participating organizations achieved blood pressure control among 68%
of patients with diabetes, compared to 55% in the non-Pioneer control group.262 These
practices also achieved greater cholesterol control for these patients with a 57%
compliance rate as opposed to the 48% rate in standard FFS practices.263 The extent to
which improvements in outcomes also translates into savings are mixed, however.264 In
general, the participating ACOs that scored higher in improving outcomes for patients
with diabetes also had modest financial performances.265 Those ACOs with stronger
financial performances scored lower in improving diabetes outcomes.266 Therefore, it is
unclear the extent to which these models can improve health for patients with diabetes
while also generating substantial savings to the Medicare program.
There a number of factors that may influence the performance of these ACOs in
caring for the diabetic population, however. Meeting diabetes targets like lower blood
259 Ashley Force. “Pioneer Accountable Care Organizations Report Successful Results,” Dorland Health, 2015, http://www.dorlandhealth.com/dorland-health-articles/Pioneer-Accountable-Care-Organizations-Report-Successful-Results. 260 Ibid. 261 Ibid. 262 The Centers for Medicare and Medicaid Services, “Pioneer Accountable Care Organizations Succeed in Improving Care, Lowering Costs,” press release, July 16, 2013. 263 Ibid. 264 Ibid. 265 Mary K. Caffrey. “Among ACO Pioneers, Data Reveal Diabetes Performance Paradox,” American Journal of Managed Care, published online December 4, 2014. 266 Ibid.
79

sugar levels are largely contingent upon the patient adhering to his or her treatment
protocols. Poor diet, a lack of exercise, and a complex regimen of medications and/or
insulin dosages are key barriers often seen in this patient population. In addition, these
ACOs care largely for Medicare patients who are older and often have more complex
diabetes and comorbid conditions. These factors may also impact the amount of time
and resources needed to spend on these patients to achieve better results. Finally,
these data are only from the first two years of these programs. Oftentimes, overall
improvements in the health of patients with diabetes take more time as lifestyle
interventions and educational sessions are needed for successful treatment.
Furthermore, additional data are needed to assess whether similar results would occur
in the nonelderly population who may have less complex cases of diabetes. Leveraging
these team-based approaches to coordinating care earlier in the progression of the
disease may also help ensure that these individuals can appropriately manage and treat
their diabetes from the outset.
Patient Centered Medical Homes & the Primary Care Problem
The ACA also included provisions to encourage widespread adoption of the
Patient-Centered Medical Home (PCMH). The PCMH is a care model that promotes the
use of a strong primary care foundation and patient-centered approaches to improve
healthcare delivery. As described by Rittenhouse and colleagues, “the model combines
the core tenets of primary care (first-contact care that is continuous, comprehensive,
and coordinated across the care continuum) with 21st century practice innovations such
80

as the use of electronic information systems, population-based management of chronic
illness, and continuous quality improvements.”267 While PCMHs serve as the basis for
ACOs, instead of a shared-risk/shared-reward model for improving outcomes, the PCMH
believes that incentives for an enhanced infrastructure and a primary care base can
result in higher quality at lower costs. Evidence has found that PCMH’s resulted in
better overall patient experiences, improved patient outcomes through the receipt of
preventive services, and better chronic care management. These studies have also
shown that if scaled nationally, PCMHs could save Medicare and Medicaid an estimated
$175 billion through 2020.268
PCMHs focus on shared decision-making between physicians and patients to
make joint decisions that can improve wellness. These decisions are patient-centered,
meaning that the patient’s needs and preferences are an integral component to
enhancing care. This runs counter to a top-down approach often utilized by physicians
who diagnose their patients and tell them how to get better, rather than a holistic
understanding causes and barriers including and beyond clinical factors. These practices
also coordinate care with the patients, caregivers, pharmacists, and specialty practices
to ensure that the entire care team is working together to improve patient outcomes.
The PCMH model is based on studies that have found that patients who have
access to a regular primary care physician are more likely to receive preventive health
267 Diane R. Rittenhouse, Stephen Shortell, and Elliot Fisher. “Primary Care and Accountable Care—Two Essential Elements of Delivery-System Reform,” The New England Journal of Medicine 361 (2009) 2301. 268 Cathy Schoen. “The Path to a High Performance U.S. Health System: A 2020 Vision and the Policies to Pave the Way,” (New York, NY, The Commonwealth Fund Commission on a High Performance Health System, 2009) 13.
81

services and to receive treatment before more serious, costly complications develop.269
These individuals also have fewer preventable hospitalizations and emergency room
visits than those without access to a main primary care physician.270 The PCMH
approach generally takes more time to treat patients than many primary care physicians
are able to afford. Due to workforce shortages in primary care along with the high rates
of uninsured Americans, only two-thirds of adults reported having access to a primary
care provider while nearly three-quarters had difficulty getting an appointment.271 As a
result, particularly among chronically-ill, elderly, and low-income individuals, this has
further driven up costs due to unnecessary hospitalizations and emergency room visits.
As such, in order for this model to work, it will require incentives that reward high-
performing primary care physicians.
269 Karen Davis, Melinda Abrams, and Kristof Stremikis. “How the Affordable Care Act Will Strengthen the Nation’s Primary Care Foundation,” (New York, NY, The Commonwealth Fund, 2010) 1201. 270 Ibid. 271 Ibid.
82

Fig. 12: Key Principles of the Patient-Centered Medical Home272
To address these problems, the ACA included a number of provisions to bolster
the primary care workforce and to promote the use of the PCMH. States were offered
an option to increase reimbursement to “health homes” that utilized principles of the
PCMH but that also served Medicaid patients with chronic illnesses.273 States that
participate in this program will receive a two-year, 90 percent federal match on costs
associated with implementing care teams for Medicaid patients.274 Health homes
diverge slightly from a true PCMH due to a greater emphasis on integration with public
health. This PCMH-derivative also varies in that state can design an appropriate
272 Carman A. Ciervo, Jay H. Shubrook, and Paul Grundy. “Leveraging the Principles of Osteopathic Medicine to Improve Diabetes Outcomes Within a New Era of Health Care Reform,” The Journal of the American Osteopathic Association 115, no. 4 (2015) eS10. 273 Karen Davis, Melinda Abrams, and Kristof Stremikis. “How the Affordable Care Act Will Strengthen the Nation’s Primary Care Foundation,” Journal of General Internal Medicine 26, no. 10 (2011) 1201. 274 Kenneth E. Thorpe. “The Affordable Care Act Lays Groundwork for a National Diabetes Prevention and Treatment Strategy,” Health Affairs 31, no 1 (2012) 64.
83
payment approach that works best for their system.275 If adopted by all states, it was
expected that up to 10 million Medicaid beneficiaries with chronic illness could
participate in a health home by 2011.276 The law also sought to address the problem of
primary care workforce shortages by allocating $3.5 billion over five years to provide a
10% bonus to primary care physicians who served Medicare beneficiaries.277 These
physicians were further incentivized to see Medicaid patients by paying for these
services at the same rate as Medicare, a provision amounting to $8.3 billion increase in
reimbursement.278 The ACA also allocated $1.5 billion to incentivize medical students to
specialize in primary care through a series of scholarship and loan forgiveness
programs.279
The PCMH model has shown great potential to improve the care for and
outcomes of patients with diabetes. A number of demonstration projections, which
have been underway since the implementation of health care reform have shown that
these care models can reduce emergency room visits and hospitalizations for these
patients. An Independence BlueCross BlueShield PCMH practice had 9.5-12% reductions
in emergency room visits and a similar facility in Colorado reported a 9% reduction in
hospital admissions.280 These PCMHs have also been successful in improving patient
outcomes. The California Academy of Family Physicians and Community Medical
Providers PCMH reported a 50% increase in the number of patients with diabetes who
275 Davis, “How the Affordable Care Act Will Strengthen the Nation’s Primary Care Foundation,” 1202. 276 Ibid. 277 Ibid. 278 Ibid. 279 Ibid. 280 Carmen A. Ciervo, Jay H. Shubrook, and Paul Grundy. “Diabetes Management Within Evolving Healthcare Delivery Models: The Osteopathic Perspective,” The Journal of the American Osteopathic Association 115, no. 4 (2015) eS6.
84

had controlled blood sugar levels.281 This practice also demonstrated improved blood
pressure control and LDL cholesterol levels among its patients with diabetes. The
Missouri Health Homes reported a 25% improvement in cholesterol, a 32%
improvement in blood pressure, and a 35% improvement in hemoglobin A1C in their
patients with diabetes as well.282 As for costs, GroupHealth Cooperative, a PCMH that
has operated since 2006, has reported that it recouped its expenditures for increased
infrastructure within the first year.283 The Cooperative received a return on investment
of 1.5:1 by 21 months, or $1.50 in return for every dollar spent.284
The use of new technology by these alternative payment models has also been
successful in improving outcomes and reducing costs for patients with diabetes. The use
of telehealth to facilitate care management has decreased hospital inpatient stays by
10%, emergency room visits by 10%, and decreased overall cost of patient care by
9%.285
281 Ibid. 282 Ibid. 283 Robert J. Reid, et al. “The Group Health Medical Home At Year Two: Cost Savings, Higher Patient Satisfaction, and Less Burnout for Providers,” Health Affairs 29, no. 5 (2010) 842. 284 Ibid. 285 Medical Cost Trend: Behind the Numbers 2016. (Washington, D.C., PriceWaterhouseCoopers, 2015).
85
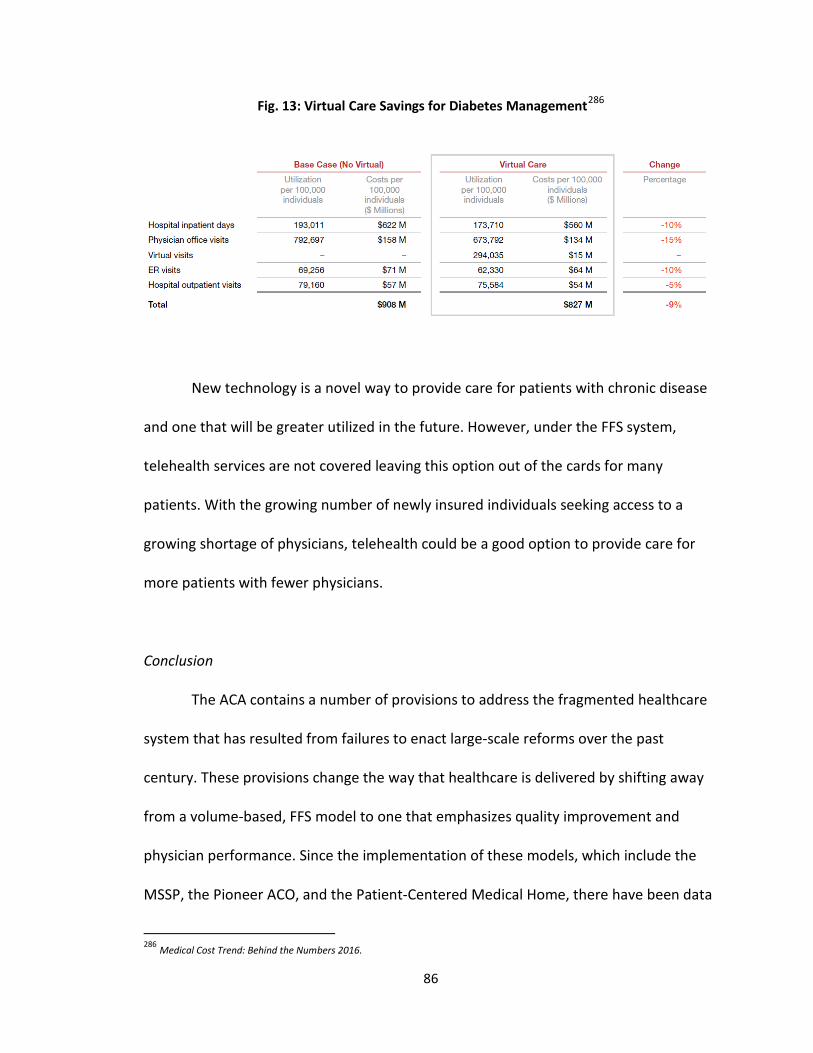
Fig. 13: Virtual Care Savings for Diabetes Management286
New technology is a novel way to provide care for patients with chronic disease
and one that will be greater utilized in the future. However, under the FFS system,
telehealth services are not covered leaving this option out of the cards for many
patients. With the growing number of newly insured individuals seeking access to a
growing shortage of physicians, telehealth could be a good option to provide care for
more patients with fewer physicians.
Conclusion
The ACA contains a number of provisions to address the fragmented healthcare
system that has resulted from failures to enact large-scale reforms over the past
century. These provisions change the way that healthcare is delivered by shifting away
from a volume-based, FFS model to one that emphasizes quality improvement and
physician performance. Since the implementation of these models, which include the
MSSP, the Pioneer ACO, and the Patient-Centered Medical Home, there have been data
286 Medical Cost Trend: Behind the Numbers 2016.
86
suggesting that there is great potential to generate savings to the Medicare program
and to improve the care that is delivered. The MSSP and Pioneer ACO models have
already saved Medicare hundreds of millions of dollars in two years. Projections indicate
that fully scaling PCMHs nationwide would save an additional $175 billion through
2020.287 Data also suggest that integrated delivery models can improve patient
outcomes. Medicare beneficiaries that receive care from ACOs report a stronger
relationship with their provider, fewer hospitalizations and emergency room visits, and
a better safety net to ensure adherence to treatment recommendations. Patients
receiving care through PCMHs or PCMH-derivative models like health homes have
reported similar outcomes. Therefore, in evaluating whether new care delivery models
enacted by the ACA have potential to reduce costs and improve care, existing data
would indicate that can achieve this goal in the aggregate.
When assessing whether these new models improve care and reduce costs for
patients with diabetes, however, the data are mixed. ACOs that have demonstrated that
they could improve outcomes and reduce complications for patients with diabetes also
generated limited savings, on the whole. In the same regard, the ACOs that generated
the most savings had the most limited improvement in patient outcomes for these
patients. While there is data to suggest that a few of these organizations could achieve
both goals, without additional piloting it is unclear that these successes could be
extrapolated nationally.
287 Karen Davis, Melinda Abrams, and Kristof Stremikis. “How the Affordable Care Act Will Strengthen the Nation’s Primary Care Foundation,” Journal of General Internal Medicine 26, no. 10 (2011): 1201-1203.
87

ACOs that were successful in improving outcomes and reducing costs were more
likely to mimic those models developed under PCMH principles. These practices were
more likely to be physician-led rather than hospital-run and utilize more primary care
services.288 It is likely that these practices, because they were smaller, were better able
to be flexible in their approaches to care and in their ability to implement continuous
improvement processes for chronic disease management and care coordination.289
These processes lend themselves well to a primary care environment that provides
evaluation and management services more than procedures and surgeries.290 Evaluation
and management services can be bolstered by care teams comprised of nurses,
pharmacists, and clerical staff who can coordinate care and ensure that the patient
receives the needed services. For practices that are largely procedural-based, it is more
difficult for these services to be shared among multiple members of a care team to the
same degree. Therefore, it is possible that these smaller, more successful patients were
able to deliver care to more patients at a lower cost because they could utilize other
members of their team to supplement these efforts. In turn, the patient received
additional services, including follow-up care management services to ensure that the
treatment regimen was being followed, which helped to improve the patient outcomes.
Understandably, it could be difficult for large ACOs, particularly those comprised
of hospitals, to achieve cost savings by improving quality because doing so could affect
their bottom line. Hospitals receive a substantial portion of their revenue from high-cost
288 Farzad Mostashari and Ross White. “The ACO Hypothesis: What We’re Learning,” The Health Care Blog. March 12, 2014. http://thehealthcareblog.com/blog/2014/03/12/the-aco-hypothesis-what-were-learning/ 289 Ibid. 290 Ibid.
88
services like admissions, emergency department visits, and surgeries. For ACOs still
operating under the FFS system, too much of a reduction in procedures, admissions, and
emergency visits could seriously erode revenue even with the added potential of shared
savings.291 While factors influencing why larger ACOs have been less successful in
improving outcomes and reducing costs for patients with diabetes are complex, it is
clear that a FFS model hinders potential improvements in quality because of its impact
on revenue. Hospitals under the FFS system will always make more than those under an
ACO model because of the number of high cost services that they provide. The greater
emphasis on prevention and wellness under integrated delivery models are services
rendered at a lower cost, meaning lower revenue. Because of this, it is important for the
federal government to evaluate new payment mechanisms for providing these services
that prevents hospitals from driving up unnecessary costs.
The Pioneer ACO program seeks to evaluate such payment mechanisms and the
results to date have been better than those under the MSSP program. Under the
Pioneer ACO model, systems receive a per-patient per-month fee, called capitation, for
the care provided. Those ACOs operating under this model performed far better in
improving care and reducing costs. In two years, the Pioneer ACOs prevented 70,000
hospital readmissions and saved Medicare $384 million.292 This was achieved through
enhanced care coordination and wellness practices that kept patients healthier overall.
Patients will diabetes excelled under this model because of these services and had
291 Mostashari, 2014. 292 The U.S. Department of Health and Human Services. “Affordable Care Act Payment Model Saves More than $384 Million in Two Years, Meets Criteria for First-ever Expansion,” press release, May 4, 2015, http://www.hhs.gov/news/press/2015pres/05/20150504a.html.
89
overall reductions in blood pressure, cholesterol, and blood sugar levels. As healthcare
could be moving in the direction of bundled payments like those under the Pioneer
model, these findings are important to note.
Critics of ACOs argue that the movement toward bundled payment systems
would be a failure similar to that seen under the FFS system contemporary, capitation.
In the 1980s and 1990s, many providers operated under capitation, a fixed payment by
managed care organizations to providers for each patient that they care. This is similar
to the per-patient per-month fee utilized by Pioneer ACOs. Providers who cared for the
patient at a lower cost than the payment were able to keep the difference. However,
there was not a parallel approach to ensure quality improvement in tandem. As a result,
this model may have incentivized undertreatment which caused greater use of FFS
payments. Through the FFS system, the federal government and private payers could
attempt to contain costs through the number of services that were provided rather than
the patients seen. While capitation was an abject failure because of poor resources,
weak management, and an inability to control the use of healthcare services to contain
costs, many are concerned about the potential to venture down the same again with the
new delivery models under the ACA.293 However there are a number of key differences
that prevent what ACOs and PCMHs are trying to achieve from repeating the mistakes of
the past.
During the period of capitation, financial risk for patients was not tied to quality
care. Under the ACA, ACOs must meet high standards in terms of quality and patient
293 Samuel H. Zuvekas and Joel W. Cohen. “Paying Physicians by Capitation: Is the Past Now Prologue?,” Health Affairs 29, no. 9 (2010): 1661.
90

outcomes in order to share in cost-savings earned by more efficient care. In addition,
the advent of new technology to provide better tracking and reporting that can enable
care teams to manage more patients efficiently was not available when capitation was
used previously. These advances can also enable continuous improvement processes for
each practice based on their patient composite and available resources. Because of
these factors, it is unlikely that failures of new care models would mimic those seen
through capitation previously. However, failure is still a possibility.
Until additional testing and refinement can be conducted, it is unclear the extent
to which these care models will be able to make a significant impact on patients with
diabetes. Diabetes-specific ACOs and PCMHs will need to be tested to better understand
why some models cannot improve both quality and care for this patient population.
However, overarching data on these models has shown a great potential to help address
primary care shortages and to improve care coordination and patient outcomes. It will
be critical however, for these models to be accepted broadly by the medical community
to increase uptake and for large-scale advances to take hold.
91

Conclusion & Key Findings
The implementation of the Affordable Care Act (ACA) provides a critical
opportunity to assess whether the law has the ability to truly reform the nation’s
healthcare system. Provisions contained in the ACA purport to improve quality care and
to reduce outcomes; however, until recently, there have been little opportunity to
examine whether these claims hold true. As the federal government moves forward in
expanding access to health insurance and in scaling prevention and new care delivery
programs, these data are now becoming available. Because of these factors, this thesis
sought to understand whether expanding access to key prevention programs and
healthcare delivery models will actually improve care and reduce costs to examine the
extent to which the ACA will be successful. Because of the impact that chronic diseases
have on healthcare expenditures and overall patient health, this portfolio used one such
disease, diabetes, as a case study to assess the success of these prevention and
92
healthcare delivery provisions. By using diabetes as a lens in which to examine these
outcomes, one can better understand the impact that the ACA could have on a more
individual level. This evaluation determined that the ACA does have potential to
improve care and to reduce costs but that continuous improvement processes to refine
existing programs and healthcare delivery models will be critical to this success.
The first chapter delved into the necessitation of healthcare reform through a
historical review of policy failures to improve public health. This chapter found that the
economic and political unviability of large-scale, comprehensive reforms created an
environment in which policymakers could only address the needs of the most vulnerable
populations. Significant programs like Medicare and Medicaid resulted from this
approach but it also resulted in a fragmented system that left many of the lower-
income, working class without access to affordable health insurance. The decline of
organized labor, discriminatory practices by insurance companies, and rising healthcare
costs further exacerbated these coverage gaps resulting in 49 million uninsured
individuals by 2010.294 Failures to access care because of the lack of insurance and/or
high costs contributed to a decline in population health that could only be addressed
through a comprehensive effort to expand access to insurance and to reduce healthcare
costs.
The passage of the ACA was the first comprehensive effort to achieve these goals
in the nation’s history. The second chapter of this thesis evaluated how the ACA
increased access to insurance as well as key prevention and wellness services that were
294 The Department of Health and Human Services. Assistant Secretary for Planning and Evaluation Issue Brief. Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey. Washington, DC, 2014, http://aspe.hhs.gov/health/reports/2011/cpshealthins2011/ib.pdf (accessed July 1, 2015).
93
included with the intent to improve overall population health. Provisions included to
improve access to affordable insurance were largely successful. Federal subsidies were
given to individuals with incomes up to 400% of the federal poverty level.295 Public
programs like Medicaid were expanded to serve as a safety net for the most vulnerable
populations. Insurance companies were prohibited from using predatory practices like
denying coverage because of pre-existing conditions or implementing lifetime limits. As
a result of these provisions, 11.7 million Americans had enrolled in healthcare
exchanges which were established to make insurance more affordable.296 Eight-five
percent of these individuals were eligible for subsidies to help cover these costs.297 By
2017, it is estimated that the number of individuals enrolled in these exchanges will
increase to 25 million.298
This chapter also explored whether expanded access to health insurance will also
correlate with expanded access to care. Efforts to decrease rates of the uninsured will
be fruitless in improving population health unless these individuals utilize the services
afforded to them under new, more comprehensive health plans. As increased use of
preventive services by even 5% has the potential to save 100,000 each year, accessing
these services are critically important to improving overall population health.299 The
chapter found that increasing access to insurance did correlate with increased utilization
of healthcare services. By 2014, 76 million Americans had accessed no-cost preventive
295 Ibid. 296 Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report. (Washington, D.C. The Department of Health and Human Services, 2015). 297 Ibid. 298 David Blumenthal and Sara Collins. “Health Care Coverage under the Affordable Care Act—A Progress Report,” The New England Journal of Medicine 371(2014):275. 299 Ashley B. Coffield and Michael Maciosek. Preventive Care: A National Profile on Use, Disparities, and Health Benefits. (Washington, D.C., The Robert Wood Johnson Foundation, 2007,) 1.
94
services provided under the Essential Health Benefits provision in the ACA.300 The
Medicaid expansion resulted in a 23% increase in newly identified patients with earlier
stage diabetes as a result of these preventive services.301 The closure of the Part D
Medicare donut hole reduced co-payments for medications that seniors were being
forced to pay out-of-pocket saving an estimated $425 million on diabetes medications in
2012 alone.302 As many of these individuals were forgoing treatment because of these
costs, this closure helped to prevent disease progression and the onset of complications
and hospitalizations. For patients with diabetes, this is of particular importance given
the multiple daily medications these individuals need to keep their disease in control.
The aforementioned data indicate that newly insured individuals are utilizing
preventive services and that those individuals who were underinsured have benefited
from more comprehensive requirements in health plans. Individuals who had insurance
prior to the passage of the ACA and were able to access the services they need may
have seen deductibles and the cost of their insurance plans increase. This will need to
be addressed moving forward to ensure that new coverage gaps do not emerge because
of these increases.
Finally, lifestyle intervention programs under the ACA, like the National Diabetes
Prevention Program, have demonstrated a great degree of success in preventing or
delaying the onset of diabetes through moderate weight loss and physical activity. This
serves as a key example of how evidence-based programs can make a significant
300 The Department of Health and Human Services, “Affordable Care Act Helps 76 Million Americans with Private Coverage Access Free Preventive Services,” press release, June 27, 2014, http://www.hhs.gov/news/press/2014pres/06/20140627b.html. 301 Kaufman, 835. 302 Burge, 402.
95
difference in the lives of individuals living with chronic disease. However, these
programs must be scaled nationally and fully funded in order for these successes to be
transformational in reducing the rates of diabetes in America.
The final chapter discussed how new care delivery models can help improve the
quality of care and reduce costs to the U.S. healthcare system. Fragmented approaches
to care and a fee-for-service, volume-based system has created a defensive medicine
model emphasizing treatment over wellness. Wasteful and unnecessary spending
caused by inefficiency, overtreatment, and outright fraud and abuse has increased
healthcare costs and poor patient outcomes. The ACA sought to address this sick care
system by incentivizing the use of new care delivery models that utilize team-based
approaches to care and enhance care coordination. This chapter discussed the Medicare
Shared Savings Program (MSSP), the Pioneer ACO, and the Patient-Centered Medical
Home (PCMH) to assess whether these new models could improve care and reduce
costs for patients with diabetes.
The accountable care organizations (ACOs) participating in the MSSP generated
$300 million in savings to the Medicare program in 2012-2013.303 Findings were mixed
in whether these ACOs could also improve patient outcomes, however. Of the models
evaluated in this chapter, the MSSP ACOs were the least successful in improving care for
patients with diabetes. Overall, these ACOs were purported to have achieved cost-
savings while meeting quality benchmarks. However, the data on improving outcomes
303 Andrew J. Shin, Stephen M. Weiner, and Stephanie D. Willis. “CMS Releases MSSP and Pioneer ACO Data on Shared Savings and Loses—Where Do We Go From Here?,” Health Law and Policy Matters, last modified September 23, 2014, http://www.healthlawpolicymatters.com/2014/09/23/cms-releases-mssp-and-pioneer-aco-data-on-shared-savings-losses-where-do-we-go-from-here/
96
for diabetes widely varied between ACOs. Some were successful in improving patient
outcomes however other ACOs saw minimal success. While there could be a number of
factors contributing to these variances, further examination will be necessary.
Similarly, the ACOs participating in the Pioneer ACO program also demonstrated
cost reduction while meeting quality benchmarks. These ACOs were estimated to have
saved Medicare $384 million over two years and they performed better overall in
improving patient care when compared to fee-for-service practices.304 However, when
assessing its performance on patients with diabetes, these data are mixed. Practices
that scored the best in improving diabetes outcomes only generated modest cost
reductions. Those with the lowest scores in diabetes improvement generated the most
cost savings. Therefore, while these ACO models have generally shown to improve
outcomes and reduce costs, when evaluating specific disease performance these results
may not be able to be extrapolated.
PCMHs had the most possibility in improving outcomes for patients with
diabetes while reducing costs. However, these practices are not set up to achieve a
great degree of cost reduction for federal programs. Rather, they are intended to
streamline the practice of primary care and to utilize care coordination and technology
to help provide better care and to reduce unnecessary complications and
hospitalizations. These principles lend themselves well to treatment of patients with
diabetes that require a great deal of self-management, training, and coordination.
Because of this, these practices were consistently shown to reduce hospital admissions
304 The U.S. Department of Health and Human Services. “Affordable Care Act Payment Model Saves More than $384 Million in Two Years, Meets Criteria for First-ever Expansion,” press release, May 4, 2015, http://www.hhs.gov/news/press/2015pres/05/20150504a.html.
97
and to improve diabetes control. The small scaled nature of these models does not
generate substantive savings to federal programs by their very nature. However, if these
models were scaled nationally they could save up to $175 billion by 2020.305
Overall, this chapter found that there is a great deal of potential in the further
development and use of new care models like PCMHs and ACOs. However, continuous
improvement processes will be necessary to ensure that these models can achieve both
cost savings and improvement in patient outcomes. However, when considering the
current FFS model used and its resulting failures to achieve either goal, it is important to
continue to pilot and test these new care models.
Lessons Learned
There are a number of lessons learned through the evaluation of key provisions
in the ACA that expand access to affordable health insurance, preventive services, and
quality care. The first lesson is that the U.S. healthcare system was broken and could not
be reformed without addressing coverage gaps and the high cost of care. Small scale
efforts to reform this system had been attempted in the past and only served to further
fragment the care provided and to drive up the cost of healthcare. The ACA addresses
these problems by mandating that all Americans obtain health insurance and that all
businesses with more than 50 employees provide coverage.306 Making insurance more
affordable for low-to-middle class individuals was achieved by establishing healthcare
exchanges and by offering federal subsidies to help drive down the costs of health
305 Schoen, 13. 306 Ung, 459.
98
insurance. Insurance prices for individuals beyond 400% of the federal poverty level
have increased because of more comprehensive plans and because of the business
mandate in the ACA.307 However, these increases have been modest thus far. The
movement towards more high-deductible plans may be problematic in the future,
however, and an issue that should be considered if these prices continue to increase.
The second lesson learned is that population health cannot be improved without
a higher utilization of preventive services. Data has shown that increased access to
health insurance increases the use of these services and creates longer term cost
savings by keeping more Americans healthier. For patients with diabetes, access to
these services is particularly important to ensure that the vast majority of Americans
who are unaware that they have the disease are diagnosed and treated at an early
stage. Provisions included in the ACA to expand the Medicaid program, to include
Essential Health Benefits in all health plans, to decrease out-of-pocket costs to seniors
for prescription drugs, and to utilize lifestyle intervention programs to slow or prevent
the onset of disease have each benefited patients with diabetes. Long-term studies will
be needed to effectively assess the extent to which these programs have made an
impact on patient health, however. In addition, the increased detection of diseases
caused by these services could mean more healthcare expenditures per person over the
course of an individual’s lifetime. Data has shown that increased detection has had a
minimal impact on overall health spending, particularly because of the offset in costs of
307 Ibid.
99

having to treat later-stage illness and the complications and hospitalizations that result.
However, this should be kept in mind as expansion efforts to continue to be scaled up.
The third lesson from this analysis is that the high cost of healthcare cannot be
addressed without reforming the way that healthcare is delivered. The current volume-
based system incentivizes overtreatment and unnecessary testing because of fee-for-
service reimbursement. Failures to effectively coordinate care have caused many
patients to fall through the cracks and end up in emergency rooms or be hospitalized
because of avoidable complications. These factors have contributed to an increase in
healthcare costs which have been further exacerbated by outright fraud and abuse. The
ACA has sought to address these costs by streamlining healthcare delivery through the
use of new models that incentivize physicians to improve patient outcomes and reduce
costs. These models have shown to be successful overall but additional refinement must
be conducted to improve patient outcomes. For patients with diabetes, this is
particularly important as this disease lends itself well to enhanced care coordination and
physician engagement.
Limitations
In assessing the potential for the ACA to reform the nation’s healthcare system
by improving patient health while lowering costs, there were a number of data
limitations. This thesis evaluated the growth in the uninsured and the high costs of
healthcare and ways in which the ACA intends to address these factors. While data thus
far have indicated that the ACA has been successful in reducing the number of the
100

uninsured, there are 31 million Americans who will not be covered after all of the law
has been implemented.308 Addressing ways in which these individuals can be afforded
health insurance will be critical to improving overall population health. In addition, while
the Congressional Budget Office estimates that the ACA will reduce the deficit in the
long-term, short-term costs may impact insurance uptake and coverage gaps.
Healthcare costs continue to rise modestly as well. As a result, more employers are
moving towards high-deductible plans that will raise premiums for their employees. It
will be important to conduct further studies as to how and if this will impact insurance
coverage and the use of healthcare services. In addition, it will also be important for
care delivery models to be implemented effectively in order for these systems to reduce
unnecessary and wasteful spending. Data indicate that these models have
demonstrated that they have potential to reduce healthcare costs; however, physician
engagement and utilization of these models will be necessary for broad-scale success.
Individuals will need to access preventive services for additional savings to occur in the
long run. While studies have suggested that these services have been utilized by many
of the newly insured, these individuals will need to continue to receive these services to
transform the healthcare system away from the practice of defensive medicine.
Recommendations
Increasing the number of Americans who have access to insurance is critical in
reforming the healthcare system and in ensuring that individuals access care before
308 Frederic E. Shaw, Chisara N. Asomugha, Patrick H. Conway, Andrew S. Rein. “The Patient Protection and Affordable Care Act: Opportunities for Prevention and Public Health.” Lancet 384 (2014): 78.
101
diseases progress. However, the 25 million Americans who are expected to be newly
insured by 2017 will put a great amount of pressure on an already overloaded physician
workforce.309 While there are provisions included in the ACA that seek to incentivize
more physicians to enter the workforce, these efforts will take a number of years to
take hold. Because of this, while millions of Americans may now be able to access
healthcare services, many physicians may not be able to see new patients. For those
newly insured under the Medicaid programs, this could be especially problematic as the
rate of reimbursement is significantly lower for these patients than those under
employer-sponsored plans. Reimbursement for providing care to Medicaid individuals
should continue to be bolstered to increase access for these patients. New health
delivery models like PCMHs and ACOs enable physicians to see more patients by
expanding the use of care teams to track, manage, and coordinate care. While these
models need some refinement, these principles should continue to be used moving
forward to ensure that newly insured individuals can access care. The use of telehealth
and other technologies should also be ramped up to increase access to care and to
extend the limited amount of primary care physicians.
Failures to nationally scale the Medicaid expansion have created coverage gaps
for individuals who make too much to qualify for the program but who make too little to
receive subsidies under the ACA. As such, efforts to close this gap must be employed to
ensure that this vulnerable population can receive the services that they need. In
addition, to address the rising rates of diabetes in America, efforts to increase public
309 Blumenthal, 275.
102

awareness and to cover preventive programs like the NDPP will be essential to delaying
or avoiding the onset of the disease. While modest funding has been allocated as part of
the ACA to achieve this goal, additional resources will be needed to fully scale these
programs. Therefore, this thesis concludes that the following policies should be
implemented in order to ensure that the ACA can successfully reform the healthcare
system and address the diabetes epidemic:
• Bolster Medicaid payments to increase access to primary care services; • Utilize telehealth and other technologies to address workforce shortages; • Enhance care coordination and the use of care teams to effectively track
and manage more patients; • Work with states to expand the Medicaid nationally to ensure that more
low-income individuals have access to care; • Close the coverage gap caused by failures of states to expand
Medicaid programs; • Continue to incentivize physicians to specialize in primary care to create
a robust workforce to care for the newly insured; • Fully scale the NDPP and provide coverage for similar lifestyle
intervention programs; and • Test new care models that have the potential to improve quality and
reduce costs.
Evaluating the potential of the ACA to address diabetes and to reform the healthcare
system has produced mixed, yet optimistic results. While there continues to be a
number of areas in need of refinement, the nation is generally heading in the right
direction in resolving problems that developed because of the fragmented approach to
health policy in years past. Additional research will be necessary to ensure that the
comprehensive nature of the law does not drive up healthcare costs and impede access
to affordable health insurance. However, the subsidies in place ensure that the most
103

vulnerable populations have better access to care. Future policies to further decrease
the number of the uninsured will be necessary to ensure universal coverage, however.
Bibliography for Introduction
Blumenthal, David, and Sara Collins. “Health Care Coverage under the Affordable Care Act—A Progress Report,” The New England Journal of Medicine 371(2014):275-281.
Brown, Derek, and Timoth McBride. “Impact of the Affordable Care Act on Access to
Care for US Adults with Diabetes, 2011–2012,” Preventing Chronic Disease 12 (2015) 140431. doi: 10.5888/pcd12.140431.
Kaufman, Harvey W., Zhen Chen, Vivian A. Fonseca, and Michael J. McPhaul. “Surge in Newly Identified Diabetes Among Medicaid Patients in 2014 Within Medicaid Expansion States,” Diabetes Care 38 (2015) 833-837.
Miller, Tom. “Conservative Health-Care Reform: A Reality Check,” National Affairs 17 (2013): 3-18.
National Diabetes Statistics Report 2014. (Atlanta, GA: Centers for Disease Control and
Prevention, 2014). Shaw, Frederic E., Chisara N. Asomugha, Patrick H. Conway, and Andrew S. Rein. “The
Patient Protection and Affordable Care Act: Opportunities for Prevention and Public Health,” The Lancet 384, no. 14 (2014): 75-82.
The United States of Diabetes: Challenges and Opportunities in the Decade Ahead. (Washington, D.C., UnitedHealth Center for Health Reform & Modernization, 2010) 1-159.
Yang, Wenya, Timothy Dall, Pragna Halder, Paul Gallo, Stacey Kowal, and Paul Hogan.
104

“Economic Costs of Diabetes in the U.S. in 2012,” Diabetes Care, 35 (2013): 1033- 1046.
Bibliography for Chapter One Armour, Stephanie. “States Offer a Mixed Picture of Health Insurance Costs,” The Wall
Street Journal, June 24, 2015.
Ayanian, John Z., Joel S. Weissman, Eric C. Schneider, Jack A. Ginsburg, and Alan M. Zaslavsky. “Unmet Health Needs of Uninsured Adults in the United States,” The Journal of the American Medical Association 284, no. 16 (2000): 2061-2069.
Belluck, Pam. “Children’s Life Expectancy Being Cut Short by Obesity,” New York Times,
March 17, 2005.
Blumenthal, David. “Health Care Coverage under the Affordable Care Act—A Progress Report,” The New England Journal of Medicine 371 (2014) 275.
Bodenheimer, Thomas, Ellen Chen, Heather D. Bennett. “Confronting the Growing
Burden of Chronic Disease: Can the US Health Care Workforce Do the Job?” Health Affairs 28 (2009): 64–74.
Burge, Mark R., and David S. Schade. “Diabetes and Affordable Care Act,” Diabetes Technology & Therapeutics 16 (2014): 399-413.
The Centers for Medicare and Medicaid Services. Emergency Medical Treatment & Labor Act. https://www.cms.gov/Regulations-and-Guidance/Legislation/EMTALA/ Claxton, Gary, Matthew Rae, Nirmita Panchal, and Anthony Damico. 2014 Employer
Health Benefits Survey (Chicago, Illinois: The Henry J. Kaiser Family Foundation, 2014).
Coughlin, Teresa A., John Holahan, Kyle Caswell, and Megan McGrath. “Uncompensated Care for the Uninsured in 2013: A Detailed Examination,” (Washington, D.C., The Henry J. Kaiser Family Foundation, 2014) 1-34.
Crane, Thomas S., Lauren Moldawer, and Andy Shin. “Beyong SGR—MACRA Provides Additional Payment Provisions and Offsets,” Health Policy & Law Matters, April 21, 2015. http://www.healthlawpolicymatters.com/2015/04/21/beyond-sgr- macra-provides-additional-payment-provisions-and-offsets/
Davis, Karen. National Health Insurance: Benefits, Costs and Consequences (Washington, D.C.: Brookings Institution, 1975).
Davis, Karen. “Universal Coverage in the United States: Lessons from Experience of the
105

20th Century,” Journal of Urban Health 78, no. 1 (2001): 46-58.
Fox, Daniel M. Health Policies, Health Politics: the British and American Experience, 1911–1965 (Princeton, New Jersey: Princeton University Press, 1986).
Franks, Paul, Robert L. Hanson, William C. Knowler, Maurice L. Sievers, Peter H. Bennett, and Helen C. Looker. “Childhood Obesity, Other Cardiovascular Risk Factors, and Premature Death.” The New England Journal of Medicine 362 (2010): 485-493.
Goetzel, Ron Z. “Do prevention or treatment services save money? The Wrong Debate.”
Health Affairs 28, no. 1 (2009): 37-41. Garfield, Rachel, Rachel Licata, and Katherine Young. The Uninsured at the Starting Line:
Findings from the 2013 Kaiser Survey of Low-income Americans and the ACA (Menlo Park, CA: The Kaiser Family Foundation, 2014).
Gruber, Johnathan and James Poterba. “Tax Incentives and the Decision to Purchase
Health Insurance: Evidence from the Self-Employed.” The Quarterly Journal of Economics 109, no. 3 (1994): 701-703.
Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report.
(Washington, D.C. The Department of Health and Human Services, 2015).
Hoffman, Beatrix. “Health Care Reform and Social Movements in the United States,” American Journal of Public Health 93, no. 1 (2003): 75-85.
Key Facts about the Uninsured Population. (Washington, D.C.: The Kaiser Commission on Medicaid and the Uninsured, 2014) 1-9.
Manchikanti, Laxmaiah, David L. Caraway, Allan T. Parr, Bert Fellows, and Joshua A.
Hirsch. “Patient Protection and Affordable Care Act of 2010: Reforming the Health Care Reform for the New Decade.” Pain Physician 14, no. 1 (2011): E35- E67.
McAuliff, Michael. “House Passes 56th Anti-Obamacare Measure,” The Huffington Post,
February 3, 2015.
Medical Cost Trend: Behind the Numbers 2016. (Washington, D.C., PriceWaterhouseCoopers, 2015,) 3.
Narayan, K.M., James P. Boyle, Theodore J. Thompson, Stephen W. Sorenson, and David
F. Williamson. “Lifetime Risk for Diabetes Mellitus in the United States.” The Journal of the American Medical Association 290, no. 14 (2003): 1884-1890.
106
The National Bureau of Economic Research. Tax Breaks for Employer-Sponsored Health Insurance (Cambridge, MA: National Bureau of Economic Research, August 13, 2015).
National Health Expenditures 2013 Highlights. (Washington, D.C., The Centers for Medicare and Medicaid Services. 2013).
Oberlander, Jonathan. “Unfinished Journey—A Century of Health Care Reform in the United States,” New England Journal of Medicine 367 (2012) 585-590.
Organization for Economic Co-operation and Development. “Health at a Glance 2011
OECD Indicators.” http://www.oecd.org/els/health-systems/49105858.pdf Overview of the Uninsured in the United States: A Summary of the 2011 Current
Population Survey. (Washington, D.C., The Department of Health and Human Services, 2014).
Premium, Affordability, Competition, and Choice in the Health Insurance Marketplace, 2014. (Washington, D.C., The Department of Health and Human Services, 2014).
Rosenbaum, Sara. “The Patient Protection and Affordable Care Act: Implications for Public Health Policy and Practice,” Public Health Reports 126, no. 1 (2011): 130- 135.
Rising Health Care Costs. (Washington, D.C. America’s Health Insurance Plans, 2015).
Schoen, Cathy, Susan L. Hayes, Sara R. Collins, Jacob A. Lippa, and David C. Radley. America’s Underinsured: A State-by-State Look at Health Insurance Affordability Prior to the New Coverage Expansions, (Washington, D.C.: The Commonwealth Fund, 2014) 1-26.
Shaw, Frederic E., Chisara N Asomugha, Patrick H. Conway, Andrew S. Rein. “The Patient Protection and Affordable Care Act: Opportunities for Prevention and Public Health.” Lancet 384 (2014): 75-82.
Stevens, Rosemary. American Medicine and the Public Interest (Berkeley: University of California Press, 1971, rev. 1998).
Thorpe, Kenneth E., Curtis S. Florence, David H. Howard, and Peter Joski. “The Rising Prevalence of Treated Disease: Effects on Private Health Insurance Spending,” Health Affairs (2005), accessed June 27, 2015, doi: 10.1377/hlthaff.w5.317.
Truman, Harry S. Public Papers of the Presidents of the United States (Washington, D.C.: U.S. Government Printing Office, 1945).
107
The President’s Health Care Reform Proposal (Washington, D.C., Congressional Research
Service, 1992). Ung, Brian L. and C. Daniel Mullins. “The Affordable Care Act, Health Care Reform,
Prescription Drug Formularies and Utilization Management Tools,” Research in Social & Administrative Pharmacy 11(2015): 459-467.
Bibliography for Chapter Two
American’s Uninsured Crisis: Consequences for Health and Health Care. (Washington, D.C., National Academies Press, 2009) 61.
Anderson, John, Meghan Riley, and Tekisha Everette. “How Proven Primary Prevention
Can Stop Diabetes,” Clinical Diabetes 30, no. 2 (2012): 76-79. Ayanian, John Z., Joel S. Weissman, Eric C. Schneider, Jack A. Ginsburg, and Alan M.
Zaslavsky. “Unmet Health Needs of Uninsured Adults in the United States,” The Journal of the American Medical Association 284, no. 16 (2000): 2061-2069.
Bachrach, Deborah, Patricia Boozang, and Dori Glanz. “States Expanding Medicaid See Significant Budget Savings and Revenue Gains.” State Health Reform Assistance Network Issue Brief. April 2015.
Bodenheimer, Thomas, Ellen Chen, Heather D. Bennett. “Confronting the Growing
Burden of Chronic Disease: Can the US Health Care Workforce Do the Job?” Health Affairs 28 (2009): 64–74.
Burge, Mark R., and David S. Schade. “Diabetes and Affordable Care Act,” Diabetes Technology & Therapeutics 16 (2014): 399-413.
Coffield, Ashley B. and Michael Maciosek. Preventive Care: A National Profile on Use, Disparities, and Health Benefits. (Washington, D.C., The Robert Wood Johnson Foundation, 2007,) 1-41.
Diabetes Prevention Program Research Group. “The Diabetes Prevention Program
Description of Lifestyle Intervention,” Diabetes Care 25, no. 12 (2002): 2165. Diabetes Prevention Program Research Group. “Reduction in the Incidence of Type 2
Diabetes with Lifestyle Intervention or Metformin,” The New England Journal of Medicine 346, No. 6 (2002): 1.
Garfield, Rachel, Rachel Licata, and Katherine Young. The Uninsured at the Starting Line:
108

Findings from the 2013 Kaiser Survey of Low-income Americans and the ACA (Menlo Park, CA: The Kaiser Family Foundation, 2014).
Holahan, John, Matthew Buettgens, Caitlin Carroll, Stan Dorn. “National and State-by-
State Analysis,” (Washington, D.C., The Urban Institute, 2012). Health Insurance as a Family Matter. (Washington, D.C., Institute of Medicine, 2002)
Joyce, Geoffrey F., Julie Zissimopoulos, and Dana Goldman. “Digesting the Doughnut
Hole,” Journal of Health Economics 32, no. 6 (2013) 1345-1355.
Kaufman, Harvey W., Zhen Chen, Vivian A. Fonseca, and Michael J. McPhaul. “Surge in Newly Identified Diabetes Among Medicaid Patients in 2014 Within Medicaid Expansion States,” Diabetes Care 38 (2015) 833-837.
Mangan, Dana. “Higher Costs for Obamacare’s New Medicaid Patients,” CNBC, July 13,
2015. Medical Cost Trend: Behind the Numbers 2016. (Washington, D.C.,
PriceWaterhouseCoopers, 2015). Medicare Health Support Overview. (Washington, D.C., The Centers for Medicare and
Medicaid Services, 2015). National Diabetes Statistics Report 2014. (Atlanta, GA: Centers for Disease Control and
Prevention, 2014). Nearly Half of U.S. Adults Were Not Receiving Key Preventive Services Before 2010.
(Atlanta, GA, The Centers for Disease Control and Prevention, 2012).
Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey. (Washington, D.C., The Department of Health and Human Services, 2014).
Preventing Type 2 Diabetes. (Atlanta, GA, The Centers for Disease Control and Prevention, 2014) 3.
Paradise, Julia. “Medicaid Moving Forward,” (Washington, D.C., The Kaiser Commission on Medicaid and the Uninsured, 2015) 8.
Status of State Action on the Medical Expansion Decision. (Washington, D.C., The Henry J. Kaiser Family Foundation, 2015).
The Affordable Care Act—A Stronger Medicare Program in 2012. (Washington, D.C., The
109
Centers for Medicare & Medicaid Services. 2012)
The Centers for Disease Control and Prevention. “Building a Healthier Community,” fact sheet, October 29, 2014, http://www.cdc.gov/nccdphp/dch/programs/communitytransformation/.
The Centers for Medicare and Medicaid Services. “Medicaid & CHIP: June 2014 Monthly Applications, Eligibility Determinations and Enrollment Report,” press release, August 8, 2014. http://medicaid.gov/medicaid-chip-program-information/program-information/downloads/june-2014-enrollment-report.pdf
The U.S. Department of Health and Human Services, “Affordable Care Act Helps 76
Million Americans with Private Coverage Access Free Preventive Services,” press release, June 27, 2014, http://www.hhs.gov/news/press/2014pres/06/20140627b.html.
The U.S. Department of Health and Human Services. “Building Healthier Communities by
Investing in Prevention,” fact sheet, February 9, 2011, http://www.hhs.gov/healthcare/facts/factsheets/2011/09/prevention02092011.html.
The U.S. Department of Health and Human Services. “Increased Coverage of Preventive
Services with Zero Cost Sharing Under the Affordable Care Act,” issue brief, June 27, 2014.
The U.S. Department of Health and Humans Services. “At Risk: Pre-Existing Conditions
Could Affect 1 in 2 Americans: 129 Million People Could Be Denied Affordable Coverage without Health Reform,” November 2011, http://aspe.hhs.gov/health/ reports/2012/pre-existing/index.shtml.
The United States of Diabetes: Challenges and Opportunities in the Decade Ahead.
(Washington, D.C., UnitedHealth Center for Health Reform & Modernization, 2010,) 5.
Thorpe, Kenneth E. “The Affordable Care Act Lays The Groundwork For A National Diabetes Prevention and Treatment Strategy,” Health Affairs 31, no.1 (2012): 61-66.
Updated Estimates of the Insurance Coverage Provisions of the Affordable Care Act—The
Budget and Economic Outlook: 2014 to 2024. (Washington, D.C. Congressional Budget Office, 2014).
Yang, Wenya, Timothy Dall, Pragna Halder, Paul Gallo, Stacey Kowal, and Paul Hogan.
“Economic Costs of Diabetes in the U.S. in 2012,” Diabetes Care, 35 (2013): 1033-
110
1046.
Bibliography for Chapter Three Accountable Care Organization 2014 Program Analysis Quality Performance Standards
Narrative Measure Specifications. (Baltimore, Maryland, The Centers for Medicare and Medicaid Services, 2014).
Altschuler, Justin, David Margolius, Thomas Bodenheimer, and Kevin Grumback.
"Estimating a Reasonable Patient Panel Size for Primary Care Physicians with Team-Based Task Delegation." The Annals of Family Medicine (2012): 396-400.
Bodenheimer, Thomas, Ellen Chen, Heather D. Bennett. “Confronting the Growing
Burden of Chronic Disease: Can the US Health Care Workforce Do the Job?” Health Affairs 28 (2009): 64–74.
Burton, Rachel. “Improving Care Transitions,” Health Affairs Policy Brief, last modified September 13, 2012, http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_76.pdf.
Caffrey, Mary K. “Among ACO Pioneers, Data Reveal Diabetes Performance Paradox,” American Journal of Managed Care, published online December 4, 2014.
Ciervo, Carman A. Ciervo, Jay H. Shubrook, and Paul Grundy. “Leveraging the Principles
of Osteopathic Medicine to Improve Diabetes Outcomes Within a New Era of Health Care Reform,” The Journal of the American Osteopathic Association 115, no. 4 (2015) eS8-eS19.
Ciervo, Carmen A., Jay H. Shubrook, and Paul Grundy. “Diabetes Management Within Evolving Healthcare Delivery Models: The Osteopathic Perspective,” The Journal of the American Osteopathic Association 115, no. 4 (2015) eS5-eS7.
Davis, Karen, Melinda Abrams, and Kristof Stremikis. “How the Affordable Care Act Will Strengthen the Nation’s Primary Care Foundation,” Journal of General Internal Medicine 26, no. 10 (2011): 1201-1203.
Force, Ashley. “Pioneer Accountable Care Organizations Report Successful Results,” Dorland Health, 2015, http://www.dorlandhealth.com/dorland-health-articles/Pioneer-Accountable-Care-Organizations-Report-Successful-Results.
Godsen, Toby, Frode Forland, Ivar Kristiansen, Matthew Sutton, Brenda Leese, Antonio Giuffrida, Michelle Sergison, Lone Penderson. "Capitation, Salary, Fee-for-service and Mixed systems of Payment: Effects on the Behaviour of Primary Care Physicians," The Cochrane Library 3(2000), doi: 10.1002/14651858.CD002215.
111
Gold. Jenny. “FAQ on ACOs: Accountable Care Organizations, Explained,” Kaiser Health
News, last modified April 16, 2014, http://kaiserhealthnews.org/news/aco- accountable-care-organization-faq/.
Jencks, Stephen F., Mark V. Williams, and Eric A. Coleman. “Rehospitalizations among Patients in the Medicare Fee-for-Service Program,” The New England Journal of Medicine 360 (2009) 1418-1428.
Medical Cost Trend: Behind the Numbers 2016. (Washington, D.C., PriceWaterhouseCoopers, 2015).
Menachemi, Nir and Robert G. Brooks. "Reviewing the Benefits and Costs of Electronic Health Records and Associated Patient Safety Technologies." Journal of Medical Systems: 159-168.
Mostashari, Farzad and Ross White. “The ACO Hypothesis: What We Are Learning,” The
Healthcare Blog, March 12, 2014, http://thehealthcareblog.com/blog/2014/03/12/the-aco-hypothesis-what-were-learning/.
National Diabetes Statistics Report 2014. (Atlanta, GA: Centers for Disease Control and
Prevention, 2014).
Pfuntner, Anne, Lauren M. Wier, and Claudia Steiner. “Costs for Hospital Stays in the United States, 2010,” Agency for Healthcare Research and Quality, last modified January 2013, http://www.hcup-us.ahrq.gov/reports/statbriefs/sb146.pdf.
“Pioneer ACO Model Frequently Asked Questions,” (Washington, D.C., The Centers for Medicare and Medicaid Services, 2015).
Rau, Jordan. “Medicare Data Show Wide Differences in ACOs’ Patient Care. Kaiser
Health News, last updated February 27, 2014, http://khn.org/news/medicare- data-shows-wide-differences-in-acos-patient-care/.
Reid, Robert J., Katie Coleman, Eric A. Johnson, Paul A. Fishman, Clarissa Hsu, Michael P. Soman, Claire E. Trescott, Michael Erikson, and Eric B. Larson. “The Group Health Medical Home At Year Two: Cost Savings, Higher Patient Satisfaction, and Less Burnout for Providers,” Health Affairs 29, no. 5 (2010) 835-843.
Rittenhouse, Diane R., Stephen Shortell, and Elliot Fisher. “Primary Care and
Accountable Care—Two Essential Elements of Delivery-System Reform,” The New England Journal of Medicine 361 (2009) 2301-2303.
112
”Rising Health Costs,” American’s Health Insurance Plans, accessed June 20, 2015. https://www.ahip.org/Issues/Rising-Health-Care-Costs.aspx.
Schoen, Cathy. “The Path to a High Performance U.S. Health System: A 2020 Vision and the Policies to Pave the Way,” (New York, NY, The Commonwealth Fund Commission on a High Performance Health System, 2009).
Shin, Andrew J., Stephen M. Weiner, and Stephanie D. Willis. “CMS Releases MSSP and Pioneer ACO Data on Shared Savings and Loses—Where Do We Go From Here?,” Health Law and Policy Matters, last modified September 23, 2014, http://www.healthlawpolicymatters.com/2014/09/23/cms-releases-mssp-and- pioneer-aco-data-on-shared-savings-losses-where-do-we-go-from-here/.
Shortell, Stephen M., Lawrence P. Cassalino, and Elliott S. Fisher. “How The Center for
Medicare and Medicaid Innovation Should Test Accountable Care Organizations,” Health Affairs 29, no. 7 (2010): 1293-1298.
“A Survey of America’s Physicians: Practice Patterns and Perspectives,” (Washington, D.C., The Physician Foundation, 2012) 1-127.
The Centers for Medicare and Medicaid Services, “Pioneer Accountable Care Organizations Succeed in Improving Care, Lowering Costs,” press release, July 16, 2013.
The U.S. Department of Health and Human Services. Assistant Secretary for Planning and Evaluation Issue Brief. Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey. Washington, DC, 2014, http://aspe.hhs.gov/health/reports/2011/cpshealthins2011/ib.pdf.
The U.S. Department of Health and Human Services. “Affordable Care Act Payment
Model Saves More than $384 Million in Two Years, Meets Criteria for First-ever Expansion,” press release, May 4, 2015, http://www.hhs.gov/news/press/2015pres/05/20150504a.html.
Thorpe, Kenneth E. “The Affordable Care Act Lays The Groundwork For A National
Diabetes Prevention and Treatment Strategy,” Health Affairs 31, no.1 (2012): 61-66.
Ung, Brian L. and C. Daniel Mullins. “The Affordable Care Act, Health Care Reform,
Prescription Drug Formularies and Utilization Management Tools,” Research in Social & Administrative Pharmacy 11(2015): 459-467.
Zuvekas, Samuel H. and Joel W. Cohen. “Paying Physicians by Capitation: Is the Past Now Prologue?,” Health Affairs 29, no. 9 (2010): 1661-1666.
113
Bibliography for Conclusion Blumenthal, David, and Sara Collins. “Health Care Coverage under the Affordable Care
Act—A Progress Report,” The New England Journal of Medicine 371(2014):275-281.
Overview of the Uninsured in the United States: A Summary of the 2011 Current
Population Survey. (Washington, D.C., The Department of Health and Human Services, 2014).
Schoen, Cathy, Susan L. Hayes, Sara R. Collins, Jacob A. Lippa, and David C. Radley.
America’s Underinsured: A State-by-State Look at Health Insurance Affordability Prior to the New Coverage Expansions, (Washington, D.C.: The Commonwealth Fund, 2014) 1-26.
Shaw, Frederic E., Chisara N. Asomugha, Patrick H. Conway, and Andrew S. Rein. “The Patient Protection and Affordable Care Act: Opportunities for Prevention and Public Health,” The Lancet 384, no. 14 (2014): 75-82.
Ung, Brian L. and C. Daniel Mullins. “The Affordable Care Act, Health Care Reform, Prescription Drug Formularies and Utilization Management Tools,” Research in Social & Administrative Pharmacy 11(2015): 459-467.
114

Curriculum Vitae
Meredith Dyer is the Associate Director of Health Policy at the Endocrine Society where
she analyzes legislative and regulatory policies related to diabetes, obesity, and
Medicare coverage. In this capacity, Dyer serves as an advocate on Capitol Hill and with
federal agencies to improve health care quality and to educate members of Congress on
programs and services needed to address the growing epidemic of diabetes and obesity
in America. Prior to joining the Society, Dyer was a behavioral health lobbyist during
healthcare reform and served as the co-chair of the Mental Health Liaison Group’s Social
Services Committee. Meredith’s advocacy experience includes work with The Clinton
Group, The National Foundation for Women's Legislators, The National Association for
Behavioral Health, The American Association of Political Consultants, M&R Strategic
Services, and the Democratic Congressional Campaign Committee.
115


![On the conjecture of Birch and Swinnerton-Dyer for Abelian ... · Birch-Swinnerton-Dyer and the Artin-Tate conjecture for the base a curve, see Gordon’s PhD thesis [Gor79]. Let](https://img.pdfslide.net/doc/110x75/5f05f0fd7e708231d4157de5/on-the-conjecture-of-birch-and-swinnerton-dyer-for-abelian-birch-swinnerton-dyer.jpg)