Embed Size (px)
Citation preview

Dysregulation of calcium homeostasis
in muscular dystrophies
Ainara Vallejo-Illarramendi1,2,3,*, Ivan Toral-Ojeda1,2,Garazi Aldanondo1 and Adolfo López de Munain1,2,4,5
Muscular dystrophies are a group of diseases characterised by the primarywasting of skeletal muscle, which compromises patient mobility and in themost severe cases originate a complete paralysis and premature death.Existing evidence implicates calcium dysregulation as an underlying crucialevent in the pathophysiology of several muscular dystrophies, such asdystrophinopathies, calpainopathies or myotonic dystrophy among others.Duchenne muscular dystrophy is the most frequent myopathy in childhood,and calpainopathy or LGMD2A is the most common form of limb-girdlemuscular dystrophy, whereas myotonic dystrophy is the most frequentinherited muscle disease worldwide. In this review, we summarise recentadvances in our understanding of calcium ion cycling through the sarcolemma,the sarcoplasmic reticulum and mitochondria, and its involvement in thepathogenesis of these dystrophies. We also discuss some of the clinicalimplications of recent findings regarding Ca2+ handling as well as novelapproaches to treat muscular dystrophies targeting Ca2+ regulatory proteins.
IntroductionCa2+ ions are involved in the regulation of avariety of cellular processes such as musclecontraction, secretion, proliferation or cell death(Ref. 1). Therefore, there is a need of precisetemporal and spatial control of Ca2+ fluxesand Ca2+ concentration within the cell. Indeed,Ca2+ concentration is tightly controlled in alleukaryotic cells by complex interactions among
voltage sensors, Ca2+ transporters, Ca2+ channels,Ca2+ exchangers, Ca2+-binding proteins, ionpumps and ion exchangers (Refs. 2, 3, 4). Thisfine regulation of Ca2+ homeostasis allows thision to act as one of the most important secondmessengers in signal transduction.
In skeletal muscle fibres, the status ofthe excitation–contraction–relaxation cycle isdetermined by the cytosolic Ca2+ levels: high
1Neuroscience Area, Biodonostia Institute, San Sebastian, Spain2Centro de Investigación Biomédica en Red para Enfermedades Neurodegenerativas (CIBERNED),Instituto de Salud Carlos III, San Sebastian, Spain3Euskampus, University of the Basque Country (UPV-EHU), San Sebastian, Spain4Department of Neuroscience, University of the Basque Country (UPV-EHU), San Sebastian, Spain5Department of Neurology, Donostia Hospital, San Sebastian, Spain
*Corresponding author: Ainara Vallejo-Illarramendi, Instituto Biodonostia, Po Dr Begiristain s/n,20014 San Sebastian, Spain. E-mail: [email protected]
expert reviewshttp://www.expertreviews.org/ in molecular medicine
1Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

Ca2+ levels are crucial for triggering musclecontraction, while low levels are critical forinitiating muscle relaxation. Hence, a fastCa2+-cycling mechanism and an efficient storageprocess are absolutely essential in muscle fibres.During normal contractions, local cytosolic Ca2+
concentration is greatly increased reaching up to20 μM (Refs. 5, 6). In addition to these Ca2+
transients associated with muscle contraction,smaller but prolonged increases in intracellularCa2+ levels associated with long-duration fatiguehave been described (Ref. 7). Additionally, smallbut persistent increases in basal intracellular Ca2+
concentration likely occur during certain musclediseases and in ageing (Ref. 8). Since changes incytosolic Ca2+ levels are particularly frequentand diverse in the skeletal muscle, a tight controlin Ca2+ homeostasis is most significant in thissystem. In this regard, small changes in the Ca2+
handling apparatus in the skeletal muscle mightresult in major pathophysiological consequences.Indeed, abnormal expression patterns of ion-regulatory proteins have been reported repeatedlyin muscular dystrophy (Refs. 9, 10, 11, 12, 13).Existing evidence implicates Ca2+ dysregulation
as a common underlying event in thepathophysiology of muscular dystrophies, agroup of diseases characterised by a primarydegeneration of skeletal muscle tissue that resultsin progressive muscle weakness. This reviewexamines Ca2+ handling in muscular dystrophies,with a special focus on dystrophinopathies,calpainopathies and myotonic musculardystrophies. We also summarise recent advancesin our understanding of Ca2+ ion cycling throughthe sarcolemma, the sarcoplasmic reticulum (SR)and mitochondria, and its involvement in thepathogenesis of these dystrophies. Finally, wediscuss some of the clinical implications of thesefindings, and in particular, novel pharmacologicaltherapeutic approaches for muscular dystrophiesthat target Ca2+ regulatory proteins.
Calcium handling in the skeletal muscleStructure and physiology of the skeletalmuscleThe skeletal muscle is under the control of thesomatic nervous system through innervation ofmuscle fibres by motoneurons. Muscle fibres arelong, cylindrical multinucleated cells thatoriginate from the fusion of myoblasts duringembryonic development and behave as a singleunit. Each fibre contains several bundles of
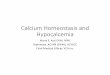
myofibrils, with inter-digitating myosin (thick)and actin (thin) filaments arranged longitudinallyin repeating units known as sarcomeres. Thisparticular arrangement of the cytoskeletalelements accounts for the banding pattern,characteristic of skeletal fibres. Actin filaments arebound to the Z line, which forms the borders ofthe sarcomere. At this location, deepinvaginations of the sarcolemma (T-tubules)permit the conduction of the electrical impulses tothe cell interior (Fig. 1).
A single motoneuron innervating one or moremuscle fibres with similar functional propertiesconstitutes a motor unit. A muscle is formed bymany motor units, each one bringing its ownspecific contribution (Ref. 14). Motor units differin the size of motoneurons and also in the typeof innervated muscle fibres. They are dividedinto three categories: (a) slow; (b) fast fatigable;and (c) fast fatigue-resistant motor units (Ref. 15).
(a) Slow motor units: Constituted by type I, slowtwitch muscle fibres, are essential forsustained muscular contraction. Type I fibrescontract very slowly and generate smallforce, but they are very resistant to fatigue.They contain high mitochondria density andthey generate ATP by the aerobic metabolism.
(b) Fast fatigable motor units: Constituted by typeIIB fibres, or type IIX in humans, are usedfor tasks that require large brief bursts ofenergy such as sprinting. Type IIB/IIX orfast glycolytic fibres have a fast contractionvelocity but they fatigue easily. They containfew mitochondria and they generate ATPmainly by the anaerobic system.
(c) Fast fatigue-resistant motor units:Constituted bytype IIA, fast twitch A fibres or fast oxidativefibres, which contain many mitochondria and,thus, can generate ATP by aerobicmetabolism.They have a fast contraction velocity and theyare resistant to fatigue, although not as muchas type I fibres (Ref. 16).
Some of the fibre-type differences in twitchkinetics are also likely due to differences in Ca2+
handling. Indeed, the amount of Ca2+ releasedin type II fibres is up to fourfold larger than intype I fibres, there is a faster decline of thecalcium transient in type II fibres (Ref. 14) andthe proportion of Ca2+ that binds troponin toactivate contraction is substantially smaller(Ref. 5). On the other hand, type I fibres showincreased affinity for SR Ca2+ uptake, higher
expert reviewshttp://www.expertreviews.org/ in molecular medicine
2Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

relative levels of SRCa2+ loading and increased SRCa2+ leakage compared with type II fibres (Refs.17, 18). Muscle fibres display a high plasticity,being able to adapt to changing demands bymodifying size or fibre-type composition(Ref. 19). Specific types of muscle fibres arepreferentially affected in different forms ofmuscular dystrophies. In Duchenne musculardystrophy, for example, type IIB fibres areprogressively replaced by type I and IIA fibres(Ref. 20). Recently, we have also found incollaboration with Dr Spencer’s group that slow
fibres are preferentially involved in Limb-girdle muscular dystrophy-type 2A (LGMD2A)dystrophic patients (Ref. 21). Interestingly, somevery specific muscle types present in extraocular muscles show great resistance to damagein Duchenne muscular dystrophy, partially dueto an enhanced Ca2+ buffering (Ref. 22).
The Ca2+ cycle duringexcitation–contraction (E–C)Skeletal muscle contraction is initiated bydepolarisation of the sarcolemma in response to
Sarcolemma
Mitochondrion
SR
NCLX
ATP
ATP
PTP
Sarcomere
Glycolysis
SERCA
Ca2+Ca2+
Ca2+
Ca2+
Calstabin
Ca2+
MCU
NCX
Ca2+
Na+
Na+
Ca2+DHPR
PMCA
Ca2+CSQ
T-tu
bul
e
RYR1
RYR1
STIM1SR
TRPC
TRPC
Orai1
Relaxation
Contraction
Representation of calcium signalling dynamics in the muscle fibreExpert Reviews in Molecular Medicine © 2014 Cambridge University Press
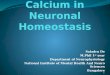
Figure 1. Representation of calcium signalling dynamics in the muscle fibre. Signalling begins whensarcolemmal depolarisation reaches the T-tubules. In these structures, DHPR respond with a conformationalchange that activates closely apposed RyR1, resulting in Ca2+ release from the sarcoplasmic reticulum(SR). Ca2+ diffuses out to activate contraction by binding with Troponin C. Relaxation occurs as Ca2+ isreturned into the SR by SERCA ATPase or is pumped out of the cell by NCX or PMCA. A portion of thisCa2+ reaches the mitochondria and driven by the negative membrane potential, it enters through MCU andLETM1 importers, where it stimulates the metabolism to provide the ATP required for maintainingcontraction. Ca2+ can be released from mitochondria through NCLX exchanger and the mitochondrial PTP.Low SR Ca2+ levels are detected by STIM1 and activate SOCE, an extracellular Ca2+ influx through Orai1or TRPC channels to refill intracellular Ca2+ stores.
expert reviewshttp://www.expertreviews.org/ in molecular medicine
3Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

acetylcholine release from motoneurons. Thesarcolemmal depolarisation propagates down theT-tubular system and activates dihydropyridinereceptors (DHPRs) (Refs. 5, 23). The resultingconformational change of DHPRs activatesclosely apposed ryanodine receptors (RyRs),which are Ca2+ release channels localised in theSR membranes (Ref. 24). As these releasechannels open, Ca2+ moves from the SR into thecytosol, driven by a steep Ca2+ concentrationgradient. Afterwards, Ca2+ diffuses throughoutthe sarcomere and binds to various cytosolicconstituents or Ca2+ buffers. Binding of Ca2+ totroponin triggers the contractile response of themyofibrils: Ca2+-bound troponin undergoes aconformational change that leads to themovement of tropomyosin, which unmasksmyosin-binding sites on actin filaments andallows myosin and actin ATP-dependent cross-bridge cycling and shortening of the muscle.Lastly, relaxation is initiated by Ca2+ diffusionfrom the myofilaments to the cytosol and Ca2+
transfer back to the SR by the sarco/endoplasmicreticulum Ca2+ pump SERCA (Ref. 25). Thesarcolemmal Na+/Ca2+-exchanger (NCX) andthe plasmalemmal Ca2+-ATPase (PMCA) areother mechanisms involved in relaxation, sincethey remove cytosolic Ca2+ to the extracellularspace (Ref. 26). Figure 1 illustrates the majorintracellular movements of Ca2+ taking placeduring E–C coupling in skeletal muscle fibres.
Cytosolic Ca2+ buffersCytosolic Ca2+ buffering is the rapid binding ofcytosolic incoming Ca2+ ions to different cellularbinding sites, and constitutes a critical processimplicated in the precise regulation of Ca2+
signalling and homeostasis. Ca2+ buffers arecytosolic Ca2+-binding proteins that modulateintracellular Ca2+ transients by controllingdiffusion of free Ca2+ ions within the cytosol. Thisprocess occurs at the sub-second scale, much fasterthan Ca2+ sequestration into intracellular stores.Concentration of Ca2+ buffers and otherparameters, such as mobility and Ca2+-bindingaffinity, are important for determining theirspecific role in modulation of Ca2+ signalling(Ref. 27).In skeletal muscle fibres, the most significant
Ca2+ buffers in order of binding occurrence intime are, first, troponin C is a component of thinfilaments that allows interaction of actin andmyosin and initiates contractile activation when
its regulatory sites are bound to Ca2+. Differenttypes of muscle fibres have specific versions oftroponin C with different Ca2+-binding capacities.Second, ATP acts as a cytosolic mobile buffer forCa2+ and Mg2+ (Ref. 5). Then parvalbumin playsan important role in regulating the speed ofrelaxation in mice (Ref. 28), although it isexpressed at very low concentrations in humanskeletal muscle (Ref. 29). Afterwards, Ca2+ bindsto calmodulin, contributing to the regulation ofcontractile function via myosin light-chain kinase.It is also conducive to the activation of Ca2+-dependent signalling pathways involved inmuscle gene regulation. Lastly, Ca2+ binds toSERCA pumps for Ca2+ sequestration into the SR.
Contribution of sarcolemma to Ca2+
homeostasisIn skeletal muscle, Ca2+ entry through thesarcolemma has been shown to play animportant role in store repletion (Ref. 30),limiting fatigue under conditions of extensiveexercise (Ref. 31), activation of NFATtranscription factor signalling (Refs. 32, 33) andmuscle differentiation (Ref. 34). The sarcolemmahas a very low permeability to Ca2+ and a veryparticular organisation with the majority of thesarcolemma internalised as the tubular system,which allows for tightly regulated Ca2+ trans-sarcolemmal fluxes. Aside from voltage-gatedchannels, Ca2+ may enter the muscle fibre viaSOCE or store-operated Ca2+ entry (Ref. 30);ECCE, or excitation-coupled Ca2+ entry (Ref. 35);SAC or stretch-activated cation channels (Ref. 36);SIC or stretch-inhibitable cation channels (Ref. 37);and leak channels (Ref. 38). Previous studies haveshown that dysregulation of Ca2+ entry may leadto severe muscle pathologies. In particular, severalgenetic mouse models of muscular dystrophypoint towards an enhanced Ca2+ influx throughSOCE or SAC that leads to Ca2+-dependentapoptosis and muscle degeneration (Refs. 39, 40).On the other hand, Ca2+ extrusion from cells mayalso play an important role in maintaining Ca2+
homeostasis. In muscle fibres, Ca2+ is pumpedout of the cell by the Na+/Ca2+ exchangersNCX1-3 and the Ca2+-ATPase PMCA isoforms 1,3 and 4, localised at the sarcolemma (Ref. 14).
Ca2+-handling proteins in the sarcoplasmicreticulumThe SR, the major reservoir of intracellular Ca2+ inthe muscle fibre, is a highly specialised form of
expert reviewshttp://www.expertreviews.org/ in molecular medicine
4Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

endoplasmic reticulum. It is organised as anextensive tubular network surrounding myofibrilswith periodical dilated end sacs or terminalcisternae. A central T-tubule flanked on both sidesby two terminal cisternae from the SR constitutes atriad, a highly specialised anatomical structure thatis the basis of E–C coupling (Ref. 41). In the SR, thebalance between Ca2+ storage, release andreuptake is achieved through the coordinatedaction of three major types of Ca2+-handlingproteins: luminal Ca2+-binding proteins, SR Ca2+
release channels and Ca2+-ATPase pumps for Ca2+
reuptake (Ref. 42). Ca2+-handling proteins areheterogeneously distributed within the SR, whichresults in functionally distinct subdomains whereCa2+ release and reuptake occur in the terminalcisternae and the longitudinal SR, respectively.
(a) Luminal Ca2+-binding proteins: Within the SRlumen, a large proportion of Ca2+ is boundto Ca2+-binding proteins that perform a dualfunction as Ca2+ reservoir components andas endogenous regulators of Ca2+ fluxes.Luminal Ca2+-binding proteins help toreduce the concentration of free Ca2+ withinthe SR, which assists in the reuptake of Ca2+
to the SR. They determine normal andmaximal Ca2+ levels in the SR, incombination with SERCA pump (Ref. 43).Intraluminal Ca2+ levels have been reportedto range between high micromolar and lowmilimolar concentrations, thus, constitutinga steep electrochemical gradient aimed at thecytosol. The most significant Ca2+-bindingproteins in the SR are: calsequestrin (CSQ),which is a moderate-affinity, high-capacityCa2+-binding proteins located in the terminalcisternae region; histidine-rich Ca2+-bindingprotein (HRC), which has been found to bindSERCA and triadin, and therefore, might beinvolved in the regulation of Ca2+ release byRyRs and sequestration (Refs. 44, 45);sarcalumenin, a Ca2+-binding/shuttle proteinlocalised in the longitudinal SR; andcalreticulin. In particular, CSQ is involved inthe SR Ca2+-loading capacity (Ref. 43), whilealso modulating activity of RyR channels(Ref. 46). In the skeletal muscle, CSQ1 is themain isoform, although CSQ2 is alsoexpressed in type I fibres. In fact, CSQ1 hasbeen found to both inhibit and activate RyR1depending on its binding manner to RyR1(Ref. 47). Recent work supports an essential
role of CSQ1 in the mechanism of RyR1channel closure and termination of SR Ca2+
release in mouse skeletal muscle (Ref. 48).
(b) SR Ca2+ release channels: Activation of thesechannels results in Ca2+ release from SR,which contributes to elevation of cytosolicCa2+ levels, whereas Ca2+ sequestration toSR assists termination of Ca2+ signals in thecytosol. RyRs, the largest known ion channels,are responsible for Ca2+ release from thesarco/endoplasmic reticulum and they alsoplay a central role in the regulation ofcytosolic and SR luminal Ca2+ levels. At leastthree isoforms are expressed in mammals,RyR1-3, being RyR1 the predominant isoformexpressed in the skeletal muscle. RyR2 andRyR3 are expressed in cardiac and immatureskeletal muscle, respectively (Refs. 49, 50, 51,52). RyR1 is essential for the E–C coupling inthe skeletal muscle and its gating is strictlycontrolled by DHPR activation. In fact, Ca2+
release through RyR1 is the key determinantof muscle force since skeletal musclecontraction depends on Ca2+ released fromthe SR (Ref. 7). Cytosolic Ca2+ activates RyR1in the low micromolar, but acts as an inhibitorin the low milimolar range. In addition,luminal Ca2+ levels are also able to modulateRyR1 activity, since previous reports showthat high luminal Ca2+ levels enhance RyR1responsiveness to cytosolic agonist (Ref. 49).
Ca2+ release through RyR1 is alsomodulatedby post-translational modifications and a vastvariety of proteins and small molecules, bothin the SR lumen and cytosol. In addition toCa2+ and DHPR channels, other positiveregulators of RyR1 activity in the cytosol areATP, CaMKII and PKA. Calstabin-1 stabilisesthe closed stage of the channel andcalmodulin has a biphasic effect on RyR1,functioning as an activator at the low cytosolicCa2+ levels and as and inhibitor at the highcytosolic Ca2+ levels. On the luminal side,RyR1 interacts with the CSQ–junctin–triadincomplex, which plays a dual role as luminalCa2+ sensor and RyR activity modulator.
RyRs can be phosphorylated by severalkinases, including CaMKII and PKA. A recentstudy has implicated PKA phosphorylation ofRyR1 in skeletal muscle enhancement ofcontractile force (Ref. 53). However, PKAhyper-phosphorylation of RyR1 might lead to
expert reviewshttp://www.expertreviews.org/ in molecular medicine
5Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

SR Ca2+ leak under prolonged pathologicalstress (Refs. 54, 55). Finally, RyR1 activity canalso be modulated by oxidative stress throughmodifications of cysteine thiol residues, suchas S-nitrosylation and S-glutathionylation.Although the effect of RyR1 oxidativemodifications may vary depending on whichresidue is modified, exposure of skeletalmuscle to nitric oxide has been reported toincrease RyR1 activity (Refs. 49, 51).Interestingly, RyRs have been found to releaseCa2+ spontaneously under conditions ofluminal Ca2+ overload in a process known asSOICR or Store Overload-Induced Ca2+
Release (Refs. 56, 57). This mechanism hasbeen recently linked to cardiac and musculardisorders, such as malignant hyperthermia orcatecholaminergic polymorphic ventriculartachycardia (Ref. 58).
The other major SR Ca2+ release channels arethe inositol 1,4,5-triphosphate receptors (IP3Rs).These Ca2+ channels are gated by the combinedbinding of IP3 and Ca2+, which initiates a slowwave of internal store Ca2+ release that oftenoccurs at specific subcellular locations(Ref. 59). Whereas in myoblasts IP3Rs have amajor role regulating Ca2+ homeostasis duringskeletal muscle development, the roles thatIP3Rs may play in adult skeletal muscle arecontroversial. A recent study has not foundany evidence of IP3R affecting global Ca2+
levels in adult mouse skeletal muscle (Ref. 60).Conversely, a previous work supports a role ofIP3Rs mainly at the neuromuscular junction(Ref. 61), and recent evidence indicates thatcrosstalk between IP3R1 and RyR1 underliesactivation of stress-induced Ca2+ sparks inadult mice skeletal muscle (Ref. 62).
(c) Ca2+-ATPase pumps: Ca2+ reuptake into the SRafter contraction relies on the Ca2+ ATPasepump SERCA, which actively transportsCa2+ from the cytosol to the SR against alarge concentration gradient at the expenseof ATP hydrolysis. Three genes localised ondifferent chromosomes encode for SERCA1,2 and 3 proteins, although isoform diversityis further increased by alternative splicing.Skeletal fast muscle fibres express SERCA1aexclusively, while SERCA2a is expressed inslow fibres and cardiac muscle. Duringdevelopment or regeneration, muscle fibresexpress the neonatal isoform SERCA1b (Refs.
23, 25). SERCA pumps are highly affected bychanges in cell energetics and ATP supply,since they are, together with myosinATPases, major ATP consumers (Ref. 63).SERCA pumps are also a substantialpathway for SR Ca2+ leakage and thisleakage is increased by high cytosolic ADPlevels (Ref. 64). Low levels of freeintraluminal Ca2+ are, thus, necessary sothat Ca2+ leakage does not metabolicallycompromise muscle function (Ref. 43).In addition to ATP, SERCA activity is
modulated by several cytosolic and luminalproteins, and also by post-translationalmodifications. The endogenous inhibitoryproteins phospholamban and sarcolipinmodulate SERCA activity in slow and fast-twitch fibres, respectively (Ref. 65).Phosphorylation by PKA or CaMKII, results inSERCA activation by dissociation ofphospholamban and sarcolipin from the Ca2+
pump. N-glycosylation and other post-translational modifications such asglutathiolation have been found to affectSERCA activity in different ways: SERCAactivity can be reversibly increased byoxidative modifications under normal or mildoxidative stress levels, but high oxidant levelspresent in some pathological conditions mayfurther lead to irreversible SERCAinactivation and degradation (Refs. 66, 67).This particularly susceptibility of SERCA tooxidative and nitrative modifications has ledto the hypothesis of SERCA functioning as asensor of cellular stress (Ref. 68). Moreover,these data suggest a central role of SERCA inenergy production and consumption throughregulation of Ca2+ homeostasis.
Ca2+ in mitochondriaMitochondria are located in close proximity to theSR in the skeletal muscle, and they account forabout 15% of the cytosolic volume in oxidativefibres (Refs. 69, 70). There is a significant interplaybetween the mitochondria and the SR, throughthe mitochondria-associated SR membrane(MAM), which is a structural element essential forcell physiology and Ca2+ homeostasis (Refs. 71,72). Besides playing a central role in musclebioenergetics, mitochondria are also able to storeCa2+ transiently and therefore, they contributesignificantly to Ca2+ homeostasis in the musclefibre. In fact, their ability to rapidly uptake Ca2+
expert reviewshttp://www.expertreviews.org/ in molecular medicine
6Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

for later release in response to different stimulimakes them very good cytosolic Ca2+ buffers(Ref. 73). Ca2+ fluxes between mitochondria andSR are believed to help shape mitochondrialmetabolism and ATP synthesis to thephysiological demands of skeletal fibres (Ref. 74).At the same time, mitochondria have been foundto modulate intracellular Ca2+ transients inskeletal muscle during E–C coupling (Ref. 75).The outer mitochondrial membrane is permeableto Ca2+, unlike the inner mitochondrialmembrane. Influx into the mitochondrial matrix isdriven by the negative membrane potential andoccurs through two types of importers: the low-affinity mitochondrial Ca2+ uniporter (MCU)(Ref. 76) and a high-affinity mitochondrial Ca2+/H+ exchanger, LETM1. In skeletal muscle fibres,Ca2+ release from mitochondria can occur via aNa+/Ca2+ exchange protein (NCLX) or via Ca2+-induced–Ca2+-release pathways (Ref. 76). Also, athigh matrix Ca2+ levels mitochondria releaseCa2+ through the permeability transition pore(PTP), a mechanism that can lead to cell deathand might have an important role in musculardystrophies (Refs. 77, 78). Interestingly, inhumans, mutations in the mitochondrial calciumuptake 1, a regulator of MCU, causesdysfunctional Ca2+ uptake and results in clinicaland pathological features that overlap with thoseof mitochondrial myopathies, congenital coremyopathies and muscular dystrophies (Ref. 79).
Calcium dysregulation in musculardystrophies
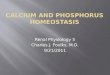
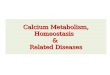
In this section, we will discuss current knowledgeregarding Ca2+ homeostasis in dystrophinopathies,calpainopathies and myotonic musculardystrophies. The main Ca2+-related pathwaysalteredinthesepathologiesaresummarisedinTable1.
DystrophinopathiesDuchenne muscular dystrophy (DMD) is aninherited X-linked neuromuscular disease thataffects 1 in 3500 male births and it is characterisedby severe and progressive skeletal muscledegeneration, weakness and premature deathcaused by respiratory failure and cardiacdysfunction (Ref. 80). DMD results from deficiencyin the structural protein dystrophin (Ref. 81), a427 kDa protein located beneath the sarcolemmawhose major role is to protect and maintainmuscle fibre integrity by linking intracellularcytoskeletal actin to the extracellular matrix. This
is achieved through its association to a group ofplasma membrane glycoproteins known as thedystrophin–glycoprotein complex (DGC) (Ref. 82).Dystrophin is essential for sarcolemmal stability,and thus dystrophin-deficient muscle fibres areprone to endure recurrent membrane damage(Ref. 83). This sarcolemma fragility, however, doesnot fully explain the onset and progression ofDMD and, up to date, the exact cause of musclefibre death still remains unsolved. Thepathological events most widely accepted to occurin DMD muscle fibres as a result of dystrophindeficiency include membrane fragility andincreased basal intracellular Ca2+ levels, whichleads to calpain activation, protein degradation,mitochondrial PTP opening and, ultimately, fibredeath by necrosis (Refs. 9, 11, 13, 84, 85, 86).Studies performed more than 30 years ago inmuscle biopsies (Ref. 85) and later on, in humanfoetuses and premature infants (Ref. 87), showedincreased Ca2+ accumulation in prenecrotic DMDfibres, which suggests that Ca2+ dysregulation isan early event in the pathophysiology of thisdisorder. Afterwards, many other studies havedemonstrated increased intracellular Ca2+ levelsin dystrophic muscles from DMD mouse models(mdx mice) and Duchenne patients compared tonormal muscles (Refs. 13, 84, 88, 89). Increasedintracellular Ca2+ levels observed in dystrophin-deficient fibres is a complex process that involves,at least, trans-sarcolemmal Ca2+ fluxes, SR Ca2+
leakage and abnormal SR Ca2+ levels.High cytosolic Ca2+ levels may result from
enhanced Ca2+ influx through the dystrophin-deficient sarcolemma (Refs. 90, 91). This abnormalinflux seems to occur mostly through TRPCchannels, a type of mechanosensitive voltage-independent Ca2+ channels with increasedexpression in dystrophic muscle fibres (Ref. 40).Indeed, several groups have found that blockageof TRPC channels in dystrophic mice reduces theabnormal extracellular Ca2+ influx. Furthermore,overexpression of TRPC3 channels in normalmouse skeletal muscle enhances Ca2+ influx andresults in a phenotype that closely resemblesDGC-lacking dystrophic mice (Ref. 86). TRPCchannels can function as both, stretch-activatedand store-operated channels, and therefore theyare also involved in SOCE response, an influx ofextracellular Ca2+ triggered by SR depletion ofCa2+ that is enhanced in dystrophic fibres(Ref. 39). An increased SOCE associated withTRPC1 channels has been reported in dystrophic
expert reviewshttp://www.expertreviews.org/ in molecular medicine
7Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

Table
1.Calcium
-related
mec
hanism
saffected
inmus
culardys
trophies
Disea
seProtein
affected
Sub
cellu
lar
loca
lisation
Propose
dmec
hanism
Sys
tem
Referen
ces
Duc
henn
e(D
MD)
Dystrop
hin
Sarco
lemma-
cytosk
eleton
Abse
nceca
uses
mem
brane
frag
ility
and
tran
sarcolem
mal
Ca2
+en
try
Mou
semdxan
dhu
man
DMD
myo
tubes
90,9
1
TRPC
chan
nels
Sarco
lemma
Increa
sedex
pressionca
uses
high
Ca2
+
entry(SOCE)
mdxfib
res,
tran
sgen
icmice,
mou
semyo
tubes
39,4
0,86
,107
NCX
Sarco
lemma
Misfunc
tion:
reve
rsal
offunc
tionca
uses
high
Ca2
+en
try
human
myo
tubes
–rat
spinal
cord
cocu
ltures
93
Orai1
Sarco
lemma
Increa
sedex
pressionca
uses
increa
sed
SOCE
mdxmus
cles
96
RyR
1SRtriad,
tran
smem
brane
Misfunc
tionca
uses
SRCa2
+leak
ageto
thecy
toso
lmdxmus
cles
101
IP3R
SRtran
smem
brane
Increa
sedleve
ls,inc
reas
edac
tivity
caus
eshigh
cytoso
licCa2
+.A
lsoinvo
lved
inmito
chon
dria
ldefec
ts
mdxan
dDMD
myo
tubes
C.e
lega
ns,z
ebrafis
h
105,
106,
107,
110,
111
SERCA1
SRne
twork,
tran
smem
brane
Red
uced
activ
ity(con
trov
ersial)
mdxmus
cles
117,
118,
165
CSQ1,
CSQ-like
proteins
SRlumen
Red
uced
expressionresu
ltsin
low
SR
Ca2
+leve
lsmdxmus
cle
119,
120
sarcalum
enin
SRlumen
Red
uced
expressionresu
ltsin
low
SR
Ca2
+leve
lsmdxfib
res
121
–Mito
chon
dria
Calcium
overload
induc
esap
optosis
Dramatic
frag
men
tatio
nea
rlyin
the
patho
logy
mdxmyo
tubes
C.e
lega
ns,z
ebrafis
h10
9,11
0,11
1
(con
tinue
don
next
pag
e)
expert reviewshttp://www.expertreviews.org/ in molecular medicine
8Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

Table
1.Calcium
-related
mec
hanism
saffected
inmus
culardys
trophies
(con
tinued
)
Disea
seProtein
affected
Sub
cellu
lar
loca
lisation
Propose
dmec
hanism
Sys
tem
Referen
ces
LGMD2A
Calpain3
Triad,c
ytos
keleton
Abse
nceresu
ltsin
dysregu
latio
nof
SR
Ca2
+releas
eCap
n3kn
ocko
utmou
se13
3
RyR
1SRtriad,
tran
smem
brane
Red
uced
expressionca
uses
reduc
edSR
Ca2
+releas
eCap
n3kn
ocko
utmou
sean
dLG
MD2A
mus
cles
21,1
33,1
34
AldoA
Triad,c
ytos
olRed
uced
loca
lisationat
thetriadco
uld
caus
emisregu
latio
nof
RyR
1ac
tivity
Cap
n3kn
ocko
utmou
se13
3
CaM
KII
Triad,c
ytos
olRed
uced
expressionan
dac
tivity
affect
SR
Ca2
+up
take
andreleas
eCap
n3kn
ocko
utmou
sean
dLG
MD2A
mus
cles
21
–Mito
chon
dria
Abno
rmal
distributionan
dstructure,
oxidativestress,A
TPdeficitca
useCa2
+
misregu
latio
n
Cap
n3kn
ocko
utmou
sean
dLG
MD2A
mus
cles
141,
142
Myo
tonic
Dys
trophy
(DM)
DHPR
Sarco
lemma,
triad
Aberrant
mRNAsp
licingen
hanc
esga
ting
propertie
s.Red
uced
expressionin
DM1
mus
cles
DM
mus
cles
and
mou
semod
el14
8,15
0
RyR
1SRtriad,
tran
smem
brane
Red
uced
protein
expressionin
DM1an
dDM2.
Aberrant
mRNAsp
licingca
uses
reduc
edac
tivity
DM1an
dDM2
mus
cles
DM1myo
tubes
149,
150,
153
SERCA1
SRne
twork,
tran
smem
brane
Aberrant
mRNAsp
licingmay
caus
eincrea
sed[Ca2
+]i
DM1myo
tubes
149
SERCA2
SRne
twork,
tran
smem
brane
Red
uced
protein
leve
lsin
DM2
DM2mus
cles
153
CSQ2
SRlumen
(slow
fibres)
Red
uced
protein
expressionin
DM1an
dDM2mus
cles
caus
esreduc
edSRCa2
+
conc
entration
DM1an
dDM2
mus
cles
153
JPH1
Triad,c
ytos
olRed
uced
proteininDM1an
dDM2mus
cles
may
caus
ereduc
edE–C
coup
ling
DM1an
dDM2
mus
cles
153
expert reviewshttp://www.expertreviews.org/ in molecular medicine
9Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

fibres, and remarkably, it can be restored to normallevels by inducing expression of minidystrophin, asmaller and partially functional dystrophin variant(Ref.92).Finally,enhancedCa2+ influxindystrophicfibres has also been reported to occur by reversalNCX sarcolemmal channels (Ref. 93) and also bythe Orai1/Stim SOCE pathway. In addition toTRPC channels, other proteins may also beresponsible for increased SOCE in DMD, such asstromal interaction molecule 1 (STIM1), whichacts as an SR Ca2+ sensor that can trigger SOCEthrough both TRPCs and Orai1 channels (Ref. 94).In this regard, it has been recently reportedincreased Orai1 (Refs. 95, 96) and STIM1 (Ref. 95)expression in dystrophic muscles from mdx mice.This indicates that enhanced activation of SOCEpathways may contribute to the disrupted Ca2+
homeostasis in DMD pathology. Several otherproteins have been involved in this enhancedSOCE activity in dystrophin-deficient musclemyotubes, such as phospholipase C, proteinkinase C (Ref. 97), phospholipase A2 (iPLA2) andits derived metabolites (Ref. 98). In this regard,increased iPLA2 activity has been known for morethan 10 years in DMDmuscles (Ref. 99). Therefore,specific inhibitors of these pathways may be ofinterest to reduce Ca2+ influx and subsequentdegeneration of dystrophic muscle (Ref. 100).Another source of elevated cytosolic Ca2+ levels
may involve SR Ca2+ leakage through RyRs orIP3Rs. Regarding RyRs, several studies havepointed to abnormally high S-nitrosylation ofRyR1 cysteine residues in mdx mice causingcalstabin-1 depletion from the RyR complex, thatlead to unstable and leaking RyR1 channels atresting conditions (Refs. 101, 102, 103). Theseabnormal S-nitrosylation levels seem to be due toinducible nitric oxide synthase (iNOS), which wasalso found increased in dystrophic mdx muscles.A recent study has found evidence of significant
Ca2+ leakage through IP3Rs as well as throughRyRs in dystrophic mdx myotubes contributingto the increased intracellular Ca2+ levels(Ref. 104), which suggests that IP3R malfunctionmay also be involved in DMD Ca2+
mishandling. Indeed, previous studies haveshown increased IP3R and IP3 levels, andenhanced IP3R-dependent Ca2+ transients inmyotubes from DMD patients and mdx mice(Refs. 105, 106, 107). Moreover, inducedexpression of minidystrophin in dystrophin-deficient myotubes reverts the IP3R-dependentincrease in Ca2+ release to normal levels
(Ref. 108), which suggests an IP3R involvementin DMD impaired Ca2+ homeostasis. Finally,there seems to be a connection between IP3Rand mitochondria that may play a relevant rolein Ca2+ dysregulation. Previous work in mdxdystrophic myotubes has shown mitochondrialCa2+ overload due to increased SR Ca2+ release(Ref. 109). Interestingly, overexpression of Bcl-2antiapoptotic protein in mdx myotubes preventsthis mitochondrial Ca2+ overload by inhibitingIP3Rs (Ref. 110). More recently, abnormalmitochondrial fragmentation has been observedin Caenorhabditis elegans and zebrafish models ofDMD, where involvement of cytochrome c inmuscle fibre death was demonstrated, acting inpart through an interaction with IP3R (Ref. 111).
In DMD and in many other neuromusculardisorders such as sarcoglinopathies, desminopathies,LGMD2B muscular dystrophy and Pompedisease, the cardiac and respiratory muscles areaffected and, consequently, there is an increasedrisk of respiratory and cardiac failure inthese patients that leads to early mortality(Ref. 84). Abnormal Ca2+ homeostasis andmitochondrial dysfunction have also beenreported in these muscles. In particular,previous works in mdx cardiac myocytes haveshown that stretch-activate channels contributeto abnormal Ca2+ influx (Ref. 112), andexcessive cytosolic Ca2+ signals induced bymechanical stress result in mitochondrialdysfunction (Ref. 113). More recently, highermitochondrial Ca2+ levels have been reported incardiac dystrophic myocytes and activation ofDHPR seems to contribute to abnormalmitochondrial Ca2+ handling (Ref. 114).Evidence for early mitochondrial dysfunction indystrophic cardiomyopathy is further supportedby alterations in mitochondrial citric acid cycle-related parameters observed in ex vivo mdxhearts preceding overt cardiomyopathy (Ref. 115).
Another controversial issue is whether SERCAexpression or function is reduced, unchanged orincreased in dystrophin-deficient fibres, withrecent examples in the literature supporting alldifferent possibilities (Refs. 96, 116, 117, 118).Regardless the need for further studies toestablish a clear understanding on this subject,the majority of the studies agree with a reducedSERCA activity in mdx muscles. In this line,nitrative stress could be causing a reducedSERCA activity in dystrophic fibres, sinceSERCA is highly sensitive to reactive nitrogen
expert reviewshttp://www.expertreviews.org/ in molecular medicine
10Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

species (Ref. 68) and high iNOS levels have beenreported in mdx fibres (Ref. 101).Ca2+ binding proteins and decreased SR Ca2+
buffering have also been involved in thepathology of dystrophinopathies. In particular,in the SR lumen, reduction of CSQ1, CSQ-likeproteins and sarcalumenin has been observed inmdx dystrophic muscles (Ref. 119, 120, 121). Asignificant reduction of the SR Ca2+ bufferingwould have a direct negative impact on theCa2+ reuptake capacity of SERCA, which inturn, would result in the increased cytosolicCa2+ levels. Remarkably, less affected musclesin the mdx muscular dystrophy mouse model,such as the extraocular and intrinsic laryngealmuscles, exhibit higher expression levels ofseveral Ca2+-handling proteins such as CSQ,calmodulin and/or SERCA (Refs. 122, 123),which suggests that these proteins are playing aprotective role in DMD pathology.
CalpainopathiesLGMDs are a large group of hereditary musculardystrophies characterisedbyprogressiveproximalweakness and a predominant involvement of thescapula, pelvic girdle and trunk muscles withoutaffecting cardiac or facial muscles (Ref. 124).Among the recessive forms of LGMDs,calpainopathy or LGMD2A is the most frequentmuscular dystrophy with a prevalence of82–100% in genetically isolated populations suchas the Basque Country (Refs. 125, 126).LGMD2A is caused by mutations in the geneencoding Calpain 3 (CAPN3), a non-lysosomalcysteine protease necessary for normal musclefunction and regeneration (Refs. 127, 128). The exactpathogenic mechanisms that underlie musculardystrophic features caused by mutations in CAPN3are still unclear, and in view of the lack of effectivetherapies available for LGMD2A patients,understanding these pathological mechanisms isneeded in order to advance in the design ofpotential treatments.In skeletal muscle CAPN3 is present in different
subcellular locations including myofibrils,membrane and cytoplasm. Most of the CAPN3is bound within the contractile filamentnetwork, where it remains in its inactive statethrough its association with titin, a giant proteinthat connects the Z line to the M line in thesarcomere (Refs. 129, 130). Absence of CAPN3from mouse and human muscles results insarcomere disorganisation (Refs. 127, 131),
which suggests that CAPN3 is involved insarcomere repair and maintenance and may alsobe acting as a sensor of its integrity andfunctionality (Ref. 129). Remarkably, sarcomerealignment is preserved in mice expressing aninactive form of CAPN3 (Capn3cs/cs mice),indicating that the structural role of CAPN3 andnot the enzymatic one is involved in sarcomericremodelling (Ref. 132).
In the membranes, CAPN3 is localised in thetriad protein complex and plays an essential rolein preserving its structure and function. CAPN3has been found to interact with RyR1 (Ref. 132),the main SR Ca2+ release channel, and regulateCa2+ release from SR (Ref. 133). CAPN3 has alsobeen found to interact with the Ca2+-handlingprotein CSQ by immunoprecipitation analysis(Ref. 132). This interaction is proposed to occurby means of connecting proteins such as triadin,since CSQ and CAPN3 are localised in differentcellular compartments. In CAPN3 knockoutmice (C3KO, Capn3-/-), reduced expression ofRyR1 is concomitant with the reduced SR Ca2+
release (Refs. 133, 134). Also, it has beenpreviously reported slower Ca2+ reuptake intoSR after SR Ca2+ depletion in CAPN3 mice,although the basis of these finding needs furtheranalysis (Ref. 134). However, loss of CAPN3proteolytic activity in Capn3cs/cs mice does notaffect Ca2+ homeostasis (Ref. 132), whichindicates that the structural role of CAPN3 isa key for maintenance of Ca2+ homeostasis.In this line, we have recently shown in acollaboration study that muscles from LGMD2Apatients with deficient CAPN3 also expressedlower RyR1 protein levels. Moreover, we founda correlation between CAPN3 and RyR1expression levels that supports a structuralfunction of CAPN3 in the preservation of thetriad protein complex (Ref. 21).
Another CAPN3-binding partner in the triadcomplex is aldolase A (AldoA) (Ref. 133), aglycolytic enzyme that may modulate Ca2+
handling in the muscle fibre through multiplemechanisms, including direct regulation of RyRactivity by intermediates and products ofglycolysis, and modulation of SERCA activitythrough local changes of glycolytically derivedATP (Ref. 135). In the skeletal muscle, AldoAdirectly interacts with RyR1 and in vitro it hasbeen shown to modulate RyR1 activity (Refs.133, 136). Interestingly, CAPN3 knockout miceshow decreased levels of AldoA in the
expert reviewshttp://www.expertreviews.org/ in molecular medicine
11Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

sarcomere due to impaired recruitment of AldoAto the triads (Ref. 133). Remarkably, mutations inthe gene encoding AldoA result in severe skeletalmuscle damage in humans (Refs. 137, 138).Ca2+ calmodulin kinase II (CaMKII) is another
triad component that is modulated by CAPN3. Inthis regard, our group has found that CaMKIIsignalling is compromised in CAPN3 knockoutmice and, thus, we propose that impairedCa2+-mediated signalling and weakened muscleadaptation are pathogenic mechanisms likelyoperating in CAPN3-deficient muscles (Ref. 21).CaMKII is a multifunctional protein activatedby muscle contraction-induced Ca2+ increasethat regulates several Ca2+-handling proteins(Ref. 7). In slow twitch skeletal fibres, CaMKIImay increase SERCA2 activity through directphosphorylation or by phosphorylation of itsinhibitory protein phospholamban (Refs. 67,139). On the other hand, CaMKII is also able tomodulate Ca2+ release through phosphorylationof related proteins, such as triadin, whichinhibits RyR1 activity when unphosphorylated(Ref. 140). Thus, decreased CaMKII signallinglevels, comparable to the ones observed inCAPN3 deficient muscles, may result inreduction of SR Ca2+ release during contractionsas well as reduced Ca2+ reuptake by SERCA.However, this hypothesis needs verificationthrough experimental analysis.Finally, there seems to be a connection between
CAPN3 and mitochondrial function, sinceLGMD2A patients and CAPN3 knockout miceshow abnormal distribution and structure ofmitochondria in skeletal fibres (Ref. 141).Moreover, CAPN3-deficient muscles show ATPproduction deficits and increase oxidative stresslevels (Ref. 142). Accordingly, muscles withhigher percentage of slow twitch fibres, whichhave higher oxidative metabolism, are the mostaffected in CAPN3 knockout mice (Refs. 21,142). These mitochondrial abnormalities arelikely associated to a severe Ca2+ dysregulationin CAPN3-deficient muscle fibres, althoughfuture experiments are still needed in order toelucidate the pathogenic mechanisms involvedin the mitochondrial dysfunction observed inLGMD2A.
Myotonic dystrophyMyotonic dystrophy type 1 (DM1), the mostfrequent adult form of muscular dystrophy(Ref. 143), is an inherited autosomal dominant
disease caused by an unstable expansion of theCTG triplet repeat located in the 3′ untranslatedregion of DMPK gene that codes for myotonicdystrophy protein kinase. This gene is locatedin the long arm of chromosome 19 and it ispredominantly expressed in skeletal muscle(Ref. 144). DM2 form is a rare disease associatedwith a CCTG tetranucleotide repeat expansion,located in the first intron of the zinc fingerprotein 9 (ZNF9) gene in chromosome 3. Thus,both DM1 and DM2 originate from long non-coding repeat expansions, which cause a similarchronic, slowly progressing, multisystemicdisease with a dominant inheritance pattern.Expanded mRNA molecules in the cell nucleusaffect expression and/or re-allocation of RNA-binding proteins and lead to alteration in RNAprocessing (Refs. 145, 146, 147). The multi-systemic nature of both diseases is thought tobe caused by aberrant splicing affecting anumber of proteins involved in multiple cellularprocesses. It has recently been shown thatmyotonic dystrophy is associated withderegulated alternative splicing of the geneCACNA1S that encodes for DHPR alpha 1Ssubunit (DHPRα1s), a voltage sensor that playsa central role in E–C coupling (Ref. 148). In DM1and DM2, skipping of CACNA1S exon 29 isenhanced, which increases DHPRα1s channelconductance and voltage sensitivity. The long-term consequences are very likely harmful tomuscle, especially when DHPR missplicing iscombined with deregulated alternative splicingof other genes related to Ca2+-handling or E–Ccoupling such as the ones encoding chloridechannel type 1, SERCA and RyR1 (Refs. 149,150). This would likely lead to a chronic Ca2+
overload, a common scenario occurring in otherforms of muscular dystrophies. In fact, severalstudies have reported that Ca2+-signallingpathways are consistently affected in DMmuscles, DM myotubes and mouse models ofthis disease (Refs. 151, 152, 153). These findingssuggest that the combined effect of misregulatedsplicing of several genes involved in Ca2+
regulation and E–C coupling contributes tomuscle degeneration in myotonic dystrophy. Inparticular, a recent study performed on humanDM samples demonstrates abnormal expressionof mRNA and proteins involved in muscle Ca2+
release, reuptake, storage and signalling, such asjunctophilin-1 (JPH1), SERCA2, RyR1, CSQ2and DHPR (Ref. 153). In DM muscles they
expert reviewshttp://www.expertreviews.org/ in molecular medicine
12Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

found reduced protein levels of JPH1, but notmRNA, which is consistent with a generaldysregulation of Ca2+ homeostasis since JPH1undergoes Ca2+-dependent proteolysis whenintracellular Ca2+ levels are elevated for asustained period (Refs. 154, 155). Interestingly,in most cases mRNA levels of Ca2+-handlingmolecules were found increased while theprotein levels were decreased, which suggeststhat the translational block may be one of theunderlying mechanisms of DM.
Therapeutic targeting ofmitochondria andcalcium homeostasis in muscular
dystrophiesOver the years, several pharmacological andmolecular therapies that target Ca2+ homeostasisand/or mitochondrial function have beenproposed as potential treatments for musculardystrophies (summarised in Table 2). Differentstudies have demonstrated beneficial effects ofRyR stabilisers on different animal models ofmuscular dystrophy and heart failure (Refs. 50,101, 156). In particular, treatment of mousemodels of Duchenne and LGMD2E musculardystrophy with the RyR stabiliser S107 results inreduced RyR1 nitrosylation, reversion ofcalstabin-1 depletion and an overall improvementof muscle function and exercise performance(Refs. 101, 156). Interestingly, a recent study hasdemonstrated that S107, as well as the RyRinhibitor dantrolene, synergise with antisense-mediated exon-skipping therapies and increasesmuscle function in mdx mice and human DMDmyotubes (Ref. 157). Also, several Ca2+ channelblockers such as nifedipine, diltiazem andverapamil have shown to improve musclestructure and function in dystrophic mice (Refs.158, 159), but they have failed to prove significantbeneficial effects on DMD patients in clinical trials(Ref. 160). Likewise, pharmacological ormolecular blockage of stretch-activated channels(TRPC, TRPV2) has also shown a beneficial effecton several dystrophic models (Refs. 89, 161).Angiotensin II-receptor blockers, β-blockers and
angiotensin-converting-enzyme inhibitors haveshown beneficial effects for the treatment ofcardiomyopathies in clinical trials and animalmodels (Refs. 162, 163). Interestingly, somepharmacological agents from these groups havealso been reported to increase SERCA2 expressionand/or function, and therefore they are potentialenhancers of cardiac Ca2+ homeostasis (Ref. 164).
In this line, different strategies comprisingoverexpression of SERCA1 or SERCA2 in skeletalmuscle of dystrophic mice, such as treatment withBGP-15, or AAV-mediated gene transfer haveconsistently shown a significant improvement inthe dystrophic phenotype (Refs. 117, 118, 165),which further supports that reduced SERCAactivity is a contributing factor in the pathology ofmuscular dystrophies.
Finally, several therapeutic approaches targetingmitochondrial dysfunction have been shown toimprove muscle function in different dystrophicmouse models. These include treatment withcyclosporine A and cyclophilin D inhibitors(Debio 025) for impaired mitochondrial PTPopening, treatment with pargyline for excessiveaccumulation of reactive oxygen species oroverexpression of peroxisome proliferator-activated receptor γ coactivator 1-gene α (PGC1α) for mitochondrial dysfunction in postnecroticdystrophic muscles (Ref. 166). In this line, anantioxidant that improves mitochondrialrespiratory function, idebenone, has shownprotection of cardiac and skeletal muscle in mdxmice and trends of efficacy in a Phase II studywith DMD patients (Ref. 167).
Conclusions and future addressThe full extent to which intracellular Ca2+
signalling influences the physiopathology ofprimary and secondary muscle diseases is onlybeginning to be understood. In the forthcomingyears, future technological advances, includingnew powerful Ca2+ indicators are neededin order to accelerate and target-specificCa2+-signalling pathways within cells. Somepromising genetically encoded Ca2+ indicatorsfrom invertebrates or algae are already underdevelopment and will likely provide us withnew clues to understanding the role of Ca2+ indegenerative processes. Since these indicatorsare both, incorporated at the genome level andtranslated as fluorescent proteins that modifytheir emission intensity as a function of Ca2+
levels, they can be used for long-termexperiments over days to months and they canalso be introduced into in vivo animal models totest Ca2+ activity over a lifetime (Refs. 168, 169).Furthermore, other imaging technologies suchas fluorescence resonance energy transfer-based(FRET) analysis can demonstrate Ca2+-dependent responses at the single protein level(Ref. 170). In the near future, these
expert reviewshttp://www.expertreviews.org/ in molecular medicine
13Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

Table
2.Trea
tmen
tstargetingca
lcium
homeo
stas
isan
dmitoch
ond
rial
func
tionin
mus
culardys
trophies
Metho
dEffec
tonCa2
+ho
meo
stas
is/
mitoch
ond
rial
func
tion
Sys
tem
Clin
ical/
pha
rmac
ological
use
Commen
tsReferen
ces
Pha
rmac
olog
ical
K20
1/JT
V51
9RyR
stab
ilise
r/regu
latorInhibits
SERCApum
ps
Mou
semod
elof
heartfailure
Can
didateca
rdioprotective
reag
ent.Preve
ntsCa2
+
leak
agefrom
SR
Antag
onistof
multip
leion
chan
nelsIm
prove
sca
rdiac
andmus
clefunc
tion
50
S10
7(K20
1an
alog
ue)
RyR
stab
ilise
r/regu
lator
mdxan
dSgc
b−/−
mice
Preve
ntsCa2
+leak
age
from
SR
Amelioratesmus
cular
dystrop
hicphe
notype
Enh
ance
sex
onsk
ipping
101,
156,
157
Dan
trolen
eRyR
antago
nist
mdxmou
sean
dDMD
myo
tubes
Mus
clerelaxa
nt.T
reatmen
tformaligna
nthy
perthermia
Enh
ance
sex
onsk
ipping
157
Nife
dipine
DHPRca
lcium
block
ermdxmice.
DMDclinical
trial
Antihyp
ertens
ive,
antia
nginal
Improve
sdystrop
hic
mus
clefunc
tion.
No
sign
ifica
nteffect
onDMD
clinical
trials
158,
160
Diltiaze
mVe
rapam
ilNon
-DHPRca
lcium
block
er.
Inhibito
rSERCA2func
tion
mdxmice.
DMDclinical
trial
Vaso
dilator
Antiang
inal,a
ntiarrythm
icProtect
dystrop
hicfib
res
from
deg
eneration.
No
sign
ifica
nteffectson
DMD
clinical
trials
159,
160,
164
BGP-15
Increa
sesSERCAac
tivity
mdx,
dko
mice
Insu
linse
nsitise
rPha
rmac
olog
icalinduc
erof
HSP70
Amelioratin
geffect
ondystrop
hicmice
118
Ena
lapril
Increa
sesSERCA2ex
pression
andfunc
tion
mdxmice.
DMDclinical
trial
Ang
iotens
in-con
verting
enzymeinhibito
rIm
prove
smus
clestreng
than
dreduc
esfib
rosis.
Like
lyprese
rves
cardiac
func
tionin
DMDpatients
162,
164
Carve
dilo
lIncrea
sesSERCA2ex
pression
andfunc
tion
DMDclinical
trials
β-block
erLike
lyprese
rves
cardiac
func
tionin
DMDpatients
163,
164
(con
tinue
don
next
pag
e)
expert reviewshttp://www.expertreviews.org/ in molecular medicine
14Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

Table
2.Trea
tmen
tstargetingca
lcium
homeo
stas
isan
dmitoch
ond
rial
func
tionin
mus
culardys
trophies
(con
tinued
)
Metho
dEffec
tonCa2
+ho
meo
stas
is/
mitoch
ond
rial
func
tion
Sys
tem
Clin
ical/
pha
rmac
ological
use
Commen
tsReferen
ces
Losa
rtan
Increa
sesSERCA2ex
pression
andfunc
tion
mdxmice
Ang
iotens
inIIrece
ptor
block
er.B
lock
sTG
F-β
sign
alling
Prese
rves
cardiacfunc
tion
Improve
sresp
iratory
func
tion
162,
164
Res
veratrol
Increa
sesSERCA2ex
pression
mdxmice
Antioxidan
tSIRTac
tivator
Hea
rtdisea
ses
Ameliorateingeffect
ondystrop
hicmice
162,
164
Strep
tomyc
inBlock
erof
stretch-ac
tivated
chan
nels
(TRPCs)
mdxmice
Amyn
olyc
oside
Doe
sno
taffect
ribos
omal
read
throug
h
Protectsag
ains
tmus
cle
dam
age
89
Cyc
losp
orin
ADeb
io02
5Mictoch
ondria
lPTP
inhibito
rs.
Red
uceSERCA2ex
pression
mdx,
Sgc
b−/−,
Col6a
1(−/−
)
mice
Immun
osup
pressan
tsIm
prove
mus
clefunc
tionin
dystrop
hicmou
semod
els
164,
166
Ideb
enon
eIm
prove
smito
chon
dria
lfun
ction
mdx,
DMD
patients
Antioxidan
tAmelioratin
geffect
ondystrop
hicmice.
Tren
dsof
effic
acyin
DMDPha
seII
clinical
stud
y
162,
167
Pargy
line
Mon
oamineox
idas
eBinhibito
rCol6a
1(−/−
)
andmdxmice
Dec
reas
eROS
accu
mulationge
nerated
byMAOB
Amelioratin
geffect
ondystrop
hicmice
166
Molec
ular
AAV
-med
iated
tran
sfer
ofSERCA
Increa
sesSERCA1/
2ex
pression
andfunc
tion
mdx,
Sgc
b−/−
Amelioratin
geffect
ondystrop
hicmice
117,
165
Aden
ovira
l-dom
inan
tne
gativ
eTR
PV2
Red
uces
TRPV2sign
alling
δ-sa
rcog
lyca
ndeficient
hamster
Amelioratin
geffect
ondystrop
hicmice
161
PGC1α
gene
tran
sfer
Res
toresmito
chon
dria
lfun
ction
mdxmice
Amelioratin
geffect
ondystrop
hicmice
166
expert reviewshttp://www.expertreviews.org/ in molecular medicine
15Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

developments will contribute to the design of newexperiments with potential applications in basicscience and translational research studies(Ref. 171).The target of these research lines in the field of
muscular dystrophies should be focused in thefirst place on disorders where Ca2+ homeostasisseems to play a central role, such as inmalignant hyperthermia, central core disease orarrythmogenic cardiomyopathies (Ref. 50).Nevertheless, as awareness of Ca2+-signallingdysregulation in other muscular diseasesprogresses, such as LGMD2A, attention shouldbe addressed to specific elements of intracellularCa2+-signalling cascades in these entities. Froma therapeutical point of view, some progress inthese areas is already taking place: the DHPRblocker nifedipine and the SR leaky-channelblockers dantrolene and S-107, for instance, havebeen successfully tested in animal models ofmuscular dystrophy (Refs. 101, 156, 158). It isvery likely that whatever achievements maycome from these on-going research projects, theywill be useful for several other muscular disorderssharing similar underlying Ca2+ pathologicalmechanisms.
Financial supportResearch in our laboratories is supported by theInstituto Carlos III (A.V.-I., grant number PI11/01499), Gobierno Vasco (A.V.-I., grant numbersSAIO12-PR12BN002, 2010111089), Marie CurieInternational Reintegration Grant (A.V.-I., grantnumber IRG256512) and Fundación de EstudiosNeurológicos ILUNDAIN. I.T.-O. and G.A. arefunded by PhD fellowships from Gobierno Vasco.
Conflicts of interestNone.
References1 Berridge, M.J., Bootman, M.D. and Roderick, H.L.
(2003) Calcium signalling: dynamics, homeostasisand remodelling. Nature Reviews Molecular CellBiology 4, 517-529
2 Leong, P. and MacLennan, D.H. (1998) Complexinteractions between skeletal muscle ryanodinereceptor and dihydropyridine receptor proteins.Biochemistry and Cell Biology 76, 681-694
3 Melzer,W., Herrmann-Frank, A. and Luttgau, H.C.(1995) The role of Ca2+ ions inexcitation–contraction coupling of skeletal musclefibres. Biochimica et Biophysica Acta 1241, 59-116
4 Murray, B.E. et al. (1998)Excitation–contraction–relaxation cycle: role ofCa2+-regulatory membrane proteins in normal,stimulated and pathological skeletal muscle(review). International Journal of MolecularMedicine 1, 677-687
5 Baylor, S.M. and Hollingworth, S. (2012)Intracellular calcium movements duringexcitation–contraction coupling in mammalianslow-twitch and fast-twitch muscle fibers. Journalof General Physiology 139, 261-272
6 Chin, E.R. and Allen, D.G. (1996) The role ofelevations in intracellular [Ca2+] in thedevelopment of low frequency fatigue in mousesingle muscle fibres. Journal of Physiology 491(Pt3), 813-824
7 Allen, D.G., Lamb, G.D. and Westerblad, H. (2008)Impaired calcium release during fatigue. Journal ofApplied Physiology 104, 296-305
8 Andersson, D.C. et al. (2011) Ryanodine receptoroxidation causes intracellular calcium leak andmuscle weakness in aging. Cell Metabolism 14,196-207
9 Alderton, J.M. and Steinhardt, R.A. (2000) Howcalcium influx through calcium leak channels isresponsible for the elevated levels of calcium-dependent proteolysis in dystrophic myotubes.Trends in Cardiovascular Medicine 10, 268-272
10 Culligan, K. and Ohlendieck, K. (2002) Diversity ofthe brain dystrophin–glycoprotein complex.Journal of Biomedicine and Biotechnology 2, 31-36
11 Gailly, P. (2002) Newaspects of calcium signaling inskeletal muscle cells: implications in Duchennemuscular dystrophy. Biochimica et BiophysicaActa1600, 38-44
12 Gillis, J.M. (1996) Membrane abnormalities and Cahomeostasis in muscles of the mdx mouse, ananimal model of the Duchenne musculardystrophy: a review. Acta PhysiologicaScandinavica 156, 397-406
13 Ruegg, U.T. et al. (2002) Pharmacological control ofcellular calcium handling in dystrophic skeletalmuscle. Neuromuscular Disorders 12(Suppl 1),S155-S161
14 Schiaffino, S. and Reggiani, C. (2011) Fiber types inmammalian skeletal muscles. PhysiologicalReviews 91, 1447-1531
15 Purves, D. and Williams, S.M. (2001)Neuroscience (2nd edn). Sinauer Associates,Sunderland, Mass.
16 Scott, W., Stevens, J. and Binder-Macleod, S.A.(2001) Human skeletal muscle fiber typeclassifications. Physical Therapy 81, 1810-1816
expert reviewshttp://www.expertreviews.org/ in molecular medicine
16Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

17 Lamboley, C.R., et al. (2013) Endogenous andmaximal sarcoplasmic reticulum calcium contentand calsequestrin expression in type I and type IIhuman skeletalmuscle fibres. Journal of Physiology591(Pt 23), 6053-6068
18 Lamboley,C.R., et al. (2014) Sarcoplasmic reticulumCa2+ uptake and leak properties, and SERCAisoform expression, in type I and type II fibres ofhuman skeletal muscle. Journal of Physiology592(Pt 6), 1381-1395
19 Pette, D. and Staron, R.S. (1997) Mammalianskeletal muscle fiber type transitions. InternationalReview of Cytology 170, 143-223
20 Webster, C. et al. (1988) Fast muscle fibers arepreferentially affected in Duchenne musculardystrophy. Cell 52, 503-513
21 Kramerova, I. et al. (2012) Impaired calciumcalmodulinkinase signalingandmuscle adaptationresponse in the absence of calpain 3. HumanMolecular Genetics 21, 3193-3204
22 Zeiger, U., Mitchell, C.H. and Khurana, T.S. (2010)Superior calcium homeostasis of extraocularmuscles. Experimental Eye Research 91, 613-622
23 Stutzmann, G.E. and Mattson, M.P. (2011)Endoplasmic reticulumCa(2+) handling in excitablecells in health and disease. PharmacologicalReviews 63, 700-727
24 Franzini-Armstrong, C. and Jorgensen, A.O. (1994)Structure and development of E–C coupling unitsin skeletal muscle. Annual Review of Physiology56, 509-534
25 Periasamy, M. and Kalyanasundaram, A. (2007)SERCA pump isoforms: their role in calciumtransport and disease. Muscle & Nerve 35, 430-442
26 Sacchetto, R. et al. (1996) Colocalization of thedihydropyridine receptor, the plasma-membranecalciumATPase isoform 1 and the sodium/calciumexchanger to the junctional-membrane domain oftransverse tubules of rabbit skeletal muscle.European Journal of Biochemistry 237, 483-488
27 Gilabert, J.A. (2012)Cytoplasmic calciumbuffering.Advances in Experimental Medicines and Biology740, 483-498
28 Schwaller, B. et al. (1999) Prolonged contraction-relaxation cycle of fast-twitch muscles inparvalbumin knockout mice. American Journal ofPhysiology 276(2 Pt 1), C395-C403
29 Heizmann, C.W., Berchtold, M.W. and Rowlerson,A.M. (1982) Correlation of parvalbuminconcentration with relaxation speed in mammalianmuscles. Proceedings of the National Academy ofSciences of the United States of America 79,7243-7247
30 Kurebayashi, N. and Ogawa, Y. (2001) Depletion ofCa2+ in the sarcoplasmic reticulum stimulates Ca2+
entry into mouse skeletal muscle fibres. Journal ofPhysiology 533(Pt 1), 185-199
31 Pan, Z. et al. (2002) Dysfunction of store-operatedcalcium channel in muscle cells lacking mg29.Nature Cell Biology 4, 379-383
32 Rosenberg, P. et al. (2004) TRPC3 channels confercellular memory of recent neuromuscular activity.Proceedings of theNationalAcademyof Sciences ofthe United States of America 101, 9387-9392
33 Stiber, J. et al. (2008) STIM1 signalling controlsstore-operated calcium entry required fordevelopment and contractile function in skeletalmuscle. Nature Cell Biology 10, 688-697
34 Darbellay, B. et al. (2009) STIM1- and Orai1-dependent store-operated calcium entry regulateshuman myoblast differentiation. Journal ofBiological Chemistry 284, 5370-5380
35 Cherednichenko, G. et al. (2004) Conformationalactivation of Ca2+ entry by depolarization ofskeletal myotubes. Proceedings of the NationalAcademy of Sciences of the United States ofAmerica 101, 15793-15798
36 Haws, C.M. and Lansman, J.B. (1991)Developmental regulation of mechanosensitivecalcium channels in skeletal muscle from normaland mdx mice. Proceedings of the Royal Society B:Biological Sciences 245, 173-177
37 Suzuki, M. et al. (1999) Cloning of a stretch-inhibitable nonselective cation channel. Journal ofBiological Chemistry 274, 6330-6335
38 Hopf, F.W. et al. (1996) A capacitative calciumcurrent in cultured skeletalmuscle cells ismediatedby the calcium-specific leak channel and inhibitedby dihydropyridine compounds. Journal ofBiological Chemistry 271, 22358-223567
39 Vandebrouck, A. et al. (2006) Regulation of store-operated calcium entries andmitochondrial uptakeby minidystrophin expression in culturedmyotubes. FASEB Journal 20, 136-138
40 Vandebrouck, C. et al. (2002) Involvement of TRPCin the abnormal calcium influx observed indystrophic (mdx) mouse skeletal muscle fibers.Journal of Cell Biology 158, 1089-1096
41 Al-Qusairi, L. and Laporte, J. (2011) T-tubulebiogenesisandtriadformationinskeletalmuscleandimplication in human diseases. SkeletalMuscle 1, 26
42 Rossi, A.E. and Dirksen, R.T. (2006) Sarcoplasmicreticulum: the dynamic calcium governor ofmuscle. Muscle & Nerve 33, 715-731
43 Murphy, R.M. et al. (2009) Calsequestrin contentand SERCA determine normal and maximal Ca2+
expert reviewshttp://www.expertreviews.org/ in molecular medicine
17Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

storage levels in sarcoplasmic reticulumof fast- andslow-twitch fibres of rat. Journal of Physiology587(Pt 2), 443-460
44 Arvanitis, D.A. et al. (2007) Histidine-rich Ca-binding protein interacts with sarcoplasmicreticulum Ca-ATPase. American Journal ofPhysiology: Heart and Circulatory Physiology 293,H1581-H1589
45 Lee, H.G. et al. (2001) Interaction ofHRC (histidine-rich Ca(2+)-binding protein) and triadin in thelumen of sarcoplasmic reticulum. Journal ofBiological Chemistry 276, 39533-39538
46 Paolini, C. et al. (2007) Reorganized stores andimpaired calcium handling in skeletal muscle ofmice lacking calsequestrin-1. Journal of Physiology583(Pt 2), 767-784
47 Beard, N.A., Wei, L. and Dulhunty, A.F. (2009)Control of muscle ryanodine receptor calciumrelease channels by proteins in the sarcoplasmicreticulum lumen. Clinical and ExperimentalPharmacology and Physiology 36, 340-345
48 Sztretye, M. et al. (2011) Measurement of RyRpermeability reveals a role of calsequestrin intermination of SR Ca(2+) release in skeletal muscle.Journal of General Physiology 138, 231-247
49 Capes, E.M., Loaiza, R. and Valdivia, H.H. (2011)Ryanodine receptors. Skeletal Muscle 1, 18
50 Mackrill, J.J. (2010) Ryanodine receptor calciumchannels and their partners as drug targets.Biochemistry and Pharmacology 79, 1535-1543
51 Van Petegem, F. (2012) Ryanodine receptors:structure and function. Journal of BiologicalChemistry 287, 31624-31632
52 Mackrill, J.J. (2012) Ryanodine receptor calciumrelease channels: an evolutionary perspective.Advances in Experimental Medicines and Biology740, 159-182
53 Andersson, D.C., et al. (2012) Stress-inducedincrease in skeletal muscle force requires proteinkinase A phosphorylation of the ryanodinereceptor. Journal of Physiology 590(Pt 24),6381-6387
54 Ward,C.W.etal. (2003)Defects inryanodinereceptorcalcium release in skeletal muscle from post-myocardial infarct rats. FASEB Journal 17, 1517-1519
55 Reiken, S. et al. (2003) PKA phosphorylationactivates the calcium release channel (ryanodinereceptor) in skeletal muscle: defective regulation inheart failure. Journal of Cell Biology 160, 919-928
56 Jiang, D., et al. (2008) Reduced threshold forluminal Ca2+ activation of RyR1 underlies a causalmechanism of porcine malignant hyperthermia.Journal of Biological Chemistry 283, 20813-20820
57 Palade, P., Mitchell, R.D. and Fleischer, S. (1983)Spontaneous calcium release from sarcoplasmicreticulum. General description and effects ofcalcium. Journal of Biological Chemistry 258,8098-8107
58 MacLennan, D.H. and Chen, S.R. (2009) Storeoverload-induced Ca2+ release as a triggeringmechanism for CPVT and MH episodes caused bymutations in RYR and CASQ genes. Journal ofPhysiology 587(Pt 13), 3113-3115
59 Marks, A.R. (1997) Intracellular calcium-releasechannels: regulators of cell life anddeath.AmericanJournal of Physiology 272(2 Pt 2), H597-H605
60 Blaauw, B. et al. (2012) No evidence for inositol1,4,5-trisphosphate-dependent Ca2+ release inisolated fibers of adult mouse skeletal muscle.Journal of General Physiology 140, 235-241
61 Zayas, R., Groshong, J.S. and Gomez, C.M. (2007)Inositol-1,4,5-triphosphate receptors mediateactivity-induced synaptic Ca2+ signals in musclefibers and Ca2+ overload in slow-channelsyndrome. Cell Calcium 41, 343-352
62 Tjondrokoesoemo, A. et al. (2013) Type 1 inositol(1,4,5)-trisphosphate receptor activates ryanodinereceptor 1 to mediate calcium spark signaling inadult mammalian skeletal muscle. Journal ofBiological Chemistry 288, 2103-2109
63 Maack, C. and O’Rourke, B. (2007)Excitation–contraction coupling andmitochondrialenergetics. Basic Research in Cardiology 102,369-392
64 Macdonald, W.A. and Stephenson, D.G. (2001)Effects of ADP on sarcoplasmic reticulum functionin mechanically skinned skeletal muscle fibres ofthe rat. Journal of Physiology 532(Pt 2), 499-508
65 MacLennan, D.H., Asahi, M. and Tupling, A.R.(2003) The regulation of SERCA-type pumps byphospholamban and sarcolipin. Annals of theNew York Academy of Sciences 986, 472-480
66 Lancel, S. et al. (2010) Oxidative posttranslationalmodificationsmediatedecreasedSERCAactivityandmyocyte dysfunction in Galphaq-overexpressingmice. Circulation Research 107, 228-232
67 Vangheluwe, P. et al. (2005) Modulatingsarco(endo)plasmic reticulum Ca2+ ATPase 2(SERCA2) activity: cell biological implications. CellCalcium 38, 291-302
68 Bigelow, D.J. (2009) Nitrotyrosine-modifiedSERCA2: a cellular sensor of reactive nitrogenspecies. Pflugers Archiv 457, 701-710
69 Franzini-Armstrong, C. (2007) ER-mitochondriacommunication. How privileged? Physiology(Bethesda) 22, 261-268
expert reviewshttp://www.expertreviews.org/ in molecular medicine
18Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

70 Eisenberg, B.R. (2011) Quantitative ultrastructureof mammalian skeletal muscle. ComprehensivePhysiology, Supplement 27: Handbook ofPhysiology, Skeletal Muscle: 73-112.
71 Hajnoczky, G. et al. (2000) The machinery of localCa2+ signalling between sarco-endoplasmicreticulum andmitochondria. Journal of Physiology529 (Pt 1), 69-81
72 Rizzuto, R. et al. (2009) Ca(2+) transfer from the ERto mitochondria: when, how and why. Biochimicaet Biophysica Acta 1787, 1342-1351
73 Challet, C. et al. (2001) Mitochondrial calciumoscillations in C2C12 myotubes. Journal ofBiological Chemistry 276, 3791-3797
74 Kavanagh, N.I., Ainscow, E.K. and Brand, M.D.(2000) Calcium regulation of oxidativephosphorylationinratskeletalmusclemitochondria.Biochimica et Biophysica Acta 1457, 57-70
75 Yi, J. et al. (2011) Mitochondrial calcium uptakeregulates rapid calcium transients in skeletalmuscle during excitation–contraction (E–C)coupling. Journal of Biological Chemistry 286,32436-32443
76 Pizzo, P. et al. (2012) Mitochondrial Ca(2+)
homeostasis: mechanism, role, and tissuespecificities. Pflugers Archiv 464, 3-17
77 Ascah,A. et al. (2011) Stress-induced opening of thepermeability transition pore in the dystrophin-deficient heart is attenuated by acute treatmentwith sildenafil. American Journal of Physiology:Heart and Circulatory Physiology 300, H144-H153
78 Fraysse, B. et al. (2010) Ca2+ overload andmitochondrial permeability transition poreactivation in living delta-sarcoglycan-deficientcardiomyocytes. American Journal of Physiology:Cell Physiology 299, C706-C713
79 Logan, C.V. et al. (2014) Loss-of-functionmutationsinMICU1 cause a brain andmuscle disorder linkedto primary alterations in mitochondrial calciumsignaling. Nature Genetics 46, 188-193
80 Emery, A.E. (2002) The muscular dystrophies.Lancet 359, 687-695
81 Hoffman, E.P., Brown, R.H. Jr. and Kunkel, L.M.(1987) Dystrophin: the protein product of theDuchenne muscular dystrophy locus. Cell 51,919-928
82 Blake, D.J., et al. (2002) Function and genetics ofdystrophin and dystrophin-related proteins inmuscle. Physiological Reviews 82, 291-329
83 Petrof, B.J. et al. (1993) Dystrophin protects thesarcolemma from stresses developed duringmuscle contraction. Proceedings of the National
Academy of Sciences of the United States ofAmerica 90, 3710-3714
84 Allen, D.G. et al. (2010) Calcium and the damagepathways inmusculardystrophy.Canadian Journalof Physiology and Pharmacology 88, 83-91
85 Bodensteiner, J.B. and Engel, A.G. (1978)Intracellular calcium accumulation in Duchennedystrophyandothermyopathies: a studyof 567,000muscle fibers in 114biopsies.Neurology28, 439-446
86 Millay, D.P., et al. (2009) Calcium influx is sufficientto induce muscular dystrophy through a TRPC-dependent mechanism. Proceedings of theNational Academy of Sciences of the United Statesof America 106, 19023-19028
87 Bertorini, T.E., et al. (1984)Calciumandmagnesiumcontent in fetuses at risk and prenecrotic Duchennemuscular dystrophy. Neurology 34, 1436-1440
88 Turner, P.R. et al. (1988) Increased proteindegradation results from elevated free calciumlevels found in muscle frommdx mice. Nature 335,735-738
89 Yeung, E.W. et al. (2005) Effects of stretch-activatedchannel blockers on [Ca2+]i and muscle damage inthe mdx mouse. Journal of Physiology 562(Pt 2),367-380
90 Fong, P.Y., et al. (1990) Increased activity of calciumleak channels inmyotubes ofDuchenne humanandmdx mouse origin. Science 250, 673-676
91 Franco, A. Jr. and Lansman, J.B. (1990) Calciumentry through stretch-inactivated ion channels inmdx myotubes. Nature 344, 670-673
92 Vandebrouck, A. et al. (2007) Regulation ofcapacitative calcium entries by alpha1-syntrophin:association of TRPC1with dystrophin complex andthe PDZ domain of alpha1-syntrophin. FASEBJournal 21, 608-617
93 Deval, E., et al. (2002) Na(+)/Ca(2+) exchange inhuman myotubes: intracellular calcium rises inresponse to external sodium depletion areenhanced in DMD. Neuromuscular Disorders 12,665-673
94 Lyfenko, A.D. and Dirksen, R.T. (2008) Differentialdependence of store-operated andexcitation–coupledCa2+ entry in skeletalmuscle onSTIM1 and Orai1. Journal of Physiology 586(Pt 20),4815-4824
95 Edwards, J.N. et al. (2010) Upregulation of store-operated Ca2+ entry in dystrophic mdx mousemuscle. American Journal of Physiology: CellPhysiology 299, C42-C50
96 Zhao, X. et al. (2012) Orai1 mediates exacerbatedCa(2+) entry in dystrophic skeletal muscle. PLoSONE 7, e49862
expert reviewshttp://www.expertreviews.org/ in molecular medicine
19Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

97 Sabourin, J. et al. (2012) Dystrophin/alpha1-syntrophin scaffold regulated PLC/PKC-dependent store-operated calcium entry inmyotubes. Cell Calcium 52, 445-456
98 Boittin, F.X. et al. (2010) Phospholipase A2-derivedlysophosphatidylcholine triggers Ca2+ entry indystrophic skeletal muscle fibers. Biochemical andBiophysical Research Communications 391, 401-406
99 Lindahl, M. et al. (1995) Phospholipase A2 activityin dystrophinopathies. Neuromuscular Disorders5, 193-199
100 Ismail, H.M. et al. (2013) Inhibition of iPLA2 betaand of stretch-activated channels by doxorubicinalters dystrophicmuscle function. British Journal ofPharmacology 169, 1537-1550
101 Bellinger, A.M. et al. (2009) Hypernitrosylatedryanodinereceptorcalciumreleasechannelsare leakyin dystrophic muscle. Nature Medicine 15, 325-330
102 Brillantes, A.B. et al. (1994) Stabilization of calciumrelease channel (ryanodine receptor) function byFK506-binding protein. Cell 77, 513-523
103 Bellinger, A.M. et al. (2008) Remodeling ofryanodine receptor complex causes “leaky”channels: a molecular mechanism for decreasedexercise capacity. Proceedings of the NationalAcademy of Sciences of the United States ofAmerica 105, 2198-202
104 Altamirano, F. et al. (2012) Increased restingintracellular calcium modulates NF-kappaB-dependent inducible nitric-oxide synthase geneexpression in dystrophic mdx skeletal myotubes.Journal of Biological Chemistry 287, 20876-20887
105 Liberona, J.L. et al. (1998) Differences in bothinositol 1,4,5-trisphosphate mass and inositol 1,4,5-trisphosphate receptors between normal anddystrophic skeletal muscle cell lines. Muscle &Nerve 21, 902-909
106 Basset, O. et al. (2004) Involvement of inositol 1,4,5-trisphosphate in nicotinic calcium responses indystrophic myotubes assessed by near-plasmamembrane calcium measurement. Journal ofBiological Chemistry 279, 47092-47100
107 Cardenas, C. et al. (2010) Abnormal distribution ofinositol 1,4,5-trisphosphate receptors in humanmuscle can be related to altered calcium signals andgene expression in Duchenne dystrophy-derivedcells. FASEB Journal 24, 3210-3221
108 Balghi, H. et al. (2006) Mini-dystrophin expressiondown-regulates overactivation of G protein-mediated IP3 signaling pathway in dystrophin-deficient muscle cells. Journal of GeneralPhysiology 127, 171-182
109 Robert, V. et al. (2001) Alteration in calciumhandling at the subcellular level in mdx myotubes.Journal of Biological Chemistry 276, 4647-4651
110 Basset,O. et al. (2006) Bcl-2 overexpressionpreventscalcium overload and subsequent apoptosis indystrophic myotubes. Biochemical Journal 395,267-276
111 Giacomotto, J. et al. (2013) Chemical geneticsunveils a key role of mitochondrial dynamics,cytochrome c release and IP3R activity in musculardystrophy. Human Molecular Genetics 22,4562-4578
112 Williams, I.A. and Allen, D.G. (2007) Intracellularcalcium handling in ventricular myocytes frommdx mice. American Journal of Physiology: Heartand Circulatory Physiology 292, H846-H855
113 Jung, C. et al. (2008) Dystrophic cardiomyopathy:amplification of cellular damage byCa2+ signallingand reactive oxygen species-generating pathways.Cardiovascular Research 77, 766-773
114 Viola, H.M. et al. (2013) L-type Ca(2+) channelcontributes to alterations in mitochondrial calciumhandling in the mdx ventricular myocyte.American Journal of Physiology: Heart andCirculatory Physiology 304, H767-H775
115 Khairallah, M. et al. (2007) Metabolic and signalingalterations in dystrophin-deficient hearts precedeovert cardiomyopathy. Journal of Molecular CellCardiology 43, 119-129
116 Robin, G., Berthier, C. and Allard, B. (2012)Sarcoplasmic reticulum Ca2+ permeation exploredfrom the lumen side in mdx muscle fibers undervoltage control. Journal of General Physiology 139,209-218
117 Goonasekera, S.A. et al. (2011) Mitigation ofmuscular dystrophy in mice by SERCAoverexpression in skeletal muscle. Journal ofClinical Investigation 121, 1044-1052
118 Gehrig, S.M. et al. (2012) Hsp72 preserves musclefunction and slows progression of severe musculardystrophy. Nature 484, 394-398
119 Culligan, K. et al. (2002) Drastic reduction ofcalsequestrin-like proteins and impaired calciumbinding in dystrophic mdx muscle. Journal ofApplied Physiology 92, 435-445
120 Doran, P. et al. (2004) Subproteomics analysis ofCa+-binding proteins demonstrates decreasedcalsequestrin expression in dystrophic mouseskeletal muscle. European Journal of Biochemistry271, 3943-3952
121 Dowling, P., Doran, P. and Ohlendieck, K. (2004)Drastic reduction of sarcalumenin in Dp427(dystrophin of 427 kDa)-deficient fibres indicates
expert reviewshttp://www.expertreviews.org/ in molecular medicine
20Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

that abnormal calcium handling plays a key role inmuscular dystrophy. Biochemical Journal 379(Pt 2),479-488
122 Ferretti, R. et al. (2009) Sarcoplasmic-endoplasmic-reticulum Ca2+-ATPase and calsequestrin areoverexpressed in spared intrinsic laryngealmusclesof dystrophin-deficient mdx mice. Muscle & Nerve39, 609-615
123 Pertille, A. et al. (2010) Calcium-binding proteins inskeletal muscles of the mdx mice: potential role inthe pathogenesis of Duchennemuscular dystrophy.International Journal of Experimental Pathology 91,63-71
124 Laval, S.H. and Bushby, K.M. (2004) Limb-girdlemuscular dystrophies – from genetics to molecularpathology. Neuropathology and AppliedNeurobiology 30, 91-105
125 Saenz, A., et al. (2005) LGMD2A:genotype–phenotype correlations based on a largemutational survey on the calpain 3 gene. Brain128(Pt 4), 732-742
126 Urtasun, M., et al. (1998) Limb-girdle musculardystrophy in Guipuzcoa (Basque Country, Spain).Brain 121 (Pt 9), 1735-1747
127 Hauerslev, S. et al. (2012) Calpain 3 is important formuscle regeneration: evidence from patients withlimb girdle muscular dystrophies. BMCMusculoskeletal Disorders 13, 43
128 Richard, I. et al. (1995) Mutations in the proteolyticenzyme calpain 3 cause limb-girdle musculardystrophy type 2A. Cell 81, 27-40
129 Beckmann, J.S. and Spencer, M. (2008) Calpain 3,the “gatekeeper” of proper sarcomere assembly,turnover and maintenance. NeuromuscularDisorders 18, 913-921
130 Murphy, R.M. and Lamb, G.D. (2009) Endogenouscalpain-3 activation is primarily governed by smallincreases in resting cytoplasmic [Ca2+] and is notdependent on stretch. Journal of BiologicalChemistry 284, 7811-7819
131 Kramerova, I. et al. (2004) Null mutation of calpain3 (p94) in mice causes abnormal sarcomereformation in vivo and in vitro. Human MolecularGenetics 13, 1373-1388
132 Ojima, K. et al. (2011) Non-proteolytic functions ofcalpain-3 in sarcoplasmic reticulum in skeletalmuscles. Journal of Molecular Biology 407,439-449
133 Kramerova, I. et al. (2008) Novel role of calpain-3 inthe triad-associated protein complex regulatingcalcium release in skeletal muscle. HumanMolecular Genetics 17, 3271-3280
134 Dayanithi, G. et al. (2009) Alteration ofsarcoplasmic reticulum Ca2+ release in skeletalmuscle from calpain 3-deficient mice. InternationalJournal of Cell Biology 2009, 340-346
135 Kockskamper, J., Zima,A.V. and Blatter, L.A. (2005)Modulation of sarcoplasmic reticulumCa2+ releaseby glycolysis in cat atrial myocytes. Journal ofPhysiology 564(Pt 3), 697-714
136 Seo, I.R. et al. (2006) Aldolase potentiates DIDSactivation of the ryanodine receptor in rabbitskeletal sarcoplasmic reticulum. BiochemistryJournal 399, 325-333
137 Kreuder, J. et al. (1996) Brief report: inheritedmetabolic myopathy and hemolysis due to amutation in aldolase A. New England Journal ofMedicine 334, 1100-1104
138 Yao, D.C. et al. (2004) Hemolytic anemia and severerhabdomyolysis caused by compoundheterozygous mutations of the gene forerythrocyte/muscle isozyme of aldolase,ALDOA(Arg303X/Cys338Tyr). Blood 103,2401-2403
139 Sacchetto, R., et al. (2000) Coordinate expression ofCa2+-ATPase slow-twitch isoform and of betacalmodulin-dependent protein kinase inphospholamban-deficient sarcoplasmic reticulumof rabbitmassetermuscle. FEBSLetters 481, 255-260
140 Rose, A.J. et al. (2007) Regulation and function ofCa2+-calmodulin-dependent protein kinase II offast-twitch rat skeletal muscle. Journal ofPhysiology 580(Pt.3), 993-1005
141 Kramerova, I., Beckmann, J.S. and Spencer, M.J.(2007) Molecular and cellular basis ofcalpainopathy (limb girdle muscular dystrophytype 2A). Biochimica et Biophysica Acta 1772, 128-44
142 Kramerova, I. et al. (2009) Mitochondrialabnormalities, energy deficit and oxidative stressare features of calpain 3 deficiency in skeletalmuscle. Human Molecular Genetics 18(17),3194-3205
143 Harper, P.S. (2009) Myotonic dystrophy (2nd edn).Oxford University Press, Oxford, New York
144 Brook, J.D. et al. (1992)Molecular basis ofmyotonicdystrophy: expansion of a trinucleotide (CTG)repeat at the 3′ end of a transcript encoding aprotein kinase family member. Cell 68, 799-808
145 Dansithong, W. et al. (2005) MBNL1 is the primarydeterminant of focus formation and aberrantinsulin receptor splicing in DM1. Journal ofBiological Chemistry 280, 5773-5780
146 Philips, A.V., Timchenko, L.T. and Cooper, T.A.(1998) Disruption of splicing regulated by a CUG-
expert reviewshttp://www.expertreviews.org/ in molecular medicine
21Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

bindingprotein inmyotonicdystrophy. Science 280,737-741
147 Timchenko, N.A. et al. (2001) RNA CUG repeatssequester CUGBP1 and alter protein levels andactivity of CUGBP1. Journal of BiologicalChemistry 276, 7820-7826
148 Tang, Z.Z. et al. (2012) Muscle weakness inmyotonic dystrophy associated with misregulatedsplicing and altered gating of Ca(V)1.1 calciumchannel. Human Molecular Genetics 21, 1312-1324
149 Kimura, T. et al. (2005) Altered mRNA splicing ofthe skeletal muscle ryanodine receptor andsarcoplasmic/endoplasmic reticulumCa2+-ATPasein myotonic dystrophy type 1. Human MolecularGenetics 14, 2189-2200
150 Santoro, M. et al. (2014) Alternative splicingalterations of Ca(2+) handling genes are associatedwith Ca(2+) signal dysregulation in myotonicdystrophy type 1 (DM1) and type 2 (DM2)myotubes. Neuropathology and AppliedNeurobiology 40, 464-476
151 Benders, A.A. et al. (1997) Myotonic dystrophyprotein kinase is involved in the modulation of theCa2+homeostasis in skeletalmuscle cells. Journal ofClinical Investigation 100, 1440-1447
152 Jacobs, A.E. et al. (1990) The calcium homeostasisand the membrane potential of cultured musclecells from patients with myotonic dystrophy.Biochimica et Biophysica Acta 1096, 14-19
153 Vihola, A. et al. (2013) Altered expression andsplicing of Ca(2+) metabolism genes in myotonicdystrophies DM1 and DM2. Neuropathology andApplied Neurobiology 39, 390-405
154 Murphy, R.M. et al. (2013) Ca2+-dependentproteolysis of junctophilin-1 and junctophilin-2 inskeletal and cardiac muscle. Journal of Physiology591(Pt 3), 719-729
155 Toral-Ojeda, I., Aldanondo, G. and Vallejo-Illarramendi, A. (2013) Junctophilins and mu-calpain: partners in excitation–contractionuncoupling. Journal of Physiology 591(Pt 15),3679-3680
156 Andersson, D.C. et al. (2012) Leaky ryanodinereceptors in beta-sarcoglycan deficient mice: apotential common defect in muscular dystrophy.Skeletal Muscle 2, 9
157 Kendall, G.C. et al. (2012) Dantrolene enhancesantisense-mediated exon skipping in human andmouse models of Duchenne muscular dystrophy.Science Translational Medicine 4, 164ra160.
158 Altamirano, F. et al. (2013) Nifedipine treatmentreduces resting calcium concentration, oxidativeand apoptotic gene expression, and improves
muscle function in dystrophic mdx mice. PLoSONE 8, e81222
159 Matsumura, C.Y. et al. (2009) Diltiazem andverapamil protect dystrophin-deficient musclefibers of MDX mice from degeneration: a potentialrole in calcium buffering and sarcolemmal stability.Muscle & Nerve 39, 167-176
160 Phillips, M.F. and Quinlivan, R. (2008) Calciumantagonists for Duchenne muscular dystrophy.Cochrane Database of Systematic Reviews 4,CD004571
161 Iwata, Y. et al. (2009) Dominant-negative inhibitionof Ca2+ influx via TRPV2 ameliorates musculardystrophy in animal models. Human MolecularGenetics 18, 824-834
162 Finsterer, J. and Cripe, L. (2014) Treatment ofdystrophin cardiomyopathies. Nature ReviewsCardiology 11, 168-179
163 Kwon, H.W. et al. (2012) The effect of enalapriland carvedilol on left ventricular dysfunction inmiddle childhood and adolescent patients withmuscular dystrophy. Korean Circulation Journal42, 184-191
164 Shareef, M.A., Anwer, L.A. and Poizat, C. (2014)Cardiac SERCA2A/B: therapeutic targets for heartfailure. European Journal of Pharmacology 724, 1-8
165 Morine, K.J. et al. (2010) Overexpression ofSERCA1a in the mdx diaphragm reducessusceptibility to contraction-induced damage.Human Gene Therapy 21, 1735-1739
166 Katsetos, C.D., Koutzaki, S. and Melvin, J.J. (2013)Mitochondrial dysfunction in neuromusculardisorders. Seminars in Pediatric Neurology 20,202-215
167 Buyse, G.M. et al. (2011) Idebenone as a novel,therapeutic approach for Duchenne musculardystrophy: results from a 12 month, double-blind,randomized placebo-controlled trial.Neuromuscular Disorders 21, 396-405
168 Kotlikoff, M.I. (2007) Genetically encoded Ca2+
indicators: using genetics and molecular design tounderstand complex physiology. Journal ofPhysiology 578(Pt 1), 55-67
169 Mank, M. et al. (2008) A genetically encodedcalcium indicator for chronic in vivo two-photonimaging. Nature Methods 5, 805-811
170 Rochefort,N.L. andKonnerth,A. (2008)Geneticallyencoded Ca2+ sensors come of age. NatureMethods 5, 761-762
171 Schoenenberger, P., Scharer, Y.P. and Oertner, T.G.(2011) Channelrhodopsin as a tool to investigatesynaptic transmission and plasticity. ExperimentalPhysiology 96, 34-39
expert reviewshttp://www.expertreviews.org/ in molecular medicine
22Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies

Further reading, resources and contacts
Disease pages in OMIM:
Duchenne muscular dystrophy, http://www.omim.org/entry/310200
Becker muscular dystrophy, http://www.omim.org/entry/300376
LGMD2A muscular dystrophy, http://www.omim.org/entry/253600
Myotonic dystrophy 1, http://www.omim.org/entry/160900
Myotonic dystrophy 2, http://www.omim.org/entry/602668
ClinicalTrialsGov offers a complete list of worldwide clinical trials on muscular dystrophies and other medicalconditions: http://clinicaltrials.gov/
The Muscular Dystrophy Association provides information on muscular dystrophies as well as helpful resourcesfor patients: http://mda.org/
Treat Neuromuscular Disorders (TREAT-NMD) provides ample information about muscular dystrophies and newtherapeutic developments: http://www.treat-nmd.eu/
Features associated with this article
FigureFigure 1. Representation of calcium signalling dynamics in the muscle fibre.
TablesTable 1. Calcium-related mechanisms affected in muscular dystrophies.Table 2. Treatments targeting calcium homeostasis and mitochondrial function in muscular dystrophies.
Citation details for this article
Ainara Vallejo-Illarramendi, Ivan Toral-Ojeda,Garazi Aldanondo and Adolfo López de Munain (2014) Dysregulation of calcium homeostasis inmuscular dystrophies. Expert Rev. Mol. Med. Vol. 16, e16, October 2014, doi:10.1017/erm.2014.17
expert reviewshttp://www.expertreviews.org/ in molecular medicine
23Accession information: doi:10.1017/erm.2014.17; Vol. 16; e16; October 2014
© Cambridge University Press 2014
Dys
regulationofca
lcium
homeo
stas
isin
mus
culardys
trophies